Embed Size (px)
Citation preview

Use of Population-Based Databases in Comparative
Effectiveness Research (CER)
Siran M. Koroukian, Ph.D.Department of Epidemiology and Biostatistics
Population Health and Outcomes Research Core
December 14, 2012

As noted by Gary H. Lyman (JCO, 2012)“CER is an important framework for systematically identifying and summarizing the totality of evidence on the effectiveness, safety, and value of competing strategies to inform patients, providers, and policy makers, and to provide valid recommendations on the management of patients with cancer.”

CER
Randomized Controlled
Trials
Observational Studies
Systematic Review of
the literature
Population-based databases
Various Methods to Conduct CER

Randomized Controlled Trials (RCTs)
Considered the “gold standard”, providing the least biased estimates for CER› Consider, however,
provide data on efficacy or outcomes in controlled setting rather than in ‘real world’ settings
RCTs not always feasible or ethically acceptable (rare conditions, vulnerable populations)

Observational studies in CER Fill evidence gaps in CER Provide outcomes data in ‘real world’
settings effectiveness Ability to study rare conditions and/or
outcomes in vulnerable populations and to compare a number of treatment alternatives
POPULATION-BASED DATABASES› Large number of subjects at an affordable cost› Longer periods of follow-up
Examine long term risks and benefits

Examples of population-based databases
Enrollment and claims data:› Medicaid (poor, aged, disabled)› Medicare (aged, disabled)› Veterans Administration (military)› Private insurance
Linked databases:› Surveillance, Epidemiology and End-Results (SEER) and
Medicare files› The Ohio Cancer Aging Linked Database (CALD),
consisting of data from the Ohio Cancer Incidence Surveillance System, Medicare, Medicaid, and clinical assessment data from home health and nursing home care
› The linked Health and Retirement Study and Medicare data

Enrollment and claims data Enrollment data:
› Demographics› Eligibility category(ies)› In the context of the Medicaid program,
Length of enrollment Gaps in enrollment Area of residence
Ability to link to contextual variables (availability of health care resources)
Claims data:› Dates of service› Diagnosis codes› Procedure codes› Prescription drugs › Charge/cost data

Advantages of enrollment and claims data
Capture all treatment modalities covered by the program, and the associated charges/costs to the program
Identify subgroups of the population receiving certain treatment modalities
Ability to follow-up long term to monitor certain outcomes› Morbidity (complications)› Mortality › Readmissions› Costs

Limitations of population-based administrative databases
Completeness/accuracy of administrative data (flu vaccine, digital rectal exam)
Limited ability to describe a patient’s clinical presentation cross-sectionally, or longitudinally› Lack of disease-specific data (e.g., cancer
stage; recurrence)› Lack of data on health and functional status,
and/or on geriatric syndromes (e.g., cognitive status, depressive symptoms) use linked databases

Limitations of population-based administrative databases
Difficult to adjust for selection bias› For example, systematic differences in the
way physicians prescribe (newer treatment to more severe cases)
Use of statistical techniques such as propensity scores or instrumental variables to address bias

Example of a CER study using large databases
Comparative assessment of the safety and effectiveness of
radiofrequency ablation among elderly Medicare beneficiaries with hepatocellular carcinoma
Massarweh et al. Ann Surg Oncol, 2012; 19:1058-
1065

Background Radiofrequency ablation (RFA) use
among patients with hepatocellular carcinoma (HCC) has increased over the last decade.
Although RFA is widely perceived as safe and effective, this has not been rigorously evaluated using population-based data.
Assessments outside specialized centers are lacking.

Study objective
Evaluate the safety and effectiveness of RFA when used to treat HCC.
Methods Data Source: Linked SEER-Medicare data
(2002-2005) Outcomes:
› 30- and 90-day mortality› Readmission› Survival
Comparison groups (treatment modalities identified based on procedure codes documented in claims data):› Resection› RFA› No treatment

Analytic approach
Multivariate and propensity score adjusted regression models.› Propensity score calculation included liver-
related comorbid conditions (e.g., ascites, hepatitis B/C, GI bleed, cirrhotic liver)

Results 2,631 patients; demographics and
comorbidities:› Average age: 76.1 ± 6.1 years› 65.9% male› 67.9% white› 68.5% having a Charlson score ≥ 1
Treatment modalities:› 84.2% untreated› RFA: 7.8% › Resection: 7.9%
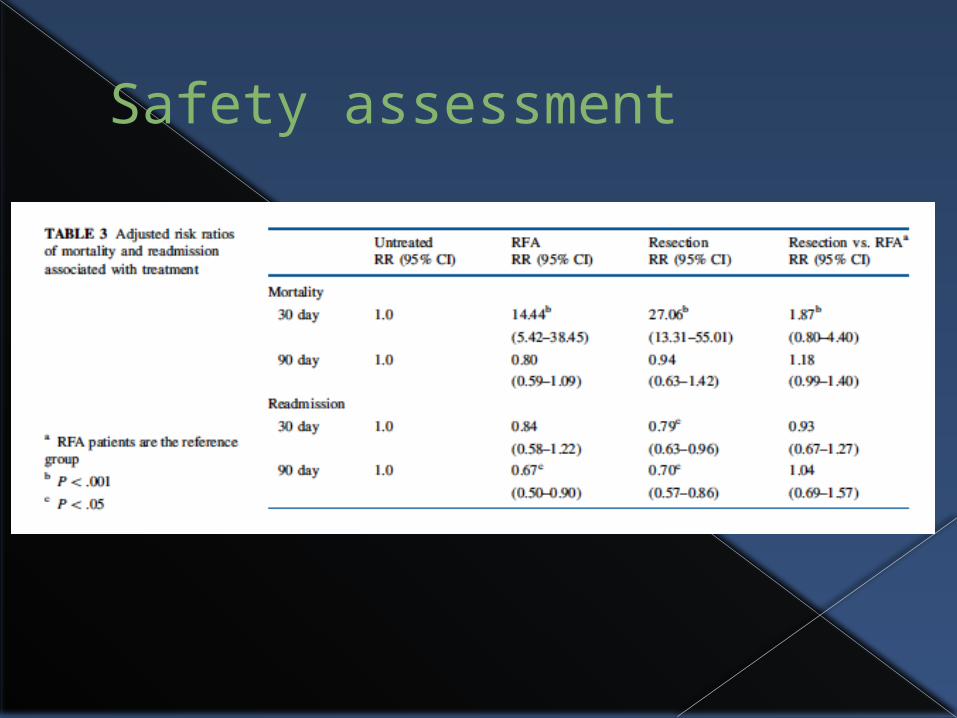
Safety assessment

Effectiveness assessment
Between RFA and resection:› 1-year survival: 72.2% vs. 79.7%, p=0.18› 3-year survival: 39.2% vs. 58.0%, p < 0.001› 5-year survival: 34.8% vs. 50.2%, p < 0.001
Multivariable results:› RFA (single session or multiple sessions) vs.
no treatment: no diff within 1 year› Resection vs. RFA or no treatment: 50-75%
decreased hazard of death

Conclusions
RFA vs. Resection: early adverse events not significantly lower in patients treated with RFA
RFA vs. no treatment: no obvious benefits in the 1-year survival
[There may be some survival benefits in certain subgroups of
patients who have not yet been well characterized..]

Study limitations
Residual confounding, despite the use of propensity scores.
Lack of pertinent clinical data to quantify surgical risk (e.g., lab data, anesthetic factors), or other clinical variables impacting surgical decision-making and patient selection.













![Bapi jco[1]](https://img.pdfslide.us/doc/110x75/55587609d8b42aaa7e8b5447/bapi-jco1.jpg)