Embed Size (px)
Citation preview

Ascites of local cause
By: Assistant lecturer
Waleed Fouad

Definition
Ascites describes the condition of pathologic fluid accumulation within the abdominal cavity.
Healthy men have little or no intraperitoneal fluid, but women may normally have as much as 20 mL depending on the phase of the menstrual cycle.

Etiology
Normal peritoneum
Portal hypertension [SAAG] >1.1 g/dL)
Hepatic congestion
Congestive heart failure
Constrictive pericarditis
Tricuspid insufficiency
Budd-Chiari syndrome
Liver disease
Cirrhosis
Fulminant hepatic failure
Alcoholic hepatitis
Massive hepatic metastases

Etiology cont.
Normal peritoneum
Hypoalbuminemia (SAAG <1.1 g/dL)
Chylous ascites
Pancreatic ascites
Bile ascites
Urine ascites
Nephrotic syndrome
Protein-losing enteropathy
Miscellaneous conditions (SAAG <1.1 g/dL)
Ovarian disease Severe malnutrition with anasarca

Etiology cont.
Diseased peritoneum (SAAG <1.1 g/dL)
Infections
Peritoneal carcinomatosis
Primary mesothelioma
Pseudomyxoma peritonei
Bacterial peritonitis
TB peritonitis
Hepatocellular carcinoma
Fungal peritonitis
Malignant conditions
Chlamydia peritonitis
Alveolar hydatid disease
HIV-associated peritonitis
Strongyloidiasis
CMV

Etiology cont.
Eosinophilic peritonitis
Whipple's disease
Primary lymphatic hypoplasia
Endometriosis
Familial Mediterranean fever
Granulomatous peritonitis
Sarcoidosis
Rare conditions
Vasculitis

Grading of ascites
A grading system for ascites has been proposed by the International Ascites Club:
An older system that grades ascites from 1+ to 4+ is also used.
Grade 1Mild ascites
detectable only by ultrasound
Grade 2 Moderate ascites manifested
by moderate symmetrical distension of the abdomen
Grade 3Large or gross ascites
with marked abdominal distension
1+ is minimal and barely detectable
2+ is moderate3+ is massive but not tense
4+ is massive and tense

Diagnosis
The diagnosis of ascites is established with a combination of a physical examination and an imaging test (usually ultrasonography).
Abdominal paracentesis with appropriate ascetic fluid analysis is the most efficient way to confirm the presence of ascites and diagnose its cause.
Peritoneoscopy with culture and histology of a biopsied nodule is the most rapid route to the diagnosis.

Tests performed on ascitic fluid
Routine tests Optional tests Unusual tests
Cell count anddifferential
Albumin concentration
Total protein concentration
Culture in blood culture bottles
Glucose concentration
LDH concentration
Gram stain
Amylase concentration
Tuberculosis smear and culture
Cytology
Triglyceride Bilirubin
Adenosine deaminase CEA
PH & lactate
Cholesterol
Fibronectin

Tuberculous Peritonitis
Tuberculous peritonitis should be considered in all patients presenting with unexplained lymphocytic ascites with a serum-ascites albumin gradient of <1.1 g/dL.
The gold-standard for diagnosis is culture growth of Mycobacterium on ascetic fluid or a peritoneal biopsy.

Tuberculous Peritonitis cont.
Other Tests
Routine laboratory tests Normocytic normochromic anemia in 50 %
Tuberculin skin testing Positive in 70 % of patients
Chest x-ray Old tuberculosis in 20 to 30 %
US & CT Peritoneal thickening, omental caking and /or ascites with fine mobile septations.

Peritoneal fluid analysis
Ascitic leukocyte count
150 to 4000 mm3
+
Lymphocytic Pleocytosis
> 50%
Albumin content
Useful in differentiating
tuberculous ascites from
carcinomatous ascites
SAAG <1.1
Sensitivity of 0 to 6 %
Direct smear for Ziehl-Neelson
stain
>3.0 g/dL
>1.1
PCR
Underlying cirrhosis
If
ADA
Rapid detection

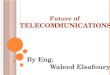
Multiple miliary nodules
over the peritoneum with an
adhesion band attached
to anterior surface
of liver capsule.

Malignant ascites
• It occurs most often with ovarian cancer in about one-third of women at the time of diagnosis.
• It is also associated with a variety of other primary cancer sites: Stomach, Liver, Uterus, Testis, Breast, Pancreas, Colon, Lymphoma, Mesothelium, Lung, Unknown primary site.

In the presence of malignant cytologic findings without a primary tumor diagnosis, further investigations of male patients may not lead to improved survival, since all primary tumour groups are associated with a uniformly poor prognosis.
Female patients may benefit from further investigations, possibly including lapa roscopy or even laparotomy, since ovarian cancer is treatable.

Serum tumour markers
Peritoneal nodules, omental caking and 1ry tumour site.
US & CT
CEA - CA125 – α feto protein
Peritoneal fluid analysis
Albumin content
>3.0 g/dL
Ascetic WBCs
Lymphocytic Pleocytosis
> 50%
Other tests
α1-antitrypsin Cyclic AMP
Cholesterol Fibronectin
GlycosaminoglycansSAAG <1.1

Cytology
Gold standardMalignancies can produce ascites
without shedding many neoplastic cells
Diagnostic sensitivity of only 40% to 60%.
Immunohistochemical staining can increase the diagnostic sensitivity
Laparoscopy
Used with caution in patients with malignant ascites
High risk for trocar implantation metastasis

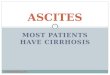
Positron Emission Tomography- CT scan shows peritoneal nodule characterized by abnormally high radiotracer uptake.
Positron emission tomography (PET) is a nuclear medicine medical imaging technique which produces a three-dimensional image or map of functional processes in the body.

• Axial intravenous contrast-enhanced abdominal CT scan shows tiny nodules in the gastrohepatic ligament (short arrows) and in the inferior portion of the falciform ligament (long arrow).

• Axial intravenous contrast-enhanced abdominal CT scan shows nodules in the lesser sac (arrows).

• Close-up view showing peritoneal implants, as well as abnormal feeding blood vessels.
• Laparoscopy demonstrated obvious diffuse carcinomatosis, with implants on all peritoneal surfaces.

Chylous ascites
Chylous ascites is a milky-appearing peritoneal fluid
Abdominal malignancy and cirrhosis
Two-thirds of all cases
Other etiologies
Infections
Primary lymphatic Hypo or hyperplasia
Filariasis
TB
Congenital Inflammatory Post-operative
yellow-nail syndrome Radiation therapy
Sarcoidosis Lymphatic injury or
compression
Malignancy particularly Lymphoma is a common cause.

CT
Can identify pathologic intra abdominal lymph nodes and masses
Lymphangiography & lymphoscintigraphy
Abnormal retroperitoneal nodes, leakage from dilated lymphatics, fistulization, and patency of the thoracic duct
Triglyceride values are typically above 200 mg/dL

PANCREATIC ASCITES Massive accumulation of pancreatic
fluid in the peritoneal cavity
The most common underlying cause is chronic pancreatitis secondary to alcohol abuse.
Following an episode of acute pancreatitis or a traumatic injury to the pancreas.
Also has been described with pancreatic pseudocysts.

US & CT Can detect the presence of a pseudocyst
Accurately demonstrate the normal pancreatic duct and detect any abnormalities arising from itMRCP
ERCP Localize the site of leakage and endoscopic therapy if possible
Peritoneal fluid analysis
SAAG <1.1
Albumin content
>3.0 g/dL
Ascitic amylase
> 1,000 IU/L
Elevated Ascitic WBCs
Ascitic/serum amylase
ratio is 6.0

Ascites due to more than 1 cause
Approximately 5 percent of patients with ascites have more than one cause, such as cirrhosis plus Tuberculous peritonitis, peritoneal carcinomatosis or heart failure.
Patients with more than one cause for ascites formation tend to be the most confusing to diagnose because each partial cause may not be severe enough to lead to fluid retention by itself.

THANK YOU