Embed Size (px)
Citation preview
The content of this activity was developed by the faculty indicated herein under the supervision of Postgraduate Institute for Medicine and assistance from MedEdicus LLC. Applied Clinical Education (ACE) is responsible for graphic design and distribution of the activity via Anesthesiology News and CMEZone.com.
All information included in this activity is believed to be true and accurate at the date of publication. ACE makes no warranty, expressed or implied, with respect to the material contained herein.
Release Date: December 1, 2015 Expiration Date: December 1, 2016
Estimated Time To Complete Activity: 1.25 hoursTarget AudienceThe target audiences for this activity include anesthe-siologists and certified registered nurse anesthetists.
Learning ObjectivesUpon completion of this activity, learners will have improved their ability to:1 Recall the incidence and complications of residual
neuromuscular blockade2 Utilize optimal techniques for assessment of neu-
romuscular blockade depth3 List patient features/comorbidities and surgical
procedures that may lead to increased risk of resid-ual neuromuscular blockade
4 Employ effective communication strategies among anesthesiologists, CRNAs, and other members of the surgical care team
5 Compare the efficacy and safety data of currently available and emerging agents for the reversal of neuromuscular blockade
6 Integrate strategies for reversal of neuromuscular blockade into plans for the care of patients under-going anesthesia
Accreditation StatementThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continu-ing Medical Education (ACCME) through the joint providership of Postgraduate Institute for Medicine and MedEdicus LLC. The Postgraduate Institute for Medicine is accredited by the ACCME to provide continuing medical education for physicians.
Credit DesignationThe Postgraduate Institute for Medicine designates this enduring material for a maximum of 1.25 AMA PRA Category 1 Credit™. Physicians should claim only the credit commensurate with the extent of their par-ticipation in the activity.
Disclosure of Conflicts of InterestPostgraduate Institute for Medicine (PIM) requires instructors, planners, managers and other individu-als who are in a position to control the content of this activity to disclose any real or apparent conflict of inter-est (COI) they may have as related to the content of this activity. All identified COI are thoroughly vetted and resolved according to PIM policy. PIM is commit-ted to providing its learners with high quality CME activities and related materials that promote improve-ments or quality in healthcare and not a specific propri-etary business interest of a commercial interest.The faculty reported the following financial relation-ships or relationships to products or devices they or
their spouse/life partner have with commercial interests related to the content of this CME activity:Sorin J. Brull, MD, has no real or apparent conflicts of interest to report.Aaron F. Kopman, MD, has no real or apparent con-flicts of interest to report.Glenn Murphy, MD, has had a financial agreement or affiliation during the past year with the following com-mercial interest in the form of Consulting Fees (e.g., advisory boards) and Fees for Non-CME/CE Services Received Directly from a Commercial Interest or their Agents (e.g., speakers’ bureaus): Merck & Co., Inc.Mark Welliver, DNP, CRNA, ARNP, has had a finan-cial agreement or affiliation during the past year with the following commercial interest in the form of Consulting Fees (e.g., advisory boards): Merck & Co., Inc.The planners and managers reported the following finan-cial relationships or relationships to products or devices they or their spouse/life partner have with commercial interests related to the content of this CME activity. The following PIM planners and managers, Trace Hutchison, PharmD, Samantha Mattiucci, PharmD, CHCP, Judi Smelker-Mitchek, RN, BSN and Jan Schultz, RN, MSN, CHCP, hereby state that they or their spouse/life partner do not have any financial rela-tionships or relationships to products or devices with any commercial interest related to the content of this activity of any amount during the past 12 months.Medical Writer: Jennifer Swanson has no real or apparent conflicts of interest to report.MedEdicus Planners: Diane McArdle, PhD, and Cynthia Tornallyay, RD, MBA, CCMEP, have no real or apparent conflicts of interest to report.
Method of Participation and Request for CreditThere are no fees for participating in and receiving CME credit for this activity. During the period December 1, 2015 through December 1, 2016, par-ticipants must read the learning objectives and faculty disclosures and study the educational activity.To receive CME credit, participants should read the preamble and the monograph, and complete the pre-test, post-test, and activity evaluation online at http://cmezone.com/activities/sr1542/2394/. Upon success-fully completing the post-test with a score of 75% or better and the activity evaluation, your certificate will be made available immediately. Or you can mail or fax the completed post-test and evaluation to Postgraduate Institute for Medicine, 304 Inverness Way South, Suite 100, Englewood, CO 80112; Fax: (303) 858-8848.
Media: Print and InternetDisclosure of Unlabeled UseThis educational activity may contain discussion of published and/or investigational uses of agents that
are not indicated by the FDA. The planners of this activity do not recommend the use of any agent out-side of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DisclaimerParticipants have an implied responsibility to use the newly acquired information to enhance patient out-comes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagno-sis or treatment discussed or suggested in this activ-ity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindi-cations and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
System Requirements for Digital EditionsIf you are viewing this activity online please ensure the computer you plan to use meets the following requirements:• Operatingsystem:Windows or Macintosh• Mediaviewingrequirements:Flash Player or Adobe• Supportedbrowsers: Microsoft Internet Explorer,
Firefox, Google Chrome, Safari and Opera• AgoodInternetconnection
This activity is jointly provided by Postgraduate Institute for Medicine (www.pimed.com) and MedEdicus LLC.
This activity is supported by an independent educational grant from Merck & Co., Inc.
Distributed via Anesthesiology News and CMEZone.com
AssessmentandReversalofNeuromuscularBlockade:CurrentandEmergingStrategies
Glenn Murphy, MD (Chair)Clinical ProfessorNorthShore University HealthSystemEvanston HospitalEvanston, IL
Aaron F. Kopman, MDProfessor of Anesthesiology (retired)Weill Cornell Medical CollegeNew York, NY
Sorin J. Brull, MDProfessor of AnesthesiologyDepartment of AnesthesiologyMayo Clinic, College of MedicineJacksonville, FL
Mark Welliver, DNP, CRNA, ARNPAssociate Professor of Professional Practice School of Nurse AnesthesiaHarris College of Nursing & Health SciencesTexas Christian UniversityFort Worth, TX
© 2015 MedEdicus LLC
Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
2
IntroductionApproximately 50 million patients in the United States receive
general anesthesia annually.1 As part of anesthesia management, a neuromuscular blocking agent (NMBA) is often administered to induce muscle relaxation, facilitate airway management, and minimize the risk for laryngeal trauma during tracheal intubation. More than 100 million doses of NMBAs are administered annu-ally in the United States.2 The use of NMBAs is associated with a risk for residual neuromuscular blockade (RNMB), which may result in respiratory complications, muscular weakness, prolonged stay in the postanesthesia care unit (PACU) and hospital, and delayed extubation.3-5 RNMB occurs in approximately one-third of surgical cases involving NMBAs.4,6-9 According to clinical reports and a statement from the American Society of Anesthe-siologists ( J. Zerwas, MD [written communication, July 2013]), the chance for complications from RNMB is also increased in patients with certain risk factors (Figure 1).10-12
RNMB is often unrecognized by clinicians and remains a sig-nificant problem in anesthesia care.13,14 In a survey of anesthe-sia providers in the United States and Europe, more than 50% of respondents estimated the incidence of clinically significant RNMB to be less than 1%.13 Contributing to the problem are the many aspects of neuromuscular blockade (NMB) that have not been standardized. These aspects include the definitions used to describe RNMB and recovery, the optimal strategies for dosing
NMBAs and reversal agents, and best practices for monitoring NMB and recovery. In the absence of definitive guidelines, col-laboration and communication among members of the perioper-ative care team are imperative for optimal patient outcomes. The following cases highlight practical considerations for assessing and managing RNMB.
CASE STUDY 1
A 35-year-old woman with a body mass index (BMI) of 56 kg/m2 presents for bariatric surgery (gastric sta-pling). Her medical history includes smoking and type 2 diabetes mellitus. She takes oral metformin, but she
did not take it this morning. She has active reflux symptoms, for which she takes omeprazole nightly. On physical examination, her blood pressure is 168/88 mm Hg, and her heart rate is 88 bpm. Examination of the airway reveals a decreased (2-cm) mouth opening, a class 2 upper lip bite test (her lower incisors can bite the upper lip below the vermillion line), and a Mallampati class 3 airway. Preoperative laboratory tests reveal the following blood levels: fasting glucose, 140 mg/dL; hemoglobin, 14.2 g/dL; and potassium, 3.9 mEq/L. The surgeon requests maximal neuromuscular block (post-tetanic count [PTC] of 0-1) to facilitate surgery.
Glenn Murphy: How would you approach airway management in this patient, considering the findings of the airway examination?
Mark Welliver: Rapid sequence intubation (RSI) with succinyl-choline is a potential option, but it could lead to rapid desaturation if airway patency is lost—which is possible with obesity. Sedation with dexmedetomidine and fiber-optic intubation (FOI) would be a conservative approach. A laryngeal mask airway (LMA) would be another option for cases in which we want to avoid the use of NMBAs to secure the airway.
Aaron Kopman: I agree that we might want to avoid the use of NMBAs to secure the airway for this patient. Selecting the appro-priate dose of the NMBA is challenging, especially in patients who are morbidly obese. Evidence suggests that the dose should be calculated according to ideal body weight—not actual body weight—for quicker recovery.15 Even with a dose of 1 mg/kg of succinylcholine, the average time to resumption of diaphragmatic activity might be 5 to 6 minutes. Full recovery at the adductor pol-licis could take 10 minutes. This patient could desaturate in 2 min-utes. Therefore, given the increased BMI, I would avoid the use of an NMBA and perform sedated awake intubation.
Sorin Brull: Sedation could be problematic in patients at risk for
Older age
Female sex
Obesity
Myasthenia gravis
Upper abdominal or thoracic surgery
Figure 1. Risk factors for development of complications from RNMB.10-12,a
aJ. Zerwas, MD (written communication, July 2013).

Why wait? Access this program and post-test @ CMEZone.com
3
aspiration. FOI could be an option, if the anesthesiologist is highly experienced in that procedure. The risks and benefits should be considered when deciding the appropriate course of action—airway loss and brain death is significantly worse than aspiration. The find-ings on airway examination suggest that this patient is at risk for difficult intubation. Therefore, the conservative approach might be to perform an awake/sedated FOI. Alternatively, RSI could be per-formed with propofol/succinylcholine with the fiberscope in place. For example, I would administer propofol, advance the endotra-cheal tube (ETT)–loaded fiberscope until the vocal cords are visu-alized, administer the NMBA (succinylcholine) when the cords are visible, and introduce the ETT over the fiberscope at the onset of vocal cord paralysis. A video laryngoscope could also be in place to facilitate vocal cord visualization. The risks and benefits of cri-coid pressure (Sellick’s maneuver) application have been discussed widely, and it remains to be proven whether it prevents aspiration more than it impedes vocal cord visualization. I would be comfort-able without its application.
Glenn Murphy: LMAs have been available for the past 20 years and would be an appropriate option for patients who are difficult to intubate and ventilate. In this patient, however, the airway should be secured. In my practice, the advent of the LMA and the video laryngoscope has reduced my use of FOI by 90%. When evaluat-ing an airway such as in this patient, each anesthesiologist must make a clinical judgment regarding the optimal management strat-egy. We have discussed different options for managing this airway, all of which are probably appropriate.
Glenn Murphy: How would maximal NMB, as requested by the surgeon, be achieved in this patient?
Sorin Brull: First, it is important to have a thorough discussion with the surgeon to define maximal NMB and determine the level of muscle relaxation required for the procedure. For example, the surgeon performing a laparoscopic procedure might want to avoid diaphragmatic movement completely, but that surgeon’s definition of maximal NMB may differ from that of another surgeon who is performing a different procedure.
Aaron Kopman: It is also important to remember that abdom-inal relaxation is multifactorial—the drugs used for anesthesia, the depth of anesthesia, and other factors might contribute to dia-phragmatic movement during the procedures. Movement does not always mean that more relaxant is needed. Instead, more nar-cotic or a change in ventilator pattern might be required. Although NMB is the primary method for achieving muscle relaxation, other methods can be considered, depending on the case.
Sorin Brull: I would probably avoid drugs with potentially active metabolites, such as vecuronium, and use cisatracurium in this patient. Another important point is that, if the surgeon needs a PTC of 0 to 1 for the surgical procedure, attempting rever-sal with an anticholinesterase reversal agent is challenging. At a PTC of 1, the average time to a train-of-four (TOF) ratio of 0.9, which has been suggested to be the threshold of adequate recov-ery,16,17 is approximately 1 hour.18 It is important to communi-cate with the surgeon about the limitations of available reversal
agents in reversing a deep block (eg, the ceiling effect of neostig-mine) and the need for prolonged anesthesia after the surgery has been completed.
Glenn Murphy: The level of NMB needed for surgical proce-dures seems to be surgeon-dependent. Some surgeons will request “no twitches” for a particular procedure, whereas others are not con-cerned with some movement, even for the same procedure.
Mark Welliver: I agree. Surgeons request no twitches to ensure that the abdominal rectus muscle and diaphragm do not move during surgery. In practice, NMBAs are often administered in boluses to maintain 1 twitch, which should be sufficient; but if subsequent boluses are not administered at the appropriate time, this level of blockade can spontaneously recover to 2 or 3 twitches and then diaphragmatic movement, prompting the surgeon to request more NMBA. In these cases, monitoring is often per-formed with a peripheral nerve stimulator (PNS) on the ulnar nerve, which does not correlate with the diaphragm.19,20 There-fore, monitoring of NMB needs to be improved to determine when the next bolus should be administered to prevent spontane-ous recovery during the procedure.
Glenn Murphy: How would you monitor this particular patient undergoing this procedure?
Mark Welliver: If this patient were intubated successfully, I would administer rocuronium to maintain a TOF count of 1/4. I would use accelerometry to monitor the facial nerve, which cor-relates with the diaphragm, measuring either the orbicularis oculi or the corrugator supercilii muscle. I would communicate with the surgeon regarding the effectiveness of this level of block. Close continual assessment of TOF would be maintained to keep a weak twitch present. I would administer opioids as needed and keep the end-tidal CO2 on the low-normal side to prevent CO2-triggered attempts at spontaneous respirations. If this level of NMB were not sufficient, I would maintain at a PTC less than 8. When the surgeon has indicated that the procedure is nearing completion, I would withhold any further rocuronium and wait for spontaneous recovery of at least twitches. I would not reverse off of twitches on the facial nerve because that could be direct muscle stimulation rather than a true corrugator supercilii or orbicularis contraction. I would begin monitoring at the ulnar nerve, the adductor pollicis, to ensure the absence of direct mus-cle stimulation and that I have an accurate twitch count repre-senting spontaneous recovery (See sidebar 1: Monitoring Neuromuscular Blockade). I would want at least 1 twitch, and pref-erably more, before reversing with neostigmine. This approach also ensures that the spontaneous recovery is occurring at a mus-cle set that is easier to paralyze—if good recovery is noted at the adductor pollicis, other muscles in the body—certainly, the dia-phragm and, hopefully, the accessory muscle for respiration—should be fully reversed.
With sugammadex (available in Europe and undergoing FDA review in the US), this scenario would be somewhat easier to man-age, because a degree of spontaneous recovery is not necessary for successful reversal (See sidebar 2: Efficacy and Safety of Sugammadex

Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
4
Versus Neostigmine). A dose of 4 mg/kg, when administered at a PTC of 1 to 2, has been shown to reverse NMB to a TOF ratio of at least 0.9.21 Because clinical dose-finding studies were based on total body weight, it is recommended to dose sugammadex for obese patients similarly, based on total body weight. Dosing based on ideal body weight increases the risk for underdosing and incom-plete reversal.22,23
Aaron Kopman: I do not think direct facial nerve stimulation occurs. First, direct muscle stimulation would result in 4 twitches of equal height, not just 1 twitch. In a study by Nepveu and col-leagues, the ulnar nerve was not stimulated with the classical tech-nique but was stimulated by applying 1 electrode on either side of the hand, at the dorsal and ventral side of the adductor pollicis.24 Similar results were observed between that method and with stim-ulation of the microfibers of the ulnar nerve. To get direct mus-cle stimulation, pulse durations in excess of 0.5 msec are usually needed. Most nerve stimulators use a 0.20-msec pulse. If 4 twitches of equal height cannot be demonstrated, then direct muscle stimu-lation is not occurring.
Sorin Brull: That is absolutely true. However, according to a study by Thilen and colleagues, monitoring the responses to facial nerve stimulation increases the risk for residual paralysis in the PACU by 5-fold compared with monitoring at the adductor polli-cis.25 Not all facial stimulation is the same. For example, some anes-thesiologists actually put the PNS on the face (temple and lower jaw) and monitor the jaw movement. I do not think this is reflective of the degree of relaxation at the respiratory muscles.
Glenn Murphy: The study by Thilen and colleagues also eval-uated various factors associated with residual block and identified the monitoring site—the eye versus the adductor pollicis—to be the primary factor.25 The eye is often monitored because it is easily accessible. If the eye is chosen as the monitoring site, it is important to recognize the limitations of this monitoring site.
Aaron Kopman: Caffrey and colleagues showed that 4 twitches could be observed at the face when barely 1 twitch could be observed at the adductor pollicis, suggesting that the facial nerve could provide misleading results.26 However, few alternatives are available if the hands are not accessible.
Sorin Brull: I agree. The facial nerve has inherent limitations and should not be used to monitor for reversal or spontaneous recovery. Several studies have investigated other potential moni-toring sites, such as the posterior tibial nerve.27,28 No correlation between the thumb and the great toe has been confirmed. Previ-ously, the peripheral muscles have been assumed to correlate sim-ilarly to the adductor pollicis because they are not as resistant to
paralysis as the diaphragm.Glenn Murphy: Electromyography (EMG) is another moni-
toring option that allows for quantitative monitoring, even if the arms are inaccessible. However, every new technology takes time to be adopted into routine use. Only about 20% of anesthesia depart-ments in the United States have objective monitors.13 Todd and colleagues recently evaluated patterns of quantitative EMG mon-itoring in operating rooms and showed that anesthesiologists were often reluctant to use EMG, but after a series of educational pro-cesses over a 2-year period, routine use of the EMG increased, and reintubations related to NMB decreased.29 This study showed that proper education can be effective.
Mark Welliver: I agree. The limited use of monitoring technol-ogy, even acceleromyography, has been a significant practice gap. Many operating rooms have accelerometry or kinemyography equipment, yet anesthesia teams do not use it routinely. The educa-tional model used in the study by Todd and colleagues was effective at increasing use of acceleromyography in anesthesia practice and can serve as a model for other institutions.
Sorin Brull: Another factor is that most clinicians have not used objective monitors during their careers. Institutional pres-sures to complete the case and make the operating room available for the next patient (production pressure) may also reduce rou-tine monitoring. The specialty organizations should provide infor-mation and recommendations on the available monitors to guide clinicians and emphasize the importance of monitoring. Simply recommending that anesthesiologists “consider using a PNS” is not sufficient.
Glenn Murphy: With this case, we have maintained a deeper level of blockade with a PTC of 1, and the surgery has been completed.
How would you manage this case now? Sorin Brull: Today, in my opinion, the only option is to wait for
spontaneous recovery to proceed until the TOF count is 3. Other anesthesiologists might allow a TOF count of 2 or 1. If neostig-mine is considered, it is important to realize that it has a ceiling effect at very deep blocks.30 It will work to a certain point, but the rest of the recovery will follow the normal spontaneous recovery. If another dose of neostigmine is administered, it can independently produce NMB. Studies have shown that sugammadex can signif-icantly reduce recovery times from a PTC 1 to 2 compared with neostigmine, suggesting that it may be beneficial in this setting.18,31
Why wait? Access this program and post-test @ CMEZone.com
5
Sidebar 1: Monitoring Neuromuscular Blockade
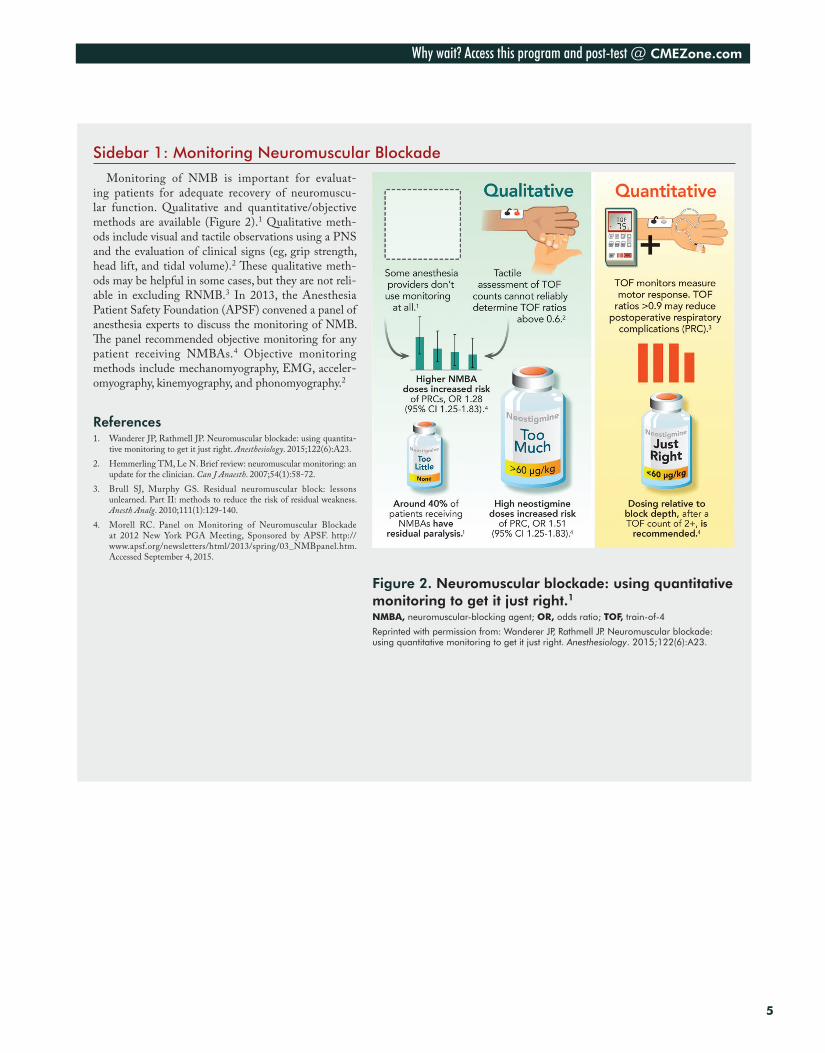
Monitoring of NMB is important for evaluat-ing patients for adequate recovery of neuromuscu-lar function. Qualitative and quantitative/objective methods are available (Figure 2).1 Qualitative meth-ods include visual and tactile observations using a PNS and the evaluation of clinical signs (eg, grip strength, head lift, and tidal volume).2 These qualitative meth-ods may be helpful in some cases, but they are not reli-able in excluding RNMB.3 In 2013, the Anesthesia Patient Safety Foundation (APSF) convened a panel of anesthesia experts to discuss the monitoring of NMB. The panel recommended objective monitoring for any patient receiving NMBAs.4 Objective monitoring methods include mechanomyography, EMG, acceler-omyography, kinemyography, and phonomyography.2
References1. Wanderer JP, Rathmell JP. Neuromuscular blockade: using quantita-
tive monitoring to get it just right. Anesthesiology. 2015;122(6):A23.2. Hemmerling TM, Le N. Brief review: neuromuscular monitoring: an
update for the clinician. Can J Anaesth. 2007;54(1):58-72.3. Brull SJ, Murphy GS. Residual neuromuscular block: lessons
unlearned. Part II: methods to reduce the risk of residual weakness. Anesth Analg. 2010;111(1):129-140.
4. Morell RC. Panel on Monitoring of Neuromuscular Blockade at 2012 New York PGA Meeting, Sponsored by APSF. http://www.apsf.org/newsletters/html/2013/spring/03_NMBpanel.htm. Accessed September 4, 2015.
Figure 2. Neuromuscular blockade: using quantitative monitoring to get it just right.1NMBA, neuromuscular-blocking agent; OR, odds ratio; TOF, train-of-4
Reprinted with permission from: Wanderer JP, Rathmell JP. Neuromuscular blockade: using quantitative monitoring to get it just right. Anesthesiology. 2015;122(6):A23.

Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
6
CASE STUDY 1, continued
The patient now has a TOF count of 3 to 4 and is reversed with 5 mg of neostigmine. Ten minutes later, she holds her head up for 5 seconds and squeezes your hands.
Glenn Murphy: Given these criteria, is extubation safe in this patient?
Sorin Brull: Absolutely not. Strong evidence suggests that head lift has a positive predictive value of about 0.5, similar to flipping a coin.8 Many studies have shown that full head lifts can be observed at degrees of paralysis that are almost surgical (ie, TOF ratio of 0.4). Clinical criteria are not sufficient to evaluate for adequacy of reversal before tracheal extubation; measuring the TOF ratio with objective monitoring is optimal.
Glenn Murphy: Are there any clinical criteria that would help to ensure that the patient had fully recovered neuromuscular function?
Aaron Kopman: We originated the tongue depressor test.16 If a tongue depressor is placed between a patient’s incisor teeth and cannot be pulled out with 2 fingers, the TOF ratio is at least 0.85. It is a very easy test to perform, is fairly sensitive, and is probably superior to other clinical criteria such as the head lift.
Glenn Murphy: Cammu and colleagues investigated 8 specific clinical tests and found that none of the tests, either used alone or in combination, were effective in detecting patients who had TOF ratios less than 0.9.8
Sorin Brull: Recovery should be evaluated before tracheal extu-bation, and although the tongue depressor test is likely the most useful clinical test to evaluate for recovery, it cannot be used in a patient whose trachea remains intubated. That is a major limitation of that test, unfortunately.
Aaron Kopman: That is a very important point. We need a test that will ensure adequate recovery before extubation, not after.
CASE STUDY 2
A 39-year-old woman is scheduled for a laparoscopic total abdominal hysterectomy. She is 163 cm tall and weighs 66 kg (BMI = 25 kg/m2). Her American Society of Anesthesiologists classification physical status is
1. Vital signs and blood chemistries are unremarkable. Anesthesia is induced with propofol 2.5 mg/kg, fentanyl 4 µg/kg, and rocuronium 0.60 mg/kg. Tracheal intubation is performed easily. The surgeon requests deep NMB, which was not well defined. Anesthesia is maintained with desflurane/oxygen and intermittent doses of fentanyl. Depth of anesthesia is monitored by a bispectral index (BIS) monitor, with BIS values maintained between 40 and 60. Because the arms are tucked at the sides, NMB is “measured” by visual evaluation of the TOF count at the facial muscles. Rocuronium is administered intermittently to keep the TOF count at less than 2. The TOF count at closure of the fascia is 2.
Glenn Murphy: Is there a specific definition in the literature for a deep NMB?
Aaron Kopman: There are no specific, universal definitions for depth of NMB. Deep block is generally defined as a TOF count of 0 and a PTC of 5 or less. Moderate blockade is generally defined as a TOF count of 1 to 3.
Sorin Brull: Several terms are being used in the literature, and the usage is not consistent. For example, deep and profound describe different levels of blockade in some studies but are used inter-changeably in others. Deep, moderate, and light are the terms that should be defined and used consistently in research and in practice.
Glenn Murphy: Is prompt reversal of a facial TOF count of 2 possible with neostigmine?
Aaron Kopman: No, I do not think that is reversible. A facial TOF count of 2 is generally considered a deep blockade, and the adductor pollicis muscle would likely have a TOF count of 0.
Mark Welliver: I agree. It is unlikely that neostigmine could reverse a TOF count of 2 at the facial muscles. I have performed TOF monitoring on the facial nerve and the ulnar nerve concurrently in an attempt to identify a correlation. Normally, there is no correlation.
Sorin Brull: I also agree. I would probably not attempt a reversal with neostigmine at that depth of block.
Why wait? Access this program and post-test @ CMEZone.com
7
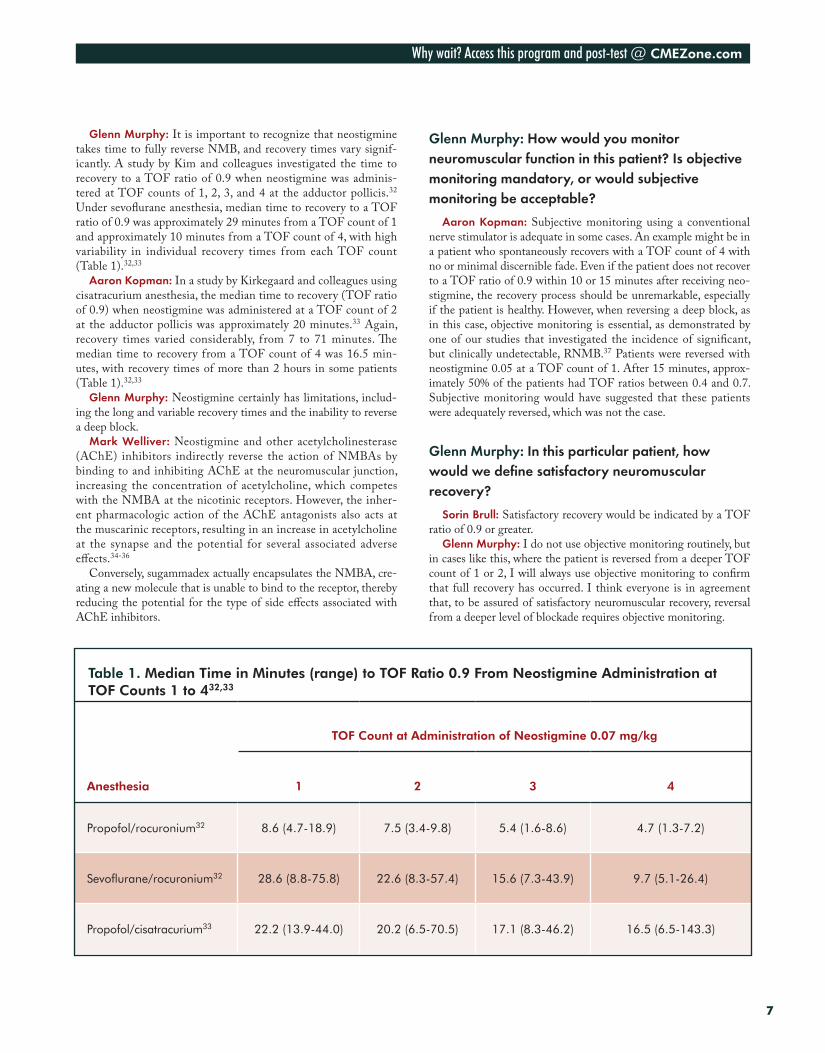
Glenn Murphy: It is important to recognize that neostigmine takes time to fully reverse NMB, and recovery times vary signif-icantly. A study by Kim and colleagues investigated the time to recovery to a TOF ratio of 0.9 when neostigmine was adminis-tered at TOF counts of 1, 2, 3, and 4 at the adductor pollicis.32 Under sevoflurane anesthesia, median time to recovery to a TOF ratio of 0.9 was approximately 29 minutes from a TOF count of 1 and approximately 10 minutes from a TOF count of 4, with high variability in individual recovery times from each TOF count (Table 1).32,33
Aaron Kopman: In a study by Kirkegaard and colleagues using cisatracurium anesthesia, the median time to recovery (TOF ratio of 0.9) when neostigmine was administered at a TOF count of 2 at the adductor pollicis was approximately 20 minutes.33 Again, recovery times varied considerably, from 7 to 71 minutes. The median time to recovery from a TOF count of 4 was 16.5 min-utes, with recovery times of more than 2 hours in some patients (Table 1).32,33
Glenn Murphy: Neostigmine certainly has limitations, includ-ing the long and variable recovery times and the inability to reverse a deep block.
Mark Welliver: Neostigmine and other acetylcholinesterase (AChE) inhibitors indirectly reverse the action of NMBAs by binding to and inhibiting AChE at the neuromuscular junction, increasing the concentration of acetylcholine, which competes with the NMBA at the nicotinic receptors. However, the inher-ent pharmacologic action of the AChE antagonists also acts at the muscarinic receptors, resulting in an increase in acetylcholine at the synapse and the potential for several associated adverse effects.34-36
Conversely, sugammadex actually encapsulates the NMBA, cre-ating a new molecule that is unable to bind to the receptor, thereby reducing the potential for the type of side effects associated with AChE inhibitors.
Glenn Murphy: How would you monitor neuromuscular function in this patient? Is objective monitoring mandatory, or would subjective monitoring be acceptable?
Aaron Kopman: Subjective monitoring using a conventional nerve stimulator is adequate in some cases. An example might be in a patient who spontaneously recovers with a TOF count of 4 with no or minimal discernible fade. Even if the patient does not recover to a TOF ratio of 0.9 within 10 or 15 minutes after receiving neo-stigmine, the recovery process should be unremarkable, especially if the patient is healthy. However, when reversing a deep block, as in this case, objective monitoring is essential, as demonstrated by one of our studies that investigated the incidence of significant, but clinically undetectable, RNMB.37 Patients were reversed with neostigmine 0.05 at a TOF count of 1. After 15 minutes, approx-imately 50% of the patients had TOF ratios between 0.4 and 0.7. Subjective monitoring would have suggested that these patients were adequately reversed, which was not the case.
Glenn Murphy: In this particular patient, how would we define satisfactory neuromuscular recovery?
Sorin Brull: Satisfactory recovery would be indicated by a TOF ratio of 0.9 or greater.
Glenn Murphy: I do not use objective monitoring routinely, but in cases like this, where the patient is reversed from a deeper TOF count of 1 or 2, I will always use objective monitoring to confirm that full recovery has occurred. I think everyone is in agreement that, to be assured of satisfactory neuromuscular recovery, reversal from a deeper level of blockade requires objective monitoring.
Table 1. Median Time in Minutes (range) to TOF Ratio 0.9 From Neostigmine Administration at TOF Counts 1 to 432,33
Anesthesia
TOF Count at Administration of Neostigmine 0.07 mg/kg
1 2 3 4
Propofol/rocuronium32 8.6 (4.7-18.9) 7.5 (3.4-9.8) 5.4 (1.6-8.6) 4.7 (1.3-7.2)
Sevoflurane/rocuronium32 28.6 (8.8-75.8) 22.6 (8.3-57.4) 15.6 (7.3-43.9) 9.7 (5.1-26.4)
Propofol/cisatracurium33 22.2 (13.9-44.0) 20.2 (6.5-70.5) 17.1 (8.3-46.2) 16.5 (6.5-143.3)
Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
8
Sidebar 2: Efficacy and Safety of Sugammadex Versus Neostigmine
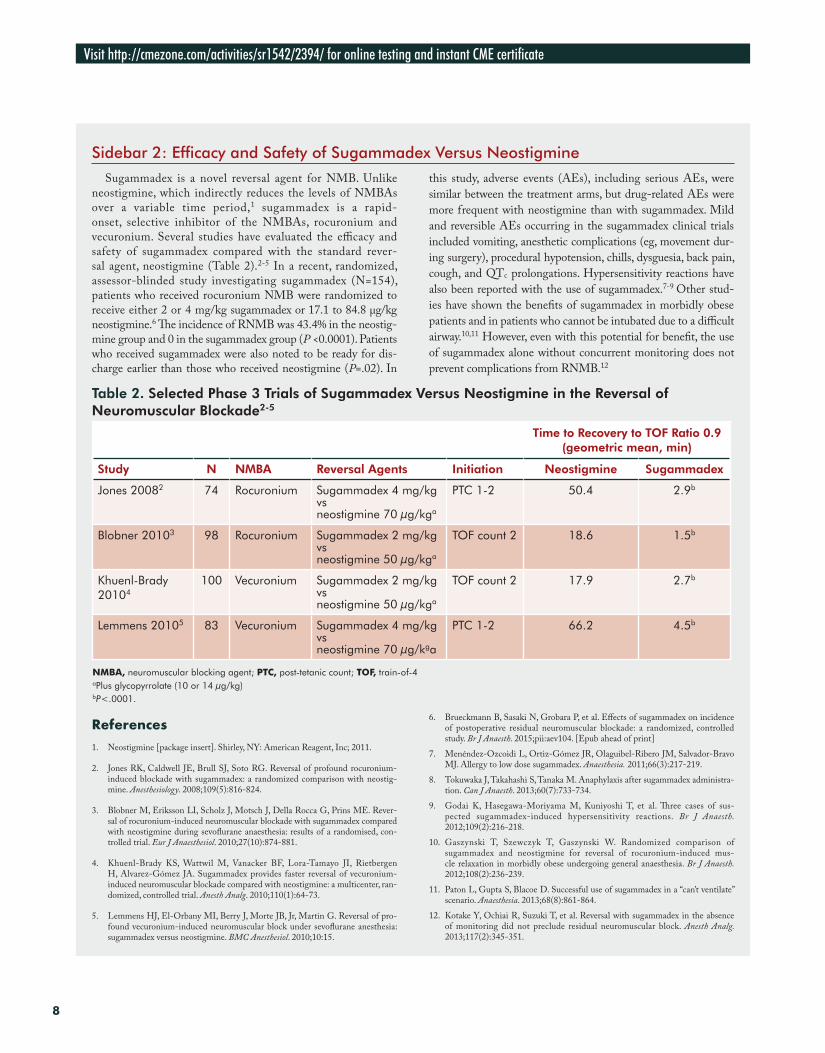
Sugammadex is a novel reversal agent for NMB. Unlike neostigmine, which indirectly reduces the levels of NMBAs over a variable time period,1 sugammadex is a rapid-onset, selective inhibitor of the NMBAs, rocuronium and vecuronium. Several studies have evaluated the efficacy and safety of sugammadex compared with the standard rever-sal agent, neostigmine (Table 2).2-5 In a recent, randomized, assessor-blinded study investigating sugammadex (N=154), patients who received rocuronium NMB were randomized to receive either 2 or 4 mg/kg sugammadex or 17.1 to 84.8 μg/kg neostigmine.6 The incidence of RNMB was 43.4% in the neostig-mine group and 0 in the sugammadex group (P <0.0001). Patients who received sugammadex were also noted to be ready for dis-charge earlier than those who received neostigmine (P=.02). In
this study, adverse events (AEs), including serious AEs, were similar between the treatment arms, but drug-related AEs were more frequent with neostigmine than with sugammadex. Mild and reversible AEs occurring in the sugammadex clinical trials included vomiting, anesthetic complications (eg, movement dur-ing surgery), procedural hypotension, chills, dysguesia, back pain, cough, and QTc prolongations. Hypersensitivity reactions have also been reported with the use of sugammadex.7-9 Other stud-ies have shown the benefits of sugammadex in morbidly obese patients and in patients who cannot be intubated due to a difficult airway.10,11 However, even with this potential for benefit, the use of sugammadex alone without concurrent monitoring does not prevent complications from RNMB.12
Table 2. Selected Phase 3 Trials of Sugammadex Versus Neostigmine in the Reversal of Neuromuscular Blockade2-5
Time to Recovery to TOF Ratio 0.9 (geometric mean, min)
Study N NMBA Reversal Agents Initiation Neostigmine Sugammadex
Jones 20082 74 Rocuronium Sugammadex 4 mg/kg vs neostigmine 70 µg/kga
PTC 1-2 50.4 2.9b
Blobner 20103 98 Rocuronium Sugammadex 2 mg/kg vs neostigmine 50 µg/kga
TOF count 2 18.6 1.5b
Khuenl-Brady 20104
100 Vecuronium Sugammadex 2 mg/kg vs neostigmine 50 µg/kga
TOF count 2 17.9 2.7b
Lemmens 20105 83 Vecuronium Sugammadex 4 mg/kg vs neostigmine 70 µg/kga
PTC 1-2 66.2 4.5b
NMBA, neuromuscular blocking agent; PTC, post-tetanic count; TOF, train-of-4aPlus glycopyrrolate (10 or 14 µg/kg)bP<.0001.
References1. Neostigmine [package insert]. Shirley, NY: American Reagent, Inc; 2011.
2. Jones RK, Caldwell JE, Brull SJ, Soto RG. Reversal of profound rocuronium-induced blockade with sugammadex: a randomized comparison with neostig-mine. Anesthesiology. 2008;109(5):816-824.
3. Blobner M, Eriksson LI, Scholz J, Motsch J, Della Rocca G, Prins ME. Rever-sal of rocuronium-induced neuromuscular blockade with sugammadex compared with neostigmine during sevoflurane anaesthesia: results of a randomised, con-trolled trial. Eur J Anaesthesiol. 2010;27(10):874-881.
4. Khuenl-Brady KS, Wattwil M, Vanacker BF, Lora-Tamayo JI, Rietbergen H, Alvarez-Gómez JA. Sugammadex provides faster reversal of vecuronium-induced neuromuscular blockade compared with neostigmine: a multicenter, ran-domized, controlled trial. Anesth Analg. 2010;110(1):64-73.
5. Lemmens HJ, El-Orbany MI, Berry J, Morte JB, Jr, Martin G. Reversal of pro-found vecuronium-induced neuromuscular block under sevoflurane anesthesia: sugammadex versus neostigmine. BMC Anesthesiol. 2010;10:15.
6. Brueckmann B, Sasaki N, Grobara P, et al. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. Br J Anaesth. 2015;pii:aev104. [Epub ahead of print]
7. Menéndez-Ozcoidi L, Ortiz-Gómez JR, Olaguibel-Ribero JM, Salvador-Bravo MJ. Allergy to low dose sugammadex. Anaesthesia. 2011;66(3):217-219.
8. Tokuwaka J, Takahashi S, Tanaka M. Anaphylaxis after sugammadex administra-tion. Can J Anaesth. 2013;60(7):733-734.
9. Godai K, Hasegawa-Moriyama M, Kuniyoshi T, et al. Three cases of sus-pected sugammadex-induced hypersensitivity reactions. Br J Anaesth. 2012;109(2):216-218.
10. Gaszynski T, Szewczyk T, Gaszynski W. Randomized comparison of sugammadex and neostigmine for reversal of rocuronium-induced mus-cle relaxation in morbidly obese undergoing general anaesthesia. Br J Anaesth. 2012;108(2):236-239.
11. Paton L, Gupta S, Blacoe D. Successful use of sugammadex in a “can’t ventilate” scenario. Anaesthesia. 2013;68(8):861-864.
12. Kotake Y, Ochiai R, Suzuki T, et al. Reversal with sugammadex in the absence of monitoring did not preclude residual neuromuscular block. Anesth Analg. 2013;117(2):345-351.

Why wait? Access this program and post-test @ CMEZone.com
9
CASE STUDY 3
A n 89-year-old woman presents for a transfemoral aortic valve replacement. Her medical history includes type 2 diabetes mellitus, hypertension, chronic renal insufficiency (creatinine 1.8 mg/dL), chronic obstruc-
tive pulmonary disease (COPD) requiring home oxygen therapy, morbid obesity (148 kg), and a stroke 1 year before admission, with residual weakness in her right arm and leg. Her medications include candesartan, atenolol, albuterol, hydrochlorothiazide, metformin (stopped 2 days ago), insulin, and warfarin. On physical examination, her blood pressure is 148/83 mm Hg and heart rate is 65 bpm. She has decreased breath sounds bilaterally (but no wheezing) and a Mallampati class 2 airway. An 18-gauge IV line is started in each arm, and a 20-gauge catheter is placed in the right radial artery. No premedication is used. Anesthesia is induced with etomidate 18 mg, lidocaine 30 mg, fentanyl 50 µg, and rocuronium 40 mg. Anesthesia is maintained with sevoflurane 0.4% to 1.5%. A phenyl-ephrine infusion is used to maintain blood pressure within 20% of baseline values. Forty-five minutes into the pro-cedure, the patient moves and is administered rocuronium 10 mg and fentanyl 100 µg (no other opioid is given intraoperatively). The patient is hemodynamically stable throughout the case, which lasts a total of 90 minutes. At the end of surgery, 2 responses to TOF stimulation are observed at the eye with peripheral nerve stimulation, and 3 mg of neostigmine with 0.6 mg glycopyrrolate (a standard prepared syringe by the pharmacy) is administered. Eight minutes later, when no fade is observed with TOF stimulation, the patient is observed reaching for the ETT and is extubated. During transport to the recovery room, the pulse oximeter indicates that oxygen saturation is decreasing, and the patient appears to be in respiratory distress. On arrival to the recovery room, oxygen saturation is 78%, and the patient appears in extreme distress.
Glenn Murphy: This patient has several risk factors for having an adverse respiratory event in the early postoperative period, including older age, obesity, poor cardiovascular and pulmonary reserve, and renal failure. Was the dose of rocuronium appropriate? Should the dose be reduced in this particular patient, and if so, why?
Sorin Brull: In the elderly, unless you have a need for RSI, all drugs should be used sparingly. It is always easier to administer more drug than it is to correct an overdose. The rocuronium dose of 40 mg was appropriate and sufficient. Forty-five minutes later, if t he patient had no responses to TOF—meaning that less than 5% of the receptors were unoccupied and still functioning—the administration of 10 mg rocuronium may have caused a rel-ative overdose. I am not surprised that she did not breathe well after reversal.
Aaron Kopman: I agree that the dose of rocuronium was appropriate.
Glenn Murphy: The elderly have decreased organ function and decreased metabolism and elimination of steroidal muscle relaxants such as rocuronium. They also have less muscle mass. A study by Arain and colleagues showed that the duration of action of rocuronium can be longer and more variable in the elderly, compared with cisatracurium.38 Reversal also takes longer in an
elderly patient than in a younger patient.39 Also, each subsequent dose of a steroidal muscle relaxant prolongs the effect. Extreme caution is needed when dosing rocuronium in elderly patients. Cisatracurium provides a greater margin of safety in this patient population.
Sorin Brull: Rocuronium does not have active metabolites, but it probably has a wider variability in its duration of action, partic-ularly in the elderly, compared with other muscle relaxants, such as benzylisoquinolinium compounds.
Glenn Murphy: Also, in this particular case, the patient did not move on the table; her diaphragm started moving. It is important to emphasize that the diaphragm is the muscle that is most resis-tant to NMBAs. Often, when breathing begins, the surgeon thinks the patient is moving and requests more NMBA, but it is actually just the diaphragm starting to move, not inadequate blockade.
Mark Welliver: In some of these cases, perhaps the diaphrag-matic movement could be better addressed by administering more fentanyl or increasing the respiratory rate and lowering the end-tidal CO2.
Glenn Murphy: In retrospect, was this patient at increased risk for having postoperative RNMB?
Aaron Kopman: Yes. She is elderly, obese, and has renal failure.Mark Welliver: I agree. A younger person will recover from a
small degree of residual neuromuscular paralysis, but in a patient of this age who already has pulmonary problems (and is receiving

Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
10
oxygen for COPD), that same degree of residual paralysis could worsen the respiratory status. Residual sevoflurane, even in the absence of an NMBA, could also increase the risk for respiratory compromise.
Aaron Kopman: It is also important to emphasize the effect of sevoflurane on the potency of the NMBA. During sevoflurane anesthesia, the 95% effective dose of nondepolarizing relaxants is decreased by about 30% to 35%. Put differently, this represents a 50% increase in potency for the neuromuscular blocker.40,41
Glenn Murphy: At the end of the case, no fade was observed with TOF stimulation and the patient was reaching for the ETT.
Does the absence of fade indicate adequate neuromuscular recovery?
Sorin Brull: If it is absence of fade to visual or tactile detec-tion, these are subjective responses. The TOF ratio can be anywhere between 1.0 and 0.4, and fade cannot be detected when it is as low as 0.4. At that point, I would probably administer a very small dose: 0.01 to 0.02 mg of neostigmine.
Aaron Kopman: It is also important to know how to recognize when the patient is trying to move and is becoming agitated. Obvi-ously, somebody did here and reintubated the patient.
CASE STUDY 4
A 42-year-old woman with hypertension and gastroesophageal reflux disease (controlled with medication) underwent laparoscopic cholecystectomy. Rocuronium 50 mg was used for NMB. A TOF count of 1 at the
facial nerve was observed at surgical closure, and neostigmine 5 mg with glycopyrrolate 1 mg was administered. Shortly after, a TOF count of 4 with no fade was observed. She had 5-second head lift to command and good hand grasp, and the patient’s trachea was extubated. She was receiving 50% oxygen by face mask and was prepared for transport to the PACU, when the oxygen saturation (SpO2) decreased to the low 90% range. She was unable to cough strongly or clear secretions and became agitated. With mask-assisted ventilations, SpO2 increased to 99%. The TOF count at the ulnar nerve was 3. Anesthesia was induced, her trachea was intubated, and she was sent to the PACU with mechanical ventilation. Her trachea was extubated approximately 1 hour later.
Glenn Murphy: What is the potential role of sugammadex in the rescue of residual paralysis due to inadequate reversal by AChE inhibitors?
Mark Welliver: During the early use of sugammadex, it was actu-ally used in this scenario, to rescue poor reversal by an AChE inhib-itor.42 Case reports found no interaction with sugammadex and the AChE inhibitors—it encapsulated all of the NMBA molecules.43-45 Rocuronium and vecuronium will still be fully reversed. Sugamma-dex is not approved by the US Food and Drug Administration, due to the potential for hypersensitivity reactions,46-48 but if it becomes available, it would provide an option for rescuing residual paralysis.
Sorin Brull: An important consideration with sugammadex is that the dose needs to be determined based on the degree of recov-ery, so the dose will differ by patient. Quantitative monitoring will be necessary to determine the degree of recovery. Studies have shown that, if recovery with sugammadex is not guided by objec-tive monitoring, the rate of residual block is about 10% to 15%.49,50 This is not a limitation of the drug; it is a limitation of the clinician who chooses the incorrect dose of sugammadex based on inade-quate assessment of depth of neuromuscular block.
Aaron Kopman: Is subjective, qualitative monitoring of neuromuscular function adequate when sugammadex is used?
Sorin Brull: If clinicians are defining the level of NMB as deep block and moderate block, which, by definition, are subjective eval-uations, then the answer would be no. Clinicians can choose to use subjective monitoring, but they must ask themselves to what extent it is reasonable to continue to “cut corners” when it comes to patient safety. We already know that reversal with sugammadex, when guided by subjective evaluation and clinical criteria, results in residual neuromuscular block.50
Glenn Murphy: For the cases we have discussed, please comment on the key points of communication among members of the perioperative surgical team.
Sorin Brull: Communication with the surgeon and the rest of the perioperative team is essential. We need to understand how the sur-geon defines the level of NMB requested and why that level is needed for the surgical procedure. The team should also communicate about intraoperative monitoring because it is important for guiding reversal and deciding on the appropriate time for tracheal extubation.
Aaron Kopman: It is important for the anesthesia team to understand that surgeons are not always wrong—they sometimes need exactly what they request. Conversely, surgeons need to under-stand that their request may be imposing limitations on the anes-thesia team. Understanding the issues from the perspectives of both the surgeon and the anesthesia provider is critical for reducing com-plications associated with RNMB.

Why wait? Access this program and post-test @ CMEZone.com
11
Glenn Murphy: I agree. Some cases probably benefit from deeper levels of NMB. Currently, we cannot maintain “no twitches” until the end of the case. If sugammadex becomes available, we will be able to offer that option to surgeons who request it.
Mark Welliver: I think we need a consistent standard termi-nology for reversal. It is incumbent upon whoever is monitoring the patient at the bedside to communicate to the team how the patient was specifically evaluated for reversal: include the site of TOF measurement, the TOF count, and, better yet, the objec-tive TOF measurement by accelerometry. Give a complete, thor-ough description of the degree of spontaneous recovery, the dose
of reversal agent administered, and the response, including post-tetanic facilitation, if present. We also need to consider expanding our use of the PNS into the PACU, to provide a thorough assess-ment to the attending anesthesiologist, who often is going to be monitoring the patient postoperatively when the rest of the team moves on to the next case.
Glenn Murphy: That is an excellent point. We also should com-municate that information to the recovery room nurses, who are also important team members. If they are aware that we have some concerns about a potential residual block, they may pay closer attention or call us if they think that the patient is at risk for devel-oping problems or residual block.
CONCLUSION
Clinicians may not appreciate the true incidence of RNMB in their anesthesia practice. Furthermore, no definitive guidelines are available on monitoring NMB and managing RNMB, should it occur. The suc-cessful management of patients through NMB and recovery requires a multidisciplinary effort, whereby the anesthesia and surgical teams
have a thorough understanding of the depth of NMB required for a procedure and the optimal methods for inducing, monitoring, and reversing that blockade. Effective communication among these team members is necessary to optimize patient outcomes and reduce post-operative RNMB and its associated complications.
REfERENCES1. Ishizawa Y. Special article: general anesthetic gases and the global environment.
Anesth Analg. 2011;112(1):213-217.2. Grosse-Sundrup M, Henneman JP, Sandberg WS, et al. Intermediate acting non-
depolarizing neuromuscular blocking agents and risk of postoperative respira-tory complications: prospective propensity score matched cohort study. BMJ. 2012;345:e6329.
3. Murphy GS, Szokol JW, Avram MJ, et al. Postoperative residual neuromuscular block-ade is associated with impaired clinical recovery. Anesth Analg. 2013;117(1):133-141.
4. Murphy GS, Brull SJ. Residual neuromuscular block: lessons unlearned. Part I: def-initions, incidence, and adverse physiologic effects of residual neuromuscular block. Anesth Analg. 2010;111(1):120-128.
5. Murphy GS, Szokol JW, Marymont JH, et al. Intraoperative acceleromyographic monitoring reduces the risk of residual neuromuscular blockade and adverse respira-tory events in the postanesthesia care unit. Anesthesiology. 2008;109(3):389-398.
6. Murphy GS, Szokol JW, Marymont JH, Franklin M, Avram MJ, Vender JS. Resid-ual paralysis at the time of tracheal extubation. Anesth Analg. 2005;100(6):1840-1845.
7. Murphy GS. Residual neuromuscular blockade: incidence, assessment, and relevance in the postoperative period. Minerva Anestesiol. 2006;72(3):97-109.
8. Cammu G, De Witte J, De Veylder J, et al. Postoperative residual paralysis in outpa-tients versus inpatients. Anesth Analg. 2006;102(2):426-429.
9. Yip PC, Hannam JA, Cameron AJ, Campbell D. Incidence of residual neuromuscu-lar blockade in a post-anaesthetic care unit. Anaesth Intensive Care. 2010;38(1):91-95.
10. Pietraszewski P, Gaszynski T. Residual neuromuscular block in elderly patients after surgical procedures under general anaesthesia with rocuronium. Anaesthesiol Intensive Ther. 2013;45(2):77-81.
11. Gaszynski T, Szewczyk T, Gaszynski W. Randomized comparison of sugammadex and neostigmine for reversal of rocuronium-induced muscle relaxation in morbidly obese undergoing general anaesthesia. Br J Anaesth. 2012;108(2):236-239.
12. Kaan N, Kocaturk O, Kurt I, Cicek H. The incidence of residual neuromuscular blockade associated with single dose of intermediate-acting neuromuscular blocking drugs. Middle East J Anaesthesiol. 2012;21(4):535-541.
13. Naguib M, Kopman AF, Lien CA, Hunter JM, Lopez A, Brull SJ. A survey of cur-rent management of neuromuscular block in the United States and Europe. Anesth Analg. 2010;111(1):110-119.
14. Fortier LP, McKeen D, Turner K, et al. The RECITE Study: a Canadian prospective, multicenter study of the incidence and severity of residual neuromuscular blockade. Anesth Analg. 2015;121(2):366-372.
15. Lemmens HJ, Brodsky JB. The dose of succinylcholine in morbid obesity. Anesth Analg. 2006;102(2):438-442.
16. Kopman AF, Yee PS, Neuman GG. Relationship of the train-of-four fade ratio to clinical signs and symptoms of residual paralysis in awake volunteers. Anesthesiology. 1997;86(4):765-771.
17. Heier T, Caldwell JE, Feiner JR, Liu L, Ward T, Wright PM. Relationship between normalized adductor pollicis train-of-four ratio and manifestations of residual neuro-muscular block: a study using acceleromyography during near steady-state concentra-tions of mivacurium. Anesthesiology. 2010;113(4):825-832.
18. Lemmens HJ, El-Orbany MI, Berry J, Morte JB, Jr., Martin G. Reversal of profound vecuronium-induced neuromuscular block under sevoflurane anesthesia: sugamma-dex versus neostigmine. BMC Anesthesiol. 2010;10:15.
19. Hemmerling TM, Donati F. Neuromuscular blockade at the larynx, the diaphragm and the corrugator supercilii muscle: a review. Can J Anaesth. 2003;50(8):779-794.
20. Donati F, Meistelman C, Plaud B. Vecuronium neuromuscular blockade at the diaphragm, the orbicularis oculi, and adductor pollicis muscles. Anesthesiology. 1990;73(5):870-875.
21. Duvaldestin P, Kuizenga K, Saldien V, et al. A randomized, dose-response study of sugammadex given for the reversal of deep rocuronium- or vecuronium-induced neu-romuscular blockade under sevoflurane anesthesia. Anesth Analg. 2010;110(1):74-82.
22. Llauradó S, Sabaté A, Ferreres E, Camprubí I, Cabrera A. Sugammadex ideal body weight dose adjusted by level of neuromuscular blockade in laparoscopic bariatric sur-gery. Anesthesiology. 2012;117(1):93-98.
23. Van Lancker P, Dillemans B, Bogaert T, Mulier JP, De Kock M, Haspeslagh M. Ideal versus corrected body weight for dosage of sugammadex in morbidly obese patients. Anaesthesia. 2011;66(8):721-725.
24. Nepveu ME, Donati F, Fortier LP. Train-of-four stimulation for adductor pollicis neuromuscular monitoring can be applied at the wrist or over the hand. Anesth Analg. 2005;100(1):149-154.
25. Thilen SR, Hansen BE, Ramaiah R, Kent CD, Treggiari MM, Bhananker SM. Intraoperative neuromuscular monitoring site and residual paralysis. Anesthesiology. 2012;117(5):964-972.
26. Caffrey RR, Warren ML, Becker KE Jr. Neuromuscular blockade monitor-ing comparing the orbicularis oculi and adductor pollicis muscles. Anesthesiology. 1986;65(1):95-97.
27. Saitoh Y, Koitabashi Y, Makita K, Tanaka H, Amaha K. Train-of-four and double burst stimulation fade at the great toe and thumb. Can J Anaesth. 1997;44(4):390-395.
28. Kitajima T, Ishii K, Kobayashi T, Ogata H. Differential effects of vecuronium on the thumb and great toe as measured by accelography and electromyography. Anaesthe-sia. 1995;50(1):76-78.
29. Todd MM, Hindman BJ, King BJ. The implementation of quantitative electromyo-graphic neuromuscular monitoring in an academic anesthesia department. Anesth Analg. 2014;119(2):323-331.
Visit http://cmezone.com/activities/sr1542/2394/ for online testing and instant CME certificate
1288
SR1542
30. Bartkowski RR. Incomplete reversal of pancuronium neuromuscular blockade by neostigmine, pyridostigmine, and edrophonium. Anesth Analg. 1987;66(7):594-598.
31. Jones RK, Caldwell JE, Brull SJ, Soto RG. Reversal of profound rocuronium-induced blockade with sugammadex: a randomized comparison with neostigmine. Anesthesi-ology. 2008;109(5):816-824.
32. Kim KS, Cheong MA, Lee HJ, Lee JM. Tactile assessment for the reversibility of rocuronium-induced neuromuscular blockade during propofol or sevoflurane anes-thesia. Anesth Analg. 2004;99(4):1080-1085.
33. Kirkegaard H, Heier T, Caldwell JE. Efficacy of tactile-guided reversal from cisatra-curium-induced neuromuscular block. Anesthesiology. 2002;96(1):45-50.
34. Srivastava A, Hunter JM. Reversal of neuromuscular block. Br J Anaesth. 2009;103(1):115-129.
35. Nair VP, Hunter JM. Anticholinesterases and anticholinergic drugs. Contin Educ Anaesth Crit Care Pain. 2004;4(5):164-168.
36. Neostigmine [package insert]. Shirley, NY: American Reagent, Inc; 2011.37. Kopman AF, Kopman DJ, Ng J, Zank LM. Antagonism of profound cisatracurium
and rocuronium block: the role of objective assessment of neuromuscular function. J Clin Anesth. 2005;17(1):30-35.
38. Arain SR, Kern S, Ficke DJ, Ebert TJ. Variability of duration of action of neuromus-cular-blocking drugs in elderly patients. Acta Anaesthesiol Scand. 2005;49(3):312-315.
39. McCarthy GJ, Cooper R, Stanley JC, Mirakhur RK. Dose-response relationships for neostigmine antagonism of vecuronium-induced neuromuscular block in adults and the elderly. Br J Anaesth. 1992;69(3):281-283.
40. Lowry DW, Mirakhur RK, McCarthy GJ, Carroll MT, McCourt KC. Neuromuscu-lar effects of rocuronium during sevoflurane, isoflurane, and intravenous anesthesia. Anesth Analg. 1998;87(4):936-940.
41. Vanlinthout LE, Booij LH, van Egmond J, Robertson EN. Effect of isoflurane and sevoflurane on the magnitude and time course of neuromuscular block produced by vecuronium, pancuronium and atracurium. Br J Anaesth. 1996;76(3):389-395.
42. Welliver M, Cheek D, Osterbrink J, McDonough J. Worldwide experi-ence with sugammadex sodium: implications for the United States. AANA J. 2015;83(2):107-115.
43. Lenz A, Hill G, White PF. Emergency use of sugammadex after failure of standard reversal drugs. Anesth Analg. 2007;104(3):585-586.
44. Weekes G, Hayes N, Bowen M. Reversal of prolonged rocuronium neuromuscu-lar blockade with sugammadex in an obstetric patient with transverse myelitis. Int J Obstet Anesth. 2010;19(3):333-336.
45. de Menezes CC, Peceguini LA, Silva ED, Simões CM. Use of sugammadex after neostigmine incomplete reversal of rocuronium-induced neuromuscular blockade. Rev Bras Anestesiol. 2012;62(4):543-547.
46. Menéndez-Ozcoidi L, Ortiz-Gómez JR, Olaguibel-Ribero JM, Salvador-Bravo MJ. Allergy to low dose sugammadex. Anaesthesia. 2011;66(3):217-219.
47. Tokuwaka J, Takahashi S, Tanaka M. Anaphylaxis after sugammadex administration. Can J Anaesth. 2013;60(7):733-734.
48. Godai K, Hasegawa-Moriyama M, Kuniyoshi T, et al. Three cases of suspected sugammadex-induced hypersensitivity reactions. Br J Anaesth. 2012;109(2):216-218.
49. Ledowski T, Hillyard S, O’Dea B, et al. Introduction of sugammadex as standard reversal agent: impact on the incidence of residual neuromuscular blockade and post-operative patient outcome. Indian J Anaesth. 2013;57(1):46-51.
50. Kotake Y, Ochiai R, Suzuki T, et al. Reversal with sugammadex in the absence of monitoring did not preclude residual neuromuscular block. Anesth Analg. 2013;117(2):345-351.
CME Post-Test
1. Which of the following is the approx-imate incidence of residual neuro-muscular blockade in surgical cases involving neuromuscular blocking agents?a. <10% of all casesb. 10%-20% of bariatric surgery casesc. Approximately 30% of all casesd. Approximately 30% of geriatric sur-
gery cases
2. Which of the following is true regard-ing clinical assessment of residual paralysis?a. Head lift for 5 seconds is the most reli-
able determinate of adequacy of NMB reversal
b. Hand-grasp ability signifies full recov-ery of motor function
c. Inability to smile, swallow, or speak is highly indicative of residual paralysis
d. Clinical signs are unreliable to exclude the presence of residual paralysis
3. Which of the following is the best cri-terion for measuring the optimal tar-get for neuromuscular recovery after NMB?a. Head-lift for 5 secondsb. Train-of-Four ratio (TOFr) >0.9c. Equal 4/4 Train-of-Four count (TOFc)d. Equal double-burst stimulation
4. A 39-year-old, healthy female is undergoing laparoscopic total abdom-inal hysterectomy. Rocuronium is used as the neuromuscular blocking agent and administered intermittently to keep the train-of-four (TOF) count at less than 2 at the adductor pollicis. At
the time of surgical completion, rever-sal with neostigmine was initiated. According to Kim et al, what average time to recovery to a TOFr of 0.9 would you expect?a. 5-10 minutesb. 15-20 minutesc. 25-30 minutesd. 35-40 minutes
5. A 64 year old female patient with morbid obesity (body mass index of 56 kg/m2) presents for bariatric sur-gery. The airway examination reveals the potential for difficult intubation. Which of the following is not a risk factor for complications from RNMB?a. Ageb. Female sexc. Obesityd. Difficult airway
6. For the patient in question 4, which of the following options would be the safest approach to securing the air-way in this patient?a. Awake/sedated intubationb. Laryngeal mask airwayc. Rapid sequence intubation with NMBAd. Sedated fiberoptic intubation
7. When monitoring for neuromuscu-lar blockade, which of the follow-ing nervs would provide the strongest correlation with the diaphragm?a. Facialb. Common peronealc. Posterior tibiald. Ulnar
8. Which of the following neuromuscu-lar blocking agents has been shown to have the greatest variability of duration in elderly patients?a. Atracuriumb. Cisatracuriumc. Rocuroniumd. Succinylcholine
9. Studies have shown that when sugammadex is used for reversal of deep neuromuscular blockade (post-tetanic count 1-2; train-of-four [TOF] count 2), average time to recovery to a TOF ratio of 0.9 is approximately:a. 1-5 minutesb. 10-15 minutesc. 20-25 minutesd. 30-35 minutes
10. Considering factors that may contrib-ute to prolonged or residual paraly-sis and the challenges of managing and reversing NMB, which of the fol-lowing has been recommended to improve outcomes and patient safety?a. Avoidance of NMBAsb. Maintenance of only shallow levels of
NMB (TOFc 3-4/4)c. Effective communication among all
team membersd. Increased doses of cholinesterase
inhibitors
Assessment and Reversal of Neuromuscular Blockade: Current and Emerging Strategies
ID # 11148-EJ-42