Embed Size (px)
Citation preview

Lee Williams, Helen Lodder, Rhys Jones, Steve Jordan, Richard Calverley, Matthew Cleeve & Joanna Caulfield. Biotage GB Limited, Dyffryn Business Park, Ystrad Mynach, Mid Glamorgan, CF82 7RJ, UK.
Introduction Traditional liquid-liquid extraction (LLE) provides very clean extracts. In many cases lower recoveries, laborious liquid handling issues and difficulty during automation can limit its success in sample preparation. Supported Liquid Extraction (SLE) is a 96-well high throughput technique that is analogous to traditional LLE. In SLE, the extraction interface occurs between the buffered sample absorbed onto an inert solid support and a water immiscible solvent. The high surface area of the material provides excellent extraction efficiency, while alleviating many of the liquid handling issues associated with traditional LLE. This poster compares ISOLUTE SLE+ with traditional LLE in terms of recoveries and demonstrates equivalent limits of quantitation with smaller sample volumes using the supported liquid extraction (SLE+) approach.
Comparison of Liquid-liquid Extraction (LLE)
and Supported Liquid Extraction (SLE):- Equivalent Limits of Quantitation with
Smaller Sample Volumes.
Lee Williams, Helen Lodder, Rhys Jones, Steve Jordan, Richard Calverley, Claire Desbrow, Gary Dowthwaite & Joanna Caulfield Biotage GB Limited, Dyffryn Business Park, Ystrad Mynach, Mid Glamorgan, CF82 7RJ, UK.
Experimental Procedure Reagents Non-steroidal anti-inflammatory drugs (NSAIDs), β-blockers, ammonium hydroxide and formic acid were purchased from Sigma Chemical Co. (Poole, UK). Human plasma was obtained via the Welsh Blood Service (Pontyclun, UK). Urine was donated by a healthy human volunteer. All solvents were HPLC grade from Fisher Scientific (Loughborough, UK). Sample Preparation Supported Liquid Extraction Procedure Plate: ISOLUTE SLE+ 400 Supported Liquid Extraction Plate, part number 820-0400-P01 Sample pre-treatment:- Acidic analytes (NSAIDs):- Plasma (200 µL) pre-treated 1:1 v/v with 1% formic acid aq. Basic analytes (β-blockers):- Plasma (200 µL) pre-treated 1:1 v/v with 0.5M ammonium hydroxide.

Step 1:
Apply aqueoussample
Step 2:
Wait for 5 min.
Step 3:
Add organic solvent
Step 1:
Apply aqueoussample
Step 2:
Wait for 5 min.
Step 3:
Add organic solvent
Figure 1. Schematic of ISOLUTE SLE+ Supported Liquid Extraction procedure. A single well of the 96-well plate is shown
Sample Application: The pre-treated plasma (total 400 µL) was loaded onto the plate, a pulse of vacuum applied to initiate flow and the samples left to absorb for 5 minutes. Analyte Elution: Addition of 2 x 900 µL of either MTBE (NSAIDs) or EtOAc (β-blockers).
Liquid-liquid Extraction Procedure Plasma (500 µL) was pre-treated 1:1 v/v with: 1% formic acid aq and extracted with 1.8 mL of MTBE (NSAIDs); or 0.5M ammonium hydroxide and extracted with EtOAc (β-blockers). The layers were left to separate and the organic aliquot removed. Post Extraction: The eluate was evaporated to dryness and the analytes reconstituted in 500 µL of appropriate H2O/MeOH mixtures prior to analysis. HPLC Conditons Instrument: Waters 2795 Liquid Handling System (Waters Assoc., Milford, MA, USA). Column: Zorbax Eclipse XDB C18 3.5 µm analytical column (100 x 2.1 mm id,
3.5 µm) (Agilent Technologies, Berkshire, UK). Guard Column: C8 guard column (Agilent Technologies, Berkshire, UK). Mobile Phase: 0.1% formic acid aq and MeCN (acetonitrile) at a flow rate of 0.25 mL/min using various gradients. Injection Volume: 15-25 µL Temperature: Ambient Mass Spectrometry Instrument: Ultima Pt triple quadrupole mass spectrometer (Waters Assoc., Manchester, UK) equipped with an electrospray interface for mass analysis. Positive and negative ions were acquired in the multiple reaction monitoring mode (MRM). All β-blockers were analysed in positive ion mode, whereas, the NSAIDs required both positive and negative MRM transitions.

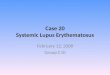
Desolvation Temperature: 350 °C Ion Source Temperature: 100 °C Collision Gas Pressure: 2.4 x 10-3 mbar Results Figures 2 and 3. show SLE+/LLE recovery data for the β-blockers and NSAID’s, respectively. This data is based on the recovery compared to blank plasma sample fortified post extraction at the same concentration. Figures 4 and 5. show spiked sample response against a standard at the same concentration for the β-blockers and NSAID’s, respectively. This data takes into account the recovery and suppression observed from the two techniques. Figure 6. shows β-blocker MRM transitions for plasma extracted at 50 pg/mL with both SLE+ and LLE. Tables 1 and 2. Show limits of quantitation observed for the β-blockers and NSAIDs, respectively. Some analyte LoQ’s were lower than the lowest level extracted and as a result the level was estimated based on the lowest level signal to noise.
0
20
40
60
80
100
Atenolol Nadolol Metoprolol Oxprenolol Propranolol Alprenolol
β-blocker Recovery Comparison
LLE Plasma LLE Urine SLE+ Plasma SLE+ Urine
Figure 2. SLE+/LLE β-blocker recovery comparison (200 pg/mL).

0
20
40
60
80
100
NSAID Recovery Comparison
LLE Plasma LLE Urine SLE+ Urine SLE+ Plasma
Figure 3. SLE+/LLE NSAID recovery comparison (10 ng/mL).
0
20
40
60
80
100
120
Atenolol Nadolol Metoprolol Oxprenolol Propranolol Alprenolol
β-blocker Signal Response Comparison
LLE Urine LLE Plasma SLE+ Plasma SLE+ Urine
Figure 4. SLE+/LLE β-blocker spiked signal comparison (100 pg/mL).

0
20
40
60
80
100
NSAID Signal Response Comparison
LLE Plasma LLE Urine SLE+ Urine SLE+ Plasma
Figure 5. SLE+/LLE NSAID spiked signal comparison (10 ng/mL).
Time1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
5: MRM of 2 Channels ES+ 250.1 > 116.1
4.28e36.35
5: MRM of 2 Channels ES+ 260.1 > 116.1
2.67e36.27
4: MRM of 2 Channels ES+ 266.1 > 72.1
6.25e35.43
3: MRM of 1 Channel ES+ 268.1 > 116.1
2.25e34.35
2: MRM of 2 Channels ES+ 310.1 > 254.1
1.50e32.10
1: MRM of 2 Channels ES+ 267.1 > 190
1.16e31.52
LLE 50 pg/ml Plasma
Atenolol
Nadalol
Metoprolol
Oxprenolol
Propranolol
Alprenolol
Time1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
1.00 2.00 3.00 4.00 5.00 6.00 7.00
%
0
100
5: MRM of 2 Channels ES+ 250.1 > 116.1
2.37e36.35
5: MRM of 2 Channels ES+ 260.1 > 116.1
1.42e36.26
4: MRM of 2 Channels ES+ 266.1 > 72.1
3.81e35.44
3: MRM of 1 Channel ES+ 268.1 > 116.1
1.38e34.34
2: MRM of 2 Channels ES+ 310.1 > 254.1
1.79e32.14
1: MRM of 2 Channels ES+ 267.1 > 190
1.01e31.52
SLE+ 50 pg/ml Plasma
Atenolol
Nadalol
Metoprolol
Oxprenolol
Propranolol
Alprenolol
Figure 6. β-blocker MRM Comparison between LLE and SLE+ extracted plasma (50 pg/mL).

Plasma Urine Analyte SLE+ LoQ
(ng/mL) LLE LoQ (ng/mL)
SLE+ LoQ (ng/mL)
LLE LoQ (ng/mL)
Acetaminophen 5 10 - -
Sulindac <1 (0.5) <1 (0.5) <1 (0.5) <1 (0.3) Ketoprofen 3 2 3 2
Naproxen 10 10 10 5 Flurbiprofen 10 10 10 5
Indomethacin 2 2 3 2 Diclofenac 1 (0.5) 1 (0.5) 1 (0.4) 1 (0.2)
Mefenamic Acid <1 (0.2) <1 (0.2) <1 (0.1) <1 (0.05)
Plasma Urine
Analyte
SLE+ LoQ (pg/mL)
LLE LoQ (pg/mL)
SLE+ LoQ (pg/mL)
LLE LoQ (pg/mL)
Atenolol 100 100 200 200
Nadalol 50 50* 50 50*
Metoprolol <50 (25) <50 (20) <50 (25) <50 (20)
Oxprenolol <50 (25) <50 (15) <50 (25) <50 (15)
Propranolol <50 (25) <50 (15) <50 (25) <50 (15)
Alprenolol <50 (25) <50 (15) <50 (25) <50 (15)
Table 1. LLE/SLE+ β-blocker LoQ comparison.
*RSD > 10%. - acetaminophen detected in urine. Parentheses – estimated levels based on S/N at previous level
Table 2. LLE/SLE+ NSAID LoQ comparison.

Europe Service and Support Telephone: +46 18 56 59 00 E-mail: [email protected]
United States Service and Support Telephone: 1 800 446 4752 press (3) at the auto attendant E-mail: [email protected]
Japan Service and Support Telephone: +81 422 28 1233 E-mail: [email protected]
Europe and ROW If your country is not listed here, contact your local distributor. Please visit our website at www.biotage.com for your local distributor contact details.
www.biotage.com
© 2009 Biotage. All rights reserved. All trademarks are the property of their respective companies.
Conclusions • SLE+ showed higher recoveries than LLE for all analytes. • SLE+ also showed better spiked signal response than LLE for all analytes. • SLE+ showed similar LoQ’s for a number of the analytes screened when extracting 200 µL
compared to 500 µL plasma extractions using LLE. Illustrating the fact that lower sample volumes can be used with ISOLUTE SLE+ compared to traditional LLE.
• Some analytes showed lower LoQ’s in LLE. However, the differences were not substantial and similar levels could be obtained using a higher plasma to buffer ratio with SLE+.