Embed Size (px)
Citation preview

Aspirin – It Isn’t for Everyone Anymore
John L. Petersen II, MD, MHS
Medical Director, CV Research and Education Swedish Heart and Vascular Institute
T
CONFIDENTIALITY NOTICE: Confidential and Privileged Quality Information per Washington State Law (RCW 4.24.240, RCW 43.70.510, and RCW 70.41.200) and Federal Statutes.

Disclosures • Speaker: CSI • Education Grants: Boston Scientific, CSI, Abbot
Vascular, Philips • Investigator Research Grants: Abbott Vascular, CSI • Clinical Trial Participation: Novartis, Kiniksa,
SinoMed, Svelte Medical, • Clinical Trial Operations DSMB: Keystone CEC:
Biosensors • Stock/Ownership: Veravanti
2

Objectives • Review Aspirin’s Development and Mechanism of
Action
• Recapitulate Recent Studies Regarding Aspirin Use, Prevention of Cardiovascular Disease, and Combined Therapies
• Discuss Guideline Changes and Gaps in Recommendations
• Consider Implications for Changes in Practice
3

Managing Clot is Important in Cardiovascular Disease
4

Unfortunately Different Diseases Create Different Types of Clot
5

6
And the Consequences Can Be Bad

Prevention is Better than Cure
7

Historical Perspective of Salicylates
8

Prostaglandin Synthesis and Effects
9

Mechanism of Action – Cox-1 Inhibition
10

Aspirin and Anticoagulation No Long Term Anticoagulation Indicated • Primary Cardiac Prevention
– Is Aspirin Creating Harm? – Better Risk Factor
Modification Has Reduced Need
• Secondary Cardiac
Prevention – Aspirin is Still Felt to Have a
Strong Indication after ACS – Debate about correct dose – DAPT after Elective PCI – Aspirin Resistance
Long Term Anticoagulation Indicated • Primary Cardiac Prevention
– No Evidence that Aspirin Adds Value to Anticoagulation
• Secondary Cardiac
Prevention – Is Aspirin Creating Harm as a
Component of Triple Therapy?
11

Primary Prevention – USPSTF 2014
12
Population Recommendation Grade (What's This?)
Adults aged 50 to 59 years with a ≥10% 10-year CVD risk
The USPSTF recommends initiating low-dose aspirin use for the primary prevention of cardiovascular disease (CVD) and colorectal cancer (CRC) in adults aged 50 to 59 years who have a 10% or greater 10-year CVD risk, are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose aspirin daily for at least 10 years.
B
Adults aged 60 to 69 years with a ≥10% 10-year CVD risk
The decision to initiate low-dose aspirin use for the primary prevention of CVD and CRC in adults aged 60 to 69 years who have a 10% or greater 10-year CVD risk should be an individual one. Persons who are not at increased risk for bleeding, have a life expectancy of at least 10 years, and are willing to take low-dose aspirin daily for at least 10 years are more likely to benefit. Persons who place a higher value on the potential benefits than the potential harms may choose to initiate low-dose aspirin.
C
Adults younger than 50 years
The current evidence is insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of CVD and CRC in adults younger than 50 years.
I Adults aged 70 years or older
The current evidence is insufficient to assess the balance of benefits and harms of initiating aspirin use for the primary prevention of CVD and CRC in adults aged 70 years or older.
I

Physician’s Health Study
13

ARRIVE Trial CV Death, MI, UA, Stroke or TIA
14

ARRIVE Trial
15

16
ASCEND Trial

ASPREE Trial Cardiovascular Events
17

ASPREE Trial Bleeding events
18

Meta-Analysis
19

ACC AHA Prevention Guidelines 2019
20

ACC AHA Stable Ischemic Heart Disease 2012
21

ACC AHA STEMI Guidelines 2012
22

ISIS-2 STEMI Patients
23

ACC AHA UA/NSTEMI Guidelines 2014
24

ACC AHA UA/NSTEMI Guideline 2014
25

Danish National Patient Registry Atrial Fibrillation Patients (N= 82854)
26

VKA (INR 2–3)
Apixaban 5 mg BID Apixaban 2.5 mg BID in selected patients
Primary outcome: ISTH major / CRNM bleeding Secondary outcome(s): death / hospitalization, death / ischemic events
Randomize n=4600 patients
INCLUSION •Atrial fibrillation (prior, persistent, >6 hr) –Physician decision for OAC •Acute coronary syndrome or PCI –Planned P2Y12 inhibitor for ≥6 months
EXCLUSION •Contraindication to DAPT •Other reason for VKA (prosthetic valve, moderate / severe mitral stenosis)
AUGUSTUS Trial Design
Aspirin for all on the day of ACS or PCI Aspirin versus placebo after randomization
Open Label
Aspirin Placebo Double Blind Aspirin Placebo Double
Blind
Lopes RD, et al. Am Heart J. 2018;200:17-23.

VKA + Placebo (27.3%)
Apixaban + Placebo (22.0%) Apixaban + Aspirin (24.9%)
VKA + Aspirin (27.5%)
AUGUSTUS Trial Death / Hospitalization
Apixaban + Placebo vs. VKA + Aspirin: 5.5% absolute risk
reduction (NNT=18)

VKA + Aspirin (18.7%)
Apixaban + Aspirin (13.8%)
Apixaban + Placebo (7.3%)
VKA + Placebo (10.9%)
AUGUSTUS Trial Major / CRNM Bleeding
Apixaban + Placebo vs. VKA + Aspirin: 11.4% absolute risk reduction (NNT=9)

30

31

32

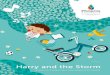
PIONEER AF-PCI
• Clinically significant bleeding: 16.8% in group 1 vs. 18.0% in group 2 vs. 26.7% in group 3 (HR 0.59, p < 0.001 for group 1 vs. 3); (HR 0.63, p < 0.001 for group 2 vs. 3)
• Stent thrombosis: 0.8% in group 1 vs. 0.9% in group 2 vs. 0.7% in group 3 (HR 1.20, p = 0.79 for group 1 vs. 3; HR 1.44, p = 0.57 for group 2 vs. 3)
Trial design: Patients with AF and PCI randomized to: Group 1: Rivaroxaban 15 mg daily plus P2Y12 inhibitor for 12 months (n = 709). Group 2: Rivaroxaban 2.5 mg twice daily plus DAPT for 1-12 months (n = 709). Group 3: warfarin plus DAPT for 1-12 months (n = 706).
Results
Conclusions • Among patients with nonvalvular AF who
underwent PCI, a rivaroxaban-based strategy was associated with a lower frequency of clinically significant bleeding compared with a warfarin/DAPT strategy
• Stent thrombosis appeared to be similar between the three groups
Gibson CM, et al. N Engl J Med 2016;375:2423-34
(p < 0.001 for group 1 or 2 vs. group 3)
Rivaroxaban 15 mg daily, P2Y12 for 12 months
Rivaroxaban 2.5 mg daily, DAPT for 1-12 months
Warfarin, DAPT for 1-12 months
% 16.8 18.0
26.7

400 Volunteers Platelet Aggregation with Arachadonic Acid Assay
34

35

In vivo vs Ex vivo treatment of “non responders”
36

Weight Based Dosing
37

Weight Based Dosing
38

Optimizing Aspirin Effectiveness
• Use the lowest dose • Bid dosing in DM and ET • Non-enteric formulas • Improve adherence • Avoid NSAIDs • Avoid Steroids • Consider PPI for GI Risk
• Maximize Efficacy • High platelet turnover • Ensure absorption • Avoid “resistant” label • Competitive agonist • GI bleeding • If steroids or NSAID
necessary
39

Conclusions • Aspirin is a wonder drug
– Cheap and Effective, Prevents Deadly Diseases
• Which patients to treat still remains debated – Much more restrictive for primary prevention
• Minimize Triple Therapy – Dropping aspirin and continuing P2Y12 Drugs (clopidogrel,
ticagrelor, prasugrel)
• There is no such thing as true aspirin resistance (or if there is, its very rare and reportable) – Poor Response Related to absorption, interactions, drug
formulation, increased platelet turnover
40

ACC AHA Guidelines • 1990: Current Recommendations Class I • 1. Aspirin (160 mg/day) should be started as soon as
the patient is admitted and given daily until discharge from the hospital, at which time it can be continued at a dose of 160 to 325 mg daily.
• 1996: Aspirin Recommendations • Class I. A dose of 160 to 325 mg should be given on
day 1 of acute MI and continued indefinitely on a daily basis thereafter.
• Class lIb 1. Other antiplatelet agents such as dipyridamole or ticlopidine may be substituted if true aspirin allergy is present.
41

• 1999 Aspirin Update • Class IIb Other antiplatelet agents such as
dipyridamole,ticlopidine, or clopidogrel may be substituted if trueaspirin allergy is present or if the patient isunresponsive to aspirin
42

Aspirin as an Anticoagulant • 1945 Identified as
causing more bleeding following tonsillectomy
• Also used as analgesic during angina
• 1953 Craven studied as primary prevention
• 1st RCT 1974, Trends toward benefit
• 1980 Peto Meta-analysis demonstrating reduction in MI
43