Embed Size (px)
Citation preview

Assessing Heart Rate Variability as a Surrogate Measure of Cardiac Autonomic Function in Chronic Traumatic
Spinal Cord Injury
by
Rasha El-Kotob
A thesis submitted in conformity with the requirements for the degree of Master of Science in Rehabilitation Science
Graduate Department of Rehabilitation Science University of Toronto
© Copyright by Rasha El-Kotob 2015

ii
Assessing Heart Rate Variability as a Surrogate Measure of
Cardiac Autonomic Function in Chronic Traumatic Spinal Cord
Injury
Rasha El-Kotob
Master of Science in Rehabilitation Science
Graduate Department of Rehabilitation Science
2015
Abstract
Individuals with a spinal cord injury (SCI) are at greater risk of cardiovascular disease (CVD)
than able-bodied individuals. A major CVD contributing factor is the presence of autonomic
disturbances, but the SCI-related changes in cardiac autonomic function are poorly understood.
Heart rate variability (HRV) has been reported to non-invasively assess the cardiac autonomic
nervous system (ANS). The following thesis involves investigating resting HRV in 56 subjects
with a traumatic chronic SCI with the aim to 1) describe the overall distribution of HRV in SCI;
2) determine whether there are HRV differences based on level and/or severity of injury; and, 3)
determine whether there is a relationship between parasympathetic and sympathetic frequency
measures. The results revealed that HRV is variable between-subjects, there were no significant
HRV differences based on level and/or severity of impairment, and the low frequency-to-high
frequency ratio (LF:HF), may not be an applicable measure in traumatic chronic SCI.

iii
Acknowledgments
I would like to thank my supervisor, Professor Molly Verrier, for accepting me as a Master’s
student, introducing me to the world of research, providing me with true mentorship, and
stimulating my interests. I would also like to thank my co-supervisor, Dr. Sunita Mathur, for her
constant genuine encouragement and for offering me valuable on-going guidance even beyond
the scope of my research. I took pleasure in conducting my Master’s study and I owe it to both of
my supervisors.
I would like to acknowledge the members of my advisory committee, Dr. Catherine Craven, Dr.
Dave Ditor, and Dr. Paul Oh for their insightful input and even assistance regarding the planning
and execution of my research work.
Thank you to the research staff, graduate students and co-op students at Toronto Rehabilitation
Institute-UHN, Lyndhurst Centre. I was fortunate to work in such a fruitful research environment
with such knowledgeable colleagues. I would also like to especially thank Dr. Masae Miyatani
for allowing me to run a secondary data analysis on her collected data.
I am forever grateful for my parents who have always believed in me and never stopped cheering
me on. Thank you to my siblings, for being the reasons why I smile even during the stressful
times. Finally, I would like to express my gratitude to my university sweetheart and devoted
husband- not only did you support me relentlessly, but also you sincerely showed an immense
interest in my research which undeniably contributed to my eagerness.
I would also like to acknowledge the funder of this research: The Canadian Institute of Health
Research (Grant #: TCA-118348).

iv
Table of Contents
Acknowledgments .......................................................................................................................... iii
Table of Contents ........................................................................................................................... iv
List of Tables ................................................................................................................................ vii
List of Figures .............................................................................................................................. viii
List of Appendices ......................................................................................................................... ix
Glossary .......................................................................................................................................... x
Chapter 1: ........................................................................................................................................ 1
1 Introduction ................................................................................................................................ 1
1.1 Spinal cord injury ................................................................................................................ 1
1.1.1 Cardiovascular disease in spinal cord injury .......................................................... 2
1.1.2 The function of the autonomic nervous system in spinal cord injury ..................... 3
1.2 Heart rate variability ........................................................................................................... 5
1.3 Literature review ................................................................................................................. 8
1.3.1 The findings on heart rate variability in spinal cord injury .................................... 8
1.3.2 Factors affecting heart rate variability .................................................................. 10
1.4 Study rationale .................................................................................................................. 12
Chapter 2: ...................................................................................................................................... 15
2 Objectives and Hypothesis ....................................................................................................... 15
2.1 Objectives ......................................................................................................................... 15
2.1.1 Primary Objective ................................................................................................. 15
2.1.2 Secondary Objective ............................................................................................. 15
2.1.3 Tertiary Objective ................................................................................................. 16
2.2 Hypothesis ......................................................................................................................... 16
2.2.1 Primary Hypothesis ............................................................................................... 16
2.2.2 Secondary Hypothesis ........................................................................................... 16

v
2.2.3 Tertiary Hypothesis ............................................................................................... 17
Chapter 3: ...................................................................................................................................... 18
3 Methodology ............................................................................................................................ 18
3.1 Overview ........................................................................................................................... 18
3.2 Study variables .................................................................................................................. 19
3.2.1 Heart rate variability indices and related factors .................................................. 19
3.3 Subject selection. .............................................................................................................. 20
3.3.1 Electrocardiogram recordings ............................................................................... 20
3.3.2 Medications ........................................................................................................... 20
3.4 Heart rate variability analysis ........................................................................................... 21
3.5 Statistical Analysis ............................................................................................................ 24
3.5.1 Objective 1: Heart rate variability frequency distributions ................................... 24
3.5.2 Objective 2: Comparison of heart rate variability based on level and/or
severity of injury ................................................................................................... 24
3.5.3 Objective 3: Assessing the LF and HF indices ..................................................... 25
Chapter 4: ...................................................................................................................................... 26
4 Results ...................................................................................................................................... 26
4.1 Subject selection ............................................................................................................... 26
4.2 Frequency distributions of the heart rate variability indices ............................................. 28
4.3 Heart rate variability comparisons across level and/or severity of injury ........................ 31
4.3.1 Comparison of heart rate variability related factors across cohorts ...................... 35
4.4 Assessing the heart rate variability frequency domain indices: LF, HF and LF:HF ........ 38
4.4.1 Relationship between LF and HF ......................................................................... 38
4.4.2 Relationship between LF, HF, LF:HF and influencing factors ............................ 39
4.4.3 Predicting LF and HF from heart rate variability-related factors ......................... 41
Chapter 5: ...................................................................................................................................... 43

vi
5 Discussion ................................................................................................................................ 43
5.1 Implications and future directions .................................................................................... 51
5.2 Study limitations ............................................................................................................... 52
Chapter 6: ...................................................................................................................................... 54
6 Conclusions .............................................................................................................................. 54
References ..................................................................................................................................... 55
Appendices .................................................................................................................................... 61

vii
List of Tables
Table 1. HRV time domain and frequency domain measures* ...................................................... 8
Table 2. Factors reported to influence HRV ................................................................................. 11
Table 3. Potential HRV-related variables selected from the primary data ................................... 19
Table 4. Demographics and vital signs of the participants in total sample and per cohort........... 28
Table 5. Descriptive statistics for each HRV index in the entire sample (N=56) ......................... 29
Table 6. Comparison of HRV indices based on level of injury .................................................... 31
Table 7. Comparison of HRV indices based on severity of injury ............................................... 32
Table 8. Comparison of HRV indices based on level and severity of injury ................................ 33
Table 9. Relationship of the LF and HFindices based on level or severity of injury ................... 39
Table 10. Relationship of the LF and HF indices based on level and severity of injury .............. 39
Table 11. The relationship between LF, HF indices and the scalar HRV-related factors ............ 39
Table 12. Multiple linear regression analysis to predict LF for the entire sample (R2=0.039) .... 41
Table 13. Multiple linear regression analysis to predict HF for the entire sample (R2=0.009) .... 42
Table 14. Comparison of inter-individual variations in HRV between healthy subjects and
chronic traumatic SCI ................................................................................................................... 44

viii
List of Figures
Figure 1. Possible contributors to greater CVD risk in individuals with SCI............................... 13
Figure 2. Parasympathetic and sympathetic innervations of the heart and peripheral muscles. ... 14
Figure 3. Representative example of HRV analysis using LabChart
(v.7.0) .............................. 22
Figure 4. Representative example of Poincaré Plot before and after the application of 45Hz low
pass filter ....................................................................................................................................... 23
Figure 5. CONSORT flowchart reflecting the inclusion and exclusion of the final data sample. 27
Figure 6. Frequency distribution of LF:HF. .................................................................................. 30
Figure 7. Boxplot representing LF:HF distribution. ..................................................................... 30
Figure 8. Boxplot representation, with and without the outliers, of LF:HF based on level and
severity of SCI .............................................................................................................................. 34
Figure 9. Boxplot representation of LTPAQ-SCI based on level and severity of injury. ............. 36
Figure 10. Boxplot representation of LEMS based on level and severity of injury. .................... 37
Figure 11. Boxplot representation of SCIM-III based on level and severity of injury. ................ 37
Figure 12. The relationship between LF and HF for total sample. ............................................... 38
Figure 13. Possible contributors to greater CVD risk in individuals with chronic traumatic SCI.48

ix
List of Appendices
Appendix A ................................................................................................................................... 62
Appendix B ................................................................................................................................... 65
Appendix C ................................................................................................................................... 67
Appendix D ................................................................................................................................... 69
Appendix E ................................................................................................................................... 75
Appendix F .................................................................................................................................... 78
Appendix G ................................................................................................................................... 80
Appendix H ................................................................................................................................... 83
Appendix I .................................................................................................................................... 91
Appendix J .................................................................................................................................... 94
Appendix K ................................................................................................................................... 97

x
Glossary
Absolute VO2 peak: Highest value of oxygen uptake attained during an incremental exercise
test. Expressed in litres of oxygen per minutes (L/min)
Activities of daily living (ADL): refers to daily self-care activities with an individual’s place of
residence, in outdoor environments, or both.
American Spinal Cord Injury Association (ASIA) impairment scale (AIS): a five point scale
(A-E), where A corresponds to a complete injury, B-D is an incomplete injury, E is
normal motor and sensory function
Autonomic nervous system (ANS): the system of nerves and ganglia that innervates the blood
vessels, heart, smooth muscles, viscera, and glands and controls their involuntary
functions, consisting of sympathetic and parasympathetic branches
Body mass index (BMI): An index for assessing overweight and underweight, obtained by
dividing body weight in kilograms (kg) by height in meters squared (m2). A measure of
25 kg/m2 or more is considered overweight
Bootstrapping: The sampling distribution of a statistic is estimated by taking repeated samples
from the data set in order to ensure that analytical models are reliable and will produce
accurate results
Bradycardia: a slow heart rate, usually less than 60 beats per minute (bpm)
Cardiac disease: congenital or acquired disease of only the heart
Cardiorespiratory fitness: the ability of the circulatory and respiratory systems to supply
oxygen to skeletal muscles during sustained physical activity
Cardiovascular disease (CVD): congenital or acquired disease of the heart and blood vessels
Chronic: having for a long duration
Complete Injury: No motor or sensory function in the lowest sacral segments (S4-S5)

xi
Co-morbidities: Two or more diseases present simultaneously in a patient
Distribution: A graph plotting values of observations on the horizontal axis
Differences in HRV-related factors: Includes differences in age, sex, body mass index (BMI),
waist circumference (WC), time post injury, current smoking status, smoking history,
cardiorespiratory fitness level (absolute VO2 peak, relative VO2 peak, peak heart rate),
leisure time physical activity questionnaire-spinal cord injury (LTPAQ-SCI), lower
extremity motor score (LEMS), spinal cord independence measure (SCIM-III), number of
co-morbidities, family history of heart disease and sleep apnea.
Fast Fourier transform (FFT): Mathematical transformation of a function of time into a
function of frequency.
Heart rate variability: commonly used term to describe the oscillation of the heart rate and is
determined by measuring the R peak to R peak intervals, also referred to as NN intervals,
in an electrocardiograph (EGG)
High frequency (HF): A heart rate variability frequency domain measure representing vagal
modulation of the heart
Hypotension: Low resting blood pressure; in men systolic blood pressure less than 110mmHg
and in women systolic blood pressure less than 100mmHg
Incomplete injury: motor and/or sensory function preservation below neurological level of
injury and includes sacral segments (S4-S5)
Leisure time physical activity questionnaire (LTPAQ): Total number of minutes of physical
activity, not including activities of daily living, performed over the past week
Low frequency (LF): A heart rate variability frequency domain measure representing
parasympathetic and sympathetic, although more indicative of the latter, modulation of
the heart

xii
Lower extremity motor score (LEMS): Measures voluntary motor strength in five myotomes
each scored out of five for a bilateral total of 50. A score of 30 or more suggests that the
individual is likely to walk
Mean Ranks: The data is ranked from lowest to highest to eliminate the effect of outliers
Neurological level of injury (NLI): This is the lowest segment where motor and sensory
function is normal in both the left and right side of the body
Paraplegia: complete or partial loss of sensation and movement in legs and in part or all of the
trunk due to an injury below the cervical vertebrae
Peak heart rate: Highest value of heart rate attained during an exercise test. Expressed in beats
per minute (bpm).
Physical activity: Any bodily movement produced by the skeletal muscles that increases heart
rate and breathing and requires energy expenditure
Physical capacity: a measure of ability to perform
Physical fitness: A state of physiological well being
Poincaré Plot: A diagram in which each R-R interval is plotted as a function of the previous R-
R interval. The values of each pair of successive R-R interval define a point in the plot.
Proportion of the number of interval differences of the consecutive NN intervals greater
than 50ms (pNN50): The proportion of the number of interval differences of the
consecutive R peak to R peak intervals greater than 50ms derived from an
electrocardiogram. A heart rate variability time domain measure that represents cardiac
parasympathetic modulation
Relative VO2 peak: Highest value of oxygen uptake attained during an incremental exercise
test. Expressed in milliliters of oxygen per kilogram of subject’s bodyweight per minute
(mL/kg/min)

xiii
Sleep apnea: Sleeping disorder in which breathing repeatedly stops and starts. Obstructive sleep
apnea occurs when the throat muscles relax and Central sleep apnea occurs when the
brain doesn’t send proper signals to the muscles that control breathing.
Spinal cord independence measure (SCIM-III): Measures independence, out of a total of 100,
in performing activities of daily living.
Spinal cord injury: An injury that damages the spinal cord, due to trauma or disease, and results
in complete or partial paralysis.
Statistical Power: The power of a test is the probability that a given test will find an effect
assuming that one exists in the population.
Square root of the mean squared differences (RMSSD): square root of the mean squared
differences of the consecutive R peak to R peak intervals derived from an
electrocardiogram. A heart rate variability time domain measure that represents cardiac
parasympathetic modulation
Surrogate measure: a measurement taken with the intent to gain insight into a variable that is
either impractical to measure directly, or in principle impossible to measure.
Sympatho-vagal balance: The interaction between the sympathetic and parasympathetic
modulation of the heart.
Tachycardia: Rapid heart rate, usually greater than 100 beats per minute (bpm)
Tetraplegia: complete or partial paralysis of all four limbs due to an injury at the cervical
vertebrae
Traumatic: injury occurred due to physical damage to the spinal cord
Waist circumference (WC): a measure of the distance around the abdomen with the aim to
assess abdominal fat for chronic disease risk such as type 2 diabetes, high cholesterol,
high blood pressure, and heart disease

1
Chapter 1:
1 Introduction
The likelihood of developing cardiac disease is 4.01 times greater in individuals with a spinal
cord injury (SCI) than individuals without a SCI.1 It has been speculated that a possible reason
could be the disruption of the cardiovascular autonomic nervous system (ANS) as evidenced by
the prevalence of autonomic dysreflexia and orthostatic hypotension within the SCI population.1-
5 The underlying physiological mechanisms responsible for the ANS disruptions in SCI have not
yet been fully determined.6 Heart rate variability (HRV) has been reported to non-invasively
measures the modulation of the cardiac ANS and has the potential to assess risk of cardiac
disease.7
Consequently in this study, HRV was assessed to examine the cardiac autonomic
changes in chronic traumatic SCI.
1.1 Spinal cord injury
In 2010, it was reported that around 86, 000 people were living with a SCI in Canada with the
prevalence to increase to 121,000 by 2030.8 Also it was reported that there are around 4,300 new
cases of SCI per year, 42% due to traumatic injuries and 58% due to non-traumatic causes.8
Traumatic SCIs arise due to a physical cause, for instance motor vehicle accidents, falls, or acts
of violence.8 Non-traumatic injuries, on the other hand, occur as a result of diseases, infections or
tumors that disrupt the normal functioning of the spinal cord.8
The cardiac risk factors for non-
traumatic SCI are more challenging to identify than for traumatic SCI since non-traumatic
injuries include tumor-related, congenital/developmental, infectious inflammatory and ischemic
causes.1 In addition, given that most of the SCI studies mainly focus on traumatic injuries,
9 there
is more information available regarding cardiac health within the traumatic group. There are also
demographic differences between the two groups: mean age is higher in the non-traumatic than
in the traumatic group, and although the proportion of females and males is the same in the non-
traumatic group there are three times more males than females in the traumatic group.9
Additionally, there are more incomplete injuries than complete injuries reported within the non-
traumatic group than in the traumatic group.9
There are less secondary complications, such as
spasticity and pressure ulcers, in the non-traumatic group than in the traumatic group.10
Finally,

2
the traumatic group improves with rehabilitation to a greater extent than the non-traumatic
group.9
The spinal cord, which is located within the spinal canal, provides motor and sensory
information between the brain and the body.11-12
In humans, the spinal cord is comprised of 31
segments: 8 cervicali, 12 thoracic, 5 lumbar, 5 sacral and 1 coccygeal.
11 Each segment receives
sensory information from skin areas referred to as dermatomes, and each segment innervates a
group of muscles referred to as a myotome.12
After a SCI, the International Standards for
Neurological and Functional Classification of Spinal Cord Injury (ISNCSCI) are used to
evaluate the neurological level of impairment (NLI) and severity of the injury [American Spinal
Cord Injury Association (ASIA) impairment scale (AIS)] in terms of motor and sensory function
(Appendix A).13-15
AIS is measured by a five point scale (A-E), where A corresponds to a
complete injury (no motor or sensory function in the lowest sacral segments), B-D is an
incomplete injury (motor and/or sensory function preserved below neurological level of injury
and includes sacral segments) and E is normal motor and sensory function.13-14,12
1.1.1 Cardiovascular disease in spinal cord injury
Cardiovascular disease (CVD) has been identified as the leading cause of morbidity and
mortality accounting for approximately 30-50% of deaths within the SCI population; in contrast
to 5-10% in an age and sex matched able-bodied population.2-5,15-16
There is supporting evidence
in the literature indicating that individuals with a SCI are at an increased risk of cardio-metabolic
syndrome (CMS).17-19
CMS is characterized by having three or more of the following five
clinical features: central obesity (waist circumference men>120cm, women>88cm),
hypertriglyceridemia (≥1.7mmol/l), low plasma high density lipoprotein cholesterol
(men<1.03mmol/l, women<1.29mmol/l), hypertension (≥130/85mmHg or on relevant
medications), and fasting hyperglycemia (≥100mg/dl or on relevant medications).18-20
All of the
aforementioned risk factors lead to atherosclerotic plaque formation and earlier onset of CVD.18-
19 In addition, after a SCI, the often sedentary lifestyle, physical deconditioning and inflated
post-injury inflammatory cytokines contribute to the pro-atherogenic outcome and CVD
i The 8
th cervical nerve emerges between the 7
th cervical (C7) and the first thoracic (T1) vertebrae
9

3
development.17-19
As the number of CMS risk factors increases, CVD vulnerability greatly
increases.19
Some of the CMS risk factors overlap with the traditional CVD risk factors such as
sex, age, diabetes, blood lipid profile, elevated systolic blood pressure, smoking status,
sedentary lifestyle, unhealthy diet for example diet high in saturated fats, and obesity.5,21
Also,
investigators have reported that the risk of developing CVD increases with level and severity of
injury i.e. higher and complete injury.16,22
Nevertheless, a recent study by Miyatani et al.23
found
that there was greater arterial stiffness, an emerging indicator of coronary artery disease, in
subjects with paraplegia than tetraplegia. Surprisingly, only 48% of the subjects with arterial
stiffness met the diagnostic criteria for CMS.23
Therefore, the CMS and traditional CVD risk
factors do not completely explain why individuals with a SCI are at such great risk.5
Consequently, there must be additional unexplained factors that contribute to the high prevalence
of CVD within the SCI population. Cardiovascular autonomic disruption is common after a SCI
and the impairment has been reported to increase the risk of developing CVD.2-5
In able-bodied
subjects, a poorly balanced cardiovascular ANS measured via the assessment of vital signs, has
been associated with myocardial infarction, congestive heart failure, life threatening arrhythmias,
and atherosclerotic plaque progression.24
1.1.2 The function of the autonomic nervous system in spinal cord injury
In comparison to studies examining motor and sensory dysfunction post SCI, there are fewer
studies examining disturbances in the ANS.16,25
After a SCI, there is a disruption in the ANS
resulting in abnormal regulation of heart rate, blood pressure, bladder, bowel and temperature
regulation, as well as respiratory and/or sexual dysfunction.6,26
The parasympathetic
preganglionic neurons are situated in the brain stem, specifically in the nuclei of four cranial
nerves: oculomotorius (III), facialis (VII), glossopharyngeus (IX), and vagus (X).5-6,17,27
The
vagus nerve supplies most of the internal organs with the exceptions of the genital organs,
bladder, distal intestine and anus, which are innervated by the parasympathetic sacral (S2-S4)
nerves.5-6,17,28
There is no parasympathetic innervation of the peripheral blood vessels except for
the vessels that supply the pelvic organs.5-6,28
As for the sympathetic preganglionic neurons they
are situated in the grey matter of the spinal column at T1-L2.4-6,26,28

4
With respect to cardiovascular autonomic function, the sympathetic preganglionic neurons at T1-
T5 innervate the heart and the blood vessels of the upper body, while T6-L2 innervate the blood
vessels of the lower body.4-5,11,25-26,29
The parasympathetic innervation of the heart, arises from
the vagal nuclei of the brainstem.4-5,11,25-26,29
Therefore, depending on the level of injury,
sympathetic function may be disrupted resulting in impaired control of heart rate and/or blood
pressure and hypotension and bradycardia are both prevalent after a cervical injury.16-17,25,27
Parasympathetic activity, via beat-to-beat control, decreases heart rate and conversely
sympathetic activity gradually increases heart rate.17,29-30
The level and degree of SCI has been
reported to be directly linked to the extent of cardiovascular autonomic dysfunction.4,16-17,26
For
instance, individuals with a complete cervical injury suffer from an absolute disconnection
between the upper autonomic centres in the brain and the intermediolateral cell column at T1-
L2.17
Early after a SCI, sympathetic activity is quickly disrupted resulting in bradycardia and the vagus
nerve is hypersensitive for at least 2-3 weeks.17
Some treatment approaches that may be required
to maintain an adequate heart rate involve either implanting a temporary pacemaker or
administering atropine which is a competitive muscarinic acetylcholine receptor antagonist.17
Unfortunately, the acute period of cardiac autonomic disruption does not necessarily normalize
and may become a chronic issue, especially among individuals with complete cervical or high
thoracic injuries.5,6,17,25
The disrupted cardiovascular ANS is characterized by a low resting
sympathetic tone and an unaffected resting parasympathetic tone leading to a reduced resting
blood pressure and heart rate and an abnormal cardiovascular response to exercise.26
Furthermore, 91% of individuals with high and complete injuries are more prone to autonomic
dysreflexia (AD) than those with low (below T6) and incomplete injuries (27%).16,26-27
AD arises
from a sensory stimulus below the level of injury and results in episodes of hypertension (20-40
mmHg above baseline) accompanied by a baroreflex mediated bradycardia.5,17,25-26
Similarly,
orthostatic hypotension (OH) is also related to the level and severity of the SCI. The incidence of
OH is as high as 74% in individuals with high (T5 and above) and complete SCI.4,16,25,27
OH is
characterized by a decrease in systolic blood pressure ≥20 mmHg and/or a decrease in diastolic
blood pressure ≥ 10 mmHg from baseline, immediately after transferring from a supine to a
seated position.4-5
The exact mechanisms resulting in both AD and OH are not clearly

5
understood and are probably multifactorial, however the loss of sympathetic control has been
reported to be a predominant factor.4-6
To evaluate autonomic function, a guideline was recently published (2012) outlining the
International Standards to Document Remaining Autonomic Function after Spinal Cord Injury
(ISAFSCI).6 It is recommended to use the guideline in addition to the ISNSCI, and it can be
administered at any time following the injury.6 In the autonomic standards assessment form
(Appendix B), a general description of the remaining autonomic function is recorded for each
system/organ.6 For the urinary tract, bowel and sexual function there is a grading system similar
to the ISNSCI scoring system.6
Also, the assessment form incorporates self-reported history, if
any, regarding the function of the ANS.6 In terms of assessing the cardiovascular ANS, general
autonomic control of the heart is reported as normal, abnormal (bradycardia, tachycardia and/or
any other dysrhythmias), unknown, or unable to assess. Similarly, autonomic control of the
blood pressure, is described as normal, abnormal (resting systolic blood pressure is below 90
mmHg, OH and/or AD), unknown or unable to assess.6 Nonetheless, it is important to consider
that the use of ISAFSCI has not yet been validated.6 In addition, the autonomic assessment,
particularly for the heart, lacks sensitivity and specificity and does not definitively determine the
degree of cardiac autonomic function/dysfunction.
1.2 Heart rate variability
HRV is the most commonly used term to describe the oscillation of the heart rate and is
determined by measuring the peak R to R intervals, also referred to as NN intervals, on an
electrocardiogram (ECG).31
The sinoatrial (SA) node, located in the right atrium of the heart, is
responsible for generating each heartbeat and its firing rate is modulated by the ANS.29-30,32-34
It
has been reported that HRV analysis can non-invasively reflect cardiac regulation via the ANS
which controls heart rate through parasympathetic and sympathetic innervation of the
heart.24,29,33,35-36
Studies have shown that low HRV is an independent predictor of cardiovascular
dysfunction and cardiovascular risk.31,33-34,36-40
Diminished levels of HRV in able-bodied
subjects, have been associated with heart failure,38
diabetes,38,40
hypertension,38,40
abnormal
cholesterol,40
asymptomatic left ventricular dysfunction,38
fatal arrhythmias,41
and death due to
cardiac causes.31

6
HRV standardize guidelines were developed in 1996 by a Task Force composed of members
from the European Society of Cardiology and the North American Society of Pacing and
Electrophysiology.7 Based on the recommended guidelines, there are a number of methods that
can be utilized to measure HRV: 1. Time domain measures- subdivided into statistical measures
and geometric measures; 2. Frequency domain measures; and, 3. Non-linear measures.7 In the
published literature, the two most commonly applied measurement methods for HRV are the
time domain statistical measures and the frequency domain measures (Table 1). Investigators
may have a preference towards these methods since some of the parameters are thought to be
physiological markers and therefore can be used to directly assess sympathetic and
parasympathetic modulation of the heart.
The statistical measures, the square root of the mean squared differences of the consecutive NN
intervals (RMSSD) and the proportion of the number of interval differences of the consecutive
NN intervals greater than 50ms (pNN50), are a reflection of cardiac parasympathetic
modulation.31,35,37
As for the frequency domain measures, the high frequency (HF) component
has been reported to reflect cardiac parasympathetic modulation24,31-32,40-41
while the low
frequency (LF) component is controversial. Some claim that LF is both a marker of
parasympathetic and sympathetic modulation24,31-32,40-41
while others claim that it is more
indicative of sympathetic modulation.2,26,30,33,42-45
Further understanding of the simultaneous
actions of the neurotransmitters on the heart rate may assist in elucidating the physiological
interpretations. The LF:HF has been described as a measure of the sympatho-vagal balance of
the cardiac autonomic nervous system; higher ratio indicating greater sympathetic activity and a
lower ratio indicating lower sympatheticactivity.2,29-30,33,42-44
It is important to note that HRV
measures the modulation of the cardiac ANS rather than the mean level of autonomic activity.2,30
Therefore, comparing HRV, for instance between able-bodied individuals and individuals with a
SCI or pre and post exercise intervention, may be more informative than solely reporting the
value on its own.
The HRV time domain measures are calculated directly from the NN intervals on an ECG,7
while the frequency domain measures are derived using either parametric (e.g. autoregressive
model) or non-parametric [e.g. fast Fourier transform (FFT)] mathematical algorithms.7 The FFT
is the most commonly used and recommended measure as it is simple and quick to apply.7,31,33

7
Using FFT, the NN intervals in the ECG are transformed to provide the amount of variation as a
function of frequency.7,31,33
In the calculated power spectrum, the total power represents the total
variance and each frequency component corresponds to a specific bandwidth7,41
(Table 1). The
frequency components are measured in absolute values of power (ms2).
7
There are currently no widely accepted HRV normative values,37
and this is probably due to the
dynamic nature of the sympatho-vagal system and the intrinsic and/or extrinsic factors that may
influence it.44
The Task Force provided normal HRV values of the frequency measures in
healthy adults extracted from a short term recording. However, a systematic review paper by
Nunan and colleagues37
questions the Task Force’s normal values since they were approximated
from small sample size studies. In comparison with the literature, the Task Force LF and HF
power values were higher; Task Force figures being 1,170ms2 for LF power and 975 ms
2 for HF
power while the literature reported 519 ms2 for LF power and 657 ms
2 for HF power.
37 Also, the
LF:HF ratio reported by the Task Force (1.5-2.0) was lower than the ratio that was extracted
from the literature (2.8).37

8
Table 1. HRV time domain and frequency domain measures*
Time Domain- Statistical Measures Frequency Domain Measures
Statistical variables include:
Standard deviation of the NN interval
(SDNN)
Square root of the mean squared
differences of the consecutive NN
intervals (RMSSD)
Number of the interval differences of
the consecutive NN intervals greater
than 50ms (NN50)
Proportion of the NN50 (pNN50) which
is calculated by dividing the NN50 by
the total number of NN intervals
Frequency variables include:
Ultra low frequency (ULF)
Bandwidth: below 0.0033 Hz
Very low frequency (VLF)
Bandwidth: 0.0033-0.04 Hz
Low frequency (LF)
Bandwidth: 0.04-0.15 Hz
High frequency (HF)
Bandwidth: 0.15-0.40 Hz
* Table was developed using the Task Force guidelines.7
1.3 Literature review
1.3.1 The findings on heart rate variability in spinal cord injury
Assessing HRV in SCI is valuable as it can quantify the extent of cardiac autonomic dysfunction
that is distinctively experienced by each individual, and can be regularly used to evaluate and
monitor changes in a clinical setting over time.2,29,42
Unlike HRV analysis, most ANS
measurement tools are invasive and/or require specialized expertise and equipment making it
difficult to assess routinely in a clinical setting; for instance administering a sympathetic skin
response testii or measuring resting plasma catecholamine concentrations.
2,4,16 HRV analysis is
currently the only assessment tool that solely examines cardiac autonomic modulation in SCI.
ii Sympathetic skin response involves the momentary change of the electrical potential of the skin with the aim to
assess sympathetic function. The response may be either spontaneously or reflexively induced by applying an
internal or external arousal stimulus46

9
The psychometric properties of measuring HRV have been minimally studied, but HRV analysis
in SCI has been shown previously to be a reproducible measure (LF:HF and LF, intraclass
correlation coefficient (R)=0.82-0.88; HF, R=0.53).47
Additionally, Claydon and colleagues2
revealed that the HRV frequency indices (HF, LF, LF:HF), measured in the supine position,
correlated with clinical measures of the cardiovascular autonomic function including sympathetic
skin response, orthostatic cardiovascular response, and plasma catecholamine levels.
A number of studies have used time domain measures to assess HRV in chronic SCI. Bunten and
colleagues42
did not observe any differences in the time domain measures between the complete
and incomplete cervical SCI, thoracic (T1-L5) SCI and able-bodied subjects. As well, Wang and
colleagues29
reported no differences in RMSSD and pNN50 when comparing complete cervical
injuries against complete low thoracic injuries (T10-L2). Provided that the cardiac
parasympathetic innervations remain intact after a SCI, the investigators expected that the
parasympathetic time domain markers would not be disrupted.42
Bunten and colleagues42
explain
that there is parasympathetic predominance, but without an increase in parasympathetic activity.
However, Rosado-Rivera and colleagues15
reported that the low paraplegia group (T7-T12)
displayed lower RMSSD values compared to able-bodied, high paraplegia (T2-T5) and
tetraplegia (C4-C8) groups. Therefore, as expected, the low paraplegia group displayed the
highest mean heart rate (83±12bpm) and mean heart rate was significantly higher than the able-
bodied (70±9bpm) group and the tetraplegiac group (69±10bpm).15
Frequency domain measures have also been used to evaluate HRV in chronic SCI. A study by
Claydon and colleagues2 showed that individuals with complete and incomplete cervical SCIs
displayed lower LF values, in comparison to thoracic (T2-T11) SCI and able-bodied subjects.
The reduced LF in individuals with SCI is most likely due to the loss of sympathetic control.2,42
Similarly, Wang and colleagues29
reported low LF values in individuals with complete cervical
injuries versus those with complete thoracic (T10-L1) injuries. Individuals with incomplete
cervical injuries had greater LF values than those with complete cervical injuries given that there
was less damage to the descending sympathetic pathways.30,42
They also showed that the LF
power in the thoracic group was similar to the controls indicating undisrupted sympathetic
cardiac autonomic control. However, when examined per case, the two subjects with high
thoracic SCI (above T5) displayed lower LF values than the controls.2 On the contrary; the study

10
by Bunten and colleagues42
found that both the thoracic group (T1-L5) and cervical group had
lower LF values than the able-bodied subjects. Similarly, Castiglioni et al.48
reported reduced LF
values in the thoracic group (T5-L4) with respect to the able-bodied group.
As for the HF component, the results by Claydon et al.2 revealed that it was higher in the
complete and incomplete cervical group than in the thoracic SCI and control group. The increase
in vagal tone explained the presence of bradycardia within the cervical group.2,49-50
In addition,
the lower LF:HF outcome in the cervical group compared to the thoracic group and the control
group further suggests that there is parasympathetic predominance after a cervical SCI.2,42
However, Grimm and colleagues30
found that individuals with a complete cervical injury had
lower HF values than those with an incomplete cervical injury, thoracic (below T7) injury and
able-bodied individuals. Wang et al.29
also reported lower HF in a cervical group when
compared to a thoracic group (T10-L1). Both Wang et al.29
and Grimm et al.30
found no
differences in the LF:HF between the cervical and thoracic injuries. They suggested that the lack
of difference in LF:HF indicated that the cardiac ANS was trying to maintain sympatho-vagal
homeostasis.29-30
The study by Bunten and colleagues,42
on the other hand, found no differences
in the HF component between the three groups indicating normal resting vagal tone. In the
thoracic group (T2-T11), Claydon et al.2 found that the HF was lower, and LF:HF was higher
than that observed in the able-bodied group. In addition, Rosado-Rivera et al.15
suggested that a
reduced HF and higher LF:HF is a possible explanation for the prevalence of elevated heart rates
among individuals with high and low paraplegia. Unfortunately, it is unclear why vagal tone is
reduced but some have hypothesized that it could be a compensatory reduction with the aim to
maintain sympatho-vagal balance2,15,29-30
or be due to cardiovascular deconditioning.15
Castiglioni and colleagues,48
on the contrary, reported no differences in the HF values and
LF:HF between the able-bodied and thoracic group (T5-L4). The reasons for the HRV
discrepancies reported in the literature are still uncertain, however, there are a number of factors,
including the experimental paradigm used for ECG collection that could have a major influence.
1.3.2 Factors affecting heart rate variability
The relationship between HRV and potential influencing factors has been examined in previous
literature. Factors including age, sex, obesity, fitness level, sleep apnea, emotional state, and

11
smoking status have all been confirmed (Table 2). There is a well-established relationship
between age and HRV, with younger individuals showing higher HRV.32,37,40
The decrease of
HRV with increasing age could be due to the reduction of both parasympathetic and sympathetic
activity.33
The relationship between sex and HRV remains unclear. A review by Nunan and
colleagues37
found that the chosen unit of measurement influenced the relationship between sex
and HRV. There is a confirmed link between ANS dysfunction and obesity40,51
as Alrefaie et
al.52
and Mehta et al.53
found a relationship between body mass index (BMI) and HRV while
Farah et al.54
reported a negative correlation between waist circumference and HRV, but no
relationship between BMI and HRV. Farah et al.54
argue that central obesity measured via waist
circumference is a better indicator of cardiac autonomic dysfunction than general obesity
measured by BMI.54
Melanson and colleagues55
examined the effect of endurance training on
HRV in previously sedentary subjects and found that engaging in regular physical activity
increased HRV. As for sleep apnea, Flevari et al.56
hypothesized that sleep disordered breathing
increased autonomic tone. Also, Chalmers and colleagues57
conducted a meta-analysis and found
reduced HRV in individuals with anxiety disorders. Finally, Lee et al.58
reported that smoking
decreases cardiac parasympathetic activity and increases sympathetic function.
Table 2. Factors reported to influence HRV
Factors Influence on HRV
Age Negative relationship between age and
HRV
Sex Females displayed lower time domain
measures than males (8-11% lower)
LF and HF lower in males when expressed
in absolute units (ms2) (14% and 8% lower
than females, respectively)
When the units were normalized, LF was
higher in males (17% higher than females)
and HF was comparable
When expressed in log units, females had
20% lower LF, and 18% lower HF than
males
LF:HF lower in females than males
regardless of the measurement unit

12
Obesity Individuals with body mass index greater
than or equal to 30 kg/m2 had lower
RMSSD, HF and LF but similar LF:HF in
comparison to non-obese control group
Negative correlation between waist
circumference and RMSSD (r2=0.15) and
PNN50 (r2=0.16)
Fitness level RMSSD and HF increased above baseline
after 12 weeks of moderate-vigorous
intensity exercise
Sleep apnea Constant HF but higher RMSSD, pNN50,
LF, and LF:HF in patients with positional
obstructive sleep apnea
Emotional state People with panic disorder, post-traumatic
stress disorder, generalized anxiety
disorder, social anxiety disorder all showed
lower HF values relative to the control
group
Smoking status Smokers had lower HF and higher LF and
LF:HF than non-smokers
RMSSD the same in smokers and non-
smokers
1.4 Study rationale
The combination of an increased risk of cardio-metabolic syndrome, physical deconditioning,
increase in inflammatory cytokines, cardiac autonomic dysfunction, and barriers to a physically
active lifestyle all lead to an increased risk of developing CVD after a SCI (Figure 1). The
currently available autonomic evaluation guidelines, unlike HRV, provide general information
regarding cardiac ANS activity but do not measure the extent of cardiac autonomic dysfunction.
Since the degree of cardiac autonomic dysfunction in SCI depends on the neurological level of
impairment and severity of injury, resting HRV measures may vary accordingly.
Parasympathetic innervation of the heart is still intact after a SCI, as it arises from the brainstem,
and therefore cardiac autonomic function is thought to be disrupted due to sympathetic damage
(Figure 2). Given the location of sympathetic innervation [T1-T4(T5)], HRV is expected to be
disrupted in individuals with a SCI above the level of T5 and the degree of disruption is expected
to be greater in complete injuries. Unfortunately, due to the few studies in SCI and the

13
inconsistent HRV findings, the relationship between HRV and SCI remains unclear. The
limitations of current literature are: small sample size, combining different etiology of SCI,
and/or cohort selection (discrepancies in neurological level of impairment). Consequently, the
cardiac autonomic changes contributing to ANS dysfunction in SCI, as measured via HRV, are
yet to be fully determined. In this thesis, resting supine HRV was examined in a large and
representative sample of chronic traumatic SCI while still considering autonomic innervations
based on the anatomy of the cardiac ANS. Chronic SCI, as opposed to acute or sub-acute, is
considered to be a stable state and as a result is the ideal phase to study the adaptive state of ANS
in individuals with a SCI.3 Also, given that there are important etiological, comorbidities and
demographic differences between traumatic and non-traumatic SCI it was decided to examine
HRV and influencing factors in traumatic SCI only.
Figure 1. Possible contributors to greater CVD risk in individuals with SCI. The theoretical
framework summarizes the relationship between SCI and CVD. After a SCI, increased risk of
cardio-metabolic syndrome, elevated levels of inflammatory cytokines, lifestyle changes,
disrupted ANS, and some non-modifiable factors all contribute to overall CVD development
(modified from Figure 1.0 on page 128 in the Rehabilitation Environmental Scan Atlas:
Capturing Capacity in Canadian SCI Rehabilitation.59
)

14
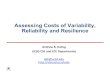
Figure 2. Parasympathetic and sympathetic innervations of the heart and peripheral
muscles. Sympathetic innervations arise from T1-T4/T5 cord segments. Consequently, level of
injury may affect cardiac autonomic function as measured by HRV.

15
Chapter 2:
2 Objectives and Hypothesis
2.1 Objectives
2.1.1 Primary Objective
To describe the distribution of HRV indices in a population of individuals with a chronic
traumatic SCI.
Primary HRV index: Low frequency to high frequency ratio (LF:HF).
Secondary HRV indices: Low frequency (LF), high frequency (HF), square root of the
mean squared differences of the consecutive NN intervals (RMSSD), and proportion of
the NN50 (pNN50) which is the percentage of pairs of adjacent NN intervals differing by
more than 50ms.
2.1.2 Secondary Objective
a) To determine whether there is a difference in HRV indices (primary and secondary)
based on level of injury (above T5 and below T5).
b) To determine whether there is a difference in HRV indices (primary and secondary)
based on severity of injury (complete injury and incomplete injury).
c) To determine whether there is a difference in HRV indices (primary and secondary)
based on level and severity of injury (complete and equal to/above T5, complete and
below T5, incomplete and equal to/above T5, and incomplete and below T5).
d) To determine whether there are any differences in the selected HRV-related factors based
on level and/or severity of injury. The selected HRV-related factors are: age, sex, body
mass index (BMI), waist circumference (WC), time post injury, current smoking status,
smoking history, cardiorespiratory fitness level (absolute VO2 peak, relative VO2 peak,
peak heart rate), leisure time physical activity questionnaire-spinal cord injury (LTPAQ-

16
SCI), lower extremity motor score (LEMS), spinal cord independence measure (SCIM-
III), number of co-morbidities, family history of heart disease and sleep apnea.
2.1.3 Tertiary Objective
a) To determine whether there is a relationship between low frequency (LF) and high
frequency (HF) indices in chronic traumatic SCI.
b) To determine whether there is a relationship between LF, HF, LF:HF and HRV related
factors in chronic traumatic SCI: age, BMI, WC, time post injury, cardiorespiratory
fitness level (absolute VO2 peak, relative VO2 peak, peak heart rate), LTPAQ-SCI,
LEMS, SCIM-III, and number of co-morbidities.
c) To determine whether there is a relationship between age, waist circumference and peak
heart rate and the LF or HF indices in the entire study sample and in individuals with a
complete injury that is equal to/above T5.
d) To determine whether there is a relationship between LF, HF, age at injury and resting
systolic blood pressure in the entire study sample and in individuals with a complete
injury that is equal to/above T5.
2.2 Hypothesis
2.2.1 Primary Hypothesis
There will be a multimodal distribution of the HRV indices based on level and severity of injury.
2.2.2 Secondary Hypothesis
a) Individuals with an injury equal to or above T5 will display lower HRV values than those
with an injury below T5.
b) Individuals with a complete injury will display lower HRV values than those with an
incomplete injury.

17
c) Individuals with a complete injury equal to or above T5 will display the lowest HRV
values. Alternately, individuals with an incomplete injury below T5 will display the
highest HRV values indicating an undisrupted cardiac ANS.
d) Age, sex, time post injury, current smoking status, smoking history, and family history of
heart disease do not depend on the level or severity of injury and thus will not show any
differences across the cohorts. However, BMI, WC, number of co-morbidities and
presence of sleep apnea will be greater in individuals with a higher level of injury and/or
a complete injury. On the contrary, cardiorespiratory fitness level, LTPAQ-SCI, LEMS,
and SCIM-III will be lower in individuals with a higher level of injury and/or a complete
injury.
2.2.3 Tertiary Hypothesis
a) The LF and HF indices will display a high positive linear relationship since the role of the
ANS is to maintain homeostasis
b) Both LF and the LF:HF will display a positive linear relationship with age, BMI, WC,
time post injury and number of co-morbidities and a negative linear relationship with
cardiorespiratory fitness level (absolute VO2 peak, relative VO2 peak and peak heart
rate), LTPAQ-SCI, LEMS, and SCIM-III. HF will display a negative linear relationship
with age, BMI, WC, time post injury and number of co-morbidities and a positive linear
relationship with cardiorespiratory fitness level, LTPAQ-SCI, LEMS, and SCIM-III.
c) Age, WC and peak heart will predict LF and HF indices in the entire sample and in
individuals with an injury equal to/above T5.
d) In the entire sample and in individuals with an injury equal to/above T5: There will be a
positive linear relationship between LF and age at injury and resting systolic blood
pressure. Whereas there will be negative linear relationship between HF and age at injury
and resting systolic blood pressure.

18
Chapter 3:
3 Methodology
3.1 Overview
This study was a secondary data analysis of a primary data set from a recently published study
that explored the associations between arterial stiffness and spinal cord impairment.23
The
inclusion criteria of the primary study were English speaking subjects between 18-80 years of
age living in the Greater Toronto Area with a chronic SCI (C1-T12, AIS A-D, ≥2 years post
impairment) of traumatic and non-traumatic etiology.23
The exclusion criteria, of the primary
study, consisted of any subjects with a previous or current history of: angina, myocardial
infarction, atypical chest pain, coronary artery bypass or revascularization, aortic stenosis,
uncontrolled arrhythmia or left bundle branch block, hypertrophic cardiomyopathy, severe
chronic obstructive pulmonary disease requiring oral steroids or home oxygen, diaphragmatic
pacer, and stroke.23
The subjects underwent medical screening, electrocardiogram, and chart
review to ensure that they met the inclusion and exclusion criteria.23
Overall, out of the 125
subjects who were screened, 100 consented to participate, 10 withdrew their consent, and three
did not meet the inclusion criteria and thus a total final sample of 87 subjects met the inclusion
criteria23
; 75 subjects had ECG data collected. Both primary and secondary studies were
approved by the University Health Network Research Ethics Board (REB#:09-019-DE) and the
secondary study was also approved by the University of Toronto Office of Research Ethics
(REB#:30133).
HRV, as measured via ECG, was collected in accordance with the Task Forceiii
guidelines.
Subjects were asked to abstain from caffeine and nicotine, and fast for at least 8 hours prior to
the ECG collection session. The subjects were also instructed to refrain from exercise 24 hours
prior to the session. The ECG data were collected between 9:00am-1:00pm. The subject was
transferred to a supine position onto a bed, in a quiet and temperature controlled (24◦C) room and
iii European Society of Cardiology and the North American Society of Pacing and Electrophysiology Task Force
HRV guidelines developed in 1996

19
allowed to rest for 20 minutes before collecting continuous 3-lead ECG (lead II system) for ten
minutes, at a sampling rate of 1000Hz (PowerLab/16SP; AD instruments, Inc., Bella Vista,
Australia).23
3.2 Study variables
3.2.1 Heart rate variability indices and related factors
Five HRV indices were selected based on the literature findings: LF:HF (primary index), LF,
HF, RMSSD and pNN50.
In addition to collecting ECG, the demographics and health status of each subject were also
recorded in the primary study. Variables that were hypothesized to have an influence on HRV
were included in this study (see Table 3).
Table 3. Potential HRV-related variables selected from the primary data
Construct of interest Measurement Method
SCI impairments Time post injury (years), neurological level of
injury, severity of injury (complete or
incomplete), and etiology of injury (traumatic
or non-traumatic)
Age Age (years)
Sex Sex (male/female)
Medications Beta blockers, calcium channel blockers and
any other cardiac rhythm drugs
Obesity BMI (kg/m2) and WC (cm)
Smoking status Current smoking status and smoking history
(yes/no)

20
Family history of heart disease Family history of heart disease (yes/no)
Sleep deprivation Sleep apnea (yes/no)
Cardiorespiratory fitness Absolute VO2 peak (L/min), Relative VO2
peak (ml/kg/min) and peak heart rate (bpm)
Physical status Self-reported physical activity: LTPAQ-SCI
(min/week)
Self-reported independence in ADL’s: SCIM-
III (/100)
Measured motor impairment: LEMS (/50)
Chronic disease Number of co-morbidities (/7)
Abbreviations: BMI, body mass index; WC, waist circumference; LTPAQ-SCI, leisure time
physical activity questionnaire; ADLs, activities of daily living; SCIM-III, spinal cord
independence measure; LEMS, lower extremity motor score
3.3 Subject selection.
3.3.1 Electrocardiogram recordings
All of the ECG recordings were reviewed visually with the assistance of an internist with
expertise in cardiovascular stress testing and ECG monitoring (Dr. P. Oh). For each subject, the
rate and rhythm (normal sinus rhythm, bradycardia, or tachycardia), presence of premature atrial
and/or ventricular contractions, electrical artifact and visual variability observed in the RR
intervals were reviewed. If the subject displayed frequent premature contractions (greater than
ten per minute), arrhythmias, or excessive artifact that prevented the proper analysis of the RR
intervals, they were excluded from the dataset for detailed analysis.
3.3.2 Medications
Medications were reviewed in consultation with a physiatrist (Dr. C. Craven) and internist (Dr.
Oh). Subjects taking medications which could have an influence on HRV (beta blockers, calcium

21
channel blockers that influence cardiac conductioniv
such as diltiazem and verapamil, and any
other cardiac anti-arrhythmic drugs such as amiodarone, procainanmide, encainide and
flecainide) were excluded from the study.
3.4 Heart rate variability analysis
HRV analysis was conducted using LabChart
(version 7.0). According to the Task Force, the
gold standard for HRV short term recording analysis is a five minute interval. Therefore, the ten
minutes of ECG were divided into three segments of five continuous minutes; first five minutes
(t=0 - t=300 seconds), middle five minutes (t=150 - t=450 seconds) and last five minutes (t=300
- t=600 seconds) with the aim to select the segment with the least noise interference. Each five
minute ECG recording was then reviewed to confirm that all and only the R peaks were marked
(Figure 3a). The Poincaré Plotv was checked to examine the normal and ectopic
vi RR interval
ranges (Figure 3b) and to detect any ectopic islandsvii
. Physiologically, “ectopic” indicates any
cardiac activity not originating from the SA node.60
Ectopic islands were detected in 26.79% of
the subjects and occurred mainly due to technical error or unknown causes. The details of the
ectopic islands per subject are summarized in Appendix C. To omit ectopic islands, according to
the noise-omitting method of Young and colleagues,61
the data was filtered with a 45Hz low pass
filter (Figure 4). The following post-filtered variables were recorded for the three segments:
average heart rate, SDNN, SDANN, RMSSD, NN50, pNN50, total power, VLF, LF, HF, LF:HF,
and noise/ectopic/artifact percentages. After analyzing all three ECG segments, the segments for
each subject with the highest percentage of normal i.e. lowest percentage of ectopic beats, was
included in the analysis. If the percentage of normal and ectopic beats were equal in all three
segments for a particular subject, then a segment was randomly chosen using a computer-based
randomizer (http://www.random.org/). If only the ectopic beats were all equal (0%) then the
highest percentage of normal was chosen (the one closest to 100%).
ivAny calcium channel blocker ending with “ine” only influences blood pressure for example amlodipine and
nifedipine; they decrease blood pressure, but do not affect heart rate v The Poincaré Plot is a LabChart
software feature used to assess the lengths of the RR intervals by plotting the
length of each RR interval against the length of the following RR interval vi
Defined as “ectopic” by the LabChart
program vii
The term “ectopic islands” refers to the clustering of certain data points

22
Figure 3. Representative example of HRV analysis using LabChart
(v.7.0). a. The threshold
was set and the R peaks were determined. The RR intervals are also referred to as NN intervals.
b. The Poincaré Plot was used to examine the lengths of the RR intervals. The interval ranges
indicates whether each RR interval is within the normal or ectopic range.
a)
b)

23
Figure 4. Representative example of Poincaré Plot before and after the application of 45Hz
low pass filter. The arrows in the first diagram indicate two clusters of data, referred to as
ectopic islands. After the filter was applied, the ectopic islands were removed and the noise in
the data was reduced from 9.2 % to 0%.

24
3.5 Statistical Analysis
Statistical analysis was conducted using IBM SPSS Statistics v.22 and is described per study
objective. If the data were not normally distributed a median was reported and if the data were
normally distributed a mean was reported.
3.5.1 Objective 1: Heart rate variability frequency distributions
To describe the distribution of HRV in chronic and traumatic SCI, descriptive statistics were
reported [mean and standard deviation or median and interquartile range (IQR)]. The frequency
distributions, for each HRV index, were also plotted and the distribution was described using
skewness and kurtosis. To assess whether the data were normally distributed, a Kolmogorov-
Smirnov (K-S) test was administered and boxplots were checked for major outliers (a minor
outlier was defined as 1.5xInterquartile range (IQR) outside the central box and a major outlier
as 3.0xIQR outside the central box). If K-S p>0.05 and there were no major outliers in the
boxplots, then the data were considered normally distributed. Furthermore, if the primary HRV
index (LF:HF) displayed any outliers, the characteristics of the subjects who were outliers were
examined with the aim to postulate possible reasons.
3.5.2 Objective 2: Comparison of heart rate variability based on level and/or severity of injury
HRV parameters and the HRV-related factors were compared between: a. Level of injury (below
versus above T5), b. Severity of injury (complete versus incomplete) and c. Level and severity of
injury. For normally distributed data, an independent t-test or ANOVA was administered. For
non-normally distributed data, a Mann-Whitney or Kruskal-Wallis test was used to compare
across cohorts. Following ANOVA or Kruskal-Wallis, if there was a significant difference a
post-hoc test was administered and was adjusted for multiple comparisons. Furthermore, if the
primary HRV index (LF:HF) displayed any outliers, the data was examined to ensure that the
outliers were not responsible for the results observed. For the categorical HRV-related factors, if
in the chi square output the expected frequencies in each cell was greater than five then a
Pearson Chi-Square test was used, if less than five then a Fisher’s exact test was chosen. An
alpha of 0.05 was set as the level of significance.

25
3.5.3 Objective 3: Assessing the LF and HF indices
The relationship between the LF and HF indices was examined using Spearman’s rho correlation
co-efficient for the entire sample and per cohorts (level and/or severity of injury). For the entire
sample, Spearman’s was also used in order to determine whether there is a relationship between
LF, HF, LF:HF and the scalar HRV-related factors. The relationship between LF, HF, age at
injury and resting systolic blood pressure was assessed using Spearman’s for the entire sample
and in the cohort considered to be the most vulnerable to CVD (complete and equal to/above
T5). The strength of each relationship was assessed using the following descriptors: r=0.0-0.25
little or no relationship, r=0.26-0.50 fair relationship, r=0.50-0.75 moderate to good relationship,
and r>0.75 good to excellent relationship.62
A multiple linear regression analysis was used to
examine the relationship of CVD risk factors (age, waist circumference and peak heart) and the
LF and HF indices. The relationship was assessed for the entire sample and in the cohort most
vulnerable to CVD (complete and equal to/above T5). If the assumption of linearity and
normality were not met, bootstrapping was conducted. An alpha of 0.05 was set as the level of
significance.

26
Chapter 4:
4 Results
4.1 Subject selection
The primary data set consisted of 75 subjects with non-traumatic and traumatic injuries. The
non-traumatic subjects (n=13) were excluded from the data set based on etiology of injury. After
the resting ECG was reviewed for each subject, three subjects were excluded: Two subjects
displayed frequent premature ventricular contractions (PVCs ≥10/min) and one due to technical
difficulties with ECG data collection. In addition, three subjects were excluded based on the
medications reported: Two subjects were on beta blockers, and one subject was taking both a
beta-blocker and a calcium channel blocker diltiazem (Tiazac XL) which decreases heart rate.
The final sample size included a total of 56 subjects which were then further subdivided based on
level and severity of injury (Figure 5). The characteristics of the participants are summarized in
Table 4.

27
Figure 5. CONSORT flowchart reflecting the inclusion and exclusion of the final data
sample. A total of 56 subjects were included for analysis.
Assessed for eligibility (N=75)
Analyzed (N=56)
Complete and equal to or above
T5
(N=27)
Complete and below T5
(N=11)
Incomplete and equal to or above
T5
(N=10)
Incomplete and below T5
(N=8)
Excluded (N=19)
- Non-traumatic SCI (N=13)
- ECG: PVCs≥10/min (N=2); Technical error (N=1)
- Medications: β-blockers (N=2); β-blocker and Ca2+ channel blocker (N=1)

28
Table 4. Demographics and vital signs of the participants in total sample and per cohort
Total
Sample
Complete and
equal to/above
T5
Complete and
below T5
Incomplete
and equal
to/above T5
Incomplete
and below T5
N 56 27 11 10 8
Age (years) 46.75±12.44 46.30 ±10.59 44.45 ±15.01 53.40 ±12.17 43.13 ±14.12
Time post injury
(years)
14.23±9.86 17.26±10.16 16.55±9.54 9.10±7.40 7.25±6.48
Sex
(males/females)
44/12 22/5 9/2 8/2 5/3
BMI (kg/m2) 26.13±4.84 25.34±4.54 25.73±4.30 28.44±6.91 26.48±3.11
WC (cm) 95.65±14.56 94.60±14.89 96.56±14.63 97.37±18.19 95.81±10.05
HR (bpm) 61.67±8.98 59.41±7.54 65.71±9.98 60.52±9.72 65.52±7.07
SBP (mmHg) 109.77±16.8
6
101.19±12.17 114.73±17.05 113.00±16.42 127.88±14.51
DBP (mmHg) 71.38±13.08 64.63±10.46 78.00±12.62 74.00±10.87 81.75±13.47
All values are mean ± standard deviation or as otherwise indicated
Abbreviations: BMI, body mass index; WC, waist circumference; HR, heart rate; SBP, systolic
blood pressure; DBP, diastolic blood pressure
4.2 Frequency distributions of the heart rate variability indices
Table 5 summarizes the LF:HF descriptive statistics for the entire sample. The frequency
distribution was positively skewed and leptokurtic indicating that the values cluster at the lower
end and it is a pointy and heavy-tailed distribution (Figure 6). The results showed that the data
were significantly different than a normal distribution as K-S p<0.001 and there were major
outliers present in the boxplot (two major and two minor) (Figure 7). The characteristics of the

29
subjects who were outliers are summarized in Appendix D, Table 1. To further examine the
influence of outliers, they were removed and the data were reassessed for normality [N=52,
Mdn=1.08(0.59, 2.45), IQR=1.86]. The frequency distribution of the LF:HF without the outliers
is in Appendix D, Figure 1. The data were still not normally distributed since K-S test p=0.002,
however, the distribution became less positively skewed (+1.13) and leptokurtic (+0.57). The
descriptive statistics of the secondary HRV indices (LF, HF, RMSSD, pNN50) are summarized
in Table 5, and none of the indices were normally distributed. The frequency distributions and
the boxplots for each HRV index are in Appendix E. The LF, HF, and RMSSD distributions
were positively skewed and leptokurtic, whereas the distribution of pNN50 was positively
skewed and platykurtic. The boxplots displayed: Five minor outliers in LF, three major and two
minor outliers in HF, three minor outliers in RMSSD, and none in pNN50. The descriptive
statistics for total power can be found in Appendix F, Table 1.
Table 5. Descriptive statistics for each HRV index in the entire sample (N=56)
LF:HF LF HF RMSSD pNN50
Median
(Lower,
Upper
quartile)
1.21
(0.63,2.85)
460.20 ms2
(207.73,1266.33)
362.32 ms2
(143.69,1086.72)
35.75 ms
(20.03,59.03)
6.62%
(1.23,23.35)
IQR 2.22 1058.60 ms2 943.03 ms
2 39.00 ms 22.12%
Skewness +2.70 +1.68 +2.29 +1.73 +1.02
Kurtosis +8.45 +2.13 +5.16 +3.39 -0.08
p-value† p<0.001* p<0.001* p<0.001* p=0.007* p<0.001*
†Kolmogorov-Smirnov (K-S) test; p≤0.05*
Abbreviations: LF:HF, low frequency to high frequency ratio; LF, low frequency; HF, high
frequency, RMSSD, square root of the mean squared differences of the consecutive NN
intervals, pNN50, proportion of the number of interval differences of the consecutive NN
intervals greater than 50ms; IQR, interquartile range

30
Figure 6. Frequency distribution of LF:HF. The data was positively skewed (+2.70) and
leptokurtic (+8.45).
Figure 7. Boxplot representing LF:HF distribution. The asterisks represent major outliers
(3.0xIQR outside the central box) and the circles represent minor outliers (1.5x IQR outside the
central box).

31
4.3 Heart rate variability comparisons across level and/or severity of injury
The HRV indices were compared between two cohorts: Level of injury (above versus below T5)
and severity of injury (complete versus incomplete injury). None of the HRV indices differed
based on level of injury (Table 6) or severity of injury (Table 7). The comparisons of total
power can be found in Appendix F, Tables 2 and 3.
Table 6. Comparison of HRV indices based on level of injury
Median (Lower, Upper quartile)
HRV Index Below T5
(N=19)
Above/Equal to
T5 (N=37)
p –Value†
LF:HF 1.54 (0.76,3.32) 1.10 (0.60,2.71) 0.431
LF (ms2) 667.88
(209.71,1945.83)
330.22
(187.32,330.22)
0.210
HF (ms2) 436.29
(177.26,1173.55)
354.27
(133.73,883.00)
0.869
RMSSD (ms) 34.58
(21.45,61.54)
39.16
(19.48,58.94)
0.869
pNN50 (%) 8.08
(1.49,26.64)
5.24
(1.13,23.07)
0.883
†Mann-Whitney test; p≤0.05*
Abbreviations: LF:HF, low frequency to high frequency ratio; LF, low frequency; HF, high
frequency, RMSSD, square root of the mean squared differences of the consecutive NN
intervals, pNN50, proportion of the number of interval differences of the consecutive NN
intervals greater than 50ms

32
Table 7. Comparison of HRV indices based on severity of injury
Median (Lower, Upper quartile) or
Mean ± Standard deviation
HRV Index Complete
(N=38)
Incomplete
(N=18)
p –Value
LF:HF 1.60 (0.69,3.06) 0.96 (0.47,1.76) 0.150†
LF (ms2) 460.20
(223.75,1075.85)
351.74
(104.85,2724.76)
0.902†
HF (ms2) 362.32
(139.41,876.10)
390.06
(127.68,2026.22)
0.461†
RMSSD (ms) 38.91 ±25.28 58.77 ±46.95 0.107§
pNN50 (%) 5.00 (1.14,22.10) 8.31 (1.78,26.95) 0.680†
†Mann-Whitney test;
§ Independent t-test; p≤0.05*
Abbreviations: LF:HF, low frequency to high frequency ratio; LF, low frequency; HF, high
frequency, RMSSD, square root of the mean squared differences of the consecutive NN
intervals, pNN50, proportion of the number of interval differences of the consecutive NN
intervals greater than 50ms
Similarly, when examined across the four cohorts, based on level and severity of injury, none of
the HRV indices were significantly different (Table 8). The comparisons in total power can be
found in Appendix F, Table 4. To examine the influence of the outliers in LF:HF (the primary
HRV index) a boxplot with and without the outliers was examined (Figure 8) and the new values
were re-tested for comparisons. There were still no differences across the cohorts (p=0.133)
when the outliers were omitted. The characteristics of the subjects who were the initial outliers
can be found in Appendix D, Table 1. Refer to Appendix G to see the boxplots across level and
severity of injury for each HRV index.

33
Table 8. Comparison of HRV indices based on level and severity of injury
Median (Lower, Upper quartile) or Mean ± Standard deviation
HRV
Index
Complete and
equal to/above
T5 (N=27)
Complete and
below T5
(N=11)
Incomplete and
equal to/above
T5 (N=10)
Incomplete and
below T5 (N=8)
p –Value
LF:HF 1.10
(0.55,2.91)
2.48
(1.51,4.84)
1.16
(0.72,1.93)
0.62
(0.35,2.00)
0.070†
LF
(ms2)
330.22
(207.07,741.10)
667.88
(455.41,1945.83)
351.74
(102.30,2810.39)
463.81
(122.14,2483.00)
0.379†
HF
(ms2)
370.37
(124.05,879.65)
295.37
(177.26,660.09)
284.53
(125.28,2321.10)
794.90
(144.60,2661.62)
0.816†
RMSSD
(ms)
40.36 ±27.92 35.38 ±17.88 65.60±55.62 50.22 ±35.00 0.373§
(Welch)
0.264§
(Brown-
Forsythe)
pNN50
(%)
4.76
(1.11,22.50)
7.91
(1.49,15.43)
6.94
(1.78,24.70)
11.73
(0.86,28.12)
0.980†
†Kruskal-Wallis test;
§One way ANOVA test; p≤0.05*
Abbreviations: LF:HF, low frequency to high frequency ratio; LF, low frequency; HF, high
frequency, RMSSD, square root of the mean squared differences of the consecutive NN
intervals, pNN50, proportion of the number of interval differences of the consecutive NN
intervals greater than 50ms

34
Figure 8. Boxplot representation, with and without the outliers, of LF:HF based on level and severity of SCI. For each color-coded
cohort there are two boxplots, the darker shaded boxes represent data with the outliers while the lighter shaded boxes represent the data
after the initial outliers were omitted. The outlier numbers correspond with the subject numbers.

35
4.3.1 Comparison of heart rate variability related factors across cohorts
SCIM-III (p=0.036), relative VO2 peak (p=0.038) and peak heart rate (p=0.033) were all greater
in individuals with an injury below T5. However, time post injury (p=0.501), BMI (p=0.883),
LTPAQ-SCI (p=0.668), LEMS (p=0.111), number of co-morbidities (p=0.179), age (p=0.221),
waist circumference (p=0.830) and absolute VO2 peak (p=0.088) were all similar. The medians
or means for each factor are summarized in Appendix H, Table 1.
Time post injury (p=0.001) was greater in individuals with a complete injury, whereas LEMS
(p<0.0001) and SCIM-III (p=0.003) were greater in the incomplete cohort. BMI (p=0.352),
LTPAQ-SCI (p=0.106), number of co-morbidities (p=0.622), age (p=0.393), waist circumference
(p=0.720), relative VO2 peak (p=0.496), absolute VO2 peak (p=0.232) and peak heart rate
(p=0.705), were all the similar. The medians or means for each factor are summarized in
Appendix H, Table 2.
There were no differences in the HRV-related categorical factors based on level of injury
(Appendix H, Table 3) or severity of injury (Appendix H, Table 4).
The HRV-related factors were also compared based on level and severity of injury. LTPAQ-SCI
(Figure 9), LEMS (Figure 10) and SCIM-III (Figure 11) all revealed significant differences
between the cohorts. Individuals with a complete injury below T5 reported less leisure time
activity than individuals with an incomplete injury below T5 (p=0.019). Individuals with a
complete injury equal to/above T5 displayed a lower LEMS than individuals with an incomplete
injury equal to/above T5 (p<0.001) and incomplete and below T5 (p<0.001). Also individuals
with a complete injury below T5 revealed a lower LEMS than individuals with an incomplete
injury equal to/above T5 (p=0.001) and incomplete and below T5 (p=0.008). Finally, individuals
with a complete injury equal to or above T5 had a lower SCIM-III score than individuals with an
incomplete injury below T5. On the other hand, time post injury (p=0.016 but was not significant
for each between group comparison), BMI (p=0.798), number of co-morbidities (p=0.583), age
(p=0.271), waist circumference (p=0.958), relative VO2 peak (p=0.302), absolute VO2 peak
(p=0.254 and p=0.154) and peak heart rate (p=0.077 and p=0.096) were similar across the four
cohorts. The medians and means for each factor are summarized in Appendix H, Table 5 and the

36
follow-up analysis is in Appendix H, Table 6. There were no differences in the HRV-related
categorical factors based on level and severity of injury (Appendix H, Table 7).
Figure 9. Boxplot representation of LTPAQ-SCI based on level and severity of injury. The
complete and below T5 cohort has a lower LTPAQ-SCI score than the incomplete and below T5
cohort (p=0.019).

37
Figure 10. Boxplot representation of LEMS based on level and severity of injury. The
complete and equal to/above T5 cohort had a lower LEMS than the incomplete and equal
to/above T5 (p<0.001) and incomplete and below T5 (p<0.001) cohorts. Also, the complete and
below T5 cohort had a lower LEMS than the incomplete and equal to/above T5 (p=0.001) and
incomplete and below T5 (p=0.008) cohorts.
Figure 11. Boxplot representation of SCIM-III based on level and severity of injury. The
complete and equal to/above T5 cohort had a lower SCIM-III score than the incomplete and
below T5 cohort (p=0.010).

38
4.4 Assessing the heart rate variability frequency domain indices: LF, HF and LF:HF
4.4.1 Relationship between LF and HF
A high positive correlation was found between LF and HF for the entire sample (r=0.708,
p<0.0001) (Figure 12) and in each of the cohorts (Table 9 and Table 10). The scatter plots of LF
and HF based on level and/or severity of injury can be found in Appendix I.
Figure 12. The relationship between LF and HF for total sample. There was a positive linear
correlation between LF and HF in individuals with a chronic and traumatic SCI. The coefficient
of determination (R2) indicated that 50.8% of the variation in LF was shared by HF.

39
Table 9. Relationship of the LF and HFindices based on level or severity of injury
Level of Injury Severity of Injury
Below T5 Above/Equal to T5 Complete
Injury
Incomplete
Injury
Spearman’s Rho† 0.665
p=0.002*
0.730
p<0.0001*
0.590
p<0.0001*
0.849
p<0.0001*
†Spearman’s correlation test; *p≤0.05
Table 10. Relationship of the LF and HF indices based on level and severity of injury
Complete and
equal
to/above T5
Complete and
below T5
Incomplete
and equal
to/above T5
Incomplete
and below T5
Spearman’s
Rho†
0.648
p<0.0001*
0.655
p=0.029*
0.879
p=0.001*
0.833
p=0.010*
†Spearman’s correlation test; *p≤0.05
4.4.2 Relationship between LF, HF, LF:HF and influencing factors
The relationships between LF, HF, LF:HF and the HRV-related factors were examined in the
entire sample (Table 11). LF was negatively correlated with age (r=-0.366, p=0.006) and time
post injury (r=-0.384, p=0.003). Similarly, HF was negatively correlated with age (r=-0.317,
p=0.017) and time post injury (r=-0.344, p=0.009) and was positively correlated with SCIM-III
(r=0.299, p=0.025). LF:HF did not reveal a significant relationship with any of the HRV indices.
The scatter plots of the significant correlations listed in Table 13 can be found in Appendix J.
Table 11. The relationship between LF, HF indices and the scalar HRV-related factors
LF† HF
† LF:HF
†
Age -0.366 -0.317 -0.012

40
p=0.006* p=0.017* p=0.930
Time post injury -0.384
p=0.003*
-0.344
p=0.009*
-0.043
p=0.750
BMI -0.093
p=0.497
-0.106
p=0.436
-0.043
p=0.750
WC -0.091
p=0.506
-0.218
p=0.107
0.153
p=0.259
Absolute VO2 peak 0.052
p=0.722
-0.065
p=0.652
0.201
p=0.162
Relative VO2 peak 0.047
p=0.748
-0.006
p=0.969
0.146
p=0.311
Peak heart rate 0.096
p=0.506
0.031
p=0.832
0.084
p=0.564
LTPAQ-SCI -0.010
p=0.940
0.124
p=0.361
-0.182
p=0.180
LEMS 0.078
p=0.569
0.118
p=0.386
-0.105
p=0.442
SCIM-III 0.224
p=0.097
0.299
p=0.025*
-0.133
p=0.330
Number of
comorbidities
-0.204
p=0.131
-0.256
p=0.057
0.084
p=0.539
†Spearman’s correlation test; *p≤0.05
Abbreviations: BMI, body mass index; WC, waist circumference; LTPAQ-SCI, leisure time
physical activity questionnaire-spinal cord injury; LEMS, lower extremity motor score; SCIM-
III, spinal cord independence measure

41
There was no significant relationship between age at injury, resting systolic blood pressure, LF
or HF when examined in the entire sample (Range of values: Spearman’s rho (r=-0.005 –
r=0.073; p>0.05). Similarly, in individuals with a complete injury at or above T5 (hypothesized
to be the cohort at greatest risk for CVD) also showed no significant relationship between age at
injury, resting systolic blood pressure, LF or HF (Range of values: Spearman’s rho (r=-0.008 –
r=0.170; p>0.05).
4.4.3 Predicting LF and HF from heart rate variability-related factors
The HRV related factors, age, waist circumference, peak heart which are also CVD risk factors,
were assessed using multiple linear regressions to determine whether they can predict LF and/or
HF. Table 12 and Table 13 depict that there were no significant relationships when assessed in
the entire sample. Similarly, when assessed in individuals with a complete injury equal to/above
T5 (expected to be more vulnerable to CVD) there was still no significant relationship; results
are summarized in Appendix K.
Table 12. Multiple linear regression analysis to predict LF for the entire sample (R2=0.039)
Parameter Regression
Coefficient
95% CI p-value
Intercept 830.89 -1533.96,3634.78 0.557
Age -14.67 -39.07,14.16 0.255
WC 4.89 -15.55,22.43 0.604
Peak heart rate 2.48 -6.88,13.38 0.661
*p≤0.05
Abbreviations: WC, waist circumference; CI, confidence interval

42
Table 13. Multiple linear regression analysis to predict HF for the entire sample (R2=0.009)
Parameter Regression
Coefficient
95% CI p-value
Intercept 1252.59 -2592.42,4551.481 0.483
Age -9.68 -38.97,24.47 0.601
WC 2.32 -14.70,22.20 0.789
Peak heart rate -1.46 -12.51,10.84 0.798
*p≤0.05
Abbreviations: WC, waist circumference; CI, confidence interval

43
Chapter 5:
5 Discussion
This is the first study to examine the HRV characteristics in a large and representative sample of
individuals with chronic traumatic SCI. The primary and secondary HRV indices were not
normally distributed and revealed high inter-individual variability in HRV which is similar to
what has been reported in the able-bodied population. Nevertheless, it was unclear why some
subjects (n=4) were outliers when LF:HF was examined in the entire sample. Also, the primary
and secondary HRV indices were not significantly different when compared across cohorts. It is
possible that the lack of a relationship between HRV and level and/or severity of injury is due to
other unaccounted factors influencing the ANS, or because between-subject comparisons were
made instead of within-subjects. In addition, even though some of the HRV-related factors were
different across cohorts, the HRV results were still similar when compared based on level and/or
severity of injury. Therefore, the HRV-related factors may have little influence on HRV in
individuals with chronic traumatic SCI in this study, despite being reported to influence HRV in
the able-bodied population. In addition, a strong positive linear relationship was found between
LF and HF and thus the LF:HF ratio may remain unchanged in individuals with chronic
traumatic SCI. Finally, the bivariate and multivariate analysis between LF, HF and the potential
factors that may influence HRV did not display any significant relationships. There are many
biophysiological changes that occur after a SCI and thus it may be challenging to determine
which factors may be influencing the HRV results.
The frequency distributions of the primary and secondary HRV indices were all positively
skewed indicating that the HRV values in this SCI sample were mainly low. The observed high
inter-individual variability in HRV aligns with the able-bodied population. Nunan et al.37
conducted a systematic review to determine the normal values of HRV in healthy adults. The
systematic review was comprised of studies that measured short term HRV, in accordance with
the Task Force guidelines, in healthy adult participants (n≥30). Nunan and colleagues37
found
large inter-individual variations (up to 260, 000% of variation was reported) between the studies,
especially for the frequency domain measures. Nevertheless, according to Malliani et al.44
it
should not be surprising that there are no HRV normative values within the healthy population

44
since the cardiac ANS is a dynamic system, consists of a large range of values, and is influenced
by a number of internal and external factors. Table 14 depicts the mean and median of the
LF:HF, LF and HF that were reported in healthy subjects based on the systematic review37
and in
chronic traumatic SCI based on the thesis findings. Both the mean and median values depict a
large standard deviation and interquartile range, respectively. Consequently, even though the
HRV values cannot be generalized to the SCI population, the values do indicate that, similar to
able-bodied subjects, there are inter-individual differences in cardiac ANS function within
individuals with chronic traumatic SCI. In addition, the large variations in HRV values
emphasize the importance of reporting HRV as a median as opposed to a mean.
Table 14. Comparison of inter-individual variations in HRV between healthy subjects and
chronic traumatic SCI
Mean ±SD
Median (Lower, Upper quartile)
HRV Indices
Healthy Subjects
(Systematic review)37
Chronic Traumatic SCI
(Current thesis findings)
LF:HF 2.8±2.6
2.1 (1.1, 11.6)
2.2±2.6
1.2 (0.63, 2.85)
LF ms2 519±291
458 (193, 1009)
886±1038
460 (208,1266)
HF ms2 657±777
385 (82, 3630)
834±1138
362 (143,1087)
Abbreviations: SD, standard deviation; LF:HF, low frequency to high frequency ratio; LF, low
frequency; HF, high frequency

45
The LF:HF is a primary measure of HRV as it is reported to examine the level of sympathetic to
parasympathetic activity and thus assesses the modulation of the cardiac ANS. After the LF:HF
outliers were examined, the characteristics of the subjects who were considered outliers did not
provide any further insights. The subjects did not demonstrate any consistent factors to account
for the high LF:HF as they varied in terms of both level and severity of injury, and displayed
diverse HRV-related factors (e.g. differences in sex, time post injury, smoking status, and
physical fitness). In addition, when the subjects were compared to the median of the rest of the
study sample, each subject displayed different factors that were outside the median range. Based
on the data available it was not possible to determine why they were outliers leading one to
expect that perhaps more sensitive biophysiological differences, for instance arterial stiffness
and/or high levels of inflammatory cytokines, may be responsible.
Given that both ANS dysfunction and CVD have been reported to be linked with level and
severity of SCI,4-6,22
it was hypothesized that HRV will differ across cohorts. However, in this
study there were no differences and thus the results suggest that HRV does not depend on type of
SCI (injury level and completeness). Nevertheless, cardiac autonomic regulation is part of two
larger complex systems: the cardiovascular system and the autonomic nervous system. The
cardiovascular component includes peripheral circulation, often altered in SCI, and influences
cardiac function.63
In addition, heart rate is not only modulated by the autonomic nervous
system, but also by the intrinsic cardiac system, baroreflex function, respiration and humoural
factors.63
The ANS controls many other body functions that may also be disrupted in individuals
with a SCI depending mainly on the level and completeness of pathology44
and thus cardiac
autonomic function may be influenced by other intrinsic ANS dysfunctions. Consequently, the
differences in pathophysiology of cardiac autonomic function in individuals with a chronic
traumatic SCI may not be ideal to examine in isolation without considering other cardiovascular
abnormalities. In addition, despite the HRV differences reported in the literature (described in
Chapter 1, Section 1.3.1) some investigators have emphasized that HRV is not a direct measure
of the parasympathetic and sympathetic nerve activity, but instead quantifies cardiac autonomic
responsiveness.7,45
The interpretation of HRV values raises the question if discrete measurement
of HRV at a single point in time is indicative of cardiac ANS modulation and whether comparing
discrete HRV values between subjects has biological merit.

46
Based on only level of injury, the results showed that relative VO2 peak, peak heart rate, and
SCIM-III scores, were greater in the subgroup of individuals with an injury below T5. In
agreement with the literature, Simmons and colleagues64
classified level of SCI as a major
determinant of relative VO2 peak. The established general reference value for cardiorespiratory
fitness is significantly higher in people with paraplegia (median: 16.0 ml/kg/min) than those with
tetraplegia (median: 8.8 ml/kg/min).64
Furthermore, in accordance with the literature,
Ravensbergen and colleagues25
reported that a person with a SCI at the level of T5 or above
attains a reduced peak heart rate during exercise due to diminished sympathetic control. Hagen et
al.17
reported that individuals with complete tetraplegia are unable to raise their peak heart rate to
more than 125 bpm. The increased heart rate observed during exercise has been thought to be the
result of vagal withdrawal.4,25
As SCIM-III provides insight regarding physical capacity, it was not surprising that SCIM-III
was related to the level of injury. For instance, an increase in physical capacity signifies that the
individual has greater voluntary functional muscle mass.64
Even though the results indicate
greater cardiorespiratory fitness (relative VO2 peak and peak heart rate) and greater physical
capacity (SCIM-III) in individuals with an injury below T5, cardiorespiratory fitness and
physical capacity appeared to have a minimal impact on the HRV results as they failed to
contribute to the expected higher HRV values. From our analysis we would have to conclude
that, cardiorespiratory fitness level and physical capacity may not have a major influence on
HRV when assessed based on level of SCI alone.
Physical capacity, measured by LEMS and SCIM-III, was higher in incomplete injuries and the
time post injury was longer in complete injuries. Previous findings have shown that level and
severity of SCI may influence HRV results,2 but other SCI characteristics have not been
examined. For instance, it is unknown if and how time post SCI influences HRV. Based on this
study, however, time post injury in addition to physical capacity may not have an influence on
HRV when assessed based on severity of injury since there were no differences observed
between the cohorts.
As expected LTPAQ-SCI, LEMS and SCIM-III, differed based on both level and severity of
injury. Bucholz and colleagues65
found that LTPAQ-SCI has been associated with a decrease of

47
CVD risk factors in individuals with chronic traumatic SCI. Previous studies have shown that
individuals with a complete and cervical injury report less leisure time physical activity than
those with an incomplete and lower level of injury.65-66
In addition, the differences in physical
activity are probably because individuals with complete tetraplegia are limited in terms of in
which exercises they can participate and require greater assistance with exercise protocols.65-66
Also, individuals with high lesions, especially cervical, often have bradycardia and thus their low
level of cardiac sympathetic function makes it difficult to participate in physical activity.25
The
results did show that individuals with complete injury engaged in less leisure time physical
activity than those with an incomplete injury, but these findings were only observed in
individuals with injuries below the level of T5. A possible reason as to why, contrary to the
literature, severity of injury did not influence the physical activity results in individuals with high
level injuries, could be the method of measuring leisure time physical activity. Most studies use
the Physical Activity Recall Assessment for People with Spinal Cord Injury (PARA-SCI)
questionnaire which involves recording both activities of daily living in addition to leisure time
physical activity and is collected over three days as opposed to over a week. The present study,
however, used the LTPAQ-SCI which recorded the number of minutes of physical activity per
week and did not include activities of daily living.
Expected and consistent with the literature, LEMS were lower in individuals with a complete
injury and/or with an injury above the level of T5 illustrating less voluntary muscle function in
the lower limbs. Similarly, SCIM-III revealed lower scores for individuals with complete and
equal to/above T5 injuries than those with in incomplete and below T5 injuries. Lower physical
capacity and physical activity can be used to determine whether the individual is likely to be
sedentary64
and thus has been reported to contribute to lower HRV values.25
However, in this
study, despite the differences in the physical activity observed amongst the cohorts, the HRV
indices were still similar when compared based on both level and severity of injury. Therefore,
physical activity and capacity may not have a substantial impact on HRV in a chronic traumatic
SCI population.
When revisiting the theoretical framework illustrating the link between SCI and CVD for chronic
traumatic SCI, it is important to include impaired cardiac autonomic modulation as a component
of the disrupted autonomic nervous system (Figure 13). Many studies have reported a diminished

48
LF in individuals with a cervical and/or thoracic SCI.2,29,42,48
A reduced LF, a purported cardiac
sympathetic marker, indicates a greater challenge to participate in physical activity25
and thus
contributes to sedentary behavior. A decrease in HF, a parasympathetic marker, is problematic
for this population since parasympathetic activity decreases the amount of work on the heart and
thus has been linked to restoring and protecting the cardiovascular system in other populations.67
Therefore, if LF does indeed decrease after a SCI, the positive relationship between LF and HF
may indicate increased risk of CVD development in individuals with a chronic and traumatic
SCI. Since the primary study excluded any subjects with a cardiac disease, including
arrhythmias, we have no indication of how arrhythmias interact with cardiac autonomic
modulation. Furthermore, with the non-modifiable factors of age, sex, genetic history, sedentary
lifestyle, smoking status and obesity being accounted for in this study albeit considering the
collinearity but demonstrating a lack of effect on the HRV indices suggests that other biological
contributors to CVD development will need to be examined in this chronic population.
Figure 13. Possible contributors to greater CVD risk in individuals with chronic traumatic
SCI. The theoretical framework represents the relationship between SCI and CVD while also
considering the findings from the thesis. Impaired cardiac autonomic modulation has been added
as a subgroup of disrupted autonomic nervous system to indicate that impairment also
contributes to CVD development in chronic traumatic SCI. The arrow between the sympathetic

49
and parasympathetic cardiac activity is bidirectional since the ANS represents a shifting balance
between the two systems (Modified from Figure 1.0).
There is a debate in the literature regarding the relationship between LF and HF in individuals
with a SCI. In this study, LF and HF displayed a positive linear relationship when assessed in the
entire sample and based on level and/or severity of injury. After a cervical SCI, Claydon et al.2
observed lower LF and higher HF, whereas Grimm et al.30
and Wang et al.29
reported both lower
LF and HF. As for the thoracic group, Claydon et al.2 reported no change in LF and a reduced
HF while Bunten et al.42
and Castiglioni et al.48
reported reduced LF but no change in the HF
values. Although the findings from the current study did not show a decrease in any of the HRV
parameters, it did show that in the entire sample, 50.8% of the variation in LF was shared by HF
and thus a decrease or even an increase in both components could result in a similar LF:HF ratio.
The LF and HF relationship was strongest in individuals with an incomplete injury and equal
to/above T5, as 84.3% of the variability in LF was shared by HF. In incomplete injuries the cord
is not completely disconnected from the brain30,42
and with an injury that occurs at or above T5
the sympathetic activity is disrupted,25
thus it is possible that the modulation of ANS system was
altered to a greater extent in this group. There is low resting sympathetic tone in individuals with
a SCI in comparison with able-bodied subjects.26
Consequently, most investigators indicate that a
change in HF is required to align with the low levels of LF since the ANS re-balances to
maintain homeostasis.2,15,29-30
However, the physiological basis of how the ANS re-balances
remains unclear. However, Billman68
challenged the presumption of the ANS re-balancing and
argued that the LF index is not more indicative of sympathetic function but is rather a complex
combination between the two ANS branches along with other unidentified factors. Furthermore,
the correlation between the LF and HF indices does not meet the nine Bradford-Hill criteria69
for
causation and thus it is not certain that a change in LF caused a change in HF. Therefore, the
positive correlation between the LF and HF indices may not necessarily represent a re-balanced
ANS system. Despite the indeterminate physiological reasons for the positive correlation
observed between the LF and HF indices, overall this finding questions whether the LF:HF, the
most common HRV measure, is an appropriate marker of the cardiac sympatho-vagal balance in
individuals with chronic traumatic SCI.

50
None of the HRV related factors that were tested displayed a significant correlation with the
LF:HF even though some variables did display a significant correlation with the LF and HF
indices. After examining the scatter plots of LF, HF and the significantly correlated HRV-related
factors, it appeared that the variation in LF and HF were only minimally shared by age, SCIM-
III, and time post injury (ranging from almost 1% to 15%). The mean age (46.75±12.44) reported
in the SCI and resting HRV literature is similar to the mean age reported in this study. It was
expected that as age increases sympathetic activity increases, represented by higher LF, and
parasympathetic activity decreases, represented by lower HF.32
Surprisingly, however, an inverse
relationship was observed between LF and age, but only 4.1% of variation in LF was shared by
age. Also, unexpectedly, HF displayed a weak negative relationship with age and only 1% of
variation in HF was shared by age.
A higher degree of physical capacity usually indicates capability to be physically active which in
turn has been linked to the predominance of the parasympathetic function.31,67,70-71
As a result, it
was surprising that the HF was only slightly positively correlated with SCIM-III; where only
0.8% of the variability in HF was shared by SCIM-III. However, SCIM-III may not be a good
indicator of physical capacity. The relationship between HRV and time post injury has not yet
been established for SCI, but the findings revealed that time post injury was negatively
correlated with both LF and HF; 14.7% of the variability in LF was shared by time post injury,
and 12.8% of variability in HF was shared by time post injury. Therefore, the results might be
interpreted that as time post injury increased, both sympathetic and parasympathetic function
decreased illustrating the persistence of CVD risk (for the same reasons mentioned earlier). The
strengths of the relationships between LF, age and time post injury, and between HF, age, time
post injury and SCIM-III were all of fair magnitude at best and thus over interpretation without
further analysis is not warranted.
Similarly, the multiple linear regression analysis did not reveal any significant relationships
between the CVD risk factors (age, waist circumference, peak heart rate) and LF or HF when
examined in the entire sample. The multivariate relationship was also assessed in individuals
with a complete injury at or above T5, the cohort that is most likely to develop CVD, but again
no relationships were observed. Consequently, according to our results, the CVD risk factors,
which are also HRV-related factors, do not have a substantial impact on LF and HF in

51
individuals with a traumatic and chronic SCI. The presence of a SCI, associated with various
physiological and functional changes, may minimize the impact of the HRV-related factors that
have been observed in the able bodied population.
When age at injury and resting systolic blood pressure were examined to determine if they were
contributors to HRV in both the entire sample and in the cohort with a complete injury equal
to/above T5, age at injury and LF or HF both appeared to have no relationship. Therefore, the
cardiac ANS does not behave differently if a SCI occurred at a younger or older age our range
being 37to 54 years. Resting systolic blood pressure has been reported to be linked with level
and severity of SCI; higher level and complete injuries display lower resting systolic blood
pressure5 and the reduction in blood pressure has been reported to occur due to the reduction in
sympathetic activity after a SCI.3 Again we could not demonstrate these expected findings in the
entire sample or in individuals with a complete injury at or above T5. Consequently, in
individuals with a chronic and traumatic SCI, it appears that the sympathetic and
parasympathetic cardiac activity is not influenced by sympathetic reduced resting blood pressure.
The ANS is a complex biological system and therefore it is difficult to ascertain what and how
other changing ANS activity could be influencing the HRV parameters without conducting
physiological experiments that challenge the ANS system over time.
5.1 Implications and future directions
Cardiac autonomic disturbances are believed to be a major contributor to the development of
CVD within the SCI population. Therefore, quantifying the cardiac parasympathetic and
sympathetic modulation of the heart, via a non-invasive measure, is important for diagnostic,
prognostic and/or rehabilitative purposes. However, HRV values for SCI have not yet been
established and the lack of HRV differences observed in this study indicate that HRV does not
directly reflect the anatomical sympathetic and parasympathetic autonomic innervations and
response of the heart in individuals with a chronic and traumatic SCI. The proposed HRV-related
factors, in addition to age at injury and resting systolic blood pressure did not have an impact on
the HRV results, which further emphasizes the complexity of the ANS. The findings from this
data set suggests limited potential for assessing HRV at a single point in time in individuals with
a chronic traumatic SCI to measure autonomic cardiac function..

52
There is disagreement in the literature as to whether the subjects should be divided into three
levels i.e. cervical, high thoracic, low thoracic and lumbar, or two levels i.e. above a level of
injury and below a level of injury. Consequently, to check whether there are any HRV
differences between different types of SCI, in addition to a larger sample size, this work could be
repeated with a different cohort selection: cervical (C1-C8), high thoracic (T1-T5), and low
thoracic (T6-T12). The presence of a strictly cervical cohort allows for the assessment of
completely disconnected cardiac sympathetic innervation. In addition, West et al.5
have reported
that in individuals with a chronic SCI, autonomic completeness of the injury, which can be
estimated via catecholamine concentrations as well as blood pressure variability, is more closely
related to the function of the cardiovascular ANS than the neurological completeness of injury.5
Therefore, it may be more important to measure concomitantly the autonomic completeness of
injury and additional autonomic dysfunctions such as orthostatic hypotension and autonomic
dysreflexia to gain further insights. Also, provided that HRV represents the modulation of the
cardiac ANS, it may be a valuable tool to test the responsive of the cardiac ANS to different
testing conditions.45
The testing conditions will eliminate the problem of high HRV inter-subject
variability since the HRV comparisons will be made within-subjects. It may also be useful to
combine HRV assessments with other cardiac measurements to assess the risk of cardiac disease
in individuals with a SCI such as combining left ventricular ejection fractions with HRV
assessments in order to identify cardiac patients as suggested by Kleiger and colleages41
. The
International Standards to document remaining Autonomic Function after Spinal Cord Injury
(ISAFSCI)6 have been recently considered the gold standard for ANS assessment in SCI and
includes measures of the heart rate, blood pressure, sweating, temperature regulation and the
broncho-pulmonary system etc. and could add value to future studies using different testing
paradigms to assist with interpreting the results.
5.2 Study limitations
A major study limitation was that HRV was compared across cohorts and subjects that were
highly variable. Intra–subject comparisons using HRV may be a far better paradigm. Also,
contrary to the literature, no differences were observed in HRV when compared based on level
and severity of injury. The total sample size divided into four cohorts may have been too small to
detect significant differences. Post-hoc power analysis revealed that based on the mean per

53
cohort of the primary HRV index, LF:HF, a total sample size of 72 would be required to detect a
difference.
Also the completeness of injury, as assessed by the International Standards for Neurological and
Functional Classification of Spinal Cord Injury indicates whether there is sensory or motor
function preserved in the lowest sacral segments (S4-S5).13
Therefore neurological completeness
which was used in this study, provided little information regarding the severity of autonomic
dysfunction after a SCI.
A final study limitation was that the breathing pattern was not monitored or recorded
simultaneously with the ECG data collection in the primary study so the data were not available
for analysis. Respiratory sinus arrhythmia is the natural variation of the heart rate and is driven
by the breathing pattern via vagal influence of the heart.31
The HF bandwidth has been linked to
the respiratory sinus arrhythmia and thus the breathing pattern during data collection may alter
the results of HRV.31-32,35
Nunan and colleages37
showed that the parasympathetic activity was
elevated when testing was done in a resting supine position along with paced breathing.
Billman68
also suggested that all subjects must engage in paced breathing to ensure precise
measurement of HRV. Consequently, depending on whether the subjects in this study engaged in
controlled or spontaneous breathing, the HF component may have disproportionally represented
the parasympathetic modulation of the heart.

54
Chapter 6:
6 Conclusions
Traditional CVD risk factors, such as age, sex, obesity, and lifestyle, in addition to SCI-related
changes pose an increased risk of CVD development among individuals with a SCI. Autonomic
dysfunction, particularly of the cardiovascular ANS has been recently classified as a major CVD
contributor in SCI and thus requires further investigation. HRV analysis was examined since it
has been hypothesized to have the potential to non-invasively measure of cardiac autonomic
disruption and thus assess cardiac risk in individuals with a SCI. The findings illustrated that
there was an extremely wide range of HRV values in a chronic cross-sectional population thus
making it difficult to develop HRV reference values for this population of SCI. Nonetheless, the
inter-subject variability has also been observed in the able-bodied population which may indicate
that, likewise, individuals with a SCI also experience diverse cardiac ANS function.
Furthermore, despite the fact that cardiac autonomic dysfunction has been shown to be related to
the level and severity of injury, our results revealed no differences across the selected cohorts.
The disparity with the literature might have been due to a number of reasons: 1. Between subject
comparisons were made in spite of the fact that HRV has high inter-subject variability; 2. HRV
is not exclusively linked to level and severity of SCI, and 3. Cardiac autonomic function has
multiple biological complexities that cannot be measured exclusively by heart rate parameters.
Given that the LF:HF, is the most commonly used HRV measure of cardiac sympatho-vagal
balance and the physiological interpretation of the positive relationship between LF and HF
remains undetermined, HRV indices may not be applicable in individuals with a traumatic and
chronic SCI. Further understanding of the biological interpretation of the HRV indices is
required before routinely using HRV in SCI to monitor and/or manage CVD progression.

55
References
1. Cragg JJ, Noonan VK, Krassioukov A, Borisoff J. Cardiovascular disease and spinal cord
injury results from a national population health survey. Neurology. 2013;81(8):723-8.
2. Claydon VE, Krassioukov AV. Clinical correlates of frequency analyses of
cardiovascular control after spinal cord injury. American Journal of Physiology - Heart &
Circulatory Physiology. 2008 Feb;294(2):H668-78. PubMed PMID: 18024546.
3. Myers J, Lee M, Kiratli J. Cardiovascular disease in spinal cord injury: An overview of
prevalence, risk, evaluation, and management. American Journal of Physical Medicine &
Rehabilitation. 2007 Feb;86(2):142-52. PubMed PMID: 17251696.
4. Sahota IS, Ravensbergen HJ, McGrath MS, Claydon VE. Cerebrovascular responses to
orthostatic stress after spinal cord injury. J Neurotrauma. 2012;29(15):2446-56.
5. West CR, Bellantoni A, Krassiokouv AV. Cardiovascular function in individuals with
incomplete spinal cord injury: A systematic review. Top Spinal Cord Inj Rehabil. 2013
Fall;19(4):267-78. PubMed PMID: 24244092. Pubmed Central PMCID: PMC3816721
Epub 2013/11/19.eng.
6. Krassioukov A, Biering-Sorensen F, Donovan W, Kennelly M, Kirshblum S, Krogh K, et
al. International standards to document remaining autonomic function after spinal cord
injury. J Spinal Cord Med. 2012 Jul;35(4):201-10. PubMed PMID: 22925746. Epub
2012/08/29. Eng
7. Task Force of the European Society of Cardiology and the North American Society of
Pacing and Electrophysiology. Heart rate variability: standards of measurement,
physiological interpretation and clinical use. Task Force of the European Society of
Cardiology and the North American Society of Pacing and Electrophysiology.
Circulation. 1996 Mar 1;93(5):1043-65. PubMed PMID: 8598068. Epub 1996/03/01. eng.
8. Farry A, Baxter D. The incidence and prevalence of spinal cord injury in Canada:
Overview and estimates based on current evidence. Rick Hansen Institute and Urban
Futures Institute; 2010 December.
9. Ones K, Yilmaz E, Beydogan A, Gultekin O, Caglar N. Comparison of functional results
in non-traumatic and traumatic spinal cord injury. Disability & Rehabilitation.
2007;29(15):1185-91. PubMed PMID: 17653992.
10. Chapman J. Comparing medical complications from nontraumatic and traumatic spinal
cord injury. Arch Phys Med Rehabil. 2000;81:1264.
11. Bican O, Minagar A, Pruitt AA. The spinal cord: a review of functional neuroanatomy.
Neurologic Clinics. 2013;31(1):1-18. PubMed PMID: 23186894.
12. Maynard FM, Jr., Bracken MB, Creasey G, Ditunno JF, Jr., Donovan WH, Ducker TB, et
al. International standards for neurological and functional classification of spinal cord
injury. Spinal Cord. 2007;35(5):266-74. PubMed PMID: 9160449.
13. Kirshblum SC, Biering-Sorensen F, Betz R, Burns S, Donovan W, Graves DE, et al.
International Standards for Neurological Classification of Spinal Cord Injury: cases with

56
classification challenges. Journal of Spinal Cord Medicine.2014;37(2):120-7. PubMed
PMID: 24559416.
14. Kirshblum SC, Burns SP, Biering-Sorensen F, Donovan W, Graves DE, Jha A, et al.
International standards for neurological classification of spinal cord injury (revised
2011). J Spinal Cord Med. 2011 Nov;34(6):535-46. PubMed PMID: 22330108. Pubmed
Central PMCID: PMC3232636. Epub 2012/02/15. eng.
15. Rosado-Rivera D, Handrakis JP, Cirnigliaro CM, Jensen AM, Kirshblum S, Bauman
WA, et al. Comparison of 24-hour cardiovascular and autonomic function in paraplegia,
tetraplegia, and control groups: Implications for cardiovascular risk. Journal of Spinal
Cord Medicine. 2011;34(4):395-403. PubMed PMID: 21903013.
16. West C, Mills P, Krassioukov A. Influence of the neurological level of spinal cord injury
on cardiovascular outcomes in humans: A meta-analysis. Spinal Cord. 2012;50(7):484-92
17. Hagen E, Rekand T, GrÃnning M, Faerestrand S. Cardiovascular complications of spinal
cord injury. Tidsskrift for den Norske laegeforening: tidsskrift for praktisk medicin, ny
raekke. 2012;132(9):1115-20.
18. Nash MS, Cowan RE, Kressler J, Nash MS, Cowan RE, Kressler J. Evidence-based and
heuristic approaches for customization of care in cardiometabolic syndrome after spinal
cord injury. Journal of Spinal Cord Medicine. 2012 Sep;35(5):278-92. PubMed PMID:
23031165.
19. Wahman K, Nash MS, Lewis JE, Seiger A, Levi R. Cardiovascular disease risk and the
need for prevention after paraplegia determined by conventional multifactorial risk
models: The Stockholm spinal cord injury study. J Rehabil Med. 2011;43(3):237-42.
20. Rice BH, Cifelli CJ, Pikosky MA, Miller GD. Dairy components and risk factors for
cardiometabolic syndrome: Recent evidence and opportunities for future research.
Advances in Nutrition: An International Review Journal. 2011 Sep;2(5):396-407
21. Pearson TA, Blair SN, Daniels SR, Eckel RH, Fair JM, Fortmann SP, et al. AHA
guidelines for primary prevention of cardiovascular disease and stroke: 2002 update:
Consensus panel guide to comprehensive risk reduction for adult patients without
coronary or other atherosclerotic vascular diseases. Circulation. 2002 July;106(3):388-91.
22. Furlan JC, Fehlings MG. Cardiovascular complications after acute spinal cord injury:
Pathophysiology, diagnosis, and management. Neurosurgical Focus.2008;25(5):E13.
PubMed PMID: 18980473.
23. Miyatani M, Szeto M, Moore C, Oh PI, McGillivray CF, Craven BC. Exploring the
associations between arterial stiffness and spinal cord impairment: A cross-sectional
study. J Spinal Cord Med. 2014;37(5):556-64.
24. Xhyheri B, Manfrini O, Mazzolini M, Pizzi C, Bugiardini R. Heart rate variability today.
Prog Cardiovasc Dis. 2012 Nov-Dec;55(3):321-31. PubMed PMID: 23217437. Epub
2012/12/12. Eng.
25. Ravensbergen HJ, de Groot S, Post MW, Slootman HJ, van der Woude LH, Claydon VE.
Cardiovascular function after spinal cord injury: Prevalence and progression of

57
dysfunction during inpatient rehabilitation and 5 years following discharge. Neurorehabil
Neural Repair. 2014 Mar;28(3):219-29. PubMed PMID: 24243916. Epub 2013/11/19.
eng.
26. Krassioukov A. Autonomic dysreflexia: current evidence related to unstable arterial
blood pressure control among athletes with spinal cord injury. Clinical Journal of Sport
Medicine. 2012;22(1):39-45.
27. Wecht JM, Bauman WA. Decentralized cardiovascular autonomic control and cognitive
deficits in persons with spinal cord injury. J Spinal Cord Med. 2013;36(2):74-81.
28. Alexander MS, Biering-Sorensen F, Bodner D, Brackett NL, Cardenas D, Charlifue S, et
al. International standards to document remaining autonomic function after spinal cord
injury. Spinal Cord. 2009;47(1):36-43. PubMed PMID: 18957962.
29. Wang YH, Huang TS, Lin JL, Hwang JJ, Chan HL, Lai JS, et al. Decreased autonomic
nervous system activity as assessed by heart rate variability in patients with chronic
tetraplegia. Arch Phys Med Rehabil. 2000 Sep;81(9):1181-4. PubMed PMID: 10987159.
Epub 2000/09/15. Eng.
30. Grimm DR, De Meersman RE, Almenoff PL, Spungen AM, Bauman WA.
Sympathovagal balance of the heart in subjects with spinal cord injury. Am J Physiol.
1997 Feb;272(2 Pt 2):H835-42. PubMed PMID: 9124446. Epub 1997/02/01. eng.
31. Freeman JV, Dewey FE, Hadley DM, Myers J, Froelicher VF. Autonomic nervous
system interaction with the cardiovascular system during exercise. Progress in
Cardiovascular Diseases. 2006 Mar-Apr;48(5):342-62. PubMed PMID: 16627049.
32. McMillan DE. Interpreting heart rate variability sleep/wake patterns in cardiac patients. J
Cardiovasc Nurs. 2002 Oct;17(1):69-81. PubMed PMID: 12358094. Epub 2002/10/03.
eng.
33. Montano N, Porta A, Cogliati C, Costantino G, Tobaldini E, Casali KR, et al. Heart rate
variability explored in the frequency domain: A tool to investigate the link between heart
and behavior. Neuroscience & Biobehavioral Reviews. 2009 Feb;33(2):71-80. PubMed
PMID: 18706440.
34. Stauss HM. Heart rate variability. American Journal of Physiology - Regulatory
Integrative & Comparative Physiology. 2003 Nov;285(5):R927-31. PubMed PMID:
14557228.
35. Bertsch K, Hagemann D, Naumann E, Schachinger H, Schulz A. Stability of heart rate
variability indices reflecting parasympathetic activity. Psychophysiology. 2012
May;49(5):672-82. PubMed PMID: 22335779.
36. Lauer MS. Autonomic function and prognosis. Cleveland Clinic Journal of Medicine.
2009 Apr;76 Suppl 2:S18-22. PubMed PMID: 19376976.
37. Nunan D, Sandercock GR, Brodie DA. A quantitative systematic review of normal values
for short-term heart rate variability in healthy adults. Pacing Clin Electrophysiol. 2010
Nov;33(11):1407-17. PubMed PMID: 20663071. Epub 2010/07/29. eng.

58
38. Sandercock GRH, Bromley PD, Brodie DA. Effects of exercise on heart rate variability:
inferences from meta-analysis. Medicine & Science in Sports & Exercise. 2005
Mar;37(3):433-9. PubMed PMID: 15741842.
39. Schroeder EB, Whitsel EA, Evans GW, Prineas RJ, Chambless LE, Heiss G, et al.
Repeatability of heart rate variability measures. Journal of Electrocardiology. 2004
Jul;37(3):163-72. PubMed PMID: 15286929.
40. Thayer JF, Yamamoto SS, Brosschot JF. The relationship of autonomic imbalance, heart
rate variability and cardiovascular disease risk factors. Int J Cardiol. 2010 May
28;141(2):122-31. PubMed PMID: 19910061. Epub 2009/11/17. eng.
41. Kleiger RE, Stein PK, Bigger JT, Jr. Heart rate variability: Measurement and clinical
utility. Ann Noninvasive Electrocardiol. 2005 Jan;10(1):88-101. PubMed PMID:
15649244.
42. Bunten DC, Warner AL, Brunnemann SR, Segal JL. Heart rate variability is altered
following spinal cord injury. Clin Auton Res. 1998 Dec;8(6):329-34. PubMed PMID:
9869550. Epub 1998/12/30. eng.
43. Ditor DS, Macdonald MJ, Kamath MV, Bugaresti J, Adams M, McCartney N, et al. The
effects of body-weight supported treadmill training on cardiovascular regulation in
individuals with motor-complete SCI. Spinal Cord. 2005 Nov;43(11):664-73. PubMed
PMID: 15968298.
44. Malliani A. Heart rate variability: From bench to bedside. European journal of internal
medicine. 2005 Feb;16(1):12-20. PubMed PMID: 15733815. Epub 2005/03/01. Eng.
45. Perini R, Veicsteinas A, Perini R, Veicsteinas A. Heart rate variability and autonomic
activity at rest and during exercise in various physiological conditions. European Journal
of Applied Physiology. 2003 Oct;90(3-4):317-25. PubMed PMID: 13680241.
46. Vetrugno RM, Liguori RM, Cortelli PM, Montagna PM. Sympathetic skin response. Clin
Auton Res. 2003;13(4):256-70.
47. Ditor DS, Kamath MV, Macdonald MJ, Bugaresti J, McCartney N, Hicks AL.
Reproducibility of heart rate variability and blood pressure variability in individuals with
spinal cord injury. Clin Auton Res. 2005;15(6):387-93.
48. Castiglioni P, Di Rienzo M, Veicsteinas A, Parati G, Merati G. Mechanisms of blood
pressure and heart rate variability: An insight from low-level paraplegia. Am J Physiol
Regul Integr Comp Physiol. 2006 Apr;292(4):R1502-9. PubMed PMID: 17122332. Epub
2006/11/24. eng.
49. Claydon VE, Hol AT, Eng JJ, Krassioukov AV. Cardiovascular responses and
postexercise hypotension after arm cycling exercise in subjects with spinal cord injury.
Archives of Physical Medicine and Rehabilitation. 2006;87(8):1106-14.
50. Claydon VE, Krassioukov AV. Orthostatic hypotension and autonomic pathways after
spinal cord injury. J Neurotrauma. 2006;23(12):1713-25
51. Kaikkonen KM, Korpelainen RI, Tulppo MP, Kaikkonen HS, Vanhala ML, Kallio MA,
et al. Physical activity and aerobic fitness are positively associated with heart rate

59
variability in obese adults. J Phys Act Health. 2014. Ahead of print. PubMed PMID:
24508687. eng.
52. Alrefaie Z. Brief assessment of supine heart rate variability in normal weight,
overweight, and obese females. Ann Noninvasive Electrocardiol. 2014;19(3):241-6.
53. Mehta RK. Impacts of obesity and stress on neuromuscular fatigue development and
associated heart rate variability. Int J Obes. 2014. Ahead of print.
54. Farah BQ, Prado WL, Tenorio TR, Ritti-Dias RM. Heart rate variability and its
relationship with central and general obesity in obese normotensive adolescents. Einstein.
2013;11(3):285-90. PubMed PMID: 24136753.
55. Melanson EL, Freedson PS. The effect of endurance training on resting heart rate
variability in sedentary adult males. European Journal of Applied Physiology. 2001
Sep;85(5):442-9. PubMed PMID: 893734373; 11606013.
56. Flevari A, Vagiakis E, Zakynthinos S. Heart rate variability is augmented in patients with
positional obstructive sleep apnea, but only supine LF/HF index correlates with its
severity. Sleep Breath. 2014. Ahead of print.
57. Chalmers J, Quintana DS, Abbott MJ-A, Kemp AH. Anxiety disorders are associated
with reduced heart rate variability: A meta-analysis. Frontiers in Psychiatry. 2014
July11;5.
58. Lee CL CW. The effects of cigarette smoking on aerobic and anaerobic capacity and
heart rate variability among female university students. International Journal of Women's
Health. 2013 Oct;5:667-79
59. Craven C, Verrier M, Balioussis C, Wolfe D, Hsieh J, Noonan V, et al. Rehabilitation
environmental scan atlas: Capturing capacity in Canadian SCI rehabilitation. Rick
Hansen Institute, Vancouver, BC. 2012.
60. Brennan M, Palaniswami M, Kamen P. Do existing measures of Poincare plot geometry
reflect nonlinear features of heart rate variability? Biomedical Engineering, IEEE
Transactions on. 2001;48(11):1342-7.
61. Young FL, Leicht AS, Young FLS, Leicht AS. Short-term stability of resting heart rate
variability: influence of position and gender. Applied Physiology, Nutrition, &
Metabolism Physiologie Appliquee, Nutrition et Metabolisme. 2011 Apr;36(2):210-8.
PubMed PMID: 21609282.
62. Portney LG, Watkins MP. Foundations of Clinical Research: Applications to Practice.
2nd ed. Upper Saddle River, NJ: Prentice-Hall Inc, 2000.
63. Diego JB, Pedrosa DF, Gava AL. Cardiac Arrhythmias - New Considerations Croatia:
InTech; 2012. Chapter 8, Neurohumoral Control of Heart Rate; p.167-192.
64. Simmons OL, Kressler J, Nash MS. Reference fitness values in the untrained spinal cord
injury population. Arch Phys Med Rehabil. 2014;95(12):2272-8.

60
65. Buchholz AC, Martin Ginis KA, Bray SR, Craven BC, Hicks AL, Hayes KC, et al.
Greater daily leisure time physical activity is associated with lower chronic disease risk
in adults with spinal cord injury. Appl Physiol Nutr Metab. 2009;34(4):640-7.
66. Martin Ginis KA, Jetha A, Mack DE, Hetz S. Physical activity and subjective well-being
among people with spinal cord injury: A meta-analysis. Spinal Cord. 2010;48(1):65-72.
67. Routledge FS, Campbell TS, McFetridge-Durdle JA, Bacon SL. Improvements in heart
rate variability with exercise therapy. Canadian Journal of Cardiology. 2010 Jun-
Jul;26(6):303-12. PubMed PMID: 20548976.
68. Billman GE. The LF/HF ratio does not accurately measure cardiac sympatho-vagal
balance. Frontiers in Physiology. 2013;4(26):1-5.
69. Bradford-Hill A. The environment and disease: Association or causation? Proc R Soc
Med. 1965;58:295-300.
70. de la Cruz Torres B, Lopez Lopez C, Naranjo Orellana J. Analysis of heart rate
variability at rest and during aerobic exercise: a study in healthy people and cardiac
patients. Br J Sports Med. 2008 Sep;42(9):715-20. PubMed PMID: 18199627. Epub
2008/01/18. eng.
71. Grant CC, Viljoen M, van Rensburg DC, Wood PS. Heart rate variability assessment of
the effect of physical training on autonomic cardiac control. Ann Noninvasive
Electrocardiol. 2012 Jul;17(3):219-29. PubMed PMID: 22816541. Epub 2012/07/24. eng.

61
Appendices

62
Appendix A

63

64

65
Appendix B

66

67
Appendix C
The table below summarizes the average percentage of noise, ectopic, and artifact for each five minute segment, and the possible reasons
for displaying ectopic islands. The Poincaré plot was examined after the subjects were selected and therefore a total sample of 56 subjects.
Table 1. Summary of the subjects who displayed ectopic islands in their Poincaré plots before the filter was applied
Subject
ID
Complete
(C)/Incomplete
(I) injury
Level of injury Normal (%) Ectopic (%) Artifact (%) Possible Reason
2
C T4
84.03 15.28 0.69
Unclear- Normal ECG &sinus
rhythm
5
I T10
88.66 7.32 4.02
R peak 0.001V (very small
compared to others)
11
I C4
88.59 11.05 0.36
Unstable baseline;
unifocal/premature ventricular
beat # 35, 16, 157, 163, 206, 522
12 I C6 90.94 6.43 2.63
Unclear- Normal ECG &sinus
rhythm
23 C C6 82.70 6.89 10.41 Unstable baseline
26 I T5 38.78 34.51 26.71 Unstable baseline
30 C T4 84.47 14.32 1.21
Unclear- Normal ECG &sinus
rhythm

68
31 C C5 91.29 7.37 1.34
Unclear-Normal ECG &sinus
rhythm
34 I T12 51.94 48.06 0.33 Read two R peaks for each one
39 C T4 86.33 8.52 5.15
Unclear- Normal ECG &sinus
rhythm
45 I C6
66.72 1.32 31.96
Unclear-Normal ECG &sinus
rhythm
71 I C6
93.24 0.26 6.49
High T waves (at times larger
than R wave due to unstable
baseline)
72 I C4 95.29 3.30 1.41 Unstable baseline
88 I T12 90.66 9.17 0.51 Read two R peaks for each one
91 I T12 85.66 4.78 9.56 Read two R peaks for each one

69
Appendix D
The following appendix examines the outliers present when the primary HRV index (LF:HF) was plotted. Table 1 describes the
characteristics of the subjects who were outliers when the data was examined for the entire sample and based on level and severity of
injury. Figure 1 is the frequency distribution after the outliers were omitted from the entire sample.
Table 1. The characteristics of the subjects who were outliers when LF:HF was assessed in the entire sample and based on level
and severity of injury, in comparison to the rest of the study sample
Shaded areas indicate that the value is outside the median range
Factors Study sample
(without the
outliers)
Subject 82 Subject 17 Subject 40 Subject
19
Subject 45 Subject 61
Type of SCI Level of Injury NA C6 T6 T7 C7 C6 C2
Severity of Injury NA Complete Complete Complete Complete Incomplete Incomplete
Time post injury
(years)
Mean:
13.78±9.74
Median: 11.00
(5.00, 21.25)
30 22 25 6 22 3
HRV
Frequency
domain
measures
LF (ms2) Mean:
900.76±1070.26
Median: 460.20
(202.78,
26.84 2053.79 499.02 453.74 211.51 1326.25

70
1230.49)
HF (ms2) Mean:
917.25±1177.12
Median: 439.38
(177.14,
1173.75)
1.94 196.73 60.29 61.84 69.08 425.96
LF:HF Mean:
1.49±1.24
Median: 1.03
(0.57, 2.15)
13.81 10.44 8.28 7.34 3.06 3.11
Demographics Age (years) Mean:
46.04±12.64
Median: 44.00
(37.00, 54.25)
50 43 53 70 54 46
Sex
(male/female)
30/12 Male Male Male Male Male Male
Cardiovascular
status
BMI (kg/m2) Mean:
25.83±4.73
Median: 27.06
(21.97, 29.08)
22.48 31.24 27.77 26.32 38.34 25.63
Waist
Circumference
(cm)
Mean:
94.25±14.22
Median: 94.90
95.50 123.50 99.50 103.20 124.00 98.00

71
(83.05, 104.70)
Absolute VO2
peak (L/min)
Mean:
1.29±0.61
Median: 1.14
(0.82, 1.59)
1.10 2.37 1.92 1.05 NT 1.09
Relative VO2
peak (ml/kg/min)
Mean:
16.71±7.62
Median: 16.29
(11.38, 22.34)
14.61 23.36 20.68 13.36 NT 13.45
Peak Heart rate
(bpm)
Mean:
130.42±29.08
Median: 128.00
(105.00,
155.00)
94 176 146 121 NT 107
Resting systolic
blood pressure
(mmHg)
Mean:
110.82±16.70
Median: 109.00
(98.00, 122.00)
88 132 100 90 108 88
Resting diastolic
blood pressure
(mmHg)
Mean:
71.02±13.37
Median: 70.00
(59.50, 80.50)
60 90 80 68 80 68

72
Resting heart rate
(bpm)
Mean:
61.44±8.90
Median: 60.72
(55.51, 67.67)
71.83 55.82 67.71 58.78 77.19 50.48
Family history of
heart disease
(yes/no)
26/24 Yes Yes No Yes Yes Yes
Smoker (yes/no) 13/37 Yes No No No No No
Smoking history
(yes/no)
31/19 Yes No Yes No No No
Number of co-
morbidities
Mean:
1.74±1.24
Median: 2.00
(1.00, 2.25)
2 2 3 2 2 1
Functional
status
LTPAQ-SCI
(min/week)
Mean:
281.00±520.03
Median: 112.50
(0, 420.00)
120 240 30 380 NT 180
LEMS (/50) Mean:
10.84±16.55
Median: 0 (0,
22.75)
0 0 0 0 35 50

73
SCIM-III (/100) Mean:
61.08±21.28
Median: 67.50
(50.00, 74.25)
33 66 70 25 60 91
General Sleep apnea
(yes/no)
11/39 No No Yes No No No
Height (cm) Mean:
171.73±23.96
Median: 175.63
(167.91,
181.92)
182.88 180.34 183 172.72 183 178
Weight (kg) Mean:
79.24±16.96
Median: 81.20
(65.77, 89.10)
75.2 101.6 93 78.5 128.4 81.2
NA: not applicable; NT: not tested due to subject’s choice

74
Figure 1. Frequency distribution of the LF:HF plotted without the outliers for the entire sample.
LF:HF

75
Appendix E
The following appendix includes all the frequency distributions and boxplots for the secondary HRV indices when examined in the entire
sample. The numbers in the boxplots correspond with the SPSS cell numbers and not the subject numbers.

76
LF (ms2) LF (ms2)
HF (ms2) HF (ms2)

77
pNN50 (%) pNN50 (%)
RMSSD (ms) RMSSD (ms)

78
Appendix F
The following appendix includes the descriptive statistics of total power in the entire sample (Table 1)
and comparisons of total power based on level and/or severity of injury (Tables 2, 3 and 4).
Table 1. Descriptive statistics of total power in the entire sample (N=56)
Total Power
Mean ± SD 4233.51±5659.95
Median
(Lower, Upper quartile)
2192.24
(1229.12,5547.04)
IQR 4317.92
Skewness +3.41
Kurtosis 15.36
p-value† p<0.0001*
†Kolmogorov-Smirnov (K-S) test; p≤0.05*
Abbreviations: SD, standard deviation; IQR interquartile range
Table 2. Comparison of median total power based on level of injury
Below T5 (N=19) Above/Equal to
T5 (N=37)
p –Value†
Total Power
(ms2)
2121.44
(1264.10,6013.27)
2263.03
(1112.54,5177.26)
0.789†
†Mann-Whitney test; p≤0.05*

79
Table 3. Comparison of median total power based on severity of injury
Complete (N=38) Incomplete
(N=18)
p –Value
Total Power
(ms2)
2514.90
(1216.39,5078.26)
2035.08
(1181.18,7889.27)
0.847†
†Mann-Whitney test;
p≤0.05*
Table 4. Comparison of median total power based on level and severity of injury
Complete and
equal to/above
T5 (N=27)
Complete and
below T5 (N=11)
Incomplete and
equal to/above T5
(N=10)
Incomplete and
below T5 (N=8)
p –
Value
Total
Power
(ms2)
2516.98
(922.97,
4228.42)
2512.82
(1429.34,
6013.27)
2105.88
(1181.18,
11434.80)
1741.22
(876.03,
6067.28)
0.805†
†Kruskal-Wallis test; p≤0.05*

80
Appendix G
The following appendix includes all the boxplots representing the primary and secondary HRV indices based on level and severity of
injury. The numbers in the boxplots correspond with the SPSS cell numbers and not the subject numbers.
LF:H
F

81
HF
(ms2
)
LF (
ms2 )

82
pN
N5
0 (
%)
RM
SSD
(m
s)

83
Appendix H
The following appendix includes a total of seven tables: six tables comparing the scalar and categorical
HRV-related factor based on level and/or severity on injury, and one table summarizing the multiple
comparisons of the significant factors; p≤0.05 indicates that there was significant difference across the
cohorts.
Table 1. Comparison of the HRV-related factors based on level of injury
Median (Lower, Upper
quartile) or Mean ± Standard
deviation
Below T5 Above/equal
to T5
p –Value
Time post
injury
10.00
(6.00,22.00)
16.00
(5.00,22.00)
0.510†
BMI 27.15
(22.71,29.05)
26.58
(21.99,29.46)
0.883†
LTPAQ-SCI 120.00
(30.00,420.00)
120.00
(0.00,405.00)
0.668†
LEMS 7.00
(27.00,0.00)
0.00
(0.00,16.00
0.111†
SCIM-III 71.00
(77.00,64.00)
65.00
(32.00,72.00)
0.036†*
Number of
Comorbidities
2.00
(0.00,2.00)
2.00
(1.00,2.50)
0.179†

84
Age (years) 43.89 ±14.25 48.22 ±11.33
0.221§
Waist
circumference
(cm)
96.24 ±12.58 95.35 ±15.63 0.830
§
Relative VO2
peak
(ml/kg/min)
19.01 ±7.29 15.36 ±7.13 0.038
§*
Absolute
VO2 peak
(L/min)
1.56 ±0.75 1.15 ±0.44 0.088
§
Peak heart
rate (bpm)
141.37 ±25.14 123.45 ±29.64 0.033
§*
†Mann-Whitney test;
§ Independent t-test; p≤0.05*
Abbreviations: BMI, body mass index; LTPAQ-SCI, leisure time physical activity questionnaire-spinal
cord injury; LEMS, lower extremity motor score; SCIM-III, spinal cord independence measure
Table 2. Comparison of the HRV-related factors based on severity of injury
Median (Lower, Upper
quartile) or Mean ± Standard
deviation
Complete
Injury
Incomplete
Injury
p –Value
Time post
injury
17.50
(6.75,25.00)
6.00
(3.00,11.50)
0.001†***
BMI 26.84
(21.97,28.91)
27.06
(23.98,30.17)
0.352†

85
LTPAQ-SCI 80.00
(0.00,382.50)
225.00
(40.00,471.25)
0.106†
LEMS 0.00
(0.00,0.00)
33.00
(20.75,41.25)
<0.0001†***
SCIM-III 65.00
(43.50,71.00)
77.00
(55.25,91.00)
0.003†**
Number of
Comorbidities
2.00
(1.00,2.00)
1.50
(0.75,3.00)
0.622†
Age (years) 45.76 ±11.85 48.83 ±13.71
0.393§
Waist
circumference
(cm)
95.16 ±14.64 96.68 ±14.75 0.720
§
Relative VO2
peak
(ml/kg/min)
16.20 ±6.58 17.81 ±8.74 0.469
§
Absolute
VO2 peak
(L/min)
1.23 ±0.50 1.45 ±0.76 0.232
§
Peak heart
rate (bpm)
131.39
±32.30
128.06 ±22.38 0.705
§
†Mann-Whitney test;
§ Independent t-test; p≤0.05*; p≤0.01**; p≤0.001***
Abbreviations: BMI, body mass index; LTPAQ-SCI, leisure time physical activity questionnaire-spinal
cord injury; LEMS, lower extremity motor score; SCIM-III, spinal cord independence measure

86
Table 3. Comparison of HRV-related categorical characteristics based on level of injury
Below T5 Above/equal
to T5
p-value
Sex
(males/females)
14/5 30/7
p=0.516†
Current smoker
(no/yes)
13/6
29/8
p=0.518†
Smoking
history (no/yes)
7/12
16/21
p=0.645§
Family history
of heart disease
(no/yes)
8/11
17/20
p=0.784§
Sleep apnea
(no/yes)
14/5
30/7
p=0.516†
†Fisher exact test;
§Pearson chi-square; p≤0.05*
Table 4. Comparison of HRV-related categorical characteristics based on severity of injury
Complete
Injury
Incomplete
Injury
p-value
Sex
(males/females)
31/7
13/5
p=0.494†
Current
Smoker
(no/yes)
31/7
11/7
p=0.133†

87
Smoking
history (no/yes)
15/23
8/10
p=0.724§
Family history
of heart disease
(no/yes)
19/19
6/12
p=0.241§
Sleep apnea
(no/yes)
32/6
12/6
p=0.171†
†Fisher exact test;
§Pearson chi-square; p≤0.05*
Table 5. Comparison of the HRV-related factors based on level and severity of injury
Median (Lower, Upper
quartile) or Mean ± Standard
deviation
Complete and
equal to/above
T5
Complete and
below T5
Incomplete
and equal
to/above T5
Incomplete
and below T5
p –Value
Time post
injury
17.00
(6.00,26.00)
19.00
(7.00,24.00)
6.00
(3.75,17.00)
6.00
(3.00,9.00)
0.016†*
BMI 26.31
(21.98,28.86)
27.15
(20.53,29.05)
26.84
(23.25,34.54)
27.12
(23.43,29.27)
0.798†
LTPAQ-SCI 170.00
(0.00,420.00)
30.00
(0.00,120.00)
75.00
(0.00,317.50)
420.00
(217.50,607.5
0)
0.029†*
LEMS 0.00
(0.00,0.00)
0.00
(0.00,0.00)
37.50
(23.00,42.50)
26.50
(15.25,39.25)
<0.0001†***

88
SCIM-III 63.00
(25.00,70.00)
66.00
(61.00,71.00)
74.00
(39.00,81.75)
79.00
(66.75,95.25)
0.009†**
Number of
Comorbidities
2.00
(1.00,2.00)
2.00
(0.00,2.00)
1.50
(1.00,3.00)
1.00
(0.00,3.50)
0.583†
Age (years) 46.30 ±10.59 44.45 ±15.01 53.40 ±12.17 43.13 ±14.12 0.271§
Waist
circumference
(cm)
94.60 ±14.89 96.56 ±14.63 97.37 ±18.19 95.81 ±10.05 0.958
§
Relative VO2
peak
(ml/kg/min)
15.44 ±7.49 17.73 ±4.13 15.18 ±6.57 20.76 ±10.31 0.302
§
Absolute
VO2 peak
(L/min)
1.14 ±0.47 1.42 ±0.54 1.18 ±0.37 1.76 ±0.98 0.254
§
(Welch)
0.154§
(Brown-
Forsythe)
Peak heart
rate (bpm)
124.09
±34.04
146.00
±23.52
121.89
±15.78
135.00
±27.49 0.077
§
(Welch)
0.096§
(Brown-
Forsythe)
†Kruskal-Wallis test;
§One way ANOVA test; p≤0.05*; p≤0.01**; p≤0.001***
Abbreviations: BMI, body mass index; LTPAQ-SCI, leisure time physical activity questionnaire-spinal
cord injury; LEMS, lower extremity motor score; SCIM-III, spinal cord independence measure

89
Table 6. Follow up analysis on the HRV-related factors that were different based on level and
severity of injury
Time Post Injury
Adjusted Sig.
LTPAQ-SCI
Adjusted Sig.
LEMS
Adjusted Sig.
SCIM-III
Adjusted Sig.
Complete and
equal to/above T5
vs. Complete and
below T5
1.000 1.000 1.000 1.000
Complete and
equal to/above T5
vs. Incomplete and
below T5
0.073 0.173 0.000*** 0.010**
Complete and
equal to/above T5
vs. Incomplete and
equal to/above T5
0.152 1.000 0.000*** 0.257
Complete and
below T5 vs.
Incomplete and
below T5
0.156 0.019* 0.008** 0.491
Complete and
below T5 vs.
Incomplete and
equal to/above T5
0.305 1.000 0.001*** 1.000
Incomplete and
below T5 vs.
1.000 0.203 1.00 1.000

90
Incomplete and
equal to/above T5
†Kruskal-Wallis multiple comparison follow up test; p≤0.05*; p≤0.01**; p≤0.001***
Table 7. Comparison of HRV-related categorical subject characteristics based on level and
severity of injury
Complete and
equal
to/above T5
Complete and
below T5
Incomplete
and equal
to/above T5
Incomplete
and below T5
p-value
Sex
(males/females)
22/5
9/2
8/2
5/3
p=0.701†
Current smoker
(no/yes)
24/3
7/4
5/5
6/2
p=0.055†
Smoking
history (no/yes)
12/15
3/8
4/6
4/4
p=0.761†
Family history
of heart disease
(no/yes)
14/13
5/6
3/7
3/5
p=0.694†
Sleep apnea
(no/yes)
23/4
9/2
7/3
5/3
p=0.441†
†Fisher exact test;
§Pearson chi-square; p≤0.05*

91
Appendix I
The following appendix includes all the scatter plot of the LF and HF based on level and/or severity of injury.
LF (
ms2
)
LF (
ms2 )
HF (ms2) HF (ms2)

92
LF (
ms2 )
LF (
ms2 )
LF (
ms2
)
LF (
ms2 )
HF (ms2) HF (ms2)
HF (ms2) HF (ms2)

93
LF (
ms2 )
LF (
ms2 )
HF (ms2) HF (ms2)

94
Appendix J
The following appendix includes the scatter plots of the significant correlations between LF or HF and other selected HRV-related factors.
The factors include: age, time post injury and SCIM-III.
LF (
ms2 )
HF
(ms2 )

95
LF (
ms2 )
HF
(ms2
)

96
HF
(ms2 )

97
Appendix K
The following appendix includes the multiple linear regression tables to predict LF (Table 1) or HF
(Table 2) in individuals with a complete injury equal to/above T5.
Table 1. Multiple linear regression analysis to predict LF for individuals with a complete injury
equal to/above T5 cohort (R2=0.261)
Parameter Regression
Coefficient
95% CI p-value
Intercept -663.03 -4198.33,1651.80 0.661
Age -36.25 -76.21,-12.67 0.116
WC 25.33 -8.07,72.51 0.290
Peak heart rate 4.38 -3.94,17.48 0.403
*p≤0.05
Abbreviations: CI, confidence interval; WC, waist circumference
Table 2. Multiple linear regression analysis to predict HF for individuals with a complete injury
equal to/above T5 cohort (R2=0.261)
Parameter Regression
Coefficient
95% CI p-value
Intercept 830.89 -1434.01,3226.77 0.527
Age -14.67 -38.45,13.15 0.279
WC 4.89 -15.55,22.29 0.617
Peak heart rate 2.48 -7.11,12.61 0.637
*p≤0.05
Abbreviations: CI, confidence interval; WC, waist circumference