Embed Size (px)
Citation preview

Assessing Drug Transfer into Breast
Milk
Shinya Ito, MDHospital for Sick Children
Toronto, Canada

Four discussion points
•Why do we need data?•What data do we need?•Transporters in the mammary gland?
•Graded approach

1. Why do we need data?
• Uncertainty compromises breastfeeding– Antibiotics and Propylthiouracil
(PTU)
• Identifying a “TDM” drug– Lithium
• Identifying a “contraindicated” drug

• Morbidity (Infection) Diarrhea Dewey et al. Pediatrics 1995
Lower respiratory tract infection
Wright et al. BMJ 1989
Otitis mediaOwen et al. J Pediatr 1993
Bacteremia Takala et al. J Pediatr 1989
Bacterial meningitisCochi et al. J Pediatr 1986
NEC Lucas & Cole. Lancet 1990
Silva et al. Aust Ped J 1978Morley et al. Arch Dis Child 1988Lucas et al. Lancet 1992Pollock. Dev Med Child Neurol 1994Gale & Martyn. Lancet 1996Horwood & Fergusson Pediatrics 1998
• Cognitive function
IQ 8 pts
“No hard data” leads to formula-feeding by
default
• Compliance and antibiotics in breastfeeding (Ito et al. Ann Pharmacother 1993;27:40-42)
• PTU– labeling/imprinting
(Lee et al. Pediatrics 2000;106:27-30)

Propylthiouracil (PTU) and breastfeeding
Amounts excreted into milk<0.3% of the mother’s dose
on a weight basis
Low et al. Lancet 1979;2:1011Kampman et al. Lancet 1980;1:736-7Cooper. N Eng J Med 1984;311:1353-62
<10%

Eight infants Mother’s PTU (50-300 mg/day) Low T4/high TSH at birth Normalized despite breastfeeding
No effect on the thyroid gland of the breastfed infantMomotani et al. Clin Endocrinol 1989;31:591-5

• AAP (1989,1994): “compatible”
• Briggs/Freeman/Yaffe (1994): “no significant risk”
• Bennett/WHO (1988): “probably safe”
• CPS (2001): “contraindication”

Women on PTU do not start breastfeeding
0
50
100%
Control
Lee et al. Pediatrics 2000
PTU

Women on PTU do not start breastfeeding
0
50
100% Lee et al. Pediatrics 2000
Adviced by MDs
Breastfeeding
Formula

“TDM” drug
• TDM to individualize management
• % wt-adj maternal dose: >10%• large interindividual variation• dose-dependent effects • lithium as an example

Identifying contraindicated drug
•% wt-adj maternal dose: >10%• toxicity (dose-dependent,
dose-independent)•TDM unsuitable

2. What data do we need?
• To estimate infant exposure level– Infant dose (%wt-adj maternal dose)
• [C]milk and maternal dose
– Infant serum [C], PD endpoints– Exposure Index
• To assess effects on milk yield
• To assess transfer mechanisms, PK factors in [C]milk variations– MP ratio (maternal PK-[C]milk)

Exposure Index
EI (%) = MP ratio x 10
CL (ml/kg/min)
Ito & Koren 1994
EI>10%Phenobarbital 100%Ethosuximide 50%Atenolol 25%Lithium 2-30%Metronidazole 3-18%

3. Carrier-mediated systems
•clinical implications– interactions–potential intervention
•net transfer: may or may not deviate from a diffusion model

[Cmilk] [Cplasma]
Maternal plasmaMilk
EpitheliaMyoepithelia
pH 7.0 pH7.4
?Organic cation transporters
Diffusion +: McNamara lab

Organic cation transporters
•P-glycoprotein•Organic Cation Transporters(OCT1, OCT2, OCT3, OCTN1, and OCTN2, etc)

Human mammary gland
P-glycoprotein ???
hOCT1
hOCT212A

hOCTN1 and N2
hOCTN2
800 base pairproduct
hOCTN1
785 base pairproduct

P-gp expression in MCF12A
MRK16
intracellular surface
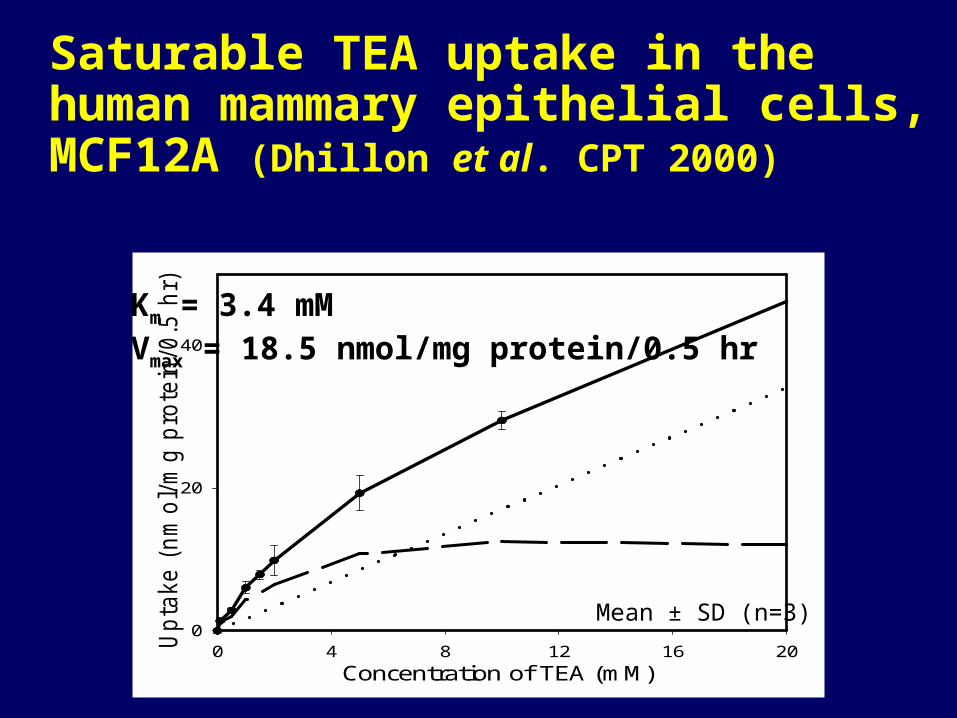
Saturable TEA uptake in the human mammary epithelial cells, MCF12A (Dhillon et al. CPT 2000)
Concentration of TEA (mM)0 4 8 12 16 20U
pta
ke (
nm
ol/m
g p
rote
in/0
.5 h
r)
0
20
40
Mean ± SD (n=3)
Km = 3.4 mMVmax = 18.5 nmol/mg protein/0.5 hr

time (min)
0 20 40 60 80 100 120 140 160 180 200
upta
ke (
pm
ol/
106
cells)
0
20
40
60
80
100
120
140
Mean ± SD (n=3)
Carnitine uptake results
with Na+
without Na+
4oC

Saturable carnitine uptake in MCF12A (Kwok et
al. CPT 2001)
[carnitine] mM
0.00 0.01 0.02 0.03 0.04 0.05 0.06 0.07
upta
ke (
pm
ol/106
cells
/hr)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
Mean ± SD (n=3)
Km = 1.9 MVmax = 158 pmol/106 cells/hr

[inhibitors] mM
10-7 10-6 10-5 10-4 10-3 10-2 10-1 100 101 102
perc
enta
ge c
arni
tine
upta
ke
0
20
40
60
80
100
120
140
Inhibitor specificity
CarnitineCimetidineTEACholineGuanidine
Mean ± SD (n=3)
inhibition
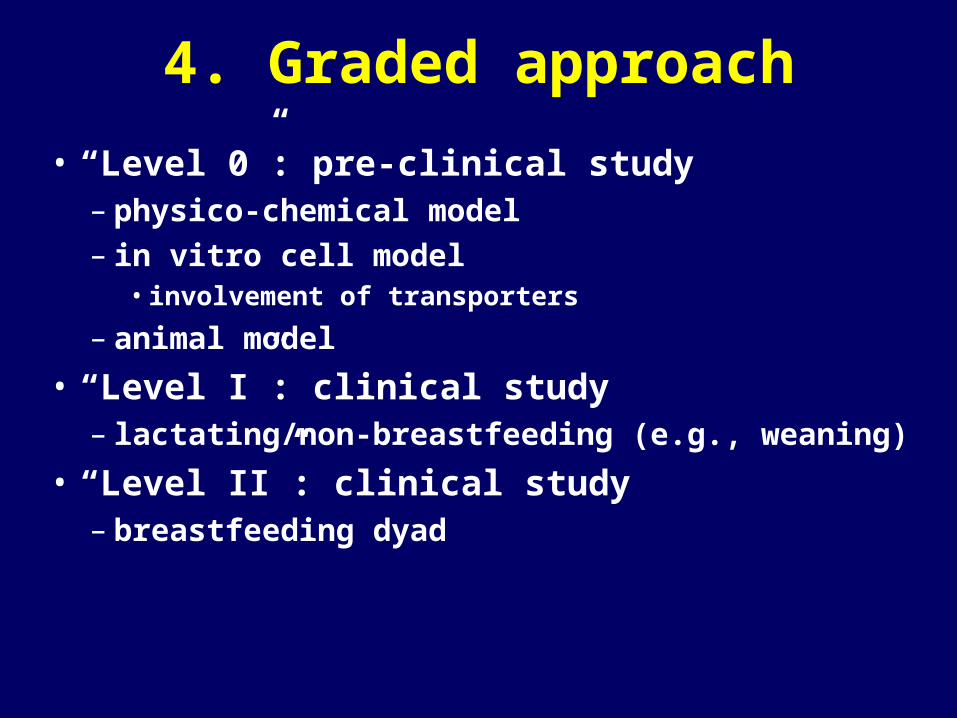
4. Graded approach
• “Level 0”: pre-clinical study– physico-chemical model– in vitro cell model
• involvement of transporters
– animal model
• “Level I”: clinical study– lactating/non-breastfeeding (e.g., weaning)
• “Level II”: clinical study– breastfeeding dyad

“Level 0” Preclinical Study
• various models• predict in vivo [C]milk,
transport systems etc.• potential effects on prolactin
etc.• provide ethical framework for
human experimentation

“Level I” Clinical Study
• lactating/non-breastfeeding women
• dose-[C]milk (AUC): infant dose, %wt-adj maternal dose
• MP ratio: Exposure Index – in colostrum, transitional, and
mature milk; in foremilk and hindmilk

“Level II” Clinical Study
• breastfeeding dyad• dose-[C]milk to estimate
variations• [C]infant • PD endpoints
– infant effects– milk yield





























