Embed Size (px)
Citation preview

JACC Vol. 5, No. IJanuary 1985:113S-9S
Assessment of Aortic Blood Flow Velocities With Continuous WaveDoppler Ultrasound in the Neonate and Young Child
LIV HATLE, MD
Trondheim, Norway
ll3S
Aortic flow velocities can be recorded with pulsed orcontinuous wave Doppler ultrasound. In the absence ofobstruction or regurgitation, changes in flow can be assessed and stroke volume obtained. Continuous waveDoppler ultrasound has the advantage that there is nolimit to the velocities that can be recorded. In left ventricular outflow obstruction and coarctation, the pressure drop across these can be calculated from increasesin maximal velocity using a modification of the Bernoulliequation. Other systolic high velocity jets such as mitral
Blood flow velocities in the aorta in children and neonatescan easily be recorded with continuous wave Doppler ultrasound. With the continuous wave Doppler technique,velocities are recorded all along the ultrasonic beam. Although there is the advantage that high velocities can berecorded, a signal cannot be localized in depth with continuous wave Doppler techniques. Pulsed Doppler ultrasound has the advantage that a signal can be localized indepth, but there is a limit to the velocities that can berecorded.
From the velocity of blood flow, it is possible to assesschanges in volume flow. An increase in flow causes anincrease in velocity, and velocity decreases with a decreasein flow. By measuring both the velocity of flow and thecross-sectional area, estimation of volume flow is possible(1-3). The shape of the velocity curve is, in addition tovolume flow, influenced by left ventricular function and thecapacity and resistance in the systemic circulation (4,5).Until recently, the clinical information this may give hasbeen utilized little (6,7). Such assessment of aortic bloodflow velocities can be performed equally well with pulsedand continuous wave Doppler ultrasound.
Obstruction to flow causes much larger increases in velocity than are seen with increases in flow. The increase in
From the Section of Cardiology. Regional Hospital, and Departmentof Medicine, University of Trondheim, Trondheim, Norway.
Address for reprints: Liv Hatle, MD, Section of Cardiology, RegionalHospital, Trondheim, Norway.
© 1985 by the American College of Cardiology
regurgitation or ventricular septal defect may also berecorded with continuous wave Doppler ultrasound fromthe suprasternal notch, but they can be distinguishedfrom aortic flow velocities by their timing and durationwhen the flow signals are recorded together with theelectrocardiogram and phonocardiogram. In aortic regurgitation, reversal of flow across the aortic valve indiastole can be shown and with high velocity in the regurgitant jet.
(} Am Coil Cardiol 1985;5:1135-95)
velocity is related to the pressure drop across the obstructionand can be calculated from the maximal velocity using amodified Bernoulli equation (8). By recording maximal velocity in the ascending aorta, left ventricular outflow obstructions can be diagnosed and assessed (9). In obstructionsto blood flow velocities usually exceed the limit for mostpulsed Doppler systems, and to assess obstructions the continuous wave Doppler mode, therefore, is preferable. Aorticregurgitation is diagnosed by the continuous wave Dopplerultrasound recording across the aortic valve, while reversediastolic flow in the aorta in regurgitation and shunts is betterrecorded with pulsed Doppler ultrasound (10).
InstrumentationStand-alone Doppler systems. A separate continuous
wave Doppler system can be used. Equipment with carrierfrequencies of 2 to 5 MHz is commercially available. Thehigher frequencies are in instruments intended for peripheralvascular disease and these can be used for neonates andinfants. Instruments with the lower frequencies can be usedin older children as well as in infants and neonates. Theoutput from the Doppler system can be recorded either withspectral analysis where all the frequencies in the signal areseen or with analog curves giving the outline of the spectralcurve or the mean of the frequencies in the signal. Even inchildren in whom good Doppler signals are easily obtained,the spectral display has clear advantages. It provides a muchbetter visual documentation of the Doppler signal recorded,
0735-1097/85/$3.30

114S HATLEASSESSMENT OF AORTIC BLOOD FLOW
JACC Vol. 5. No. IJanuary 1985:113S-9S
estimator artifacts are avoided and it is possible to distinguish between the various components of a mixed signal.
With a combined pulsed and continuous wave Dopplersystem, a signal recorded in the continuous mode can alsobe localized in depth by changing to the pulsed mode. Thiscan help to ascertain the origin of signal recorded withcontinuous wave Doppler ultrasound (10).
Combined Doppler and two-dimensional echocardiography. The combination of continuous wave and pulsedDoppler ultrasound with two-dimensional imaging makeslocalization of flow signals easier and quicker and avoidsambiguity, especially in patients with complex lesions (11).It is most helpful when recording from apical or subcostalpositions because from the suprasternal notch and right sternal border, access is often easier with a smaller separateDoppler transducer than a larger one for combined imagingand Doppler ultrasound. Simultaneous imaging and continuous wave Doppler ultrasound is especially useful in neonates and infants in whom minimal movements may changethe site of recording completely.
Electrocardiography and phonocardiography. WhenDoppler ultrasound is used without imaging, correct identification of a flow signal is essential. This can be obtainedby recording the valve movements, electrocardiogram andphonocardiogram simultaneously with the Doppler signal(Fig. 4). This can be useful also if continuous wave Dopplerultrasound is used with imaging, as when two high velocityjets of similar direction are present.
aortic flow velocity
Aortic Flow VelocityDoppler recording technique. Flow velocity in the as
cending aorta can be recorded from the suprasternal notch,a high right parasternal position, the apex and a subcostalposition. In the descending aorta, flow velocities are bestrecorded from the suprasternal notch.
The Doppler ultrasound signal contains the frequencyshift of the backscattered ultrasound. The velocity is obtained from the frequency shift by the Doppler equation thatincludes the cosine of the angle between the ultrasound beamand the velocity. With angles between 20 and 0°, the cosinewill be from 0.94 to I and can, therefore, be disregarded.If the angle is larger and it is disregarded, velocity will beunderestimated. If ignored, an angle of 25 to 30° will causea 9 to 13% underestimation of velocity and with largerangles this underestimation increases rapidly. The audiosignal that represents the frequency shift is used to findwhere the angle to a flow signal is smallest; as the anglebecomes smaller, the signal becomes more high frequent.More than one position and beam direction should, therefore, be tried to find the signal with the highest frequencies,which will give the velocity closest to that present. Evidencein support of the technique is shown in studies on reproducibility (12,13) and simultaneous velocity and pressuremeasurements in obstructive lesions (8,9,14).
Angle correction. When Doppler ultrasound is used together with two-dimensional imaging, another possibility is
..... Il .., .ntl "
pulsed ~
aortic stenosis
CW Doppler Figure 1. Pulsed Doppler recording from a normalsubject (top) shows a narrow band of frequencies.By switching to the continuous wave (CW) mode,the signal also contains some lower frequencies. Inaortic stenosis (bottom), the continuous wave modeshows the high velocities exceeding the limit forthe pulsed mode which shows aliasing.

JACC Vol. 5, No.1January 1985:113S-9S
HATLEASSESSMENT OF AORTIC BLOOD FLOW
115S
to correct for the angle to the velocity as measured fromthe image. The drawbacks are that velocity may not beparallel to the imaged walls, the image is only two-dimensional so that there may be a considerable angle in the thirdplane that is not seen and the possibility of overestimationof velocity by angle correction is also introduced. A differentdirection of velocity from that assumed from the imageoccurs especially with flow through stenotic and regurgitantvalves, but perhaps not as often in infants and young children as in adults. Operating at an angle to flow also increasesthe error introduced by a certain angle. Therefore, an attemptto obtain alignment between ultrasound beam and velocityis preferred.
Pulsed versus continuous wave Doppler ultrasound.With aortic flow velocities within normal limits, there islittle difference between the use of pulsed and continuouswave Doppler ultrasound. With pulsed Doppler ultrasounda signal with a more narrow band of frequencies is obtainedand the maximal velocity may be little higher than thatobtained with continuous wave Doppler ultrasound in thesame direction because of a better signal to noise ratio withthe pulsed mode. The signal obtained with the continuouswave Doppler technique contains a larger variation of frequencies from all along the beam (Fig. 1). The best Dopplersignal is usually quicker to find with the continuous wavemode because various depths will not have to be checkedfor each beam direction. With increased flow or force ofejection, the velocity profile in the aorta may no longer beflat and, thus, the pulsed mode will be more sensitive tothe location of the sample volume within the cross-sectionalarea of the aorta (15). For practical purposes, however, theinformation obtained with pulsed and continuous wave Doppler recording from the aorta is similar when there is noleft ventricular outflow obstruction.
Obtaining cardiac output. In the absence of aortic obstruction or regurgitation, aortic flow velocity can be usedto obtain cardiac output. Integrating the area under the velocity curve and multiplying with the cross-sectional areaof flow gives the stroke volume. Good correlation with othermethods has been shown (1-3,16,17). The critical measurement in children as well as in adults is the diametermeasurement of the aorta. Other problems include underestimation of velocity and the fact that the assumption thatthe velocity profile is flat may not always hold, especiallywhen there is increase in flow. With the good reproducibilityshown for aortic flow velocity measurements, relative changesin velocity can be useful in assessing changes in flow.
Obstruction to FlowWith obstruction to blood flow, the maximal velocity of
flow across the obstruction increases. The increase is related
to the drop in pressure drop. With a modified Bernoulliequation, the pressure drop can be calculated from the increase in the maximal velocity (8,9).
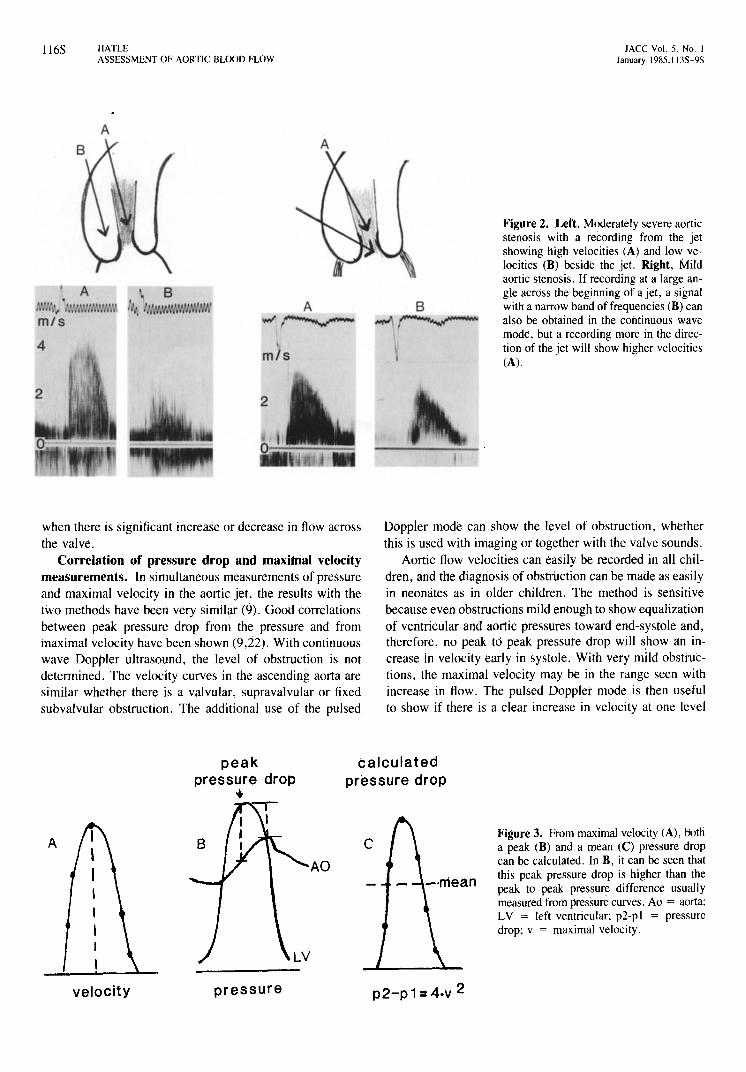
Obstruction to flow produces a high velocity jet thatextends for some centimeters beyond the obstruction (18).Along the jet, a gradual decrease in velocity occurs, andbeside it there may be disturbed flow with low velocitiesand of various directions. The Doppler signal from the beginning of a jet is pure with high frequencies only; alongthe jet it is more mixed with lower frequencies. Beside thejet, only low frequencies are present, but these are often ofhigh intensity. To obtain the maximal velocity, the recordingmust be made from the jet and at a small angle. The audiosignal is again used to find the highest frequencies (Fig. 2).Underestimation of velocity will result in a larger underestimation of the pressure drop because the velocity is squaredwhen calculating the pressure drop.
Velocity before an obstruction is often so low that it canbe ignored in the calculation, but if it is increased it mustbe considered. With continuous wave Doppler ultrasound,the velocity patterns from both sides of the valves will bepresent in the signal, and with spectral display they may beclearly separated. For flow across the aortic valve, the velocity in the left ventricular outflow tract can usually berecorded separately with the continuous wave Doppler technique with a slight change in beam direction from an apicalor subcostal position. The velocity below the valve can alsobe recorded with the pulsed Doppler technique.
Left Ventricular Outflow ObstructionsCalculation of pressure drop. It was shown experi
mentally (19-21) that pressure drop calculated from maximal velocity across an obstruction comes close to that recorded by pressure except for very small orifice sizes «0.1cm2
) where underestimation of lower pressure drops occurs.To date, practical experience has been that even in neonateswith severe aortic stenosis, a small orifice size has not ledto underestimation of the pressure drop.
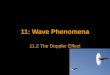
From the maximal aortic jet velocities recorded with continuous wave Doppler ultrasound, a peak pressure drop canbe calculated. This corresponds to the instantaneous peakpressure difference during systole (Fig. 3). With use ofspectral display and fluid-filled catheters, the delay in thevelocity compared with the pressure is so small that a meanpressure drop can also be calculated. With maximal frequency estimation, the velocity will be a little more delayedand may lead to some underestimation of the mean pressuredrop. The course of the velocity curve shows whether thepressure drop is sustained during systole or if it decreasesrapidly as is the case in mild obstructions. The velocitycurve then shows an early peak and a rather low velocityin late systole. This helps in assessing severity, especially
II6S HATLEASSESSMENT OF AORTIC BLOOD FLOW
JACC Vol. 5, No. IJanuary 1985: 113S-9S
A
Figure 2. Left, Moderately severe aorticstenosis with a recording from the jetshowing high velocities (A) and low velocities (B) beside the jet. Right, Mildaortic stenosis. If recording at a large angIe across the beginning of a jet, a signalwith a narrow band of frequencies (B) canalso be obtained in the continuous wavemode, bui a recording more in the direction of the jet will show higher velocities(A).
A
m/s
when there is significant increase or decrease in flow acrossthe valve.
Correlation of pressure drop and maxihial velocitymeasurements. In simultaneous measurements of pressureand maximal velocity in the aortic jet, the results with thetwo methods have been very similar (9). Good correlationsbetween peak pressure drop from the pressure and frommaximal velocity have been shown (9,22). With continuouswave Doppler ultrasound, the level of obstruction is notdetermined. The velocity curves in the ascending aorta aresimilar whether there is a valvular, supravalvular or fixedsubvalvular obstruction. The additional use of the pulsed
Doppler mode can show the level of obstruction, whetherthis is used with imaging or together with the valve sounds.
Aortic flow velocities can easily be recorded in all children, and the diagnosis of obstruction can be made as easilyin neonates as in older children. The method is sensitivebecause even obstructions mild enough to show equalizationof ventricular and aortic pressures toward end-systole and,therefore, no peak to peak pressure drop will s,how an increase in velocity early in systole. With very mild obstructions, the maximal velocity may be in the range seen withincrease in flow. The pulsed Doppler mode is then usefulto show if there is a clear increase in velocity at one level
peakpressure drop,.
calculatedpressure drop
A c
-·mean
Figure 3. From maximal velocity (A), botha peak (B) and a mean (C) pressure dropcan be calculated. In B, it can be seen thatthis peak pressure drop is higher than thepeak to peak pressure difference usuallymeasured from pressure curves. Ao = aorta;LV = left ventricular; p2-p I = pressuredrop; v = maximal velocity.
velocity pressure p2-p1=4.v 2

JACC Vol. 5, No. IJanuary 1985: 113S-9S
HATLEASSESSMENT OF AORTIC BLOOD FLOW
117S
or if it is high all the way as when flow is increased. Thismay also be seen wpen the continuous wave poppler technique is used with a spectral display.
Differentiation of aortic jet and oth~r high velocityjets. A' high velocity jet toward the transducer in systolerecorded from the suprasternal notch will most often be dueto valvular or fixed subvalvular aortic stenosis. It is unusualfor other high v~locity jets to have a clearly superior d~rec
tion toward the suprasternal notch, but it occurs occasionallywith both pulmonary stenosis and mitral regurgitation. ItCan also occur with a ventricular septal defect jet, and tricuspid regurgitation may show a direction toward a highright parasternal position. To avoid possible confusion withother high velocity jets, even if this is rare, the timing ofthe flow signal should be recorded either by electrocardiography and comparison with the other flow signals or byalso recording the valve movements or the phonocardiogram. Figure 4 shows the high velocity of ajet due tomitral regurgitation recorded from the suprasternal notchand the longer duration of the regurgitation than of flowthrough the' aortic valve. With timing, an aortic jet can,therefore, be distinguished from other high velocity jets.
Clinical applications. The easy diagnosis of aortic obstruction together with adequate assessment of severity makesthe Dopp'ler ultrasound a useful technique. It helps in theplanning of follow-up, timing of surgery, in postoperativeevaluation and further follow-up. In older children, it is alsopossible to record maximal velocity in the aorta and obtaina pressure drop during exercise. The method should also be
CW Doppler
useful in obtaining more information on the progression ofthe obstruction in aortic stenosis. The experience in patientsfollowed up to 6 years has been that none of the patientswith mild to moderate lesions have shown signs of progression of stenosis. In patients with moderately severe obstruction, the pressure drop has ~Iso changed little duringfollow-up studies despite agreat change in body surfacearea, but one patient became symptomatic. In the patientswith the highest pressure drop, these were recorded alreadyon the first examination and with little change during followup study. Some of these patients have become symptomatic.
Aortic RegurgitationDifferentiation from otller conditions. With continu
ous wave Doppler echocardiography and the beam directionacross the aortic valve, the high velocity of aortic regurgitation can be recorded in diastole. With both obstructionand regurgitation, the beam direction to record these may
Figure 4. A, A high velocity jet toward the transducer in thesuprasternal notch. B, Normal aortic ~ow velocity with aortic valveopening (A.,) and closure (Ae). The timing of the valve movementsshows that the high velocity jet starts at the beginning of the firstheart sound and continues past aortic closure. It represents mitralregurgitation which could also be recorded from the apex (C). Me= mitral valve closure; Mo = mitral valve opening; dotted lines= start and end of high velocity jet.
A suprasternal notch
r~~I
B,", .
'•••'....\\ " 'I', U." tn' \itt'.'1 ' nn f' I -I,tl itII • ,.ff"
apex c
t
Me
.1 •
m/s
4
2
. .'->cw-.J~---:;~'LJ~·"_\=v--.;:::ll~~W~ _----::rI~~--:;::::K..:._o/I_·~--.:.:._''w_':>:........;;;:::._.:,_...
•Ao Ac

118S HATLEASSESSMENT OF AORTIC BLOOD FLOW
JACC Vol. 5, No. IJanuary 1985: II3S-9S
be similar or may differ. The two jets will be continuous,but they will have opposite directions. With continuouswave Doppler echocardiogrllphy and the beam passing theaortic orifice, flow velocities from the coronary arteries mightalso be recorded in diastole. This is unusual, prohably because flow in these arteries will be at an almost transverseangle. These two diastolic flow velocity patterns can alsobe distinguished by the high velocity in the aortic regurgitation compared with the low velocity and sound of normalflow from the coronary arteries. Pulmonary regurgitationwill also show lower velocities unless there is severe pulmonary hypertension with diastolic pressure in the pulmonary artery approaching that in the aorta. The diagnosis ofaortic regurgitation is, therefore, specific and it is sensitiveespecially when aortic flow velocities are recorded from theapex. Aortic regurgitation is easily distinguished from leftventricular inflow obstruction by the higher velocity and thelonger duration of the regurgitation.
Degree of regurgitation. This has been assessed withpulsed Doppler ultrasound from its extension in the leftventricle and from the reverse diastolic flow velocities inthe descending or ascending aorta (23-28). For the latter,both continuous wave and pulsed Doppler ultrasound havebeen used, but the pulsed Doppler mode is probably preferable. With continuous wave Doppler ultrasound, the intensity of the signal from the regurgitation compared withthat of forward flow can give some indication of the severity,as can the decrease in velocity of the regurgitation duringdiastole (11). With the combined use of pulsed and continuous wave Doppler ultrasound, semiquantitation of aorticregurgitation can be obtained. Reverse diastolic flow is alsoseen in patent ductus arteriosus, shunts and in aorticopulmonary window. The first two conditions can be distinguished from aortic regurgitation by showing reverse diastolic flow in the descending but not ascending aorta. Withthe pulsed Doppler technique, they can all be distinguishedfrom regurgitation by showing the level where reversal offlow starts.
Coarctation of the aorta. With continuous wave Doppler recording from the suprasternal notch toward the descending aorta, the high velocity jet across a coarctation canbe recorded. This is easily done in patients with mild tomoderately severe coarctation and in residual lesions aftersurgery. In severe coarctation, the jet may be more difficultto find. This may be due, in part, to a more eccentric jetand, in part, to less flow because the major flow may bethrough collateral vessels. In these patients, combined Doppler ultrasound and two-dimensional imaging is especiallyhelpful. A Small angle to the jet can usually be obtainedand the pressure drop across the coarctation can be calculated. This has been helpful in the assessment of coarctation,especially after surgery. With combined Doppler ultrasoundand two-dimensional imaging the presence of an obstructioncan be excluded.
Other ChangesWith heart failure, changes in aortic flow velocity curves
are seen in children as well as in adults. Clear respiratorychanges are seen in constrictive pericarditis (10). In hypertrophic cardiomyopathy, the increased ejection in early systole is shown by an early peak velocity and low velocitiesin late systole (29). Similar changes can be seen in severemitral regurgitation (30), but left ventricular ejection timeis then shortened, whereas in obstructive cardiomyopathyit is prolonged.
Value and LimitationsThe use of continuous wave Doppler ultrasound to record
aortic flow velocities is quite easy in neonates and children.The method is inexpensive and measurements can easily berepeated. Assessment of aortic stenosis and aortic flow velocities to estimate volume flow can be performed with astand-alone continuous wave Doppler instrument. Combined with imaging, the information may be obtained quickerin some patients and more complete information on associated lesions can be provided.
The main drawback is the possibility of underestimationof the velocity by recording at an angle that is too large.Being aware of this and using various transducer positionsand directions, current experience indicates that significantunderestimation can be avoided, especially in children andneonates. The other drawback is possible confusion withother high velocity jets if care is not taken to identify theflow signal by recording the aortic valve's movements orthe phonocardiogram as described. The level of obstructioncannot be shown without the use of pulsed Doppler ultrasound or two-dimensional imaging, or both.
With some pulsed Doppler systems, higher velocities canbe recorded in the pulsed mode (10,31). This makes itpossible to assess obstructions with the pulsed Doppler technique, especially in infants and children in whom the flowsignals are recorded at a low depth. Continuous wave Doppler ultrasound has the advantage of being easier to usebecause it is quicker to find both a jet and the optimaldirection to the jet.
There are no known hazards. The ultrasonic effect ofDoppler instruments is higher than in instruments used forimaging and higher for continuous wave than for pulsedDoppler echocardiography. The level can be up to 5 to 10%of that for therapeutic use. To date, biologic effects havenot been demonstrated for ultrasound used for diagnosticpurposes, but further research is necessary to exclude this(32).
Conclusions. With continuous wave Doppler echocardiography, aortic stenosis, regurgitation and coarctation canbe diagnosed and assessed. In the absence of obstruction or

JACC Vol. 5, No.1January 1985: 1I3S-9S
HATLEASSESSMENT OF AORTIC BLOOD FLOW
1198
regurgitation, aortic flow velocity can be used to assessaortic flow and changes in flow. In most cases, this information can be obtained with a stand-alone Doppler systemas easily as it can with a system combining Doppler ultrasound and two-dimensional imaging. But because the lattermay be better suited for evaluation of other congenital lesions and is necessary for complex lesions, this is likely tobe preferred despite a higher cost. For measurements in theaorta, it should also be possible in combined systems to usea separate Doppler transducer unless the combined transducer becomes much smaller and easier to use from the suprasternal notch.
References1. MagninPA, StewartJA, Myers S, von RammO, KissloJA. Combined
Doppler and phased-array echocardiographic estimation of cardiacoutput. Circulation 1981;63:388-92.
2. Alverson DC, Eldridge M, Dillon T, Yabek SM, Berman W. Noninvasive pulsed Doppler determination of cardiac output in neonatesand children. J Pediatr 1982;101:46-50.
3. Valdes-Cruz LM. Sahn DJ. Two-dimensional echo Doppler for noninvasive quantitation of cardiac flow: a status report. Mod ConceptsCardiovasc Dis 1982;51: 123-7.
4. Elzinga G. Westerhof N. Pressure and flow generated by the leftventricle against different impedances. Circ Res 1973;32: 178-86.
5. Murgo JP. Westerhof N, Giolma JP, Altobelli SA. Manipulation ofascending aortic pressure and flow wave reflections with the Valsalvamaneuver: relationship to input impedance. Circulation 1981;63:122-32.
6. Buchtal A. Hanson C. Peisach AR. Transcutaneous aortovelography.Potentially useful technique in management of critically ill patients.Br Heart J 1976;38:451-6.
7. Elkayam U. Gardin JM. Berkley R. Hughes CA, Henry WL. The useof Doppler flow velocity measurement to assess the hemodynamicresponse to vasodilators in patients with heart failure. Circulation1983;67:377-83.
8. Hatle L. Brubakk A. Tromsdal A. Angelsen B. Noninvasive assessment of pressure drop in mitral stenosis by Doppler ultrasound. BrHeart J 1978;40:131-40.
9. Hatle L. Noninvasive assessment and differentiation of left ventricularoutflow obstruction with Doppler ultrasound. Circulation 1981 ;64:381-7.
10. Hatle L, Angelsen B. Pulsed and continuous wave Doppler in diagnosis and assessment of various heart lesions. In: Doppler Ultrasoundin Cardiology. Philadelphia: Lea & Febiger. 1982:105-9.
II. Hatle L. Combined 2D-echo and Doppler compared to Doppler withoutimaging. In: Spencer M. ed. Cardiac Doppler Diagnosis, The Hague:Martinus Nijhoff, 1983:327-35.
12. Gisvold SE, Brubakk AO. Measurement of instantaneous blood-flowvelocity in the human aorta using pulsed Doppler ultrasound. Cardiovasc Res 1982;16:26-33.
13. Gardin JM. Dabestani A. Matin K, Allfie A. Russell D. Henry WL.Are Doppler aortic blood flow velocity measurements reproducible?Studies on day-to-day and inter-observer variability in norr.1al subjects(abstr). J Am Coli Cardiol 1983;1:657.
14. Holen J, Aaslid R. Landmark K. Simonsen S. Determination of pres-
sure gradient in mitral stenosis with a noninvasive ultrasound Dopplertechnique. Acta Med Scand 1976;199:455-60.
15. Falsetti HL. Carrol RJ, Swope RD, Chen CJ. Turbulent flow in theascending aorta in dogs. Cardiovasc Res 1983;17:427-36.
16. Goldberg SJ. Sahn DJ, Allen HD. Valdes-Cruz LM, Hoenecke H,Carnahan Y. Evaluation of pulmonary and systemic blood flow by 2dimensional Doppler echocardiography using fast Fourier transformspectral analysis. Am J Cardiol 1982;50:1394-400.
17. Stevenson JG, Kawabori I. Noninvasive determination of pulmonicto systemic flow ratio by pulsed Doppler echo (abstr). Circulation1982;66(suppl; 11):11-232.
18. Hatle L. Maximal blood flow velocities-haemodynamic data obtained noninvasively with CW Doppler. Ultrasound Med Bioi1984;10:225-37.
19. Holen J. Aaslid R, Landmark K. Simonsen S. 0strem T. Determination of effective orifice area in mitral stenosis from noninvasiveultrasound Doppler data and mitral flow rate. Acta Med Scand1977;201:83-8.
20. Takeda p. Kwan OL. Water J. Low R, DeMaria AN. Determinationof peak aortic pressure gradient by continuous wave Doppler measurements of maximal blood flow velocity, experimental validation(abstr). J Am Coli Cardiol 1983;1:657.
21. Valdes-Cruz LM. Sahn DJ, Horowitz S. et al. Does two-dimensionalecho Doppler measurement of maximal flow velocity across a restrictive orifice provide an estimate of pressure gradient? Validation studiesin an open chest animal model (abstr). J Am Coli CardioI1983;1:657.
22. Lima CO. Sahn DJ. Valdes-Cruz LM. et al. Prediction of the severityof left ventricular outflow tract obstruction by quantitative twodimensional echocardiographic Doppler studies. Circulation 1983;68:348-54.
23. Ciobanu M, Abbasi AS. Allen M. Hermer A. Spellberg R. PulsedDoppler echocardiography in the diagnosis and estimation of severityof aortic insufficiency. Am J Cardiol 1982;49:339-43.
24. Boughner DR. Assessment of aortic insufficiency by transcutaneousDoppler ultrasound. Circulation 1975;52:874-9.
25. Sequeira RF, Watt J. Assessment of aortic regurgitation by transcutaneous aortovelography (abstr). Br Heart J 1977;39:929.
26. Quinones MA. Young 18. Waggoner AD. Ostojic MC. Ribeiro LGT.Miller RR. Assessment of pulsed Doppler echocardiography in detection and quantification of aortic and mitral regurgitation. Br HeartJ 1980;44:612-20.
27. Hatteland K, Semb B. Assessment of aortic regurgitation by meansof pulsed Doppler ultrasound. Ultrasound Med Bioi 1982;8: 1-5.
28. Diebold B. Peronneau p. Blanchard D. et al. Noninvasive quantification of aortic regurgitation by Doppler echocardiography. Br HeartJ 1983;49:167-73.
29. Boughner DR, Shield RL. Persaud lA. Hypertrophic obstructive cardiomyopathy. Assessment by echocardigraphy and Doppler ultrasoundtechniques. Br Heart J 1975;37:917-23.
30. Nichol PM, Boughner DR. Persaud JA. Noninvasive assessment ofmitral regurgitation by transcutaneous Doppler ultrasound. Circulation1976;54:656-61.
31. Stevenson JG. Noninvasive measurement of high blood flow velocityat depth using a pulsed Doppler system. In Ref II.
32. The Committee on Bioeffects of the American Institute of Ultrasoundin Medicine. Biological effects of ultrasonic energy on living material.Ultrasound Med BioI 1976;2:351.

















![Doppler spreading of internal gravity waves by an inertia-wave …maeresearch.ucsd.edu/nomura/papers/JGRO_JCV_08.pdf · DOPPLER SPREADING OF INTERNAL WAVES 2of14 C05018 [13] The numerical](https://img.pdfslide.us/doc/110x75/5f3ad4d23fa0830c982b39a7/doppler-spreading-of-internal-gravity-waves-by-an-inertia-wave-doppler-spreading.jpg)









