Embed Size (px)
Citation preview
Assessing Mothers' Attitudes aboutthe Physician's Role inChild Health PromotionTina L. Cheng MD, MPH, Judith A. Savageau, MPH, Carol Bigelow, PhD,Evan Chamey, MD, Sanjaya Kumar, MD, MPH, and Thomas G. DeWitt, MD
IntroductionTradition and training have led physi-
cians and parents to believe that childhealth supervision (well-child care) isimportant and efficacious. A large num-ber and variety of health promotion topicshave been suggested for discussion inwell-child visits. Some issues, such ascounseling on car seats, have been studiedand associated with positive changes inbehavior leading to decreased morbidityand mortality. The effectiveness of manycomponents of well-child care, however,has not been conclusively demonstrated,particularly in the areas of health educa-tion, counseling, and anticipatory guid-ance.1-3 One key to the study of meaning-ful outcomes is to identify what parentsperceive as important. Current guidelines,including the recent Bright Futures4 re-port, have been developed largely fromthe consensus of physicians. The per-ceived effectiveness of well-child carefrom the perspective of the consumer canprovide important insight into the needsof parents.
This investigation examines parents'attitudes regarding 15 health issues fordiscussion in well-child care within theframework of the Health Belief Model.This model has been utilized to explain,predict, and influence health behavior. Ithypothesizes that health attitudes andaction are dependent on three factors: (1)existence of sufficient concern abouthealth to make the issue salient, (2) beliefthat one is susceptible to the healthproblem, and (3) belief that a particularhealth recommendation would be benefi-cial in reducing the susceptibility.5 Describ-ing parental views in the context of thismodel affords a deeper understanding ofexpectations and avenues for more effec-tive health promotion.
MethodsStudy participants were drawn from
a health maintenance organization activein health promotion in central Massachu-setts. Eligible mothers had a child be-
tween 24 and 36 months, had beenenrolled with one of the five pediatriciansfor at least 1 year, and gave informedconsent. A letter was sent to a randomsample inviting them to participate, and anonphysician interviewer arranged a homeinterview. The study was approved by theInstitutional Review Boards at the Univer-sity of Massachusetts Medical Center andFallon Community Health Plan.
The 45-minute interview examinedperceptions of the physician's role in 15health promotion topics. Twenty-eightmothers were reinterviewed 1 to 4 monthslater for reliability testing. For individualquestions with a 4- to 7-point Likert scaleor ranking, the percentage agreementbetween the two interviews (t 1 Likertpoint) was 50% to 100% (mean 81%agreement for 84 questions).
Mothers were asked about the impor-tance of discussion of 15 topics in wellcare during the first 3 years. The topicswere chosen from the American Academyof Pediatrics' Guidelines for Health Super-vision6 and from recent pediatric litera-ture. For each of the topics, four healthbelief model predictor questions wereadapted from Wheeler and Rundall7: (1)"How likely do you think it is that childrenmight get or have the following problem?"(2) "How much of an effect do you think itwould have on a child and a family's life ifthe child had one of the following prob-lems?" (3) "How much do you think adoctor or nurse can do to prevent thefollowing problem?" (4) "How much do
Tina L. Cheng is with the Department ofGeneral Pediatrics, George Washington Uni-versity, and Children's National Medical Cen-ter, Washington, DC. At the time of the study,Dr Cheng, Judith A. Savageau, Evan Charney,and Thomas G. DeWitt were with the Depart-ment of Pediatrics, University of MassachusettsMedical Center, Worcester. Carol Bigelow andSanjaya Kumar were with the Department ofBiostatistics and Epidemiology, University ofMassachusetts School of Public Health, Am-herst.
Requests for reprints should be sent toTina L. Cheng, MD, MPH, Children's NationalMedical Center, 111 Michigan Ave, NW,Washington, DC 20010.
This paper was accepted April 23, 1996.
American Journal of Public Health 1809
Public Health Briefs
you think a doctor or nurse can do to help Belief Mlparents and children that have the follow- variablesing problem?" scale; be
Characteristics of the sample were were logasummarized using descriptive statistics.Multivariable analyses were performed Resultwith the importance of discussion of thetopic in well care as the dependent Of tlvariable. Hypothesis testing focused on contactedthe predictive significance of four Health and 72 i
lodel constructs. All dependentwere measured on a Likertcause of skewness, responsesrithmically transformed.
analyzed by provider, family size, maritalstatus, race, and insurance status. Refus-ers were more likely to be single or
divorced parents compared with partici-pants (P = .006).
All mothers had a child between 2and 3 years, and 79% had more than one
child, with an average of 2.2 children(range 1 to 6). Of the mothers, 99% were
Caucasian; 92% were married; 34% had a
high school education or less; 42% hadsome college or vocational school, and25% had completed college. Ninety-ninepercent rated their child's health status as
good to excellent; 29% smoked, and 28%were not regular users of seat belts.
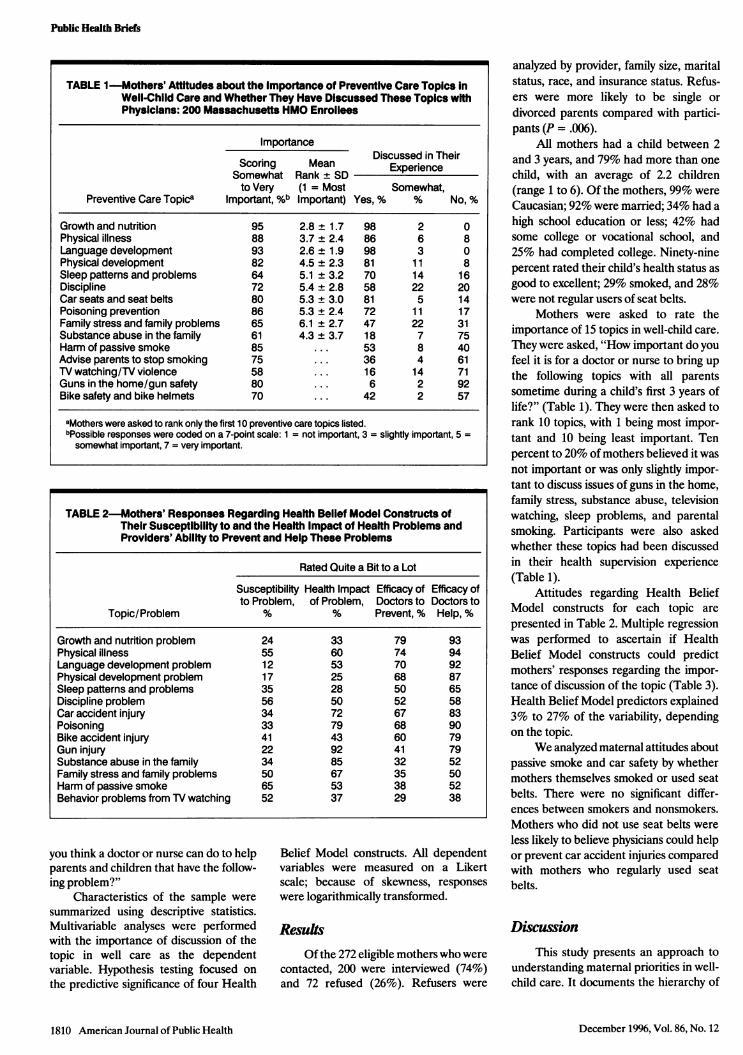
Mothers were asked to rate theimportance of 15 topics in well-child care.
They were asked, "How important do youfeel it is for a doctor or nurse to bring upthe following topics with all parentssometime during a child's first 3 years oflife?" (Table 1). They were then asked torank 10 topics, with 1 being most impor-tant and 10 being least important. Tenpercent to 20% of mothers believed it wasnot important or was only slightly impor-tant to discuss issues of guns in the home,family stress, substance abuse, televisionwatching, sleep problems, and parentalsmoking. Participants were also askedwhether these topics had been discussedin their health supervision experience(Table 1).
Attitudes regarding Health BeliefModel constructs for each topic are
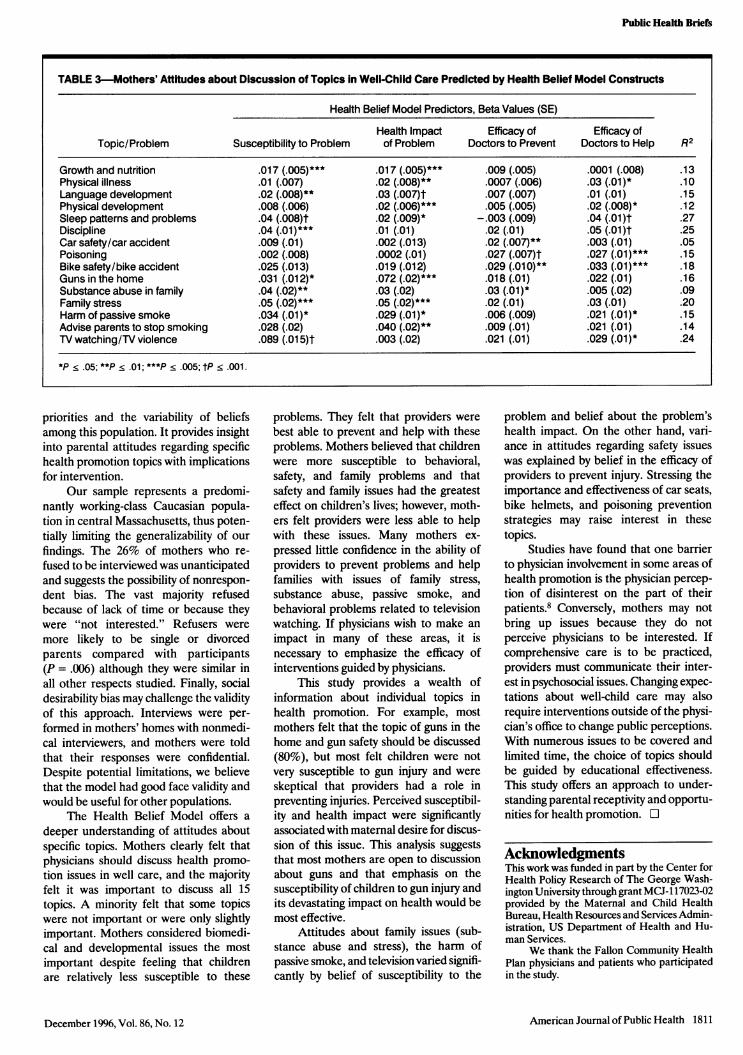
presented in Table 2. Multiple regressionwas performed to ascertain if HealthBelief Model constructs could predictmothers' responses regarding the impor-tance of discussion of the topic (Table 3).Health Belief Model predictors explained3% to 27% of the variability, dependingon the topic.
We analyzed maternal attitudes aboutpassive smoke and car safety by whethermothers themselves smoked or used seatbelts. There were no significant differ-ences between smokers and nonsmokers.Mothers who did not use seat belts wereless likely to believe physicians could helpor prevent car accident injuries comparedwith mothers who regularly used seatbelts.
Discussion
he 272 eligible mothers who were1, 200 were interviewed (74%)refused (26%). Refusers were
This study presents an approach tounderstanding maternal priorities in well-child care. It documents the hierarchy of
1810 American Journal of Public Health
TABLE 1-Mothers' Attitudes about the Importance of Preventive Care Topics InWell-Child Care and Whether They Have Discussed These Topics withPhysicians: 200 Massachusetts HMO Enrollees
Importance
Scoring MeanDiscussed in Their
Somewhat Rank ± SD Experienceto Very (1 = Most Somewhat,
Preventive Care Topica Important, %b Important) Yes, % % No, %
Growth and nutrition 95 2.8 ± 1.7 98 2 0Physical illness 88 3.7 ± 2.4 86 6 8Language development 93 2.6 ± 1.9 98 3 0Physical development 82 4.5 ± 2.3 81 11 8Sleep patterns and problems 64 5.1 ± 3.2 70 14 16Discipline 72 5.4 ± 2.8 58 22 20Car seats and seat belts 80 5.3 ± 3.0 81 5 14Poisoning prevention 86 5.3 ± 2.4 72 11 17Family stress and family problems 65 6.1 ± 2.7 47 22 31Substance abuse in the family 61 4.3 ± 3.7 18 7 75Harm of passive smoke 85 ... 53 8 40Advise parents to stop smoking 75 ... 36 4 61TV watching/TV violence 58 ... 16 14 71Guns in the home/gun safety 80 ... 6 2 92Bike safety and bike helmets 70 ... 42 2 57
aMothers were asked to rank only the first 10 preventive care topics listed.bPossible responses were coded on a 7-point scale: 1 = not important, 3 = slightly important, 5 =somewhat important, 7 = very important.
TABLE 2-Mothers' Responses Regarding Heaith Belief Model Constructs ofTheir Susceptibility to and the Heaith Impact of Health Problems andProviders' Ability to Prevent and Help These Problems
Rated Quite a Bit to a Lot
Susceptibility Heaith Impact Efficacy of Efficacy ofto Problem, of Problem, Doctors to Doctors to
Topic/Problem % % Prevent, % Help, %
Growth and nutrition problem 24 33 79 93Physical illness 55 60 74 94Language development problem 12 53 70 92Physical development problem 17 25 68 87Sleep patterns and problems 35 28 50 65Discipline problem 56 50 52 58Car accident injury 34 72 67 83Poisoning 33 79 68 90Bike accident injury 41 43 60 79Gun injury 22 92 41 79Substance abuse in the family 34 85 32 52Family stress and family problems 50 67 35 50Harm of passive smoke 65 53 38 52Behavior problems from TV watching 52 37 29 38
December 1996, Vol. 86, No. 12
Public Health Briefs
priorities and the variability of beliefsamong this population. It provides insightinto parental attitudes regarding specifichealth promotion topics with implicationsfor intervention.
Our sample represents a predomi-nantly working-class Caucasian popula-tion in central Massachusetts, thus poten-tially limiting the generalizability of our
findings. The 26% of mothers who re-
fused to be interviewed was unanticipatedand suggests the possibility of nonrespon-dent bias. The vast majority refusedbecause of lack of time or because theywere "not interested." Refusers were
more likely to be single or divorcedparents compared with participants(P = .006) although they were similar inall other respects studied. Finally, socialdesirability bias may challenge the validityof this approach. Interviews were per-
formed in mothers' homes with nonmedi-cal interviewers, and mothers were toldthat their responses were confidential.Despite potential limitations, we believethat the model had good face validity andwould be useful for other populations.
The Health Belief Model offers a
deeper understanding of attitudes aboutspecific topics. Mothers clearly felt thatphysicians should discuss health promo-
tion issues in well care, and the majorityfelt it was important to discuss all 15topics. A minority felt that some topicswere not important or were only slightlyimportant. Mothers considered biomedi-cal and developmental issues the mostimportant despite feeling that childrenare relatively less susceptible to these
problems. They felt that providers were
best able to prevent and help with theseproblems. Mothers believed that childrenwere more susceptible to behavioral,safety, and family problems and thatsafety and family issues had the greatesteffect on children's lives; however, moth-ers felt providers were less able to helpwith these issues. Many mothers ex-
pressed little confidence in the ability ofproviders to prevent problems and helpfamilies with issues of family stress,substance abuse, passive smoke, andbehavioral problems related to televisionwatching. If physicians wish to make an
impact in many of these areas, it isnecessary to emphasize the efficacy ofinterventions guided by physicians.
This study provides a wealth ofinformation about individual topics inhealth promotion. For example, mostmothers felt that the topic of guns in thehome and gun safety should be discussed(80%), but most felt children were notvery susceptible to gun injury and were
skeptical that providers had a role inpreventing injuries. Perceived susceptibil-ity and health impact were significantlyassociated with maternal desire for discus-sion of this issue. This analysis suggeststhat most mothers are open to discussionabout guns and that emphasis on thesusceptibility of children to gun injury andits devastating impact on health would bemost effective.
Attitudes about family issues (sub-stance abuse and stress), the harm ofpassive smoke, and television varied signifi-cantly by belief of susceptibility to the
problem and belief about the problem'shealth impact. On the other hand, vari-ance in attitudes regarding safety issueswas explained by belief in the efficacy ofproviders to prevent injury. Stressing theimportance and effectiveness of car seats,bike helmets, and poisoning preventionstrategies may raise interest in thesetopics.
Studies have found that one barrierto physician involvement in some areas ofhealth promotion is the physician percep-
tion of disinterest on the part of theirpatients.8 Conversely, mothers may notbring up issues because they do notperceive physicians to be interested. Ifcomprehensive care is to be practiced,providers must communicate their inter-est in psychosocial issues. Changing expec-tations about well-child care may alsorequire interventions outside of the physi-cian's office to change public perceptions.With numerous issues to be covered andlimited time, the choice of topics shouldbe guided by educational effectiveness.This study offers an approach to under-standing parental receptivity and opportu-nities for health promotion. O
AcknowledgmentsThis work was funded in part by the Center forHealth Policy Research of The George Wash-ington University through grant MCJ-117023-02provided by the Maternal and Child HealthBureau, Health Resources and Services Admin-istration, US Department of Health and Hu-man Services.
We thank the Fallon Community HealthPlan physicians and patients who participatedin the study.
American Journal of Public Health 1811
TABLE 3-Mothers' Attitudes about Discussion of Topics in Well-Child Care Predicted by Health Belief Model Constructs
Health Belief Model Predictors, Beta Values (SE)
Health Impact Efficacy of Efficacy ofTopic/Problem Susceptibility to Problem of Problem Doctors to Prevent Doctors to Help R2
Growth and nutrition .017 (.005)*** .017 (.005)*** .009 (.005) .0001 (.008) .13Physical illness .01 (.007) .02 (.008)** .0007 (.006) .03 (.01)* .10Language development .02 (.008)** .03 (.007)t .007 (.007) .01 (.01) .15Physical development .008 (.006) .02 (.006)*** .005 (.005) .02 (.008)* .12Sleep patterns and problems .04 (.008)t .02 (.009)* -.003 (.009) .04 (.01)t .27Discipline .04 (.01)*** .01 (.01) .02 (.01) .05 (.01)t .25Car safety/car accident .009 (.01) .002 (.013) .02 (.007)** .003 (.01) .05Poisoning .002 (.008) .0002 (.01) .027 (.007)t .027 (.01)*** .15Bike safety/bike accident .025 (.013) .019 (.012) .029 (.010)** .033 (.01)*** .18Guns in the home .031 (.01 2)* .072 (.02)*** .018 (.01) .022 (.01) .16Substance abuse in family .04 (.02)** .03 (.02) .03 (.01)* .005 (.02) .09Family stress .05 (.02)*** .05 (.02)*** .02 (.01) .03 (.01) .20Harm of passive smoke .034 (.01)* .029 (.01)* .006 (.009) .021 (.01)* .15Advise parents to stop smoking .028 (.02) .040 (.02)** .009 (.01) .021 (.01) .14TV watching/TV violence .089 (.015)t .003 (.02) .021 (.01) .029 (.01)* .24
*p < .05; **P < .01; ***P < .005; tP < .001.
December 1996, Vol. 86, No. 12
Public Health Briefs
References1. Healthy Chidren: Investing in the Future.
Washington, DC: Office of TechnologyAssessment; 1988:13-25, 242-255. Publica-tion OTA-H-345.
2. Homer CJ. Evaluation ofthe Evidence on theEffectiveness of Well Child Care Services forChildren. Washington, DC: Office of Tech-nology Assessment; 1988 (July). ContractorDocument, Health Program.
3. Casey P, Sharp M, Loda F. Child-health
supervision for children under two years ofage: a review of its content and effectiveness.Pediatrics. 1979;95:1-9.
4. Green M., ed. Bright Futures: Guidelines forHealth Supewvision of Infants, Children andAdolescents. Arlington, Va: National Centerfor Education in Maternal and Child Health;1994.
5. Rosenstock IM, Strecher VJ, Becker MH.Social learning theoxy and the health beliefmodel. Health Educ Q. 1988;15:175-183.
6. Guidelines for Health Supervision II. ElkGrove Village, Ill: American Academy ofPediatrics, Committee on Psychosocial As-pects of Child and Family Health. 1988.
7. Wheeler JRC, Rundall TG. Secondarypreventive health behavior. Health Educ Q.1980;7:243-262.
8. Hickson GB, Altemeier WA, O'Connor S.Concerns of mothers seeking care in privatepediatric offices: opportunities for expand-ing services. Pediatrics. 1983;72:619-624.
Inappropriately Timed Immunizations:Types, Causes, and Their Relationshipto Record KeepingJulie Shea Hamlin, MPH, David Wood, MD, MPH, Margaret Pereyra, MPH,and Mark Grabowsky, MD, MPH
*g eO: ... .. .....
-2SiM |El
IntroductionFailure to deliver appropriately timed
immunizations was cited as a majorreason for the low immunization ratesthat led to the measles epidemic of 1989through 1991.1 Many urban residents relyon government-operated public healthclinics for early childhood immunizations,and use of these clinics has been associ-ated with low immunization levels.24 AnInstitute of Medicine report has criticizedthe level of performance of public healthclinics, calling for closer scrutiny of thequality of care delivered.5
It is common for public healthcenters to administer immunizations inboth well child clinics and immunization-only clinics that operate independently inthe same health center with separaterecords (G. Koops, National Immuniza-tion Program, oral communication, May1995). This practice can lead to recordkeeping problems and errors (e.g., omis-sions and inappropriately administeredimmunizations) in the administration ofimmunizations. In order to assess theextent to which record keeping practicesmay contribute to inappropriately timedimmunizations and low immunization cov-erage rates, we abstracted and comparedimmunization records at both well childand immunization-only clinics in four LosAngeles County Department of HealthServices public health centers.
MethodsSix hundred two medical records of
children between 25 and 36 months of age
as of June 1, 1992, were randomlysampled from a computerized listing of allactive well child medical records at fourpublic health centers in Los Angeles.Centers for Disease Control and Preven-tion (CDC) chart abstraction guidelines6were used in selecting and abstractingcharts. We physically searched by childname and birth date for correspondingimmunization cards kept in the immuniza-tion-only clinics. Of the 602 children withwell child visits, 211 had also receivedvaccinations in immunization-only clinicsprior to their second birthday.
Immunization histories were recon-structed from both sources for each child.We abstracted the date each immuniza-tion was given, the presence of parent/guardian signature, vaccine lot number,and nurse signature. The following vac-cines were recorded and included in theanalyses: diphtheria, tetanus, and pertus-sis (DTP); oral polio vaccine (OPV); andmeasles, mumps, and rubella (MMR).Haemnophilus influenza type b vaccine andhepatitis B were recorded but not in-cluded in this analysis because they were
At the time of the study, Julie Shea Hamlin,David Wood, and Margaret Pereyra were withthe Ahmanson Department of Pediatrics, Ce-dars-Sinai Medical Center, Los Angeles, Calif.David Wood was also with the RAND Corp,Santa Monica, Calif. Mark Grabowsky waswith the National Immunization Program,Centers for Disease Control and Prevention,Atlanta, Ga.
Requests for reprints should be sent toJulie Shea Hamlin, MPH, 1 Coronet Ln, EastHampton, NY 11937.
This paper was accepted June 14, 1996.
December 1996, Vol. 86, No. 12