Embed Size (px)
Citation preview

Assessing level of consciousness and cognitive changes
from vegetative state to full recovery
Tristan Bekinschtein, Cecilia Tiberti, Jorge Niklison, MercedesTamashiro, Melania Ron, Silvina Carpintiero, Mirta Villarreal,
Cecilia Forcato, Ramon Leiguarda, and Facundo Manes
Institute for Neurological Research (FLENI), Buenos Aires, Argentina
Although investigations addressing cognitive recovery from the vegetativestate have been reported, to date there have been no detailed studies ofthese patients combining both neuropsychology and functional imaging tomonitor and record the recovery of consciousness. This paper describesthe recovery of a specific vegetative state (VS) case. The patient (OG)remained in the vegetative state for approximately two months, increasingher level of awareness to a minimally conscious state, where she continuedfor approximately 70 days. In the course of the ensuing 18 months, she wasable to reach an acceptable level of cognitive functioning, with partial levelsof independence. Throughout this two year period, she received continuouscognitive evaluation, for which several different tools were applied includingcoma and low functioning scales, full cognitive batteries, and structural andfunctional magnetic resonance imaging (MRI). We present here preliminarydata on fMRI using a word presentation paradigm before and after recovery;we also discuss the difficulty of how to determine level of consciousnessusing the tools currently available, and the subsequent improvement indifferent cognitive domains. We confirm that accurate diagnosis andproper cognitive assessment are critical for the rehabilitation of patientswith disorders of consciousness.
Correspondence should be sent to Facundo Manes, Cognitive Neurology Section, Neurology
Department, Institute for Neurological Research (FLENI), Montaneses 2325 (C1428AQK),
Buenos Aires, Argentina. Tel: (54) 11 5777 3200 ext 2802, Fax: (54) 11 5777 3209. Email:
NEUROPSYCHOLOGICAL REHABILITATION
2005, 15 (3/4), 307–322
# 2005 Psychology Press Ltd
http://www.tandf.co.uk/journals/pp/09602011.html DOI:10.1080/09602010443000443

INTRODUCTION
Disorders of consciousness can be categorised in terms of degree of patientawareness into different levels: (1) coma (very low arousal level and no aware-ness); (2) vegetative state (VS; higher level of arousalwithout awareness of selfor environment); and (3) minimally conscious state (MCS; full arousal leveland inconsistent but reproducible evidence of awareness) (Multi-SocietyTask Force on PVS, 1994; Giacino et al., 2002). However, these conditionscan also be considered as a single awareness level continuum, ranging fromcoma to high minimally conscious state. Accurate diagnosis is crucial in lowawareness patients, because of the potential effect on patient prognosis, aswell as the way in which the families and/or caregivers perceive the condition.
New imaging techniques such as positron emission tomography (PET) andfunctional magnetic resonance imaging (fMRI) have been used to assess brainfunction in VS and MCS patients (see Laureys, Owen, & Schiff, 2004 for arecent review). Menon et al. published results from a patient in VSshowing fusiform gyrus activity, indistinguishable from what was observedin control groups after presentation of facial stimuli (Menon et al., 1998).Recently, Laureys and coworkers reported increased activity in the auditorytemporal area and related structures after click stimulation in VS patients,with decreased functional connectivity (Laureys et al., 2000). Higher brainactivity was also found in MCS patients as compared to VS (Boly et al.,2004). Our group has recently reported a case of MCS that showed decreasedtemporal auditory cortex activity after speech stimuli presentation andincreased amygdala activity while hearing a voice with emotional valence(Bekinschtein et al., 2004). To our knowledge, there are no reports of func-tional imaging during both VS and after recovery using complex stimuli.
The cognitive assessment plays a key role in the management of thesepatients with disorders of consciousness, due to the fact that even minimalimprovement or change in behaviour may influence treatment and prognosis.However, simple cognitive tests traditionally used in clinical practice are insuf-ficient to capture the subtle changes that may occur under different states ofconsciousness. The Rancho Los Amigos Scale or the Glasgow Coma Scale(GCS; Teasdale, Knill-Jones, & van der Sande, 1978) offer limited sensitivitycompared to changes that can be detected using other more extended scales,such as the Coma Rating Scale (CRS; Giacino, Kalmar, & Whyte, 2004;Giacino, Kezmarsky, DeLuca, & Cicerone, 1991) or the Wessex HeadInjury Matrix (WHIM; Shiel et al., 2000). These extended scales coverdifferent cognitive and physiological responses, allowing improvement indifferent cognitive domains to be easily detected when patients are followedfor weeks or even months (Wilson, Harpur, Watson, & Morrow, 2002).
To date, few detailed investigations addressing cognitive recovery fromthe vegetative state have been described. BarbaraWilson et al. have published
308 BEKINSCHTEIN ET AL.

one case in which a patient, having remained in VS/MCS for six months,underwent several cognitive assessments after recovery (Wilson, Gracey, &Bainbridge, 2001). This patient showed a slow pattern of cognitive improve-ment, only partly dependent on physical recuperation. Unfortunately, the datapresented by Wilson’s group lacked behavioural assessment while in VS andMCS and functional imaging after recovery. Other authors have used onlylimited cognitive assessments, and cognitive recovery was tested to aminimum degree (Passler & Riggs, 2001).
The objective of this study was, therefore, to redress this imbalance in theliterature and to monitor and record the recovery of consciousness in abrain-injured patient (OG); initially diagnosed as vegetative, from very lowfunctioning to high cognitive ability levels, combining a breadth of neuro-psychological assessments with structural and functional imaging.
CASE REPORT
OG was 20 years old when she sustained a motor vehicle accident. She wastransferred almost immediately, unconscious, to the nearest regional hospital.Six hours later she was admitted to FLENI Intensive Care Unit with aGlasgow Coma Scale (GCS) score of 3. On arrival the patient presenteddecerebration, bilateral decorticate posturing and unreactive right, and hypo-reactive left pupils. On day 2, a computed tomography (CT) scan showed sub-arachnoideal haemorrhages and small concussions in the right frontal and lefttemporoparietal regions. She subsequently developed hydrocephalus andrequired ventriculoperitoneal shunt decompression. A follow-up CT scanon day 6 showed partial haemorrhagic lesions on the left side of the pons,as well as in the upper left cerebellum and right frontal subcortical regions.Hypodense lesions were also observed in the region surrounding the leftcatheter. A third CT scan on day 23 revealed a decrease in lesion size, withpersistent limited bifrontal tissue hypodensities in the cortical and subcorticalregions. These findings were confirmed through structural MRI on day 30.During the first month, both a tracheotomy and a gastrostomy were per-formed. The patient also presented central fever, tachycardia, hypertensionand pneumonia during the acute phase of her condition. Only after thepatient was clinically stable was she admitted to the FLENI RehabilitationCentre (day 50) where she immediately began physical and occupationaltherapy, together with a complete multisensory stimulation programme.Methylphenidate and dopaminergic agonists were subsequently introducedaiming to improve arousal and other attentional mechanisms (Matsudaet al., 2003; Richer & Tell, 2003). For the first four months, patient levelof consciousness was assessed using coma or low functioning assessmentscales, and for the ensuing year and a half, Addenbrooke’s Cognitive
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 309

Examination was used for patient cognitive status follow up. Also, two fullcognitive batteries were administered during this second period and twofMRI studies were undertaken, the first during the VS phase, and thesecond after partial recovery.
Methods
Patient consciousness level was assessed following the Multi-Society TaskForce on PVS Guidelines (1994) and the recent clinical definition of MCS(Giacino et al., 2002). Also, as behavioural assessment tools, the JFKComa Recovery Scale (CRS; Giacino et al., 1991) was applied weekly, orevery two weeks, and the Wessex Head Injury Matrix (WHIM; Shiel et al.,2000) was administered monthly. In addition, the Functional IndependenceMeasure (FIM; Granger, Deutsch, & Linn, 1998) and Disability RatingScale (DRS; Rappaport, Herrero-Backe, Rappaport, & Winterfield, 1989),were used both to monitor degree of disability and as measures of clinicaloutcome. All assessments were carried out by the same examiners, both foreach scale and for the entire duration of the study.
Initial cognitive status of the patient was monitored using BedsideLanguage Assessment (BLA), a screening test battery developed at ourcentre specifically for low functioning patients; comprising spontaneouslanguage tests, yes/no responses to specific questions, repetition tests,writing tests and reading tests. The maximum score for the BLA is 25/25and patients with severe cognitive deficits, but capable of communication,usually reach this score. Once a ceiling effect for the BLA is observed, it isreplaced with Addenbrooke’s Cognitive Examination (ACE), which thenbecame the cognitive tool that was need to follow OG’s cognitive recovery.This test has six components evaluating separate cognitive domains: (1)orientation, (2) attention, (3) memory, (4) verbal fluency, (5) language, and(6) visual-spatial abilities (Mathuranath et al., 2000). Also, a completecognitive evaluation was conducted on two separate occasions. The batteryincluded the following tests: Raven’s Progressive Matrices, the RivermeadBehavioural Memory Test (Wilson, Cockburn, Baddeley, & Hiorns, 1989),the Rey List, Logical Memory Test, Rey-Osterreith Complex Figure Test,the Wechsler Adult Intelligence Scale (WAIS III)—Digits Span, Vocabulary,Letter Number, and the Reitan Trail Making Test.
A Frontal Assessment Battery (FAB; Dubois, Slachevsky, Litvan, &Pillon, 2000) was used as a screening battery for frontal function threetimes during this study. FAB performance gives a composite global score,which evaluates the severity of the dysexecutive syndrome, and maysuggest a descriptive pattern of executive dysfunction in a given patient. Itconsists of six subtests exploring conceptualisation, mental flexibility,
310 BEKINSCHTEIN ET AL.

motor programming, sensitivity to interference, inhibitory control andenvironmental autonomy, and takes approximately 10 minutes to administer.
An fMRI study was performed during VS and after recovery, including a5 minute passive auditory task, consisting of 30-second blocks of silence,white noise and simple words as stimuli. The BOLD images were acquiredusing a T2-weighted gradient echo sequence (TR 3 s, 8 mm slice thickness),on a General Electric Signa CVI 1.5T system. Five slices covering thetemporal lobe region were acquired both during stimulation periods and atrest. The data were analysed with SPM2 (developed by members and colla-borators of the Wellcome Department of Imaging Neuroscience, London,UK). EPI images underwent slice-timing, realign and smooth processing,without normalisation because of the major differences occurring in braintissue in the VS and after TBI. Activation maps were co-localised followingco-registration with the corresponding anatomical T1-IR volume. A correctedsignificance threshold of p , .05 and an uncorrected p value of , .001 wereused for comparative analysis.
Treatment
From day 50 until day 113 after trauma OG followed an integrative multisen-sory programme at the rehabilitation institute. The multidisciplinary teamincluded an occupational therapist (OP), a physical therapist (PT), and aspeech language pathologist (SPL). This approach is based on the applicationof combined visual, acoustic, tactile, taste and smell stimulation. Acousticstimulation included reading familiar literature to the patient, playing herfavourite music or bells, or exposing her to familiar voices; visual stimulationincluded showing her bright colourful objects or familiar items or pictures;olfactory stimulation involved exposure to familiar smells both pleasantand unpleasant; tactile stimulation included feeling objects of differenttexture and/or temperature, and buco-facial massage; kinaesthetic and pro-pioceptive stimulation included both vestibular and proprioceptive stimuli.General goals for this stage were to increase arousal and alertness, enhancerecognition of the environment, and improve posture and body movementcapacity. During this first rehabilitation period she underwent two two-hoursessions a day.
On day 114, a cognitive rehabilitation programme was started, wheredifferent goals were established depending on the degree of recoveryalready achieved. Initially, the focus was on sustained attention and orien-tation (daily individual 30 minute sessions). Higher cognitive functionsincluding memory, executive functions, and abstract reasoning wereaddressed at a later stage. As an outpatient, she received both individualand group therapy, in an attempt to solve problems in daily living (such asmemory deficits or social skills issues). As part of group therapy, she also
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 311

began, and continues to attend, weekly group sessions on understanding braininjury (since May 2003). Under a holistic approach, OG began cognitive-behavioural therapy sessions (from February 2004), in order to address“emotional reactions”. Cognitive (thoughts associated with emotions), beha-vioural (increasing activity) and emotional techniques (identification andexpression of emotions) were all used to improve her ability to identify,express and recognise emotional reactions and states. Currently, shecontinues to work on these deficits.
Results
From VS to MCS. The patient arrived at the FLENI ICU presenting aGCS score of 3 (day 1). On the following day she received sedation lastingfive days. Once discontinued (day 6), the GCS score fluctuated between 3and 7 throughout the day. For the next 44 days the GCS score rangedbetween 4 and 9. When the patient was finally discharged to the rehabilitationclinic on day 50, she presented a score of 8, localising painful stimuli, eyeopening responses to pain, but still lacking verbal response capacity or anysign of awareness.
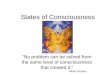
The CRS and WHIM results are summarised in Figure 1. The CRScaptured a few changes in OG’s level of consciousness. Between days 66and 108, total CRS values ranged between 17/25 and 19/25, with inconsist-ent responses to simple commands, corresponding therefore to a minimally
Figure 1. CRS, DRS and WHIM performance over time. CRS and DRS data are from days 66 to 122
post-trauma, WHIM data are from days 51 to 235. The values are converted to 0–100 scale for each
assessment tool. Triangles are used to show WHIM data, open circles for DRS data and open squares
for CRS data. The estimated periods in which the patient was diagnosed as VS or MCS are shown in
the horizontal bar (dark grey for VS and light grey, for MCS)
312 BEKINSCHTEIN ET AL.

conscious state. Also, she was able to track nearby moving objects, and erra-tically move one hand to touch the other. Arousal level, as measured by theCRS, fluctuated between the ability to maintain her eyes open for 15–30minutes (days 66 to 86), to being able to do so only for a few minutes ondays 101 and 108, and finally on day 122, she was able to maintain acertain degree of sustained attention. The patient recovered verbal reflexeson day 66, presenting spontaneous vocalisation on days 80 and 86, laterexpressing isolated words, sometimes abusive (swearing) on days 101 and108 (CRS 19/25), and finally yes/no responses on day 122, but stilllacking spontaneous speech.
On day 122 considerable improvement in awareness level was observed,the patient scored 24/25 on tests for movement reproduction prompted bysimple commands, as well as for object recognition; more importantly, shebegan to show clear signs of communication, e.g., saying no to the therapist(MT) whenever she was asked to show how to move her lower limbs. At thisstage the ceiling effect clearly revealed the limitations of CRS when evaluat-ing this patient in high MCS, fortunately the improvement was readilycaptured by other tools.
The Wessex Head Injury Matrix was first administered on arrival of thepatient at the rehabilitation centre (day 51), two weeks prior to the firstCRS assessment. At the time, with a score of 10/62, OG could not followsimple commands but sustained visual pursuit was observed, a sign of tran-sition from VS to MCS (Giacino & Trott, 2004). One month later (day 81),the patient was able to inconsistently follow simple commands, and shewas therefore diagnosed as being in MCS (with a WHIM score of 24/62).On day 112, having reached scores of 41/62, the patient began to show spora-dic signs of communication, as observed whenever she was forced to choosean object, or vocalising to protest forcibly against a blood extraction, evenbeing able to name one of the nurses. The first Bedside Language Assessmenttaken on day 105 showed a very low score of 8/25, with 5 points for rep-etition, 2 points for spontaneous language, and 1 point for an yes/no question.By that time she was showing highly complex behaviour for an MCS patient,probably in high MCS or emerging from this state. This was also reflected inthe patient’s CRS score of 24/25 on day 122, and her WHIM score of 41/62on day 112, both indicating some degree of communication.
Disability rating measures. As a measure of disability degree, theDisability Rating Scale was administered and assessed on the same days asthe CRS; both results are shown in Figure 1. From days 66 to 122, OG pre-sented spontaneous eye opening. During the first two assessments (on days66 and 80) she manifested no communication ability and finally, on day86, she began to show signs of verbal response, but remained incomprehen-sible. As expected, scale application revealed motor withdrawal in response
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 313

to noxious stimuli (greater than a simple reflex) on day 66, noxious localisa-tion a few days later and command-following capacity on the last day (122).Cognitive independent self-care skills remained absent until day 108, and onday 122 were classified as minimal. OG continued to be totally dependent onothers until day 108. Yet, by day 122, she had become moderately indepen-dent (she was back at home by then). Total agreement between the DRS andthe CRS scale was observed; the main difference being absence of ceilingeffect for the DRS (see Figure 1).
The Functional Independence Measure (FIM) proved to be the best assess-ment instrument to make an appropriate follow up, and accurately reflectedOG’s rate of recovery during the period from September 2002 to June 2004(Figure 2). The first 130 days showed scores in the lower third of the scale,middle values were registered between days 131 and 230, reflecting animprovement in almost all items except social adjustment; and from day231 to 683, the FIM was only able to detect minor improvements in self-care, sphincter control and cognition.
Recovery from MCS. In January 2003 the second Bedside LanguageAssessment (BLA), on day 162, confirmed the presence of significantrecovery with a very high score of 24/25, so Addenbrooke’s CognitiveExamination (ACE) was immediately performed, with a score of 50/100(see Table 1). This corresponded to clear deficits in all cognitive domains.Despite profound deficits in memory, attention, motor skills and other cogni-tive functions, she could consistently communicate with staff, relatives, andfriends. Three months later, on day 235, the last WHIM scale was performed
Figure 2. FIM performance over time from days 59 to 683 post-trauma. Circles are used to show FIM
data, top FIM score is 126
314 BEKINSCHTEIN ET AL.

with a score of 52/62. All unassigned points corresponded to motor tasksthat the patient was unable to execute. However, she had scored top pointsin all other domains, demonstrating that the WHIM was no longer usefulfor cognitive recovery follow up monitoring. The second ACE was adminis-tered 4 months (day 270) after the first, with improvement in all domains, butmost especially in language and memory skills, jumping from 15/35 to25/35, and 18/30 to 24/30, respectively (total score of 74/100). Onemonth later (day 302) as her cognitive recovery continued, she scored81/100 in the ACE (MMSE of 28).
Cognitive recovery. Patient cognitive recovery dynamics are described inTable 1 and the detailed cognitive analysis in Table 2. A sustained improve-ment in her cognitive abilities has been observed between days 162 to 690, asshown from the five ACEs performed during this period. Between the first(50/100) and the second ACE (74/100), clear progress in all cognitivedomains could be seen. The third ACE (day 302) showed some improvementsin language, attention and fluency, compared to the second assessment. Sevenmonths later, the fourth ACE (day 527) only showed slight progress inmemory, language and praxis abilities.
A lack of sensitivity for the ACE was observed at this time and it becamenecessary to assess in detail the different cognitive domains. Therefore, twofull cognitive evaluations were conducted on days 307–314 and 520–527(June 2003 and January 2004), the results can be seen in Table 2.
Full cognitive assessment suggested that OG was impaired in delayedrecall in the Logical Memory Test, but not in immediate recall or recognition(see Table 2). Both the immediate and delayed recall improved during thesecond assessment marking significant progress in OG’s anterograde
TABLE 1OG’s Addenbrooke’s Cognitive Examinations from January 2003 to July 2004
January 2003 May 2003 June 2003 January 2004 July 2004
Day 162 270 302 492 690
ACE 50 74 81 87 95
MMSE 17 27 28 29 30
Orientation 7 10 10 10 10
Attention 3 7 8 8 8
Memory 15 25 25 28 35
Fluency 6 5 8 8 9
Language 18 24 27 28 28
Praxis abilities 1 3 3 5 5
Total ACE and MMSE values and sub-values for each cognitive domain are shown. Highest poss-
ible scores for ACE domains are: 100 for total score; 10 for orientation; 8 for attention; 35 for memory;
14 for fluency; 28 for language; and 5 for praxis abilities
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 315

TABLE 2OG’s results for first (June 2003) and second (January 2004) full cognitive assessments,
and WAIS-III and FAB for June 2003, January 2004 and July 2004
Test June 2003 January 2004 July 2004
Wechsler Adult Intelligence Scale III
Forward digits 8 8 8
Backward digits 2 4 6
Digit Span (Aged scale score) 5 7 8
FAB (Frontal Assessment Battery) 14/18 18/18 17/18
Ravens Coloured Progressive
Matrices (Raw Score)
25/36 28/36
Wechsler Memory Scale—Revised
Logical Memory (Prose Recall)
Immediate Recall Mean (SD)
27.4 (9.6)
20 27
Delayed Recall Mean (SD)
19.8 (6.7)
13 26
Recognition 18/20 19/20Rey Auditory—Verbal Learning Test
Recall Mean (SD)
52.3 (8.0)
36 35
Delayed Recall Mean (SD)
1.1 (2.7)
6 3
Recognition Mean (SD)
13.5 (1.6)
1 9
Rey-Osterreith Complex Figure
Copy Mean (SD)
33.9 (1.5)
could not
complete
34
Delayed Recall Mean (SD)
21.8 (6.5)
10.5
Recognition correct
Rivermead Behavioural Memory Test
Screening Score 8 (Poor
memory)
9 (Poor
memory)
Standardised Profile Score 17 (Poor
memory)
19 (Poor
memory)
Trail Making Test
Part A Mean (SD)
27.4 (9.6)
250 sec 177sec
Part B Mean (SD)
58.7 (15.9)
discontinued
at 300 s
308 sec
Wisconsin Card Sorting Test cancelled
Categories 6/6Total errors 1
316 BEKINSCHTEIN ET AL.

long-term memory capacity. Very limited learning capacity was evidenced oneither cognitive evaluations (no learning curve) as seen with the Rey List.However, significant recognition improvement was observed in the secondassessment. This enhanced cue recall capacity suggests some degree of recov-ery for memory storage ability. Finally, the Rivermead Behavioural MemoryTest, built up to detect impairment of everyday memory functioning and tomonitor changes following treatment for memory difficulties, showed poormemory results on both evaluations.
Visuospatial and praxis abilities were assessed with the Rey-OsterreithComplex Figure. Unfortunately, OG was unable to draw for the first evalu-ation due to right hand motor impairment. However, after intense physicaltherapy, she managed to copy the figure within normal limits. Deficit inverbal and visual memory were present. Scores for delayed recall of Reyfigure were only half of normal values. Also, as for other test results, shewas able to recognise the figure correctly.
Coloured Raven Matrices were used to assess intelligence. However, thepatient was too slow to complete a full Raven test and unable to give acorrect response for the analogical reasoning items. She did show a better per-formance during the second assessment, but still within impairment range.
Executive and frontal functions were assessed using the Frontal Assess-ment Battery, the WAIS-III, Trail Making Test A and B and WCST(Table 2). The Immediate Memory Span revealed small but consistentworking memory improvement. Trail Making Test performance observedduring patient recovery was indicative of some degree of set shiftingand working memory capacity. Further complementary information wasobtained with the Wisconsin Card Sorting Test (WCST). Unable toperform the test in the first evaluation, the patient surprisingly completedsix of six categories during the second assessment, thus presenting strongevidence of partial executive function recovery after seven months of therapy.
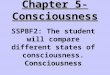
Brain activation after word presentation. Both fMRI results are shown inFigure 3.The first was completed while the patient was in VS (September2002), and the second after recovery (May 2003). Word vs. silence compari-son showed a small area of left temporal activation in the transverse temporalgyrus and superior temporal gyrus during the vegetative state. However,much stronger bilateral temporal activation was observed after recovery(speech and auditory areas) with some degree of frontal activity as well.This second scan activation pattern was similar to the one of normal subjects(Bekinschtein & Manes, unpublished data). Transverse temporal gyrus andsuperior temporal gyrus focal activity was slightly higher after recoverythan while in VS. However, activation variability was much higher in VS(see Figure 4). Extended spread of activation to other areas from superior
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 317

Figure 3. Brain activation after word presentation (words vs. silence contrast). Fig. 3a OG’s brain
activity after recovery (May 2003) showing large bilateral activation in the temporal cortex,
bilateral parietal activation stronger on the left and bilateral medial prefrontal cortex activation
(corrected p , .05); Fig. 3b brain activity while in vegetative state (September 2002) showing left
transverse and superior temporal gyri activation and striate cortex activation near the precuneus
(uncorrected p , .001). Global maximum for this contrast is in both, VS and recovered states, in
the left superior temporal gyrus (being more posterior in VS). The activation maps are
superimposed on 3D-T1 images according to each scan
Figure 4. Left superior temporal gyrus activity after words vs. silence contrast. The bars show the
mean values and standard error of the higher activity voxel for each state of consciousness
318 BEKINSCHTEIN ET AL.

temporal gyrus to middle temporal gyrus, temporoparietal and frontalregions, also suggested integrated brain processing after recovery.
DISCUSSION
This work adds to growing evidence that full cognitive recovery from thevegetative or minimally conscious state is possible, and demonstrates theneed for the development of new tests, better able to capture both degreeand rate of recovery in this type of patient. This study also showed severalfindings: (1) the WHIM Scale was able to capture several different awarenesslevels, ranging from VS to MCS to partial recovery; (2) the CRS allowedmapping of both MCS and high MCS; (3) the BLA and ACE overlappedwith WHIM, when used to unmask differences during the cognitive recoverycurve, and (4) the ACE proved to be a good brief cognitive assessment toolfor recovery monitoring once a degree of communication is attained.
In comparison to previous studies on patients transitioning from very lowfunctioning states to high cognitive capabilities, two strengths arising fromthis investigation merit consideration. First, whereas previous authors(Wilson et al., 2001) had no information regarding assessment tools likethe WHIM or CRS, in this case both were included from VS to recoveryand different cognitive and functional scales were also examined. Second,this work included MRI data during VS and after recovery.
Although it is important to understand the limitations of the neuropsycho-logical tools employed, assessment of cognitive function is critical, and mayinfluence decisions about level of care or treatment provided.
Once the patient had reached a relatively high score in the ACE (81/100),full cognitive assessment was performed. Strikingly, the comparatively smalldifferences observed between the third and fourth ACE tests contrasts withthe enhanced cognitive abilities found during full cognitive evaluation,where the tests clearly captured the degree of cognitive improvementgained between these two points in time.
Seven months later, a second assessment showed improvement in allcognitive domains, particularly memory and language. The patient hasrecently achieved a normal score in the ACE (95/100). Despite the fact sheis still experiencing social skills deficits, this result demonstrates an almostcomplete recovery.
As it has been clearly established in clinical practice, significantspontaneous recovery frequently occurs during the subacute period (Wilsonet al., 2002; Giacino & Trott, 2004). Furthermore, two other favourablefactors were also presented in this case; that is to say, the patient’s youngage, and the fact that she received immediate medical assistance after theaccident. Although fluctuations were observed during the acute and subacute
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 319

period, in the end there was a clear trend towards higher levels of conscious-ness (from GCS 3–5 to GCS 7–9 in 50 days). On day 51 the patient receivedmethylphenidate, and this was replaced one week later by levodopa,coinciding with transition from VS to MCS, as documented using theWessex Head Injury Matrix (days 50 to 81). Unlike the WHIM, the CRShad to be interrupted on two separate occasions because the patient lackedthe arousal level necessary to complete the test. A few weeks later (day66), the first full CRS was completed; also, because it was administeredmore often than the WHIM, the CRS evaluations were able to show improve-ment in different aspects of the MCS, and even register the fluctuationsobserved during this period. The DRS performed during recovery showedsimilar results to the CRS but without registering fluctuations, probablybecause the DRS measures more general features of recovery. AlthoughDRS (not CRS) could have been used to follow the recovery for a longerperiod, FIM was the tool finally selected to measure the patient’s functionalrecovery.
Day 112, the point at which she was able to call a nurse by name, wasconsidered the beginning of exiting the minimally conscious state. Somemight argue that the day of the first BLA (day 105) could be taken asthe end of the MCS, but on day 108 the patient was not able to communicatespontaneously (CRS score was 19/25). This would, therefore, appear torepresent more a fluctuation in awareness level, rather than a clear-cut endto the MCS. From day 112 until now, patient cognitive status has continuedto show uninterrupted improvement. The fMRI study revealed particularphysiological features in this patient. It was able to capture increased corticalactivity during a passive word listening task, showing small but consistentfocal processing in VS, as compared to the large bilateral cortical processingobserved after recovery. The first assessment showed limited cortical acti-vation, probably residual, automatic and unconscious. This result wasexpected due to the very limited behavioural responses demonstrated bythe patient in September 2002. This activation pattern coincides with recentfindings concerning differences in brain activity observed between VSpatients, MCS patients and control subjects (Boly et al., 2004). Also, theincreased variability (Figure 4) in the focal temporal activity (STG-TTG/Brodmann area 22) revealed qualitative differences in the cortical processingduring these two states of consciousness. It is important to note that OG’srecovered brain activity was very similar to that seen in controls, suggestinggood functional and physiological recovery 10 months after the accident, and5 months after abandoning the MCS. Several studies have highlighted theneed for careful, repeated and reliable assessment of patients with impairedlevels of consciousness (McMillan & Herbert, 2004; Lombardi et al., 2002;Lippert-Gruner, Wedekind, & Klug, 2003). Once again, we confirm theneed for appropriate cognitive supervision after leaving MCS, since this
320 BEKINSCHTEIN ET AL.

could shed light on recovery mechanisms activated during consciousness dis-orders. Although the patient’s cognitive abilities were meticulously assessed,the clear deficit in social skills persisting to date was not captured either byACE tests, nor even a full cognitive assessment. Cognition abilities withtheory of mind tasks, decision-making tasks, social performance tests andan expanded cognitive assessment, to further characterize post-traumaticvegetative patients after recovery remain under evaluation at this time. Thisstudy suggest that the cognitive recovery in patients with disorders of con-sciousness is a continual process rather than a step-by-step phenomenonand confirms that a good recovery assessment should include objectivemeasures of behavioural, cognitive and functional domains, and neurophysio-logical data to support the diagnosis.
REFERENCES
Bekinschtein, T., Leiguarda, R., Armony, J., Owen, A., Carpintiero, S., Niklison, J., et al.
(2004). Emotion processing in the minimally conscious state. Journal of Neurology, Neuro-
surgery, and Psychiatry, 75(5), 788.
Boly, M., Faymonville, M. E., Peigneux, P., Lambermont, B., Damas, P., Del Fiore, G., et al.
(2004). Auditory processing in severely brain injured patients: Differences between the
minimally conscious state and the persistent vegetative state. Archives of Neurology,
61(2), 233–238.
Dubois, B., Slachevsky, A., Litvan, I., & Pillon, B. (2000). The FAB: A Frontal Assessment
Battery at bedside. Neurology, 55(11), 1621–1626.
Giacino, J. T., Ashwal, S., Childs, N., Cranford, R., Jennett, B., Katz, D. I., et al. (2002). The
minimally conscious state: Definition and diagnostic criteria. Neurology, 58(3), 349–353.
Giacino, J. T., Kalmar, K., & Whyte, J. (2004). The JFK Coma Recovery Scale—Revised:
Measurement characteristics and diagnostic utility. Archives of Physical Medicine Rehabi-
litation, 85(12), 2020–2029.
Giacino, J. T., Kezmarsky, M. A., DeLuca, J., & Cicerone, K. D. (1991). Monitoring rate
of recovery to predict outcome in minimally responsive patients. Archives of Physical
Medicine Rehabilitation, 72(11), 897–901.
Giacino, J. T., & Trott, C. T. (2004). Rehabilitative management of patients with disorders of
consciousness: Grand rounds. Journal of Head Trauma Rehabilitation, 19(3), 254–265.
Granger, C. V., Deutsch, A., & Linn, R. T. (1998). Rasch analysis of the Functional Independence
Measure (FIM) Mastery Test. Archives of Physical Medical Rehabilitation, 79(1), 52–57.
Laureys, S., Faymonville, M. E., Degueldre, C., Fiore, G. D., Damas, P., Lambermont, B., et al.
(2000). Auditory processing in the vegetative state. Brain, 123(8), 1589–1601.
Laureys, S., Owen, A. M., & Schiff, N. D. (2004). Brain function in coma, vegetative state, and
related disorders. Lancet Neurology, 3(9), 537–546.
Lippert-Gruner, M., Wedekind, C., & Klug, N. (2003). Outcome of prolonged coma following
severe traumatic brain injury. Brain Injury, 17(1), 49–54.
Lombardi, F., Taricco, M., De Tanti, A., Telaro, E., & Liberati, A. (2002). Sensory stimulation
of brain-injured individuals in coma or vegetative state: Results of a Cochrane systematic
review. Clinical Rehabilitation, 16(5), 464–472.
Mathuranath, P. S., Nestor, P. J., Berrios, G. E., Rakowicz, W., & Hodges, J. R. (2000). A brief
cognitive test battery to differentiate Alzheimer’s disease and frontotemporal dementia.
Neurology, 55(11), 1613–1620.
ASSESSING LEVEL OF CONSCIOUSNESS IN VS 321

Matsuda, W., Matsumura, A., Komatsu, Y., Yanaka, K., & Nose, T. (2003). Awakenings from
persistent vegetative state: Report of three cases with Parkinsonism and brain stem lesions
on MRI. Journal of Neurology, Neurosurgery and Psychiatry, 74(11), 1571–1573.
McMillan, T. M., & Herbert, C. M. (2004). Further recovery in a potential treatment withdrawal
case 10 years after brain injury. Brain Injury 18(9), 935–940.
Menon, D. K., Owen, A. M., Williams, E. J., Minhas, P. S., Allen, C. M., Boniface, S. J., &
Pickard, J. D. (1998). Cortical processing in persistent vegetative state. Wolfson Brain
Imaging Centre Team. Lancet, 352(9123), 200.
Multi-Society Task Force on PVS (1994). Medical aspects of the persistent vegetative state,
1. New England Journal of Medicine, 330, 1499–1508.
Passler, M. A., & Riggs, R. V. (2001). Positive outcomes in traumatic brain injury-vegetative
state: Patients treated with bromocriptine. Archives of Physical Medical Rehabilitation,
82(3), 311–315.
Rappaport, M., Herrero-Backe, C., Rappaport, M. L., & Winterfield, K. M. (1989). Head injury
outcome up to ten years later. Archives of Physical Medical Rehabilitation, 70(13),
885–892.
Richer, E., & Tell, L. (2003). Indications, efficacy and tolerance of drug therapy in view of
improving recovery of consciousness following a traumatic brain injury. Ann Readapt
Med Phys, 46(4), 177–183.
Shiel, A., Horn, S. A., Wilson, B. A., Watson, M. J., Campbell, M. J., &McLellan, D. L. (2000).
The Wessex Head Injury Matrix (WHIM) main scale: A preliminary report on a scale to
assess and monitor patient recovery after severe head injury. Clinical Rehabilitation,
14(4), 408–421.
Teasdale, G., Knill-Jones, R., & van der Sande, J. (1978). Observer variability in assessing
impaired consciousness and coma. Journal of Neurology, Neurosurgery and Psychiatry,
41(7), 603–610.
Wilson, B., Cockburn, J., Baddeley, A., & Hiorns, R. (1989). The development and validation of
a test battery for detecting and monitoring everyday memory problems. Journal of Clinical,
Experimental and Neuropsychology, 11(6), 855–870.
Wilson, B. A., Gracey, F., & Bainbridge, K. (2001). Cognitive recovery from “persistent
vegetative state”: Psychological and personal perspectives. Brain Injury, 15(12), 1083–1092.
Wilson, F. C., Harpur, J., Watson, T., & Morrow, J. I. (2002). Vegetative state and minimally
responsive patients—regional survey, long-term case outcomes and service recommen-
dations. NeuroRehabilitation, 17(3), 231–236.
322 BEKINSCHTEIN ET AL.