Lower Limb Coordination in Early Stance Following Multiple
Ligament Knee Reconstruction
Assessing the Outcome of Multiple-ligament Knee Reconstruction
Using Gait Analysis1Corey Scholes PhD, 1Brett Fritsch FRACS1, Joe
Lynch MSc, 1,2Jack Batchen Beng, 1Milad Ebrahimi BEng, 1Myles
Coolican FRACS, 3Richard Smith PhD, 1David Parker FRACS
1Sydney Orthopaedic Research Institute, Chatswood, NSW2School of
Aerospace, Mechanical and Mechatronic Engineering, University of
Sydney3Faculty of Health Sciences, University of Sydney
Sydney Orthopaedic Research InstituteDr Joe Costa (FRCSC),
Laurant Kang, Amy Brierley BEngStudy participants
University of SydneyRay Patton (Biomechanics Laboratory)
FundingRoyal Australasian College of Surgeons Brendan
Dooley-Gordon Trinca Trauma ScholarshipFriends of Mater Hospital
FoundationAcknowledgements
None of the authors have received any payment or consideration
from any source for the conduct of this study.
Sydney Orthopaedic Research Institute has received
fellowship/study funding from;Smith & Nephew;Global
OrthopaedicArthritis AustraliaRoyal Australasian College of
SurgeonsFriends of Mater Hospital FoundationDeclaration of
Interest
IntroductionAt least 2 of 4 major ligaments torn
Usually high velocity trauma
Associated injuries commonReduced long-term joint function
IntroductionLimited information on functional outcomeCan
reconstruction restore normal kinematics?Altered
kinematicsIncreased joint loadingIncreased risk of OAWeight
Acceptance (Ratcliffe et al 1997, Whittle et al 1999)Knee angle
determines load distribution Peak forcesRelated to shock
attenuation
Database (N = 163); Invited (N = 30); Agreed (N = 16)
Controls matched within 10% age, weight, heightPatient
SampleMLKRControlP-valueAge at F/U (yrs)43.2 + 13.541.5 +
14.50.68Height (cm)172.1 + 11.1174.7 + 10.30.47Weight (kg)78.0 +
16.776.8 + 14.70.79BMI26.1 + 3.824.95 + 2.70.38Ave F/U
(yrs)4.7+3.5-
(0-20%)
6Injury PatternsLigamentClassificationMeniscal
TreatmentAssociated Injuries1ACL/PLCCLPMMx2ACL/MCL/PARTIAL
PCLBMPelvic Fracture3ACL/PCL/MCLBM4PCL/MCLCM5PCL/LCL/PLCCL-Open
Patella Fracture-Non Displaced Lateral Femoral Condyle-Fracture
Right Ankle6ACL/PCL/MCLCM-Tibial Plateau
Fracture7ACL/MCLCM8PCL/LCL/PLCBL-Fracture Base Of
Skull9ACL/PCL/LCL/PLCBLMMR10PCL/PLCCL11ACL/LCL/PLCCM-CPN Injury
With Foot Drop12ACL/PCL/MCL/PMCBM-No Distal Pulse at
Operation13ACL/PCL/MCL/PMCBMPLMx14ACL/MCLCM15ACL/PCL/LCL/PLCBL16ACL/PCL/MCLBMPLMxDemographic
dataAgeGenderSurgery-followup time
Injury dataLigament patternB/CL/M
Outcome dataPassive flexion contractureKT1000 (194N;
max)KOOSIKDC
Clinical follow-up
Conducted at the Biomechanics Laboratory, University of
Sydney
3D Motion Capture14x Infrared strobing cameras37 reflective
markers
Overground walking at self-selected speed
Step descent and turn @90deg
Motion Capture
Discrete Angles and Range of motion3-dimensional angles at0% of
stance (foot strike)60% of stance (begin Propulsion)
3-dimensional range of motion0-20% of stance (Weight
Acceptance)60-85% of stance (Propulsion)
Vertical ground reaction force10Methods - Spatiotemporal
VariablesDefinitionVelocity (m/s)Stride length / Stride
timeCadence (steps/min) Step count / time in minutesStep Length
(m)Distance between the proximal end position of the foot at
ipsilateral heel strike to the proximal end position of the foot at
the consecutive contralateral heel strikeStep Width (m)Distance
between the ipsilateral heel strike to the proximal end position of
the foot at the next contralateral heel strikeSingle Support time
(%)Time between toe-off and heel strike of the contralateral
limbInitial Double Support time (%)Time between heel strike of the
ipsilateral limb and toe off of the contralateral limbDouble
Support time (%)Sum of initial double support times for the left
and right limbsStance time (%)Time between heel strike and toe off
of the ipsilateral limbNormality and equality of variance
checks
GroupPaired t-tests, Kruskal-Wallis ANOVA (Dunn-Sidak post-hoc
comparisons) performed where appropriate
Single subject pair matched comparisonsProportion (%) of
patients with sig difference to matched control for each
measure
Statistical analysisAre differences in knee kinematics and
spatiotemporal characteristics related to clinical symptoms
?PredictorsAgeGenderSurgery-followup delayLigament
patternB/CL/MPassive flexion contractureKT1000 (194N;
max)KOOSIKDC
Output variablesVelocityStep lengthStep widthCadenceStance
durationDouble/single support durationInitial double support
durationPartial Least Squares Regression
A regression analysis to look for strength of association
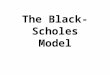
between factors13Mean (+95%CI) for MLKI patient responses to IKDC
questionnaire and KOOS subscales with solid line denoting mean for
healthy controls. Clinical Results
Results - Subjective Scores
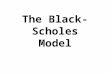
Group comparisons -walkingSignificantly internal tibial rotation
during propulsion between reconstructed and control knees
Group comparisons - Spatiotemporal Mean+95%CI
P-ValueMLKIControlVelocity (m/s)1.49+0.061.59+0.060.04Step
Length (m)0.73+0.020.78+0.02