Embed Size (px)
Citation preview

THE NAT IONAL ACADEMIES
e x e c u t i v e s u m m a r y
HUMAN REPRODUCTIVE
CLONING
ScientificMedicaland
ASPECTSof

Advances in animal reproductive cloningmethods have encouraged some practitioners
to attempt human reproductive cloning toproduce newborn humans from a predetermineddonor. The decision as to whether the self-proposed practitioners of human reproductivecloning should be allowed to proceed is mostproperly a societal decision, and likely one thatwill be made by the government. An informeddecision requires two kinds of inputs, medical-scientific and ethical. It is the responsibility of thescientific and medical community to informsociety if current methods are scientificallyfeasible and reproducible, and medically safe; andto provide guidelines to assure that if humanreproductive cloning is carried out, the humanparticipants involved are adequately advised andprotected. Once society is so informed, it will bein a position to determine whether an attempt touse reproductive cloning methods with humans isacceptable in any circumstance. The scope of thisreport is limited to informing society by providingan assessment of the medical and scientific aspectsof human reproductive cloning.
The public debate on the possible reproductivecloning of humans is often linked to the debateon human embryonic stem (ES) cells. Because oneproposed method to establish new humanembryonic stem cell lines uses a process verysimilar to the first steps in the reproductivecloning of complete humans, it is easy tounderstand how even a scientifically literatesociety could become confused about theseissues. Clarity on these matters is vitallyimportant since these issues involve both medicalrisk and opportunity, and the government isconsidering the use of sanctions on the freeinquiry that normally characterizes effectiveresearch.
The panel, which I chaired, was charged toconsider the biomedical issues surrounding thequestion of reproductive cloning of human beings,including making clear the distinctions betweenreproductive cloning and the related methodsused to derive new ES cells.1 As biomedicalscientists and physicians it is our job to seek newscientific principles, and from them new therapiesto ameliorate the personal tragedies brought onby disease. And we must do so without subjectingpatients and society to unwarranted medical
experimentation. Medical progress requiresclinical experimentation, but that process must goforward with the highest ethical standards—andonly when the risks and potential benefits areunderstood and agreed on by patient, physician,scientist, and participating institution.
Last year, at least three groups declared thatthey not only were in the process of modifying themethods used first to produce a cloned livinglamb (Dolly) in order to apply them to humans,but that they intended to carry out thereproductive cloning of human beings in the nearfuture. In response to the prospect of thosemedical experiments, the presidents of theNational Academies convened a joint panel of theCommittee on Science, Engineering, and PublicPolicy (COSEPUP) and the Board on Life Sciences(BLS) to examine the scientific and medical issuesrelevant to human reproductive cloning and toconsider the ethical issues that apply specificallyto the participation of human subjects in cloningresearch. The panel also considered a somewhatrelated technology—nuclear transplantation toproduce stem cell lines. Again, the analysis of thistechnology was limited to understandingpotential scientific or medical risks as well asscientific or medical opportunity offered bynuclear transplantation to produce pluripotenthuman stem cell lines. The purpose of thisundertaking, by the panel, is to clarify andprovide as much understanding as possible ofthese issues in order to inform the much broaderdebate that will be carried out by a larger crosssection of society.
Our panel of 11 members has been unanimousin reaching the recommendations and conclusionspresented in this Executive Summary. In makingour decisions, we carefully considered the resultsof our workshop. We also read widely andextensively, consulted experts, and took intoaccount the findings of the important recentreport from the National Academies entitled StemCells and the Future of Regenerative Medicine.
The panel believes that all concerned segmentsof society should examine and debate the broadethical issues associated with human cloning.Although we have only examined the scientificand medical aspects, we hope that our reporthelps to inform this broader consideration bysociety.
Preface
1 Stem cells are the subject of a complementary report from the National Academies entitled Stem Cells and the Future of Regenerative Medicine, which was released to thepublic in September 2001. The full text of that report is available at http://www.nap.edu/catalog/10195.html
Note: This preface is an abbreviated version of that which appears in the report.
Irving L. WeissmanChair
Human reproductive cloning is anassisted reproductive technology thatwould be carried out with the goal of
creating a human being. It is currently thesubject of much debate around the world,involving a variety of ethical, religious, societal,scientific, and medical issues. However, thisreport from the National Academies addressesonly the scientific and medical aspects of humanreproductive cloning. Consideration of themedical aspects has required the panel toexamine issues of scientific conduct and human-subjects protection. But we have not attemptedto address the issue of whether producing a newindividual by reproductive cloning, if it werefound to be scientifically safe, would or wouldnot be acceptable to individuals or society.Instead, the panel defers to others on thefundamental ethical, religious, and societalquestions, and presents this report on thescientific and medical aspects to inform thebroader debate. Our report differs in this respect
from the last major report on the topic in theUnited States, Cloning Human Beings, a 1997report developed by the National BioethicsAdvisory Commission [1].
THE PANEL’S CONCLUSIONS ANDRECOMMENDATIONS
The panel has examined and analyzed thescientific, medical, and legal literature on theissues and heard testimony at a workshop fromexperts in animal cloning, assisted reproductivetechnologies, and science, technology, and legalpolicy—including people who, on scientific andmedical grounds, either oppose or defendhuman reproductive cloning. After carefullyconsidering the issues raised, we conclude thatthe case has not been proved that humanreproductive cloning would lead to fewernegative outcomes at this time than reproductivecloning of other mammals. We therefore makethe following recommendations:
1
RECOMMENDATIONSHuman reproductive cloning should not now be practiced. It is dangerous and likely to fail.
The panel therefore unanimously supports the proposal that there should be a legallyenforceable ban on the practice of human reproductive cloning. For this purpose, we definehuman reproductive cloning as the placement in a uterus of a human blastocyst derived by thetechnique that we call nuclear transplantation. In reaching this conclusion, we considered therelevant scientific and medical issues, including the record from cloning of other species, and thestandard issues that are associated with evaluating all research involving human participants.
The scientific and medical considerations related to this ban should be reviewed within 5years. The ban should be reconsidered only if at least two conditions are met: (1) a new scientificand medical review indicates that the procedures are likely to be safe and effective and (2) a broad national dialogue on the societal, religious, and ethical issues suggests that areconsideration of the ban is warranted.
Finally, the scientific and medical considerations that justify a ban on human reproductivecloning at this time are not applicable to nuclear transplantation to produce stem cells. Becauseof its considerable potential for developing new medical therapies for life-threatening diseasesand advancing fundamental knowledge, the panel supports the conclusion of a recent NationalAcademies report that recommended that biomedical research using nuclear transplantation toproduce stem cells be permitted. A broad national dialogue on the societal, religious, and ethicalissues is encouraged on this matter.
Executive Summary
THE FINDINGS THAT SUPPORT A BANON HUMAN REPRODUCTIVE CLONING
It is a serious event when any group that haspotential authority over research intercedes toban it, and the reasons must therefore becompelling. We are convinced that the scientificand medical data concerning the likely danger tothe implanted fetus or the eventual newborn ifreproductive cloning of humans is attempted inthe near future are compelling.
The panel has based its support for theproposed ban on human reproductive cloning onthe following findings:
Finding 1The scientific and medical criteria used to
evaluate the safety of reproductive cloning mustbe the potential morbidity and death of thewoman carrying the clone as a fetus and of the newborn and the risk to women donatingthe eggs.
Finding 2Data on the reproductive cloning of animals
through the use of nuclear transplantationtechnology demonstrate that only a smallpercentage of attempts are successful; that manyof the clones die during gestation, even in latestages; that newborn clones are often abnormalor die; and that the procedures may carryserious risks for the mother. In addition, becauseof the large number of eggs needed for suchexperiments, many more women would beexposed to the risks inherent in egg donation fora single cloning attempt than for thereproduction of a child by the presently used in vitro fertilization (IVF) techniques. Thesemedical and scientific findings lead us toconclude that the procedures are now unsafe for humans.
Finding 3At least three criteria would have to be
fulfilled before the safety of human reproductivecloning could be established:
(1) The procedures for animal reproductive cloning would have to be improved to suchan extent that the levels of observedabnormalities in cloned animals, includingnon-human primates, were no more thanthat seen with existing human assistedreproductive technology (ART) procedures.
If that could not be achieved, researcherswould have to demonstrate that humans aredifferent from other animals with regard tocloning-related defects. Reproducible datademonstrating that a successfulreprogramming of the donor nucleus andproper imprinting can be achieved inanimals would be essential, as would anunderstanding of the mechanismsresponsible for such events.
(2) New methods would have to bedeveloped to demonstrate that the human preimplantation embryos produced throughthe use of nuclear transplantation technology are normal with respect to imprinting and reprogramming. That wouldbest be done by first establishing the normalstate of reprogramming and imprinting in non-human primates and then documentingthat the processes in preimplantation humanembryos are substantially similar.
(3) Methods would have to be developed tomonitor—effectively and comprehensively—preimplantation embryos and fetuses in the uterus for cloning-related defects, such as those outlined in Chapter 3; these includealterations in gene expression andimprinting.
Finding 4The issues of responsible conduct of research
raised by the prospect of cloning a person arethose of medical ethics—in particular, theprotection of the participants (the egg donor, thehost mother, and the child produced throughcloning) in any human cloning research.Participants in any human cloning researchefforts require full protection as human researchparticipants, although it should be noted that, aswith fetal surgery, this protection cannot beextended fully to the cloned fetus. Humanreproductive cloning has not been performedbefore, and its introduction, if it ever occurred,would require systematic research. That researchwould likely entail full review by institutionalreview boards and other human-subjectsprotections, including informed consent ofdonors and recipients of all biological materials.
2

3
Finding 5If any attempts at human reproductive
cloning were ever to occur, they wouldconstitute research, not merely innovativetherapy. Such research would then be subject toexternal technical and ethical review by reviewboards to ensure that the proposed experimentsare both technically and ethically sound and thatthe rights and welfare of all research participantsare protected. This institutional review processshould be applied equally to both public- andprivate-sector research and be transparent to the public.
Finding 6Because medical and scientific findings
indicate that cloning procedures are currentlynot safe for humans, cloning of a human throughthe use of nuclear transplantation technology isnot now appropriate. The panel believes that noresponsible scientists or physicians are likely toundertake to clone a human. Nevertheless, novoluntary system that is established to restrictreproductive cloning is likely to be completelyeffective. Some organizations have alreadyannounced their intention to clone humans, andmany of the reproductive technologies neededare widely accessible in private fertility clinicsthat are not subject to federal regulations. Thepanel therefore concludes that a legallyenforceable ban that carries substantial penaltieshas a much greater potential than a voluntarysystem or moratorium to deter any attempt toclone a human using these techniques.
Finding 7If no ban is imposed, it is possible that some
organizations will attempt the reproductivecloning of humans. Although such attemptswould most likely fail, there is a high probabilitythey would be associated with serious risks toany possible fetus or newly born child and mayharm the woman carrying the developing fetus.
Finding 8There is a concern that legislation or
regulation that would ban reproductive humancloning would set a troubling precedent withrespect to the restriction of innovative,experimental research and medical procedures.Modern scientific research proceeds rapidly, and
its findings are unpredictable and oftensurprising. It is probable that at least every 5years there will be significant new informationregarding the issues of the safety andapplicability of human cloning to medicalpractice. The above concern can be amelioratedby including in any legislation or regulation arequirement for an updated evaluation of thescientific, medical, and societal issues within 5years. Such a requirement for periodic reviewswould allow for extensive public debateregarding reproductive human cloning and theconsideration of modifications to the legislation.Part of that evaluation would include arecommendation as to when the next suchevaluation should be conducted.
Finding 9Two activities will be particularly important
for an updated evaluation of humanreproductive cloning: a thorough scientific andmedical review to evaluate whether theprocedures are likely to be safe and effective anda broad national dialogue on the societal,religious, and ethical issues. As part of thisprocess, any persons advocating the practice ofhuman reproductive cloning would need toacknowledge the extent of the abnormalitiesseen in animal cloning experiments and todemonstrate that these problems—assuming thatthey persist—are unlikely to occur in humans.
Finding 10Any future process designed to evaluate the
scientific and medical evidence on cloning aperson would likely need to involve scientists,physicians, ethicists, and the public. A publicdebate could be facilitated by a committee thatissues regular updates on the state of the sciencesurrounding animal cloning and reaches out toinvolved constituencies in a systematic manner.Such a body could derive its powers byexecutive order, by executive action within theDepartment of Health and Human Servicesunder the Public Health Service Act, or bylegislation. Among many other issues, the debateshould be structured to inform the public thatclones are not precise replicas, but persons withidentical genetic material.

Finding 11The science of cloning is an international one
with research conducted throughout the world.Furthermore, the issue of human reproductivecloning is the subject of worldwide debate. Anumber of countries and internationalorganizations have prepared reports and issuedstatements on the issue. Participation by theUnited States in such international debates abouthuman reproductive cloning will be beneficial toany future process to evaluate the scientific andmedical evidence on this issue.
Finding 12The limited regulation and monitoring of
experimental ART procedures in the UnitedStates means that important data needed forassessing novel ART procedures are in somecases lacking, in other cases incomplete and hardto find. Because the panel was not charged toinvestigate ART regulation and did not solicitexpert testimony thereon, we make norecommendations regarding oversight of,registration of, or required data collection fromART clinics. But we do believe that a requestfrom Congress or the Executive Branch for apanel of experts to study the matter and reportits findings and recommendations publiclywould probably be useful. Having suchinformation is likely to be beneficial to anyprocess of evaluating future scientific andmedical evidence regarding both reproductivecloning and new ART procedures.
REDUCING CONFUSION CONCERNINGTHE USE OF THE TERM “HUMAN CLONING“
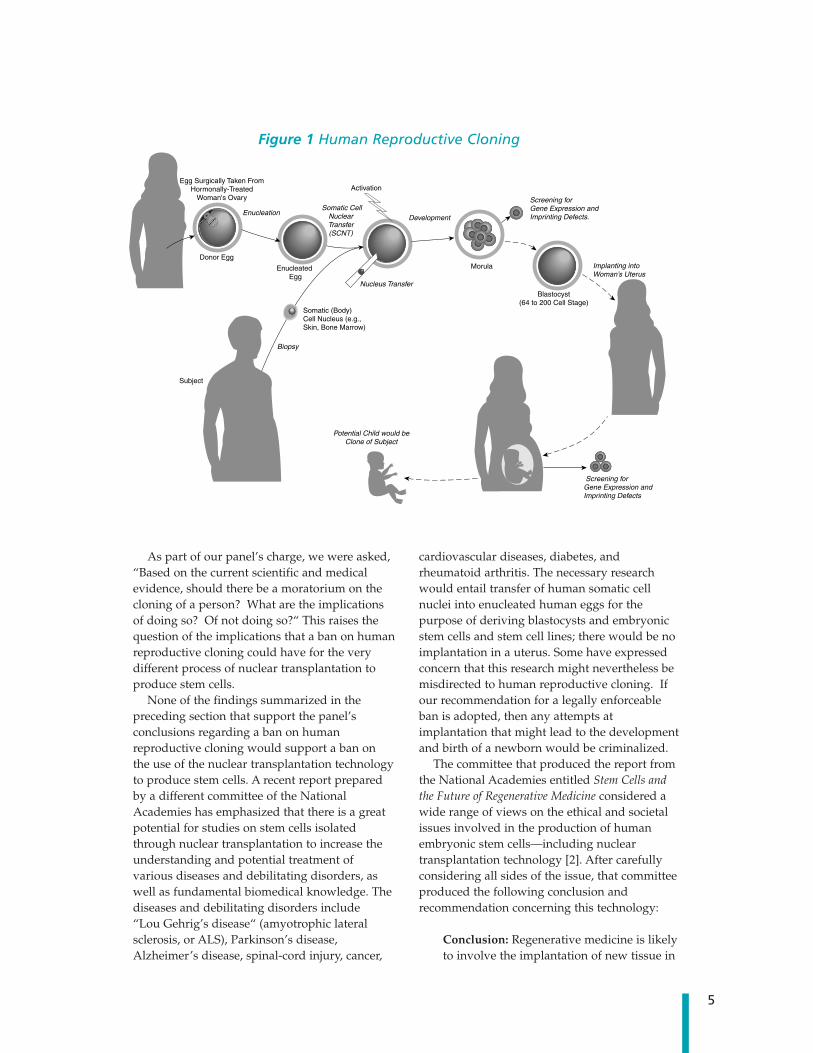
As we have just discussed, humanreproductive cloning is an assisted reproductivetechnology that would be carried out with thegoal of creating a human being (see Figure 1).There is a very different procedure, here termednuclear transplantation to produce stem cells—but variously called nonreproductive cloning,therapeutic cloning, research cloning, or somaticcell nuclear transfer (SCNT) to produce stemcells—whose aim is the creation of embryonicstem (ES) cells for clinical and research purposes(see Figure 2).
Unlike reproductive cloning, the creation ofES cells by nuclear transplantation does notinvolve implantation of a preimplantation
embryo, or blastocyst, in a uterus. For thisreason, it cannot produce a complete, live bornanimal (a “clone“). Some confusion arisesbecause in both cases researchers would usenuclear transplantation, which is an initial stepin the successful procedures used to cloneanimals—beginning with the sheep Dolly andincluding several other mammals since then. Innuclear transplantation, the nucleus of an eggcell (containing its chromosomes) is removedand replaced with the nucleus of a cell takenfrom the body of an adult (a “somatic cell“).Thus, nuclear transplantation accuratelydescribes the process.
For both reproductive cloning and stem cellproduction, a reconstructed egg cell produced bynuclear transplantation is stimulated to cause itto begin dividing. If that is successful, severalsequential cell divisions can give rise to thepreimplantation embryo known as a blastocystthat is composed of 64-200 cells (see Figure 2).
It is at this stage that the procedures used forreproductive cloning and for nucleartransplantation to produce stem cells becomeentirely different. In reproductive cloning, ablastocyst formed by the nuclear transplantationprocedure is implanted in a uterus, where itbegins the process of forming a fetus. Anyanimals produced in this way will have the samenuclear genes as the adult cells used to producethem, and when the nuclei from several somaticcells from a single animal are transferred to aseries of eggs, all the animals born are said to be“clones“ of the original adult animal.
Although these clones will be physically verysimilar, the animals will not be physically orbehaviorally identical, because of various factors,including their different uterine and postnatalenvironments and experiences.
In nuclear transplantation to produce stemcells, cells are isolated from the blastocyst 4-5days after the procedure, and the cells are usedto make a stem cell line for further study andclinical applications. Neither the blastocyst northe stem cells are ever placed into a uterus.Moreover, as described in Chapter 2, humanstem cells do not themselves have the capacity toform a fetus or a newborn animal. Nevertheless,in the popular press and other media, the term“human cloning“ has often been misleadinglyapplied to both this procedure and reproductivecloning whenever either is proposed to be usedin a human context.
4
As part of our panel’s charge, we were asked,“Based on the current scientific and medicalevidence, should there be a moratorium on thecloning of a person? What are the implicationsof doing so? Of not doing so?“ This raises thequestion of the implications that a ban on humanreproductive cloning could have for the verydifferent process of nuclear transplantation toproduce stem cells.
None of the findings summarized in thepreceding section that support the panel’sconclusions regarding a ban on humanreproductive cloning would support a ban onthe use of the nuclear transplantation technologyto produce stem cells. A recent report preparedby a different committee of the NationalAcademies has emphasized that there is a greatpotential for studies on stem cells isolatedthrough nuclear transplantation to increase theunderstanding and potential treatment ofvarious diseases and debilitating disorders, aswell as fundamental biomedical knowledge. Thediseases and debilitating disorders include “Lou Gehrig’s disease“ (amyotrophic lateralsclerosis, or ALS), Parkinson’s disease,Alzheimer’s disease, spinal-cord injury, cancer,
cardiovascular diseases, diabetes, andrheumatoid arthritis. The necessary researchwould entail transfer of human somatic cellnuclei into enucleated human eggs for thepurpose of deriving blastocysts and embryonicstem cells and stem cell lines; there would be noimplantation in a uterus. Some have expressedconcern that this research might nevertheless bemisdirected to human reproductive cloning. Ifour recommendation for a legally enforceableban is adopted, then any attempts atimplantation that might lead to the developmentand birth of a newborn would be criminalized.
The committee that produced the report fromthe National Academies entitled Stem Cells andthe Future of Regenerative Medicine considered awide range of views on the ethical and societalissues involved in the production of humanembryonic stem cells—including nucleartransplantation technology [2]. After carefullyconsidering all sides of the issue, that committeeproduced the following conclusion andrecommendation concerning this technology:
Conclusion: Regenerative medicine is likelyto involve the implantation of new tissue in
Donor Egg
Egg Surgically Taken FromHormonally-Treated
Woman's Ovary
Enucleated Egg
Somatic (Body)Cell Nucleus (e.g., Skin, Bone Marrow)
Activation
Morula
EnucleationDevelopment
Screening for Gene Expression and Imprinting Defects.
Screening for Gene Expression andImprinting Defects
Implanting intoWoman’s Uterus
Somatic CellNuclearTransfer(SCNT)
Subject
Biopsy
Potential Child would beClone of Subject
Nucleus TransferBlastocyst
(64 to 200 Cell Stage)
5
Figure 1 Human Reproductive Cloning

patients with damaged or diseased organs.A substantial obstacle to the success oftransplantation of any cells, including stemcells and their derivatives, is the immune-mediated rejection of foreign tissue by therecipient’s body. In current stem celltransplantation procedures with bonemarrow and blood, success hinges onobtaining a close match between donor andrecipient tissues and on the use ofimmunosuppressive drugs, which oftenhave severe and potentially life-threateningside effects. To ensure that stem cell-basedtherapies can be broadly applicable formany conditions and people, new means ofovercoming the problem of tissue rejectionmust be found. Although ethicallycontroversial, the somatic cell nucleartransfer technique promises to have thatadvantage. Other options for this purposeinclude genetic manipulation of the stemcells and the development of a very largebank of ES cell lines [2].
Recommendation: In conjunction withresearch on stem cell biology and thedevelopment of potential stem celltherapies, research on approaches thatprevent immune rejection of stem cells andstem cell-derived tissues should be activelypursued. These scientific efforts include theuse of a number of techniques to manipulatethe genetic makeup of stem cells, includingsomatic cell nuclear transfer [2].
Our panel includes members whoparticipated in the workshop on stem cells heldat the National Academies on June 23, 2001. Thisworkshop was convened as part of the data-gathering process for the separate committeethat produced the above report focused on stemcells. In our own workshop, held on August 7,2001, we consulted with many of the world'sleaders in nuclear transplantation to producestem cells—I. Wilmut, R. Jaenisch, R.Yanagimachi, J. Cibelli, P. Mombaerts, and A.Trounson—and we have also conducted our own
6
Donor Egg
Enucleated Egg
Blastocyst(64 to 200 Cell Stage)
TrophoblastInner Cell Mass
Pluripotent Embryonic Stem Cells
Activation
Enucleation Development
Nucleus Transfer Propagationin Culture
Somatic CellNuclearTransfer(SCNT)
Subject
Biopsy
Heart Muscle Cells
Nerve Cells
Liver Cells
Kidney Cells
Development of Specialized Cells
Blood Cells
PancreaticIslet Cells
Cells Transplanted into Subjectwith Diabetes, Alzheimer's, Parkinson’s,
Spinal Cord Injury, Lou Gehrig’s Disease,Cancer, Cardiovascular Disease,
Rheumatoid Arthritis, etc.
Egg Surgically Taken FromHormonally-Treated
Woman's Ovary
Somatic (Body)Cell Nucleus (e.g., Skin, Bone Marrow)
Morula
Figure 2 Nuclear Transplantation to Produce Stem Cells

extensive literature review. On the basis of thisreview and discussion, the panel determinedthat although there is a clear therapeuticpotential for techniques in which stem cells areproduced through nuclear transplantation (as inFigure 2), this potential is nascent and needsconsiderable research. The potential of thisresearch includes developing a broaderunderstanding of how human tissue cellsdevelop normally, and how human diseases thathave a genetic component are caused at acellular level.
The panel concludes this executive summarywith a review of the scientific subjects thatwere covered.
ANIMAL CLONINGSince the report in 1997 of the birth of the
sheep Dolly, the first successful reproductiveclone of a mammal from an adult cell,reproductive cloning has been carried out withseveral kinds of animals. Five mammalianspecies have been reproductively-cloned fromadult or fetal cells—sheep, mice, pigs, goats, andcattle—and similar attempts are being made, sofar without success, in monkeys, dogs, andhorses.
The panel reviewed the scientific literature onanimal cloning and heard from animal-cloningexperts at its workshop. It found that cloningefficiencies in animals remain extremely lowdespite several years of experimentation. Thislow efficiency means that any humanreproductive cloning attempt would probablyrequire large numbers of eggs. The collection ofthese eggs would bring with it the risk ofovarian hyperstimulation syndrome in donors,as with all IVF. However, in the case of cloning itwould probably involve either scores of womenfor one cloning attempt or a few women beingexposed to high levels of hormones.
Furthermore, animal cloning is associatedwith a wide variety of abnormalities in the fetusand offspring. The abnormalities include agreater than normal size of fetus and placenta(both during gestation and after birth), poorinteraction between fetal and maternalcomponents of the placenta, greater early-gestation and late-gestation fetal morbidity andmortality, greater postnatal mortality, andvarious developmental defects in the immune,cardiovascular, and possibly nervous systems. Inaddition, it is important to note that subtle
behavioral and mental defects that could createmajor problems for humans may not bedetectable in animal models.
The most likely reasons for the abnormalitiesthus far observed are failures in geneticreprogramming (the process that changes a cellnucleus from one developmental state toanother) and errors in genetic imprinting (theprocess of establishing, maintaining, andinterpreting parent-specific chemical marks onthe DNA, which indicate how specific genesshould function in specific cells).
On the basis of the animal data, it is alsolikely that human cloning will be associated withrisks to the women involved. Among these risksare increased maternal morbidity and mortalityand the risks inherent in the overproduction ofoocytes from egg donors. The psychologicalburden of late-term abortions or the birth ofinfants with severe defects must also beconsidered.
HUMAN REPRODUCTIVE CLONINGThose who plan to clone humans have
indicated that they will take additionalprecautionary steps beyond those currentlyundertaken in animal cloning. The steps includepreimplantation testing to detect chromosomedefects and errors in imprinting (methylation) atone or more DNA sites, and postimplantationtesting of the imprinting (methylation) status atup to 30 DNA sites. All participants would signan informed-consent form that would outline therisks to both the mother and the child and thelow probability of success. Those who havepublicly stated their intention to undertakehuman reproductive cloning are thus far usingprivate funding in a nonuniversity setting, andin some cases they are operating or planning tooperate outside the United States.
LESSONS FROM OTHER ASSISTEDREPRODUCTIVE TECHNOLOGIES RELEVANT TO HUMANREPRODUCTIVE CLONING
Assisted reproductive technology (ART) refers toall treatments or procedures for assisting humanreproduction that include the laboratoryhandling of human eggs, sperm, or embryos,including IVF. IVF involves the mixing of eggand sperm in the laboratory to generate embryossuitable for transfer to a uterus 2 or 3 days later.
7

ART as currently practiced does not provide abasis for evaluating all the risks inherent inreproductive cloning, because reproductivecloning involves the use of adult somatic nucleirather than the germ cell (egg and sperm) nucleiused in ART [3]. Germ-cell nuclei arepreprogrammed to support early embryonicdevelopment and to respond to the egg’sregulatory signals, whereas adult cell nuclei arenot and must therefore undergo an extensivereprogramming to be successful in their newenvironment.
The panel compared the experiences thus farobtained in animal cloning with knowledge ofcurrent human ART procedures and found thatthe reproductive outcomes from clonedblastocysts observed in animals are very lowcompared with the efficiencies seen with currenthuman IVF—as well as being highly variable. Inaddition, serious defects and deaths occur inanimal cloning, often late in pregnancy and soonafter birth, at rates never seen with human ormost animal ART procedures.
Existing preimplantation andpostimplantation testing methods areinappropriate and inadequate for the needs ofhuman reproductive cloning. Assessing theshape and structure of embryos is of little use indetermining the likelihood of successfulimplantation of a particular embryo, andmolecular tests to detect all the possible errors ingenetic imprinting and reprogramming do notyet exist. Moreover, such tests, if they becomeavailable, would be difficult to adapt to thesmall amount of material available forpreimplantation diagnosis.
Experimental ART procedures have beenminimally regulated and monitored in theUnited States, so there is a shortage of datapertaining to innovative ART procedures.Certification of clinics could allow greatercontrol over any new ART procedures andcollection of important information. The UKHuman Fertilisation and Embryology Authoritymight provide a model for certifying ART clinicsand clinical and research protocols andprocedures, although the terms of the UKlegislation would have to be adapted to thefederal style of US government.
USING NUCLEAR TRANSPLANTATIONTO PRODUCE EMBRYONIC STEM CELLS
Stem cells are cells that have an extensiveability to self-renew and to differentiate (turn intospecialized cells). Embryonic stem cells obtainedfrom blastocysts (5- to 7-day-old preimplantationembryos of about 150 cells each) are particularlyimportant because they can give rise to the widestvariety of cells and are immortal. If embryonicstem cells are derived by nuclear transplantationusing a nucleus from a patient as the somaticnucleus transferred into the egg, the resultingcells will be immunologically very similar to thepatient’s cells. However, the nuclear DNA donorand mitochondrial DNA donor will generally bedifferent. Only if the egg donor is the mother ofthe patient or the patient herself, will the stemcells be genetically identical with the patient’scells—containing not only the same nucleargenome, but also the same mitochondrial DNA.As described in the recent report from theNational Academies entitled Stem Cells and theFuture of Regenerative Medicine, present researchwith such cells has the goal of producing cells andtissues for therapeutic transplantation with areduced risk of rejection [2]. However,mitochondrial gene products that differ can elicittransplant rejection (see Chapter 2).
The panel recognizes that a blastocyst derivedfor scientific purposes by nuclear transplantationcould be implanted in a human uterus inviolation of a ban on reproductive cloning. But alegally enforceable ban that criminalizes theimplantation step should be sufficient to preventsuch proscribed activity. Moreover, because allnuclear transplantation experiments will requirethe participation of human subjects (the donor ofthe eggs and the donor of the somatic cell nuclei,who may be the same person or differentpersons), all this work would necessarily beregulated and controlled by the procedures andrules concerning human-subjects research—subjecting it to close scrutiny.
Stem cells derived directly from an adult’sown tissues are an alternative to nucleartransplantation-derived embryonic stem cells asa source of cells for therapies. Two types of adultstem cells—bone marrow and skin stem cells—currently provide the only two stem celltherapies. But, as noted in the above mentioned
8

report, many questions remain before thepotential of other adult stem cells can beaccurately assessed. Few studies on adult stemcells have sufficiently defined the stem cell bystarting from a single isolated cell or defined thenecessary cellular environment for correctdifferentiation or the factors controlling theefficiency with which the cells repopulate anorgan. There is a need to show that the cellsderived from introduced adult stem cells arecontributing directly to tissue function and toimprove the ability to maintain adult stem cellsin culture without having the cells differentiate.Finally, most of the studies that have garnered somuch attention have used mouse rather thanhuman adult stem cells.
The previous report also notes that unlikeadult stem cells, it is well established thatembryonic stem cells can form multiple tissuetypes and be maintained in culture for longperiods of time. However, embryonic stem cellsare not without their own potential problems asa source of cells for transplantation. The growthof human embryonic stem cells in culture nowrequires a “feeder“ layer of mouse cells that maycontain viruses, and when allowed todifferentiate the embryonic stem cells can form amixture of cell types at once. Human embryonicstem cells can form benign tumors whenintroduced into mice, although this potentialseems to disappear if the cells are allowed todifferentiate before introduction into a recipient.
In addition to possible uses in therapeutictransplantation, embryonic stem cells and celllines derived by nuclear transplantation could bevaluable tools for both fundamental and appliedmedical and biological research [2]. This researchwould begin with the transfer of geneticallydefined donor nuclei from normal and diseasedtissues. The resulting cell lines could be used tostudy how inherited and acquired alterations ofgenetic components might contribute to diseaseprocesses. The properties of the cell lines couldbe studied directly, or the embryonic stem cellscould be studied as they differentiate into othercell types. For example, the way in which cellsderived by nuclear transplantation from anAlzheimer’s disease patient acted whiledifferentiating into brain cells, compared withthose derived from a normal patient, might yieldnew clues about Alzheimer’s disease. Such cell
lines could also be used to ensure that researchcovers a more genetically diverse humanpopulation than that represented in theblastocysts stored in IVF clinics, promotingstudies of the causes and consequences ofgenetic diseases by allowing researchers to studyhow embryonic stem cells with different geneticendowments differ in the way that they form celltypes and tissues. Finally, studies of geneticreprogramming and genetic imprinting will besubstantially enhanced through the use of stemcells derived by nuclear transplantation,compared with studies with stem cells derivedfrom other sources.
SUMMARYThis panel was charged with assessing the
scientific and medical issues surrounding humanreproductive cloning. Most of the relevant dataon reproductive cloning are derived from animalstudies. The data reveal high rates ofabnormalities in the cloned animals of multiplemammalian species and lead the panel toconclude that reproductive cloning of humans isnot now safe. Our present opposition to humanreproductive cloning is based on science andmedicine, irrespective of broader considerations.The panel stresses, however, that a broad ethicaldebate must be encouraged, so that the publiccan be prepared to make decisions if humanreproductive cloning is some day consideredmedically safe for mothers and offspring.
The panel's discussion inevitably included acomparison of the methods used for reproductivecloning and for nuclear transplantation toproduce stem cells. The panel is in agreementwith the recent report from the NationalAcademies entitled Stem Cells and the Future ofRegenerative Medicine [2] in affirming the potentialof studies on stem cells isolated through nucleartransplantation. The probable benefits includeadvances in fundamental biomedical knowledge,as well as the understanding and treatment ofvarious diseases and debilitating disorders.
9

CURRENT ARGUMENTS AND COUNTERARGUMENTS REGARDING HUMAN REPRODUCTIVE CLONING
10
Provided below is a summary of some of thecurrent arguments and counter argumentsregarding human reproductive cloning. Thepanel’s analysis of each is based on the scientificand medical literature and on presentations at itsworkshop.
Argument 1: Animal-safety data do not apply,because humans are very different from theanimals under study [4]. In particular, a recentstudy [5] indicated that an important imprintedgene in mice is not imprinted in humans;therefore, imprinting errors would not be aproblem in cloned humans.
Counterargument: Placental function,development, and genetic regulation are similarin humans and animal models, such as mice, sosimilar SCNT-related defects would be expected[6]. Numerous studies have emphasized thathumans and other organisms have the samebasic pathways for governing early embryonicand fetal development.
Furthermore, widespread defects in all fiveof the mammalian species that have beenreproductively cloned thus far suggests that thedefects would affect basic biological functions inhumans.
Even if one less gene is imprinted in humansthan in mice, humans are known to have manyimprinted genes (possibly as many as 100), andany number of these are likely to cause problemsin reproductively cloned humans.
Argument 2: Frequent failures are seen innormal human reproduction; cloning would beno different [4].
Counterargument: Errors in normal humanreproduction occur primarily early in pregnancy;many of the women in question are never awarethat they are pregnant. In contrast, many of thedefects in reproductively cloned animals ariselate in pregnancy or after birth.
Argument 3: Inappropriate culture media forthe initial cells cause most cloning-relatedproblems [7; 8]. Culture media for humanassisted reproductive technologies have beenbetter optimized [8; 4]. Synchronization betweenthe implanted embryo and the recipient uterushas also been better in human than in animalassisted reproductive technology procedures.
Counterargument: Culture effects appear toaccount for only some of the defects observed [9;10]. Many defects in various organ systems arepeculiar to reproductive cloning. Expertise inexisting human assisted reproductivetechnologies is not relevant to these problems,because the defects appear to arise frombiological rather than purely technical causes [9].

11
Argument 4: Those who have cloned animalsstress the failures, but there are also manysuccesses in animal reproductive cloning [8; 4].
Counterargument: The statement is true but does not necessarily apply to humanreproductive cloning. In humans, the likelihoodand benefit of success must be weighed againstthe probability, severity, and lifelongconsequences of failure. Failures are all butcertain in any human reproductive cloningattempt at this time, based on the experiencewith animals, and in humans, the consequencescould be far more devastating. The likelihoodand benefit of possible success must be weighedagainst the high probability and severeconsequences of failure.
Argument 5: Existing preimplantation andpostimplantation genetic tests could be used todetect abnormalities, allowing selection ofembryos to be implanted and therapeuticabortion in case of any problems. In contrast,there has been no genetic testing and weedingout of animal reproductive clones.
In preimplantation testing, two cells could beremoved from an eight-cell morula. One cellcould be tested for correctness of thechromosome complement and the other forimprinting errors at one or more DNA sites [11].It has been claimed that such imprinting testshave been performed with DNA from cells aftersomatic cell nuclear transfer (SCNT) [4],although no data have been presented.
Postimplantation testing could includetesting for chromosomal errors, the checking ofimprinting status at up to 30 sites, and themeasurement of production levels from manygenes with DNA chips [12] or reverse-transcription polymerase chain reaction [11].
Counterargument: Many errors would not bedetectable until late in pregnancy or after birth,when therapeutic abortion would not be anoption. Many of the relevant genetic tests havenot yet been developed [8; 9]; existing genetictests appropriate for single-gene inheriteddisorders or gross chromosomal rearrangementsare insufficient because they are not relevant tothe major sources of errors expected in humancloning. Ultrasonographic tests cannot detect thesmall-scale defects in tissues, such as lung, thathave had devastating consequences in newbornanimal clones [13; 14], and there is insufficientevidence regarding the possible impact ofimprinting errors on brain development inhumans.
Argument 6: Voluntary informed consent allowspotential participants to make their owndecisions and elect to take the risks if they sochoose.
Counterargument: Our current regulatorysystem recognizes that when information islacking it can be difficult or impossible to informsubjects fully. That is the case with respect tohuman reproductive cloning because the extentof the risks is unknown, and the greatest risk ofabnormality, morbidity, and mortality is borneby the cloned fetus/child, who cannot giveinformed consent. In addition, there are risksborne by the woman donating the eggs and thegestational mother.
When subjects cannot be fully informed, andwhen a procedure is clearly risky, there is a rolefor both regulatory agencies and professionals tolimit the options available to a subject if theevidence supports such a limitation [14]. Societalconcerns can also be taken into account.
1. NATIONAL BIOETHICS ADVISORY COMMISSION. Cloning Human Beings, Volume I: Report and Recommendations of the National Bioethics Advisory Commission. Rockville, MD. 1997 Jun. Online at: http://bioethics.gov/pubs/cloning1/cloning.pdf.
2. COMMITTEE ON STEM CELLS AND THE FUTURE OF REGENERATIVE MEDICINE, BOARD ON LIFE SCIENCES AND BOARD ON NEUROSCIENCE AND BEHAVIORAL HEALTH. Stem Cells and the Future of Regenerative Medicine. Report of the National Research Council and the Institute of Medicine. 2001 Sept.
3. KRAKAUER DC, MIRA A. Mitochondria and germ-cell death. Nature 1999 Jul 08, 400 (6740): 125-6.
4. BOISSELIER B, Clonaid, Bahamas. Reproductive cloning in humans. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
5. KILLIAN JK, NOLAN CM, WYLIE AA, LI T, VU TH, HOFFMAN AR, JIRTLE RL. Divergent evolution in M6P/IGF2R imprinting from the Jurassic to the Quaternary. Hum Mol Genet 2001 Aug 15, 10 (17): 1721-1728.
6. CROSS J, University of Calgary, Alberta, Canada. Assisted reproductive technologies. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
7. ANTINORI S, International Associated Research Institute, Italy. Cloning in reproductive medicine. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7.Online at: www.nationalacademies.org/humancloning
8. ZAVOS P, Andrology Institute of America. Human therapeutic cloning: Indications, ethics, and other considerations. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
9. JAENISCH R, Massachusetts Institute of Technology/ Whitehead Institute. Scientific issues underlying cloning: Epigenetics. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
10. FARIN PW, North Carolina State University. Large offspring effects in cattle. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
11. ZAVOS P, Andrology Institute of America. Expert witness. Human cloning. U.S. House of Representatives, Committee on Energy and Commerce. Subcommittee on Oversight and Investigations. 2001 Mar 28. Online at: http://energycommerce.house.gov/107/ hearings/03282001Hearing141/print.htm
12. BRENNER C, COHEN J. The genetic revolution in artificial reproduction: A view of the future. Hum Reprod 2000 Dec, 15 Suppl 5 :111-6.
13. HILL J, Cornell University. Placental defects in nuclear transfer (cloned) animals. Workshop: Scientific and Medical Aspects of Human Cloning. 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
14. WILMUT I, Roslin Institute, Scotland. Application of animal cloning data to human cloning. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington, D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
15. CHARO RA, University of Wisconsin, Madison. Regulation of cloning. Workshop: Scientific and Medical Aspects of Human Cloning. National Academy of Sciences, Washington D.C., 2001 Aug 7. Online at: www.nationalacademies.org/humancloning
12
REFERENCES
13
NATIONAL ACADEMY OF SCIENCESNATIONAL ACADEMY OF ENGINEERING
INSTITUTE OF MEDICINECommittee on Science, Engineering, and Public Policy (COSEPUP)
Policy and Global Affairs (PGA)
NATIONAL RESEARCH COUNCILDivision on Earth and Life Studies (DELS)
Board on Life Sciences (BLS)
Panel on Scientific and Medical Aspects of Human Cloning
Irving L. Weissman, M.D.1 (chair)Karel and Avice Beekhuis Professor of
Cancer Biology, and Professor of Pathology and
Developmental BiologyStanford UniversityStanford, Calif.
Arthur L. Beaudet, M.D.2
Henry & Emma Meyer Professor and Chair
Department of Molecular and Human Genetics, and
ProfessorDepartment of Pediatrics and
Department of Cell Biology Baylor College of MedicineHouston
Patricia K. Donahoe, M.D.1 ,2
Chief of Pediatric Services, and Director of Pediatric Surgical Research
LaboratoriesMassachusetts General Hospital, andMarshall K. Bartlett Professor of SurgeryHarvard Medical SchoolBoston
David J. Galas, Ph.D.Vice President, Chief Academic Officer,
and Norris Professor of Applied Life Science
Keck Graduate Institute of Applied Life Sciences
Claremont, Calif.
Judith G. Hall, O.C., M.D.Clinical Geneticist and Pediatrician, andProfessor of Pediatrics and Medical
GeneticsDepartment of PediatricsUniversity of British ColumbiaChildren’s and Women’s Health Centre
of British ColumbiaVancouver, Canada
Brigid L.M. Hogan, Ph.D.2
InvestigatorHoward Hughes Medical Institute, andHortense B. Ingram ProfessorDepartment of Cell BiologyVanderbilt University School of MedicineNashville, Tenn.
Robert B. Jaffe, M.D.2
Fred Gellert Professor of Reproductive Medicine and Biology, and
Director, Center for Reproductive Sciences
Department of Obstetrics, Gynecology, and Reproductive Sciences
School of MedicineUniversity of California San Francisco
Edward R.B. McCabe, M.D., Ph.D.2
Professor and Executive ChairDepartment of PediatricsSchool of MedicineUniversity of California Los Angeles
Anne McLaren, M.S., D. Phil.Principal Research AssociateWellcome Trust and Research CampaignInstitute of Cancer and Developmental
BiologyUniversity of CambridgeUnited Kingdom
Gerald M. Rubin, Ph.D.1
Vice President for Biomedical ResearchHoward Hughes Medical Institute, andProfessor of GeneticsUniversity of CaliforniaBerkeley
Mark Siegler, M.D.Lindy Bergman ProfessorDepartment of Medicine, andDirectorMacLean Center for Clinical Medical
Ethics
Pritzker School of MedicineUniversity of ChicagoChicago
OVERSIGHTMaxine Singer, Ph.D.1 ,2 (chair)Committee on Science, Engineering, and
Public Policy andPresidentCarnegie Institution of WashingtonWashington, D.C.
Corey S. Goodman, Ph.D.1 (chair)Board on Life Sciences National Research Council, andPresident and Chief Executive OfficerRenovis Inc., andProfessor of NeurobiologyDepartment of Molecular and Cell
BiologyUniversity of CaliforniaBerkeley
PROFESSIONAL STAFF
Deborah D. Stine, Ph.D.Study Director and Associate Director,COSEPUP
William Wells, Ph.D.Consultant Science Writer
Susan A. Daniels, Ph.D.Consultant Research Associate
Robert Cook-Deegan, Ph.D.Senior Program Officer, IOM
Frances E. SharplesDirector, BLS
Richard E. BissellExecutive Director, PGA/COSEPUP
and
Funding: The development of this report was supported by the National Research Council.Copyright 2002 by the National Academy of Sciences. All rights reserved. This document may be reproduced solely for educational purposes without the written permission of the National Academy of Sciences.Printed in the United States of America.
1 Member, National Academy of Sciences2 Member, Institute of Medicine

About the National Academies
For more than 100 years, the National Academies have provided independentadvice on issues of science, technology, and medicine that underlie many questionsof national importance. The National Academies, comprising the NationalAcademy of Sciences, the National Academy of Engineering, the Institute ofMedicine, and the National Research Council, work together to enlist the nation'stop scientists, engineers, health professionals, and other experts to study specificissues. The results of their deliberations have inspired some of America's mostsignificant and lasting efforts to improve the health, education, and welfare of thenation. To learn more about the Academies activities, check our Web site atnational-academies.org.
For More Information
Additional Information on this report, the panel membership, and its study isavailable at www.nationalacademies.org/humancloning. The entire report,Scientific and Medical Aspects of Human Reproductive Cloning, is available fromthe National Academy Press, 2101 Constitution Avenue, NW, PO Box 285,Washington, DC 20055 (1-800-624-6242 or 202-334-3313 in the Washingtonmetropolitan area; Internet http://www.nap.edu).