Embed Size (px)
Citation preview

1
Assessment of AACN Baccalaureate Nursing Education Curriculum
Model in the People’s Republic of China: A Transcultural Explorative Study
Yu Xu
Debra C. Davis [email protected]
Carol Clements (deceased)
University of South Alabama College of Nursing, Mobile, Alabama
Zhaomin Xu [email protected]
Zhengzhou University, Zhengzhou, P. R. of China
2
Abstract
This study examines the relevance of The Essentials of Baccalaureate Education for Professional
Nursing Practice (American Association of Colleges of Nursing [AACN], 1998) as a guide for
baccalaureate nursing curriculum development in the People’s Republic of China. A Likert-type
survey was developed to measure Chinese nurse educators’ perceptions regarding the 21 key
concepts extracted from The Essentials document in both the present curriculum and an ideal
curriculum across three dimensions: importance, cultural relevance, and extent of exposure.
Surveys were sent to all known baccalaureate nursing programs in China (N = 22) with a 50%
return rate. Descriptive statistical analyses supported the universality of the majority of the 21
key concepts from The Essentials document. Some of the concepts, however, were not as readily
transferable due to differences in the Chinese sociopolitical and cultural contexts for
baccalaureate nursing education. Findings from this study lend support for the potential global
relevance of The Essentials document. Additional transcultural and comparative studies are
recommended to further test the relevance of The Essentials document in other cultures.
Meanwhile, international nurse educators need to be aware of the possible limits of adopting The
Essentials document without values clarification, critical discrimination, and adaptation to their
home cultures.
[Key words : China, American Association of Colleges of Nursing, baccalaureate nursing
education, curriculum model/framework]
3
Assessment of AACN Baccalaureate Nursing Education Curriculum
Model in the People’s Republic of China: A Transcultural Explorative Study
This study examines the perceived relevance of The Essentials of Baccalaureate
Education for Professional Nursing (The Essentials hereafter, American Association of Colleges
of Nursing [AACN], 1998) to curriculum development for baccalaureate nursing education in the
People’s Republic of China. Similar to the United States, China has a multi- tier nursing
education system consisting of programs at the secondary, associate, baccalaureate, and graduate
levels (Xu, Xu, & Zhang, 2000). To a large extent, baccalaureate nursing education is perceived
as the pinnacle of nursing education in China. There are only about 10 master’s programs in the
country and the first doctoral program is still in the planning stage.
Chinese baccalaureate nursing education has been expanding rapidly since the restoration
of the first five-year program at Tianjin Medical College (now Tianjin Medical University) in
1983. Prior to this time there was a 30-year abolition of collegiate nursing education in the
country. Accurate statistics on the actual numbers of baccalaureate nursing programs in China
are difficult to obtain because the administrative control of baccalaureate nursing programs was
delegated to provinces in the last few years. Published sources have reflected this challenge. For
example, there were 18 baccalaureate nursing programs in 1998 according to Chang (1999). Just
one year later in 1999, Li (2001) reported 67 programs. However, the vice-president of the
Chinese Nursing Association could only identify 22 programs in existence in spring 2000
(Guifang Guo, personal communication, February 22, 2000).
Following in the footsteps of medical education, the Chinese nursing education has
adopted the medical model to construct curricula (Xu, Xu, & Zhang, 2000). This model relies
heavily on knowledge of pathophysiology, pharmacology, and medical interventions with an
4
emphasis on illness care rather than prevention. Recent reforms in the nursing education system
led to on-going debates on baccalaureate nursing curricula. The tenor of these debates indicate
that Chinese nurse educators are interested in restructuring the baccalaureate nursing curriculum
by using a nursing model (Shen, 1998, 2000). For Chinese nurse educators, it is logical that the
initial step to develop this new nursing curriculum framework is to examine what is available
from other countries.
The Essentials Document
The Essentials serves as a blueprint for curricular development in baccalaureate nursing
education programs in the United States (AACN, 1998). This landmark document was first
released in 1986 after a two-year consensus building process that synthesized the input from
nurse educators, administrators, researchers, and clinicians across the country (Johnson, 1987).
In 1998, it was revised in light of the major changes in the health care system after its initial
publication. The document “provides a framework for developing, defining, and revising
baccalaureate nursing curricula” (AACN, 1998, p. i).
According to The Essentials, five components (domains) are essential for the
baccalaureate nursing curriculum: liberal education, professional values, core competencies, core
knowledge, and role development. Liberal education consists of course content from the arts,
sciences, and humanities that develop critical thinking skills and higher order problem-solving
skills. According to AACN (1998) “Liberal education is not a separate or distinct segment of
professional education, but an integrated educational experience” (p. 7).
Baccalaureate nursing programs must also structure learning experiences that facilitate
the development and internalization of professional nursing values. These values provide for
socialization into the professional nursing role and “support empathetic, sensitive, and
5
compassionate care for individuals, groups, and communities” (AACN, 1998, p. 9). Professional
nursing values include caring, altruism, autonomy, human dignity, integrity, and social justice,
with caring as a central concept to the practice of professional nursing.
Core competencies for the baccalaureate prepared nurse include critical thinking,
communication, assessment, and technical skills. These competencies, along with the core
knowledge of health promotion, risk reduction, and disease prevention, illness and disease
management, information and health care technologies, ethics, human diversity, global health
care, and health care systems and policy, are essential to the safe and comprehensive practice of
professional nursing.
Additionally, The Essentials outlines areas of role development for the baccalaureate
nurse. These roles include provider of care, designer/manager/coordinator of care, and member
of a profession. Grounded in the Western philosophy, values, and assumptions, The Essentials
has been well accepted and integrated into educational programs that prepare baccalaureate
nurses in the United States.
A systematic literature review through the Cumulative Index to Nursing and Allied
Health Literature and Medline has generated two studies on the application of The Essentials in
curriculum assessment and revision in the United States (Elfrink & Lutz, 1991; Henley &
Anema, 1989). However, no studies were located that address the relevance of The Essentials in
a different cultural context, particularly its application to professional nursing education and
practice within the Eastern cultural and values system. With increasing numbers of nurses
traveling across international borders to practice nursing and to pursue additional education in
our global society, it is imperative to understand the differences in the philosophies, values, and
assumptions underlining baccalaureate nursing education worldwide.
6
Methods
A survey approach was used to obtain the perceptions of Chinese nurse educators
regarding the relevance of 21 key concepts extracted from The Essentials. In keeping with the
intent of The Essentials, this study was limited to baccalaureate nursing programs in China. The
principal author, in consultation with the research team and other experienced nurse researchers,
developed a three-part survey instrument.
The first part of the survey was designed to seek demographic information on the targeted
programs. The second part of the questionnaire was developed to obtain the perceptions of the
respondents regarding the importance, cultural relevance, and extent of exposure of the 21 key
concepts from The Essentials in their present as well as in an ideal nursing curriculum.
Respondents used a six-point Likert-type scale (with “6” as highest and “1” as lowest) for each
of the 21 key concepts extracted from the five domains of baccalaureate nursing education as
outlined in The Essentials. To ensure the accuracy of its intended meanings, each concept was
defined using direct quotations from The Essentials. The third part of the survey was designed to
elicit qualitative data concerning any additional areas that the Chinese nurse educators
considered important for inclusion in a baccalaureate nursing education curriculum. A content
analysis procedure was used to analyze the respondents’ comments.
The instrument was then translated into Chinese by the principal author. Linguistic
accuracy of the instrument was ensured by having it reviewed by two independent Chinese
health sciences scholars (one nurse educator and one medical doctor/educator) with extensive
knowledge of the Chinese healthcare system and teaching experience in nursing. The instrument
was then piloted on a Chinese visiting nurse educator in the United States. Refinement to the
7
instrument was made according to feedback received. Subsequent approval for the study was
obtained from the Institutiona l Review Board (IRB).
Following IRB approval, the surveys were mailed to the chief executive administrators
(i.e. deans or directors/chairs) of all known baccalaureate nursing programs in China (N = 22).
Each survey was completed by the chief executive administrators or by a designated faculty with
the most knowledge of the program’s curriculum. Eleven programs returned their completed
surveys (50% return rate). One of the returned surveys was improperly completed and therefore
was excluded from the study. Data from the remaining 10 valid surveys were then coded and
entered into SPSS 10.0. Descriptive statistical analyses were performed on the demographic and
quantitative data, and content analysis was used to analyze the qualitative data.
Findings
Demographics of the Baccalaureate Nursing Programs
All of the programs (N = 10) were established between 1985 and 1998. Of the 10
programs, nine programs also offered the associate degree in nursing; six had an associate-
bachelor mobility program; and three offered a master’s program. Nine of the programs had a 5-
year curriculum at the time of the survey. Annual admission of students to the freshmen class
ranged from 20 to 105 across all programs, with total enrollments ranging from 90 to 530. Two
of the programs were new and had not graduated any students. The remaining eight programs
reported having graduated from 35 to 277 students each. Full-time faculty ranged from 10 to 52.
Analysis of Quantitative Data
Part two of the survey employed a six-point Likert-type scale to obtain the perceptions of
Chinese nurse educators. Means and ranges are used to display the respondents’ perceptions
regarding the importance of the 21 key concepts from The Essentials in their present curriculum
8
and in an ideal curriculum, the cultural relevance of each concept to their present and ideal
curriculum, and the extent of exposure of each concept in their present and in an ideal
curriculum.
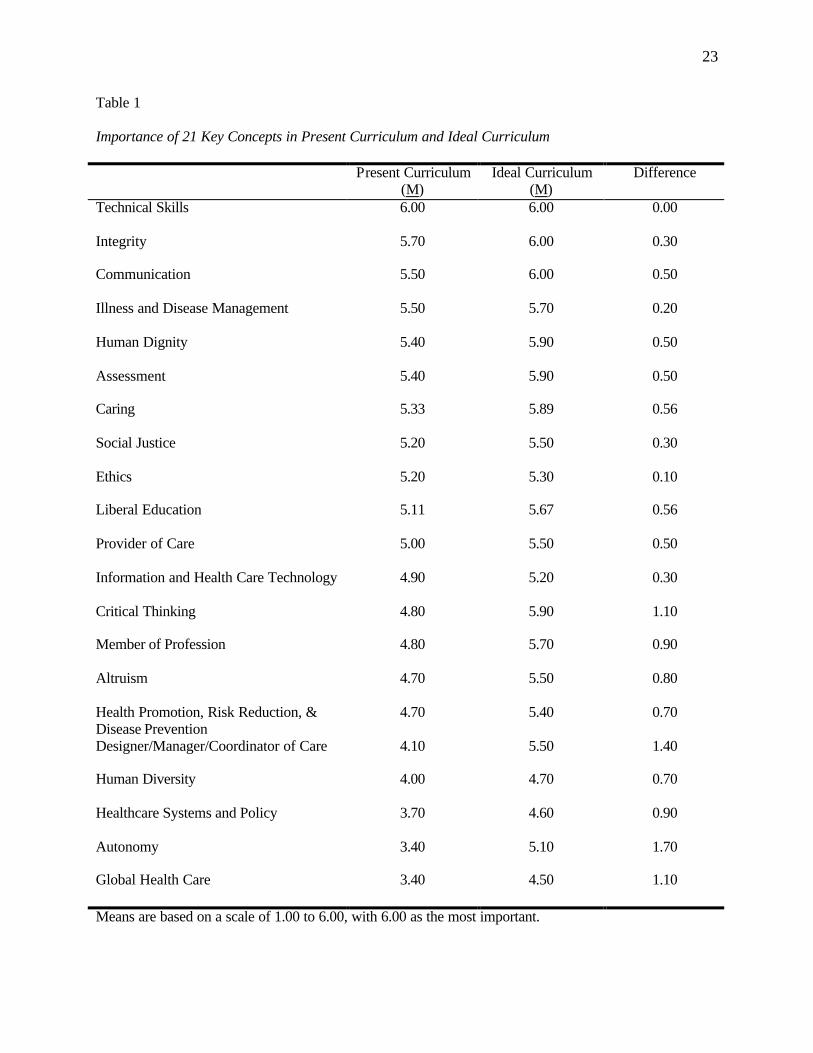
The dimension of “importance.” The means of the 21 key concepts for the dimension of
importance in the present curriculum ranged from 3.40 to 6.00 (Table 1). Concepts receiving the
highest ratings (5.0 and above) were “technical skills” (6.00) “integrity” (5.70),
“communication” (5.50), “illness and disease management” (5.50), “human dignity” (5.40),
“assessment” (5.40), “caring” (5.33), “social justice” (5.20), “ethics” (5.20), “liberal education”
(5.11), and “provider of care” (5.00). In contrast, “autonomy” (3.40), “global health care”
(3.40), “healthcare systems and policy” (3.70), “human diversity” (4.00), and
“designer/manager/coordinator of care” (4.10) were rated the lowest in importance in the present
curricula. For the ideal nursing curriculum, the means for the 21 key concepts ranged from 4.50
to 6.00. Only three of the concepts (“global health care,” 4.50; “healthcare systems and policy,”
4.60; and “human diversity,” 4.70) received mean scores below 5.00 (Table 1).
Mean scores for each concept were used to determine the amount of discrepancy or
difference between the perceptions of the nurse educators regarding the importance of each
concept in their present curriculum and perceptions of the same concept in an ideal curriculum.
As indicated in Table 1, concepts that had the least discrepancies were “technical skills” (0.00),
“ethics” (0.10), “illness and disease management” (0.20), “integrity” (0.30), and “social justice”
(0.30). The largest discrepancies were found for the concepts of “autonomy” (1.70),
“designer/manager/coordinator of care” (1.40), “global health care” (1.30), “critical thinking”
(1.30), and “healthcare systems and policy” (0.90).
9
Insert Table 1. Importance of 21 Key Concepts in Present Curriculum and Ideal Curriculum
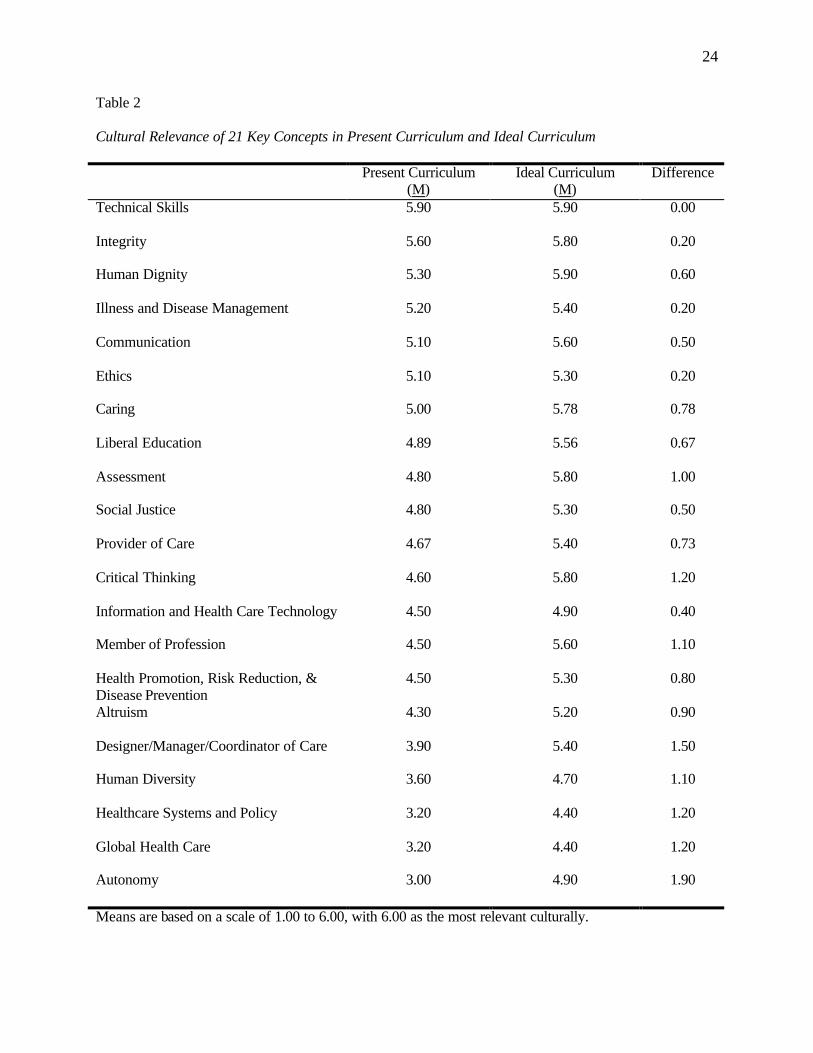
The dimension of “cultural relevance.” When the 21 key concepts were rated on the
dimension of cultural relevance in the present curriculum the mean scores ranged from 3.00 to
5.90. Concepts that received the highest mean scores were “technical skills” (5.90), “integrity”
(5.60), “human dignity” (5.30), “illness and disease management” (5.20), “communication”
(5.10), “ethics” (5.10), and “caring” (5.00). In contrast, “autonomy” (3.00), “global health care”
(3.20), “healthcare systems and policy” (3.20), “human diversity” (3.60), and
“designer/manager/coordinator of care” (3.90) were rated as having the least cultural relevance
in the present curriculum (Table 2). In the ideal curriculum, the means for the 21 key concepts
ranged from 4.90 to 5.90. Five concepts scored below 5.00 (“global health care,” 4.40;
“healthcare systems and policy, ” 4.40; “human diversity,” 4.70; “autonomy,” 4.90; and
“information and health care technology,” 4.90) (Table 2).
Concepts with the least discrepancies for cultural relevance between the present
curriculum and the ideal curriculum were “technical skills” (0.00), “member of profession”
(0.10), “integrity” (0.20), “healthcare systems and policy” (0.20), “ethics” (0.20),
“communication” (0.50), and “social justice” (0.50). By contrast, “autonomy” (1.90),
“designer/manager/coordinator of care” (1.50), “critical thinking” (1.20), “global health care”
(1.20), and “healthcare systems and policy” (1.20) presented the largest discrepancies (Table 2).
Insert Table 2. Cultural Relevance of 21 Key Concepts in Present Curriculum and Ideal Curriculum
10
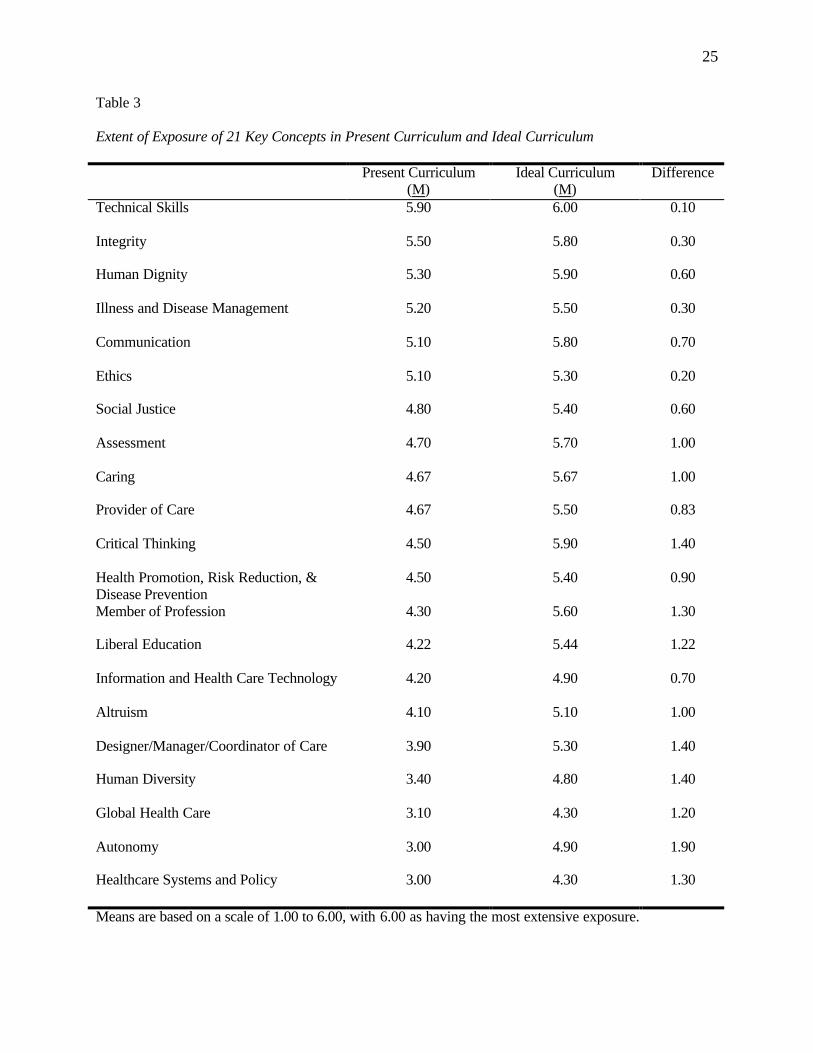
The dimension of “extent of exposure.” When the 21 key concepts were examined for the
dimension of extent of exposure in the present curriculum, mean scores ranged from 3.00 to
5.90. The highest means were for “technical skills” (5.90), “integrity” (5.50), “human dignity”
(5.30), “illness and disease management” (5.20), “communication” (5.10), and “ethics” (5.10).
The lowest scores were for “autonomy” (3.00), “global health care” (3.10), “healthcare systems
and policy” (3.20), “human diversity” (3.40), and “designer/manager/coordinator of care” (3.90)
(Table 3).
When discrepancies were calculated between the means for concept exposure in the
present curriculum and in an ideal curriculum, concepts that presented the least discrepancies
included “technical skills” (0.10), “ethics” (0.20), “integrity” (0.30), “illness and disease
management” (0.30), “human dignity” (0.60), and “social justice” (0.60). Consistent with
findings for the other two dimensions, concepts with the largest discrepancies were: “autonomy”
(1.90), “critical thinking” (1.40), “designer/manager/coordinator of care” (1.40), “human
diversity” (1.40), “member of profession” (1.30), “healthcare systems and policy” (1.30), “liberal
education” (1.22), and “global health care” (1.20) (Table 3).
Insert Table 3. Extent of Exposure of 21 Key Concepts in Present Curriculum and Ideal Curriculum
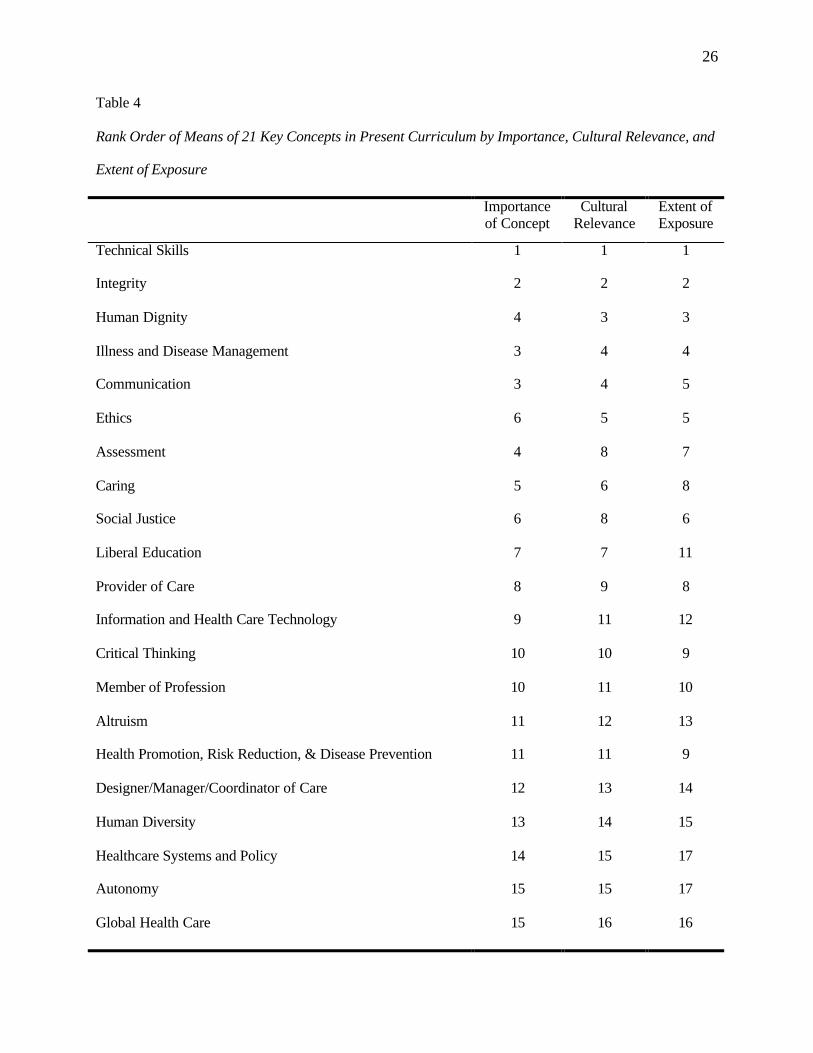
Discussion. Several observations merged from the data. First, there was a similar data
pattern or trend across the three measured dimensions in the present curriculum, indicating an
internal consistency across the measurements. Second, with the exception of “technical skills”,
the mean scores for concepts in the ideal curriculum were rated consistently higher than in the
present. These findings indicate that Chinese nurse educators were unsatisfied, in various
degrees, with the current status of 20 out of the 21 key concepts from The Essentials in their
11
present curricula. Third, the highest- and lowest-rated concepts and their respective rank orders
remained relatively stable across the three measured dimensions in both the present curriculum
and the ideal curriculum. Concepts that were perceived as most important, most culturally
relevant, and most exposed included “technical skills,” “integrity,” “communication,” “illness
and disease management,” and “human dignity,” indicating that these concepts have the highest
transferability to the Chinese baccalaureate nursing education. In contrast, “autonomy,” “global
health care,” “healthcare systems and policy,” “human diversity,” and
“designer/manager/coordinator of care” were ranked the lowest consistently in the present
curriculum, suggesting the greatest deficits in these areas (Table 4). Last, “autonomy”,
“designer/manager/coordinator of care,” “critical thinking,” “global health care,” “healthcare
systems and policy,” and “human diversity” consistently presented the largest discrepancies
between the present curriculum and the ideal curriculum across the three measured dimensions.
Insert Table 4. Rank Order of Means of 21 Key Concepts by Importance, Cultural Relevance, and Extent of Exposure in Present Curriculum
Analysis of Qualitative Data
Professional values. In addition to the existing concepts in the professional values
domain of The Essentials, the respondents recommended the following concepts as important
professional values to include in a baccalaureate nursing curriculum: “respect for patient
privacy,” “informed consent,” “initiative to help others,” “collectivism and team spirit,” “self
perfection,” and “nurses' rights and obligations.” Two of the suggested professional values (i.e.
“respect for patient privacy” and “informed consent”) were implied by the concepts of “human
dignity” and “autonomy” from The Essentials and mirrored the progress of the Chinese society
12
as a whole toward a genuine concern and respect for the individual. Other added concepts (i.e.
“initiative to help others,” “collectivism and team spirit,” “self perfection,” and “nurses' rights
and obligations”) reflected the preservation of traditional cultural values and the awakening of
the profession’s self-consciousness.
Core competencies. The respondents added the following concepts that further expanded
The Essentials competencies: “innovation and pioneering spirit,” “courage and vision,” “the
capability and perseverance to deal with adversary,” “pedagogical competence,” and
“management skills.” The emphasis on the affective domain of professional socialization from
the respondents might grow out of the concern for the maturity of the Chinese baccalaureate
nursing graduates to provide adequate patient care. Virtually all Chinese students in generic
baccalaureate nursing programs are traditional college females. Each is likely to be an only child
in the family as the result of China’s one-child family planning policy. Brought up in a
prevailingly over-protective family environment, many graduates from the generic baccalaureate
nursing programs have demonstrated deficits in their ability and skills of decision-making,
conflict resolution, collaboration, delegation, and leadership (Chan & Wong, 1999; Xu, Xu, &
Zhang, 2000).
In addition, the suggested additions of “pedagogical competence” and “management
skills” were a response to the dire demand for nursing faculty, the increasing need for patient
education and the administrative skills required of the baccalaureate nurse both in the clinical
setting and academic contexts.
Core knowledge. Additional knowledge areas identified by respondents as important
included “fundamentals of medical knowledge,” “epidemiology,” and “nursing research.” The
recommendation to incorporate “nursing research” into the baccalaureate nursing curriculum
13
signified the recognition that research must assume greater prominence if nursing practice in
China is to advance scientifically. However, the request to build into the curriculum more
“fundamental medical knowledge,” if defined as knowledge of anatomy, pathophysiology, and
other medicine-related courses, is controversial since the present Chinese baccalaureate nursing
education curriculum is perceived predominantly as “physiologically-based and disease-
oriented” (Chan & Wong, 1999). This recommendation is also in conflict with the nation-wide
efforts to build a nursing education model independent of medical education (Shen, 1998, 2000;
Xu, Xu, & Zhang, 2000).
Role development. Only one addition was suggested to the domain of role development:
“Contributes to the development of the profession.” This suggests that the respondent did not
interpret the existing key concept “member of a profession” to be inclusive of role development.
Interpretation and Discussion
Findings from this study suggest that baccalaureate nursing education in China and the
United States share some pedagogical components (universality). This universality derives from
the shared dimensions of the philosophies, beliefs, and values underpinning baccalaureate
nursing education in the two countries. Moreover, the universality stems from the identical or
similar outcomes (i.e. desirable professional values, core competencies, core knowledge, and
roles) required of baccalaureate nursing graduates for professional practice in the two countries.
This study also indicates a diversity dimension of baccalaureate nursing education in
China and the United States. The suggestion of the universality dimension does not diminish, in
any sense, the differences in the two systems that derive from the sociopolitical and cultural
differences between the two countries. The universality does not reduce the importance and
challenge to adapt The Essentials to the Chinese context. The perceived differences and even
14
conflicts were reflected from the low ratings on a number of the 21 key concepts, as well as from
the contrasting values for baccalaureate nursing education revealed through the qualitative
comments by the respondents. These perceived differences and conflicts warrant further
intellectual scrutiny. The following interpretation and explanations intend to be provocative and
explorative rather than conclusive.
Autonomy. While autonomy is one of the core values that have been upheld by the
Western, including American, nursing profession, this value orientation poses a challenge and
conflict to the traditional Chinese cultural values. In the West, particularly in the United States,
autonomy is deeply rooted in the belief in individualism that values and promotes self- reliance
and self-determination. In a sharp contrast, collectivism is the predominant and preferred value
in the Chinese society; in other words, collectivity, rather than individuality, is the common
denominator in most Chinese contexts. Family as a unit making treatment decisions for its sick
members, the expectation of the individual to sacrifice self interest for the good the family, and
promotion of team spirits are just but a few manifestations. There is, however, growing empirical
evidence that the Chinese nursing profession is gradually accepting, to some degree, the Western
value of autonomy as evidenced by giving patient treatment options.
A number of scholars (Davis, 2000; Doutrich, 2001; Hisama, 2001; Minami, 1985; Shin,
2001) documented and examined conflicts between Western and Eastern cultural values in
nursing. Davis (2000) demonstrated in her case study of Japan that some of the endearing
American values in nursing such as autonomy were on a direct collision course with the
dominant Japanese cultural values that cherish group cohesion over individuality as embodied in
“we” coming before “me.” Even the Japanese word for self (jibun) literally means a part of the
15
larger whole that consists of groups and relationships and interdependency. “There is no man
without another man according to the Japanese concept” (Minami, 1985).
Logically, this values orientation is also extended into the medical and nursing practice in
Japan. For example, terminally- ill patients are not always informed of their diagnosis and
prognosis. Usually, the physician informs the family members who then decide whether or not to
tell the patient (Davis, 2000). Families may decide to withhold information from the patient
because they believe that to reveal “the truth” would unduly burden the patient and hasten a poor
outcome. It is the family as a unit that most often makes all treatment decisions for its ill
member. On the other hand, the individual patient expects to be protected and supported by
family decisions.
Another example of this collectivistic orientation in Japan was a recent legislative ruling
that the family could override an individual’s pre-made decision to donate their organs. The idea
that one family member has individual rights that are independent of the family is an unaccepted
notion in Japan (Davis, 2000). The idealized Western professional nursing value of autonomy, as
evidenced in the promotion of independence and the ethical/legal concept of informed consent
and advanced directive, is incongruent with dominant Japanese cultural values (Davis, 2000;
Doutrich, 2001). Consequently, ethical conflicts were created in value orientations for those
Japanese nurses whose professional socialization was heavily influenced by the Western nursing
paradigm, but whose private lives were rooted in the traditiona l Japanese culture (Minami,
1985).
Doutrich (2001) also documented dissonance and confusion of sampled Japanese nurse
scholars in U.S. graduate programs when they were asked to adopt American views of nursing.
The incongruence included, but not limited to, role and power, patient expectations,
16
conceptualization of aspects of nursing, and caring practices. The study also recorded difficulty
of one nurse scholar’s re-adjustment to Japanese nursing practice upon her return after practicing
many years in the United States.
Human diversity. Human diversity is another cardinal value promoted by the American
nursing profession and has evolved from the basic premises upon which this country was
founded. The United States is a melting pot for immigrants from all over the world. According to
the census projection, racial and ethnic minorities combined will become the majority in the
population by 2050, hence the birth of the new notion “the emerging majority.” A mosaic
multitude of cultural, religious, and lifestyles characterize American society. In stark contrast,
many Asian countries are largely homogeneous. In China, for example, more than 99% of the
population belongs to the Han nationality (Lin & Li, 2000). The variety of religious faith and
beliefs is also considerably fewer than in the United States since the country claims officially to
be an atheist nation. Variations of lifestyles such as different sexual orientations are perceived
predominantly as socially deviant, and thus still largely confined behind closed doors.
Health care system and policy. Political consciousness and involvement are highly
advocated by American nursing leaders and are a core value for the profession as a method of
establishing an independent professional identity and political clout. As the largest group of
health professionals in the United States, nurses are encouraged by professional organizations to
make their voices heard and to become politically astute. China also has a national nursing
organization - the Chinese Nursing Association (CNA). However, CNA is a semi-political
bureaucracy rather than an autonomous professional organization in the Western sense because
its entire budget comes from government appropriations. Moreover, CNA functions under the
direct leadership of the Chinese Communist Party. Consequently, independent thinking and
17
involvement in policy-making are not encouraged. This sociopolitical context underscores the
reason why policy making and political involvement were not emphasized in the curriculum.
Global health care. Globalization has been one of the driving forces not only for
international economic activities, but also for the nursing profession internationally, including
nursing education. With modern means of transportation, the global community is becoming
increasingly intertwined. National public health issues can no longer be confined within national
borders. Moreover, as a consequence of the technology advancement in the age of the Internet,
telemedicine, and distance learning, nation states are becoming increasingly interdependent. In
many developing countries such as China, integration into the global community has not
achieved the desired level due, in part, to limited domestic resources and unequal international
power relationships. However, China joined the World Trade Organization in 2001. Building
upon this and other major inroads made within the past two decades, China will quickly become
more globally integrated. It is predicated that more content on global health care will be
incorporated into the baccalaureate nursing education curriculum in the future.
Designer/manager/coordinator of care. The responsibility for the professional nurse to
assume responsibility and accountability for the design, management, and coordination of care
received only minimal emphasis in the Chinese baccalaureate nursing curriculum. This may be
attributed to the lack of independent professional identity of nursing in the country. Medicine has
assumed this responsibility and nurses tend to function in the traditional handmaiden role as
evidenced in the popular metaphor: “A doctor’s mouth directs a nurse’s legs.” As a
“handmaiden” critical thinking skills are devalued and therefore have not been an important
consideration within the existing baccalaureate nursing curriculum. Clearly, the data from this
study supports that these concepts are of increasing importance to the Chinese nurse educators.
18
Implications and Conclusions
This study examined the relevance of The Essentials as a guide for the development of
baccalaureate nursing curriculum in the People’s Republic of China. Findings from the study
revealed that universality and diversity co-existed in the baccalaureate nursing education
curricula in China and in the United States. While the universality dimension recognized the
shared concepts underpinning both systems, the diversity dimension alerted international nurse
educators to the potential pitfalls of transplanting The Essentials without first assessing its
cultural relevancy. Therefore, values clarification, discrimination, and adaptation to home
cultures are imperative if The Essentials is to be applied to a new cultural context.
Further, this study suggested the feasibility of adopting The Essentials as a plausible
launching board to conceptualize a baccalaureate nursing education curriculum model that has
global relevance. It is hypothesized that this proposed model will consists of two components.
One component, which encompasses most concepts from all five domains in The Essentials, can
be readily transferred across cultures (universality). The second component, which is likely to be
made up of a number of concepts primarily from the domains of professional values, core
knowledge, and role development that deal with the ethical, cultural, and sociopolitical
dimensions of nursing, is culture-specific (diversity) and, therefore, requires adaptation in
varying degrees. Further, a few concepts might defy transferability to a particular culture
completely.
Nursing education and professional nursing practice are never value free. On the
contrary, both are deeply embedded, either explicitly or implicitly, in the cultural values and
norms of a given group. Self-awareness, caution, sensitivity, and in-depth studies of the host
culture must be undertaken to prevent ignorance, imposition, and ethnocentrism if cross-cultural
19
transplantation of The Essentials is attempted in a non-Western setting, because the document is
rooted in the Western, American in particular, values, norms, and assumptions. Such cognizance
is vital to international nursing organizations and nurse educators/scholars involved in education,
research, and consulting in international and transcultural nursing.
In a recent article, Ludwick & Silva (2000) discussed the challenges of cultural values
and ethical conflicts in the context of globalization, and cautioned “North Americans and others
with Western ethical perspectives” against unwitting cultural imposition through export of
textbooks, curricula, and used products, even though these academic and humanitarian activities
were well intentioned. Such advice is well warranted since about 70% of the world cultures are
collectivistic rather than individualistic (Davis, 2000).
Meanwhile, American nurse educators involved in training international students need to
become aware that international students may find what they have learned in the United States
may be incongruent with their traditional cultures and professional values. Consequently, these
Western-educated nurses may have to go through the re-socialization process after returning to
their home countries. Such awareness and specific strategies to address this issue are not only an
educational challenge, but also an ethical and moral imperative.
The global influence of American nursing is mounting (Davis, 2000; Lash, Lust, &
Nelson, 2000; Ludwick & Silva, 2000). As long as the United States is perceived as the country
with the most progressive nursing profession, including nursing education, many countries will
continue to turn to the United States for insights, suggestions, and cultural borrowings. In order
to build a baccalaureate nursing education curriculum model that is of global relevance, it is the
shared challenge and responsibility for both American and international nurse educators/scholars
to conduct more transcultural and comparative studies to (a) test the validity and reliability of
20
The Essentials and (b) to substantiate the universality as well as the diversity of baccalaureate
nursing education around the world.
Limitations of Study
Small sample size is one limitation imposed upon the study. This limitation was also
directly related to the fact that there was a limited number of known Chinese baccalaureate
nursing programs in existence at the time of the study (N= 22). Consequently, more rigorous
statistical analysis on the returned data was not an option.
Another limitation might have derived from the different definitions of “patient”. AACN
(1998) defines patient as “recipient of nursing care or services” and patients “may be individua ls,
families, groups, or communities” (p. 2). Possible unawareness of this difference might have
affected the responses from the Chinese nurse educators.
21
References
American Association of Colleges of Nursing. (1998). The essentials of baccalaureate education
for professional nursing practice. Washington, D.C.: Author.
Chan, S., & Wong, F. (1999). Development of basic nursing education in China and Hong Kong.
Journal of Advanced Nursing, 29, 1300-1307.
Chang, W. Y. (1999). Interview with visiting health administrators from the Ministry of Health,
Beijing, China. Image: Journal of Nursing Scholarship, 31, 185-187.
Davis, A. J. (2000). Global influence of American nursing: Some ethical issues. Nursing Ethics:
An International Journal for Health Care Professionals, 6, 118-125.
Doutrich, D. (2001). Experiences of Japanese nurse scholars: Insights for U.S. faculty. Journal of
Nursing Education, 40, 210-216.
Elfrink, V., & Lutz, E. M. (1991). American Association of Colleges of Nursing essential values:
National study of faculty perceptions, practices, and plans. Journal of Professional
Nursing, 7, 239-245.
Henley, J. E., & Anema, M. G. (1989). Curriculum assessment using The Essentials of College
and University Education for Professional Nursing. Nurse Educator, 14, 18-20.
Hisama, K. K. (2001). The acceptance of nursing theory in Japan: A cultural perspective.
Nursing Science Quarterly, 14, 255-259.
Johnson, B. M. (1987). Essentials of college and university education for professional nur sing.
Journal of Professional Nursing, 3, 207-213.
Lash, A. A., Lust, B., & Nelson, M. A. (2000). American nursing scholars abroad, 1985-1995.
Journal of Nursing Scholarship, 32, 415-420.
Li, S. Z.. (2001). Today’s nursing education in the People’s Republic of China. Journal of
22
Nursing Education, 40, 217-221.
Lin, L. Q., & Li, M. (Eds.). (2000). China: Facts & figures 2000. Beijing, China: New Star
Publishers.
Ludwick, R., & Silva, M. C. (2000, August 14). Nursing around the world: Cultural values and
ethical conflicts. Online Journal of Issues in Nursing. Retrieved October 6, 2001, from
http://www.nursingworld.org/ojin/ethicol/ethics_4.htm
Minami, H. (1985). East meets West: Some ethical considerations. International Journal of
Nursing Studies, 22, 311-318.
Shen, N. (1998). Facing 21st century: exploring a new model of educating baccalaureate nurses.
China Higher Medical Education, 4, 10-12. (in Chinese)
Shen, N. (2000). A holistic approach to a new model of baccalaureate nursing. China Higher
Medical Education, 2, 32-33. (in Chinese)
Shin, K. R. (2001). Developing perspectives on Korean nursing theory: The influences of
Taoism. Nursing Science Quarterly, 14, 346-353.
Xu, Y., Xu, Z., & Zhang, J. (2000). Nursing education system in the People’s Republic of China:
Evolution, structure, and reform. International Nursing Review, 47, 207-217.
23
Table 1
Importance of 21 Key Concepts in Present Curriculum and Ideal Curriculum
Present Curriculum (M)
Ideal Curriculum (M)
Difference
Technical Skills 6.00 6.00 0.00
Integrity 5.70 6.00 0.30
Communication 5.50 6.00 0.50
Illness and Disease Management 5.50 5.70 0.20
Human Dignity 5.40 5.90 0.50
Assessment 5.40 5.90 0.50
Caring 5.33 5.89 0.56
Social Justice 5.20 5.50 0.30
Ethics 5.20 5.30 0.10
Liberal Education 5.11 5.67 0.56
Provider of Care 5.00 5.50 0.50
Information and Health Care Technology 4.90 5.20 0.30
Critical Thinking 4.80 5.90 1.10
Member of Profession 4.80 5.70 0.90
Altruism 4.70 5.50 0.80
Health Promotion, Risk Reduction, & Disease Prevention
4.70 5.40 0.70
Designer/Manager/Coordinator of Care 4.10 5.50 1.40
Human Diversity 4.00 4.70 0.70
Healthcare Systems and Policy 3.70 4.60 0.90
Autonomy 3.40 5.10 1.70
Global Health Care 3.40 4.50 1.10
Means are based on a scale of 1.00 to 6.00, with 6.00 as the most important.
24
Table 2
Cultural Relevance of 21 Key Concepts in Present Curriculum and Ideal Curriculum
Present Curriculum (M)
Ideal Curriculum (M)
Difference
Technical Skills 5.90 5.90 0.00
Integrity 5.60 5.80 0.20
Human Dignity 5.30 5.90 0.60
Illness and Disease Management 5.20 5.40 0.20
Communication 5.10 5.60 0.50
Ethics 5.10 5.30 0.20
Caring 5.00 5.78 0.78
Liberal Education 4.89 5.56 0.67
Assessment 4.80 5.80 1.00
Social Justice 4.80 5.30 0.50
Provider of Care 4.67 5.40 0.73
Critical Thinking 4.60 5.80 1.20
Information and Health Care Technology 4.50 4.90 0.40
Member of Profession 4.50 5.60 1.10
Health Promotion, Risk Reduction, & Disease Prevention
4.50 5.30 0.80
Altruism 4.30 5.20 0.90
Designer/Manager/Coordinator of Care 3.90 5.40 1.50
Human Diversity 3.60 4.70 1.10
Healthcare Systems and Policy 3.20 4.40 1.20
Global Health Care 3.20 4.40 1.20
Autonomy 3.00 4.90 1.90
Means are based on a scale of 1.00 to 6.00, with 6.00 as the most relevant culturally.
25
Table 3
Extent of Exposure of 21 Key Concepts in Present Curriculum and Ideal Curriculum
Present Curriculum (M)
Ideal Curriculum (M)
Difference
Technical Skills 5.90 6.00 0.10
Integrity 5.50 5.80 0.30
Human Dignity 5.30 5.90 0.60
Illness and Disease Management 5.20 5.50 0.30
Communication 5.10 5.80 0.70
Ethics 5.10 5.30 0.20
Social Justice 4.80 5.40 0.60
Assessment 4.70 5.70 1.00
Caring 4.67 5.67 1.00
Provider of Care 4.67 5.50 0.83
Critical Thinking 4.50 5.90 1.40
Health Promotion, Risk Reduction, & Disease Prevention
4.50 5.40 0.90
Member of Profession 4.30 5.60 1.30
Liberal Education 4.22 5.44 1.22
Information and Health Care Technology 4.20 4.90 0.70
Altruism 4.10 5.10 1.00
Designer/Manager/Coordinator of Care 3.90 5.30 1.40
Human Diversity 3.40 4.80 1.40
Global Health Care 3.10 4.30 1.20
Autonomy 3.00 4.90 1.90
Healthcare Systems and Policy 3.00 4.30 1.30
Means are based on a scale of 1.00 to 6.00, with 6.00 as having the most extensive exposure.
26
Table 4
Rank Order of Means of 21 Key Concepts in Present Curriculum by Importance, Cultural Relevance, and
Extent of Exposure
Importance of Concept
Cultural Relevance
Extent of Exposure
Technical Skills 1 1 1
Integrity 2 2 2
Human Dignity 4 3 3
Illness and Disease Management 3 4 4
Communication 3 4 5
Ethics 6 5 5
Assessment 4 8 7
Caring 5 6 8
Social Justice 6 8 6
Liberal Education 7 7 11
Provider of Care 8 9 8
Information and Health Care Technology 9 11 12
Critical Thinking 10 10 9
Member of Profession 10 11 10
Altruism 11 12 13
Health Promotion, Risk Reduction, & Disease Prevention 11 11 9
Designer/Manager/Coordinator of Care 12 13 14
Human Diversity 13 14 15
Healthcare Systems and Policy 14 15 17
Autonomy 15 15 17
Global Health Care 15 16 16
27