-
7/27/2019 asimp Na 1950
1/13
ASYMPTOMATICHYPONATREMIA IN PULMONARYTUBERCULOSIS 1
BY E. A. H. SIMS,2 LOUIS G. WELT,3 JACK ORLOFF,4 AND JAMES W.
NEEDHAM
(From the Department of Internal Medicine, Yale UniversitySchool
of Medicine,Ne-w Haven, Conn.)
(Submitted for publicationJune 21, 1950;accepted,August 28,
1950)
INTRODUCTION
In the Goulstonian lecture of 1936 McCance (1)first clearly def
ined thephysiologicaland chemicalchanges induced by the depletionof
salt in normalman. He confirmed Gamble's (2 ) postulate ofthe
jealouslyguarded constancy of the concentra-tion of total base in
the serum. This was largelyeffectedby the elaborationof a
urinevirtually freeof salt soon after th e institution of salt
deprivation.More recently Platt (3 ) noted that the concen-tration
of total base may fall very slightly in anormal person just
beforemaximal tubular reab-sorp tio n ofsalt occurs. This renal
defenseislacking in Addison's disease and in those casesof kidney
diseasein which salt continuesto be ex-creted in the urine at a
timewhen th e concentra-tion of sodium in th e serum has fallen
belownormal.
Subsequent to McCance's classical description,Winkler and
Crankshaw (4 ) describeda new syn-drome characterizedby renal
salt-wasting andsubnormal concentrationsof sodium in the serumin
patients with pulmonary disease. Of th e threecases documented, two
had far-advanced pul-monary tuberculosisand one had carcinoma of
thelung. Besidesexcreting salt under conditionswhich would normally
be associatedwith maximalreabsorptionof sodium, these pat ients
rapidlyeliminated intravenouslyadministeredsalt andwere unable to
maintain the concentrationof so-
dium in the serum at a normal level. Adrenal1 Aided by a grant
from the Fluid Research Funds of
the Yale UniversitySchool of Medicine,and by an insti-tutional
grant from the National Heart Institute, U. S.Public Health
Service.
2Present address: College of Medicine, University ofVermont,
Burlington,Vt .
8 Work done in part during the tenure of a Postdoc-torate
Fellowship,U. S. Public Health Service.
4Work done in part while a fellow of th e DazianFoundation for
Medical Research and during the tenureof a Life Insurance Medical
Research Fellowship. Pres-ent address: National Heart Institute,
Bethesda, Md .
cortical extractwas without influenceon the per-sistent wastage
of salt in one patient.
Thorn, Howard and Dayman (5) analyzed alarge number of cases
with pulmonary tubercu-losis and found none with a subnormal
concentra-tion of sodium in th e serum. However, tw o ofhis
patients did continue to excrete sodium afterthree days on an
intakelow in salt. They did notconfirm Winkler's findingsand
attributedthe lowconcentrationof chloride in the serum in manyof
his patientsto retention ofbicarbonate.' Westover, Stiven,and Garry
(6) observed lowconcentrationsof sodium in the serum of 55 of
114patients with tuberculosis. In a smallnumber inwhom balanceswere
calculatedtherewas evidencesuggestiveof wastage of salt. More
recentlyKolmer and his associates(7) analyzed the chem-ical data of
a group of tuberculoussubjectsstatis-tically. The concentrationof
total base was some-what lower than normal. It is of interest that
thisdepressionwa s better correlatedwith magnitudeof daily
temperature variations than with theseverity of the disease as
estimated by X-rayexaminations.
Sincenone of these studies clearly definedthechemicalanatomy or
elucidatedthe mechanism ofthe syndrome of pulmonary salt-wasting,
thisstudy wa s undertaken. -It wa s hoped that by in-vestigatingthe
role of the kidneys, the adrenalcortices, as wellas the status of
the cellular struc-
tures of the body,an explanationfo r the chronicdepressionof the
effective osmotic pressure ofthe extracellular water might be
found. Alsoof importance to this study was the developmentof a
means of differentiating this conditionfromAddison's disease since
both are encountered inpatients with tuberculosis.
EXPERIMENTAL MATERIAL AND PROCEDURE
Ten male patients with advanced tuberculous diseaseand
hyponatremia were studied. Four of the ten wereNegroes. One of the
patients had miliary tuberculosis
1545
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
2/13
E. A. H. SIMS, LOUIS G. WELT, JACK ORLOFF, AND JAMES W.
NEEDHAM
0
0z
0 0 Bo4J 4-.01.4 4-i~~~~~~~~~~~.
Ca~~~~~C
- a a ) -oa0. )d ..c I..C
CL c l a a a
0
+..* 4) m a:) m) m) uCl ) ~~~ ~ ~U) U) U) U ) 0
.-~~~~~~~~~~~~~~~~~~~~~~~~~~~~~4 ."2otE ~~e to~ -*i ra ) auE
0'~E. O a-. e~i '3 '3 ' if) 130 ~ ~ ~ ~ ~ ~ ~ ~ ~ 0
0 ei if) if)}* ..iiI SS4 if 0% - '34 _ _ C a ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
~ ~ ~ ~ ~ ~ ~ W -^ S nI 'C 0% 0 ' C
. ' % ) 0
zo-
in
.azSe U) U) U) U) Ce - C
.tDemX~~X N %m
00~~~~~
C . , ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~
1
.0to 0 0 0 0 0 0 0 0 0
< X I Z'.+ ei 00 0 a ei 0 00 if i H1u C)
i U) U ) U U0Po 0 0 0 00 C) Ouf) 00 0 0 0 0 0 0o
w o o o o2ouooo o o o o oo0oa-C 0 0 c D Qf) C)' i C) Q QC0 0%
0
t~~~~~~~~~~~6m- 0 :z:1 o 0 to o t- o- o w o- o o, , o to to ol '
o Oe
_4 _ 4 ___ 4 _ f ) _4 if00
e 4
C) 0 0o to U t 00
-
7/27/2019 asimp Na 1950
3/13
ASYMPTOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
with pulmonary infiltration limited to one lobe. On eNegro male
with tuberculosis of th e adrenals and Ad -dison's disease was also
investigated during a crisis.Normal concentrationsof sodium in th e
serum werefound in 14 other patients with moderate or advanced
tu-berculosis, in three with advanced bronchiectasis,and infive
with various conditionsassociated with malnutri-tion. In addition,
th e hospital records of a large numberof patients with abnormally
low concentrationsof so-dium in the serum and continued excretionof
sodiumwere searched for ins tances in which the hyponatremiawas not
definitely secondary to kidney disease, adrenalinsufficiency, or
over-hydration during therapy. Threesuch instances were found, but
there was no t sufficientevidence to includethem definitely in th e
present group.The course, follow up, and subsidiarydiagnoses of
theten tuberculous patients are indicated in Table I. Someor all of
the following investigativeprocedures were car-ried ou t on each
patient depending upon th e clinical
conditionand severityof the illness.Subjects studied over an
extended period were pro-vided with a basic diet adequate in
calories and protein,but containingnot over 0.5 gm. of sodium
chloride perday. This was supplemented in some instances by milkand
cream containing0.3 gm. of salt. To this, weighedquantities of
table salt were added daily. Consecutive24-hour collectionsof urine
were made during the entireperiod of study and were analyzed fo r
chloride and so-dium. Five of the patients were treated with 1-2
gm.of streptomycin and one with 10 gm. of para-aminosalicylicacid
per day as well, but no essential change in theirregime was made
during the period of investigation.
Renal clearancesof endogenous creatininewere meas-
ured in seven patients. These patients were not cathe-terized,
but a moderate diuresis was induced to minimizeth e error from
residual urine. In one patient th e clear-ances of mannitol and of
urea were determined.
In five patients acute balances of sodium and ofchloride were
measured on one or more occasions overperiods of 24 hours at th e
beginning of which an in-fusioncontaining15 gm. of sodium
chlorideas a 39%solu-tion was given. Additional salt was given by
vein orper os in all but one patient.
Five or 20 mgm. of desoxycorticosteroneacetate inoil 5 were
administered to four patients in on e or twointramuscular doses
daily. Te n cc . of aqueous adrenalcortical extract (Wilson) or 1
cc. of Lipo-adrenal ex-tract (Upjohn) were given in intramuscular
doses at in-tervals of 12 hours.
Both procedures of the "water test" fo r adrenal insuffi-ciency
were carried ou t as describedby Robinson, Power,and Kepler (8).
The decrease in circulatingeosinophiles
following th e infus ion of1.5 mgm. of epinephrinein nor-mal
saline given over a periodof one hour was studiedin three patients
according to the technique of Recant,Forsham, and Thorn (9). In the
remaining patients0.3 mgm. of epinephrine was given subcutaneously
asdescribed by Thorn and his col leag ues (10 ).
Totaleosinophilecounts were made four hours after the epi-nephrine
was given,and in th e majority of pat ientsat twohours as well.
Urine for determination of 17-ketosteroidswas preserved with 1 cc.
of concentrated hydrochloricacid per liter and refrigerated until
analyzed.
5 Kindlyfurnished by Dr. Kenneth Thompson of Or-ganon,
Inc., Orange, N. J.
TABLE II
Effectof variationsin the intakeof sodium chloride;analysesof
serum and urine
Free intake of sodium chloride Maximum intakeof Minimum intake
of sodium chloridesodium chloride
Subject Serum Urinary excretionFia
_ _ _ _ _
-_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ -Intake
Total srmAverage Total Final Foinalime sodium intake time sodium
excretionNa Cl HCOa Sodium C h l o r i d e s o i m o d u exrtn
mEq./L mEq.IL mEq./L mEq./L mEq./day mEq./L mEq./day mEq./day
days mEq./L mEq. Iday days mEq./L mEq. /dayI 126 88.8 26.4 40 64
220 12 134.0 8 7 128.0 8II 127 90.9 25.8 85 72 130 110 85 2 134.0
43 3 125.0 29III 124 80.8 32.6* 44 67 108 166 260t 6 132.0IV 131
87.5 28.3 92 93V 128 93.4 25.0 35 114 97 3 134.0VI 122 95.0 26 20
43 23 51 13 1 118.0 12
2 112.0 41VII 123 90.0 25.8t 103 170 268 11 135.0 13 3 132.0
11
6 126.0 5VIII 128 95.2 15 51 14 47 185 8 135.0 13 4 126.0 27IX
127 89.2 18.0 345 198 230 5 124.0 8 3 119.0 6.7X 129 92.8 33 88 44
117 97 13 133.0
* On e day previouslyt Desoxycorticosterone acetate in oil 5
mgm. per da y given over this period
Two dayspreviously 24.8on admission seven days previously As
chloride
1547.
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
4/13
E. A. H. SIMS, LOUIS G. WELT, JACK ORLOFF, AN D JAMES W. N EED H
A M
TABLE II I
Alterationsassociatedwith administrationof largeamounts of
NaCL
Concentrations of Na in extracellularwaterSubject Sodium
rSetaind Wt . Plasma a
Initial Final Anticipated* volume
mEq. % mEq./L mEq./L mEq./L Kgm. % mEq.I-A 427 93 133 134 145
1.5 18 - 87I-B 427 20 137 137 139 -0.4 1 - 42II 256 61 128 .136 133
7 - 92VI 856 98.5 114 135 137 35 -132VII 427 58 129 137 136 0.2 8 -
22X 324 41 131 136 134 -0.3 - 45
EV t 739 95.3 129 136 147 - 27 +104
* Estimated from positivebalance of Na an d assuming no change
in total body water.t Patient with adrenal cortical insufficiencyin
crisis.
Th e urinary excretionof sod ium and chlorideas in-fluencedby
the gradual reductionof dietary salt wasmeasured.
METHODS
Serum proteinfractions were determined by the
Milnemodificationof th e techniqueof Majoor (11), urea bythe
gasometric method of Van Slykeusingurease or hy-pobromite (12), and
mannitol by Elkinton'smodification-of the Smith, Finkelstein, and
Smith procedure (13).Creatininewas determined by the method of
Peters (14).Readings were made exactly 20 minutes after the
ad-dition of alkaline picrate, since filtrates from serumdarken
progressivelyon standing. 17-Ketosteroidsinurinewere
estimatedcolorimetricallyeither by the method
of Cahen and Salter (15) or of Holtorffand Koch
(16).Easinophileswere stained by th e techniqueof Randolph(17),
using phloxineB in a 1: 1 aqueous dilution ofpropyleneglycol. Th e
average of from two to fourcounts in a Levy chamber 0.2 mm. in
depthwa s taken.Other methods used in this laboratory have been
re-
TABLE IV
Effectof variationsof the concentrationof sodium in theserum on
renalckarances in patientswith
asymptomatic hyponatremia
Renal clearance*
Subject Wt . Serums o d iu m
EndogenousMannitol UreacreatinineKgm. mEq./L cc./min.
I 44 134 111, 108126 101, 102133 69, 66127 82, 76
IV 43 131 61VI 54 112 73VII 45 135 67, 69
126 64,69ViII 54 .1-3 62,62
128 73, 75X 49 125 80, 73
* Calculationsforconsecutiveclearanceperiodsare given.
ported in previous publica tions (18). Th e methods fo
rcalculating changes in plasma volume from changes inrelative re d
cell volume and hemoglobin and for changesin t he dis tributi on o
fwater and electrolytes have beendescribedelsewhere (19, 20).
RESULTS
The analytical and derived data are presentedin Tables I-VI and
Figures 1-4.
I. General Clinical ObservationsAll the members of this group of
patients in
whom hyponatremia was found were chronically
ill and malnourished, and four (II, III, VI, an dVII) were
acutelyill when first studied. Sevenof the patientsdied within on e
to five months fol-lowing admission,an d th e remaining three have
apoor prognosis for ultimate recovery. The essen-tial clinical data
on thesepatientsare summarized
TABLE V
Robinson-Power-Keplerwater tests in threeptientswith
asymptomatichyponatremia
Procedure I Procedure II
Urine volume
Subject Date SedriumNiiht Maximum valueperiod day.(9 hrs.) vr
o
mEq.IL cc. cc.I 11- 8-48 126.0 400 240 40
11-27-48 127.0 650 205 3012- 7-48 129.7 330 195 39
VII 3-17-49 135.0 920 355 10*X 8-30-49 130.0 615 265 43
* The intakeof sodium chloridewas 15.8gm. for sevendays prior to
the test.
1548
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
5/13
ASYMPTOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
TABLE VI
The effectof administrationof epinephrineon
circulatingcosinophilesin six patients with asymp-
tomatichyponatremia
Circulating eosinophiles
Epineph-Subject rine % fall
admin. Initialcount
2 hrs. 4 hrs.
mgm. per cu. mm. % NI (11-18) 1.5 300 56 38
(12-4) 1.5 300 31 33III
-
7/27/2019 asimp Na 1950
6/13
E. A. H. SIMS,LOUIS G. WELT, JACK ORLOFF, AND JAMES W.
NEEDHAM
nitrogenin the blood was normal in al l patientsandin none was
there gross evidenceof renal orcardiovasculardisease, with the
exceptionof one(I), who had calcification of th e abdominal aortaby
X-ray, and another who gave a history of hy-
pertensionof unknown degree nine years previ-ously. Only one
patient (III) wa s observed tohave significantcarbon dioxide
retention, in spiteof the severity of th e pulmonary involvement
inthe majorityof th e other patients. Concentrationsof potassium in
th e serum were within normallimits. When these patientswere eat
ing thewarddiet with a free intake of salt, which wa s usuallythe
casewhen they were first studied,they contin-ued to excrete from 40
to 90 mEq. of sodium perday in spite of the fact that the
concentrationsofsodium in the serum ranged from 122 to 131mEq./L
(Table II).
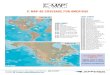
In two patients th e tendency toward hypona-tremia was found to
be reversible. It is shown inFigure 2 that when this patient (VII)
was againgivena diet low in sodium 75 days after the first
periodof deprivation,he maintained his concen-tration of sodium
in the serum between 138 and136 mEq./L. During th e interval his
weight hadincreased2 Kgm. on a regime of bed rest
andstreptomycin,his sputum production had de-
creased by a third, and his daily temperature riseshad decreased
from an average of 102 to 100 de-grees F. However, the X-ray of his
chest wasunchanged. Nine months after his first period
ofdeprivationof salt, a second patient (I ) was placedon a diet for
seven days which wa s as low in so-dium as could be arranged at th
e sanitorium towhich he had been sent. Over this periodhis
con-centrationof sodium in the serum remained con-stant at 133 to
134 mEq./L. During this intervala pneumoperitoneum had been induced
and he hadgainedconsiderableweight.
II . Th e effects of variationin salt intakeFive patients (I,
III, VII, VIII, and IX) were
given a moderate or high intake of salt for a pe-riod of five to
12 days. In one who sufferedfrom
CHLORIDE'
UE /0AY 0 o _I 0 le it to ts so 3 40 4 o 59 o t 75 0 es 900 e
lo, #O * liO*,
FIG.2. CHANGESIN BLOODPRESSURE, SERUM CONCENTRATIONS OF SODIUM,
AND URINARY EXCRETION OFSODIUMAND CHLORIDEIN RELATIONTO
VARIATIONSIN INTAKE OF SALT AN DTO ADMINISTRATION OF
DESOXY-CORTICOSTERONEACETATEAN D OF ADRENAL CORTICALEXTRACT IN A
PATIENT (VII) WITH ASYMPTOMATICHYPONATREMIA
1550s
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
7/13
ASYMPTOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
24
iIW
010
'ZIa10
a11
10
w
IUVWA _ VILVvs q / _ 5 mo/d _
..... . ..............I a . .. . .. .a .
5 l0 15 20 0 5 20TIME IN DAYS
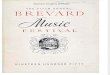
FIG.3. EFFECT OF DESOXYCORTICOSTERONEACETATE UPON THE
URINARYEXCRETIONOF SODIUMAND CHLORIDEIN FOURPATIENTS WITH
ASYMPTOMATICHYPONATREMIA
advanced tuberculosisand carcinoma of the phar-ynx treated with
irradiation, daily infusionscon-taining 13.5 gm. of sodium
chlorideover a five-day period failed to raise the concentration of
so-dium in the serum above 125 mEq./L. Therewas no evidence of
congestivefailure and noperipheraledema in this case. Three of the
pa-tients given more than 185 mM. of salt per dayhad
final concentrationsof sodium in the serum inthe low normal
range, 132-135 mEq./L. In twoother patients (I I and X) final
concentrations ofsodium in the serum of 133-135 mEq./L wereobserved
followinga somewhat lower intake ofsalt.
The sodium in the diet of five patients (I, VI,VII, VIII, an d
IX ) was reduced to 8-13 mEq./day for two days or more. Since the
quantityofsalt added to the basic diet ha d been variouslyre
-stricted during the preceding periods,this did no t
constitute an abrupt deprivationof salt. In allbut one
instancethe renalexcretionof sodium wa sreduced to 8 mEq./day or.
less, and in all instancesthe concentrationof sodium in the serum
fell be-fore the minimal urinaryexcretionof this ion wasreached.
This is illustrated in Figure 1, days 2-8and Figure 2, days 40-42.
A fifth subject (II)who was acutely ill with
tuberculouspneumonia
had an excretionof 29 mEq./day of sodium and aconcentrationin
the serum of 125 mEq./L whenthe intakeof salt was reduced to 43
mEq./day.However, during these studies of deprivationtheexcretionof
sodium, while often sharplyreduced,did not reach th e extremelylow
valuesusuallyas-sociated with hyponatremia due to depletionofsalt
in other conditions. It was strikingto observethroughout the
studiesthat thesepatientswere freeof symptoms attributableto
depletionof salt andsometimes had an indifferenceto their
dietarysalt
1551
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
8/13
E. A. H. SIMS, LOUIS G. WELT, JACK ORLOFF, AND JAMES W.
NEEDHAM
20
4-
lS
6
Sn
a
1:z;
z
L.B. A- 004T KG 45 45 445SERUMNA 136 135 136 132 135 135SERUMCL
92 97 96 95
.i0.| l l L A ill
.
M a C 13759WT KG 493 495 49.6SERUMNA 131 127 133 13 2 3SERUMCL
93
993 9 3
DC_
l o
hpoAreo
"M1. C 2960 s W.W.9 93703S E R U M A 32 132 129 132 133
SERU CL 96 9X 93 9f 91
DO
soe .... z1e 0 ^ .. ._ . _ .
Time in Dole
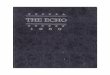
FIG.4. EFFECT OF ADRENALCORTICALEXTRACTUPON THE
URINARYExCRE-TION OF SODIUM AND CHLORIDEIN FOUR PATIENTS WITH
ASYMPTOMATICHYPONATREMIA
when the concentrationsof sodium in the serumwere at levels
generallyassociatedwith collapseinother situations
involvingdepletionof salt. Onlyone patient (X ) exhibited craving
for salt whenon a sodium restricted regime. Muscle crampswere not
seen.
One patient (VI) demonstrated that this groupis not immune to
the effects of true depletionofsalt. This patient was acutely ill,
febrile, andsweating considerably. It was later learnedthathe had
rejected a considerable portion of the 85mEq. of sodium that were
added to hi s diet for athree-day period. He excreted only 12 mEq.
ofsodium the first day that hi s intake of this ionwas reduced to
13 mEq. During the followingdaya bout of mild diarrhea added to the
loss of sodiumin sweat and sputum, and the concentration of
sodium in his serum fell from 118 to 112 mEq./L.At this pointhe
developed diaphoresis,acute anx-iety, and borderline
vascularcollapse,al l of whichwere rapidly improved by an
infusionof hyper-tonic saline. It is notable that these signs
andsymptoms developed when the concentration ofsodium in the serum
was only 6 mEq. below thatat which the renal excretion of sodium
had beensharplyreduced. In contrast to the crisis in Ad -dison's
disease, the non-protein nitrogen concen-tration of the blood did
not rise above 33 mgm. %o,nor th e potassium above 5.1 mEq./L.
Therewas no elevationof temperature.
When there were alterations in the quantityofsalt ingestedas
described above, there were varia-tions in the concentrations of
sodium in the se -rum of 2. to 12. mEq./L. An additionalpatient
1552
25
20
IN
O0
2c
2 4 6 a 10 12 14 Z 4 6 a so 12 14
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
9/13
ASYMPTOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
(X) whose intake of salt wa s not pushed to ahigh level had a
variationof only 3.5 mEq./L inhis concentrationof sodium in th e
serum. Theminimum concentrationsof sodium in Table IIoccurred
before orapproximately at the time whenthe excretionof sodium had
first reached a lowlevel, so they reflect a loss of sodium via the
urine.
Infusionsof 256 mM. of sodium chlor ide asa3% solution were
administeredto five patients.In addition, al l but one
receivedadditionalsaltin the course of a 24-hour periodeither as
normalsaline intravenouslyor as table salt by mouth(Table III). Fo
r comparison, data ar e also pre-sented from a patient with
Addison's disease(EV) in crisis during the first 18 hours of
therapy.A ll th epatientsexcept VI and EV had free access
to water during the balanceperiod. When the ini-tial
concentrationof sodium was low, from 41 %to 98.5%oof the
administered salt was retained(althoughin this calculation no
correctionwa smade for the variable loss of sodium in sweat).There
were no significantshifts of sodium betweenthe intracellular and
extracellular compartments.
It is assumed that where an antecedent deple-tion of both water
and sodium exist, water will beretained followingthe
administrationof salt andwill be manifestby increasesin body weight
andplasma volume. In addition, the observed con-centrationof sodium
in th e extracellularwater atthe end of the balanceperiodshould be
less thanthe concentrationof sodium as estimatedfromthe positive
balanceof this ion with the assump-tion tha t there had been no
increasein total bodywater. This "anticipated"concentrationof
so-dium in the extracellular water is presentedinTable III.
Th e insignificantchanges in weightand in theper cent increasein
plasma volume and the goodagreement between th e observed and
anticipatedconcentrationsof sodium in the extracellular
fluidsuggest that in patients I-B, II, VII, and X thevolume of
water was not previouslycontracted.In contrast, in patients I-A and
VI, who hadsuffered antecedentextrarenal losses of salt andwater,
there were retentionsof salt and increasesin plasma volume similar
to those of th e patient(EV) with Addison's disease. Moreover,
therewa s considerabledisagreementbetween th e ob-served and
anticipatedconcentrationsof sodium inthe extracellularwater in
patients I- A and EV.
Th e agreement of this functionin patient VI maybe explainedin
part by a marked diaphoresisthatoccurred early in th e
balanceperiod.
Endogenous creatinineclearancesranged from61 to 80 cc./min.
(Table IV). Figures for theheightsof these patients ar e not
available,but inview of their low weights,averaging 49 Kgm., itis
probable that correctedclearanceswould fallwithinthe low normal
range. In two of the pa-tients (VII and VIII) creatinine
clearancesweremeasured when the concentrationof sodium inth e serum
had been forced to a maximum by ahigh intake of salt and again when
the subjecthad been deprived of salt. Under these
varyingconditionsthe creatinineclearanceeither did notchange (VII)
(Figure 2, days 13 and 43) or was
actuallyhigherin the hyponatremic state (VIII).In an additional
patient(I) mannitol clearanceswere similarly measured both when the
concen-tration of sodium in the serum was low and whenit was
normal. These did not differ significantly.Urea clearanceswere
somewhat higher at thelower concentrationof sodium in the serum
inthis same patient.
III. The response to adrenal steroidsIn two patients (I and VII)
20 mgm. of
desoxycorticosteroneacetate (DOCA) in oil ad-ministeredfor four
days produced a sharp re-ductionin sodium excretion, followedby an
in-creasedexcretionon discontinuingthe injections(Figure 3). In
patient I a gain in weight of 2.6Kgm. and the development of
pitting edema of th eextremities wa s noted during the period
whenDOCA was administered,while patient VIIgained 2.1 Kgm. over the
same period. Althoughan exact balance cannot be computed from
thedata .available, both patients appeared to retainmore water than
could be accounted for on thebasis of the quantity of sodium
retained. Fivemgm. of DOCA per day produced a similar butless
marked reductionin the excretionof sodiumin patients I, VII, and X
which wa s also followedby a secondary increase in excretionabove
thebasal level after cessationof th e injections. Th eeffect of
injectionsat 12-hour intervals of 10 cc.of adrenal cortical extract
(Wilson) or of anequivalentamount of lipo-adrenal extract (Up-john)
was studied in four patients. The resultsare shown in Figure 4.
There was clearlyno effect
1553
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
10/13
E. A. H. SIMS, LOUIS G. WELT, JACK ORLOFF, AND JAMES W.
NEEDHAM
when lipo-adrenalextractwa s given to patientI orwhen aqueous
extractwas given to patientVIII. Areductionin the excret ionof
sodium occurred dur-ing a portion of the period in which aqueous
ex-tract was administered to patient VI I on tw o oc-
casions. However, th e reduction preceded theinjection on th e
first occasionand was not sus-tained during the entire period of
administrationon either occasion. In the caseof pat ientX th
eexcretionof sodium varied spontaneously duringa number of weeks
both beforeand after adrenalextract wa s given and reached a low
value oneand three days prior to the injections. There wasno
secondary increasein the excretionof sodiumabove the basal level on
discontinuingthe injec-tions in any of the patients.
IV. Est imateof adrenalcortical functionAt one time or another
during their course in
the hospitala diagnosisof adrenal insufficcywas
seriouslyentertainedin four of the patients(I, III, VII, and X) on
the basis of clinical orlaboratoryfindings. It wa s of interest,
therefore,to study their response to the current tests
ofadrenocorticalfunction. The response to depriva-tion of salt has
been describedabove.
In three of the patients (I, VII, and X)
theRobinson-Power-Kepler water test was done.Th e results are
givenin Table V. Procedure I ofthe test wa s invariablypositivein
that th e normaldiuretic response to ingestedwater was not ob
-tained. In onlyone patient (VII) was ProcedureII positive, with an
"A" value of 10. This test,however, was done when the patient had
taken15.5 gm. of salt in his diet the precedingday,which is in
excess of the "usual diet without salt"specifiedby the authorsof
the test. In on e pa-tient (I) th e "A " value was not
significantlychanged when the test was repeatedafter he hadbeen
given 23 gm. of sodium chloride two daysprior to the test.
Th e eosinopeniceffect of epinephrinewas stud-ied in six
patients. In al l of these a decreaseincirculating eosinophilesof
50%o or greater wasfound on at least on e test. The
depressionofeosinophileswas, however, apparentlynot as sus-stained
as in normal subjectsgiventhese quanti-ties of epinephrine,for when
counts were made att wo hours as well as at four hours, in four
out
of five instancesthe two-hour count wa s lower.Thus, patient X
had no eosinopenic response atfour hours in the initial test; a
second test demon-strated a 70% fall in eosinophilesat two hours.Th
e initial eosinophilecount in one acutely ill
patient (III) wa s less than 3 per cu.mm., so thatepinephrine
was not given.
Th e excretionof 17-ketosteroidsper 24 hourswa s low, 3.3 mgm.,
in one patient (VII) on a dayshortly after his admission with fever
and ad-vanced tuberculosis. Five otherpatients had low-normal or
normal values, the actual excretionap-pearingto be correlatedwith
the state of nutri-tion of the patient.
A five-hourintravenousglucose tolerancetestwas normal in three
patients tested (VII, VIII,
and X).Six patients came to autopsy (II, III, IV, V,IX, and
partial in VI) and al l were found to havenormal adrenals. Two
patients (I I an d III.) hadrenal lesions as described in Table
II.
DISCUSSION
The ability to excrete an almost sodium-freeurine, to retain a
large amount of intravenouslyadministeredsodium without benefitof
exogenoussalt-retaininghormone, to respond with an eosino-peniato
epinephrine,and the absence of gross orhistologicevidenceof
adrenalcortical disease atpost-mortem al l militate against adrenal
corticalhypofunctionas the primary defect responsiblefor this
clinical picture, althoughthis cannot becompletelyexcluded. Nor
does this syndromeappear to be a primary abnormalityof the
kidneys.Examination of the urine in thesepatientsusuallyrevealed no
abnormalities,and there were noevidencesof renal insufficiency. The
renal tu -bular cells responded by increasingthe reabsorp-tion of
sodium when DOCAwa s administeredindoses of 20 and 5 mgm. per
day.This abnormalityseems not to be a specificderivative of
tuberculosissince it has been re -portedin one case of
non-tuberculous pulmonarydisease(4). Moreover, althoughthe
observationsare not completelyconvincingat this time, thereare
suggestionsthat it may be found among pa-tients with non-pulmonary
disease. The commondenominator may not be an organ specific
dis-order, but a secondaryeffect in some instances
1554
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
11/13
ASYMPTOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
of severe disease associated with debility andmalnutrition.
There are reports in the literaturethat lend some support to such a
suggestion.Sunderman and Rose (21) studieda patient with
an inadequate dietary intakewho had a subnormalconcentrationof
total base in the serum. Gollan(22) reported that the average
concentrationofsodium in the sera of marasmic Italian childrenwa s
lower than normal. This must be interpretedwith some caution, as
these infants had a historyof diarrhealdisease.
The fact that this syndrome has none of thesymptoms of true
sodium depletionis most im-portant. In th e development of the
usual typesof salt depletionthere is a negativewater balancewith a
consequent contractionof the volume ofbody water as well as a
reductionin it s tonicity.It is probable that the contractionof the
plasmavolume which sharesin the decreaseof the extra-cellular water
and the dilution of th e cellular con-tents as a result of th e
hypotonicityof the extra-cellular water both contributeto the
physiologicabnormalitiesnoted in salt depletion. These
ab-normalitiesare characterizedby a persistenthypo-tension,
asthenia, disorderedrenal hemodynamics(as manifested by a depressed
rate of glomerularfiltration and urea clearance)and by nitrogen
re-tention; and, finally, peripheralvascularcollapse.Th e data from
the present investigationsdo notsuggest such a state. Although
endogenous cre-atinine clearancesmay have been somewhat re-duced ,
theywere no lower when the concentra-tion of the sodium in the
serum wa s depressed.There wa s no nitrogen retention, and
peripheralvascularcollapsedeveloped only when there hadbeen
extrarenalloss of salt and water leadingtothe development of true
salt depletion. These pa-tients do not appear to be suffering from
a con-
traction of the volume of the extracellular fluidand plasma.A
hypothesisis offered to explain the mecha-
nism of this syndrome which is admittedly specu-lative and
unproven. It is that the primary de-fect in this abnormality is a
chronic reduction ofcellular osmolarity. The overall effects of
this al-terationwould be an abnormal excretion of sodiumin an
effort to reduce the tonic ity ofthe extracel-lular f luids in
conformity with the primarily re-duced tonicity of the
intracellular fluids, but with
the maintenance of normal volumes of body wa-ter. Although there
is as yet no primary and in-dependent evidence that such a state of
chronicallyaltered cellular osmolaritydoes occur, acute al-
terationsin cellularosmolarityhave been observed.This phenomenon
has been suggested by severalgroups to explain certain resul ts
intheir investiga-tions (23-27).
The sequence of events that might followsucha primary decrease
in cellular tonicity is as fol-lows: the first event is a movement
of water fromthe cells to the extracellularspace in the interestsof
osmotic uniformity. At this point al l the bodyfluids are
relativelyhypertonicand th e intracellularvolume is contracted. The
hypertonicityand cel-lular dehydration provoke thirst and
stimulateanincreasedsecretionof th e posterior
pituitaryanti-diuretic hormone. More water is ingested andthere is
an increasein the reabsorptionof waterin the distal renal tubule.
This tends to expandthe body fluids, but reduces the tonicity of
thesefluids toward the "new" normal level. The cellu-lar
dehydration,the hypertonicityof the bodyfluids and the expanded
extracellular volumemay all be stimuli for t hedecreased
reabsorptionof sodium in the renal tubules, thus increasingthe
excretionof th is ion. As sodium is excreted,water followsuntil the
"new" level of tonicity andoriginal volumes of th e body fluids are
achieved.
This mechanism providesfo r the maintenanceof the volume of
extracellular fluid and plasma,and , hence,avoids the
undesirableeffects of theusual type of salt depletion. With this
mecha-nism in mind, it is clear why the calculationof
theanticipatedrise in concentrationof sodium in theextracellular
water agrees so closely with the ob-served when there is a net
positive balance ofsodium and the calctilation is made with the
prem-
ise that there is no change in total body water.Although this
hypothesis seems plausible andis not at variance with the observed
data, it isadmittedly unproven an d awaits a critical test.
The differentiationof this syndrome from Ad-dison's disease is
an important clinical problem.The tw o procedures that seem to
offer the mosthelp in this regard are the demonstration of
aneosinopeniafollowingadministration of epineph-rine and the
excretion of an almost sodium-freeurine on a regime of minimal salt
intake. The
1555
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
12/13
E. A. H. SIMS. LOUIS G. WELT, JACK ORLOFF, AND JAMES W.
NEEDHAM
latter procedure is hazardous, but the risk can beminimized by
careful and frequent clinical andchemical observations.
SUMMARY AND CONCLUSIONS
Tenlpatients with hyponatremia and pulmonarytuberculosiswere
studied. Nine had far-advancedpulmonary tuberculosisand one miliary
tubercu-losis with minimal pulmiionaryinvolvement. Nofrank evidence
of renal or adrenal insufficiencywa s found. Al l showed advanced
malnutrition,hypotension,and hypoalbuminem-iia.Abnormalretentioni
of carbon dioxide wa s found in onlyone patient. When given free
accessto salt, theywere found to excrete40-90 miiEq.of sodium
perday in spite of concenitrationsin the serum rang-in g from 122
to 131 mnEq./L.Five patients ex-creted as little as 5-29 mEq. of
sodium per daywhen the dietarysalt wa s severelyrestricted.
Theexcretionof sodiumn,however, did not reach thelow values usually
associatedwith hyponatremiadue to depletionof salt in other
conditions. Thesepatients did not p)resentth e clinical signs
orsymptoms or other evidence of sodium depletion.There was no
evidentdehydration,peripheralcir-culatory failure, or hyperkalemia.
Renal clear-ances of creatinine, mannitol, or urea were essen-
tially normal and were not lower when measuredin the
hyponatremic as opposed to the normalstate. Five patients retained
41%oto 98% of alarge amount of salt given in a 24-hour
period.Calculationsfrom data obtained during acute bal-ance
periodsfollowingthese infusions supportedthe hypothesisthat these
patients did not have acontractedbody water. The concentrationof
so-dium in the serum remained in the subnormal orlow normal range
despite high daily intakes ofsalt. This syndrome was reversedin two
patients
associatedwith clinical improvement. There wa smore lability in
the con-centrationof sodium inth e serum with varying intakesof
salt than is usu-ally observed in normal subjects. The
concentra-tions varied during relatively short periods overa range
of 2 to 12 mnEq./L.
In three patients procedure I of the Robinson-Kepler-Power water
test w-as positive. In onlyone was the secondIpart also positive.
Six patientshad an essentially niormiialeosinopenicresponse
toepinelhrine.
Four patients retained increasedquantities ofsodium when given
desoxycorticosterone.Therewa s no definite response to smalldoses
of adrenalcortical extract. The adrenal glands were normal
in the six patients whocame to
autopsy.It is suggested that a primary reduction in cel-lular
osmolaritymay be th e initiating factor in thedevelopment of this
syndrome. The increasedex-cretion of sodium at subnormal
concentrationsofthis ion in the serum miightrepresentan attemptto
reduce extracellular tonicity to conform witha reduced cellular
osmolarity.
An eosinopenicresponse to epinephrine and theability to reduce
th e excretionof sodium on aregimefree of salt aids in
differentiating thissyndrome from Addison'sdisease.
ACKNOWLEDGM ENTS
We are grateful to Miss Alice Cattanaclhand the staffof th e
Diet Department fo r making possiblethe diets lowin salt used in
this study and to Miss Patricia Robinson,R.N., fo r her
invaluablecooperation. The authors areindebted to Dr. John P.
Peters for his guidance an(dcriticism throughout the course of this
study.
BIBLIOGRAPHY
1. McCance, R. A., Medical problems in mineral metab-olism.
Lancet,1936,1; 643, 704,765, and 823.
2. Gamble, J. L., Ross, S. G., and Tisdall, F. F. ,
Themetabolism of fixed base during fasting. J. Biol.Chem., 1923,
57, 633.
3. Black, D. A. K., Th e renal excretion of water andsalt. Irish
J. M. Sc., 1949,715.
4. Winkler, A. W., and Crankshaw, 0. F. , Chloridede-pletion in
conditionsother than Addison's disease.J. Clin. Invest., 1938,17,
1.
5. Thorn, G. W., Howard, R. P., and Dayman, H., Elec-trolyte
changes in pulmonary tuberculosis, withspecial referenceto
adrenalcortical function. Bull.Johns Hopkins Hosp.,1940,67,
345.
6. Westwater, J. O., Stiven, D., and Garry, R. C. , A
note on th e serumsodium level in
patientssuffering
from tuberculosis. Clin. Sci., 1939,4, 73.7. Kolmer, H. S. ,
Ellis, D., Smith,T., Collins, P., and
Greisheimer, E. M. , Acid-base conditionin tuber-culosis. Am.
Rev. Tuberc., 1948,57, 400.
8. Robinson, F. J. , Power, M. H., and Kepler, E. J.,Two new
proceduresto assist in th e recognitionand exclusion of
Addison'sdisease; preliminaryreport. Proc. Staff Meet., Mayo
Clinic, 1941,16,577.
9. Recant, L., Forsham, P. H., and Thorn, G. W., Theeffect of
epinephrineon circulating eosinophils.Federation Proc., 1948,7,
99.
1556
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/
-
7/27/2019 asimp Na 1950
13/13
1557SYM I'TOMATIC HYPONATREMIA IN PULMONARY TUBERCULOSIS
10. Thorn, G. W., Bayles, T. B., Massell,B. F., Forsham,P. H. ,
Hill, S. R. , Jr., Smith, S., III, and Warren,J. E., Studies on the
relation of pituitary-adrenalfunction to rheumatic disease. New
England J.Med., 1949, 241, 529.
11. Milne, J. , Serum protein fractionation: a comparisonof
sodium sulfate precipitationand electrophoresis.J. Biol. Chem.,
1947, 169, 595.
12. Peters, J. P., and Van Slyke, D. D., QuantitativeClinical
Chemistry. Vol. II. Methods. Williams& Wilkins, Baltimore,
1932.
13. Elkinton, J. R. , The volume of distribution of man-nitol as
a measure of the volume of extracellularfluid, with a study of the
mannitol method. J.Clin. Invest., 1947,26 , 1088.
14. Peters, J. H. , The determination of creatinine andcreatine
in blood and urine with the photoelectriccolorimeter. J. Biol.
Chem., 1942, 146, 179.
15. Cahen, R. L., and Salter, W. T., Urinary 17-keto-steroids in
metabolism; standardized chemical esti-mation. J. Biol. Chem.,
1944, 152, 489.
16. Holtorff, A. F., and Koch, F. C., The colorimetricestimation
of 17-ketosteroidsand their applicationto urine extracts. J. Biol.
Chem., 1940,135, 377.
17. Randolph, T. G., Blood studies in allergy. I. The di-rect
counting chamber determination of eosinophilsby propylene glycol
aqueous stains. J. Allergy,1944,15, 89.
18. Needham, J. W., The metabolism of potassium indiabetic
acidosis. Yale J. Biol. & Med., 1949,22 ,39.
19. Elkinton,J. R., Danowski, T. S., and Winkler, A.
W.,Hemodynamic changes in salt depletionand in de-hydration. J.
Clin. Invest., 1946,25, 120.
20. Elkinton, J. R., and Winkler, A. W., Transfers of
in-tracellular potassium in experimental dehydration.J. Clin.
Invest., 1944, 23, 93.
21. Sunderman, F. W., and Rose, E., Studies in
serumelectrolytes. XVI. Changes in th e serum and bodyfluids in
anorexia nervosa. J. Clin. Endocrinol.,1948,8, 209.
22. Gollan, F., Blood and extracellular fluid studies inchronic
malnutrition in infancy. J. Clin. Invest.,1948,27, 352.
23. Yannet, H., and Darrow, D. C., The effects of de-pletion of
extracellular electrolytes on the chemi-cal composition of skeletal
muscle, liver, and car-diac muscle. J. Biol. Chem., 1940, 134,
721.
24. Elkinton, J. R., Winkler, A. W., and Danowski, T.
S.,Inactivecell base and th e measurement of changes
in cell water. Yale J. Biol. & Med., 1944, 17,383.
25. Seldin, D. W., and Tarail, R., Effect of hypertonicsolutions
on metabolism and excretionof e lect ro -lytes. Am. J. Physiol.,
1949, 159, 160.
26. Gaudino, M., and Levitt, M. F., Influence of
theadrenalcortex on body water distributionand renalfunction. J.
Clin. Invest., 1949,28, 1487.
27. Welt, L. G., Orloff, J. , Kydd, D. M., and Oltman ,J. E., An
example of cellular hyperosmolarity.J. Clin. Invest., 1950,29,
935.
Downloaded on September 28, 2013. The Journal of Clinical
Investigation. More information at
www.jci.org/articles/view/102396
http://www.jci.org/http://dx.doi.org/10.1172/JCI102396http://dx.doi.org/10.1172/JCI102396http://www.jci.org/