Embed Size (px)
Citation preview

Artificial Neural Nets in Computer-Aided Macro Motor Unit Pot en tial Classification
he electrical activity of muscle has been extensively studied since the T beginning of the century. The rapid
technological developments of succeed- ing years have permitted precise measure- ment of the properties of individual muscle fibers and the functional groups that constitute the motor unit. A motor unit consists of 2 to 1000 fibers
innervated by one motor nerve axon and hence the fibers discharge synchronously at rates typically between 2 and 30 Hz. A variety of techniques have been used to measure the motor unit potential (MUP), such as macro electromyography (EMG) introduced by Stalberg [ l ] in 1980. The macro EMG method uses a special needle electrode with a 15mm long by 0.8mm diameter cannula, with a 25pm diameter side port electrode 7.5mm from the tip.
SYSTEM
auIc I e I
Christos N. Schizas*, Constantinos S. Pattichis', Ian S. Schofieid',
Peter R. Fawcett', and Lefkos T. Middleton* *MDRTC Neuromuscular Unit
Makorios Hospitol, Nicosia, Cyprus t Deportment of Clinical Neurophysiology
Newcastle General Hospital, Newcastle Upon Tyne, U.K.
The side port electrode records the activity of one or more single muscle fibers from an individual motor unit recruited by gentle voluntary contraction of the muscle. The single fiber action potentials (SFAP) are used to trigger a signal averager into which the cannula signal is
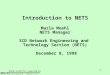
fed (Fig. 1). In general, about 200 dischar- ges of the unit are averaged over an 80 ms sweep time to obtain a macro motor unit potential (MMUP). At least 20 potentials are measured from a single muscle to ob- tain a reasonable es t imate of the parameters of an average motor unit potential.
The MMUP data is analyzed by means of the peak-to-peak amplitude and the in- tegral of the central 50 milliseconds of the signal. An additional parameter to es- timate the duration of the potential has been introduced [ 2 ] , which is the 90 per- cent power duration. This is the width of the region of the potential that contains 90% of the power. Normal ranges for the amplitude and area by age decade have been obtained by Stalberg and Fawcett [3]. Following extensive simulation
lOms
HRCRO MUP
-HORIIRL
. MOTOR HEUROH D I SERSE
-DECKERS MUSCULflR DYSTROPHY
MUSCULAR RTROPHY
, S P l N R L
I W I I I
Chl - Filters 500 Hz to 8KHz Ch2- Filters 8Hz to 8KHz D - Delay 4Oms
1. An integrated system approach for computer aided macro electromyography.
SEPTEMBER 1990 ~~~ ~
IEEE ENGINEERING IN MEDICINE AND BIOLOGY 31

7
1400 -
9 1062 - W
3 b- A -
5 726 -
17
16 Y
17 1 I
20
2. A macro MUP study of an MND patient. Short vertical lines across each macro MUP show the duration beginning and ending points.
studies [4], the amplitude and area were found to be highly correlated and propor- tional to the "size" (number of fibers) of the motor unit. The duration parameter remains to be studied adequately but ini- tial indications are that this relates to the range of muscle fiber diameters and the geometric width of the end-plate zone of the motor unit.
Of the large number of neuromuscular disorders that have been identified, three have been selected for this study as their consistency of clinical appearance is good. These are motor neuron disease (MND), Becker muscular dystrophy (BMD), and spinal muscular atrophy (SMA). MND and SMA are both as- sociated with neurogenic processes, either rapidly progressive and affecting an older population, as in MND; or more chronic and affecting a younger population, as in SMA. In both disorders, loss of motor neurons occurs followed by reinnervation of the muscle fibers by surviving neurons such that the size of the motor unit in- creases with a concomitant increase in the macro MUP amplitude. In contrast, BMD is a myopathic process where the total number of motor units remains constant, but the size of each unit falls due to loss of individual fibers. In this case the amplitude of the macro MUP is rather low.
To date, standard statistical procedures have been used to classify the results of a macro EMG study [3], limited to the clas- sification between normal and abnormal cases. Cluster analysis has been applied in the classification of normal, MND, BMD and SMA subjects [ 2 ] using macro EMG data, but produced only a relatively poor
0 0
0
0
3.3D plot of mean average power, mean duration and mean area for each subject.
32 IEEE ENGINEERING IN MEDICINE AND BIOLOGY
.~
SEPTEMBER 1990

diagnostic yield. This result is due to the fact that the cluster boundaries identifying each group overlap. Recent developments in the field of artificial neural networks (ANN) have raised the possibility of using these powerful artificial intelligence methods to analyze the macro data in a way that makes no assumptions on the relationships between the parameters and without recourse to conventional model- ing methods. It is believed that the ap- plication of ANNs opens a new era for the solution of problems of this nature for which other methods of classification failed to offer any conclusive results. Preliminary findings on the application of ANNs in EMG [5,6] have demonstrated the capacity of ANN models. The purpose of this study was to investigate further the use of a variety of network topologies and to examine methods of structuring the input data to classify macro EMG data. An integrated model for computer aided electromyography and automatic diag- nosis is suggested in Fig. 1. A number of ANN algorithms and mod-
els have been published in the literature, both for continuous and binary data. The back propagation training algorithm [7] for a continuous input has been applied on a three layer ANN model (Fig. 1). Models with two hidden layers have been docu- mented to be able to draw the boundaries of arbitrarily complex decision regions [8]. Ed. note:What Lippman calls a “3- layer” net is one with two hidden layers. What is used here is a net with one hidden layer, if you believe Fig. 1. Figs. 4-7, and Tables 3 and 4, however, reflect nets with two hidden layers. MethodMacro MUP data were collected
at the Department of Clinical Neuro- physiology of Newcastle General Hospi- tal. Twenty MMUPs from each patient were recorded from the biceps brachii muscle, at slight voluntary contraction (Fig. 2 and Table 1). The shape features extracted from each MMUP were: amplitude (the difference between the minimum positive peak and the maximum negative peak); area (the sum of the rec- tified signal integrated over the 50 ms analyzed epoch); average power (the sum of squares of each sample over the 50 ms epoch, divided by the number of samples); and duration (the segment of the macro MUP which contains 90 percent of the power).
The above analysis has been carried out on 820 MMUPs recorded from 4 1 subjects (Table 2) who were classified on the basis of a clinical opinion and the appearance of a muscle biopsy. For illustrating the com- plexity and high degree of overlapping among the groups, three of the parameters, mean amplitude, mean of the average power, and mean duration for each patient have been plotted as shown in Fig. 3 . Previous studies have shown that MMUPs of MND patients have high amplitude,
No Amp %V
1 1430
2 1449
3 1054
4 1898
5 848
TABLE 1
Area %V
3225
4564
4986
7481
3233
Macro MUP Parameters of an MND Patient (Macro MUP waveforms shown in Fig. 2)
Average Power %Vms
Duration rns
6 1632 131 90
3258
I I
11.61
10 I566 13048
10182
12 11012 13399
10.56
I 2097
13 I647 I2320
11.84
810
4633
1493
795
17 1836 14233
13.44
12.1 6
13.1 2
12.48
19 1 1 6 1 8 15577
14
15
16
I
1351 5109
619 3440
598 2474
1796
1352
4805
2398
15.68
27.52
1 1.20
13.12 20
13.44
831 4322
11 .84
1 1.20 7 15.68
2727 I 14.72
71 75 111.84
1009 I 6.00
1982 113.12
SEPTEMBER 1990 IEEE ENGINEERING I N MEDICINE AND BIOLOGY 33

4. Learning curves for the 8-input models 1 to 5 of Table 3.
19-46
27-59
__
17-63
3
Y 9
140
180
280
5. Learning curves for the 8-input models 6 to 12 of Table 3.
area and power, and short duration, whereas BMD patients should be charac- terized by MMUPs with small amplitude, area and power, and a not well defined duration range. Macro MUP findings for the SMA group are highly intermixed with the other groups, as a result of the heterogeneous nature of this disease.
ANN Models and Results We have previously described our method of analysing data in two different ways, based on how the input of the ANN in each case was chosen, in an 8-input vector and an 80-input vector [SI. In the case of the 8-input vector, the descriptive statistics, i.e., the mean value and the standard deviation of the parameters (amplitude, area, average power and duration) of all MMUPs collected from each subject
Group
Normal
Motor Neuron Dis- ease
Becker's Muscular Distrophy
Spinal Muscular Dis- trophy
formed the input set, as shown in Table 3. In the 80-input vector models the values of the individual parameters for each MMUP formed the input as shown in Table 4.
Training and evaluation of the nets was conducted in accordance with two dif- ferent protocols; in the first protocol, 20 subjects were randomly selected to form the training set and 21 formed the evalua- tion set. In the second protocol, 31 sub- jects formed the training set and 10 the evaluation, also at random (Table 3 and 4). In our previous study, logarithmic trans- formation of the parameters amplitude, area, and average power was adopted be- cause of the wide range of the observed values [SI. In the present study, log trans- formations of these parameters was only performed in certain models, but the ac- tual values of all parameters were used in most models. Surprisingly, a better diag- nostic yield was obtained using the actual values in spite of their large variability. In each of the four groups, subjects were
further subdivided into subgroups. A total of sixteen subgroups were formed for models 4 and 17, as shown in Table 3 (3 subgroups for normals, 4 for MND, 3 for BMD and 6 for SMA). Eight subgroups were formed for model 5 of Table 3 (1 for normal, 2 for MND, 2 for BMD and 3 for SMA). This subdivision was considered to be more representative because of the s ignif icant variabil i ty of electrophysiological characteristics in neuromuscular diseases. The order of placement of the parameters
to form the input vector was of no signifi- cance in the 8-input models, as MMUP parameters were represented by their de- scriptive statistics. In contrast, in the 80- input models, the input vector was constructed by the values of the individual parameters for each MMUP. Thus, struc- turing the input vector proved a more dif- ficult task. Two approaches were adopted: in models 1,2, 3, S and 8 of Table 4, the input vector was constructed by collecting
TABLE 2: Cases Under Study
----I-- No. of Subjects 1 Age Range 1 No. of Macro MUPs
7
9
14
11 21 -72
34 IEEE ENGINEERING I N MEDICINE AND BIOLOGY SEPTEMBER 1990

the parameter values of all 20 MMUPs for each patient and placing them in the order they have been recorded ([Amplitude, Area, Average Power, Duration] x 20); in models 4, 6 and 7 of Table 4 the input vector was constructed by collecting the features of all 20 MMUPs and placing them in an ascending order ( [Ampli tude 1 ,. .. Amplitude201, [ A r e a l ,.. .Area20] , [Average Power1 ,...Average Power201, [Dura- t i o n l ,... Duration201). Placing the parameter values in an ascending order was shown to enhance the diagnostic yield.
Some of the problems and limitations encountered with the back propagation algorithm are related to the lack of tools for determining an optimum architecture, gain and momentum. In addition, these parameters depend on the nature, distribu- tion and complexity of the input data. The momentum value chosen for all models under study was 0.9. The gain had a high- est value of 0.01 and a lowest value of 0.001. Learning curves for all the models investigated are shown in Figs. 4 , 5 and 6 for the 8-input model, and in Fig. 7 for the 80-input. The total sum of squares (TSS) has been plotted against epochs; TSS is the sum of the squared difference between desired and actual output for each subject, summed over all subjects in one epoch. TSS is a measure of convergence; thus, learning of the training set is achieved when TSS approaches zero. For making sure that the ANN did not learn the sub- jects in any particular order, the sequence of presenting the subjects at the input was randomly selected at every epoch.
Discussion The effect of certain factors on the diag- nostic yield and ways of improving the reliability of ANN systems were ad- dressed in this study. Such factors in- cluded structuring of the input data, architecture of the ANN, gain, number of outputs, and size of training and evalua- tion sets. Because of the number of these factors and of all possible combinations, examining all possibilities would have been a very time consuming and computa- tionally heavy exercise. In this study, we heuristically se1ected.a total of 26 models.
In the case of the 8-input models, useful information that would have helped the algorithm to converge was lost, because the data was limited to descriptive statis- tics. This may explain why the 8-input models required more epochs than the 80- input models to converge. The compara- tively larger number of weights in the 80-input ANNs increases the degrees of freedom of the ANN, thus allowing them to learn the subjects as individual cases, rather than members of groups. However, there was a performance decrement, as illustrated by the finding of an overall slightly higher diagnostic yield of 60 per-
SEPTMBER 1990
TSS 0-
% 24 20 16 12 8 4
0
6. Learning curves for the 8-input models 13 to 18 of Table 3.
TS 32 28 24 20 16 12 8 4
0
7. Learning curves for the IO-input models 1 to 8 of Table 4.
cent for the 8-input models compared to 55 percent for the 80-input models. To examine how the relative sizes of the
training and evaluation sets affect the diagnostic yield, the division of the avail- able data into training and evaluation sets was carried out in two different ways (20/21 and 31/10). The diagnostic yield was improved with the larger training set, resulting in 5 1 percent diagnostic yield for all 20/21 models and 63 percent for all 3 1/10 models. However, in addition to the increase in the training set size, other fac- tors varied at the same time, such as ar- chitecture, gain, and number of outputs. Nonetheless, the effect of training set size does suggest that generalization is occur- ing within the net but much larger data sets are required to confirm this.
Log transformation of data is common when human interpretation of complex data is carried out through plotting, tabulating etc. The results obtained indi- cate that ANNs do not require such a transformation. The following example demonstrates the wide range of the MMUP parameters for a patient in the SMA group which could have justified a log transformation: the minimum and maximum amplitude, average power, duration and area ranges were 28:1363, 8:12316, 5.6:16.4, 222:4265, respective- ly. ANN models were shown, however, to be capable of handling real data with such ranges successfully without the need of log transformation.
The division of the four groups into subgroups, or output nodes, was con-
IEEE ENGINEERING IN MEDICINE AND BIOLOGY 35

TABLE 3: Eight-input Architectures and Results
Model Inputs L1 L2 Outputs Gain Epochs TSS
I
1 8a 16 32 4 0 005 3500 1 65
2 81 16 32 4 0 005 10000 1 55
40 4 0 001 61 59 0 89 i?lb 40 16 0 005 20000 1 49
8a 20 40 8 0 005 20000 2 94
6 81 20 60 4 0 005 10000 0 02
I
-~
7 181 25 75 4 0 005 7000 0 04
8 8a 25 75 0 005 2400 ‘ 0 48 1 4
9 81 20 60 4 0 005 25000 1 42
10 181 25 75 4 0 005 1 1000 0 64
11 81 25 75 3 0 001 15000 1 30
60 120 4 0 005 5000 0 24
40 120 0 005 1150 0 49 l 4
Y 13 I 8a
14 8a 40 120 4 0 005 17000 4 10
15 81 40 120 4 0 001 17000 0 89
16 8a 40 120 4 0 001 5605 0 89
17 8a 40 120 16 0 005 10000 1 1 0
18 8a 60 180 4 0 001 7740 0 82
Momentum: 0.9 L1: number of units in the first hidden layer L2: number of units in the second hidden layer TS: Training Set ES: Evaluation Set TSS: Total Sum of Squares I: logarithmic a: actual
S U b j e c t s Diagnostic (TSIES) Yield %
(ESITS)
20121 52/95
20121 45/95
31110 7011 00
31110 70197
3111 0 60194
20121 5011 00
20121 6011 00
20121 4311 00
31110 50190
31/10 7011 00
2317 57196
20 21 6211 00
20121 4811 00
20121 57185
31/10 5011 00
31110 7011 00
31/10 8011 00
31/10 8011 00
36 IEEE ENGINEERING I N MEDICINE AND BIOLOGY SEPTEMBER 1990

Eighty-input Architectures and Results
S U b j e c t s (TSIES)
Model Inputs L1 L2 Outputs Gain Epochs TSS
1 80pl 120 240 4 0.005 160 0.10 20121
3 80pl 160 80 4 0.005 110 0.60 20121
3 80pa 160 80 4 0.005 110 0.60 20121
4 80sa 100 120 4 0.005 750 0.89 31/10
5 80pa 160 240 4 0.005 400 0.71 31/10
6 80sa 100 120 8 0.005 534 0.89 31/10
7 80sa 100 120 4 0.001 1055 0.89 31/10
8 80pa 100 120 8 0.001 965 0.89 31110
Momentum: 0.9
sidered to be more representative for data of normal subjects and patients because of the inherent physiological variability. Ad- ditional output nodes may be assigned depending on the dynamic process, such as the severity of the disease. It could be argued that the SMA group of
patients may "confuse" the training of the ANN models due to the heterogeneous pattern of this disease. This was the case when cluster analysis was applied to the same MMUP data [ 2 ] . In the present study, the exclusion of SMA patients in model 11 (Table 3) did not result in a
higher diagnostic yield. Therefore, ANN models were capable in handling all four groups successfully.
Appropriate placement of the MMUP parameter values in an ascending order improved the diagnostic yield of the 80- input ANN models. Table 4 shows that
Diagnost i l Yield 9 (ESITS)
4811 00
5311 00
4811 00
6011 00
6011 00
6011 00
6011 00
6011 00
SEPTEMBER 1990 ~
IEEE ENGINEERING IN MEDICINE AND BIOLOGY 37

models 4,6, and 7, where the input vector was structured in an ascending order, gave an overall higher diagnostic yield as com- pared to models 1, 2, 3, and 8 (Table 4) where the MMUP parameter values formed the input vector in the order of acquisit ion. Arranging the MMUP parameter values in ascending order may help the system to identify similarities within patients of the same group. Gain values above 0.01 resulted in oscil-
lations of the TSS error, which did not help in reaching a steady low TSS. Very low gains below 0.001, even though they result in a smooth drop of TSS were found unacceptable since they required an ex- tremely high number of epochs to lower TSS to a near zero value. Optimum learn- ing was achieved by adopting a variable gain technique, which means starting with high gain and, as training was progressing, lowering the gain accordingly.
One of the drawbacks of the learning procedure is that the error-surface may contain local minima so that gradient de- scent may be unable to find a global min- imum as previously shown [7]. By running several tasks, the ANN models may stagnate in poor local minima that are significantly worse than the global mini- mum. In order to escape from such a situation, three strategies may be en- visaged in the following order: (1) intro- duce a disturbance to the net while the task is running by increasing the gain by a factor of 10 for a few epochs and then dropping it down to its original value; (2) abandon the run and start with a new ar- chitecture with more nodes, thus creating extra dimensions in weight space; and (3) repeat the run with a different gain and momentum.
Macro EMG was shown in previous studies to have limited diagnostic yield in differentiating between various condi- tions, and has been mainly used to dif- ferent ia te normal f rom abnormal MMUPs. The finding of a significant diagnostic yield with the use of ANN in this study underlines the potentials of the application in clinical neurophysiology. Further studies are needed to explore this direction using other EMG techniques in neuromuscular diseases.
Acknowledgment This research was partially funded by a grant from the Levendis Foundation. The authors would like to thank Mr. Renos Constantinou, Mr. Demetris Christou, and Miss Andry Constantinides for their technical assistance.
Christos N . Schizas was born in Cyprus, 1952; received the B.Sc. degree in 1978 and Ph.D. degree in 198 1 from the Univer- sity of London, UK; MBA degree in 1988 from the University of Indianapolis, USA. After completing his research studies in 198 I , he worked for three years as a post-
doctoral research fellow on computer information systems at the University of London; his research was funded by the Science Research Council, UK. For his research work he received the William
Lincoln Shelley award of the University of London in 1979. In 1985 he joined the Higher Technical Institute, Cyprus, as a lecturer of Computer Science. His re- search interests are artificial intelligence applied to medical diagnosis; neural net- works and genetic algorithms. Dr. Schizas is a visiting professor at the University of Indianapolis, and the Director of Artificial Intelligence research at the MDRTC. He is a fellow of ABAC, member of the British Computer Society, IEE and IEEE. He can be reached at the Muscular Dystrophy Research Trust of Cyprus (MDTRC), Makarios Hospi ta l , Neuromuscular Unit, Nicosia, Cyprus.
Constantinos Pat- tichis received the B.Sc. degree in Electrical Engineer- ing from the Univer- s i ty of New Brunswick, Canada in 1983, and the M.Sc. degree in Biomedical En-
gineering from the University of Texas at Austin, USA, in 1984. In 1987-88 he was awarded a Rotary International Schol- arship, in pursuing the MSc degree in Neurophysiology at the University of Newcastle Upon Tyne, UK. Presently, he is studying towards his Ph.D. at Queen Mary College, University of London. He is employed as a Research Associate in Neurophysiology at the Muscular Dystrophy Research Trust of Cyprus. His current research interests include biosig- nal analysis, quantitative electromyog- raphy, and the application of artificial neural net models in electromyographic diagnosis.
I a n Schof ie ld received the degree of B. Med. Sci in 1975 and qualified in general medicine in 1978 . After specialty training, he obtained a con- sul tancy in neurophysiology in
1984 at the Regional Neurological Centre in Newcastle Upon Tyne. Since that time, he has been involved in research into both electromyographic techniques and evoked potentials, while acquiring exper- tise in hardware and software design. His
current interests include signal processing as applied to neurophysiology and in neu- ral networks from both the physiological and theoretical standpoints.
Peter- R.W. Fawcett, B.Sc, MBBS, FRCP, trained in Neurology and Clinical Neuro- physiology at New- castle and spent one year (1980-81) in Uppsala, Sweden, working with
Professor E. Stalberg on the development of macro EMG. He was appointed Con- sultant Clincial Neurophysiologist to the Newcastle District Hospital in 1982. His main interests are in quantitative EMG and their application in neuromuscular disorders.
Leflos T . Middleton received his medical doctorate degree in 1976 from the Univer- sity of Strasborg, France, and completed his specialization in Neurology and Neurophysiology in France, with a year at Guy's Hospital, London. Dr. Middleton was a Visiting Professor at Columbia University and Fellow at the Neurological Institute of New York in 1980-81. He is currently a Consultant Neurologist and the Medical Director of the MDRTC Neuromuscular Unit in Nicosia, Cyprus. He directs research in the field of neuromuscular diseases with emphasis in quantitative electromyography. He can be reached at the MDRTC, Makarios Hospi- tal, Neuromuscular Unit, Nicosia, Cyprus.
References 1. Stalherg E: Macro EMG, a new recording technique . J Neurol Neurosurji P sy ch iatry, 43:475-482, 1980. 2. Pattichis CS: "A morphological analysis of the Macro MUP." M.Sc. thesis, University of New- castle Upon Tyne, Newcastle Upon Tyne, U.K., 1989. 3. Stalherg E, Fawcett PRW: Macro EMG in healthy subjects of different ages. J Neurol Neurosurg Psychiatry, 45:879-878, 1982. 4. Nandedkar S, Stalberg E: Simulation of Macro EMG Motor Unit Potentials. EEG Clin Neurophysiol56:52-62, 1983. 5. Schizas CN, Pattichis CS, Schofield IS, Faw- cett PR, Middleton LT: Artificial neural net algorithms in classifying electromyographic sig- nals. First IEE Int Conference on Artifcia1 Neural NetMorks, IEE Conference Publication Number 313,London,U.K.,pp 134-138,1989. 6. Pattichis CS, Schizas CN, Middleton LT, Fincham WF: Artificial Neural Net Algorithms in MUP classification. Muscle & Nerve 12:9, 753. 7. Rumelhart DE, Hinton GE, Williams RJ: "Parallel Distributed Processing. Explorations in the Microstructure of Cognition." Vol. 1, MIT Press, USA, pp 318362, 1986. 8. Lippmann RP: An introduction to computing with neural nets. IEEEASSP Mugazine, 4(2):4-22, 1987.
38 IEEE ENGINEERING I N MEDICINE AND BIOLOGY SEFTEMBER 1990