Embed Size (px)
Citation preview

Assessment and Documentation

Head to Toe AssessmentThis is done on admission
On units every 12 hours; ICU every 4 hours
It takes 5-10 minutes.
It is done by systems
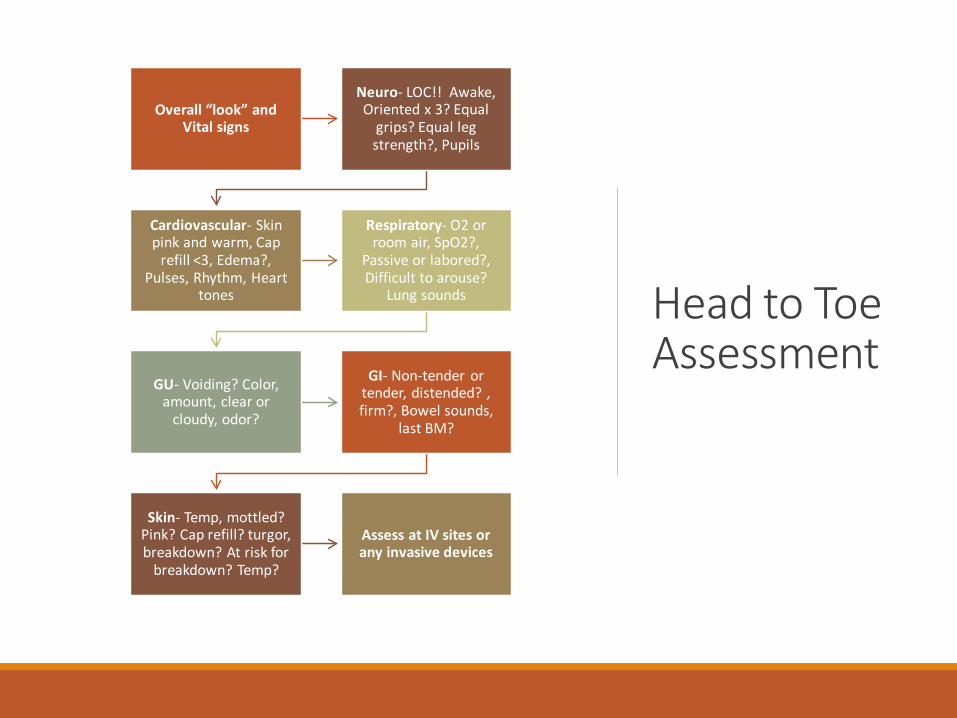
Head to Toe Assessment
Overall “look” and Vital signs
Neuro- LOC!! Awake, Oriented x 3? Equal
grips? Equal leg strength?, Pupils
Cardiovascular- Skin pink and warm, Cap
refill <3, Edema?, Pulses, Rhythm, Heart
tones
Respiratory- O2 or room air, SpO2?,
Passive or labored?, Difficult to arouse?
Lung sounds
GU- Voiding? Color, amount, clear or
cloudy, odor?
GI- Non-tender or tender, distended? , firm?, Bowel sounds,
last BM?
Skin- Temp, mottled? Pink? Cap refill? turgor, breakdown? At risk for
breakdown? Temp?
Assess at IV sites or any invasive devices

Be aware of these during assessment and document your findings
Change of status from last assessment or report is very important to document
When a new symptom emerges
• Use the patient’s own words or non-verbal cues and your observations
Patient distress
Any action taken in response to a problem (SBAR)
Critical Lab values- use the critical value note in Cerner (ADHOC) • Critical values must be called and documented
within 30 minutes

The Heart of the Matter
Where the stethoscope is placed.
Lung Assessment
◦ Clear lung sounds◦ Absent or decreased sounds –
reduced airflow or consolidation, fluid (pneumothorax, pneumonia, effusions)
◦ Wheezing – upper airways narrowed, usually expiration (Asthma)
◦ Crackles or Rales – usually inspiration fine or coarse (fluid in alveoli, atelectasis)

Lung Assessment
◦ Rhonchi – characterized by a low-pitched sounds
◦ Stridor – a high-pitched, almost whistling, sound
◦ Pleural Friction Rub – occurs when the lung is actually rubbing against the ribs

NIH STROKE SCALE
It is for all Stroke patients on admission and prior to discharge.
If the patient receives tPA, the Stroke scale is completed every 2 hours for 24 hours.

NIH STROKE SCALE (continued)

SKIN ASSESSMENT◦ SKIN ISSUES: POA ◦ Look everywhere!!! ◦ Complete admission
assessment and be sure to follow up in I-view and notes prn
◦ Complete every shift as well
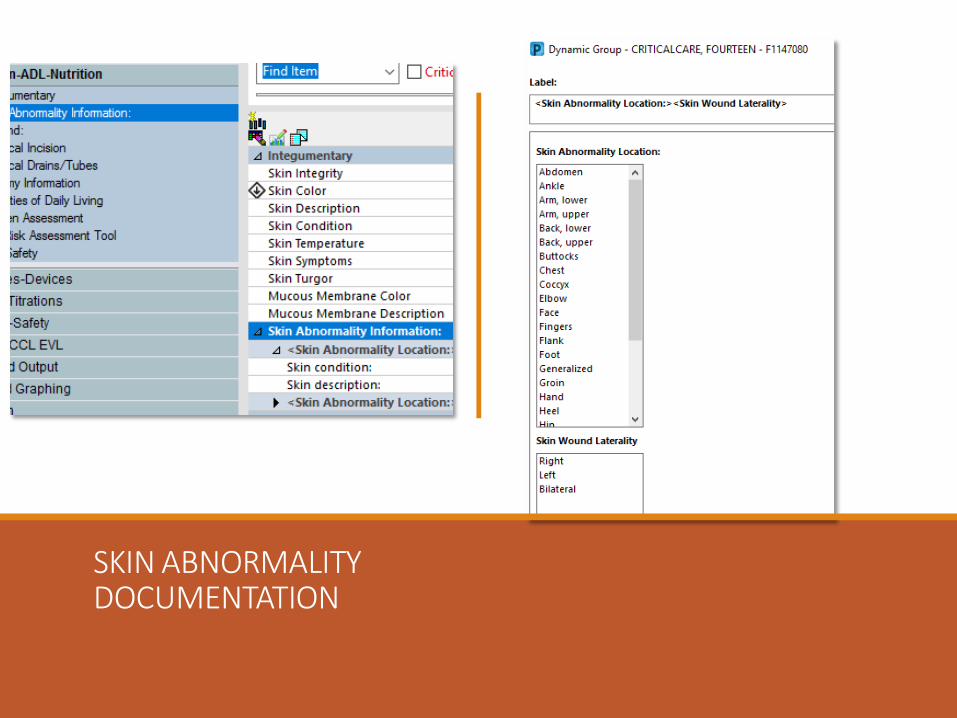
SKIN ABNORMALITYDOCUMENTATION

WOUNDS
Note: you can also document a surgical incision.

PAIN ASSESSMENT• Pain is assessed on admission.
• If pain is identified on initial screening, a more detailed assessment of pain will be performed.
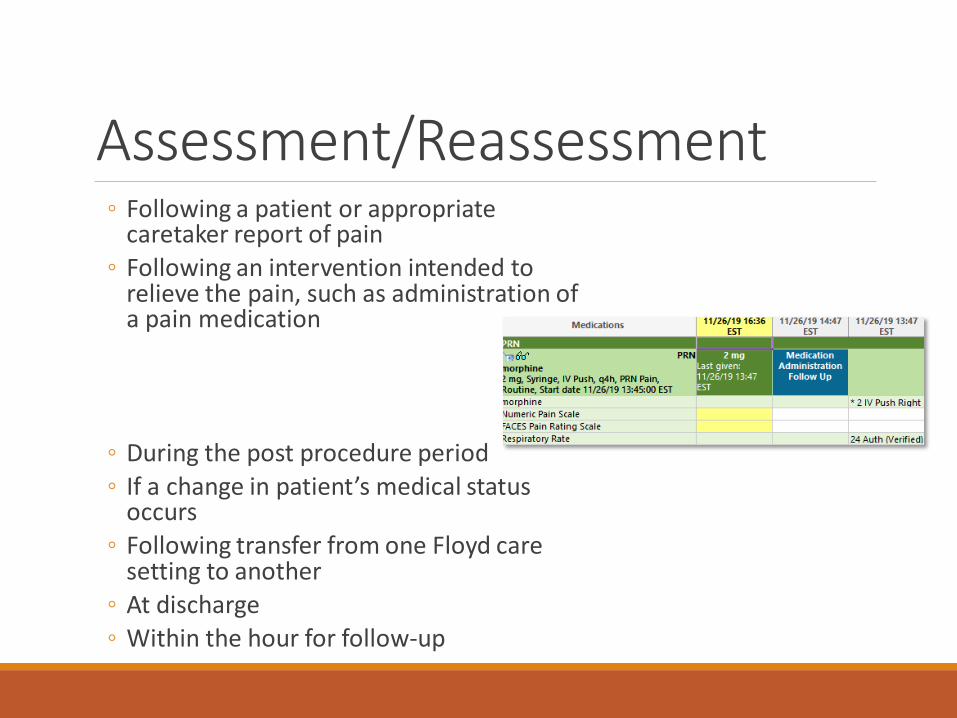
Assessment/Reassessment◦ Following a patient or appropriate
caretaker report of pain◦ Following an intervention intended to
relieve the pain, such as administration of a pain medication
◦ During the post procedure period◦ If a change in patient’s medical status
occurs◦ Following transfer from one Floyd care
setting to another◦ At discharge ◦ Within the hour for follow-up

Scales: Numeric, Faces, FLACC, CPOT
Numeric: 1-10 is most common
FACES: children over 3 (0 = smiling happy face, 10 = crying)
FLACC: children 2 months +, or patients unable to communicate pain
CPOT: used in critical care, includes compliance with the ventilator

Non-Pharmacological Interventions for Adult Patients
Physical Interventions
• Positioning• Massage• Heat/cold• Immobilization
Cognitive Behavior Interventions• Distraction/relaxation• Guided imagery• Patient education
Abbreviations
FLOYD has established uniform definitions for commonly utilized acceptable abbreviations and symbols.
The Pharmacy and Therapeutics committee maintains a current list of abbreviations that have been shown to compromise patient safety based on hospital and national experience.
When an unacceptable abbreviation is used, the Pharmacist or Nurse will verify the prescription order with the ordering physician.
Once an unacceptable abbreviation order is verified, a verbal order clarification will be placed.
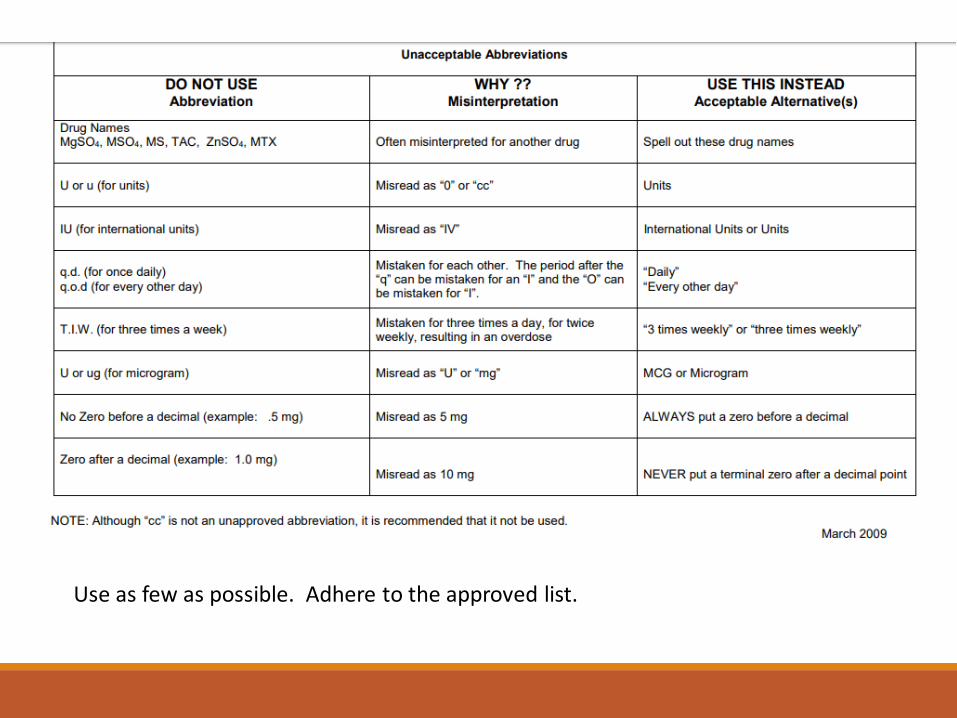
Unacceptable Abbreviations
Use as few as possible. Adhere to the approved list.
Documentation…has a History•Florence Nightingale is considered the founder of nursing documentation
• Her guidelines: Be CLEAR, CONCISE, and ORGANIZED
•The main purpose of traditional documentation was to record whether the physician’s orders were followed and policies observed

Legal Aspects of Nursing Documentation
• Charting by exception does not allow nurses to paint a true picture of the INVALUABLE care provided to patients.
Charting should:
•Accurately describe the patient’s condition and progress
•Provide communication between staff and multidisciplinary teams
•Defend the nurse legally, if necessary

Documentation Guidelines
NEVER leave gaps
NEVER document before a procedure is done or a medication is administered
ALWAYS document any condition present on admission
ALWAYS document significant changes in patient condition
Be objective and ONLY report facts….
NEVER chart subjective thoughts or comments or bias

Documentation Guidelines When in doubt… document!
Be consistent with other providers
Document unusual events or occurrences.
DO NOT CHART “SEE INCIDENT REPORT”
Do not chart “approximate time” documentation
Late entries need to be labeled as such
Documentation should be clear, concise, and specific
Use ONLY approved abbreviations!

Examples of what to chart
Oncoming/off going shift report and
assessment
Admission/receiving, document time arrival
Leaving/returning to the floor, document time of discharge or
return to floor
Bedside procedures Initiation of blood products
Communication with healthcare providers
Patient noncompliance with
plan of care/treatment
Discharge- document time of discharge, discharge location,
and mode of transport

/
Modern day technology guidelines
Don’t use your cell phone to send patient information via text
01Do not take pictures
02Do not be on Facebook on when “on stage”
03Do not access any patient’s chart that you are not involved in the patient care and need to do your job
04

Decreasing Legal Risk
Provide the highest standard of careProvide
Document very well. Be objectiveDocument
Know your medicationsKnow
Know your policies/procedures- if you’re unsure, ask for helpKnow
Continuously assess your patient- call the physician, if neededAssess
Utilize Risk ManagementUtilize

Assessment and Documentation





























