Embed Size (px)
Citation preview
Assess current standardsAssess current standardsDiscuss diagnostic methodsDiscuss diagnostic methodsHighlight new advancesHighlight new advancesDiscuss unique populationsDiscuss unique populationsReview open abdomen management optionsReview open abdomen management options
IAH and ACS recognized entitiesIAH and ACS recognized entitiesBladder pressures accepted standardBladder pressures accepted standardAbdominal decompression accepted standardAbdominal decompression accepted standardTowel clip and skin closure abandonedTowel clip and skin closure abandonedRisk Factors in trauma identifiedRisk Factors in trauma identifiedACS considered Ischemia/ReperfusionACS considered Ischemia/Reperfusion
IAH: IAP > 12 mmHgIAH: IAP > 12 mmHgACS: IAP > 20 mmHg and ACS: IAP > 20 mmHg and causing organ dysfunctioncausing organ dysfunctionPrimary ACS Primary ACS SecondarySecondary ACS Recurrent ACSRecurrent ACS
GRADE IGRADE I IAP = 12 IAP = 12 –– 15 mmHg15 mmHg
GRADE IIGRADE II IAP = 16 IAP = 16 –– 20 mmHg20 mmHg
GRADE IIIGRADE III IAP = 21 IAP = 21 –– 25 mmHg25 mmHg
GRADE IVGRADE IV IAP IAP >25 mmHg>25 mmHg
WWW.WSACS.ORG
ACS as ACS as ““second hitsecond hit””Key time: 8 hrs, earlier and later had less MOF, Key time: 8 hrs, earlier and later had less MOF, better recoverybetter recovery
Rezende. Shock Oct 2003.Rezende. Shock Oct 2003.
IAP 15mmHg for 24 hrIAP 15mmHg for 24 hrDecreased UOP, normal CI, normal labsDecreased UOP, normal CI, normal labsLow grade Necrosis liver, kidney, bowelLow grade Necrosis liver, kidney, bowel
IAP 30mmHg for 24 hrIAP 30mmHg for 24 hrAnuric, decreased CI, Increased lactate, Cr, LFTAnuric, decreased CI, Increased lactate, Cr, LFTModerate necrosis liver, kidney, bowelModerate necrosis liver, kidney, bowel
Toens. Shock. Oct 2002.Toens. Shock. Oct 2002.
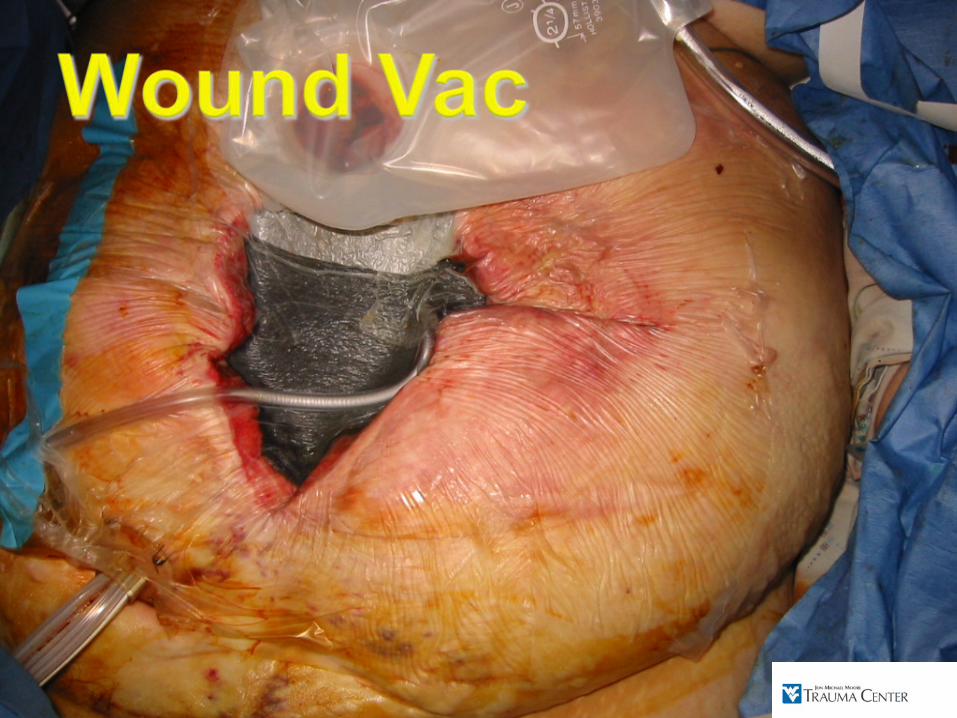
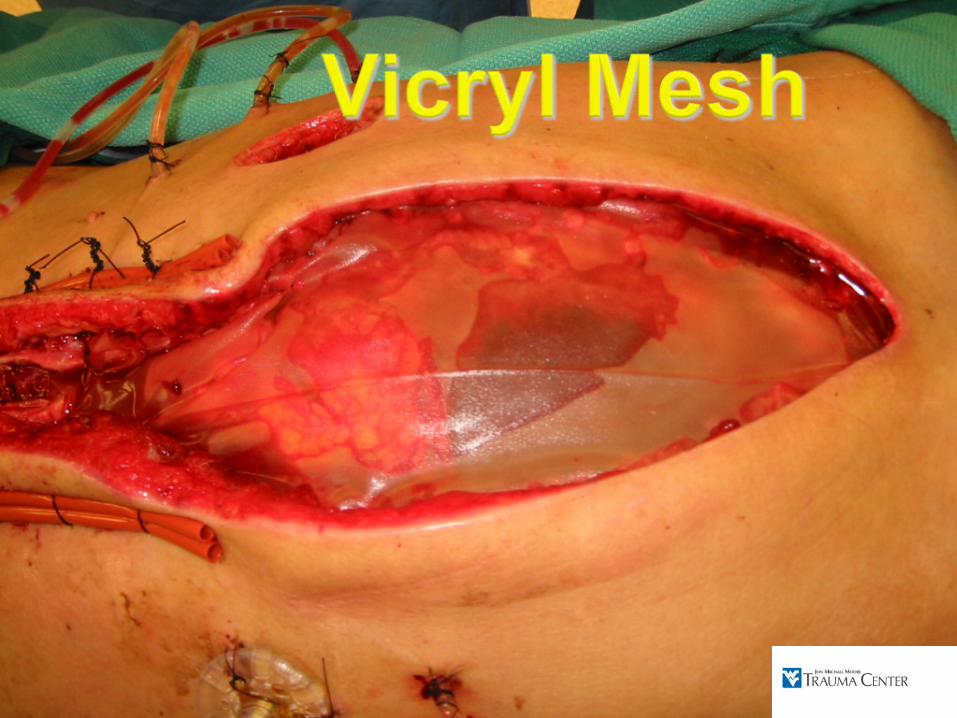
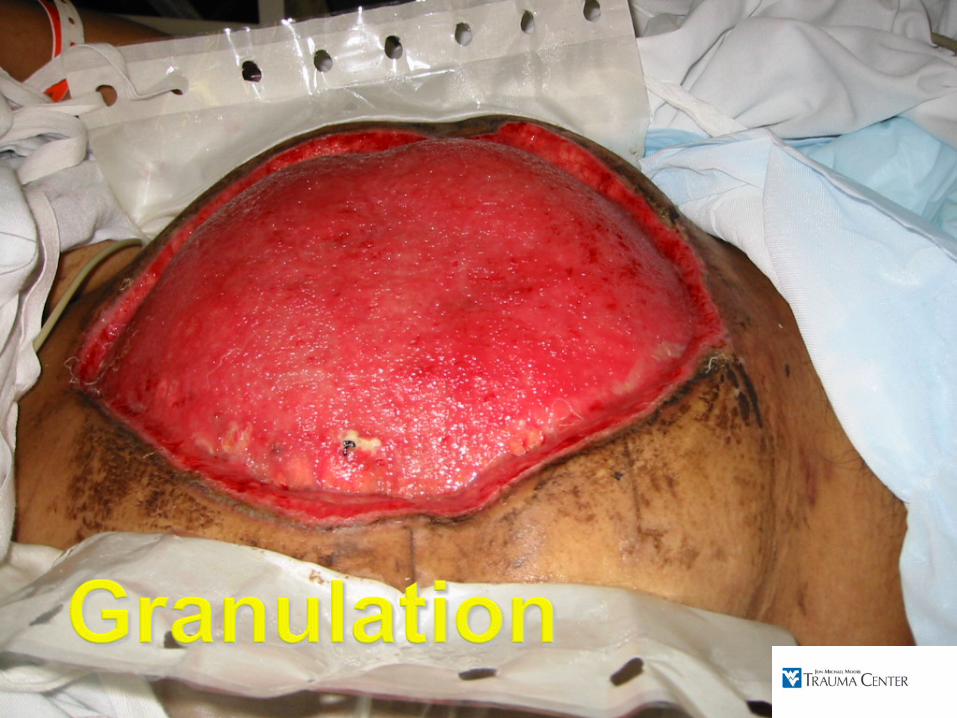
Measuring and monitoringUnique PopulationsInterventions/TherapyManaging the Open AbdomenClosure
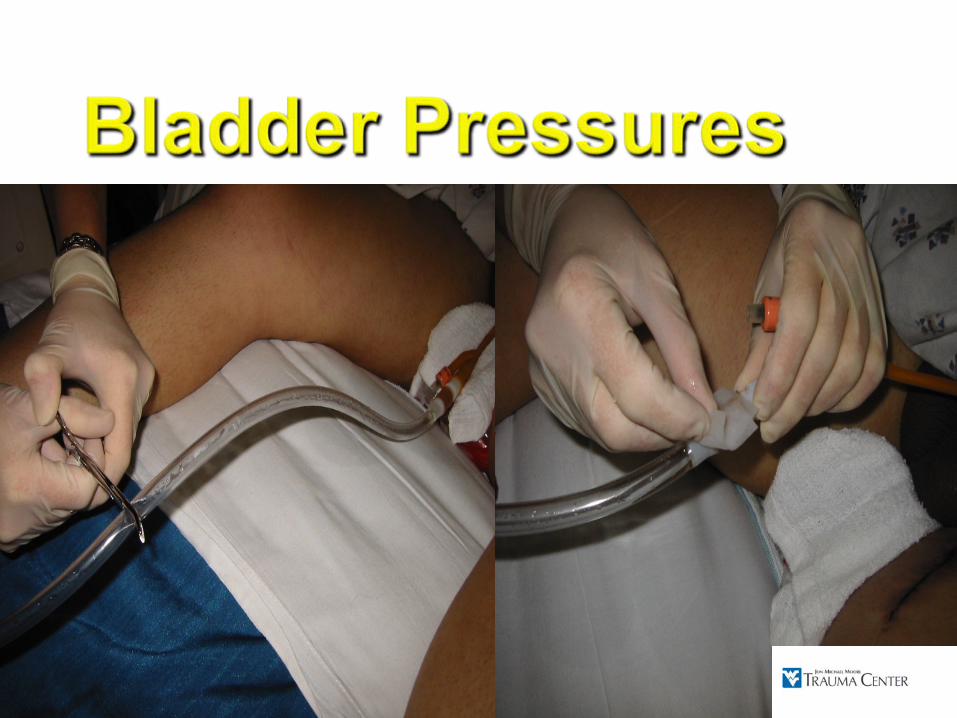
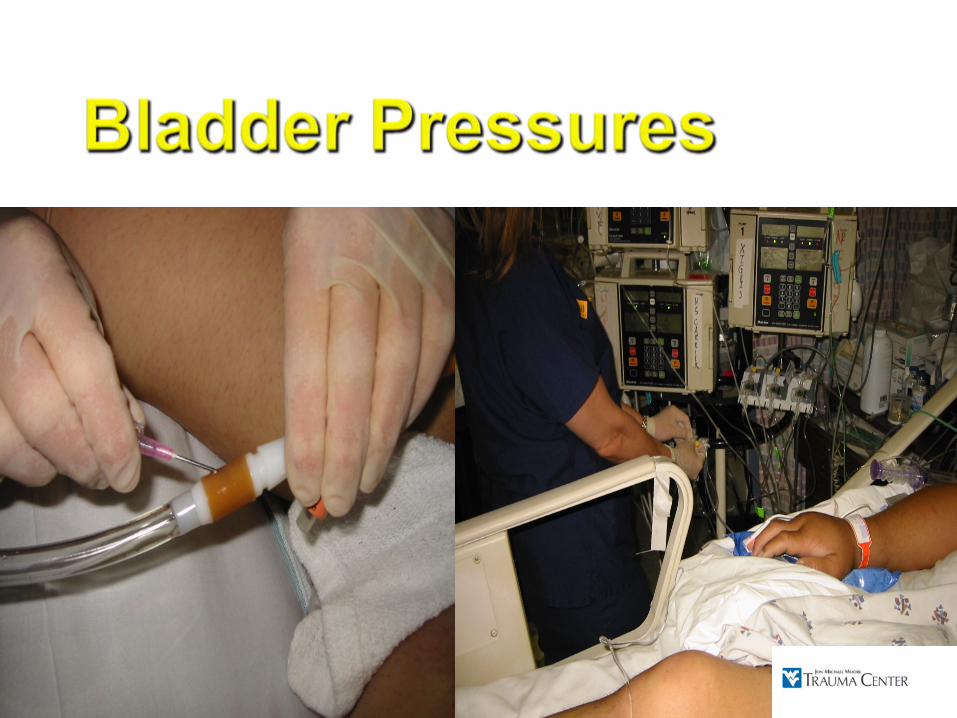
Bladder PressuresBladder Pressures◦
Normal 0-6 mmHg
Sanchez. Am Surg. Mar 2001.◦
⇑
BMI – mean IAP 9 mmHg↑.14 mmHg/ unit BMI increase
◦
Continuous vs IntermittentJ Trauma 64(5) 2008
◦
Watch units: cm H2 O vs mm Hg◦
Body position does matter - supine◦
Midaxillary line at iliac crest
DeWaele. Intensive Care Med. July 2008
EvolutionEvolution◦◦
Started: 100mlStarted: 100ml◦◦
50ml50ml◦◦
Currently: 25 ml (WSACS)Currently: 25 ml (WSACS)◦◦
NewNew
10ml (De Waele Intensive Care Med 2006)10ml (De Waele Intensive Care Med 2006)2ml (De latet Intensive Care Med 2008)2ml (De latet Intensive Care Med 2008)
Abdominal Perfusion PressureAbdominal Perfusion PressureMAPMAP--IAPIAP
Cheatham. J Trauma. Oct 2000.Cheatham. J Trauma. Oct 2000.
Doppler UltrasoundDoppler UltrasoundFlow dynamics in vasculatureFlow dynamics in vasculature
NearNear--infared Spectroscopyinfared SpectroscopyExperimentalExperimentalMuscle and stomach reflective of mesenteric flowMuscle and stomach reflective of mesenteric flow
Varela. Surgery. Mar 2001.Varela. Surgery. Mar 2001.Widder. J Trauma 2008Widder. J Trauma 2008
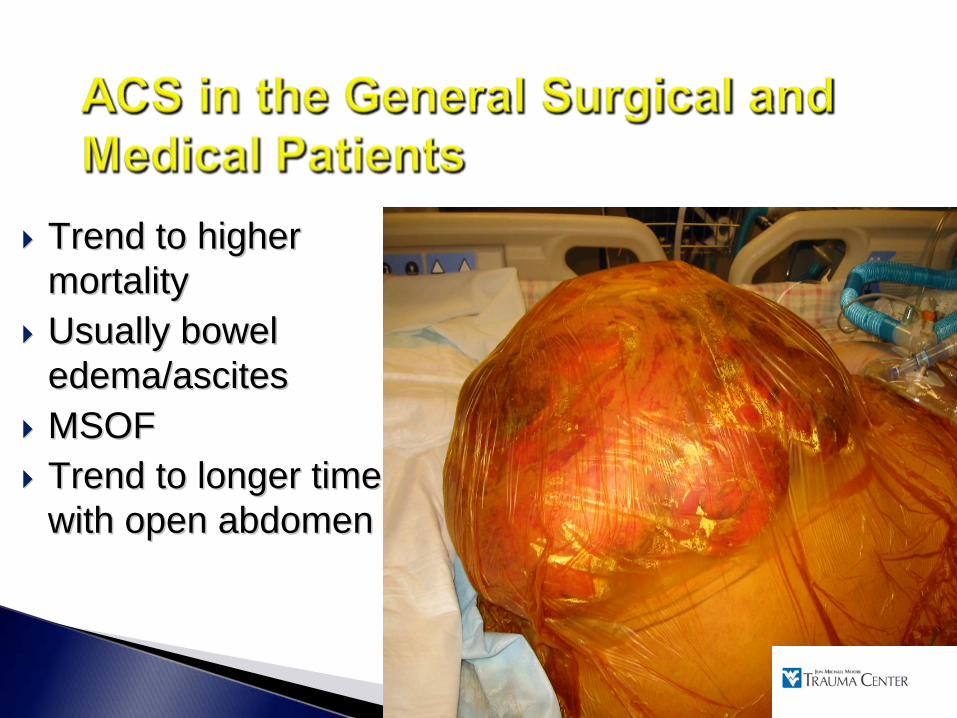
Trend to higher Trend to higher mortalitymortalityUsually bowel Usually bowel edema/ascitesedema/ascitesMSOFMSOFTrend to longer time Trend to longer time with open abdomenwith open abdomen
Incidence of IAH: 50 Incidence of IAH: 50 -- 60%60%Incidence of ACS: 10 Incidence of ACS: 10 -- 12%12%
80% mortality w/o intervention80% mortality w/o intervention
Associated with high vol. Associated with high vol. ResuscitationResuscitation
> 6 L in 6 hours> 6 L in 6 hours>15 L in 24 hours>15 L in 24 hours
Malbrain Int. Care Med 2006Malbrain Int. Care Med 2006
IAP > 12 mmHgIAP > 12 mmHg↑↑ ICU Length of StayICU Length of Stay↑↑ MortalityMortalityIndependent risk for Death (OR 2.52)Independent risk for Death (OR 2.52)
Reintam Intensive Care Med. May 2008Reintam Intensive Care Med. May 2008
Mortality: 52% vs 27%Mortality: 52% vs 27%Vidal Crit Care Med. June 2008Vidal Crit Care Med. June 2008
Mortality 40Mortality 40--67%67%Associated extremity compartment syndrome 33%Associated extremity compartment syndrome 33%Does not respond to volume loadingDoes not respond to volume loadingSupranormal resuscitation (DOSupranormal resuscitation (DO22I> 600ml/min/mI> 600ml/min/m22
significantly increased ACSsignificantly increased ACSBalogh. Arch Sur. June 2003.
Major abdominal vascular and mesenteric vessel injuryMassive transfusion and crystalloid requirementsContaminationProfound shockAcidosis, Hypothermia, and Coagulopathy
Abdominal compartment syndrome developed in 36% of patients Significant increase in LOS, ICU days, MSOF and mortalityKey Predictive Factor◦
Early elevation of peak airway pressures
Moore et al, Am J Surg Dec 2001
Resuscitation fluid Resuscitation fluid requirementrequirement?Incidence?IncidenceIntermittent peritoneal Intermittent peritoneal drainage as alternativedrainage as alternative
Latenser. J Burn Care Rehab. Latenser. J Burn Care Rehab. May 2002May 2002
40% survival 40% survival improvement if improvement if decompresseddecompressed
Hobson. J Trauma. Dec 2002.Hobson. J Trauma. Dec 2002.
Critically ill pedsCritically ill pedsMean IAP = 7 mmHgMean IAP = 7 mmHgSimilar despite wtsSimilar despite wts00--10kg, 1010kg, 10--20kg, 2020kg, 20--50kg50kgVariable mean optimal Variable mean optimal volumevolumeMin Optimal Vol = Min Optimal Vol = 3ml3ml◦◦
Ejike CCM. Jul 2008Ejike CCM. Jul 2008
Refractory Refractory ↑↑ ICPICPDecompressive Decompressive CraniectomyCraniectomyDecompressive Decompressive LaparotomyLaparotomySequence can varySequence can varyICP ICP ↓↓ 10mmHg10mmHgTransient = badTransient = bad






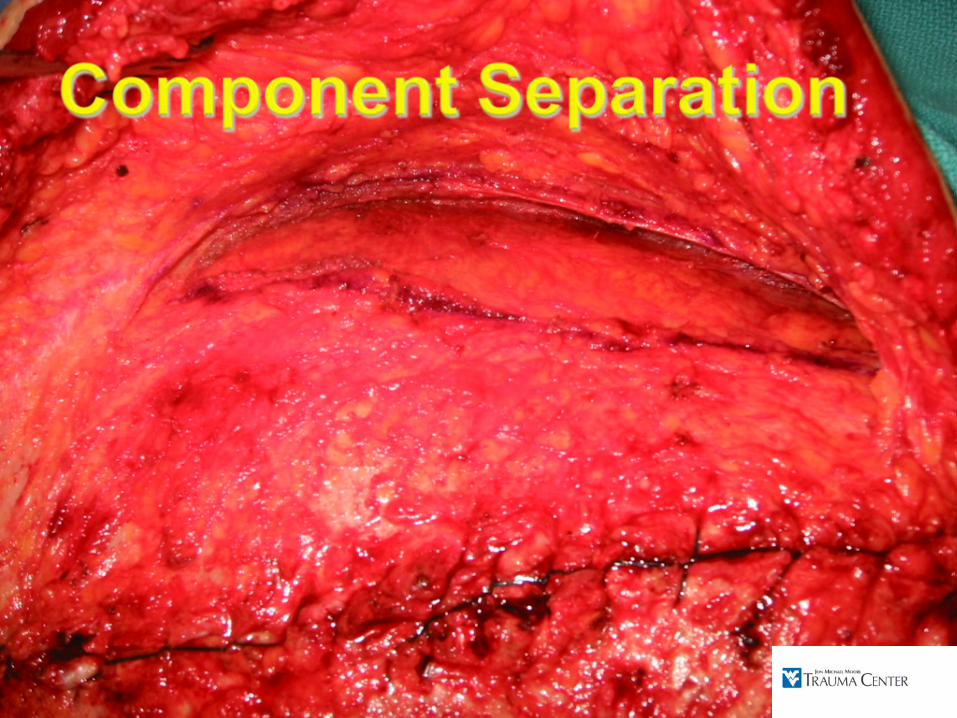
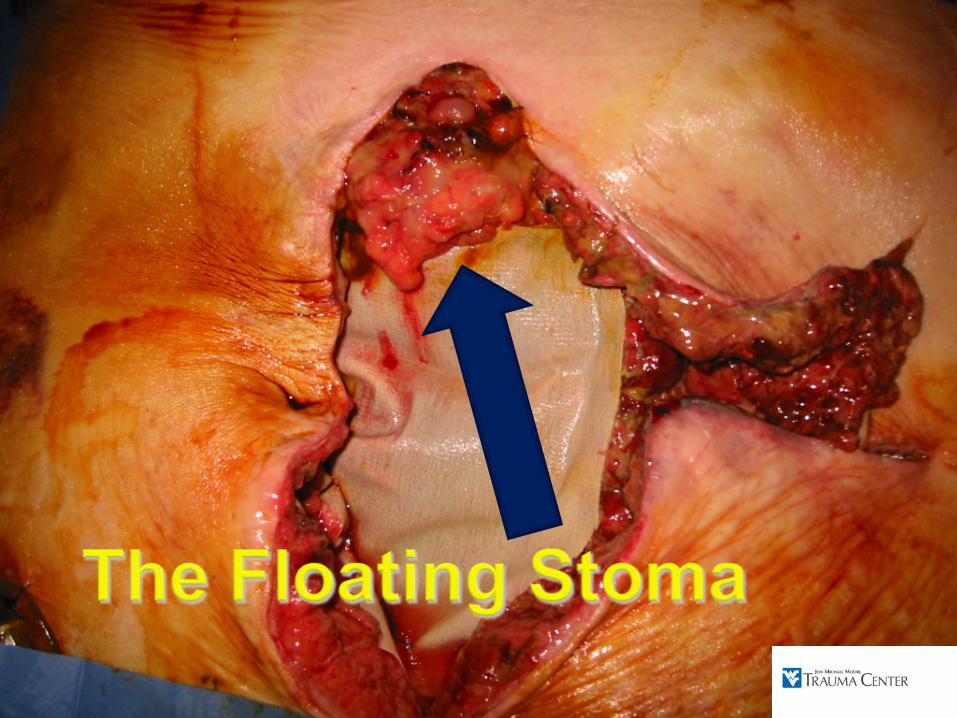
Giant herniaGiant herniaEnterocutaneous fistulaEnterocutaneous fistulaInfectionInfectionGI tract accessGI tract accessNeed for ostomyNeed for ostomy

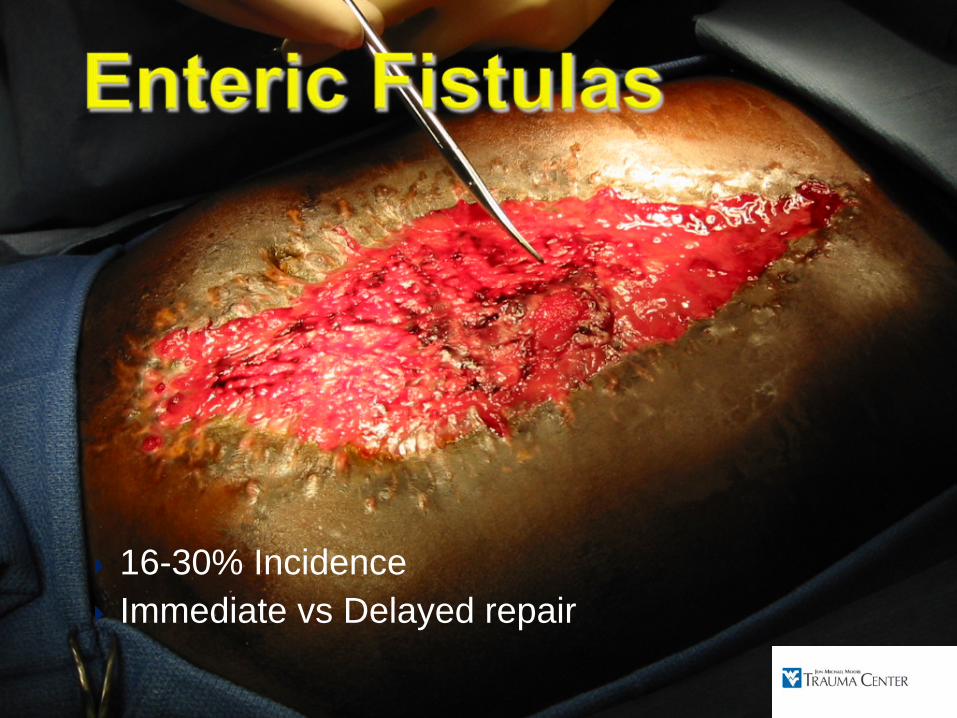
16-30% IncidenceImmediate vs Delayed repair

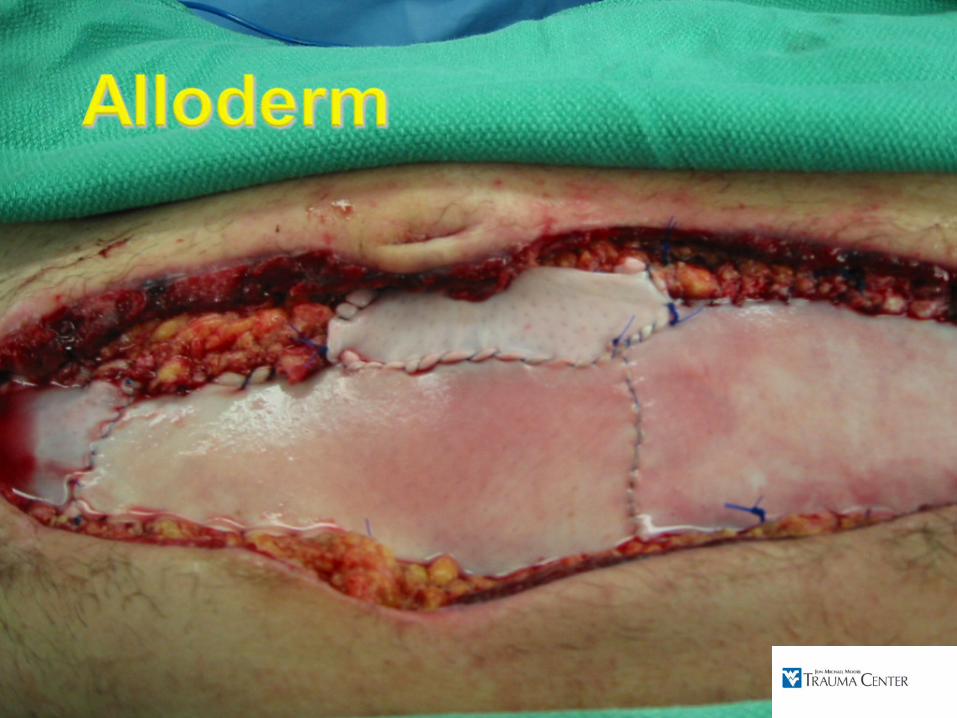
ACS/IAH more prevalent than previously recognizedACS/IAH more prevalent than previously recognizedSicker patients surviving Sicker patients surviving –– dilemmas in feeding, dilemmas in feeding,
closure, long term complicationsclosure, long term complicationsDiverse populationDiverse populationVariety of options for closure/coverageVariety of options for closure/coverage