Embed Size (px)
Citation preview

1
Asia Pacific Forum “Integrated Meets Value-Based Care: Aligning Stakeholders’ Incentives”
Session 127, 13h February 2019
Dr Jason Cheah Group Deputy CEO (Transformation), National Healthcare Group
CEO, Woodlands Health Campus

2
• Ministry of Health, Singapore (www.moh.gov.sg)
• Agency for Integrated care, Singapore (www.aic.sg)
Acknowledgements
3
• Integrated care
• Value-based care
• How could integrated care contribute towards high value care?
• Enablers
• Real world examples
• Q&A
Agenda

4
• Ref : Kings Fund Reports (www.kingsfund.org.uk)
• Ref : IFIC (www.integratedcarefoundation.org)
Integrated care
5
6
7
8

9
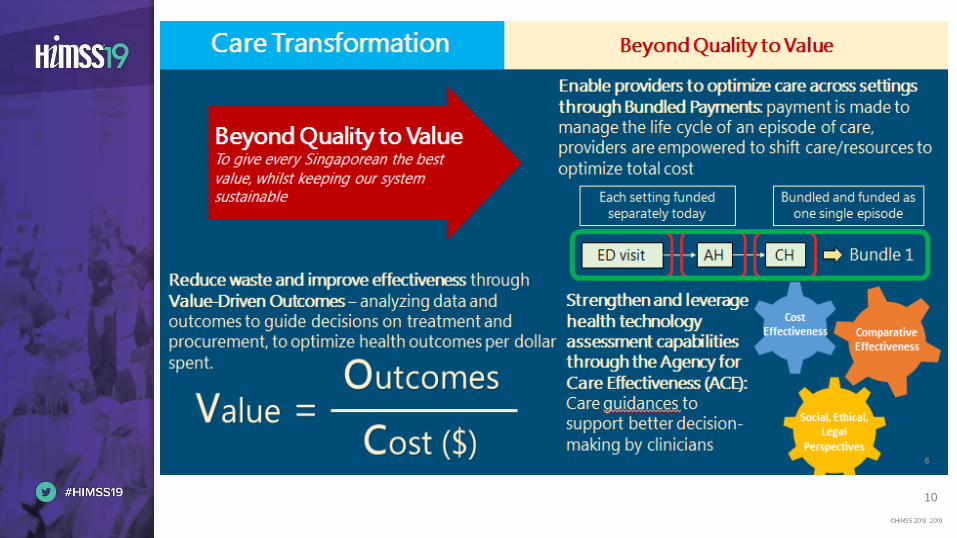
Beyond Quality to ValueTo give every Singaporean the best value, whilst keeping our system sustainable
Beyond Healthcare to
HealthTo help and support Singaporeans to live healthier lives
Beyond Hospital to CommunitySo Singaporeans can receive care in the community and nearer to home
Care Transformation
Changing the essence of what we
do.
10
Bundled and funded as one single
episode
11
12
13
14
15

16
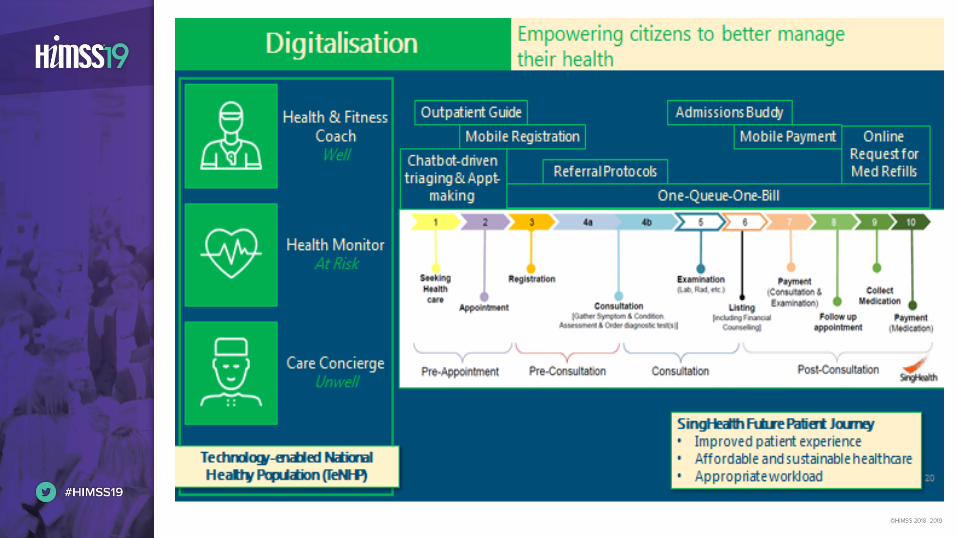
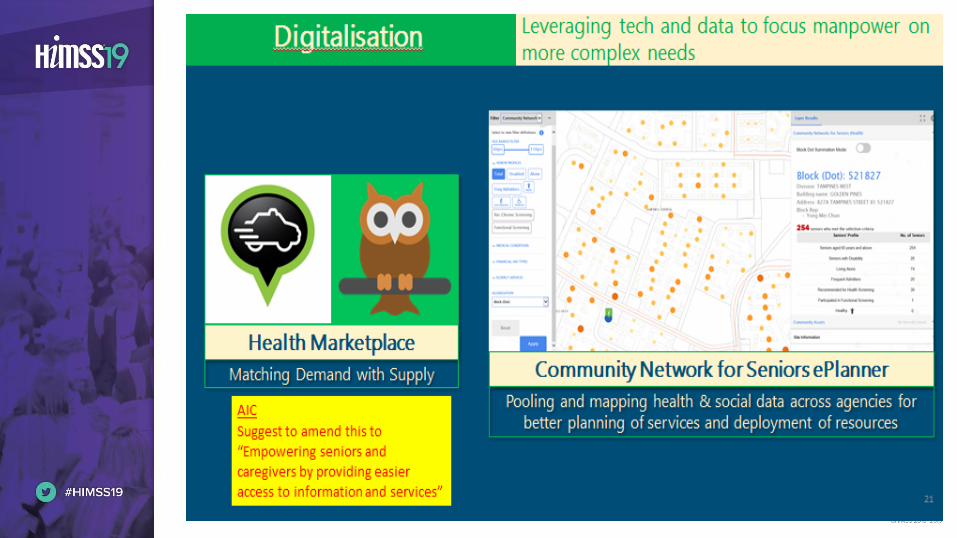
Digitalization Leveraging tech and data to focus
manpower on more complex needs
Matching Demand with Supply
Health Marketplace
Pooling and mapping health & social data across agencies for
better planning of services and deployment of resourcesAIC
Suggest to amend this to
“Empowering seniors and
caregivers by providing easier
access to information and
services”

Integrated Meets Value-Based Care:
Aligning Stakeholders’ Incentives
Kenneth KwekCEO, Singapore General Hospital
DGCEO (OT and I), SingHealth
SingHealth
• Largest healthcare cluster in Singapore• Provide care to over 50% of Singapore’s population• Spans entire continuum of healthcare from primary to tertiary care to intermediate
long term care
• 4 hospitals• 8 primary care polyclinics• 5 national specialty centers• 3 community hospitals
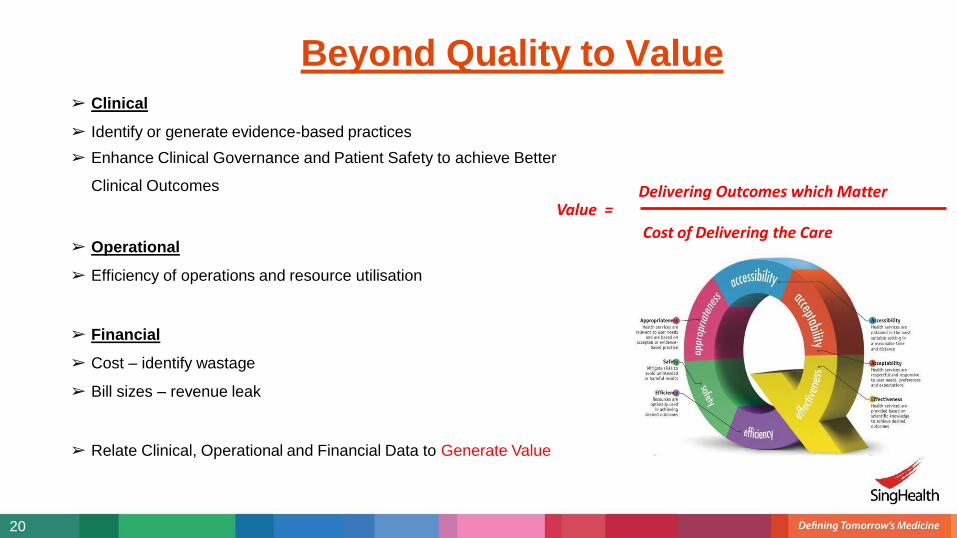
➢ Clinical
➢ Identify or generate evidence-based practices
➢ Enhance Clinical Governance and Patient Safety to achieve Better
Clinical Outcomes
➢ Operational
➢ Efficiency of operations and resource utilisation
➢ Financial
➢ Cost – identify wastage
➢ Bill sizes – revenue leak
➢ Relate Clinical, Operational and Financial Data to Generate Value
Beyond Quality to Value
Delivering Outcomes which Matter
Cost of Delivering the Care
Value =
20
Bundled Care to Deliver Value
21
• Essential to first define what is the “ideal” care– elements of care with evidence to provide the best outcomes and safest care
• Track adherence to this “ideal” care pathway and variance– measures to reduce unwarranted variability
• Assess impact on clinical outcomes
• Assess operational and financial impact of the pathway
• Critical to align stakeholders interests….staff, patients, population, regulators
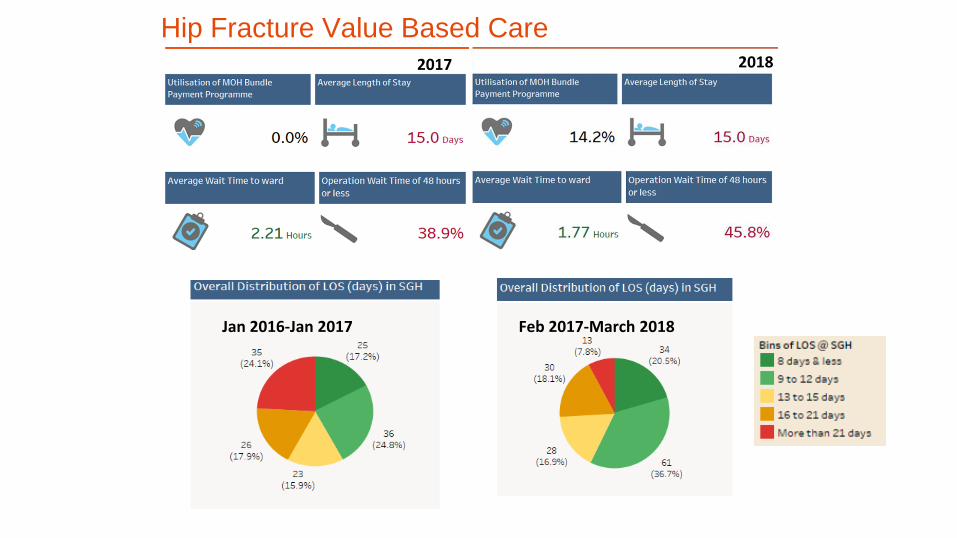
Feb 2017-March 2018Jan 2016-Jan 2017
Hip Fracture Value Based CareJan 2016-Jan 2017 Feb 2017-March 2018
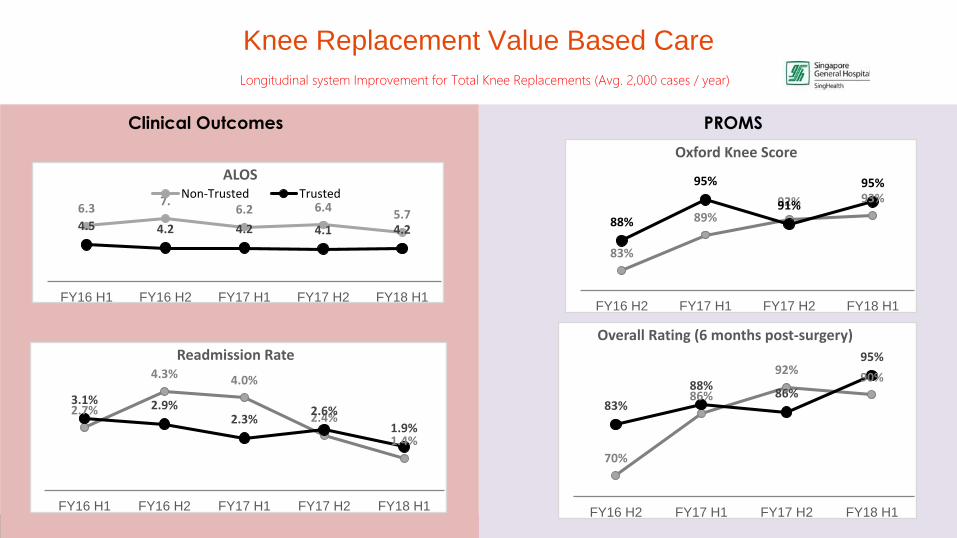
Clinical Outcomes PROMS
Longitudinal system Improvement for Total Knee Replacements (Avg. 2,000 cases / year)
6.37.
6.2 6.45.7
4.5 4.2 4.2 4.1 4.2
FY16 H1 FY16 H2 FY17 H1 FY17 H2 FY18 H1
ALOSNon-Trusted Trusted
2.7%
4.3% 4.0%
2.4%
1.4%
3.1% 2.9%2.3%
2.6%
1.9%
FY16 H1 FY16 H2 FY17 H1 FY17 H2 FY18 H1
Readmission Rate
70%
86%
92%90%
83%
88%86%
95%
FY16 H2 FY17 H1 FY17 H2 FY18 H1
Overall Rating (6 months post-surgery)
83%
89%92% 93%
88%
95%
91%
95%
FY16 H2 FY17 H1 FY17 H2 FY18 H1
Oxford Knee Score
Knee Replacement Value Based Care
8
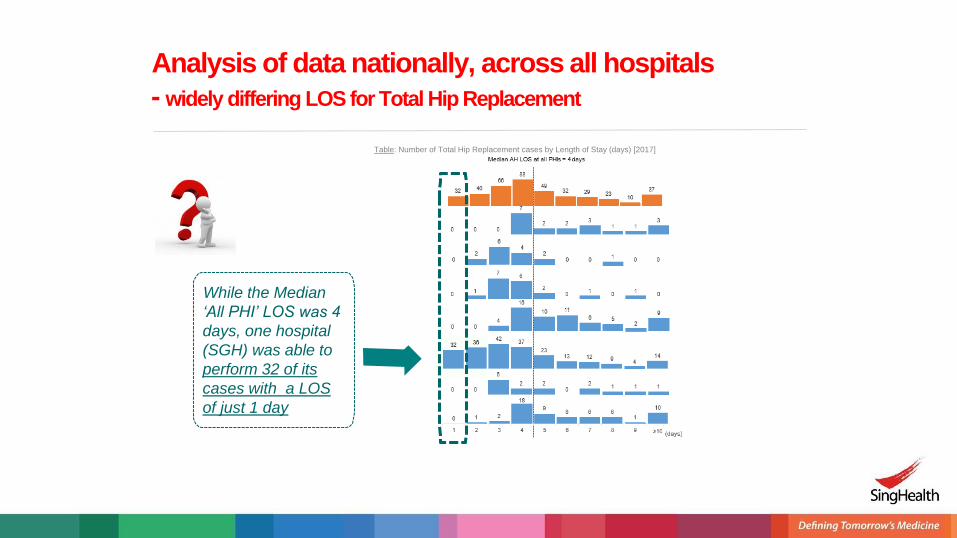
Analysis of data nationally, across all hospitals
- widely differing LOS for Total Hip Replacement
While the Median
‘All PHI’ LOS was 4
days, one hospital
(SGH) was able to
perform 32 of its
cases with a LOS
of just 1 day
Table: Number of Total Hip Replacement cases by Length of Stay (days) [2017]
9
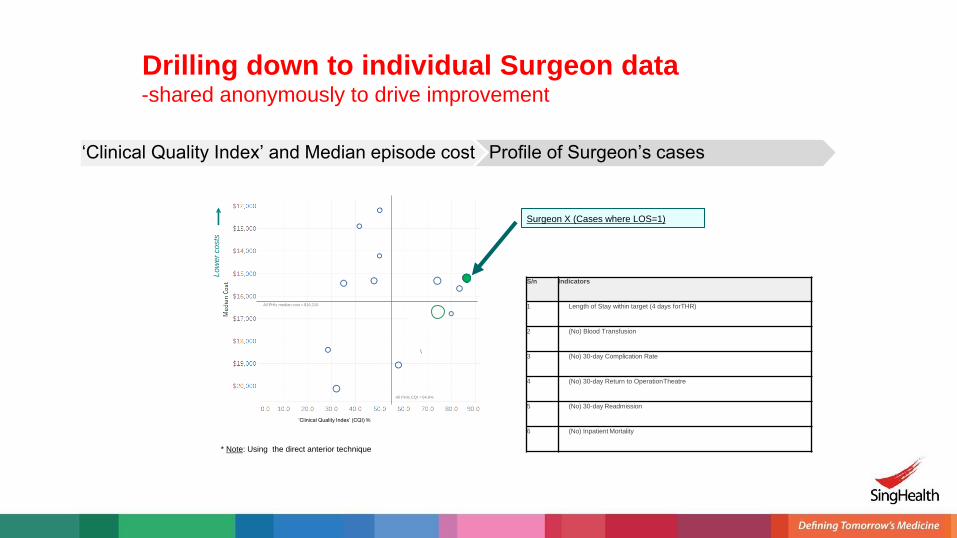
All PHIs median cost = $16,210
All PHIs CQI = 54.6%
Lo
we
rco
sts
Drilling down to individual Surgeon data-shared anonymously to drive improvement
S/n Indicators
1 Length of Stay within target (4 days forTHR)
2 (No) Blood Transfusion
3 (No) 30-day Complication Rate
4 (No) 30-day Return to OperationTheatre
5 (No) 30-day Readmission
6 (No) Inpatient Mortality
‘Clinical Quality Index’ (CQI) %
* Note: Using the direct anterior technique
‘Clinical Quality Index’ and Median episode cost Profile of Surgeon’s cases
Surgeon X (Cases where LOS=1)
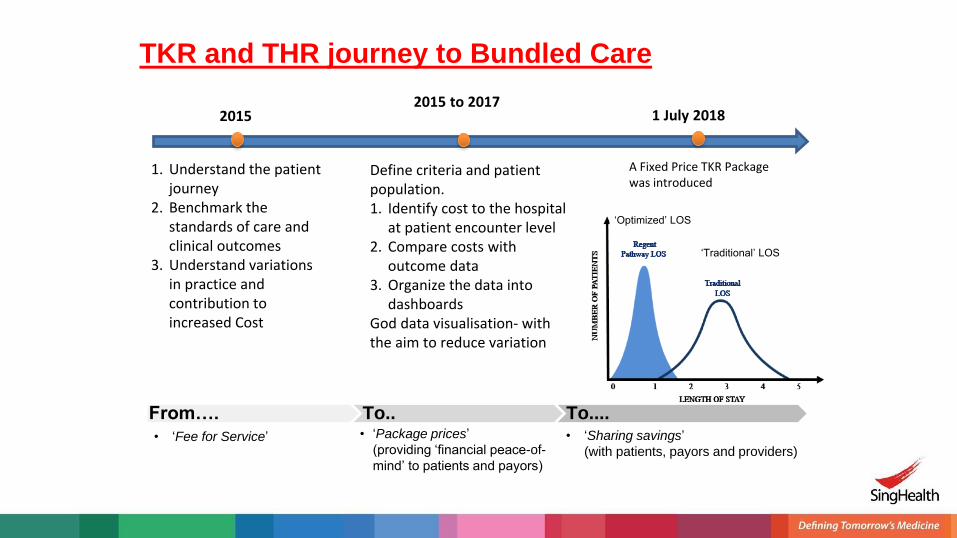
TKR and THR journey to Bundled Care
1. Understand the patient journey
2. Benchmark the standards of care and clinical outcomes
3. Understand variations in practice and contribution to increased Cost
20152015 to 2017
1 July 2018
Define criteria and patient population. 1. Identify cost to the hospital
at patient encounter level2. Compare costs with
outcome data3. Organize the data into
dashboardsGod data visualisation- with the aim to reduce variation
A Fixed Price TKR Package was introduced
• ‘Package prices’
(providing ‘financial peace-of-
mind’ to patients and payors)
• ‘Sharing savings’
(with patients, payors and providers)
From…. To.. To....• ‘Fee for Service’
‘Optimized’ LOS
‘Traditional’ LOS
6 days
Discharge fromSGH Campus
Day 1
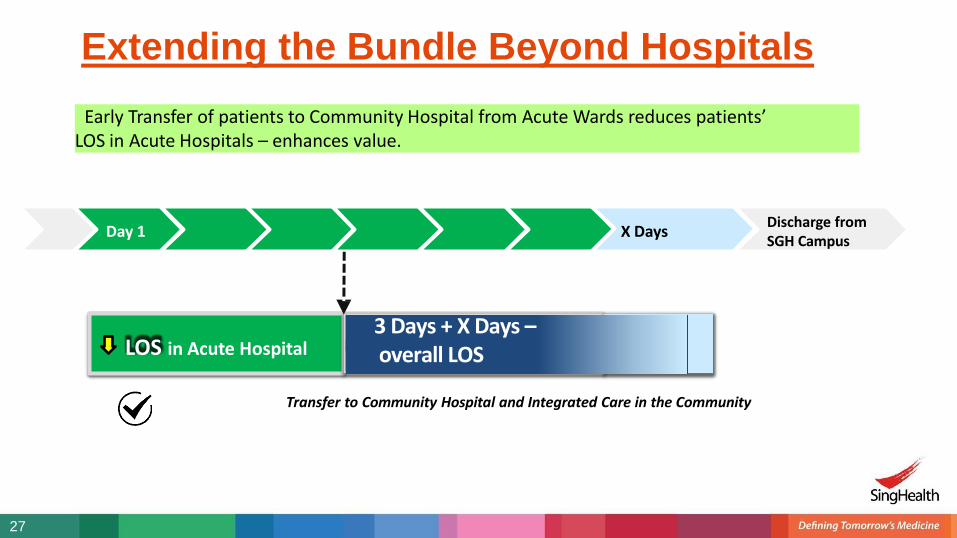
Extending the Bundle Beyond Hospitals
Early Transfer of patients to Community Hospital from Acute Wards reduces patients’LOS in Acute Hospitals – enhances value.
LOS in Acute Hospital
Transfer to Community Hospital and Integrated Care in the Community
X Days
27
3 Days + X Days –overall LOS
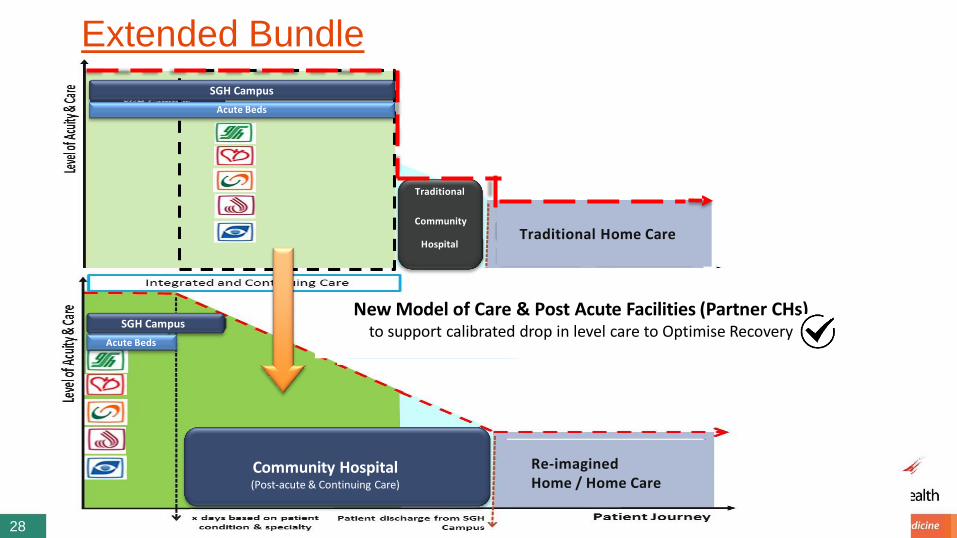
Extended Bundle
Traditional
Community
Hospital
Re-imaginedHome / Home Care
SGH Campus
Acute Beds
Community Hospital(Post-acute & Continuing Care)
SGH Campus
Acute Beds
New Model of Care & Post Acute Facilities (Partner CHs)to support calibrated drop in level care to Optimise Recovery
28
Traditional Home Care
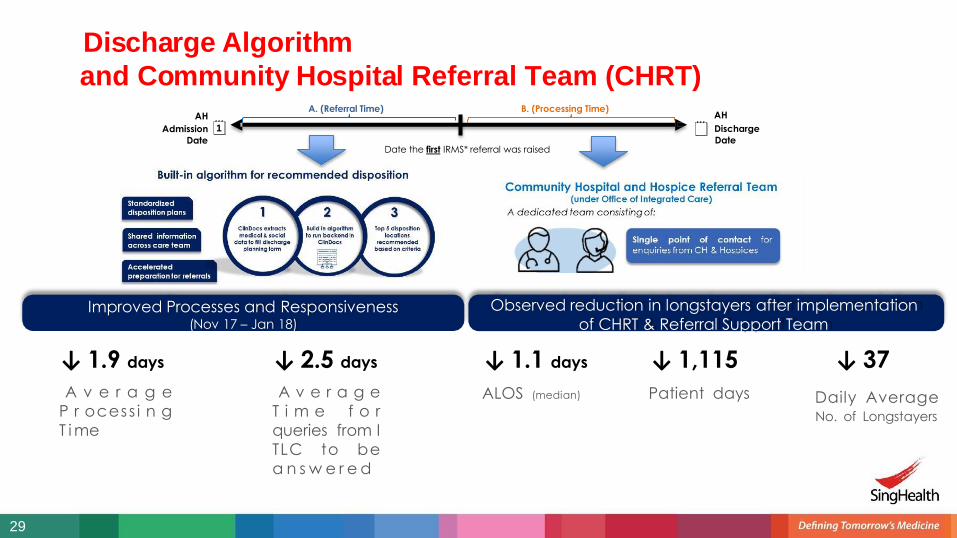
AH
Admission Date
Date the first IRMS* referral was raised
AH
Discharge
Date
A. (Referral Time) B. (Processing Time)
Discharge Algorithm
and Community Hospital Referral Team (CHRT)
↓ 1.1 days
ALOS (median)
↓ 1,115
Patient days
↓ 37
Daily Average No. of Longstayers
Observed reduction in longstayers after implementation
of CHRT & Referral Support TeamImproved Processes and Responsiveness
(Nov 17 – Jan 18)
29
↓ 1.9 days
A v e r a g e
P r ocess i n g
T i me
↓ 2.5 days
A v e r a g e
T i m e f o r
queries from I
TLC to be
a n s w e r e d
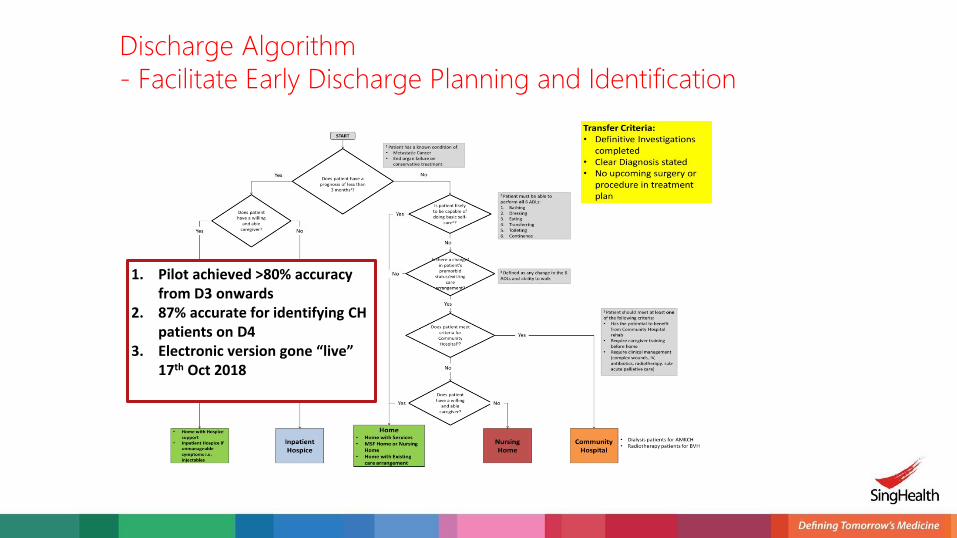
Discharge Algorithm
- Facilitate Early Discharge Planning and Identification
1. Pilot achieved >80% accuracy from D3 onwards
2. 87% accurate for identifying CH patients on D4
3. Electronic version gone “live” 17th Oct 2018
+
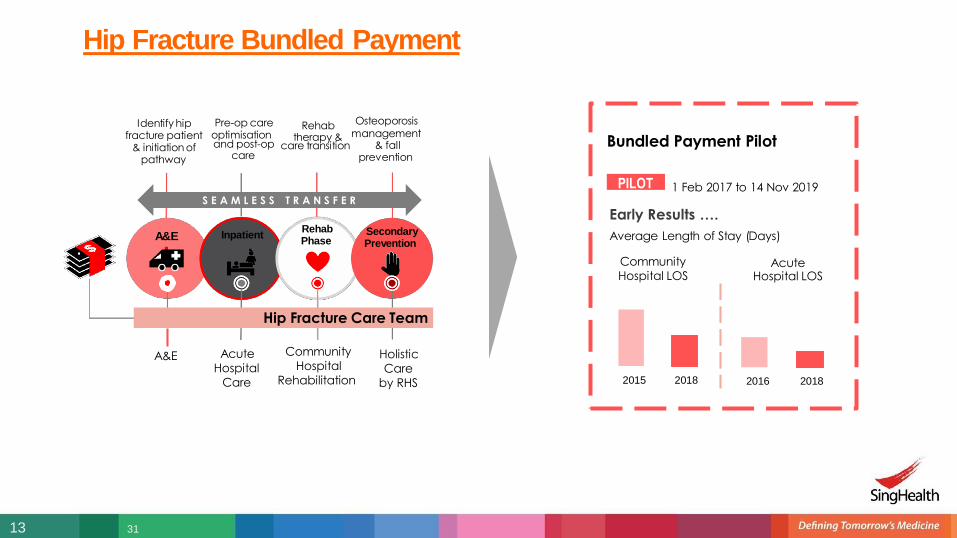
A&E InpatientRehabPhase
SecondaryPrevention
S E A M L E S S T R A N S F E R
Identify hip Pre-op carefracture patient optimisation
& initiation of pathway
and post-op care transition care
Rehabtherapy & management
Osteoporosis
& fall prevention
A&E
Bundled Payment Pilot
1 Feb 2017 to 14 Nov 2019
Early Results ….
Average Length of Stay (Days)
PILOT
Hip Fracture Bundled Payment
2015 2018 2016 2018
Hip Fracture Care Team
13 31
Acute
Hospital
Care
Community
Hospital
Rehabilitation
Holistic
Care
by RHS
Community
Hospital LOSAcute
Hospital LOS
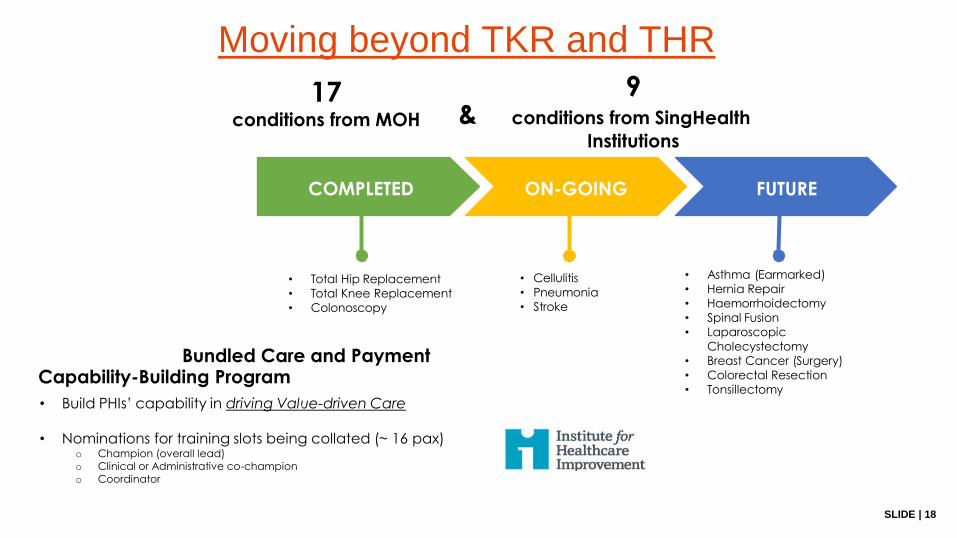
SLIDE | 18
17conditions from MOH
9& conditions from SingHealth
Institutions
FUTURE
• Total Hip Replacement
• Total Knee Replacement
• Colonoscopy
Bundled Care and Payment Capability-Building Program
• Build PHIs’ capability in driving Value-driven Care
• Nominations for training slots being collated (~ 16 pax)o Champion (overall lead)
o Clinical or Administrative co-champion
o Coordinator
COMPLETED ON-GOING
• Cellulitis
• Pneumonia
• Stroke
• Asthma (Earmarked)
• Hernia Repair
• Haemorrhoidectomy
• Spinal Fusion
• Laparoscopic
Cholecystectomy
• Breast Cancer (Surgery)
• Colorectal Resection
• Tonsillectomy
Moving beyond TKR and THR
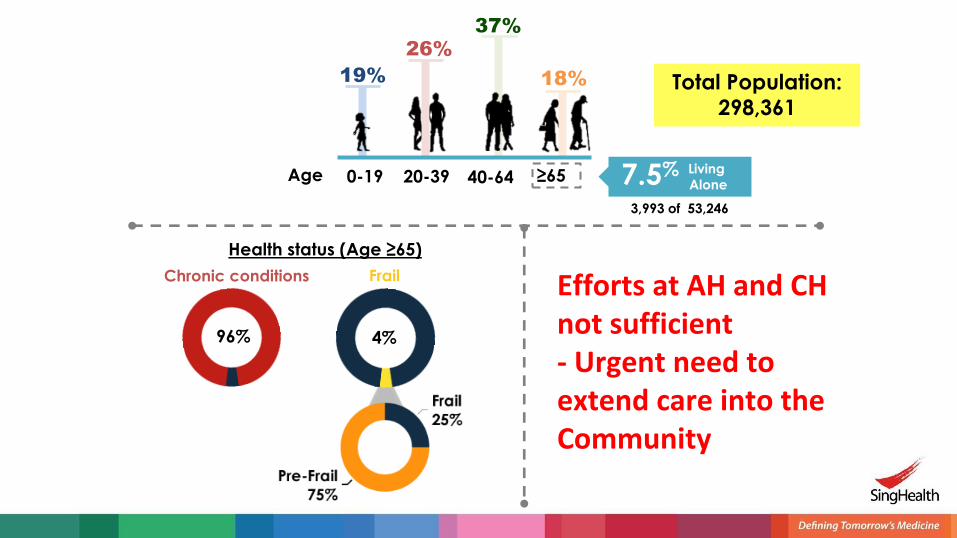
Health status (Age ≥65)
19%
0-19 20-39 40-64 ≥65
26%37%
18%
Age 7.5% Living
Alone
3,993 of 53,246
Total Population:
298,361
96% 4%
Chronic conditions Frail Efforts at AH and CH not sufficient - Urgent need to extend care into the Community
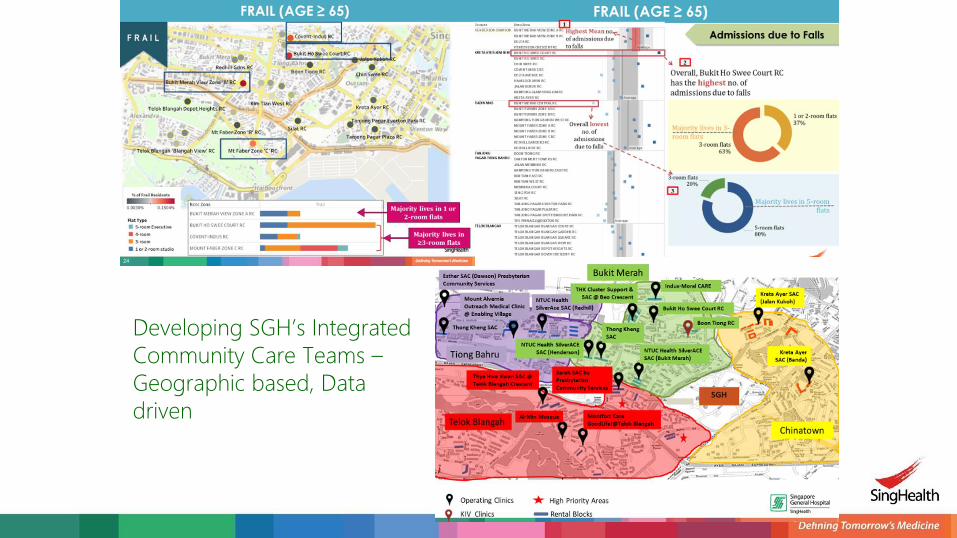
Developing SGH’s Integrated
Community Care Teams –
Geographic based, Data
driven
35
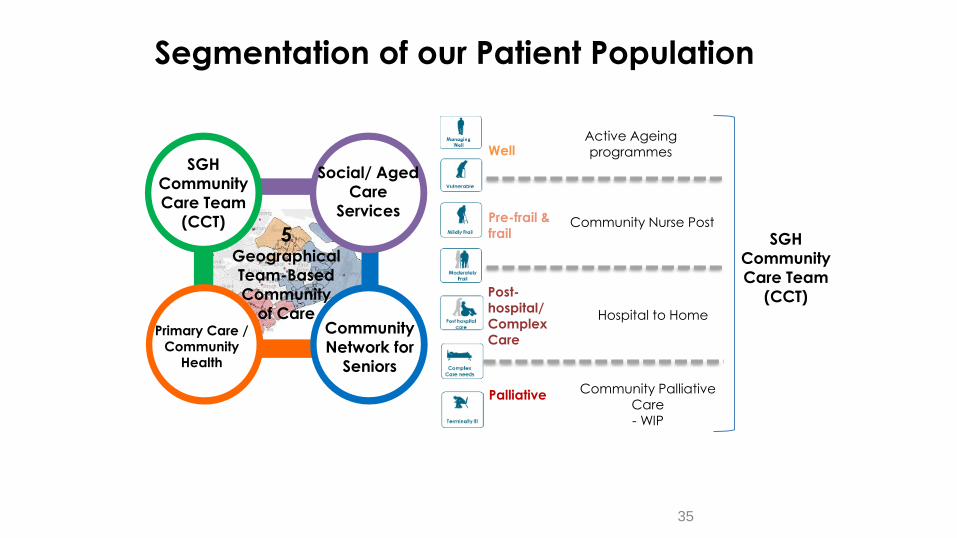
Segmentation of our Patient Population
5 Geographical
Team-Based
Community
of Care
SGH
Community
Care Team
(CCT)
Social/ Aged
Care
Services
Primary Care /
Community
Health
Community
Network for
Seniors
Well
Pre-frail &
frail
Post-
hospital/
Complex
Care
Palliative
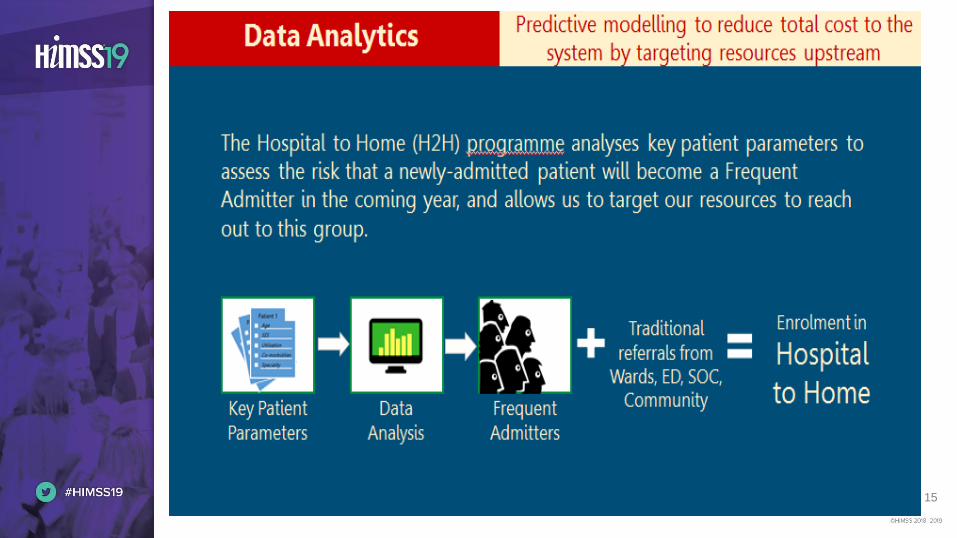
Hospital to Home
Community Nurse Post
Community Palliative
Care
- WIP
Active Ageing
programmes
SGH
Community
Care Team
(CCT)

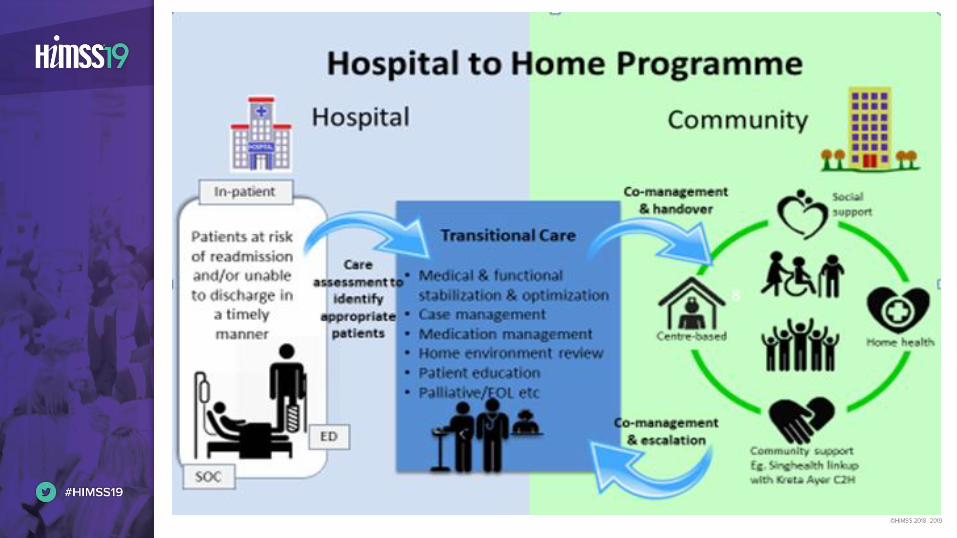
Transiting Complex Patients from
Hospital to Home
• Complex nursing / medical care & procedures
• Monitoring of chronic diseases & reinforcement of treatment compliance
• Medication management
• Patient & family education and empowerment
• Care coordination through the healthcare continuum
Hospital-to-Home (Transitional Care)
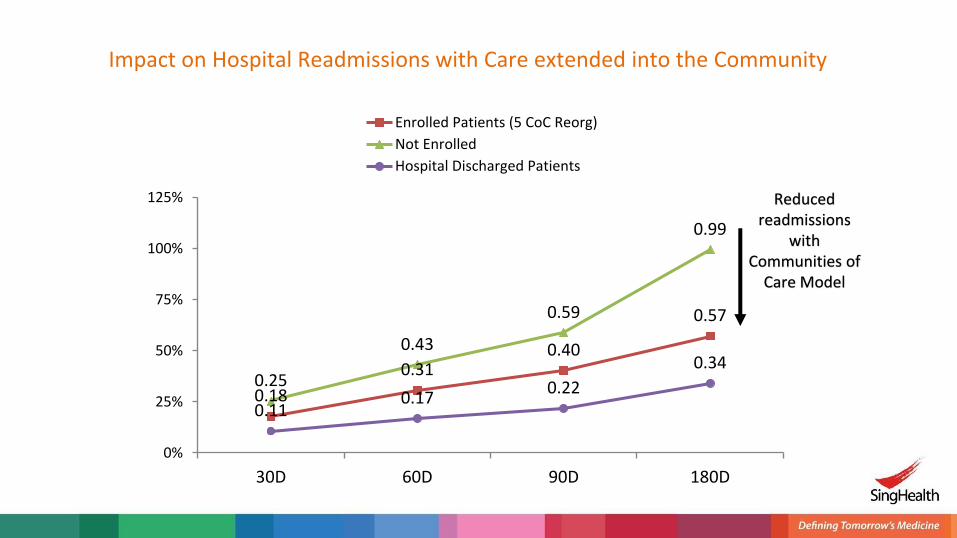
0.18
0.310.40
0.57
0.25
0.43
0.59
0.99
0.110.17
0.22
0.34
0%
25%
50%
75%
100%
125%
30D 60D 90D 180D
Enrolled Patients (5 CoC Reorg)
Not Enrolled
Hospital Discharged Patients
Reduced readmissions
with Communities of
Care Model
Impact on Hospital Readmissions with Care extended into the Community

Health & Geriatric
Assessment
Health Coaching for Disease Prevention
Chronic Disease
Monitoring & Self-care Education
Medication Support & Education
Care Referral
&
Coordination
SingHealth Community Nursing
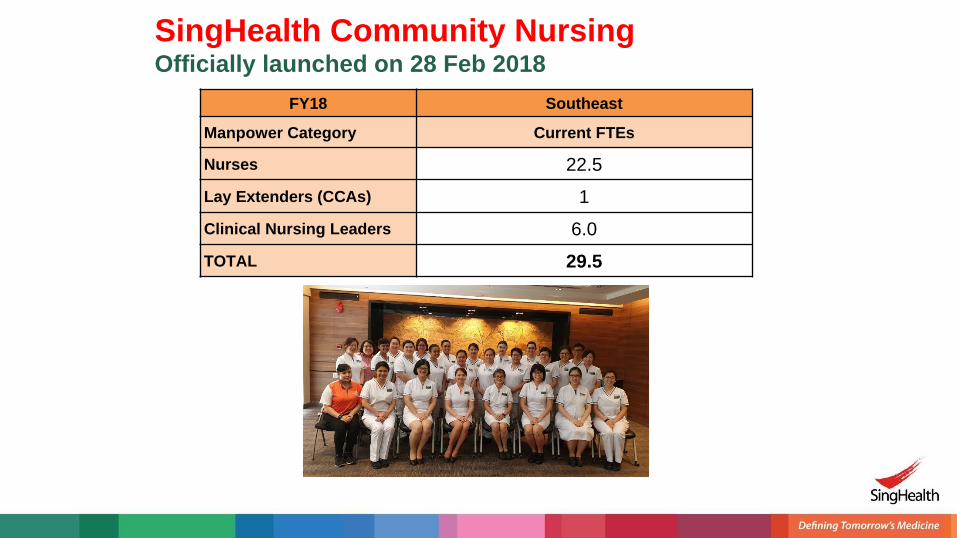
FY18 Southeast
Manpower Category Current FTEs
Nurses 22.5
Lay Extenders (CCAs) 1
Clinical Nursing Leaders 6.0
TOTAL 29.5
SingHealth Community NursingOfficially launched on 28 Feb 2018

SingHealth Community Nursing 22 Community Nurse Posts1. Kreta Ayer SAC @ Banda
2. Kreta Ayer SAC @ Jln Kukoh
3. NTUC Health SilverACE (Henderson)
4. NTUC Health SilverACE (Bukit Merah)
5. NTUC Health SilverACE (Redhill)
6. NTUC Health SilverAce SAC (Telok Blangah)
7. Montfort (Goodlife! @ Telok Blangah)
8. Montfort (Goodlife! @ 15 Marine Terrace)
9. Montfort (Goodlife! Makan) @ 52 Marine Terrace
10. THK SAC & Cluster Support @ Beo Crescent
11. THK SAC @ Cassia Crescent
12. THK SAC @ Telok Blangah Crescent
13. Masjid AI-Amin
14. Masjid Jamiyah Al Rabitah
15. Indus-Moral CARE
16. Bukit Ho Swee Court RC
17. Boon Tiong RC
18. Thong Kheng SAC @ 123 Bukit Merah View
19. Sarah SAC (PCS)
20. Esther SAC (PCS)
21. Mount Alvernia Outreach Medical Clinic @ Enabling Village
22. Sunlove SAC @ Depot Heights
Home / Home Care
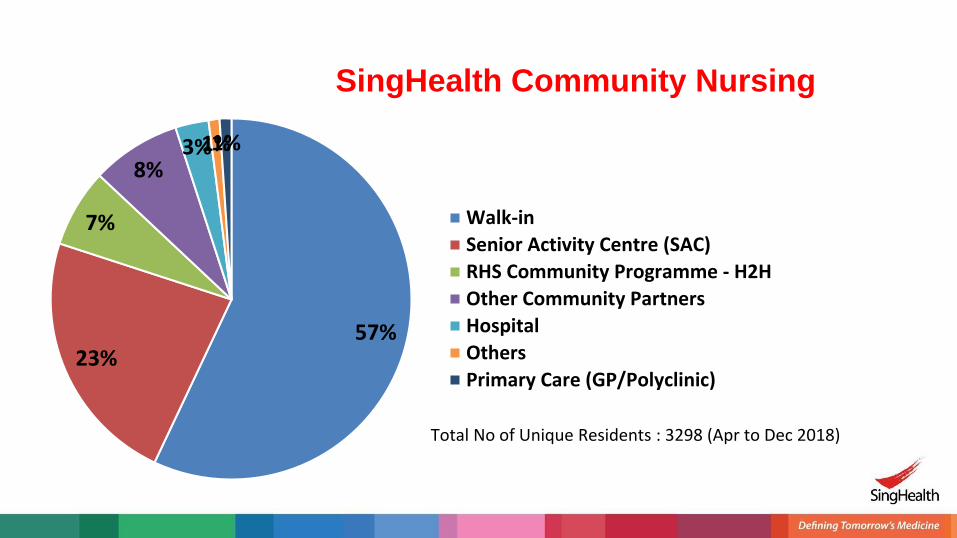
57%23%
7%
8%3%1%1%
Walk-in
Senior Activity Centre (SAC)
RHS Community Programme - H2H
Other Community Partners
Hospital
Others
Primary Care (GP/Polyclinic)
Total No of Unique Residents : 3298 (Apr to Dec 2018)
SingHealth Community Nursing
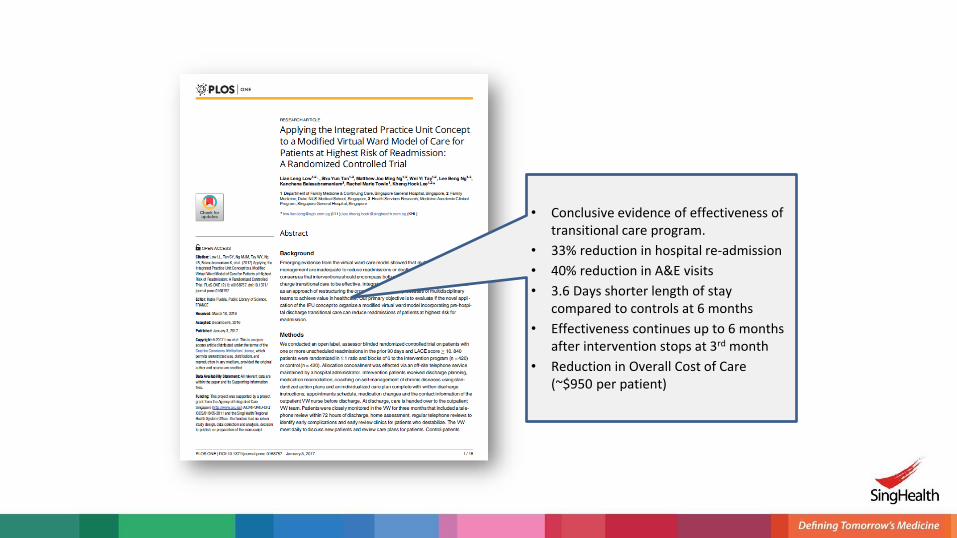
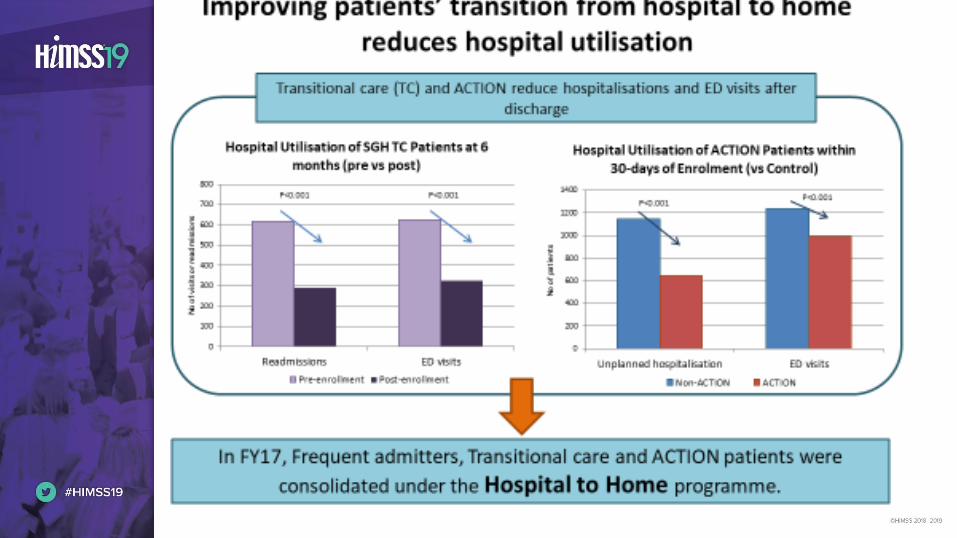
• Conclusive evidence of effectiveness of transitional care program.
• 33% reduction in hospital re-admission
• 40% reduction in A&E visits
• 3.6 Days shorter length of stay compared to controls at 6 months
• Effectiveness continues up to 6 months after intervention stops at 3rd month
• Reduction in Overall Cost of Care (~$950 per patient)

Community Engagement

Community Engagement
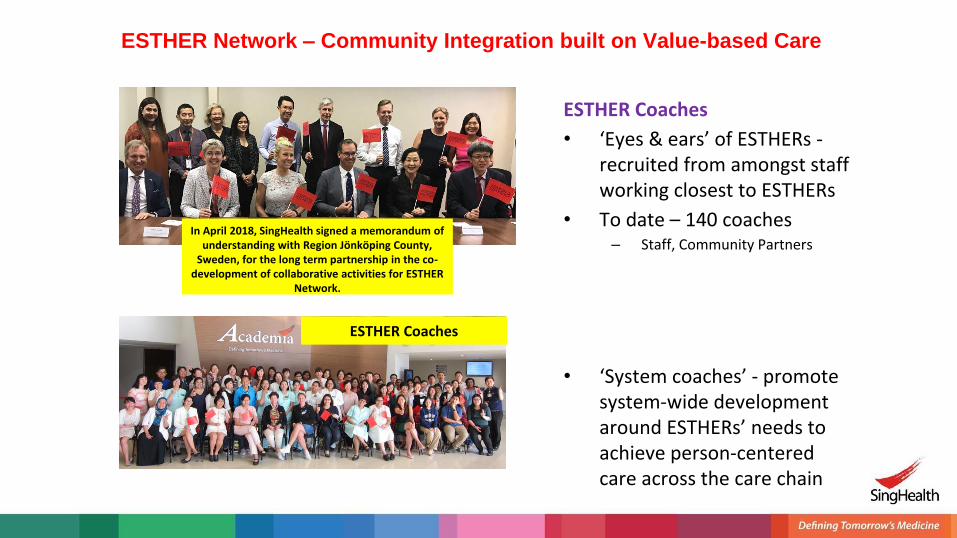
ESTHER Network – Community Integration built on Value-based Care
ESTHER Coaches
In April 2018, SingHealth signed a memorandum of understanding with Region Jönköping County,
Sweden, for the long term partnership in the co-development of collaborative activities for ESTHER
Network.
ESTHER Coaches
• ‘Eyes & ears’ of ESTHERs -recruited from amongst staff working closest to ESTHERs
• To date – 140 coaches– Staff, Community Partners
• ‘System coaches’ - promote system-wide development around ESTHERs’ needs to achieve person-centered care across the care chain
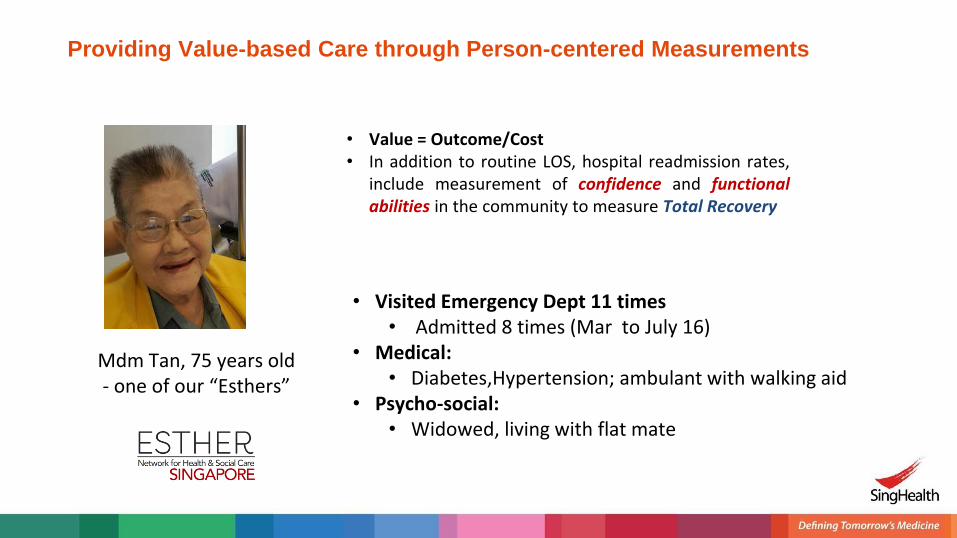
Providing Value-based Care through Person-centered Measurements
Mdm Tan, 75 years old - one of our “Esthers”
• Value = Outcome/Cost• In addition to routine LOS, hospital readmission rates,
include measurement of confidence and functionalabilities in the community to measure Total Recovery
• Visited Emergency Dept 11 times• Admitted 8 times (Mar to July 16)
• Medical:• Diabetes,Hypertension; ambulant with walking aid
• Psycho-social:• Widowed, living with flat mate
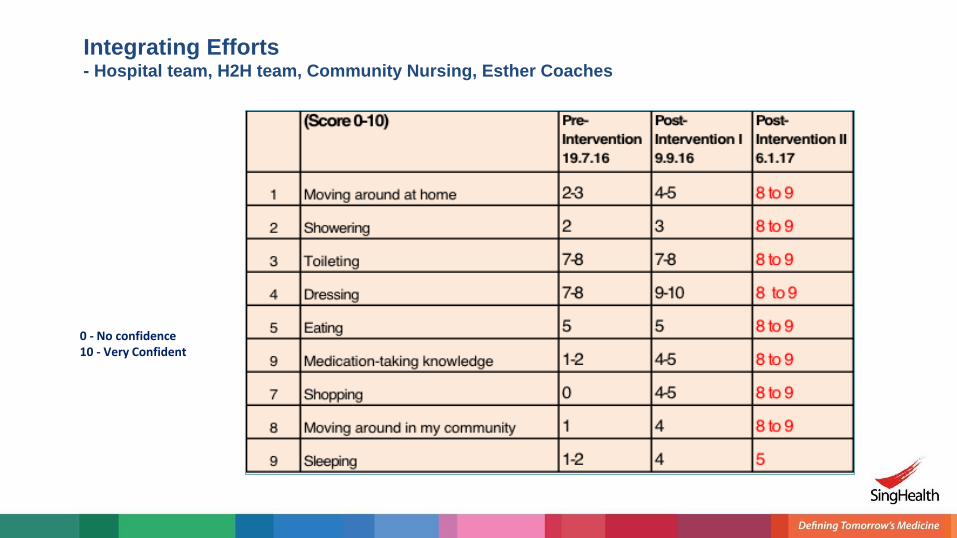
Integrating Efforts - Hospital team, H2H team, Community Nursing, Esther Coaches
0 - No confidence10 - Very Confident
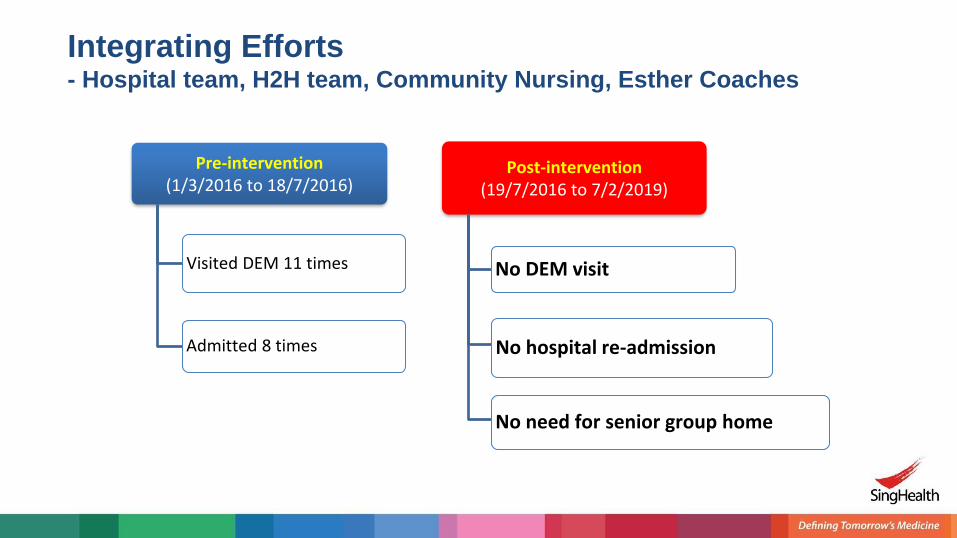
Pre-intervention(1/3/2016 to 18/7/2016)
Visited DEM 11 times
Admitted 8 times
Post-intervention(19/7/2016 to 7/2/2019)
No DEM visit
No hospital re-admission
No need for senior group home
Integrating Efforts - Hospital team, H2H team, Community Nursing, Esther Coaches
Thank You
49