Embed Size (px)
Citation preview

Asphyxia
Objectives:
• To define asphyxia and hypoxic ischemic encephalopathy and other related terms including the criteria
• To discuss the risk factors, causes and pathophysiology including affected organs
• To discuss the clinical manifestations and staging of HIE.
• To discuss diagnostics, treatment, and newer modalities.

Asphyxia
I. Definition of terms
A. - Asphyxia is also termed as Hypoxic-Ischemic
Encephalopathy (HIE)
– AAP and ACOG recommend using HIE because this term accurately describes the clinical condition, encephalopathy from asphyxia, without implying the time of brain injury

Asphyxia
I. Definition of terms
A. Hypoxic-Ischemic Encephalopathy
- Condition of impaired blood gas exchange during
the intrapartum period which may lead to
progressive hypoxemia and hypercapnea with
metabolic acidosis.
-This is an important cause of permanent damage
to CNS tissues that may result to neonatal death
or manifest later as developmental delay.

Asphyxia
I. Definition of terms
B. Hypoxemia • Refers to decreased arterial concentration of
oxygen
C. Hypoxia• Refers to decreased oxygenation to cells or organs.
D. Ischemia• Refer to blood flow to cells or organs that is
insufficient to maintain normal function.

Asphyxia
• Criteria
1. Evidence of metabolic acidosis (pH < 7.0 BE > 12mmol/L
2. Early onset of severe/moderate encephalopathy
3. Apgar 0-3 at 5 minutes of life
4. Multi organ involvement

Asphyxia
• 20-30% of HIE cases are in the neonatal period
• 33-50% of the survivors are left with permanent neurodevelopmental abnormalities (cerebral palsy, mental retardation).
• Greatest risk factors:– (ABG) pH of < 6.7 has 90% mortality and/or impairment– (ABG) base deficit > 25 mmol/L has 72% mortality

Risk factors
Antepartum :Maternal diabetes post-term gestation
Pregnancy induced hypertension multiple gestation
Chronic hypertension size-dates discrepancy
Previous Rh sensitization maternal drug abuse
Previous stillbirth maternal age >35 or<16
Bleeding in second or third trimester no prenatal care
Maternal infection
Polyhydramnios or oligohydramnios

Risk factors
Intrapartum :Elective or emergency c/s
Precipitous labour, prolonged labour
Prolonged second stage of labour
Premature labour
Abnormal presentation
Rupture of membranes > 24 hours
Foul-smelling amniotic fluid
Non reassuring fetal heart rate patterns
Use of general anesthesia
Prolapsed cord

Asphyxia
II. Causes and Pathophysiology
• The main cause of asphyxia is decreased in O2 supply resulting to hypoxia and ischemia.
• Fetal hypoxia may to caused by the following mothers conditions:
a. Hypotension due to acute blood loss spinal
anesthesia, or compression of veno cava
b. Inadequate maternal oxygenations due to cyanotic
heart disease, anesthesia, or respiratory failure.

Asphyxia
II. Causes and Pathophysiology
c. inadequate relaxation of uterus to permit
placental filling
d. Premature separation of the placenta
e. impedance to the circulation of blood through the
umbilical cord
f. placental insufficiency

Asphyxia
II. Causes and Pathophysiology
• Postnatal causes of hypoxia
a. Failure of oxygenation as a result of severe cyanotic
CHD or severe pulmonary disease
b. Severe anemia
c. Shock

Multiorgan Systemic Effects of Asphyxia
SYSTEM EFFECT
Central nervous system Hypoxic- ischemic encephalopathy, infarction, intracranial hemorrhage, seizures, cerebral edema, hypotonia, hypertonia
Cardiovascular Myocardial ischemia, poor contractility, cardiac stun, tricuspid insufficiency, hypotension
Pulmonary Pulmonary hypertension, pulmonary hemorrhage respiratory distress syndrome
Renal Acute tubular or cortical necrosis
Adrenal Adrenal hemorrhage
Gastrointestinal Perforation, ulceration with hemorrhage necrosis
Metabolic Inappropriate secretion of antidiuretic hormone, hyponatremia, hypoglycemia, hypocalcemia, myoglobinuria
Integument Subcutaneous fat necrosis
Hematology Disseminated intravascular coagulation

Asphyxia
III. Clinical Manifestations
• Fetal period:
1. Fetal heart rate slows and beat to beat variability
declines.
2. Deceleration pattern of fetal monitoring
A. Early
B. Late
C. Variable

. Hon EH: An Atlas of Fetal Heart Rate Patterns. New Haven, CT, Harty Press, 1968.)
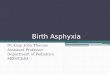
Patterns of periodic fetal heart rate (FHR) deceleration
A shows early deceleration occurring during the peak of uterine contractions as a result of pressure on the fetal head

. Hon EH: An Atlas of Fetal Heart Rate Patterns. New Haven, CT, Harty Press, 1968.)
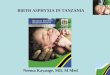
Patterns of periodic fetal heart rate (FHR) deceleration
C, Variable deceleration as a result of umbilical cord compression

. Hon EH: An Atlas of Fetal Heart Rate Patterns. New Haven, CT, Harty Press, 1968.)
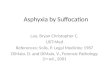
Patterns of periodic fetal heart rate (FHR) deceleration
B, Late deceleration caused by uteroplacental insufficiency

Asphyxia
III. Clinical Manifestations
• Post natal Period:
1. depressed and may fail to breath spontaneously
2. hypotonic or may change to hypertonic state (* may
also remain normal)
3. Pallor, cyanosis, apnea, bradycardia

Asphyxia
III. Clinical Manifestations
• Post natal Period:
4. Brain edema may develop
- seizure
- any change in sensorial activity
5. Multi organ failure• Ex. Acute tubular necrosis, necrotizing enterocolitis,
myocardial infarction.

Topography of Brain Injury in terms infants with hypoxic ischemic encephalopathy and clinical correlates
Area of Injury Location of Injury Clinical Correlate Long term sequelae
Selective neuronal necrosis
Entire neuroaxis, deep cortical area, brainstem and pentocubicular
Stupor or comaSeizuresHypotoniaOculomotor abnormalitiesSuck/swallow abnormalities
Cognitive delayCerebral palsyDystoniaSeizure disorderAtaxiaBulbar and pseudobulbar palsy
Parasagittal injury Cortex and subcortical white matterParasagittal regions, esp. posterior
Proximal limb weaknessUpper extremities affected greater than lower extremities
Spastic quadriparesisCognitive delayVisual and auditory processingDifficulty
Focal ischemic necrosis
Cortex and subcortical white matterVascular injury (usually MCA distribution)
Unilateral findingsSeizures common and typically focal
HemiparesisSeizuresCognitive delays
Periventricular injury Injury to motor tracts, especially lower extremity
Bilateral and symmetric weakness in lower extremity More common in preterm infants
Spastic diplegia

Hypoxic-ischemic encephalopathy in term infants
Signs STAGE I STAGE II STAGE III
Level of consciousness Hyperalent Lethargic Stuporous, coma
Muscle tone Normal Hypotonic Flaccid
Posture Normal Flexion Decerebrate
Tendon reflexes/clonus Hyperactive Hyperactive Absent
Myoclonus Present Present Absent
Moro reflex Strong Weak Absent
Pupils Mydriasis Miosis Unequal, poor light reflex
Seizures None Common Decerebration
Electroencephalographic Normal Low voltage changing to seizure activity
Burst suppression to isoelectric
Duration <24 hr. if progresses; otherwise, may remain normal
24 hr. to 14 days Days to weeks
Outcome Good Variable Death, severe deficits

Asphyxia
IV. Diagnosis
• Cord arterial blood gas
- to determine pH, pCO2, ACO3, and base excess/deficit
• Neuroimaging
- CT scan or cranial ultrasound, usually used in late stage, evaluates cortical neuronal injury
- MRI - preferred imaging at the early stage on injury because of its increased sensitivity/specificity early in the process and its ability to outline the topography of the lesion.

Asphyxia
IV. Diagnosis
• Electroencephalogram (EEG)
- provides information of the severity of asphyxial injury through electrocerebral activity.

Asphyxia
IV. Treatment
1. Immediate resuscitation
2. Maintenance of adequate ventilation
- to maintain physiologic levels of pCO2
pCO2 – intracerebral acidosis and impair cerebrovascular autoregulation
pCO2 – associated and preventricular leukomalacia (Preterm) and sensory hearing loss (Term)

Asphyxia
IV. Treatment
3. Maintenance of adequate oxygenation
4. Control seizures

Phenytoin (20 mg/kg loading dose) or lorazepam (0.1 mg/kg) may be needed for refractory seizures.
Treatment
Seizure activity may be severe and refractory to the usual doses of anticonvulsants
Phenobarbital, the drug of choice, is given with an intravenous loading dose (20 mg/kg); additional doses of 10 mg/kg (up to 40-50 mg/kg total) may be needed.
Phenobarbital levels should be monitored 24 hr after the loading dose and maintenance therapy (5 mg/kg/24 hr) are begun
Dixon G, Badawi N, Kurinczuk JJ, et al: Early developmental outcomes after newborn encephalopathy. Pediatrics
2002;109:26-33.

Asphyxia
IV. Diagnosis and Treatment
• Potential New Modality:
• Hypothermia (33.5°C)- Cerebral cooling
- whole body cooling
- lowers the incidence of cortical neuronal injury

Asphyxia
Principle of Hypothermia as Treatment for HIE:
• Hypothermia decrease rate of apoptosis and suppresses production of mediators: reducing glutamates, free radicals, lactates which can be neurotoxic.

Prognosis
The outcome of hypoxic-ischemic encephalopathy ranges from complete recovery to death
The prognosis depending on :
1.Whether the metabolic and cardiopulmonary complications
(hypoxia, hypoglycemia, shock) can be treated
2. Infant's gestational age
(outcome is poorest if the infant is preterm)
3. Severity of the encephalopathy
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia.
Pediatrics 2001;107:480.

Severe encephalopathy characterized by : 1.Flaccid coma 2.Apnea
3.Absence oculocephalic reflexes
4. Refractory seizures
“These are associated with a poor prognosis”
Prognosis
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia.
Pediatrics 2001;107:480.

1. A low Apgar score at 20 min
2. Absence of spontaneous respirations at 20 min of age
3. Persistence of abnormal neurologic signs at 2 wk of age
“predict death or severe cognitive and motor deficits”
Prognosis
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia.
Pediatrics 2001;107:480.

Brain death after neonatal hypoxic-ischemic encephalopathy is diagnosed by:
1. Clinical findings of coma unresponsive to pain, auditory, or visual stimulation
2. Apnea with Pco2 rising from 40 to over 60 mm Hg
3. Absent brainstem reflexes
(pupil, oculocephalic, oculovestibular, corneal, gag, sucking)
Prognosis
Battin MR, Dezoete A, Gunn TR, et al: Neurodevelopmental outcome of infants treated with head cooling and mild hypothermia after perinatal asphyxia.
Pediatrics 2001;107:480.

Thank you

Multiorgan Systemic Effects of Asphyxia
SYSTEM EFFECT
Central nervous system Hypoxic- ischemic encephalopathy, infarction, intracranial hemorrhage, seizures, cerebral edema, hypotonia, hypertonia
Cardiovascular Myocardial ischemia, poor contractility, cardiac stun, tricuspid insufficiency, hypotension
Pulmonary Pulmonary hypertension, pulmonary hemorrhage respiratory distress syndrome
Renal Acute tubular or cortical necrosis
Adrenal Adrenal hemorrhage
Gastrointestinal Perforation, ulceration with hemorrhage necrosis
Metabolic Inappropriate secretion of antidiuretic hormone, hyponatremia, hypoglycemia, hypocalcemia, myoglobinuria
Integument Subcutaneous fat necrosis
Hematology Disseminated intravascular coagulation

Topography of Brain Injury in terms infants with hypoxic ischemic encephalopathy and clinical correlates
Area of Injury Location of Injury Clinical Correlate Long term sequelae
Selective neuronal necrosis
Entire neuroaxis, deep cortical area, brainstem and pentocubicular
Stupor or comaSeizuresHypotoniaOculomotor abnormalitiesSuck/swallow abnormalities
Cognitive delayCerebral palsyDystoniaSeizure disorderAtaxiaBulbar and pseudobulbar palsy
Parasagittal injury Cortex and subcortical white matterParasagittal regions, esp. posterior
Proximal limb weaknessUpper extremities affected greater than lower extremities
Spastic quadriparesisCognitive delayVisual and auditory processingDifficulty
Focal ischemic necrosis
Cortex and subcortical white matterVascular injury (usually MCA distribution)
Unilateral findingsSeizures common and typically focal
HemiparesisSeizuresCognitive delays
Periventricular injury Injury to motor tracts, especially lower extremity
Bilateral and symmetric weakness in lower extremity More common in preterm infants
Spastic diplegia

Hypoxic-ischemic encephalopathy in term infants
Signs STAGE I STAGE II STAGE III
Level of consciousness Hyperalent Lethargic Stuporous, coma
Muscle tone Normal Hypotonic Flaccid
Posture Normal Flexion Decerebrate
Tendon reflexes/clonus Hyperactive Hyperactive Absent
Myoclonus Present Present Absent
Moro reflex Strong Weak Absent
Pupils Mydriasis Miosis Unequal, poor light reflex
Seizures None Common Decerebration
Electroencephalographic Normal Low voltage changing to seizure activity
Burst suppression to isoelectric
Duration <24 hr. if progresses; otherwise, may remain normal
24 hr. to 14 days Days to weeks
Outcome Good Variable Death, severe deficits