Embed Size (px)
Citation preview

Cedieclwnhate
A
CnCAttsdt
Mot
s
DU
0d
Assessment and Key Targets for Therapy in the Post-MyocardialInfarction Patient with Left Ventricular Dysfunction
James D. Flaherty, MD,a,* James E. Udelson, MD,b Mihai Gheorghiade, MD,a
Edwin Wu, MD,a and Charles J. Davidson, MDa
In the post-myocardial infarction (MI) patient with coronary artery disease (CAD)and left ventricular dysfunction (LVD), ischemia and adverse remodeling hindermyocardial performance and increase electrical instability. Collectively, the coronaryarteries, myocardium, and conduction system represent the principal pathophysio-logic targets in MI complicated by LVD. Consequently, an accurate assessment ofdisease severity in these targets is essential for the design of an effective therapeuticprogram. This review describes the current modalities for assessing the key patho-physiologic targets in post-MI patients with LVD and the effects of systemic factorson cardiac disease severity. © 2008 Elsevier Inc. All rights reserved. (Am J Cardiol
2008;102[suppl]:5G–12G)cp(cvuruippgm
poctacs
M
LmMmatTps(s
oronary atherosclerosis is the principal cause of isch-mic heart disease, producing atherosclerotic lesions thatevelop over several decades and can ultimately precip-tate myocardial infarction (MI). As coronary artery dis-ase (CAD) progresses, plaque formation can assumelinical significance, especially in lesions that are rich inipids. Although plaques can evolve into stenotic lesionsith a hard fibrous composition, they can also be “vul-erable” without necessarily being obstructive but with aigher likelihood of rupture. When lesions do rupture, thebrupt change in morphology that occurs can lead tohrombus formation and the development of acute isch-mic syndromes, including unstable angina and MI.1
ssessing Coronary Artery Disease
oronary angiography remains the “gold standard” tech-ique for assessing the presence, extent, and severity ofAD and for determining appropriate therapy. Currentmerican College of Cardiology/American Heart Associa-
ion (ACC/AHA) guidelines strongly recommend (class 1)hat coronary angiography be performed in patients withuspected CAD, including post-MI patients who are candi-ates for primary or rescue percutaneous coronary interven-ion.2 Likewise, early angiography with the goal of revas-
aDivision of Cardiology, Department of Medicine, Feinberg School ofedicine, Northwestern University, Chicago, Illinois, USA; and bDivision
f Cardiology, Department of Medicine, Tufts-New England Medical Cen-er, Boston, Massachusetts, USA.
Statement of author disclosure: Please see the Author Disclosuresection at the end of this article.
*Address for reprints: James D. Flaherty, MD, Division of Cardiology,epartment of Medicine, Feinberg School of Medicine, Northwesternniversity, 251 East Huron Street, Galter 8-130, Chicago, Illinois 60611.
cE-mail address: [email protected].
002-9149/08/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.amjcard.2008.06.005
ularization is also strongly recommended (class 1) inatients with unstable angina/non-ST-segment elevation MInon-STEMI) and any high-risk features, including elevatedardiac biomarkers, ST-segment depression, a reduced leftentricular ejection fraction (LVEF), or signs of heart fail-re (HF).3 Angiography can also identify candidates forevascularization among patients with post-MI left ventric-lar dysfunction (LVD) who present late or have had clin-cally “silent” MI. The technique is especially useful inatients with ongoing angina, ischemia, or HF. Angiogra-hy may also be necessary to identify obvious bypass sur-ery candidates, such as those with LVD and significant leftain CAD.Multislice spiral computed tomographic angiography is a
romising noninvasive imaging modality for the assessmentf CAD. Although it is not as accurate as angiography forharacterizing CAD, partly because of the rapid motion ofhe beating heart and the small dimensions of the coronaryrteries, it could prove to be a useful method for ruling outoronary stenoses in low-risk patients reporting possibleymptoms of ischemia.4
yocardium: Assessing Left Ventricular Dysfunction
eft ventricular function has long been recognized as aajor predictor of both short- and long-term survival afterI. Although LVEF has been the most frequently usedeasure of left ventricular function and a higher LVEF is
ssociated with increased survival, it is not the only factorhat predicts mortality in the post-MI patient with LVD.his was demonstrated in the Oregon Sudden Unex-ected Death Study, where an LVEF of �0.35 was ob-erved in only 30% of cases of sudden cardiac deathSCD) in which left ventricular function had been as-essed within the preceding 2 years.5 This seeming dis-
repancy might exist because although LVEF is primarilywww.AJConline.org

amtpCewc
LivEwmgBdmd
tfrTtvtlgvrt5
ta
pppc
Fiw
Fat(
6G The American Journal of Cardiology (www.AJConline.org) Vol 102 (5A) September 8, 2008
measure of chronic risk associated with the burden ofyocardial scar, there are a number of transient func-
ional disturbances and electrophysiologic events that canrecipitate a fatal arrhythmia without a lowered LVEF.onditions such as transient ischemia and reperfusion,lectrolyte disturbances, and autonomic fluctuationsould not be detected by an LVEF assessment, but they
ould precede a fatal arrhythmia.6
Several indices have been proposed as alternatives toVEF for predicting risk of SCD in patients with CAD,
ncluding end-systolic volume (ESV) and end-diastolicolume (EDV).7 White and colleagues7 measured ESV,DV, and LVEF 1–2 months post MI in 605 patients,ho were then observed for a mean duration of 78onths. A statistical analysis revealed that ESV was of
reater value for predicting survival than EDV or LVEF.ecause ESV is essentially a measure of left ventricularilation, the investigators concluded that ventricular re-odeling is the major identifiable risk factor for cardiac
eath after MI.7
Many recent trials have addressed the issue of assessinghe prognostic power of different indices of left ventricularunction by studying post-MI patients who have undergoneeperfusion. The Global Utilization of Streptokinase andissue Plasminogen Activator for Occluded Coronary Ar-
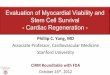
eries (GUSTO) angiographic investigators assessed leftentricular function 90 minutes after thrombolysis in pa-ients with acute MI. They found that multiple markers ofeft ventricular function, including LVEF, ESV, and re-ional wall motion, were predictive of 30-day post-MI sur-ival (Figure 1).8 Meanwhile, Bolognese and colleagues9
eported that remodeling assessed by left ventricular dila-ion (�20% increase in EDV) was a good predictor of
igure 1. Indices of left ventricular function 90 minutes after thrombolysin patients who died before 30 days after an acute MI (p � 0.001). ESVI �ith permission from N Engl J Med.8)
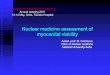
-year cardiac mortality in patients with MI who were o
reated with primary percutaneous transluminal coronaryngioplasty (Figure 2).
Ongoing ischemia after MI can be an important thera-eutic target. Recently, it was demonstrated that post-MIatients with silent ischemia randomized to balloon-onlyercutaneous coronary intervention had markedly reducedardiac events and a higher average LVEF through 10 years
ients who survived 30 days after an acute myocardial infarction (MI) andstolic volume index; LVEF � left ventricular ejection fraction. (Reprinted
igure 2. Kaplan-Meier survival curves for cardiac death in patients withnd without left ventricular remodeling at 6 months after primary percu-aneous coronary intervention for acute myocardial infarction (p � 0.005).Reprinted with permission from Circulation.9)
s in patend-sy
f follow-up versus medical management alone.10 In

pavartdfsm
atmvtrtdr(
pwl(vf
ieomtbtmvi
droedrtaon
ccswa
whein
dmrchvlprfbtu
twwvwmcrc
ctarWmMossr
E
Pucid
pSmf
7GFlaherty et al/Assessment and Key Targets for Therapy in the Post-MI Patient with LV Dysfunction
ost-MI patients without ongoing ischemia, myocardial vi-bility may be an important therapeutic target. Because leftentricular function can improve significantly in patients withdysfunctional but viable myocardium who undergo coronary
evascularization, viability testing offers a means for predictinghe reversibility of LVD. Viable but dysfunctional myocar-ium may either be “hibernating” or “stunned,” with theormer representing myocardium that has adapted to a chronictate of underperfusion and the latter an adequately perfusedyocardium that is dysfunctional because of active ischemia.11
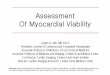
In a meta-analysis of 24 published studies, Allman et al12
ssessed late survival after revascularization or medicalherapy in patients with CAD and LVD who underwentyocardial viability testing. In patients with myocardial
iability, annual mortality was significantly lower in pa-ients treated with revascularization than it was in the groupeceiving medical treatment alone. In contrast, among pa-ients without myocardial viability, there were no significantifferences in mortality rates between those undergoingevascularization and those receiving medical therapy aloneFigure 3).12
A recent retrospective observational study examined ap-roximately 4,000 patients with HF and CAD, most ofhom (78.2%) had LVD. Patients who underwent revascu-
arization had substantially reduced mortality at 1 year11.8% vs 21.6%; hazard ratio, 0.52; 95% confidence inter-al, 0.47–0.58), which was maintained through 7 years ofollow-up.13
A number of noninvasive imaging methods are used todentify viable myocardium in patients with LVD. Positronmission tomography imaging uses enhanced 18F-fluorode-xyglucose uptake relative to myocardial blood flow as aarker for myocardial viability. Thallium-201 single-pho-
on emission computed tomography imaging assesses mem-rane integrity and myocardial perfusion by measuring up-ake several hours after radioisotope administration. A thirdethod, low-dose dobutamine echocardiography, detects
iability by measuring myocardial contractile reserve dur-ng inotropic stimulation.11
The techniques used to assess myocardial viability caniffer in their accuracy for predicting improvement afterevascularization (Figure 4). Although the combined resultsf 34 studies involving 926 patients showed that positronmission tomography and dobutamine echocardiographyisplayed similar accuracy for predicting improvement inegional left ventricular function after revascularization,hallium single-photon emission computed tomography im-ging showed a lower positive predictive value than thether 2 methods. It did, however, demonstrate a betteregative predictive value.11
A newer method of identifying regions of viable myo-ardium after MI involves the use of contrast-enhancedardiac magnetic resonance imaging (CMR). In animaltudies, hyperenhancement on CMR was found to coincideith both the extent of myocyte necrosis developing days
fter injury and with the extent of scar tissue measured t
eeks later.14 In human studies, the signal intensity ofyperenhanced regions, which correspond to infarcted ar-as, was much higher than it was for normal myocardium,ndicating that CMR can accurately differentiate betweenormal and injured regions of myocardium.15
Kim et al16 used CMR to identify reversible myocardialysfunction before revascularization. Among dysfunctionalyocardial segments, the likelihood of improvement in
egional contractility after revascularization was signifi-antly and inversely related to the transmural extent ofyperenhancement. In addition, the percentage of the leftentricle that was dysfunctional but viable before revascu-arization was strongly correlated with the degree of im-rovement in the global wall motion score and LVEF afterevascularization.16 In a subsequent study, the same groupound a strong correlation between infarct transmurality ataseline, as measured by CMR, and improvement in con-ractile function at 8–12 weeks in post-MI patients whonderwent successful revascularization.17
�-Blockers are known to improve left ventricular func-ion and reduce morbidity and mortality in post-MI patientsith LVD and HF. However, some patients do not respondell to such therapy, which suggests that they have lessiable myocardium. Evidence supporting this hypothesisas obtained in a study using CMR to visualize regions ofyocardial scarring and viability in patients with HF re-
eiving �-blocker therapy. The transmural extent of scar-ing was found to be inversely related to improvement inontractility after 6 months of �-blocker therapy.18
Another predictor of outcome is the degree of microvas-ular obstruction after MI. Obstruction of the microcircula-ion has been associated with both poor recovery of globalnd regional left ventricular function soon after successfuleperfusion19 and with a higher risk for developing HF.20
u et al21 used CMR to visualize regions of significanticrovascular obstruction at the infarct core in patients afterI. After an average follow-up of 16 months, the presence
f microvascular obstruction was found to be predictive oferious cardiovascular complications. Even with the infarctize controlled, the presence of microvascular obstructionemained a prognostic indicator of post-MI complications.21
lectrical Markers of Arrhythmic Risk
ost-MI patients with LVD are at an increased risk of SCD,sually from ventricular tachyarrhythmias. Because electri-al instability is a precursor to fatal arrhythmia, identifyingndices of myocardial electrical activity might help to pre-ict SCD risk.
A number of measures have been theorized to haverognostic value for identifying patients at high risk forCD, especially in the first year after MI. Among sucheasures is the occurrence of ambient arrhythmias, such as
requent premature depolarizations22 and nonsustained ven-
ricular tachycardia.23,24 Although early studies suggested
adta
ir
Fm om J A
FCep
8G The American Journal of Cardiology (www.AJConline.org) Vol 102 (5A) September 8, 2008
n association with SCD, a survival benefit has not beenemonstrated for suppression of such arrhythmias.25 In con-rast, spontaneous nonsustained ventricular tachycardia and
igure 3. Annual mortality rates for patients with coronary artery diseaseedical treatment and myocardial viability. (Reprinted with permission fr
igure 4. Predictive value of myocardial viability assessment tools for improABG � coronary artery bypass graft surgery; Echo � echocardiography;mission tomography; PTCA � percutaneous transluminal coronary angioermission from Circulation.11)
low LVEF have been shown to be important predictors of l
mproved survival in post-MI patients with LVD who haveeceived an implantable cardioverter defibrillator (ICD).23
Standard electrocardiographic measures, such as the
t ventricular dysfunction stratified by coronary revascularization (revasc.)m Coll Cardiol.12)
t in regional left ventricular (LV) function after coronary revascularization.18F-fluorodeoxyglucose; MBF � myocardial blood flow; PET � positron
SPECT � single-photon emission computed tomography. (Reprinted with
and lef
vemenFDG �plasty;
ength of the QRS and QT intervals, have also been pro-

plbiwspedmtQwr
mpas
S
Ai
pwoc
twnrert
acTntb
Rst
FEet
9GFlaherty et al/Assessment and Key Targets for Therapy in the Post-MI Patient with LV Dysfunction
osed as markers of arrhythmic risk in post-MI patients. Aonger QRS interval duration on initial electrocardiographyefore reperfusion therapy was associated with an increasen 30-day mortality in patients with MI who were treatedith thrombolysis.26 Similarly, a longer QRS duration ob-
erved on discharge electrocardiography was reported to beredictive of worse 4-year survival after a first MI.27 How-ver, in a study of patients receiving an ICD, QRS durationid not correlate with the occurrence of ventricular arrhyth-ias over a 12-month follow-up period.28 For post-MI pa-
ients who go on to develop symptomatic HF, a prolongedRS duration is an indicator of ventricular dyssynchrony,hich is predictive of a therapeutic response to cardiac
esynchronization therapy.29
Other markers of electrical instability predict fatal arrhyth-ias with varying degrees of success. These include QT dis-
ersion,30–33 microvolt T-wave alternans,34–36 and signal-veraged electrocardiography for detecting microvolt levelignals in the terminal QRS complex.37–39
ystemic Factors Affecting Pathophysiologic Targets
lthough the structural and proarrhythmic consequences of
igure 5. Algorithm for assessing patients with ST-segment elevation myocho � echocardiography; EF � left ventricular ejection fraction. *Higlectrical instability. †Significant ischemia includes moderate-to-severe strereadmill score. (Reprinted with permission from J Am Coll Cardiol.2)
schemia are most important in determining the prognosis in t
ost-MI patients, systemic factors play a significant role, asell. Among these is the neurohormonal activation thatccurs in patients with LVD after MI and several comorbidonditions.
Neurohormonal activation: A complex set of maladap-ive neurohormonal changes occurs in the post-MI patientith LVD. These include activation of the sympatheticervous system (SNS) and the renin-angiotensin-aldoste-one system (RAAS). Neurohormonal activation can causelectrical instability, increasing the risk of ventricular ar-hythmia, and it can induce ventricular remodeling, leadingo a worsening of LVD and the development of HF.
In LVD, a baroreceptor-mediated increase in SNSctivity has a number of consequences, including tachy-ardia, arterial vasoconstriction, and venoconstriction.40
he increased regional and circulating concentrations oforepinephrine that accompany SNS activation can beoxic to cardiac myocytes, an effect that can be reversedy �-blockade.40,41
Another important effect of increased SNS activity isAAS activation.40 The adverse effects of angiotensin make
uppression of its activity an important component of post-MIreatment. Angiotensin II is a potent peripheral vasoconstrictor
infarction (STEMI). Cath � catheterization; ECG � electrocardiography;features include cardiogenic shock and persistent hemodynamic and/orced myocardial perfusion or wall motion abnormalities and/or a high-risk
cardialh-riskss-indu
hat can induce ventricular hypertrophy.42,43 Angiotensin II

arl
dnilmibvTetp
rtoeaplmswGcwath
cpwPahgphawmp
WP
ASu
bDrfpdp
ppfot
C
Cdtaidats
A
T
TGv
G
I
P
A
P
Arnfli
10G The American Journal of Cardiology (www.AJConline.org) Vol 102 (5A) September 8, 2008
lso stimulates secretion of aldosterone, which causes sodiumetention, further contributing to the development of ventricu-ar hypertrophy.43
Comorbidities: Among comorbid conditions, type 2iabetes mellitus causes significant metabolic, hemody-amic, and neurohormonal changes, which collectivelyncrease cardiovascular risk in the post-MI patient. Insu-in resistance plays a central role through its impact onultiple regulatory pathways. The compensatory hyper-
nsulinemia associated with insulin resistance raiseslood pressure by increasing SNS activity. It also acti-ates RAAS, causing an increase in angiotensin levels.he use of a glucose-insulin infusion followed by anxtended course of subcutaneous insulin has been showno improve long-term survival in patients with diabetesresenting with an acute MI.44
Hyperinsulinemia has also been shown to decrease ad-enal medullary activity, an effect that appears to contributeo dyslipidemia, which is characterized by decreased levelsf high-density lipoprotein and increased levels of triglyc-rides.45–47 Dyslipidemia contributes to CAD progressionnd increases the risk of future coronary events. For exam-le, in men with cardiovascular disease and high total cho-esterol, the risk of death from cardiovascular disease isuch higher than for similarly affected men with normal
erum cholesterol levels.48 A study of middle-aged men,hich was a follow-up to the Primary Prevention Study inöteborg, Sweden, found that 76% of healthy men with low
holesterol and 65% of healthy men with high cholesterolere still alive 16 years after enrollment. By contrast,
mong men with prior MI, 50% of those with low choles-erol were still alive compared with only 21% of those withigh cholesterol.49
Preexisting hypertension in patients with MI is anotheromorbid condition that can negatively affect patientrognoses. Richards et al50 compared patients with MIho had antecedent hypertension with those who did not.lasma neurohormones, which included norepinephrinend the cardiac natriuretic peptides, were significantlyigher in the hypertensive group than in the normotensiveroup days after MI, and these increases were still ap-arent several months later. Patients with hypertensionad larger left ventricular systolic and diastolic volumesnd a lower average LVEF compared with patients whoere normotensive. Finally, the rate of postdischargeortality and the risk of subsequent HF were higher in
atients with hypertension.50
orkup and Management Goals in theost-MI Patient
n algorithm for appropriate workup of the patient withTEMI is presented in Figure 5. A similar scheme can be
sed for a patient with non-STEMI, although there may not te the same urgency to achieve immediate reperfusion.etermining the LVEF is crucial to the early assignment of
isk, but information beyond LVEF is also essential forurther elaborating mortality risk and deciding on a thera-eutic strategy. Angiography, electrocardiography, echocar-iography, exercise testing, and viability imaging all maylay a role in a comprehensive assessment.
There are 4 principal goals for management of theost-MI patient with LVD, each associated with �1 thera-eutic options (Table 1). The particular treatment prescribedor an individual patient should be guided by an assessmentf the key pathophysiologic targets: the coronary arteries,he myocardium, and the conduction system.
onclusion
ollectively, the coronary arteries, myocardium and con-uction system represent the principal pathophysiologicalargets in MI complicated by LVD. Systemic factors, suchs neurohormonal activation and comorbid conditions, alsompact prognosis and therapies. An accurate assessment ofisease severity in these targets is essential for the design oftherapeutic program. The therapeutic options available for
reatment of the post-MI patient with LVD are the subject ofubsequent articles in this series.51–54
uthor Disclosures
he authors who contributed to this article have disclosed
able 1oals in the management of post-myocardial infarction with leftentricular dysfunction and recommended therapies
oal Therapy
mprove symptoms Therapies aimed at ischemia and/orcongestion
revent future coronary events(CAD progression)
StatinsAntiplatelet agentsACEIs/ARBsCoronary revascularization (PCI or
CABG)ttenuate progressive pathologicLV remodeling
ACEIs/ARBs�-blockersAldosterone antagonistsCRT
rolong survival by preventingSCD or progression of HF
�-blockersICDCRTLVAD
CEIs � angiotensin-converting enzyme inhibitors; ARBs � angiotensineceptor blockers; CABG � coronary artery bypass graft; CAD � coro-ary artery disease; CRT � cardiac resynchronization therapy; HF � heartailure; ICD � implantable cardioverter defibrillator; LV � left ventricu-ar; LVAD � left ventricular assist device; PCI � percutaneous coronaryntervention; SCD � sudden cardiac death.
he following industry relationships.

t
acMB
tO
f
tHCs
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
11GFlaherty et al/Assessment and Key Targets for Therapy in the Post-MI Patient with LV Dysfunction
James D. Flaherty, MD, has no financial relationshipso disclose.
James E. Udelson, MD, has served as a member of thedvisory committee for GlaxoSmithKline and Otsuka, re-eived grant/research support from GlaxoSmithKline andolecular Insight, and served as a member of the Speakers’ureau for GlaxoSmithKline.
Mihai Gheorghiade, MD, has served as a member ofhe advisory committee for GlaxoSmithKline, Medtronic,tsuka, PDL, and Sigma Tau.Edwin Wu, MD, has received grant/research support
rom Mallinckrodt.Charles J. Davidson, MD, has served as a member of
he advisory committee for Boston Scientific and GEealthcare; received grant/research support from Abbott,ordis, and GE Healthcare; and served as a member of the
peakers’ bureau for GE Healthcare.
1. Fuster V, Lewis A. Conner Memorial Lecture. Mechanisms leading tomyocardial infarction: insights from studies of vascular biology. Cir-culation 1994;90:2126–2142.
2. Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, HandM, Hochman JS, Krumholz HM, Kushner FG, Lamas GA, et al, for theAmerican College of Cardiology, American Heart Association, Cana-dian Cardiovascular Society. ACC/AHA guidelines for the manage-ment of patients with ST-elevation myocardial infarction—executivesummary: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Writing Com-mittee to revise the 1999 guidelines for the management of patientswith acute myocardial infarction). J Am Coll Cardiol 2004;44:671–719.
3. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, CaseyDE Jr, Chavey WE II, Fesmire FM, Hochman JS, Levin TN, et al.ACC/AHA 2007 guidelines for the management of patients with un-stable angina/non-ST-elevation myocardial infarction—executivesummary: a report of the American College of Cardiology/AmericanHeart Association Task Force on Practice Guidelines (Writing Com-mittee to revise the 2002 guidelines for the management of patientswith unstable angina/non-ST-elevation myocardial infarction). Circu-lation 2007;116:803–877.
4. Achenbach S. Computed tomography coronary angiography. J AmColl Cardiol 2006;48:1919–1928.
5. Stecker EC, Vickers C, Waltz J, Socoteanu C, John BT, Mariani R,McAnulty JH, Gunson K, Jui J, Chugh SS. Population-based analysisof sudden cardiac death with and without left ventricular systolicdysfunction: two-year findings from the Oregon Sudden UnexpectedDeath Study. J Am Coll Cardiol 2006;47:1161–1166.
6. Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death:structure, function, and time-dependence of risk. Circulation 1992;85(suppl):I2–I10.
7. White HD, Norris RM, Brown MA, Brandt PW, Whitlock RM, WildCJ. Left ventricular end-systolic volume as the major determinant ofsurvival after recovery from myocardial infarction. Circulation 1987;76:44–51.
8. GUSTO Angiographic Investigators. The effects of tissue plasminogenactivator, streptokinase, or both on coronary-artery patency, ventricu-lar function, and survival after acute myocardial infarction. N EnglJ Med 1993;329:1615–1622.
9. Bolognese L, Neskovic AN, Parodi G, Cerisano G, Buonamici P,Santoro GM, Antoniucci D. Left ventricular remodeling after primarycoronary angioplasty: patterns of left ventricular dilation and long-
term prognostic implications. Circulation 2002;106:2351–2357.0. Erne P, Schoenenberger AW, Burckhardt D, Zuber M, Kiowski W,Buser PT, Dubach P, Resink TJ, Pfisterer M. Effects of percutaneouscoronary interventions in silent ischemia after myocardial infarction:the SWISSI II randomized controlled trial. JAMA 2007;297:1985–1991.
1. Bonow RO. Identification of viable myocardium. Circulation 1996;94:2674–2680.
2. Allman KC, Shaw LJ, Hachamovitch R, Udelson JE. Myocardialviability testing and impact of revascularization on prognosis in pa-tients with coronary artery disease and left ventricular dysfunction: ameta-analysis. J Am Coll Cardiol 2002;39:1151–1158.
3. Tsuyuki RT, Shrive FM, Galbraith D, Knudtston ML, Graham MM.Revascularization in patients with heart failure. CMAJ 2006;175:361–373.
4. Kim RJ, Fieno DS, Parrish TB, Harris K, Chen EL, Simonetti O,Bundy J, Finn JP, Klocke FJ, Judd RM. Relationship of MRI delayedcontrast enhancement to irreversible injury, infarct age, and contractilefunction. Circulation 1999;100:1992–2002.
5. Simonetti OP, Kim RJ, Fieno DS, Hillenbrand HB, Wu E, Bundy JM,Finn JP, Judd RM. An improved MR imaging technique for thevisualization of myocardial infarction. Radiology 2001;218:215–223.
6. Kim RJ, Wu E, Rafael A, Chen EL, Parker MA, Simonetti O, KlockeFJ, Bonow RO, Judd RM. The use of contrast-enhanced magneticresonance imaging to identify reversible myocardial dysfunction.N Engl J Med 2000;343:1445–1453.
7. Choi KM, Kim RJ, Gubernikoff G, Vargas JD, Parker M, Judd RM.Transmural extent of acute myocardial infarction predicts long-term improvement in contractile function. Circulation 2001;104:1101–1107.
8. Bello D, Shah DJ, Farah GM, Di Luzio S, Parker M, Johnson MR,Cotts WG, Klocke FJ, Bonow RO, Judd RM, Gheorghiade M, Kim RJ.Gadolinium cardiovascular magnetic resonance predicts reversiblemyocardial dysfunction and remodeling in patients with heart failureundergoing beta-blocker therapy. Circulation 2003;108:1945–1953.
9. Ito H, Tomooka T, Sakai N, Yu H, Higashino Y, Fujii K, MasuyamaT, Kitabatake A, Minamino T. Lack of myocardial perfusion imme-diately after successful thrombolysis: a predictor of poor recovery ofleft ventricular function in anterior myocardial infarction. Circulation1992;85:1699–1705.
0. Ito H, Maruyama A, Iwakura K, Takiuchi S, Masuyama T, Hori M,Higashino Y, Fujii K, Minamino T. Clinical implications of the ‘noreflow’ phenomenon: a predictor of complications and left ventricularremodeling in reperfused anterior wall myocardial infarction. Circu-lation 1996;93:223–228.
1. Wu KC, Zerhouni EA, Judd RM, Lugo-Olivieri CH, Barouch LA,Schulman SP, Blumenthal RS, Lima JA. Prognostic significance ofmicrovascular obstruction by magnetic resonance imaging in patientswith acute myocardial infarction. Circulation 1998;97:765–772.
2. Maggioni AP, Zuanetti G, Franzosi MG, Rovelli F, Santoro E, Stasze-wsky L, Tavazzi L, Tognoni G. Prevalence and prognostic significanceof ventricular arrhythmias after acute myocardial infarction in thefibrinolytic era: GISSI-2 results. Circulation 1993;87:312–322.
3. Moss AJ, Hall WJ, Cannom DS, Daubert JP, Higgins SL, Klein H,Levine JH, Saksena S, Waldo AL, Wilber D, Brown MW, Heo M, forthe Multicenter Automatic Defibrillator Implantation Trial Investiga-tors. Improved survival with an implanted defibrillator in patients withcoronary disease at high risk for ventricular arrhythmia. N Engl J Med1996;335:1933–1940.
4. Buxton AE, Lee KL, Fisher JD, Josephson ME, Prystowsky EN,Hafley G, for the Multicenter Unsustained Tachycardia Trial Investi-gators. A randomized study of the prevention of sudden death inpatients with coronary artery disease. N Engl J Med 1999;341:1882–1890.
5. Huikuri HV, Makikallio TH, Raatikainen MJ, Perkiomaki J, Castella-nos A, Myerburg RJ. Prediction of sudden cardiac death: appraisal ofthe studies and methods assessing the risk of sudden arrhythmic death.
Circulation 2003;108:110–115.
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
12G The American Journal of Cardiology (www.AJConline.org) Vol 102 (5A) September 8, 2008
6. Hathaway WR, Peterson ED, Wagner GS, Granger CB, Zabel KM,Pieper KS, Clark KA, Woodlief LH, Califf RM, for the GUSTO-IInvestigators. Prognostic significance of the initial electrocardiogramin patients with acute myocardial infarction. JAMA 1998;279:387–391.
7. Siltanen P, Pohjola-Sintonen S, Haapakoski J, Makijarvi M, Pajari R.The mortality predictive power of discharge electrocardiogram afterfirst acute myocardial infarction. Am Heart J 1985;109:1231–1237.
8. Buxton AE, Sweeney MO, Wathen MS, Josephson ME, Otterness MF,Hogan-Miller E, Stark AJ, Degroot PJ, for the PainFREE Rx IIInvestigators. QRS duration does not predict occurrence of ventriculartachyarrhythmias in patients with implanted cardioverter-defibrillators.J Am Coll Cardiol 2005;46:310–316.
9. Cleland JG, Daubert JC, Erdmann E, Freemantle N, Gras D, Kappen-berger L, Tavazzi L, for the Cardiac Resynchronization-Heart Failure(CARE-HF) Study Investigators. The effect of cardiac resynchroniza-tion on morbidity and mortality in heart failure. N Engl J Med 2005;352:1539–1549.
0. Perkiomaki JS, Huikuri HV, Koistinen JM, Makikallio T, CastellanosA, Myerburg RJ. Heart rate variability and dispersion of QT interval inpatients with vulnerability to ventricular tachycardia and ventricularfibrillation after previous myocardial infarction. J Am Coll Cardiol1997;30:1331–1338.
1. Glancy JM, Garratt CJ, Woods KL, de Bono DP. QT dispersion andmortality after myocardial infarction. Lancet 1995;345:945–948.
2. Zabel M, Klingenheben T, Franz MR, Hohnloser SH. Assessment ofQT dispersion for prediction of mortality or arrhythmic events aftermyocardial infarction: results of a prospective, long-term follow-upstudy. Circulation 1998;97:2543–2550.
3. Statters DJ, Malik M, Ward DE, Camm AJ. QT dispersion: problemsof methodology and clinical significance. J Cardiovasc Electrophysiol1994;5:672–685.
4. Hohnloser SH, Klingenheben T, Li YG, Zabel M, Peetermans J, CohenRJ. T wave alternans as a predictor of recurrent ventricular tachyar-rhythmias in ICD recipients: prospective comparison with conven-tional risk markers. J Cardiovasc Electrophysiol 1998;9:1258–1268.
5. Bloomfield DM, Bigger JT, Steinman RC, Namerow PB, Parides MK,Curtis AB, Kaufman ES, Davidenko JM, Shinn TS, Fontaine JM.Microvolt T-wave alternans and the risk of death or sustained ventric-ular arrhythmias in patients with left ventricular dysfunction. J AmColl Cardiol 2006;47:456–463.
6. Tapanainen JM, Still AM, Airaksinen KE, Huikuri HV. Prognosticsignificance of risk stratifiers of mortality, including T wave alternans,after acute myocardial infarction: results of a prospective follow-upstudy. J Cardiovasc Electrophysiol 2001;12:645–652.
7. Gomes JA, Cain ME, Buxton AE, Josephson ME, Lee KL, Hafley GE.Prediction of long-term outcomes by signal-averaged electrocardiog-raphy in patients with unsustained ventricular tachycardia, coronaryartery disease, and left ventricular dysfunction. Circulation 2001;104:436–441.
8. Bigger JT Jr, for the Coronary Artery Bypass Graft (CABG) PatchTrial Investigators. Prophylactic use of implanted cardiac defibrillatorsin patients at high risk for ventricular arrhythmias after coronary-artery
bypass graft surgery. N Engl J Med 1997;337:1569–1575.9. el-Sherif N, Denes P, Katz R, Capone R, Mitchell LB, Carlson M,Reynolds-Haertle R, for the Cardiac Arrhythmia Suppression Trial/Signal-Averaged Electrocardiogram (CAST/SAECG) Substudy Inves-tigators. Definition of the best prediction criteria of the time domainsignal-averaged electrocardiogram for serious arrhythmic events in thepostinfarction period. J Am Coll Cardiol 1995;25:908–914.
0. Schrier RW, Abraham WT. Hormones and hemodynamics in heartfailure. N Engl J Med 1999;341:577–585.
1. Mann DL, Kent RL, Parsons B, Cooper G IV. Adrenergic effects onthe biology of the adult mammalian cardiocyte. Circulation 1992;85:790–804.
2. Goodfriend TL, Elliott ME, Catt KJ. Angiotensin receptors and theirantagonists. N Engl J Med 1996;334:1649–1654.
3. Jessup M, Brozena S. Heart failure. N Engl J Med 2003;348:2007–2018.
4. Malmberg K, Norhammar A, Wedel H, Ryden L. Glycometabolicstate at admission: important risk marker of mortality in conven-tionally treated patients with diabetes mellitus and acute myocar-dial infarction: long-term results from the Diabetes and Insulin-Glucose Infusion in Acute Myocardial Infarction (DIGAMI) study.Circulation 1999;99:2626 –2632.
5. Ward KD, Sparrow D, Landsberg L, Young JB, Vokonas PS, WeissST. The relationship of epinephrine excretion to serum lipid levels: theNormative Aging Study. Metabolism 1994;43:509–513.
6. Reaven GM, Lithell H, Landsberg L. Hypertension and associatedmetabolic abnormalities: the role of insulin resistance and the sympa-thoadrenal system. N Engl J Med 1996;334:374–381.
7. Prasad A, Quyyumi AA. Renin-angiotensin system and angiotensinreceptor blockers in the metabolic syndrome. Circulation 2004;110:1507–1512.
8. Pekkanen J, Linn S, Heiss G, Suchindran CM, Leon A, Rifkind BM,Tyroler HA. Ten-year mortality from cardiovascular disease in relationto cholesterol level among men with and without preexisting cardio-vascular disease. N Engl J Med 1990;322:1700–1707.
9. Rosengren A, Hagman M, Wedel H, Wilhelmsen L. Serum cholesteroland long-term prognosis in middle-aged men with myocardial infarc-tion and angina pectoris: a 16-year follow-up of the Primary Preven-tion Study in Göteborg, Sweden. Eur Heart J 1997;18:754–761.
0. Richards AM, Nicholls MG, Troughton RW, Lainchbury JG, Elliott J,Frampton C, Espiner EA, Crozier IG, Yandle TG, Turner J. Anteced-ent hypertension and heart failure after myocardial infarction. J AmColl Cardiol 2002;39:1182–1188.
1. Abraham WT, Greenberg BH, Yancy CW. Pharmacologic therapiesacross the continuum of left ventricular function. Am J Cardiol 2008;(suppl 102):21G–28G.
2. Kadish AH, Reiffel JA, Naccarelli GV, DiMarco JP. Device therapiesin the post-myocardial infarction patient with left ventricular dysfunc-tion. Am J Cardiol 2008;(suppl 102):29G–37G.
3. Flaherty JD, Davidson CJ, Faxon DP. Percutaneous coronary inter-vention for myocardial infarction with left ventricular dysfunction.Am J Cardiol 2008;(suppl 102):38G–41G.
4. McCarthy PM. Surgical therapies for post-myocardial infarction pa-
tients. Am J Cardiol 2008;(suppl 102):42G–46G.