Embed Size (px)
Citation preview
one vision one identity
one community
ASEAN Regional Guideline
for Minimum Requirementsfor Training and Accreditation
of Skilled Birth Attendants (SBA)

ASEAN REGIONAL GUIDLINE
for Minimum Requirementsfor Training and Accreditation
of Skilled Birth Attendants (SBA)
2
TABLE OF CONTENTS
Glossary of Terms. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Foreword. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .51. INTRODUCTION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7 1.1Definition.......................................................7 1.2PurposeoftheGuideline...........................................82. REQUIREMENT FOR CORE COMPETENCIES OF SBA IN ASEAN. . . . . . . . . . . . . . . . .93. STANDARDS FOR SBA TRAINING PROGRAMMES. . . . . . . . . . . . . . . . . . . . . . . . . . . 20 3.1Typesoftraining ................................................20 3.2Admissionrequirements.......................................... 20 3.3Standardsfortrainingprogrammes..................................204. REQUIREMENTS FOR TRAINING INSTITUTIONS. . . . . . . . . . . . . . . . . .. . . . . . . . . . . 22 4.1.TeachingStaff.................................................. 22 4.2Trainingprogrammeandmaterials.................................. 22 4.3.Requiredinfrastructureandequipment..............................22 4.4.Clinicalpracticesite.................................. ...........235. ASSESSMENT AND ACCREDITATION OF SBA. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .24 5.1CandidatestobeassessedtobeaccreditedasSBA.................... 24 5.2Accreditation...................................................24 5.3InstitutionseligibleforconductingSBAassessment.....................24 5.4.AccreditationofTrainingInstitutions................................256. RE-ACCREDITATION. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27Annex1:SBAAssessment(ProposedMethodologies)...........................28 Part1:Skillssuitabletobeassessedbycasemanagement.................28 Part2:Skillssuitabletobeassessedbyobservationofpracticeonsimulators..28Annex2:GuidanceforDevelopingCurriculaandCourseContentforShortSBA UpdatingTrainingProgramme.......................................29Annex2.1:MatrixforKnowledge,SkillsandAttitudeforeachASEANSBA Competency................................................... 30Annex3:StandardClassroomandSkillsLabRoom.............................43

3
Glossary of Terms
Accreditation Acertificationprocessdonebyathirdpartyandbestoweduponapersonwhohas demonstratedacertaindegreeofproficiencyrequiredofaprofessionorinstitutionthat hascompliedwiththestandardssetaccordingtothetypeofserviceitprovides.topublicly declarethehealthworkerhasdemonstratedtheyhavereachedtherequiredlevelof proficiency.TheobjectiveofAccreditationistopromoteandensurequality,bydeclaring apersonorinstitutionhasdemonstratedtheyhavereachedarequiredstandard.
Accredited Alicensed,certifiedorregisteredhealthprofessional(e.g.midwife,medicalphysician,Health nurseorother)whohasalegalrighttopractisehisorherprofessionaccordingtoProfessional countrycontext.
Accreditation TheorganizationthathasbeengiventheauthorityeitherbylaworbyappointmentbyBody arelevantgovernmentministrytoundertakeevaluationandregulatethepracticeofa professionbasedoncertainstandards
ASEAN ThelevelofcompetencerequiredofprofessionalstobeabletopracticetheirprofessioninCompetency theASEAN(AssociationofSouthEastAsianNations)region.
Competency Asetofknowledge,skills,attitudesandexperiencesrequiredofprofessionalstobeableto practiceproficiently(A+S+K+E=competence).
EmONC EmergencyObstetricandNeonatalCareincludeslifesavingformothersandnewbornsat birth.Hasbeendefinedastheabilitytoperformanagreedsetofsignalfunctions(9signal functionsforcomprehensiveEmONCand7forBasicEmONC)
JICA JapanInternationalCooperationAgency
MDG MillenniumDevelopmentGoals
Postnatal Aperiodoftimefromthecompletedeliveryofplacentaandmembranes,until6weeksafter birth,duringwhichtimethemajorreproductiveorgansreturntotheirpre-pregnantstage andlactationisestablished;isconsideredanimportanttimeperiodforthemother-baby relationshiptobeformed.Postnatalcareisthetermmostfrequentlyconsideredto becareofboththemotherandnewbornasoneunit(mother-babydyad).
Postpartum Theprocessthebodyundergoesfollowingchildbirth,wellalltheorgansreturntopre- pregnantstate.Thepostpartumperiodhasnospecifictimelineanditcouldtakeupto 6monthsforsomeorganssuchasurinarytracttorecoverafterpregnant.Theterm postpartumisgenerallyusedtorefertothewomenafterbirth.
Proficiency Theabilitytoperformtherequiredcorefunctionstotherequiredstandard.Tobeproficient, thehealthprovidermustpossessallthenecessarycompetenciesandhavepractisedthese repeatedlyandregularlyuntilheorsheisabletoperformtheskillcorrectlywithnoneedfor supervision.

4
SelfandFamily- Thisisintendedtoinclude:adviceongoodnutritionforpregnancyandhowtoachievethem:Care Adviceonironsupplementationtopreventanemia;working,physicalactivities,hygiene(sexual organs,breast,body);whatfactorscanbeharmfultothepregnantwomanandfoetus-suchas smoking,alcoholabuseandillicitdrug,toxicworkplace,etc.andhowbesttoavoidthem;danger signsandwheretoseekmedicalhelp
SkilledBirth ASkilledBirthAttendant(SBA)isdefinedasanaccreditedhealthprofessional-suchAttendant asmidwife,doctorornurse-whohasbeeneducatedandtrainedtoproficiencyintheskillsneeded tomanagenormal(uncomplicated)pregnancies,childbirthandimmediatepostnatalperiodandin theidentification,referralandmanagementofcomplicationsinwomenandnewborns
UNFPA UnitedNationsPopulationFund
WHO WorldHealthOrganization

5
Achievingthepeople-orientedandpeople-centredASEANCommunityby2015signifiesahealthycommunityofASEANpeopleswithquality,accessibleandaffordablehealthcareandservices.InlinewiththeASEANStrategicFrameworkonHealthDevelopment(2010-2015),ensuringahealthyASEANCommunityby2015involvesvariouspartnershipsandengagementswithrelevantstakeholdersfrombothhealthandnon-healthsectors.
Inherent in this aspiration for a healthy community are the sustained thrusts of ASEANMember Statesin improvingmaternal and child health.Seeking to accelerate and sustain the reduction inmaternal andneonatalmortalityandmorbidityinASEAN,theASEANWorkPlanforMaternalandChildHealth(MCH)for2011to2015seekstoenhance,amongothers,thecompetencyofhealthcommunityworkersorpractitionersinbecomingaccreditedskilledbirthattendants(SBAs),addressing,asastrategy,thecapacityneedsofthehealthworkforceinmaternal,newbornandchildhealthcareatthelocalcommunitylevels.
Afteraseriesofconsultations,theASEANHealthMinisters’Meeting(AHMM)andSeniorOfficialsMeetingonHealthDevelopment(SOMHD)throughtheASEANTaskForceonMaternalandChildHealth(ATFMCH),withsupportfromrelevantstakeholders,haveendorsedthefirstASEANRegionalGuidelinesforMinimumRequirementforTrainingandAccreditationofSkilledBirthAttendants.TheguidelinesprovidecriticalinformationontherequiredcorecompetenciesofSBAsinASEAN,thestandardsfortheirtrainingprogrammes,aswellastherelevantrequirementsfortraininginstitutionsandfortheassessmentandaccreditationofSBAs.
ItishopedthatthisbookwillbeutilizedbytheASEANMemberStatesinaddressingtheworkforceneedsofmaternal,newborn,andchildhealthcareintheirrespectivecommunities,ultimately,contributingtobetterhealthoutcomesintheASEANCommunity.
LeLuongMinhSecretary-GeneralofASEAN
FOREWORD
6
FOREWORD
At the8thASEANSeniorOfficialsMeetingandsubsequentASEANTaskForceMeetingonMaternalandChildHealthheldinAugust2013,UNFPAandASEANagreedtocollaboratetopromotethematernalhealthofwomenintheASEANMemberStates.
LedbytheMinistryofHealthofMyanmar,andsupportedbyUNFPA,inOctober2013theASEANTaskForceonMaternalandChildHealthorganizedaworkshoptodeveloptheASEANRegionalGuidelineforMinimumRequirementsforTrainingandAccreditationofSkilledBirthAttendants.ThispublicationistheculminationofeffortsmadebyTaskForceMembersduringandafterthatworkshop.
SeveralASEANMemberStateshavebeenhighlysuccessfulinreducingmaternalandneonatalmortalityandmorbiditythroughtheadoptionofforwardlookingstrategiesprovidingmidwivesandotherpractitionerswiththenecessarytraining,skillsandcompetenciestobecomeaccreditedskilledbirthattendants(SBAs).TheRegionalGuidelineincorporatesexpertknowledgeandopinionfromwithintheregionandbeyond,providingguidanceonstrategiesandprocesses that representminimumrequirements forcoreSBAcompetencies,training,assessmentandaccreditation.
UNFPAiscommittedtoensuringthatscientificevidenceisusedtosupportthecriticalroleofSBAsinreducingmaternalmortality,andvaluestheessentialrolethatthesehealthprofessionalsperform.Recognizingthattherewillbeaneedforskilledbirthattendantswellbeyondthe2015deadlineforachievingtheMillenniumDevelopment Goals, UNFPA encourages each ASEAN Member State to use the Regional Guideline tostrengthennationaleffortstoprovidesafedeliveries,andthecareofmothersandtheirnewborninfants.
UNFPAwelcomesthisopportunitytocollaboratewithASEANandlooksforwardtoacontinuedpartnershipbothatregionalandcountrylevels.
NobukoHoribeRegionalDirector
UNFPAAsiaandthePacificRegionalOffice

7
1 AnAccreditedHealthProfessionalforthepurposesofthisguidelineis–ahealthprofessionalwhohasalegalrighttopractiseaccordingtocountrycontext
1. INTRODUCTION
Goal5–ImproveMaternalHealthisacriticalgoalamongtheeightMillenniumDevelopmentGoals(MDGs)andwillcontinuetobeprominentinthepost-2015healthagenda,asseveralcountrieswillnotreachtheMDGtargetssetoutattheMillenniumSummit.AkeyindicatorforMillenniumDevelopmentGoal(MDG)5is,“theproportionofdeliveriesassistedbyaskilledhealthprofessional/SkilledBirthAttendant(SBA)”.TheproportionofdeliveriesassistedbySBAsvarieswidelyamongASEANMemberStates(AMS).InfactthereareseveralreasonsunderlyingthesevariationsandamongstthemthemainreasonsarelackofaconsensusdefinitionofSBAbyAMSandlackofaccreditationsystemwithmidwiferycompetenciesinthecurriculumforSBAs.Nationalreportsandneedassessmentsreportthathealthprovidersareassistingavastmajorityofdeliveries.Howevermanyofthesedonothavethecompetencies,asinternationalrecommendation,forallthetaskstheskilledattendantisrequiredtoperformsafedeliveriesandsavethelivesofmothersandnewborns[1,2].
1.1 DefinitionAccordingtoJointstatementofWHO,ICM,FIGOin2004:ASkilledBirthAttendant(SBA)isdefinedas“anaccreditedhealthprofessional1-suchasmidwife,doctorornurse-whohasbeeneducatedandtrainedtoproficiency in theskillsneededtomanagenormal (uncomplicated)pregnancies,childbirthand immediatepostnatalperiodandintheidentification,managementandreferralofcomplicationsinwomenandnewborns”[3].
This applicable and consensus statement, which includes 23 competencies for qualified SBAs, helpsmedicaltrainingorganizationsdesigningtheircurriculatoachievetherequiredcompetenciesofSBA.TheJointstatementisagoodstartingpoint,howeverinitselfnotsufficienttodeveloptheprocessoftraining,certificationandlicensing.Myanmar,VietNamandLaoPDRareassignedasleadingcountriestodevelopaguidelinetohelpprovideacommonframeworkforthetrainingandaccreditationofSBAinASEANcountries.TheworkhasbeencarriedoutwiththeinvolvementandsupportfromUNFPA,WHOandJICA.
8
1.2 Purpose of the GuidelineThepurposeoftheGuidelineistoassisttheASEANMemberStates(AMS)to: (i).DefinethecorecompetenciesforSBAoftheASEANcommunityaswellasevaluationand accreditationmethods. (ii).EstablishtrainingstandardsforbirthattendantstomeettheASEAN’sSBAcorecompetencies. (iii).Definethecriteriaandprocessesforcapacityassessmentandaccreditationofatraining institutioncapableofdeliveringSBAtrainingand/oraccreditation,inaccordancewithASEAN agreedcorecompetencies.
Note: This guideline is a reference with common perspectives; each country in ASEAN will need to develop their specific regulations on qualification and accreditation process and training programme to ensure they are in line with their own national context.
9
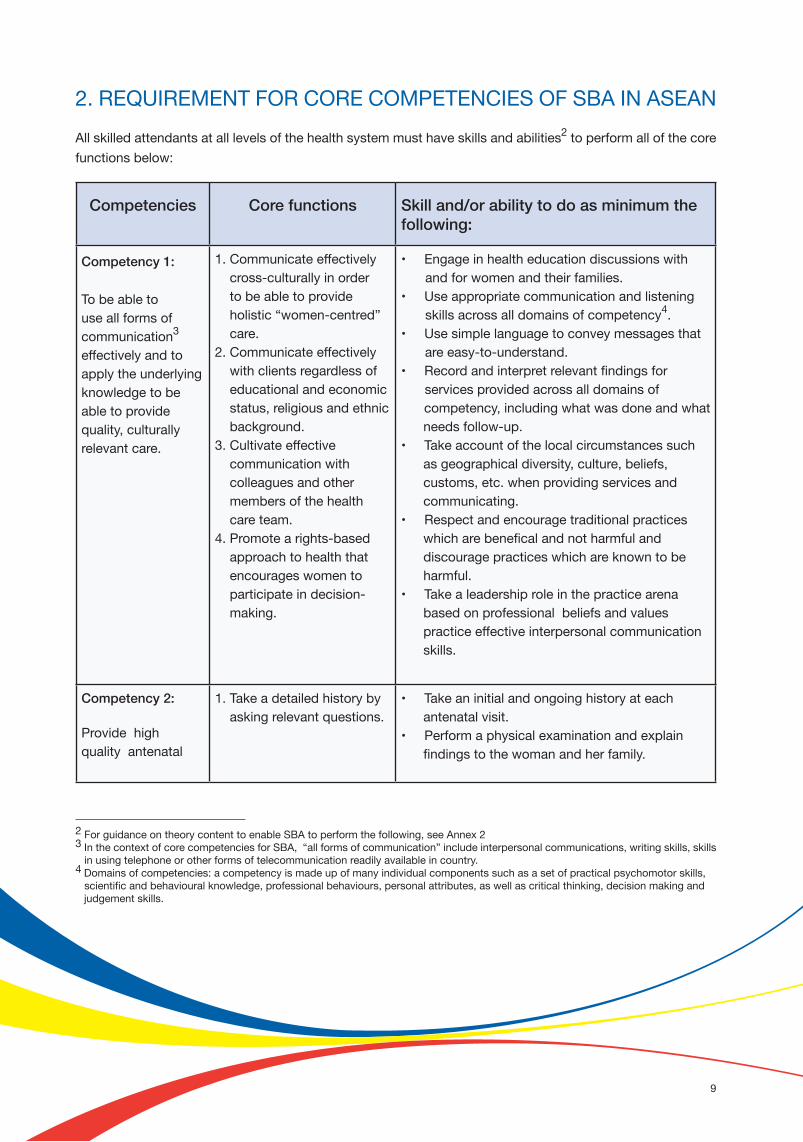
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 1:
Tobeabletouse all forms of communication3 effectivelyandtoapplytheunderlyingknowledgetobeabletoprovidequality,culturallyrelevantcare.
1.Communicateeffectivelycross-culturallyinordertobeabletoprovideholistic“women-centred” care. 2.Communicateeffectivelywithclientsregardlessofeducationalandeconomicstatus,religiousandethnicbackground.3.Cultivateeffectivecommunicationwithcolleaguesandothermembersofthehealthcareteam.4.Promotearights-basedapproachtohealththatencourageswomentoparticipateindecision-making.
•Engageinhealtheducationdiscussionswith andforwomenandtheirfamilies.•Useappropriatecommunicationandlisteningskillsacrossalldomainsofcompetency4.•Usesimplelanguagetoconveymessagesthatareeasy-to-understand.•Recordandinterpretrelevantfindingsforservicesprovidedacrossalldomainsofcompetency,includingwhatwasdoneandwhatneedsfollow-up.•Takeaccountofthelocalcircumstancessuchasgeographicaldiversity,culture,beliefs,customs,etc.whenprovidingservicesandcommunicating.•Respectandencouragetraditionalpracticeswhicharebeneficalandnotharmfulanddiscouragepracticeswhichareknowntobeharmful.•Takealeadershiproleinthepracticearenabasedonprofessionalbeliefsandvaluespracticeeffectiveinterpersonalcommunicationskills.
Competency 2:
Providehighqualityantenatal
1.Takeadetailedhistorybyaskingrelevantquestions.
•Takeaninitialandongoinghistoryateachantenatalvisit.•Performaphysicalexaminationandexplain findingstothewomanandherfamily.
2. REQUIREMENT FOR CORE COMPETENCIES OF SBA IN ASEANAllskilledattendantsatalllevelsofthehealthsystemmusthaveskillsandabilities2toperformallofthecorefunctionsbelow:
2ForguidanceontheorycontenttoenableSBAtoperformthefollowing,seeAnnex23InthecontextofcorecompetenciesforSBA,“allformsofcommunication”includeinterpersonalcommunications,writingskills,skillsinusingtelephoneorotherformsoftelecommunicationreadilyavailableincountry.4 Domainsofcompetencies:acompetencyismadeupofmanyindividualcomponentssuchasasetofpracticalpsychomotorskills, scientificandbehaviouralknowledge,professionalbehaviours,personalattributes,aswellascriticalthinking,decisionmakingandjudgementskills.

10
Competencies Core functions Skill and/or ability to do as minimum the following:
caretomaximizehealthduringpregnancythatincludesearlydetectionandtreatment5andwhereneededreferralofselectedcomplications.
2.Assessindividualneedsandgiveappropriateadviceandguidance.3.Performaphysicalexaminationtoassess healthstatusandprogress ofpregnancyandidentify problemsandgiveappropriatetreatmentand or refer.4.Performappropriatescreeningtestsasrequired5.Assistpregnantwomentomakeandupdatebirthplans.6.Educatewomen(andtheirfamiliesandotherssupportingpregnantwomen)inself-care,goodnutritionanddangersignsduringpregnancy,childbirthandthepostnatalperiod.7.Identifyobstetricandmedicalconditionsdetrimentaltothehealthofthemotherandfoetusespeciallypre-eclampsia,performfirst-linemanagement(includingperformanceoflife-savingprocedureswhenneeded)andmakearrangementsforeffective referral.
•Takeandassessmaternalvitalsignsincludingtemperature,bloodpressure,pulse.•Assessmaternalnutritionanditsrelationshiptofoetalgrowth;giveappropriateadviceonnutritionalrequirementsofpregnancyandhowtoachievethem.•Performacompleteabdominalassessmentincludingassessmentoffundalheightusingmanualmeasurements,lie,position,andpresentation.•Listentothefoetalheartrateanddeterminefoetalwell–beingandinterpretfindingsandtakeappropriateaction.•Evaluatefoetalgrowth,placentallocationandamnioticfluidvolume,usingultrasoundvisualizationandmeasurement(ifequipmentisavailableforuseandwithinscopeofpractice).• Performapelvicexamination,includingsizingtheuterus,anddeterminingtheadequacyofthebirthcanal.•PerformscreeningtestsforanaemiaHIV,syphilis,proteinuriaoranyothertestsaccordingtonationalprotocol.•Takebloodtodeterminebloodgrouping,andotherhaematologicalinvestigationsasmayberequired.•Administertetanusimmunizationaccordingtonationalprotocols.•Recordandreportallfindingsateachantenatalvisit.•Makedecisionsbasedonclinicalfindingsandtakeappropriateactionincludinggivingfeedbacktothewomanandfamilyandreferraltohigherlevelhealthfacilities.
5 Treatment–itisassumedallSBAsmustbeabletoofferasminimumfirstlinetreatment,toincludeperforminglifesavingmeasures

11
6 InformationinBirthPlanshouldincludeasminimum;peoplewhowillbepresentduringlabourandbirth,essentialsuppliesformother andnewborn(willvarybycontext):clothingneededforgingtohealthfacility,nursingbrasandpads,etc.Signsandsymptomsoftheonsetoflabour(includingwomen’sperceptionsandsymptoms);7“Selfandfamily-care”isintendedtoinclude:goodnutritionforpregnancyandhowtoachievethem.Adviseonironsupplementationtopreventanemia;working,physicalactivities,restingduringscheduledappointments;+Hygience(sexualorgans,breast,body);Avoidharmfulfactorsonthepregnantwomanandfoetussuchassmoking,alcoholabuseandillicitdrug,toxicworkplace,etc.
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 2 (contd):
•Assistpregnantwomenandtheirfamiliesinmakingandupdatingaplanforbirth6:•Makearrangementsfortimelyeffectivereferral•Discourageharmfulcustomsandpractices•Identifysignsandsymptomsofobstetricandmedicalconditionsdetrimentaltothehealthofthewomanandfoetusandmakeclinicaldecisionsbasedonfindingsandtakeappropriateactionincludinggivingfirstlinemanagementandmakingeffectivereferral.•Providefullcounsellingtothewomantoaccepttreatmentand/orreferralcheck-up,monitoring.•Educatewomen(andtheirfamiliesandotherssupportingpregnantwomenandnewborn)on:-theimportanceofregularcheck-up - Self7andfamilycare-theneedforcreatingasafeandhealthyenvironment•Counsellingon-thebenefitsofearlyandexclusivebreastfeeding. -sexualpracticeduringpregnancyandafterchildbirth-voluntaryfamilyplanningandbirthspacingfollowingchildbirth•Psychologicalsupportformother:normalpsychologicalchangesinpregnancy,information

12
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 2 (contd):
aboutreliefofcommondiscomforts, techniquesforincreasingrelaxationandpainreliefmeasuresavailableforlabour.•Explaintothewomanonhowtoidentifytheonsetoflabourandneedforgoingtohealthfacilityearlytoallowforgoodmonitoringandcareduringlabour.•Emergencypreparednessandpreparingforpossiblecommunity-basedreferral:whotocontact,whatsupport,etc.•Performfirst-linemanagement(includingperformanceoflife-savingprocedureswhenneeded.
Competency 3:
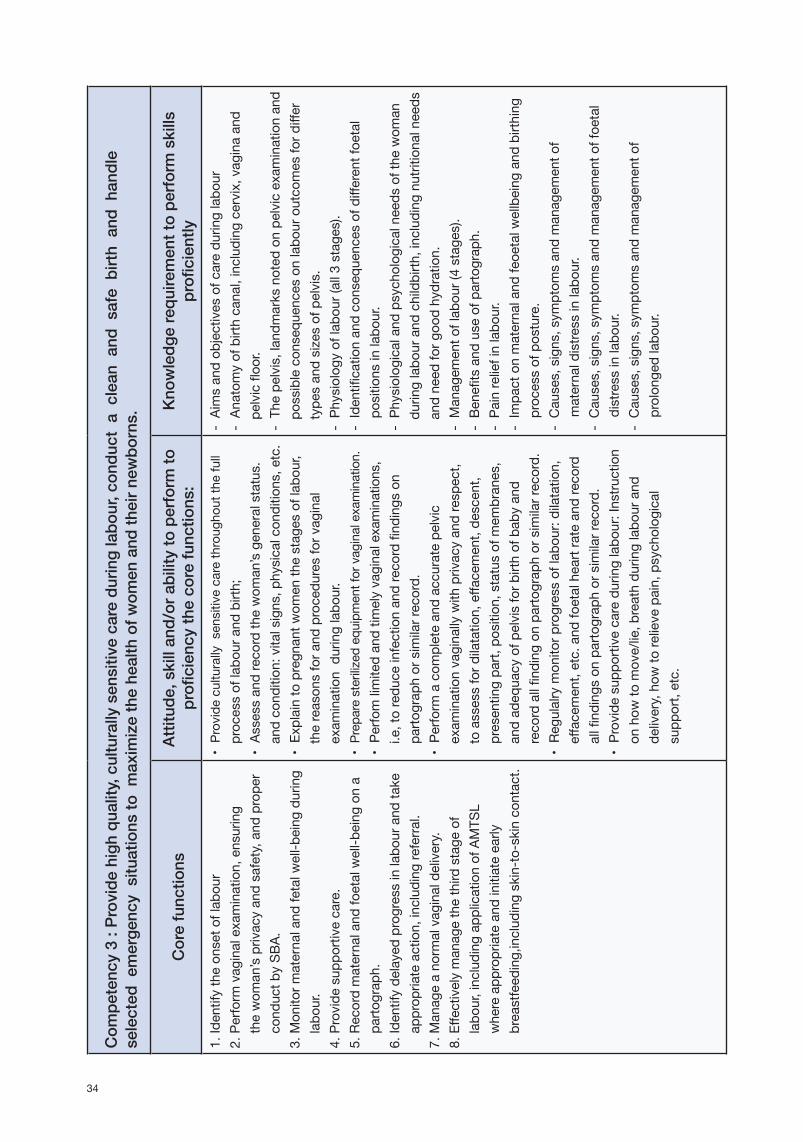
Providehighquality,culturallysensitivecareduringlabour,conductacleanandsafebirthandhandleselectedemergencysituationstomaximizethehealthofwomenandtheirnewborns.
1.Identifytheonsetoflabour2.Performvaginalexamination,ensuringthewoman’sprivacyandsafety,andproperconductbySBA.3.Monitormaternalandfetalwell-beingduringlabour.4.Providesupportivecare.5.Recordmaternalandfoetal well-beingonapartograph.6.Identifydelayedprogressinlabourandtakeappropriateaction,includingreferral.7.Manageanormalvaginaldelivery.8.Effectivelymanagethethirdstageoflabour,includingapplicationofAMTSLwhereappropriate andinitiateearlbreastfeeding,includingskin-to-skincontact.
•Provideculturalysensitivecarethroughoutthefullprocessoflabourandbirth;•Assessandrecordthewoman’sgeneralstatusandcondition:vitalsigns,physicalconditions,etc.•Explaintopregnantwomenthestagesof labour,thereasonsforandproceduresforvaginalexaminationduringlabour.•Preparesterilizedequipmentforvaginalexamination.•Perfomlimitedandtimelyvaginalexaminations,toreduceinfectionandrecordfindingsonpartographorsimilarrecord.•Performacompleteandaccuratepelvic examinationvaginallywithprivacyandrespect,toassessfordilatation,effacement,descent,presentingpart,position,statusofmembranes, andadequacyofpelvisforbirthofbabyand recordallfindingonpartographorsimilar record.•Regularlymonitorprogressoflabour:dilatation,effacement,etc.andfoetalheartrateandrecordallfindingsonpartographorsimilar record.

13
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 3 (contd):
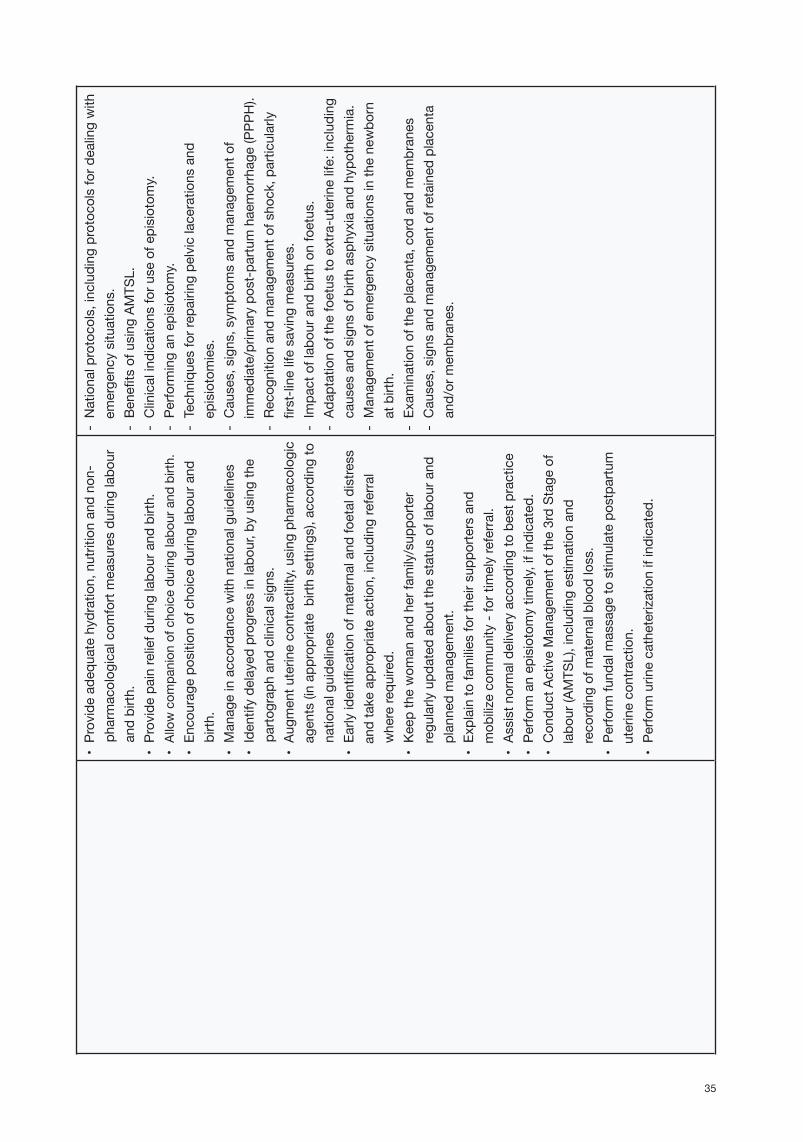
•Providesupportivecareduringlabour:Instructiononhowtomove/lie,breathduringlabouranddelivery,howtorelievepain,psychologicalsupport,etc.•Provideadequatehydration,nutritionandnon-pharmacologicalcomfortmeasuresduringlabourandbirth.•Providepainreliefduringlabourandbirth•Allowcompanionofchoiceduringlabourandbirth.•Encouragepositionofchoiceduringlabourandbirth.•Manageinaccordancewithnationalguidelines•Identifydelayedprogressinlabour,byusingthepartographandclinicalsigns.•Augmentuterinecontractility,usingpharmacologicagents(inappropriatebirthsettings),accordingtonationalguidelines.•Earlyidentificationofmaternalandfetaldistressandtakeappropriateaction,includingreferralwhererequired.•Keepthewomanandherfamily/supporterregularlyupdatedaboutthestatusoflabourandplannedmanagement.•Explaintofamiliesfortheirsupportersandmobilizecommunity-fortimelyreferral•Assistnormaldeliveryaccordingtobestpractice.•Performanepisiotomytimely,ifindicated.•Conductactivemanagementofthe3rdstageoflabour(AMTSL),includingestimationandrecordingofmaternalbloodloss.•Performfundalmassagetostimulatepostpartumuterinecontraction.
8ActivemanagementoftheThirdstageoflabour(AMTSL)hasanumberofcomponents:giveintramuscularlyanoxytocixdrug,manuallydetectuterinecontraction,encouragethewomantoexpeltheplacenta(sometimesarchivedbyhavingthewomanchangepositionorsit/squatonabed-pan).Thepracticeofcontrolledcordtractionwhilstsimultaneouslyguardingtheuterusisnolongerrecommendedunlessallotherattemptsabovedonotwork.
14
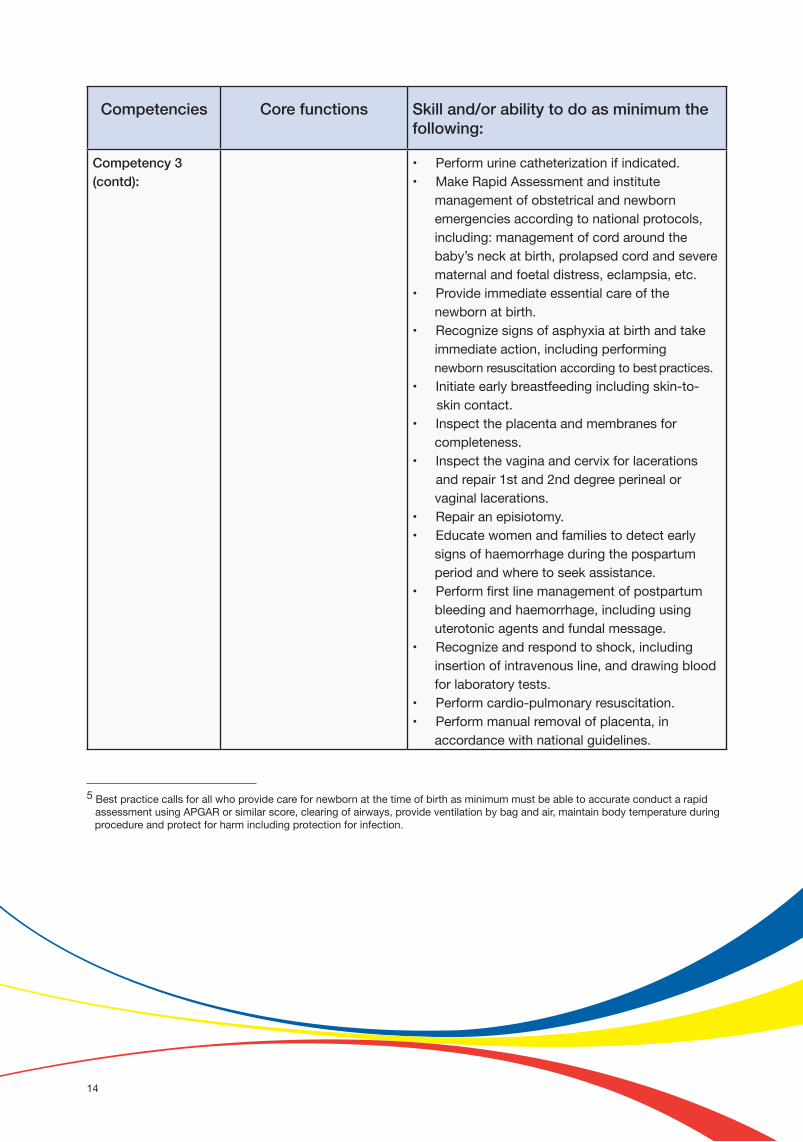
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 3 (contd):
•Performurinecatheterizationifindicated.•MakeRapidAssessmentandinstitutemanagementofobstetricalandnewbornemergenciesaccordingtonationalprotocols,including:managementofcordaroundthebaby’sneckatbirth,prolapsedcordandseverematernalandfoetaldistress,eclampsia,etc.•Provideimmediateessentialcareofthenewbornatbirth.•Recognizesignsofasphyxiaatbirthandtakeimmediateaction,includingperforming newbornresuscitationaccordingtobestpractices.•Initiateearlybreastfeedingincludingskin-to- skincontact.•Inspecttheplacentaandmembranesforcompleteness.•Inspectthevaginaandcervixforlacerationsandrepair1stand2nddegreeperinealorvaginallacerations.•Repairanepisiotomy.•Educatewomenandfamiliestodetectearlysignsofhaemorrhageduringthepospartumperiodandwheretoseekassistance.•Performfirstlinemanagementofpostpartumbleedingandhaemorrhage,includingusinguterotonicagentsandfundalmessage.•Recognizeandrespondtoshock,includinginsertionofintravenousline,anddrawingbloodforlaboratorytests.•Performcardio-pulmonaryresuscitation.•Performmanualremovalofplacenta,inaccordancewithnationalguidelines.
5 Bestpracticecallsforallwhoprovidecarefornewbornatthetimeofbirthasminimummustbeabletoaccurateconductarapid assessmentusingAPGARorsimilarscore,clearingofairways,provideventilationbybagandair,maintainbodytemperatureduring procedureandprotectforharmincludingprotectionforinfection.

15
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 3 (contd):
•Performinternalbimanualcompressionoftheuterustocontrolsevereuterinebleedingandperformaorticcompressionifindicated.•Arrangeforandundertaketimelyreferralandtransferofwomenwithseriouscomplicationstoahigherlevelhealthfacility,takingappropriatedrugsandequipmentandaccompaniedbyahealthprofessional.
Competency 4.1: Providecomprehensive,highquality,culturallysensitivecareinpostpartumperiod.
1.Identifyhaemorrhageandperformmanagementduringimmediatepostpartumperiod.2.Providepostnatalcaretowomen.3.Identifyillnessesandconditionsdetrimentaltothehealthofwomeninthepostnatalperiod.4.Provideadviceon postpartumfamilyplanning.
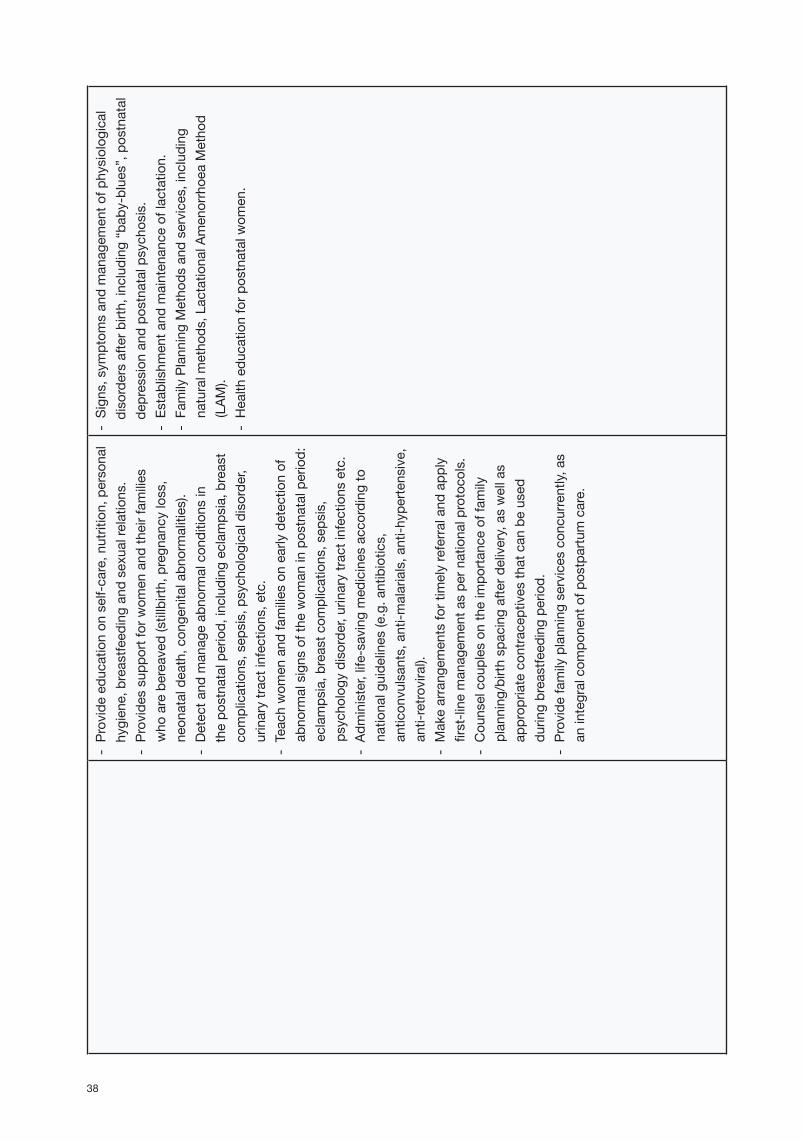
•Provideculturallysensitivecareandsupport.•Monitorcontractionoftheuterus,pulse,bloodpressuretoearlydetecthaemorrhageduringthepospartumperiod(atleastonceduringthefirst6hoursafterdelivery,firstdayafterdelivery,andfollowingdaysasneeded).•Assessforuterineinvolutionandhealingoflacerationsand/orrepairs.•Performpostnatalscreeningtestsaccordingtonationalpolicy.•Educatewomanhowtomassagetheuterustokeepitwell-contracted.•Explaintowomanandherfamilyaboutlife-threateningsituationsiftheyarise,andmanagementprocedures.•Provideeducationonself-care,nutrition,personalhygiene,breastfeedingandsexualrelations.•Providesupportforwomenandtheirfamilies whoarebereaved(stillbirth,pregnancyloss,neonataldeath,congenitalabnormalities).•Detectandmanageabnormalconditionsinthepostnatalperiod,includingeclampsia,breastcomplications,sepsis,psychologicaldisorder,urinarytractinfections,etc.• Teachwomenandfamiliesonearlydetectionofabnormalsignsinpostnatalperiod:

16
Competencies Core functions Skill and/or ability to do as minimum the following:
eclampsia, breast complications, sepsis, psychology disorder, urinary tract infections etc. • Administer, life-saving drugs according to national guidelines (e.g. antibiotics, anticonvulsants, anti-malarials, anti- hypertensive, anti-retroviral).• Make arrangements for timely referral and apply management as per national protocols.• Counsel couples on the importance of family planning/birth spacing after delivery, as well as appropriate contraceptives that can be used during breastfeeding period.• Provide family planning services concurrently, as an integral component of postpartum care.
Competency 4.2:Provide high quality, culturally sensitive, post- abortion care.
1. Detect signs of miscarriage and provide emergency management.2. Provide post abortion family planning counselling and services.
• Diagnose miscarriage.• Insert IV line.• Accompany the patient to the health facility.• Perform evacuation of retained products of conception according to national guidelines.• Provide psychological support.• Provide post-abortion family planning counselling and service according to national guidelines.
Competency 5:
Provide high-quality,
comprehensive care
for the
healthy
infant
from birth
to
two months
of
age.
1. Assess the newborn at birth and give immediate care.2. Identify any life threatening conditions in the newborn and give essential life- saving measures,including, where necessary, active resuscitation as a component of the management of birth asphyxia, and referral where appropriate.
• Provide immediate care to the newborn, including: dry the newborn; place in skin-to-skin contact on mother’s abdomen or chest and cover to keep baby warm; suctioning (if needed); cord clamping and cutting when pulsation ceases.• Take steps to prevent infection.• Assess the immediate condition of the newborn (e.g., APGAR scoring or rapid assessment method: breathing, colour of the skin and heart rate).• Promote and maintain normal newborn body temperature through skin-to-skin contact (e.g.,
17
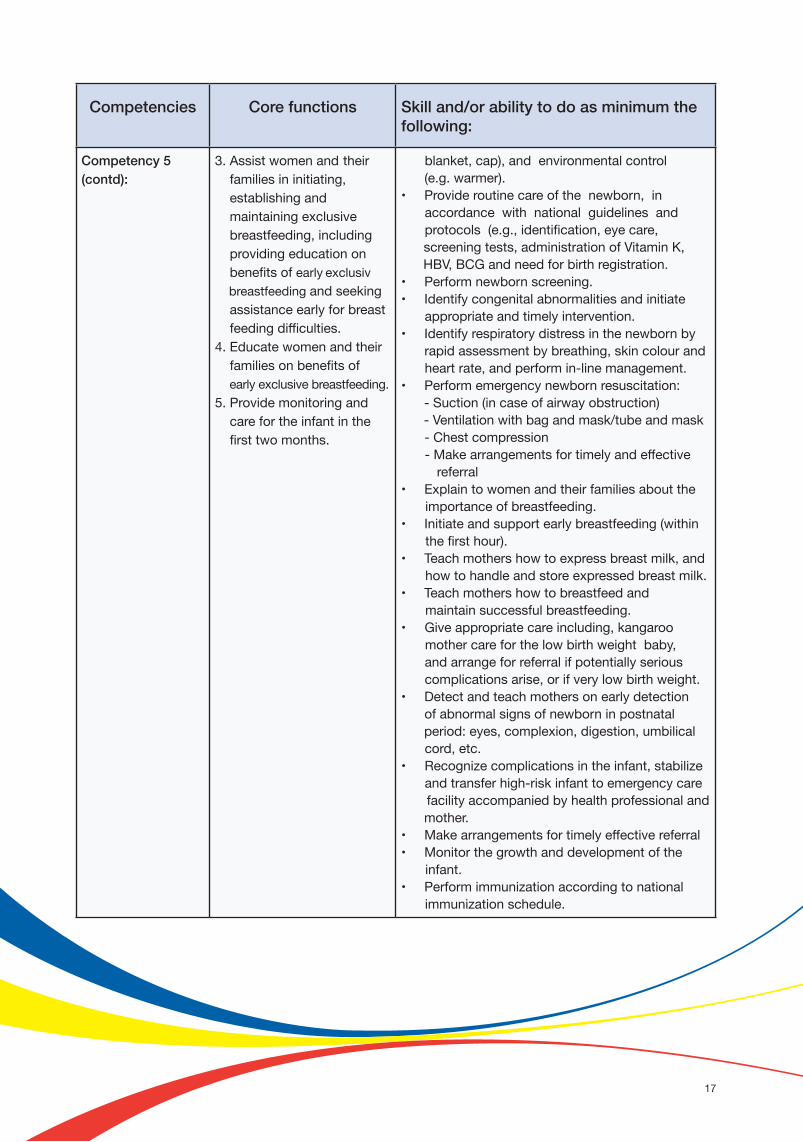
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 5 (contd):
3.Assistwomenand theirfamiliesininitiating,establishingandmaintainingexclusivebreastfeeding,includingprovidingeducationonbenefitsofearlyexclusivbreastfeedingandseekingassistanceearlyforbreastfeedingdifficulties.4.Educatewomenandtheirfamiliesonbenefitsofearlyexclusivebreastfeeding.5.Providemonitoringandcarefortheinfantinthefirsttwomonths.
blanket,cap),andenvironmentalcontrol(e.g.warmer).•Provideroutinecareofthenewborn,inaccordancewithnationalguidelinesandprotocols(e.g.,identification,eyecare,screeningtests,administrationofVitaminK,HBV,BCGandneedforbirthregistration.•Performnewbornscreening.•Identifycongenitalabnormalitiesandinitiateappropriateandtimelyintervention.•Identifyrespiratorydistressinthenewbornbyrapidassessmentbybreathing,skincolourand heartrate,andperformin-linemanagement.•Performemergencynewbornresuscitation:-Suction(incaseofairwayobstruction)-Ventilationwithbagandmask/tubeandmask-Chestcompression-Makearrangementsfortimelyandeffective referral•Explaintowomenandtheirfamiliesabouttheimportanceofbreastfeeding.•Initiateandsupportearlybreastfeeding(within thefirsthour).•Teachmothershowtoexpressbreastmilk,and howtohandleandstoreexpressedbreastmilk.•Teachmothershowtobreastfeedandmaintainsuccessfulbreastfeeding.•Giveappropriatecareincluding,kangaroomothercareforthelowbirthweightbaby,andarrangeforreferralifpotentiallyserious complicationsarise,orifverylowbirthweight.•Detectandteachmothersonearlydetectionofabnormalsignsofnewborninpostnatalperiod:eyes,complexion,digestion,umbilical cord,etc.•Recognizecomplicationsintheinfant,stabilize andtransferhigh-riskinfanttoemergencycarefacilityaccompaniedbyhealthprofessionalandmother.•Makearrangementsfortimelyeffectivereferral•Monitorthegrowthanddevelopmentoftheinfant.•Performimmunizationaccordingtonationalimmunizationschedule.

18
Competencies Core functions Skill and/or ability to do as minimum the following:
Competency 6
Provide high quality, culturally sensitive health education and services to all in the community, to promote healthy family life, planned pregnancies and positive parenting.
1. Educate women and their families on how to prevent sexually transmitted infections including HIV.2. Supervise non-skilled attendants, including TBAs where they exist, in order to ensure that the care they provide during pregnancy, childbirth and early postpartum period is of sound quality.3. Collect, analyse and report relevant data of women and their newborns4. Promote an ethos of shared responsibility and partnership with individual women, their family members and the community for the care of women and newborns throughout pregnancy, childbirth and the postnatal period
• Educate and communicate with women and
up/medical examination.• Educate women and their families on risk factors of sexually transmitted infections and how to prevent sexually transmitted infections.• Educate members of the community how to recognize sexually transmitted infections/ reproductive tract infections and seek health care.• Educate families and communities on dangers of early teenage pregnancies.
• Identify birth attendants who are not yet SBAs, including TBAs where they exist (numbers, workplace).• Work in partnership with non-skilled attendants to identify pregnant women and encourage them to seek antenatal care, safe delivery and postnatal care with skilled health professionals.• Educate non-skilled attendants on practices to avoid during pregnancy, delivery and postnatal period.• Collect, report data on a monthly, quarterly and yearly basis, as the national reporting guidelines dictate.• Analyse relevant data on women and their
to promote good health care practice (evidence- based practices).• Promote partnership with colleagues to provide high-quality Maternal and Newborn Health care in health facilities: manage and provide comprehensive health care, provide adequate information on maternal and newborn care.• Promote partnership with the community to provide quality evidence-based home-based care for mothers and newborns.• Make arrangements for referrals including for emergency care, etc.• Health education and promotion to families and communities, including community leaders and
newborn health practices and services.

19
The above Competencies were developed based on:Makingpregnancysafer:thecriticalroleoftheskilledattendant,ajointstatementbyWHO,ICMandFIGO,2004[3];StrengtheningMidwiferyToolkit,WHO2011[4]);Essentialcompetenciesforbasicmidwiferypractice2010,revised2013,ICM2013[6].Memberstatesmayaddtothesecompetenciesandorskillsaccordingtonationalcontext.ForknowledgebasetoperformthesecompetenciesseeAnnex2.TheASEANregionalcompetencylistabovehasbeendevelopedasaguidetominimumrequirementsfortheskillsandcorefunctionofwhatSBAsinASEANcountriesshouldbeabletoprovide.

20
3. STANDARDS FOR SBA TRAINING PROGRAMMES
3.1 Types of training Four types of training are recognized as applicable in the ASEAN region: 1. SBA Accreditation as part of an initial pre-service programme (e.g. for nursing, midwifery or medicine). 2. SBA Accreditation as integral to a recognized Post-basic Nursing programme to obtain an additionalLicense/Certification/Registration(e.g.:asamidwife/nurse-midwife)oraspecialized clinical course for Medical Practitioners. 3. Specialized Post-basic/part of Continuing Professional Development (CPD) for Accreditation for Health Providers who are not SBAs. 4. Professional updating for midwives, nurse-midwives, doctors or others, to meet competencies for SBA in the ASEAN region.
3.2 Admission requirementsType 1 and 2: determined by national regulations depending on the type of programme.Type 3 and 4: to be recognized as SBA for existing health providers, entry requirements should, as a minimum,
include: - Hold a professional accreditation/registration or license as a health provider according to National Human Resources for Health (HRH) system. - Currently working on maternal and newborn care. - Willing to be trained for improvement and for SBA accreditation.Regardless of type of training, on completing of any of above the health providers must be able to demonstrate they have all the required competencies of SBA in the ASEAN region. As such they should be able to demonstrate they have: -TherequisiteknowledgeandskillstobeabletoperformallthecorefunctionsasdefinedinSection2. -The required professional and ethical attitude to practise maternal and newborn care for safe motherhood while respecting human rights, dignity and the cultural values of the mother’s locality.
3.3 Standards for training programmes 1. All training programmes should be competency–based. 2. All courses should provide minimum of 50% clinical practice for type 1 and type 2, but for type 3 and 4 there should be a minimum of 70% (more may be needed depending on need, and decisions on length and content should be based on a detailed Needs Assessment). 3. For the minimum number of cases during the training, see matrix below:

21
Minimum number of case (for content be covered in each case see annex 2)
Type 1
SBA Accreditation -part of initial pre-service programme
Type 2
SBA Accreditation
Post-basic Nursing
programme
Type 3
Specialized Post-basic/
part of CME for Accreditation
for Health Providers
Type 4
Professional updating for midwives,
nurse-midwives, doctors
1. ANC 40 20 20 3
2.Complicated pregnancies*
10 10 10 Asneeded
3. Normal vaginal deliveries 20 10 10 3
4.Abnormal /complicated deliveries (breech/face )
2 2 2 Asneeded
5.Essential care of newborn at birth
20 10 10 3
6. Postnatal care of mother and baby - first 24 hours 40 20 20 6
7.Postnatal care mother and baby after 24 hrs up to 6 weeks
40 20 20 6
8.Complications of postpartum period** 10 10 10 Asneeded
9.Care of women following haemorrhage and/or sepsis in pregnancy
2 2 2 Asneeded
NOTE :Foritem2,3,8and9inmatrixabove:InsomecountriesstudentsundertakingType1and2wouldnotberesponsibleforthecasebutmustassistinthemanagementofcases.*Priorityshouldbegiventomanagingpre-eclampsiaandeclampsia.**Priorityshouldbegiventomanagementofpostpartumhaemorrhage.
22
4. REQUIREMENTS FOR TRAINING INSTITUTIONS
Based on global standards for initial education of professional nurses and midwives[5] (for pre-servicetraining),andstandardsofgoodpracticeformedicaleducation,all traininginstitutionswishingtoprepareSBAsmustmeetminimumrequirementsasdescribedbelow.
4.1. Teaching staffTeaching staff/Trainee ratioForclassroomteachingtheminimumstandardteachertostudentratiois1:20.Forskillslaboratorytheminimumstandardteachertostudentratiois1:5forsimulationpractices.Forclinicalpracticetheminimumstandardteacher/clinicalpreceptorormentortostudentratiois1:4.
Qualifications of Teaching StaffMustholdarecognizedprofessionalqualificationinthesubjecttheyareteaching.MusthaveundertakenapreparationforTrainingofTrainers(TOT).Musthaveundertakenrecent(withinthelast3-5years)professionalupdating.
In addition to small group teaching and clinical training, teaching staff also have the responsibility ofsupervising,coachingandmentoringoftrainees.
4.2 Training programme and materials 1.Thetraininginstitutionmustdevelopaspecifictrainingprogrammeincludingcurriculumand teachingandlearningmaterialsbasedontheminimumcompetenciesasdescribedinsection2 andthestandardfortrainingprogrammeinsection3ofthisguideline. 2.Allteachingandlearningmaterialsmustbesuitableforcompetency-basedtraining–boththeory andpracticum.Thematerialsneedtobeevidence-basedwithup-to-dateinformationonhealth promotion,obstetricsandnewborncare.
4.3. Required infrastructure and equipment 1.StandardsforType1andType2trainingwillbedefinedaccordingtonationalregulations. 2.StandardsforType3and4trainingmusthavethefollowing:
Alargeclassroomwithatleast2M2/participantthatisfullyequippedwithaudiovisualequipment.
Atleastoneskillslabroomequippedwithmodels,teaching/learningaids,posters,etcforensuringqualityoftraining.Theamountofequipmentshouldbesufficientforeachparticipanttobeabletopractisethreetimesforeachskill.(For a detailed description of classroom and skills lab room requirements see Annex 3)

23
4.4. Clinical practice siteAlltraininginstitutionsmusthaveorcooperatewithatleastoneclinicalpracticesiteofferingMCHserviceswhichmeetthefollowingminimumrequirements: 1.Havetheappropriatenumberofteachingstaff,asdescribedinitem4.1. 2.Normallyhave,asminimum,anaverageof60vaginaldeliveriespermonthinthe6monthspriorto studentpractice. 3.Havewrittencommitmenttoensureeachtraineewillhavetheopportunitytoimplementthe minimumnumberofcasesinclinicalpracticerequiredin3.3. 4.Allclinicalsitesmusthaveregularperiodicauditsofclinicalpractice,toensuretheymeetnational guidelines/protocols.
A clinical practice site could be a provincial, district level health facility or district level health facility incombinationwithsub-districtlevelhealthfacilities.

24
5. ASSESSMENT AND ACCREDITATION OF SBA
5.1 Candidates to be assessed to be accredited as SBAThecandidatesinclude: •Healthproviders(doctors,midwivesandnurses)whoareworkinginthefieldofmaternaland newborncare,providingmidwiferycareandhaveaneedtobeaccreditedasSBA; •Newgraduatesofpre-servicemidwiferyormedicalprogrammeswheretheyareexpectedtooperate asSBAimmediatelyaftergraduation(exceptwhereSBAcompetenciesareincludedinfinalexit examination); •AccreditedhealthprofessionalswhohavecompletedaspecialistSBAprogrammeorSBArefresher trainingcourse(Type4programme).
5.2 Accreditation5.2.1 Assessment methods used to accredit SBA
AllcandidatesforSBAaccreditationmustundergoaformalassessmentofcompetencies.Assessmenttoolsandprocessesmayvaryaccordingtocountrycontextbutmustasminimumhavetwocomponentsincluding: -Multiplechoiceandcasemanagement; -OSCE/OSPE(Objectivestructuredclinical/practicalexamination)usingskillchecklistsforscoring (seeAnnex1forproposedmethodsofassessment).
5.2.2 SBA accreditation
ThecandidatewillbeaccreditedasASEANSBAifshe/heobtainsallthefollowing: -Atleast70%forthewrittenexamination; -Atleast80%ofthemaximalscoreforeachassessmentdomain; -PassalltheOSCE/OSPEstations.
5.3 Institutions eligible for conducting SBA assessmentAllinstitutionsconductingSBAassessmentsand/orprovidingtrainingofSBAsmustbeformallyapprovedandaccreditedbyanauthorizedorganization(s)andMinistryofHealth.
TheinstitutionsshouldideallyhavebeeninvolvedindeliveryofSBAtraining,butregardlessofiftheyhavebeeninvolvedindeliveryorSBAtrainingornot,allinstitutionswillneedtomeetthefollowingcriteriatobeeligibleforconductingSBAassessmentandaccreditationofSBA:
5.3.1 Standards for institutions conducting SBA assessment
AllfacilitiestobeaccreditedforconductingSBAassessmentsmusthaveasminimumthefollowing: 1.Atheory-basedexaminationarea(room)foratleast20examineespersession(paper-basedor computer-basedtest),adequately-equipped(furniture/computers).
25
2.AnOSCE/OSPEexaminationarea,includinganadequatenumberofseparatedroomswithone- wayflowtolimitcommunicationbetweencandidatesgoinginandout: -Waitingroom:adequatechairsforcandidates,atleast20chairs; -Examinationroom/roomswithadequatespaceforOSCE/OSPE; -Post-examinationroom:adequatechairsforcandidateswhofinishedtheirexamination.
3.AdequatecommodityandequipmentforOSCE/OSPE,including: -Models,simulators,tools,commoditiescorrespondingtoeveryskillbeingassessed; -OthercommoditiesforOSPE:timer(tomeasureminutes);bells,etc.Ifaffordable,acamera systemwithlargedisplaytobeprovidedformonitoringpurpose.
5.3.2. Minimum standards for examiners
Theremustbeadequateexaminers(atleast2examinersperstation).Allexaminersmustmeetallthefollowingcriteria: •Beacertified/licensed/accreditedSBA,orhavepost-graduateorequivalentdegreeinobstetrics- gynaecologyormidwfery; •Haveover10yearsexperienceofpractisingasSBA; •BeaSBAtrainerormaternal/newbornhealthtrainer; •BetrainedinconductingOSCE/OSPE; •HaveattendedSBAPreparationofExaminersworkshop,tobefamiliarintoolsandprocessesfor theassessment.
5.3.3 Other human resources required
Inadditiontoexaminers,theremustbesufficentassistants,tohelpwithtimekeeping,ensureOSCE/OSPEstationsarewellmaintainedandescortcandidatestostations.
There shouldbeat least twocoordinatorsper assessment session formanaging recordsandorganizingassessment,ormanagingunforseenincidents/potentialdisruptions.
5.4. Accreditation of training institutionsAccreditation reflects thesystematicassessmentof infrastructure (which includesmanpower, equipment,etc.) requiredforconductingSBAtraining. It refers toavoluntaryprocesswherein therequirementof thetrainingfacilityisassessedagainstsetstandards.
5.4.1 Committee for Accreditation
TheCommittee forAccreditation ofSBA training siteswill be set upbyMinistry ofHealth or authorizedorganization(oranagencyassignedbyMinistryofHealth)ofASEANMemberStates.
TheCommitteeshallbecomposedoffollowing:OBGYN(1),MidwiferyTeacher(1),MidwifewhoisanaccreditedSBA(1),Paediatrician(1),Medicaleducator(1),andMCHServiceManager(1).

26
5.4.2 Accreditation procedure
AllinstitutionsprovidingtrainingofSBAsmustbeapprovedandaccreditedbyanauthorizedorganization.
5.4.3 Application for accreditation as a training institution
Training institutionsapplying for sitesneedaccreditation forSBA trainingshouldprepare theappropriateapplicationdocuments,including: •ApplicationformtotheCommittee; •Reportofthetrainingsite,includingself-assessment; •ListandCVofallteachingstaffinvolvedintrainingandaccreditationofSBAs; •Up-to-datelistandstatusofinfrastructure,equipment; •Trainingprogrammeandmaterialstobeused; •ReportonSkillslabstatus.
5.4.4 Site assessment of institutions
TheSBAAccreditationCommitteewill: -ReviewapplicationdocumentsbasedonrequirementsdescribedinPart4ofthisdocument; -Conductasitevisitandassesstheinstitutionfortheactualassessment.
5.4.5 Post site visit and awarding accreditation
If thetraininginstitutionssitemeetsall therequirementsdescribedinPart4,theCommitteewill reporttotheMinistryofHealthorauthorizedorganization(oranagencyassignedbyMinistryofHealth)oftheASEANMemberStatethatanaccreditationcertificationrecommendationshouldbeawarded.
Ifthetraininginstitutionssitevisitshowssomedeficiencies,thenareportoutliningthesedeficiencieswillbesenttotheinstitution,withacopytotheMinistryofHealthorauthorizedaccreditationbody(oranagencyassignedbyMinistryofHealth)witha recommendationon the timewhen thesecondvisitwillbemade.Accreditationcertificationshouldbepostponeduntilallcriteriaaremet.
Exceptionally, where only minor deficiencies are observed during the site visit, the Committee may decide that a return visit is not necessary, as long as evidence is sent to the Committee that remedial action has been instituted. In such cases a defined period of time for such action should be stated. The Chairperson appointed to the Committee should ensure that all action is followed up and evidence is received and adequate. The report can be sent to the Ministry of Health or authorized accreditation body (or an agency assigned by Ministry of Health) whilst waiting for the evidence that remedial action has been instituted. Such evidence when received by the Committee should be forwarded to the authorized accreditation body.
27
6. RE-ACCREDITATION
Re-accreditation of institutions
6.1AnaccreditedSBAtraininginstitutionshallseekre-accreditationafterfiveyears;howevertheprocessforapplicationmustbegininthefourthyear.Supportivemonitoringcanbeconductedeverytwoyears,orasoftenasdeemednecessarybytheapprovedaccreditationauthority.
Re-accreditation of SBA
6.2.TheaccreditedSBAindividualshallapplyforre-certificationthroughher/hisimmediatesupervisor,orbyparticipationincontinuedprofessionaleducationprogramme(CPE).TheCPEcouldincludecertificationafterfollowingon-lineorothercourses.
6.3.Re-accreditationwillbedependentuponmeetingcertaincriteriaasdefinedbyeachASEANMemberState,butshouldinclude,asminimum,evidencethattheyhaveconductedatleast24deliveriesperyear,proofofsatisfactorypracticeandprooftheyhavepractisedallofthecompetenciesasoutlinedinPart2ofthisguideline.
REFERENCES1.Campbell,O.M.,W.J.Graham,andLancetMaternalSurvivalSeriessteeringgroup,Strategiesforreducingmaternalmortality:gettingonwithwhatworks.Lancet,2006.368(9543):p.1284-99.2.Maclean,G.D.,AnhistoricaloverviewofthefirsttwodecadesofstrivingtowardsSafeMotherhood.SexReprodHealthc,2010.1(1):p.7-14.3.WorldHealthOrganization,Makingpregnancysafer:thecriticalroleoftheskilledattendant:ajointstatementbyWHO,ICMandFIGO.2004.4.WHO,Strengtheningmidwiferytoolkit,2011.5.WHOandNursing&MidwiferyHumanResourceforHealth,Globalstandardsforinitialeducationofprofessionalnursesandmidwives,2009.6.ICM,Essentialcompetenciesforbasicmidwiferypractice2010,revised2013,2013.

28
Annex 1: SBA Assessment (Proposed Methodologies)Part 1: Skills suitable to be assessed by case management: -Assistpregnantwomenandtheirfamiliesinmakingbirthplans -Identifyandmanagepre-eclampsiaandeclampsia -Identifytheonsetoflabour -Identifyandmanageobstructedlabour -Providepostnatalcaretowomenandtheirnewborninfantsandpost-abortioncare -Identifyobstetricandmedicalconditionsdetrimentaltothehealthofwomenand/ortheir newbornsinthepostnatalperiod -Supportnon-skilledattendants,includingTBAswheretheyexist,inordertoensurethatthe supporttheyprovideduringpregnancy,childbirthandearlypostpartumperiodisofsoundquality -Collectandreportrelevantdataandcollaborateindataanalysisandcaseaudits
Part 2: Skills suitable to be assessed by observation of practice on simulators: -Communicateeffectivelycross-culturallyinordertobeabletoprovideholistic“women-centred” care. -Educatewomen(andtheirfamiliesandotherssupportingpregnantwomen)inself-careduring pregnancy,childbirthandthepostnatalperiod -Examinationofapregnantwoman -Recordmaternalandfoetalwell-beingonapartograph,identifymaternalandfoetaldistressand takeappropriateaction,includingreferralwhererequired -Manageanormalvaginaldelivery -Conductactivemanagementofthethirdstageoflabour -Identifyhaemorrhageinlabour,providefirst-linemanagement -Assistwomenandtheirnewbornsininitiatingandestablishingexclusivebreastfeeding -Provideadviceonpostpartumfamilyplanningandbirthspacing -Assessthenewbornatbirthandgiveimmediatecare -Activeresuscitation,wherenecessary -Educatewomen(andtheirfamilies)onhowtopreventsexuallytransmittedinfectionsincluding HIV

29
Annex 2 : Guidance for Developing Curricula andCourse Content for Short SBA Updating TrainingProgramme -MemberStateswishingtodevelopatailor-madeshortcoursetoaccreditthosehealthworkers whoareprovidingmidwiferycareandhavebeenfoundtobelackinginsomecompetencies, orspecificknowledgeorskillstofulfillthecompetencies,shouldfirstensurethataNeeds AssessmentisconductedbasedontheASEANcompetenciesforSBA(seeSection2). -Allcoursesshouldbecompetency-basedandapplyadultlearningtechniques. -Thelengthofcourseshouldalwaysensuresufficienttimeisallocatedtohands-on-practiceunder supervisionofacompetentpractitionerintheclinicalareatoreachproficiencylevel. -Attentionshouldbegiventotheneedforevidencethatshowsthelearnerhasattainedproficiency level. -Proficiencyisdefinedas:theabilitytoregularlyperformcorrectlyinallsituationsandrequires regularrepeatedpractice. -Coursecontentshouldincludealltheelementsthatmakeupacompetency,e.g,knowledge, skills,attitudeandexperience. -ThematrixbelowhasbeendevelopedasaguideforASEANMemberStatestodefinetheminimal knowledge,skillsandattitudesrequiredtofulfillthedefinedcorefunctionsproficiently.However anindividualcountrymayneedtoincludeadditionalitems,dependingoncountrycontext/needs.
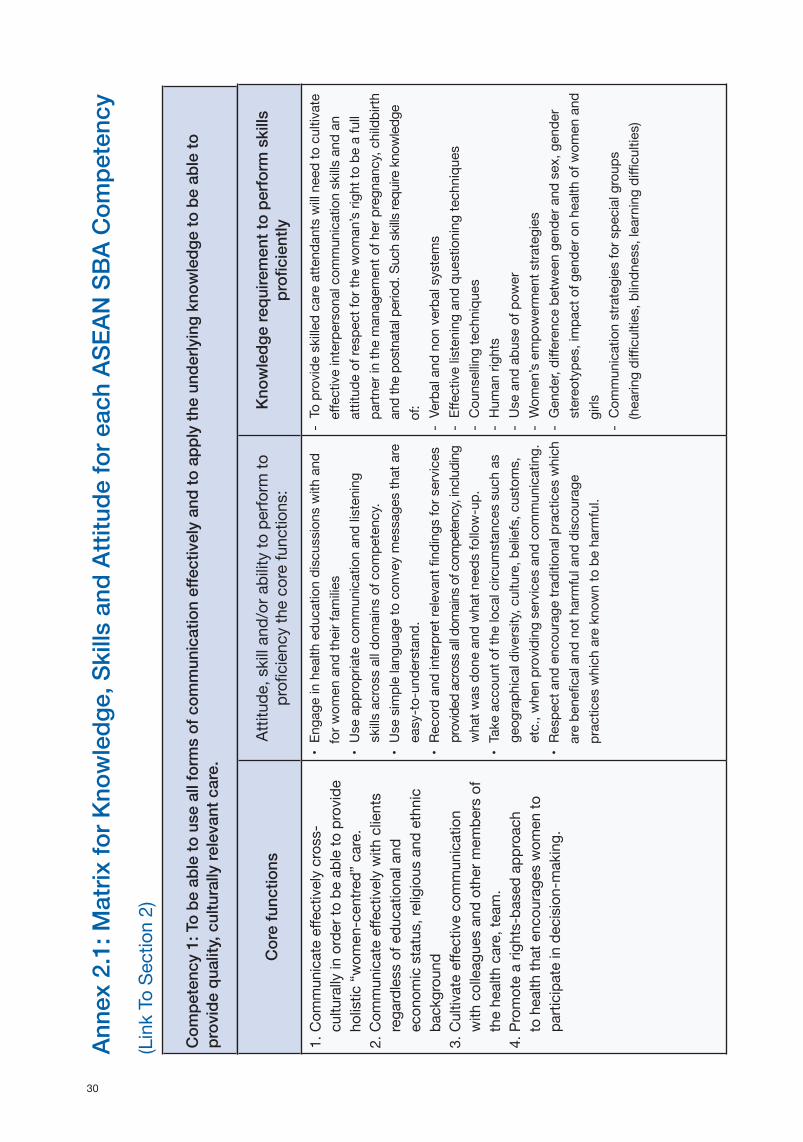
30
Com
pete
ncy
1: T
o be
abl
e to
use
all
form
s of
com
mun
icat
ion
effec
tivel
y an
d to
app
ly th
e un
derly
ing
know
ledg
e to
be
able
to
prov
ide
qual
ity, c
ultu
rally
rele
vant
car
e.
Anne
x 2.
1: M
atrix
for K
now
ledg
e, S
kills
and
Atti
tude
for e
ach
ASEA
N S
BA C
ompe
tenc
y(LinkToSection2)
Cor
e fu
nctio
nsAttitud
e,skilland/orabilitytoperform
to
proficiencyth
ecorefu
nctions:
Know
ledg
e re
quire
men
t to
perfo
rm s
kills
pr
ofici
ently
1.Com
municateeff
ectivelycross-
culturallyinorderto
beab
leto
provide
holistic“w
omen-centre
d”care.
2.Com
municateeff
ectivelywithclients
re
gardlessofedu
cationaland
econo
micstatus,re
ligiousand
ethnic
backgroun
d3.Cultivateeff
ectivecommunication
withcolleaguesandotherm
embe
rsof
th
ehealthcare,te
am.
4.Promotearig
hts-ba
sedap
proach
to
healthth
atencou
rageswom
ento
participateindecision-making.
•En
gageinhealthedu
cationdiscussion
swithand
forw
omenand
theirfam
ilies
•Useapp
ropriatecom
municationandlistening
sk
illsacrossalldom
ainsofcom
petency.
•Usesimplelang
uageto
con
veymessagesthatare
easy-to
-und
erstand.
•Re
cordand
interpretrelevantfind
ingsfo
rservices
providedacrossa
lldom
ainso
fcom
petency,including
whatw
asdon
eandwhatn
eedsfo
llow-up.
•Takeaccou
ntofthelocalcircum
stancessuchas
geog
raph
icaldiversity,culture,b
eliefs,customs,
etc.,w
henprovidingservicesand
com
municating.
•Re
specta
ndencou
ragetrad
ition
alpracticeswhich
arebe
neficaland
notharmfuland
discourage
practiceswhicharekno
wntobeharm
ful.
-Toprovide
skilledcareatte
ndantswillneed
tocultivate
eff
ectiveinterpersonalcom
municationskills
and
an
attitud
eofre
spectforth
ewom
an’srig
htto
beafull
pa
rtnerinth
emanagem
ento
fherpregn
ancy,childbirth
andthepo
stnatalperiod.Suchskillsrequireknowledg
e of:
-Verbaland
non
verba
lsystems
-Eff
ectivelistening
and
questioning
techniqu
es-Cou
nsellingtechniqu
es-Hum
anrigh
ts-Useand
abu
seofp
ower
-Wom
en’sem
powermentstra
tegies
-Gende
r,diffe
rencebe
tweengend
erand
sex,g
ende
rstereotype
s,im
pactofg
ende
ronhealthofw
omenand
girls
-Com
municationstrategiesfo
rspe
cialgroup
s(hearingdifficulties,b
lindn
ess,learning
difficulties)

31
•Takealead
ershipro
leinth
epracticearenaba
sed
on
professionalbe
liefsand
values.
•Practiseeff
ectiveinterpersonalcom
munication
skills
.
-Healthedu
cationstrategiesand
techniqu
es-Re
portwriting
-Bo
dies,respo
nsetostress(psychologicalandphysic
al)
-Griefand
theoriesofgriefrespo
nse
-Im
pactofd
ifferentreligiousand
spiritualbeliefson
pregnancy,childbirth
and
postnatalada
ptations.
Com
pete
ncy
2: P
rovi
de h
igh
qual
ity a
nten
atal
car
e, t
o m
axim
ize
hea
lth d
urin
g pr
egna
ncy
and
that
incl
udes
ear
ly d
etec
tion
and
treat
men
t or r
efer
ral o
f sel
ecte
d co
mpl
icat
ions
and
edu
catio
n, c
ouns
elin
g fo
r hea
lth d
urin
g pr
egna
ncy
and
prep
arat
ion
for b
irth
and
afte
r birt
h. Cor
e fu
nctio
nsAt
titud
e, s
kill
and/
or a
bilit
y to
per
form
to
profi
cien
cy th
e co
re fu
nctio
ns:
Know
ledg
e re
quire
men
t to
perfo
rm S
kills
pr
ofici
ently
1.Takeade
tailedhistorybyaskingrelevant
questions.
2.Assessindividu
alneedsand
giveap
prop
riate
adviceandgu
idance.
3.Pe
rform
aphysicalexaminationtoassess
healthstatusandprog
ressofp
regn
ancy
andidentifyprob
lemsandgiveapp
ropriate
tre
atmenta
nd/orrefer.
4.Perform
app
ropriatescreening
testsas
re
quired.
5.Assistp
regn
antw
omento
makeandup
date
birthplans.
6.Edu
catewom
en(and
theirfam
iliesand
otherssupp
ortingpregnantwom
en)inself
care,goo
dnutritionandda
ngersignsduring
pregn
ancy,childbirth
and
thepo
stnatal
period.
-Takeaninitialand
ong
oing
historyate
ach
antenatalvisit.
-Pe
rform
aphysicalexaminationandexplain
finding
stoth
ewom
anand
herfamily.
-Takeand
assessmaternalvitalsignsinclud
ing
tempe
rature,b
lood
pressure,pulse.
-As
sessm
aternalnutritionanditsre
lationshipto
foetalgrowth;giveapp
ropriateadviceon
nutritionalreq
uirementsofp
regn
ancyand
how
toachievethem
.-Pe
rform
acom
pleteab
dominalassessm
ent
includ
ingassessmento
ffunda
lheigh
tusing
manualm
easurements,lie,p
osition
,and
presentation.
-Listento
thefoetalheartrateand
determine
foetalbeing
-welland
interpretfind
ingsand
take
ap
prop
riateaction.
-AimsandObjectivesofA
ntenatalcare.
-De
cision
-makingskills
-Sa
feM
otherhoo
dprog
ramme(globa
land
national):
includ
ingfactorsthatputchildbe
aringwom
enatrisk
suchastoo-early,too
-freq
uentpregn
anciesand
too-
shortintervalsbetweenpregnancies.
-Ph
ysiologyofm
enstruation,con
ceptionandfoetal
de
velopm
ent.
-An
atom
yofpelvis.
-Nutritionalneedsduringpregnancy.
-Ph
ysiologyand
managem
ento
fpregn
ancy,including
sign
sandsymptom
sofpregn
ancyand
normal
psycho
logicalchang
esth
roug
houtpregn
ancy.
-Re
ason
sfortreatments,including
self-c
areform
inor
disordersofpregn
ancy.
-Causes,signssym
ptom
sandmanagem
ento
fbleed
ing
inpregn
ancy(earlyand
late).

32
7.Id
entifyob
stetricand
med
icalcon
ditions
detrim
entaltothehealthofthem
othera
nd
fo
etusespeciallypre-eclam
psia,p
erform
first-linemanagem
ent(includ
ingperfo
rmance
oflife-savingproced
ureswhenneed
ed)and
m
akearrang
ementsfo
reffe
ctivereferra
l.
-Evaluatefo
etalgrowth,p
lacentallocationand
am
nioticfluidvolume,usin
gultra
soundvis
ualization.
andmeasurement(ifeq
uipm
entisavailableforu
seandwithinscope
ofp
ractice).
-Pe
rform
apelvicexam
ination,includ
ingsizin
gthe
uterus,and
determiningthead
equacyofthebirth
canal.
-Pe
rform
screening
testsfora
nemiaHIV,syphilis,
proteinuriaora
nyotherte
stsaccordingtonational
protocols.
-Takeblood
todeterminebloo
dgrouping,and
other
haematolog
icalinvestigationsasmayberequ
ired
-Ad
ministertetanusim
muniza
tionaccordingto
nationalprotocols.
-Re
cordand
repo
rtallfind
ingsate
achantenatal
visit.
-Makede
cision
sba
sedon
clinicalfind
ingsand
takeapp
ropriateactioninclud
inggiving
feed
back
toth
ewom
anand
familyand
referra
ltohigh
erlevelhealthfacilities.
-As
sistp
regnantw
omenand
theirfam
iliesinmaking
andup
datingaplanfo
rbirth.
-Makearrang
ementsfo
rtimelyeff
ectivereferra
l.-Discou
rageharmfulcustomsandpractices.
-Identifysign
sandsymptom
sofobstetricand
med
icalcon
ditionsdetrim
entaltothewom
anand
fetusandmakeclinicaldecision
sba
sedon
find
ings
andtakeapp
ropriateactioninclud
inggiving
first
linemanagem
enta
ndm
akingeff
ectivereferra
l.
-Sign
s,m
anagem
enta
ndpotentialcon
sequ
encesof
pre-eclampsiaand
eclam
psia.
-Ph
ysiologyofformationofre
dbloo
dcellsand
haem
oglobin.
-Bloo
dgrou
ping
,Rhfactor,p
hysiolog
icalim
pactof
pregnancyon
cardiovascularsystem.
-Bloo
dgrou
pincompa
tibility.
-Causes,signsand
sym
ptom
s,con
sequ
encesand
managem
ento
fanemiainpregn
ancy.
-Causes,signs,sym
ptom
s,con
sequ
encesand
managem
ento
furinarytra
ctinfectioninpregn
ancy.
-Infectionpreventionprotocols.
-Mechanism
ofactionofvaccinesandnational
immuniza
tionprog
ramme.
-Sign
s,sym
ptom
sandtre
atmentforte
tanus.
-Cause,signsand
sym
ptom
s,includ
ingho
me-ba
sed
carefo
rminordisorde
rsofp
regn
ancy.
-Causes,signs,sym
ptom
s,con
sequ
encesand
managem
ento
fSexuallyTransmitted
Infections,
includ
ingHIV/AIDS.
-Im
pactofp
overtyand
poo
rnutritionon
pregn
ancyand
foetaldevelop
ment.
-Drug
sandpregnancy,includ
ingda
ngersofnon
-prescribed
and
trad
ition
aldrugsinpregn
ancy.
-Ap
plying
healthedu
cationap
proachesinpregn
ancy,
includ
ingbe
haviou
rchang
estrategiesand
impa
ctof
tra
ditionalbeliefsonhealthofm
othera
ndchild.
33
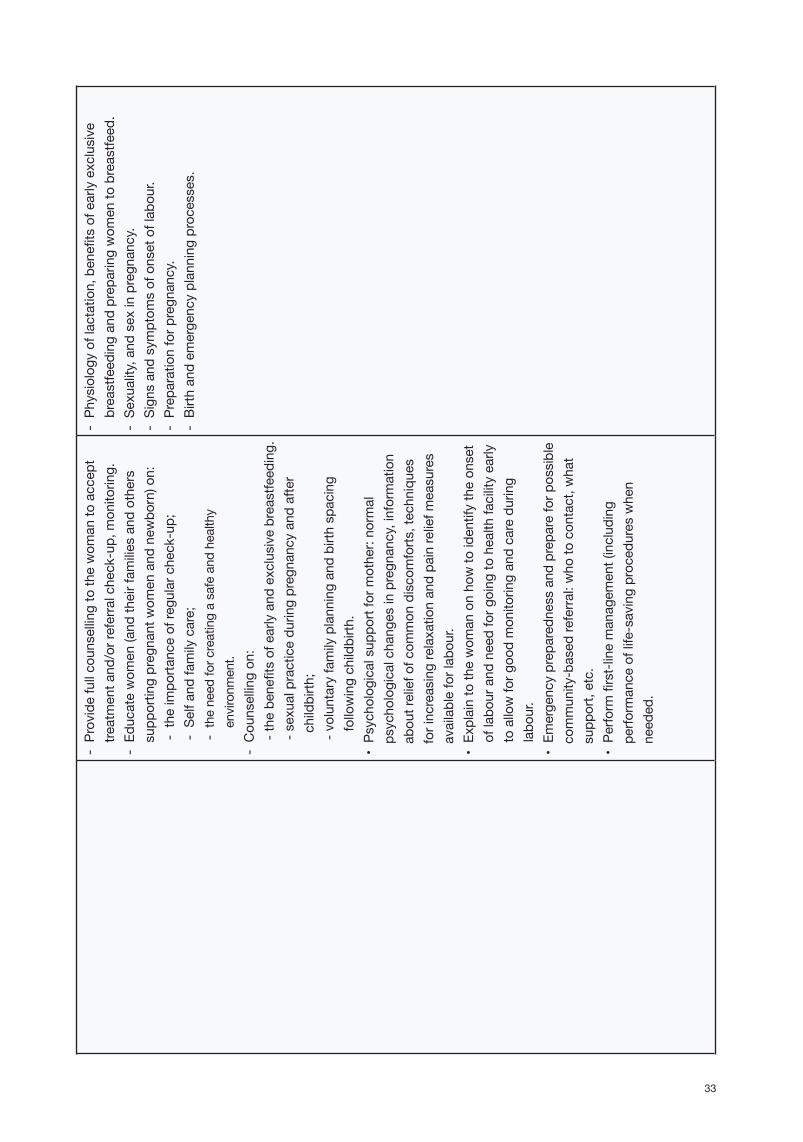
-Providefullcounsellin
gtoth
ewom
anto
accep
ttre
atmenta
nd/orreferralcheck-up,m
onitoring.
-Ed
ucatewom
en(and
theirfam
iliesandothers
supp
ortingpregnantwom
enand
new
born)on:
-th
eimpo
rtanceofre
gularc
heck-up;
-Selfand
familycare;
-
theneedfo
rcreatingasafeand
healthy
environm
ent.
-Cou
nsellingon
:-thebe
nefitsofearlyand
exclusivebreastfe
eding.
-sexualpracticedu
ringpregnancyandafter
childbirth
;-voluntaryfamilyplanningandbirth
spa
cing
followingchildbirth
.•Ps
ycho
logicalsup
portform
other:no
rmal
psycho
logicalchang
esinpregn
ancy,information
ab
outreliefo
fcom
mon
discomforts
,techniques
forincreasingrelaxationandpa
inre
liefm
easures
availableforlab
our.
•Ex
plaintoth
ewom
anonho
wto
identifytheon
set
oflabo
urand
needforg
oing
tohealthfacilityearly
toallowfo
rgoo
dmon
itoringandcareduring
labo
ur.
•Em
ergencyprep
ared
nessand
prepa
refo
rpossible
community-based
referra
l:who
tocon
tact,w
hat
supp
ort,etc.
•Pe
rform
first-linemanagem
ent(includ
ing
pe
rform
anceoflife-savingproced
ureswhen
need
ed.
-Ph
ysiologyoflactation,benefitsofearlyexclusive
breastfe
edingandprep
aringwom
ento
breastfe
ed.
-Se
xuality,and
sexinpregn
ancy.
-Sign
sandsymptom
sofonsetoflab
our.
-Prep
arationforp
regn
ancy.
-Birth
and
emergencyplanning
processes.
34
Com
pete
ncy
3 : P
rovi
de h
igh
qual
ity, c
ultu
rally
sen
sitiv
e ca
re d
urin
g la
bour
, con
duct
a c
lean
and
saf
e b
irth
and
han
dle
se
lect
ed e
mer
genc
y s
ituat
ions
to m
axim
ize
the
heal
th o
f wom
en a
nd th
eir n
ewbo
rns.
Cor
e fu
nctio
nsAt
titud
e, s
kill
and/
or a
bilit
y to
per
form
to
profi
cien
cy th
e co
re fu
nctio
ns:
Know
ledg
e re
quire
men
t to
perfo
rm s
kills
pr
ofici
ently
1.Id
entifytheon
seto
flab
our
2.Perform
vaginalexamination,ensuring
th
ewom
an’sprivacyandsafety,and
prope
rcon
ductbySB
A.3.M
onitorm
aternaland
fetalw
ell-b
eing
during
labo
ur.
4.Provide
sup
portivecare.
5.Recordmaternaland
foetalwell-b
eing
ona
partograp
h.6.Id
entifyde
layedprog
ressinlabo
urand
take
app
ropriateaction,includ
ingreferra
l.7.M
anageano
rmalvaginaldelivery.
8.Effe
ctivelymanagethethird
stageof
labo
ur,including
app
licationofAMTS
Lwhereapp
ropriateand
initiateearly
breastfe
eding,includ
ingskin-to
-skincontact.
•Provideculturallysensitivecareth
roug
houtth
efull
processoflabo
urand
birth;
•As
sessand
recordth
ewom
an’sgeneralstatus.
andcond
ition
:vitalsigns,p
hysicalcon
ditions,etc.
•Ex
plaintopregn
antw
omenth
estagesoflab
our,
thereason
sfora
ndprocedu
resforvaginal
exam
inationduringlabo
ur.
•Preparesterilizedequ
ipmentforvaginalexamination.
•Pe
rfomlimitedandtim
elyvaginalexaminations,
i.e,toredu
ceinfectionandrecordfind
ingson
pa
rtograp
horsimilarrecord.
•Pe
rform
acom
pleteandaccuratepelvic
exam
inationvaginallywithprivacyandrespect,
toassessford
ilatation,effa
cement,de
scent,
presentingpa
rt,position
,statusofm
embranes,
andad
equacyofp
elvisforb
irthofbab
yand
recordallfinding
onpa
rtograp
horsimilarrecord.
•Re
gulalrym
onitorp
rogressoflabo
ur:d
ilatation,
eff
acem
ent,etc.and
foetalheartrateand
record
allfind
ingsonpa
rtograp
horsimilarrecord.
•Providesupp
ortivecareduringlabo
ur:Instru
ction
on
how
tom
ove/lie,b
reathdu
ringlabo
urand
de
livery,ho
wto
relievepain,psycholog
ical
supp
ort,etc.
-Aimsandob
jectivesofcaredu
ringlabo
ur-An
atom
yofbirthcanal,includ
ingcervix,vaginaand
pe
lvicfloo
r.-Th
epe
lvis,landm
arksnoted
onpe
lvicexaminationand
po
ssiblecon
sequ
enceson
labo
uroutcomesfo
rdiffer
type
sandsizesofpelvis.
-Ph
ysiologyoflab
our(all3stages).
-Identificationandconseq
uencesofd
ifferentfoetal
po
sitionsinlabo
ur.
-Ph
ysiologicaland
psycholog
icalneedsofthewom
andu
ringlabo
urand
childbirth
,including
nutritionalneeds
andneed
forg
oodhydration.
-Managem
ento
flab
our(4stages).
-Be
nefitsanduseofpartograp
h.-Pa
inre
liefinlabo
ur.
-Im
pactonmaternaland
feoetalw
ellbeing
and
birthing
processofposture.
-Causes,signs,sym
ptom
sandmanagem
ento
fmaternaldistre
ssinlabo
ur.
-Causes,signs,sym
ptom
sandmanagem
ento
ffoetal
distre
ssinlabo
ur.
-Causes,signs,sym
ptom
sandmanagem
ento
fprolong
edlabo
ur.
35
•Providead
equatehydration,nutritionandno
n-ph
armacolog
icalcom
fortmeasuresdu
ringlabo
urandbirth
.•Providepa
inre
liefd
uringlabo
urand
birth.
•Allowcom
panion
ofcho
icedu
ringlabo
urand
birth.
•En
couragepo
sitionofcho
icedu
ringlabo
urand
birth
.•Manageinaccorda
ncewithnationalguide
lines
•Identifyde
layedprog
ressinlabo
ur,b
yusingthe
pa
rtograp
handclinicalsigns.
•Au
gmentu
terinecontractility,usingph
armacolog
icagents(inap
prop
riateb
irthsetting
s),according
tonationalguide
lines
•Ea
rlyidentificationofm
aternaland
foetaldistre
ssandtakeapp
ropriateaction,includ
ingreferra
lwherere
quired.
•Ke
epth
ewom
anand
herfamily/sup
porte
rregu
larlyupd
ated
abo
utth
estatusoflab
oura
ndplannedmanagem
ent.
•Ex
plaintofamilie
sfortheirsupp
ortersand
mob
ilizecommunity-fortimelyreferra
l.•As
sistnormaldeliveryaccordingtobestp
ractice
•Pe
rform
anep
isiotomytim
ely,ifindicated.
•Con
ductActiveManagem
ento
fthe3rdStageof
labo
ur(A
MTS
L),including
estimationand
recordingofm
aternalblood
loss.
•Pe
rform
fund
alm
assageto
stim
ulatepo
stpa
rtum
uterinecontraction.
•Pe
rform
urinecatheteriza
tionifindicated.
-Nationalprotocols,including
protocolsfo
rdealingwith
em
ergencysituations.
-Be
nefitsofusing
AMTS
L.-Clinicalindicationsfo
ruseofepisiotom
y.-Pe
rform
inganepisiotom
y.-Techniqu
esfo
rrep
airingpe
lviclacerationsand
ep
isiotomies.
-Causes,signs,sym
ptom
sandmanagem
ento
fimmed
iate/prim
arypo
st-partumhaemorrhage(PPP
H).
-Re
cogn
ition
and
managem
ento
fsho
ck,p
articularly
first-linelifesavingmeasures.
-Im
pactoflab
oura
ndbirthon
foetus.
-Ad
aptationofth
efoetusto
extra-uterinelife:includ
ing
causesand
signsofb
irthasph
yxiaand
hypotherm
ia.
-Managem
ento
femergencysituationsinth
enewbo
rnatbirth.
-Ex
aminationofth
eplacenta,cordandmem
branes
-Causes,signsand
managem
ento
fretainedplacenta
and/orm
embranes.

36
•MakeRa
pidAs
sessmenta
ndinstitute
managem
ento
fobstetricaland
new
born
em
ergenciesaccordingtonationalprotocols,
includ
ing:m
anagem
ento
fcordarou
ndth
eba
by’s
neckatb
irth,prolapsed
cordandseverem
aternal
andfoetaldistre
ss,eclam
psiaetc.
•Provideimmed
iateessentialcareofth
enewbo
rnatbirth
•Re
cogn
izesignsofasphyxiaatbirthandtake
immed
iateaction,includ
ingpe
rform
ingnewbo
rnresuscitationaccordingtobestp
ractices
10
•Initiateearlybreastfe
edinginclud
ingskin-to
-skin
contact
•Inspecttheplacentaandmem
branesfo
rcompleteness
•Inspectthevaginaandcervixfo
rlacerationsand
repa
ir1sta
nd2nd
degreepe
rinealorvaginal
lacerations
•Re
pairanepisiotom
y•Ed
ucatewom
anand
familie
stodetecte
arlysigns
ofhaemorrhagedu
ringthepo
spartumperiodand
whereto
seekassistance
•Pe
rform
firstlinemanagem
ento
fpostpartum
bleeding
and
haemorrhage,includ
ingusing
uteroton
icagentsandfund
alm
essage
•Re
cogn
izeand
respon
dtosho
ck,including
insertion
ofintraveno
usline,d
rawingbloo
dfor
labo
ratoryte
sts
•Pe
rform
cardio-pu
lmon
aryresuscitation
10Bestp
racticecallsfo
rallwho
provide
careforn
ewbo
rnatthetimeofbirthasm
inimum
mustb
eab
leto
accuratecond
ucta
rapidassessmentu
sing
APG
ARorsimilarscore,clearingofairw
ays,provide
ventilationbybagand
air,m
aintainbo
dyte
mpe
ratureduringproced
ureandprotectforharminclud
ingprotectionforinfection.

37
•Pe
rform
manualrem
ovalofp
lacenta,in
accordancewithnationalguide
lines.
•Pe
rform
internalbimanualcom
pression
ofthe
uterusto
con
trolsevereuterinebleeding
and
pe
rform
aorticcom
pression
ifindicated.
•Arrang
efora
ndund
ertaketimelyreferra
land
tra
nsfero
fwom
enwithseriouscom
plications
toahigherlevelhealthfacility,taking
app
ropriate
drug
sandeq
uipm
enta
ndaccom
panied
bya
healthprofessional.
Com
pete
ncy
4: P
rovi
de c
ompr
ehen
sive
, hig
h qu
ality
, cul
tura
lly s
ensi
tive
care
in p
ostp
artu
m p
erio
d
P
rovi
de h
igh
qual
ity, c
ultu
rally
sen
sitiv
e, p
ost a
borti
on c
are
Cor
e fu
nctio
nsAt
titud
e, s
kill
and/
or a
bilit
y to
per
form
to
profi
cien
cy th
e co
re fu
nctio
ns:
Know
ledg
e re
quire
men
t to
perfo
rm s
kills
pr
ofici
ently
4.1
Post
partu
m c
are
1.Id
entifyhaem
orrhageandpe
rform
m
anagem
entd
uringimmed
iatepostpartum
period.
2.Provide
postnatalcaretowom
en.
3.Id
entifyilln
essesandcond
ition
sde
trimental
to
thehealthofw
omeninth
epo
stnatal
period.
4.Provid
eadvic
eonpostpartumfamily
planning.
-Provide
culturallysensitivecareand
sup
port.
-Mon
itorc
ontra
ctionofth
euterus,p
ulse,b
lood
pressuretoearlydetecth
aemorrhagedu
ringthe
po
spartumperiod(atleastoncedu
ringfirst6
ho
ursafterd
elivery,firstdayafte
rdelivery,and
followingda
ysasneed
ed).
-As
sessfo
ruterineinvolutionandhealingof
lacerationsand
/orrep
airs.
-Pe
rform
postnatalscreening
testsaccordingto
nationalpolicy.
-Ed
ucatewom
anhow
tom
assageth
euterusto
keep
itwell-c
ontra
cted
.-Ex
plaintowom
anand
herfamilyabo
utlife-
threateningsituationsifth
eyarise,and
managem
entp
rocedu
res.
-Aimsandob
jectivesofp
ostnatalcare.
-Ph
ysiologicalchang
esinth
ebo
dyim
med
iatelyafte
rbirth
.-Ph
ysiologicalchang
esinpostpartumperiod:includ
ing
processofinvolutionandrecommencemento
fmenses.
-Managem
ento
fpostpartumperiod,includ
enational
protocolsforp
ostnatalcare.
-Riskfactorsinpostpartumperiod.
-Re
cogn
ition
and
managem
ento
fminordisorde
rsafte
rbirth
,including
breaste
ngorgement.
-Re
cogn
ition
and
managem
ento
fmajorcom
plications
afterb
irth,includ
inghaem
orrhage,sep
sis,deepvein
thrombo
sisandUTI.
-Useoflife-savingmed
icinesinth
epo
stnatalperiod.
38
-Provideed
ucationon
self-c
are,nutrition,personal
hygiene,breastfe
edingandsexualre
lations.
-Providessup
portforw
omenand
theirfam
ilies
who
arebereaved(stillbirth,pregn
ancyloss,
neon
ataldeath,con
genitalabn
ormalities).
-De
tectand
manageab
norm
alcon
ditionsin
thepo
stnatalperiod,includ
ingeclampsia,b
reast
complications,sep
sis,psycholog
icaldisorde
r,urinarytra
ctinfections,etc.
-Teachwom
enand
familie
son
earlydetectionof
ab
norm
alsignsofthewom
aninpostnatalperiod:
eclampsia,b
reastc
omplications,sep
sis,
psycho
logydisorde
r,urinarytra
ctinfectionsetc.
-Ad
minister,life-saving
med
icinesaccording
tonationalguide
lines(e.g.antibiotics,
anticon
vulsants,anti-m
alarials,anti-h
ypertensive,
anti-retro
viral).
-Makearrang
ementsfo
rtimelyreferra
land
app
lyfirst-linem
anagem
enta
spe
rnationalprotocols.
-Cou
nselcou
plesontheimpo
rtanceoffamily
planning
/birthspacingafterd
elivery,aswellas
ap
prop
riatecon
traceptivesth
atcanbeused
du
ringbreastfeed
ingpe
riod.
-Providefamilyplanningservicescon
curre
ntly,as
anintegralcom
ponentofp
ostpartumcare.
-Sign
s,sym
ptom
sandmanagem
ento
fphysiolog
ical
disordersafterb
irth,includ
ing“bab
y-blues”,p
ostnatal
de
pression
and
postnatalpsychosis.
-Establishm
enta
ndm
aintenanceoflactation.
-FamilyPlanningMetho
dsand
services,includ
ing
naturalm
etho
ds,L
actationalA
menorrhoeaMetho
d(LAM
).-Healthedu
cationforp
ostnatalwom
en.

39
4.2
Post
-abo
rtion
car
e1.Detectsignsofm
iscarriageandprovide
emergencymanagem
ent.
2.Provide
posta
bortion
familyplanning
cou
nsellingandservices.
-Diagno
sem
iscarriage.
-InsertIVline.
-Ac
compa
nyth
epa
tientto
thehealthfacility.
-Pe
rform
evacuationofre
tained
produ
ctsof
concep
tionaccordingtonationalguide
lines.
-Providepsycho
logicalsup
port.
-Providepo
st-abo
rtion
familyplanningcounseling
andserviceaccordingtonationalguide
lines.
-Aimsandob
jectivesofp
ost-a
bortion
care.
-Bleeding
inearlypregn
ancy,including
molar
pregnancy.
-Causesofearlypregn
ancyloss,including
hab
itual
ab
ortion.
-Re
cogn
ition
ofsignsofm
iscarriage(com
pleteand
incomplete)and
immed
iatelife-savingmeasures.
-Ec
topicpregnancy,includ
ingrecogn
ition
and
managem
ent.
-Ph
ysicaland
psycholog
icalim
pactofearlypregn
ancy
lo
ss.
-Managem
entp
rotocolsfo
rpost-a
bortion
care(PAC
).-Po
st-abo
rtion
cou
nselling.
-Po
st-abo
rtion
familyplanning.
-Pregnancyfollowingmiscarriage/earlypregn
ancyloss.
Com
pete
ncy
5 : P
rovi
de h
igh
qual
ity, c
ompr
ehen
sive
car
e fo
r the
hea
lthy
infa
nt fr
om b
irth
to tw
o m
onth
s of
age
Cor
e fu
nctio
nsAt
titud
e, s
kill
and/
or a
bilit
y to
per
form
to
profi
cien
cy th
e co
re fu
nctio
ns:
Know
ledg
e re
quire
men
t to
perfo
rm s
kills
pr
ofici
ently
1.Assessthenewbo
rnatb
irthandgive
im
mediatecare.
2.Identifyanylife
-threateningcond
itionsin
th
enewbo
rnand
give
essentiallife-saving
m
easures,includ
ing,wherenecessary,
active
resuscitationasacom
ponentofthe
m
anagem
ento
fbirthasph
yxia,and
referra
lw
hereapp
ropriate.
-Provideimmed
iatecaretoth
enewbo
rn,including
:drythenewbo
rn;p
laceinskin-to-skincontacto
nmother’sabd
omenorc
hestand
coverto
keep
bab
ywarm;suctioning
(ifn
eede
d);cordclam
ping
and
cuttingwhenpu
lsationceases.
-Takestepsto
preventinfection.
-As
sessth
eimmed
iatecon
ditionofth
enewbo
rn(e.g.,AP
GAR
scoringorra
pidassessment
metho
d:breathing
,colou
roftheskinandheartrate)
-Prom
oteandmaintainno
rmalnew
bornbod
y.
-Aimsandob
jectivesofn
ewbo
rncare.
-Ph
ysiologicalneedsofthenew
bornatb
irth.
-Be
nefitsofskin-to-skincontact.
-Th
ermoregulationprocessinnew
born.
-Ex
aminationofth
enewbo
rnatb
irth,includ
inguseof
AP
GAR
oro
therscoringsystem
.-Causes,re
cogn
ition
and
managem
ento
fasphyxiaat
birth
.-New
bornre
suscitationmetho
ds.
-Causes,re
cogn
ition
and
managem
enta
nd
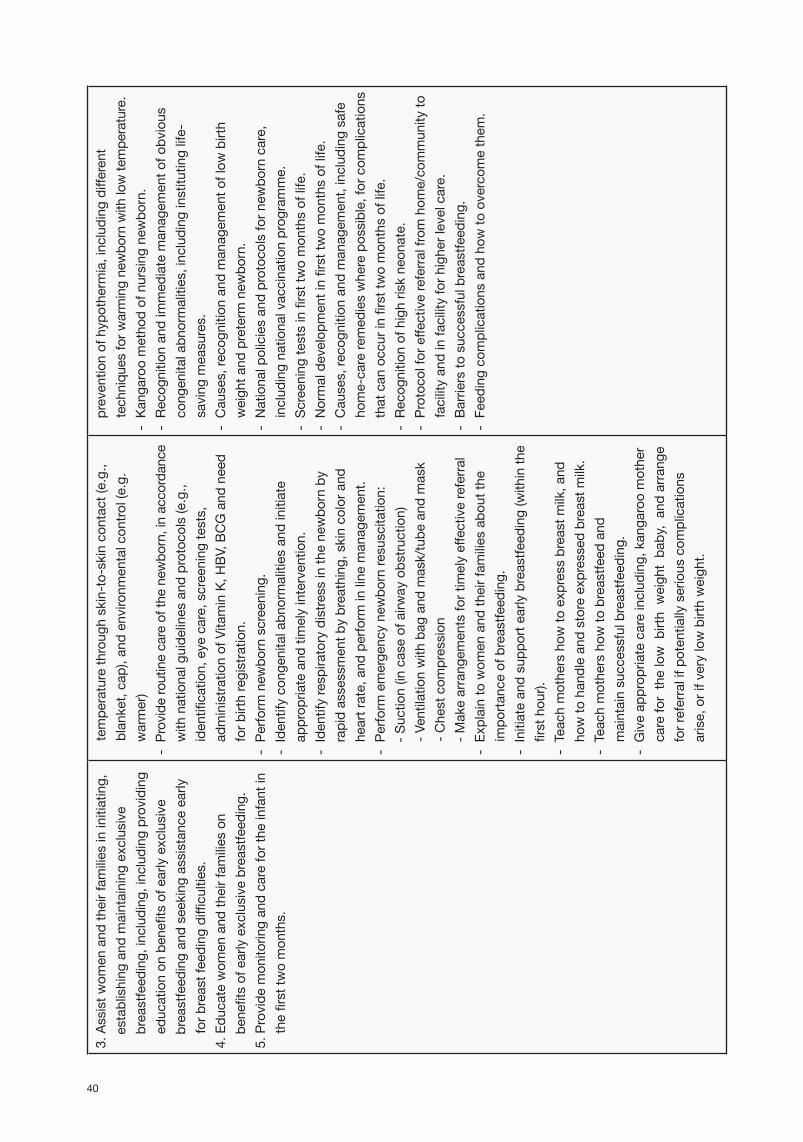
40
3.Assistw
omenand
theirfam
iliesininitiating,
establishing
and
maintaining
exclusive
breastfe
eding,includ
ing,includ
ingproviding
ed
ucationon
benefitsofearlyexclusive
breastfe
edingandseekingassistanceearly
fo
rbreastfeeding
difficulties.
4.Edu
catewom
enand
theirfam
ilieson
benefitsofearlyexclusivebreastfe
eding.
5.Provide
mon
itoringandcarefo
rtheinfantin
th
efirsttw
omon
ths.
tempe
ratureth
roug
hskin-to
-skincontact(e.g.,
blanket,cap),and
environm
entalcon
trol(e.g.
warmer)
-Provideroutinecareofthenew
born,inaccordance
withnationalguide
linesand
protocols(e.g.,
identification,eyecare,screening
tests,
ad
ministra
tionofVitaminK,H
BV,B
CGand
need
forb
irthregistration.
-Pe
rform
new
bornscreening
.-Identifycong
enitalabn
ormalitiesand
initiate
ap
prop
riateand
timelyintervention.
-Identifyrespiratorydistre
ssinth
enewbo
rnby
rapidassessmentb
ybreathing,skincolora
ndheartrate,and
perform
inlinem
anagem
ent.
-Pe
rform
emergencynewbo
rnre
suscitation:
-S
uction(incaseofairw
ayobstru
ction)
-V
entilationwithbagand
mask/tube
and
mask
-Chestcom
pression
-M
akearrang
ementsfo
rtimelyeff
ectivereferra
l-Ex
plaintowom
enand
theirfam
iliesab
outthe
impo
rtanceofbreastfe
eding.
-Initiateandsupp
orte
arlybreastfe
eding(withinth
efirsthou
r).-Teachmothershow
toexpressbreastm
ilk,and
ho
wto
handleandstoreexpressedbreastm
ilk.
-Teachmothershow
tobreastfe
edand
maintainsuccessfulbreastfe
eding.
-Giveap
prop
riatecareinclud
ing,kangaroomother
carefo
rthelowb
irthweigh
tba
by,andarrang
eforreferralifp
otentiallyseriouscom
plications
arise,orifverylowbirthweigh
t.
preventionofhypotherm
ia,including
different
techniqu
esfo
rwarmingnewbo
rnwithlowtemperature.
-Ka
ngaroo
metho
dofnursing
new
born.
-Re
cogn
ition
and
immed
iatem
anagem
ento
fobvious
cong
enitalabn
ormalities,including
institutinglife-
saving
measures.
-Causes,re
cogn
ition
and
managem
ento
flow
birth
weigh
tand
preterm
new
born.
-Nationalpoliciesandprotocolsforn
ewbo
rncare,
includ
ingnationalvaccinationprog
ramme.
-Sc
reeningtestsinfirsttwomon
thsoflife.
-Normaldevelop
mentinfirsttw
omon
thsoflife.
-Causes,re
cogn
ition
and
managem
ent,includ
ingsafe
ho
me-carere
med
ieswherepossible,fo
rcom
plications
thatcanoccurinfirsttwomon
thsoflife.
-Re
cogn
ition
ofh
ighriskneon
ate.
-Protocolfo
reffe
ctivereferra
lfromhom
e/communityto
facilityandinfacilityforh
igherlevelcare.
-Ba
rrierstosuccessfulbreastfe
eding.
-Feed
ingcomplicationsand
how
toovercom
ethem
.

41
-De
tectand
teachmothero
nearlydetectionof
ab
norm
alsignsofn
ewbo
rninpostnatalperiod:
eyes,com
plexions,d
igestion,umbilicalcord,etc.
-Re
cogn
izecom
plicationsinth
einfant,stabilize
andtra
nsferh
ighriskinfantto
emergencycare
facilityaccompa
nied
byhealthprofessionaland
mother.
-Makearrang
ementsfo
rtimelyeff
ectivereferra
l-Mon
itorthegrowthand
develop
mento
ftheinfant.
-Pe
rform
immuniza
tionaccordingtonational
immuniza
tionschedu
le.
Com
pete
ncy
6 : P
rovi
de h
igh
qual
ity, c
ultu
rally
sen
sitiv
e he
alth
edu
catio
n an
d se
rvic
es to
all
in th
e co
mm
unity
, in
orde
r to
prom
ote
heal
thy
fam
ily li
fe, p
lann
ed p
regn
anci
es a
nd p
ositi
ve p
aren
ting.
Cor
e fu
nctio
nsAt
titud
e, s
kill
and/
or a
bilit
y to
per
form
to
profi
cien
cy th
e co
re fu
nctio
ns:
Know
ledg
e re
quire
men
t to
perfo
rm s
kills
pr
ofici
ently
1.Edu
catewom
enand
theirfam
iliesonhow
topreventsexuallytransm
ittedinfections
includ
ingHIV.
2.Sup
ervis
enon-skille
dattend
ants,including
TBA
swhereth
eyexist,inordertoensure
thatth
ecareth
eyprovid
edu
ringpregnancy,
childbirth
and
earlypo
stpartu
mperiodisof
sound
quality.
3.Collect,analys
eandrepo
rtrelevantdataof
wom
enand
theirn
ewbo
rns
4.Promoteanethosofsharedrespon
sibility
and
partnershipwithindividu
alwom
en,
th
eirfam
ilym
embe
rsand
thecommunityfo
rth
ecareofw
omenand
new
bornsthroug
hout
pregn
ancy,childbirth
-Ed
ucateandcommunicatewithwom
enand
their
familie
son
thebe
nefitofregularcheck-up/
med
icalexamination.
-Ed
ucatewom
enand
theirfam
ilieson
riskfactors
ofsexuallytransm
itted
infectionsand
how
topreventsexuallytransm
itted
infections.
-Ed
ucatemem
bersofthecom
munityhow
to
recogn
izesexuallytransm
itted
infections/
reprod
uctivetra
ctinfectionsand
seekhealthcare.
-Ed
ucatefamilie
sandcommunitiesonda
ngersof
earlyte
enagepregnancies.
-Prom
otebe
nefitsofplanned
pregn
ancies.
-Identifybirth
atte
ndantswho
arenotyetSBA
s,includ
ingTB
Aswhereth
eyexist(num
bers,
workplace).
-Healthpromotiontechniqu
es.
-De
veloping
acom
munityprofile,includ
ing
identificationofsou
rcesofinformationandsupp
ortto
wom
enofrep
rodu
ctiveage.
-Makingcommunityplansfo
remergencyevacuationof
wom
enand
new
bornstoEmONCfacility.
-Vitalstatistics.
-Be
nefitsofbirthandde
athregistration.
-Protocolfo
rnotificationofm
aternalorn
eonataldeath
orstillbirth.
-Aff
ectingchange.
-Sk
illstraining
metho
dologies.
-De
veloping
training
plans.
-Workplanning
.-Re
cordkeeping
.

42
andthepo
stnatalperiod
-Workinpartnershipwithnon
-skilledattend
antsto
identifypregnantwom
enand
encou
rageth
emto
seekantenatalcare,safede
liveryandpo
stnatal
carewithskilledhealthprofessionals.
-Ed
ucateno
n-skille
dattend
antsonpracticesto
avoiddu
ringpregnancy,de
liveryandpo
stnatal
pe
riod.
-Collect,rep
ortd
ataon
am
onthly,quarte
rlyand
yearlybasis,asthenationalrep
ortinggu
idelines
dictate.
-An
alyzerelevantdataofwom
enand
their
newbo
rnsandsharefinding
swithcom
munities,to
prom
otego
odhealthcarepractice(evide
nce-
ba
sedpractices).
-Prom
otepa
rtnershipwithcolleaguestoprovide
high
qualitymaternaland
new
bornhealthcarein
healthfacilities:m
anageandprovide
comprehensivehealthcare,provide
ade
quate
inform
ationon
maternaland
new
borncare.
-Prom
otepa
rtnershipwithth
ecommunityto
providequ
alityevide
nce-ba
sedho
me-ba
sedcare
form
othersand
new
borns.
-Makearrang
ementsfo
rreferralsinclud
ingfor
em
ergencycare,etc.
-Healthedu
cationandprom
otiontofamilie
sand
communities,including
com
munitylead
ersand
influencersto
promotego
odm
aternaland
newbo
rnhealthpracticesand
services.
-Ad
vocacym
odels.
-Team
work.
-Creatinganhealthyworkenvironm
ent,includ
ing
healthand
safetyatwork.

43
Annex 3: Standard Classroom and Skills Lab RoomI. Classroom (for 15 - 20 trainees)1. General requirement: Area at least 2M2/participant2. Tools and equipment:
Item Unit Quantity
1 Table piece 252 Chair piece 303 Flipchartstand piece 24 Largewhiteboard piece 15 Television piece 16 VCD/DVDplayer piece 17 Multi-projector piece 18 Slideprojector piece 19 Projectorscreen piece 210 Videotapes,CD-Roms,DVDsforskillsdemonstration piece 1011 Desktopcomputerwithinternet piece 212 Laptopcomputer piece 213 Photocopier piece 114 FlipchartsizeAO piece 5015 Boardmarkers(3coloursofblue,red,black) piece 3016 Pens(various) piece 2017 Glassmarkers piece 1018 Whiteboardwiper piece 519 Transparencies box 220 Bookshelf/library piece 321 StandardguidelinesonRHservices22 Clinicalpracticeguideline23 Poster,flipchart set 524 Skillchecklist(sizeAO) piece 525 ReferencebooksonRH26 Scientificjournals,publications27 Airconditioner set 1
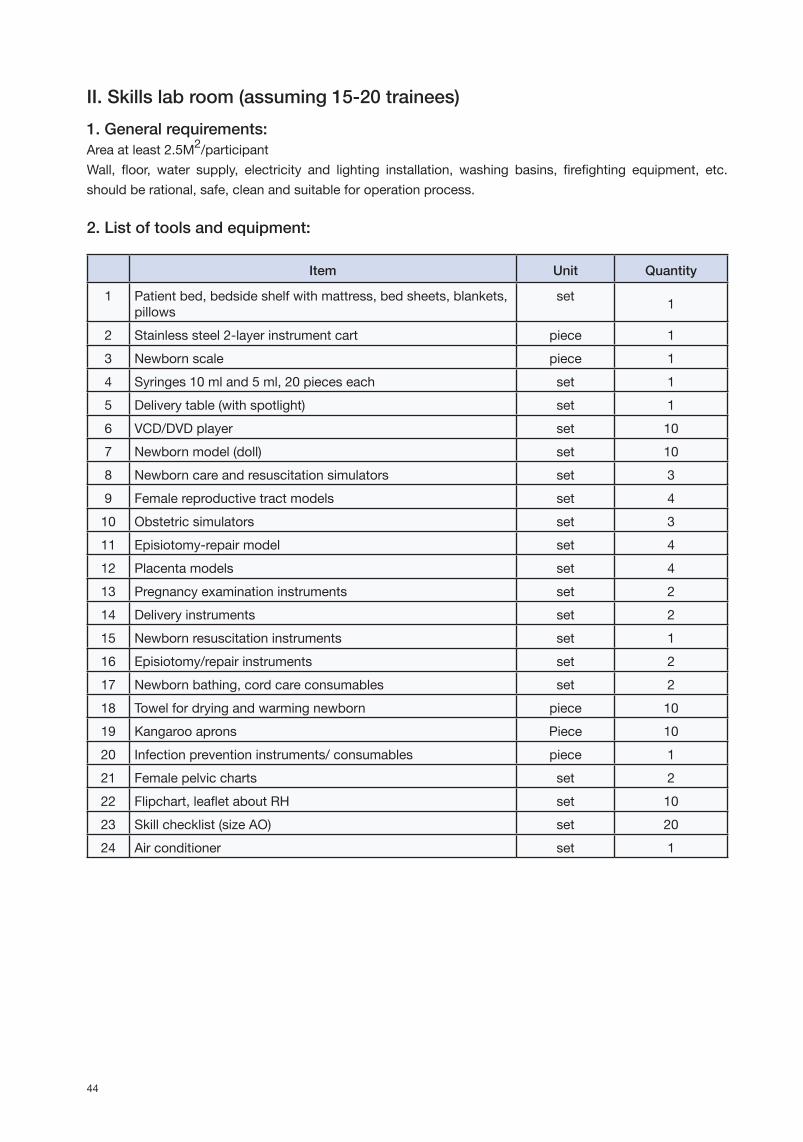
44
II. Skills lab room (assuming 15-20 trainees)1. General requirements:Areaatleast2.5M2/participantWall, floor, water supply, electricity and lighting installation, washing basins, firefighting equipment, etc.shouldberational,safe,cleanandsuitableforoperationprocess.
2. List of tools and equipment:
Item Unit Quantity
1 Patientbed,bedsideshelfwithmattress,bedsheets,blankets,pillows
set 1
2 Stainlesssteel2-layerinstrumentcart piece 13 Newbornscale piece 14 Syringes10mland5ml,20pieceseach set 15 Deliverytable(withspotlight) set 16 VCD/DVDplayer set 107 Newbornmodel(doll) set 108 Newborncareandresuscitationsimulators set 39 Femalereproductivetractmodels set 410 Obstetricsimulators set 311 Episiotomy-repairmodel set 412 Placentamodels set 413 Pregnancyexaminationinstruments set 214 Deliveryinstruments set 215 Newbornresuscitationinstruments set 116 Episiotomy/repairinstruments set 217 Newbornbathing,cordcareconsumables set 218 Towelfordryingandwarmingnewborn piece 1019 Kangarooaprons Piece 1020 Infectionpreventioninstruments/consumables piece 121 Femalepelviccharts set 222 Flipchart,leafletaboutRH set 1023 Skillchecklist(sizeAO) set 2024 Airconditioner set 1

www.asean.org





























