Embed Size (px)
Citation preview
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 1/29
2. Introduction:
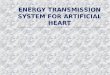
Fig 2.1 The Abiocor system
The AbioCor Total Artificial Heart System is designed to give patients with
heart failure an option other than heart transplant and Ventricular Assist Device (VAD). VAD
Systems are intended for patients with a failing left ventricle; the VAD is implanted and
replaces the ventricle by acting as a pump. Heart Patients hoping to extend their life
expectancy by having a heart transplant may not be able to realize their hope because the
amount of donor hearts in relation to the amount of patients in need of a donor heart is
1
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 2/29
minuscule. Heart patients looking to have a VAD implant may find that the system is not yet
so safe or dependable because the materials used for it have, in the past, run the risk of
causing a stroke. Due to the lack of reliable options heart patients have, researchers have been
trying to come up with a new method to aid these patients. The most recent success has been
theAbioCorTotalArtificialHeartSystem.
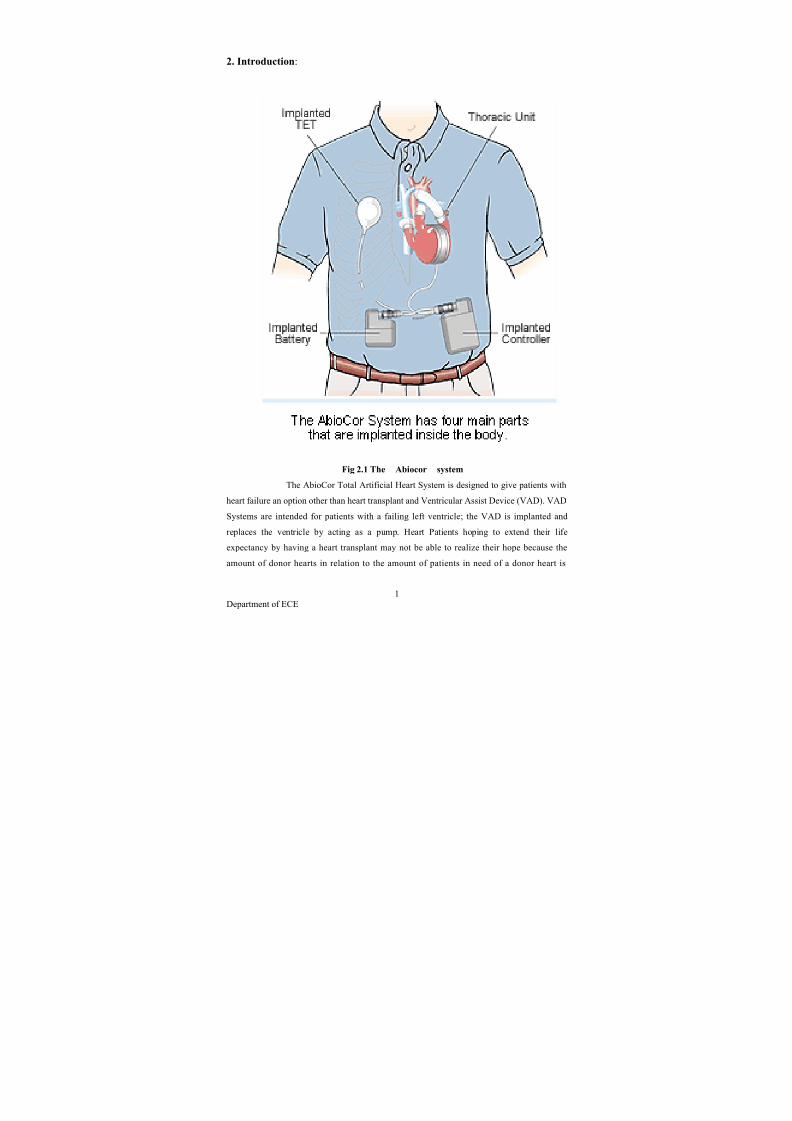
Fig 2.2 The Abiocor Artificial Heart System
2
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 3/29
The AbioCor System acts as a natural heart and allows the patient to be free
of too many restrictions; the patient is allowed to be mobile, and is also allowed to return
many of the activities he participated in before undergoing heart failure. The AbioCor is also
designed to increase the life expectancy of the heart patient by at least two times (Fact
monster).
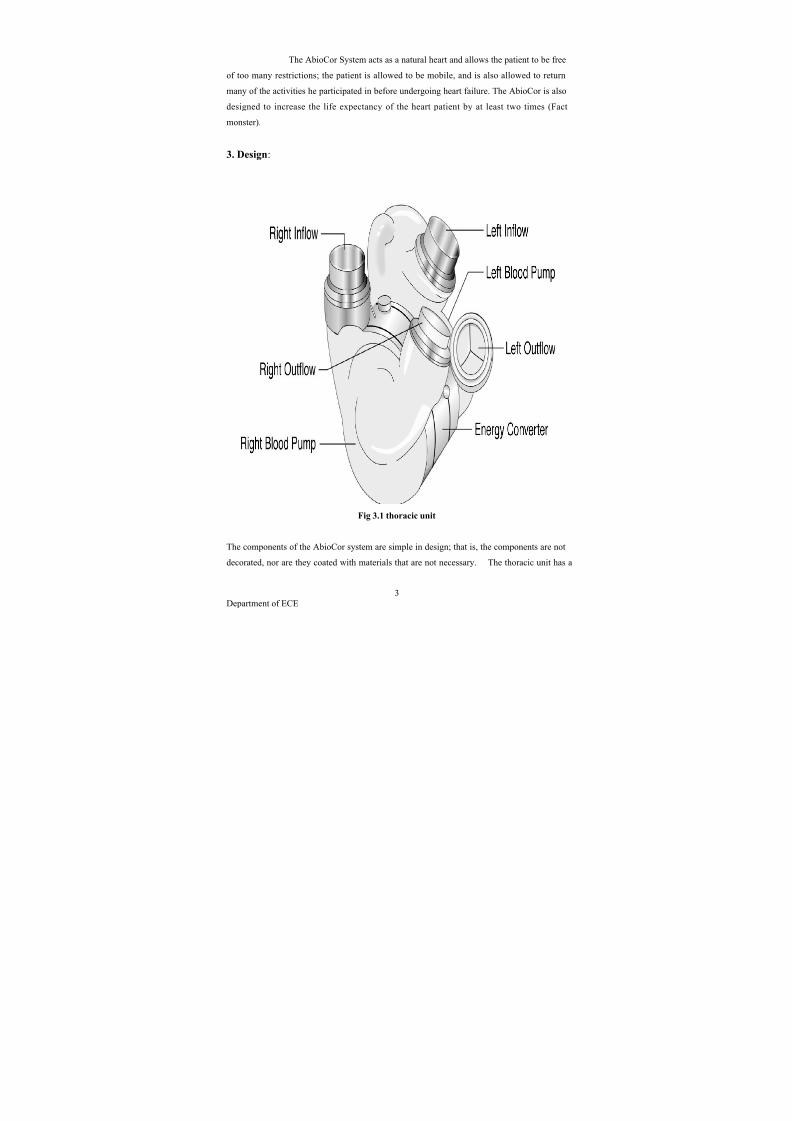
3. Design:
Fig 3.1 thoracic unit
The components of the AbioCor system are simple in design; that is, the components are not
decorated, nor are they coated with materials that are not necessary. The thoracic unit has a
3
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 4/29
similar physical appearance to the appearance of a natural heart. This is because it contains
inflows and outflows; aside from the similarity in inflows and outflows, the thoracic unit is
very different from a natural heart because it is made of plastic and titanium and it is not full
of veins as a natural heart is. The external and internal TETs are almost identical in their
design, they both have a round top and a long thin end (similar to the shape of a lollipop);
however, the external TET is covered with silicone. The rest of the AbioCor System’s
components have geometric designs (mostly rectangular) and are not extravagant in their
appearance. For example, the implanted controller and the implanted battery appear very
similar; they are both cased in titanium, they both are covered in the solid color of titanium,
and they both have the same shape. The console and the PCE control module are generally
boxes with no artistic designs or variety in color.
4. Orgins
A synthetic replacement for the heart remains one of the long-sought holy grails of modern
medicine. The obvious benefit of a functional artificial heart would be to lower the need
for heart transplants, because the demand for organs always greatly exceeds supply.
Although the heart is conceptually simple (basically a muscle that functions as a pump), it
embodies subtleties that defy straightforward emulation with synthetic materials and power
supplies. Consequences of these issues include severe foreign-body rejection and externalbatteries that limit patient mobility. These complications limited the lifespan of early human
recipients to hours or days.
5. Early developments
A heart-lung machine was used in 1953 during a successful open heart surgery. Dr. John
Heysham Gibbon, the inventor of the machine, performed the operation and developed the
heart-lung substitute himself.
On July 3, 1952, 41-year-old Henry Opitek , suffering from shortness of breath, made medical
history at Harper University Hospital at Wayne State University in Michigan. The Dodrill-
GMR heart machine, considered to be the first operational mechanical heart, was successfully
used while performing heart surgery
Dr. Forest Dewey Dodrill used the machine in 1952 to bypass Henry Opitek's left ventricle
for 50 minutes while he opened the patient's left atrium and worked to repair the mitral valve.
In Dr. Dodrill's post-operative report, he notes, "To our knowledge, this is the first instance of
survival of a patient when a mechanical heart mechanism was used to take over the complete
4
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 5/29
body function of maintaining the blood supply of the body while the heart was open and
operated on."
The scientific interest for the development of a solution for heart disease developed indifferent research groups worldwide.
Early designs of total artificial hearts
In 1949, a precursor to the modern artificial heart pump was built by Dres. William
Sewell and William Glenn of the Yale School of Medicine using an Erector Set, assorted
odds and ends, and dime-store toys. The external pump successfully bypassed the heart of a
dog for more than an hour.
On December 12, 1957, Dr. Willem Kolff, the world's most prolific inventor of artificialorgans, implanted an artificial heart into a dog at Cleveland Clinic. The dog lived for 90
minutes.
In 1958, Domingo Liotta initiated the studies of TAH replacement at Lyon, France, and in
1959-60 at the National University of Cordoba, Argentina. He presented his work at the
meeting of the American Society for Artificial Internal Organs held in Atlantic City in March
1961. At that meeting, Dr. Liotta described the implantation of three types of orthotropic
(inside the pericardial sac) TAHs in dogs, each of which used a different source of external
energy: an implantable electric motor, an implantable rotating pump with an external electric
motor, and a pneumatic pump.
In 1964, the National Institutes of Health started the Artificial Heart Program, with the goal
of putting a man-made organ into a human by the end of the decade.
In 1967, Dr. Kolff left Cleveland Clinic to start the Division of Artificial Organs at
the University of Utah and pursue his work on the artificial heart.
- In 1973, a calf named Tony survived for 30 days on an early Kolff
- In 1975, a bull named Burk survived 90 days on the artificial
- In 1976, a calf named Abebe lived for 184 days on the Jarvik 5 artificial heart.
- In 1981, a calf named Alfred Lord Tennyson lived for 268 days on the Jarvik 5.
Over the years, more than 200 physicians, engineers, students and faculty developed, tested
and improved Dr. Kolff's artificial heart. To help manage his many endeavors, Dr. Kolff
assigned project managers. Each project was named after its manager. Graduate student
Robert Jarvik was the project manager for the artificial heart, which was subsequently
renamed the Jarvik 7.
5
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 6/29
In 1981, Dr. William DeVries submitted a request to the FDA to implant the Jarvik 7 into a
human being. On December 2, 1982, Dr. Kolff implanted the Jarvik 7 artificial heart into Dr.
Barney Clark. Clark was hours from death prior to the surgery. He lived for 112 days with the
artificial heart.
fOn February 11, 2009, Dr. Kolff died at the age of 97 in Philadelphia.
First clinical implantation of a total artificial heart
On the morning of April 4, 1969, Domingo Liotta and Denton A. Cooley replaced a dying
man's heart with a mechanical heart inside the chest at the Texas Heart Institute in Houston as
a bridge for a transplant. The patient woke up and recovered well. After 64 hours, the
pneumatic-powered artificial heart was removed and replaced by a donor heart. Replacing the
artificial heart proved to be a bad decision, however; thirty-two hours after transplantation,
the patient died of what was later proved to be an acute pulmonary infection, extended to
both lungs, caused by fungi, most likely caused by an immunosuppressive-drug complication.
If they had left the artificial heart in place, the patient may have lived longer
The original prototype of Liotta-Cooley artificial heart used in this historic operation is
prominently displayed in The Smithsonian Museum "Treasures of American History" exhibit
in Washington, D.C.
First clinical applications of a permanent pneumatic total artificial heart
The eighty-fifth clinical use of an artificial heart designed for permanent implantation rather
than a bridge to transplant occurred in 1982 at the University of Utah. Artificial kidney
pioneer Dr. Willem Johan Kolff started the Utah artificial organs program in 1967. There,
physician-engineer Dr. Clifford Kwan-Gett invented two components of an integrated
pneumatic artificial heart system: a ventricle with hemispherical diaphragms that did not
crush red blood cells (a problem with previous artificial hearts) and an external heart driver
that inherently regulated blood flow without needing complex control
systems. Independently, ventriloquist Paul Winchell designed and patented a similarly shaped
ventricle and donated the patent to the Utah program. Throughout the 1970s and early 1980s,veterinarian Dr. Donald Olsen led a series of calf experiments that refined the artificial heart
and its surgical care. During that time, as a student at the University of Utah, Dr. Robert
Jarvik combined several modifications: an ovoid shape to fit inside the human chest, a more
blood-compatible polyurethane developed by biomedical engineer Dr. Donald Lyman, and a
fabrication method by Kwan-Gett that made the inside of the ventricles smooth and seamless
to reduce dangerous stroke-causing blood clots. On December 2, 1982, Dr.William
DeVries implanted the artificial heart into retired dentist Dr. Barney Bailey Clark (born
January 21, 1921), who survived 112 days with the device, dying on March 23, 1983. BillSchroeder became the second recipient and lived for a record 620 days.
6
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 7/29
Contrary to popular belief and erroneous articles in several periodicals, the Jarvik heart was
not banned for permanent use. Today, the modern version of the Jarvik 7 is known as the
SynCardia temporary Cardio West Total Artificial Heart. It has been implanted in more than
800 people as a bridge to transplantation.
In the mid-1980s, artificial hearts were powered by dishwasher-sized pneumatic power
sources whose lineage went back to Alpha-Laval milking machines. Moreover, two sizable
catheters had to cross the body wall to carry the pneumatic pulses to the implanted heart,
greatly increasing the risk of infection. To speed development of a new generation of
technologies, the National Heart, Lung, and Blood Institute opened a competition for
implantable electrically powered artificial hearts. Three groups received funding: Cleveland
Clinic in Cleveland, Ohio; the College of Medicine of Pennsylvania State University (Penn
State Hershey Medical Center ) in Hershey, Pennsylvania; and Abiomed, Inc. of Danvers,Massachusetts. Despite considerable progress, the Cleveland program was discontinued after
the first five years.
Polymeric trileaflet valves ensure unidirectional blood flow with a low pressure gradient and
good longevity. State-of-the-art transcutaneous energy transfer eliminates the need for
electric wires crossing the chest wall.
The first AbioCor to be surgically implanted in a patient was on July 3, 2001. The AbioCor is
made of titanium and plastic with a weight of two pounds, and its internal battery can berecharged with a transduction device that sends power through the skin. The internal battery
lasts for a half hour, and a wearable external battery pack lasts for four hours. The FDA
announced on September 5, 2006, that the AbioCor could be implanted for humanitarian uses
after the device had been tested on 15 patients. It is intended for critically ill patients who can
not receive a heart transplant. Some limitations of the current AbioCor are that its size makes
it suitable for only about 50% of the male population, and its useful life is only 1–2 years. By
combining its valved ventricles with the control technology and roller screw developed at
Penn State, Abiomed has designed a smaller, more stable heart, the AbioCor II. This pump,
which should be implantable in most men and 50% of women with a life span of up to five
years, ad animal trials in 2005, and the company hopes to get FDA approval for human use in
2008.
First clinical application of an intrathoracic pump
On the evening of July 19, 1963, E. Stanley Crawford and Domingo Liotta implanted the first
clinical Left Ventricular Assist Device (LVAD) at the Methodist Hospital in Houston, Texas,
in a patient who had a cardiac arrest after surgery. The patient survived for four days under
mechanical support but did not recover from the complications of the cardiac arrest; finally,the pump was discontinued, and the patient died.
7
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 8/29
First clinical application of a paracorporeal pump
On the afternoon of April 21, 1966, Michael DeBakey and Liotta implanted the first clinical
LVAD in a paracorporeal position (where the external pump rests at the side of the patient) at
the Methodist Hospital in Houston, in a patient experiencing cardiogenic shock after heart
surgery. The patient developed neurological and pulmonary complications and died after few
days of LVAD mechanical support. In October 1966, DeBakey and Liotta implanted the
paracorporeal Liotta-DeBakey LVAD in a new patient who recovered well and was
discharged from the hospital after 10 days of mechanical support, thus constituting the first
successful use of an LVAD for postcardiotomy shock.
Recent developments
In August 2006, an artificial heart was implanted into a 15-year-old girl at the Stollery
Children's Hospital in Edmonton, Alberta. It was intended to act as a temporary fixture until a
donor heart could be found. Instead, the artificial heart (called a Berlin Heart) allowed for
natural processes to occur and her heart healed on its own. After 146 days, the Berlin Heart
was removed, and the girl's heart was able to function properly on its own.
With increased understanding of the heart and continuing improvements
in prosthetics engineering, computer science, electronics, battery technology, and fuel cells, a
practical artificial heart may become a reality.
Total artificial heart
On October 27, 2008, French professor and leading heart transplant specialist Alain F.
Carpentier announced that a fully implantable artificial heart will be ready for clinical trial by
2011 and for alternative transplant in 2013. It was developed and will be manufactured by
him, Biomedical firm Carmat, and venture capital firm Truffle. The prototype uses electronic
sensors and is made from chemically treated animal tissues, called "biomaterials", or a
"pseudo-skin" of biosynthetic, microporous materials. Another US team with a prototype
called 2005 MagScrew Total Artificial Heart, including Japan and South Korea researchers
are racing to produce similar projects.Heart assist devices
Main article: ventricular assist device
Patients who have some remaining heart function but who can no longer live normally may
be candidates for ventricular assist devices (VAD), which do not replace the human heart but
complement it by taking up much of the function.
The first Left Ventricular Assist Device (LVAD) system was created by Domingo Liotta at
Baylor College of Medicine in Houston in 1962.
8
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 9/29
Another VAD, the Kantrowitz CardioVad, designed by Adrian Kantrowitz, MD, boosts the
native heart by taking up over 50% of its function. Additionally, the VAD can help patients
on the wait list for a heart transplant. In a young person, this device could delay the need for a
transplant by 10–15 years, or even allow the heart to recover, in which case the VAD can be
removed.
The first heart assist device was approved by the FDA in 1994, and two more received
approval in 1998. While the original assist devices emulated the pulsating heart, newer
versions, such as the Heart mate II, developed by the Texas Heart Institute of Houston,
Texas, provide continuous flow. These pumps (which may be centrifugal or axial flow) are
smaller and potentially more durable and last longer than the current generation of total heart
replacement pumps. Another major advantage of a VAD is that the patient can keep the
natural heart, which can receive signals from the brain to increase and decrease the heart rateas needed. With the completely mechanical systems, the heart rate is fixed.
Several continuous-flow ventricular assist devices have been approved for use in the
European Union, and, as of August 2007, were undergoing clinical trials for FDA approval.
6. Internal Components:
6.1. Thoracic Unit (Artificial Heart):
The thoracic unit weighs slightly more than two pounds (0.9 kg) and is
about the same size and shape of a natural heart. It is made of titanium, and Angioflex, a
polyurethane plastic. The thoracic unit is implanted in the chest, where a natural heart would
be located, and connects to the right and left atria, the aorta, and the pulmonary artery. In
order for blood to enter and exit from the unit, grafts must be sewed onto the right and left
atria, the aorta, and pulmonary artery of the patient. They must also be sewed onto the
thoracic unit’s four heart valves. These grafts then allow for the two arteries and the two atria
to each be snapped onto the graft of one of the heart valves. Conclusively, one valve will be
snapped onto the aorta, another valve will be snapped onto the pulmonary artery, another to
the left atrium and another to the right atrium.
The thoracic unit contains two hydraulic motors; one keeps the blood
pumping from each ventricle (blood pump), and the other operates the motion of the four
heart valves. The pumping from these hydraulic motors is caused by an oscillating pusher
plate that squeezes sacs that then emit blood to the lungs and to the rest of the body (Total
Artificial Hearts (TAH)). Additionally, the unit has a left and a right blood pump. Each blood
9
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 10/29
pump has an inflow opening and an outflow opening. When the blood moves to the right
blood pump the blood is pumped out through the outflow opening and is led to the lungs.
When the blood moves into the left blood opening it will be led to the rest of the body.
6.2. Implanted Transcutaneous Energy Transmission(TET):
Fig 6.2 Implanted TET
The implanted TET is an electric coil that provides all of the AbioCor System’s internal
devices with electrical energy. It is connected to the thoracic unit, the implanted controller,
and the implanted battery. The implanted TET is located on the upper-left area of the chest
(opposite of the artificial heart). In order to fit the patient’s insides properly, it has the
capability of adjusting its shape. Because the implanted TET provides the AbioCor System
with energy without having to run wires in and out of the patient’s body, it may also be
referred to as a wireless power transfer system. In order to provide internal devices with
energy without the use of an external power connection, the implanted TET converts energy
from radio waves, sent to it by an external TET, to electrical energy.
6.3. Implanted Controller:
The implanted controller is a small automatic computer located in the
abdomen of the patient’s body. It is secured in a titanium case and connects to all internal
components (the implanted TET, the artificial heart, and the implanted battery), meaning that
it also receives energy from the implanted TET. The job of the implanted controller is to
oversee the internal components of the AbioCor System, to communicate with the AbioCor
Console or the Patient-Carried Electronics (PCE), and to control the blood flow output of the
artificial heart. In order to monitor all internal components and communicate with external
components, the implanted controller exchanges information with the console or the PCE
(whether the implanted controller exchanges information with the console or the PCE
10
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 11/29
depends on which of these two power sources the patient is using), if a problem is detected by
either of the two external power sources, the patient is immediately notified. The implanted
controller is also able to manage the artificial heart’s cardiac output rate to make sure that the
artificial heat generates the necessary blood flow. The cardiac output rate is the “amount of
blood that flows through the heart, expressed in liters per minute. Due to monitoring of blood
outflow, the incoming blood flow is guaranteed to match the outgoing blood flow. Aside
from working automatically, the implanted controller can also be supervised by a clinician.
6.4. Implanted Battery:
Fig 6.4.1 Implanted Battery
The implanted battery is placed in the abdomen, opposite from the implanted controller, and
is implanted when the implanted controller and the artificial heart are placed in the patient’s
body. Just like the implanted controller, the implanted battery is kept in a titanium case, it
receives energy from the external TET, and is connected to all other internal components (in
the case of the implanted battery, these internal components are be the artificial heart and the
implanted controller). The battery is constantly being recharged by an external battery pack
that transfers power to the internal components of the Abercorn System through the external
and internal TETs. If the patient were to separate himself from the external TET and battery
pack (such as to take a shower), the implanted battery would provide the internal system of
the AbioCor with energy for 30 - 40 minutes (Leung, Benedict). The battery itself can last
11
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 12/29
for about a year before it would need to bed replaced. In order to replace it, the patient would
be required to receive minor surgery.
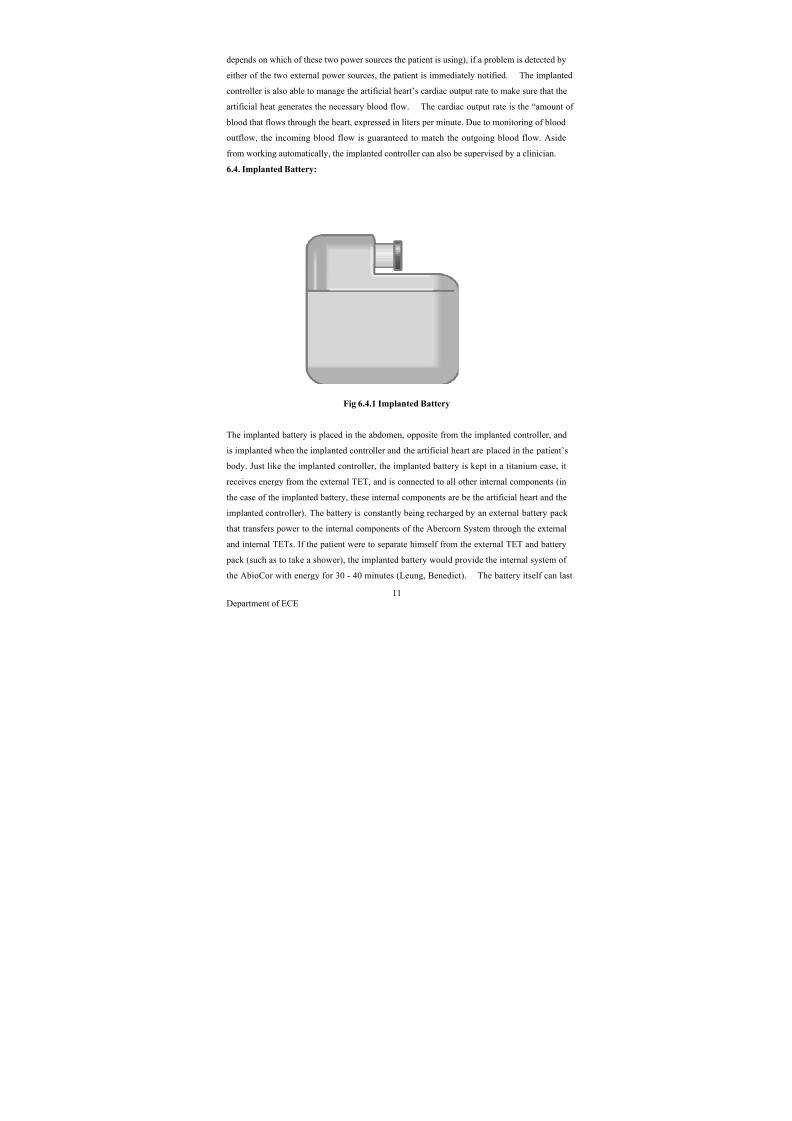
7. External Components:7.1. External Transcutaneous Energy Transmission (TET):
The external TET is placed directly over the location of the internal
TET to transfer energy through the skin (the external TET is placed over the skin, while the
internal TET is placed under the skin, inside the patient’s body). It is connected to the console
or the Patient-Carried Electronics (PCE) and is in the form of a silicone ring. The external
Fig 7.1.1 External TET
TET provides the internal TET with energy from either the PCE control module or the
AbioCor console. Both of these act as power supplies so what determines which will be used
is the location of the patient. If the patient is stationary and is near a power outlet, his source
for energy may be the console; if the patient is mobile and has no intentions of remaining in
the same location for a long period of time, he may use the PCE as a power source. The
several Watts of energy received from the external TET are transmitted to the internal TET in
the form of radio waves (Shiba, Kenji). The amount of this energy is enough to penetrate the
skin and to be received by the internal TET.
12
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 13/29
7.2. Console:
The console is a small computer containing a keyboard and screen that
is used to provide power to the external TET and the internal TET and is also used to
communicate with the implanted controller. To provide power to both TETs, the console is
plugged into an electrical outlet. The internal TET is then able to transmit energy by being
plugged into the back of the console. In order to communicate with the implanted controller,
the console uses wireless technology; it consists of an antenna that sends commands to the
implanted controller and then receives information regarding the internal components’ status.
If something goes wrong within the internal system, the console immediately notifies the
patient by setting off an alarm sound or alarm lights (Abiomed). In case of a power outage,
the console also consists of a backup battery that will keep the system powered for 35 – 40
minutes (Abiomed).
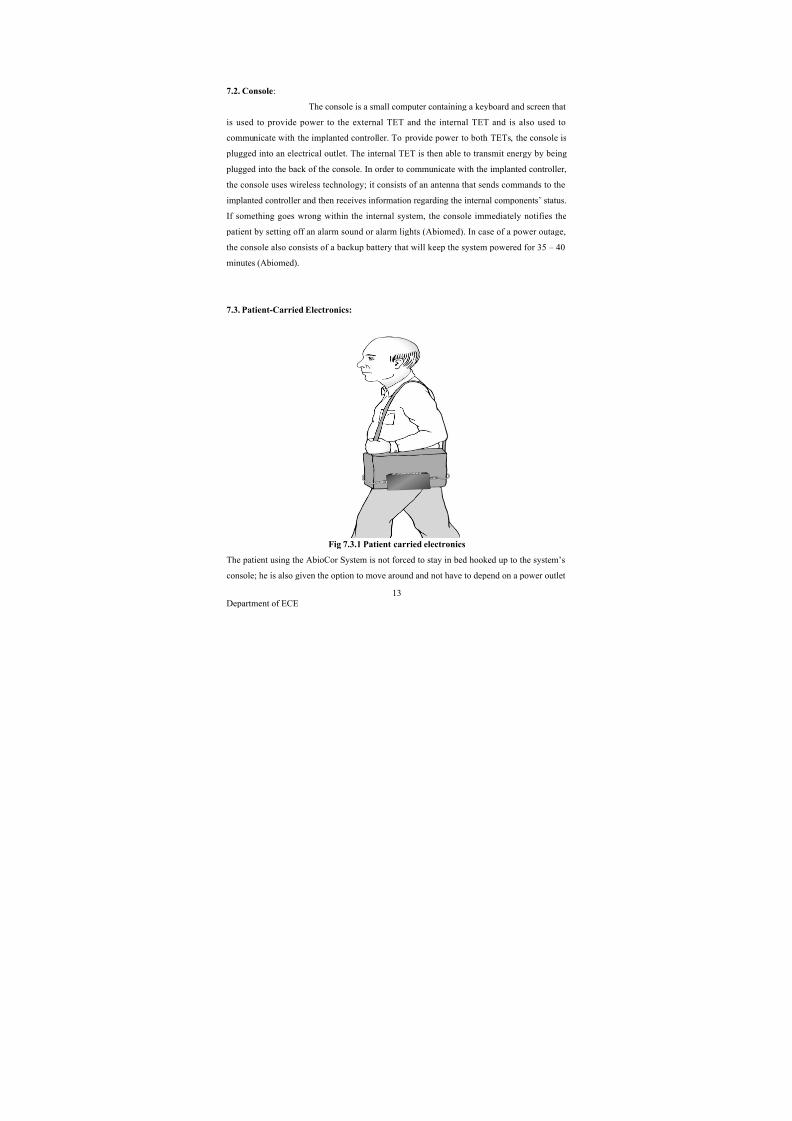
7.3. Patient-Carried Electronics:
Fig 7.3.1 Patient carried electronics
The patient using the AbioCor System is not forced to stay in bed hooked up to the system’s
console; he is also given the option to move around and not have to depend on a power outlet
13
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 14/29
to power the system’s components. If the patient chooses to be mobile he may use the
Patient-Carried Electronics (PCE) by plugging the external TET into the PCE’s control
module. The PCE serves as a portable power supply, and is placed in a shoulder bag called
the PCE Battery Bag. The battery bag stores a control module (this module takes the place of
the console when the patient is mobile) and two pairs of batteries.
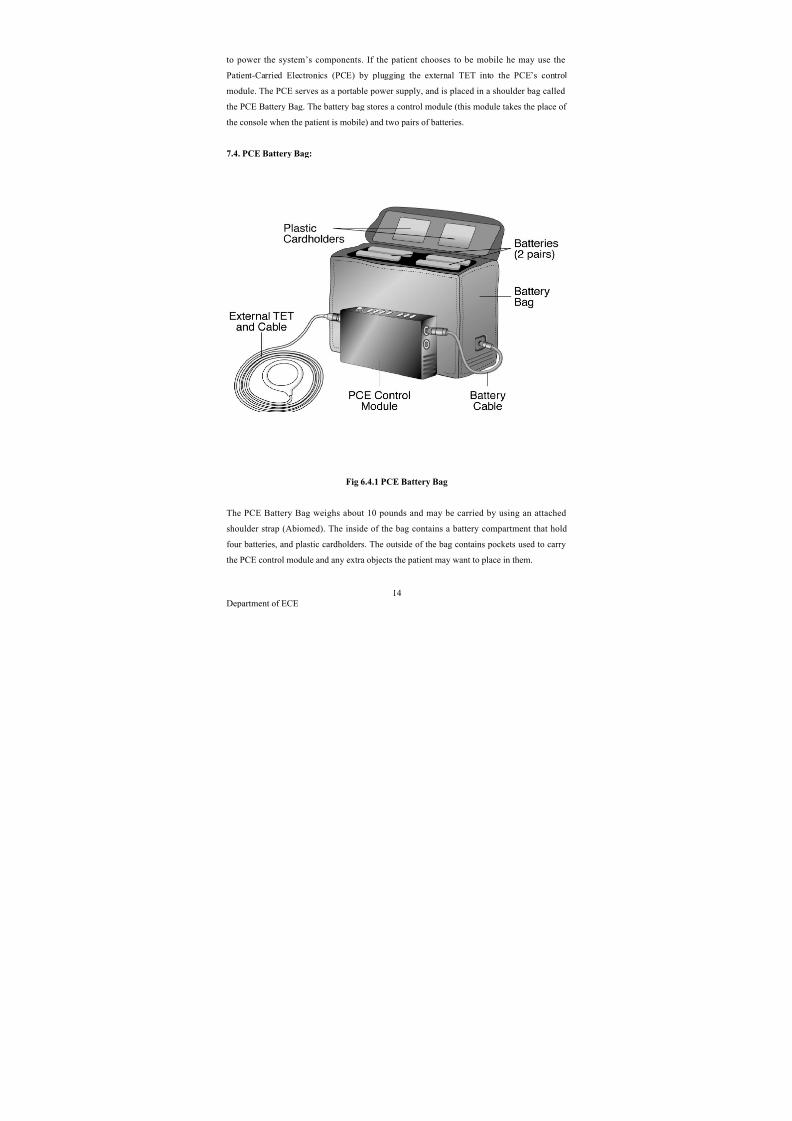
7.4. PCE Battery Bag:
Fig 6.4.1 PCE Battery Bag
The PCE Battery Bag weighs about 10 pounds and may be carried by using an attached
shoulder strap (Abiomed). The inside of the bag contains a battery compartment that hold
four batteries, and plastic cardholders. The outside of the bag contains pockets used to carry
the PCE control module and any extra objects the patient may want to place in them.
14
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 15/29
7.5. PCE Batteries:
Fig 7.5.1 PCE Batteries
Each pair of PCE Batteries supplies the AbioCor’s internal system with power for about one
hour (Abiomed). Since the battery bag can carry two pairs of PCE batteries, the internal
system may be supplied with power for about two hours if the patient uses only the two pairs
stored in the battery bag. The batteries used for the PCE package differ from common store-
bought batteries, the PCE batteries are especially made to power the AbioCor system.
Additionally, since the PCE batteries don’t last very long, they must be changed several times
a day and the patient must be aware of the amount of batteries he will be needing so he can
take extra batteries (aside from those located in the battery bag) if necessary.
15
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 16/29
7.6. PCE Control Module:
Fig 7.6.1 PCE Control Module
The PCE control module is to be placed in one of the pockets, located on the outer part of the
PCE battery bag, where it is connected to the batteries by a battery cable and is also
connected to the external TET. Instead of being connected to the batteries, the control module
may also be connected to any source of Alternating Current (AC) Power by using an AC
Power Adapter. Once connected to a power source (batteries or AC Power), the control
module converts the energy from the power source into electromagnetic energy in the form of
radio waves. By converting the energy from the power source, the external TET is able to
transfer energy to the internal TET. The control module, like the console, also monitors the
status of all of the AbioCor System’s internal components by communicating with the
implanted controller through wireless technology. If a problem occurs within one of the
internal devices, the control module immediately notifies the patient.
16
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 17/29
8. Function:
To maintain operation, the AbioCor System must first have a source of
power; depending on whether or not the patient is mobile, this power source will either be the
console or the PCE control module. Both power sources cause the AbioCor System toperform the same function and to do so in a similar way. The only difference between the two
sources is that the console receives its energy from a power outlet and is stationed in one
place and the PCE control module receives its energy from a battery pack carried in the PCE
battery bag and is portable. From the power source, energy will travel through the external
TET in the form of radio waves. These radio waves will penetrate the patient’s skin and enter
the implanted TET, which will then convert the radio waves into electrical energy. This
electrical energy will travel to the implanted battery where it will remain to keep the battery
charged. The energy stored in the battery will be used by the implanted controller to monitor
the thoracic unit’s (artificial heart) cardiac output rate. This energy supplied to the artificial
heart keeps the blood flowing into the heart and out into the body. The heart will take turns in
sending blood to the lungs and to the rest of the body because it cannot send blood to both
areas simultaneously as a natural heart would.
Besides controlling the artificial heart’s cardiac output rate, the
implanted controller also oversees the performance of all internal components to make sure
that everything is working properly. The information gathered by the controller’s supervising
is sent to the AbioCor System’s power source (the console or the PCE control module) using
wireless technology. If the power source detects a problem, an alarm light or an alarm sound
notifies the patient. Otherwise, if no problems are detected the AbioCor System follows a
cyclic function and continues to operate.
Ventricular assist devices represent a method of providing temporary mechanical circulatory
support for those patients not expected to survive until a heart becomes available for their
transplant. The scarcity of donor organs has led to the development of interim interventions,
such as mechanical assist devices.
A variety of devices have received approval from the U.S. Food and Drug Administration
(FDA), encompassing both biventricular and left ventricular devices, as well as devices that
are intended to be used in the hospital setting alone and those that can be used as an
outpatient. Devices that can be used in an outpatient setting while the patient awaits a human
donor heart include the HeartMate II and HeartMate Vented Electric Left Ventricular AssistSystem® (Thoratec Corp) and the Novacor LVAS® (World Heart, Inc.). In these two
17
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 18/29
systems, the device is surgically placed entirely within the thoracic and abdominal cavity and
connected to the power source by a percutaneous drive line.
Left ventricular assist devices (LVAD) are most commonly used as a bridge
transplantation. More recently, given the success of LVADs for prolonged periods of time,
there has been interest in using LVADs as permanent "destination" therapy for patients with
end-stage heart disease who are not candidates for human heart transplantation due to age or
other comorbidities. In November of 2002, the HeartMate device received FDA approval as
destination therapy. World Heart Corp., makers of NovaCor® LVAS, announced in 2003 that
it is engaged in clinical trials of NovaCor® VAS as destination therapy.
To date, only pulsatile LVAS devices are FDA approved for long-term use. Non-pulsatile
axial flow devices are smaller in size and have other technical advantages over pulsatile
models. The Jarvik 2000, a non-pulsatile axial flow blood pump, is in phase I clinical trials.
In April 2000, the FDA granted the Texas Heart Institute at St. Luke's Episcopal Hospital in
Houston, Texas an investigational device exemption to conduct clinical trials of the Jarvik
2000 in 25 patients as part of phase I clinical trials. The study was expanded to include the
Cleveland Clinic. Between March 2000 and February 2002, 20 patients received the device.
Devices have also been designed specifically for short-term use, typically in the post-cardiotomy setting for patients who are unable to be weaned off cardiopulmonary bypass or
for "high-risk angioplasty." The Thoratec VAD System® is paracorporeal in that the pump is
external and is connected by cannulas to the heart and great vessels. The TandemHeart
(CardiacAssist) is another device specifically designed for short-term stabilization of patients
in the postoperative setting. This device, which had its three components cleared for
marketing through the FDA 510(k) process, is unique in that it allows for percutaneous
access through the femoral vein, permitting rapid deployment. In addition, it is the first
ventricular assist device that uses continuous axial flow, as opposed to pulsatile flow.
In February 2004, the FDA approved the DeBakey VAD® Child under the Humanitarian
Device Exemption (HDE) approval process. According to the FDA, this device is indicated
under HDE for both home and hospital use for children who are between ages 5 and 16 years
and who have end-stage ventricular failure requiring temporary mechanical blood circulation
until a heart transplant is performed.
18
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 19/29
Total artificial hearts, in which the recipient undergoes cardiectomy, represent a natural
extension of ventricular assist devices as destination therapy. In 2004, the CardioWest Total
Artificial Heart received FDA approval as a bridge to transplantation. This device is unique
in that a pulsatile biventricular device is placed after the native ventricles are excised. The
labeled indication states that this device should only be used in the inpatient setting. On
September 5, 2006 the first totally implanted artificial heart for patients with advanced heart
failure involving both pumping chambers was approved under the Humanitarian Use Device
(HUD) provisions of the FDA . The AbioCor Implantable Replacement Heart, manufactured
by Abiomed, Inc. (Danvers, Mass.), is intended for people who are not eligible for a heart
transplant and who are unlikely to live more than a month without intervention. The AbioCor
system consists of a two-pound mechanical heart that takes over the pumping function of the
diseased heart, which is removed during the implantation procedure; a power transfer coil
that powers the system across the skin and recharges the internal battery from the outside;
and a controller with an internal battery, which are implanted in the patient’s abdomen. The
controller monitors and controls the functioning of the device, including the pumping rate of
the mechanical heart. The internal battery allows the recipient to be free from all external
connections for up to one hour. The system also includes two external batteries that allow
free movement for up to two hours. During sleep and while batteries are being recharged, the
system can be plugged into an electrical outlet. In order to receive the artificial heart, in
addition to meeting other criteria, patients must undergo a screening process to determine if
their chest volume is large enough to hold the device. The current, approved device is too
large for about 90% of women and for many men. Abiomed, Inc. has indicated that initially
it would provide the artificial heart at five centers around the country and eventually expand
to ten centers equipped to use the device.
Scientific Background
Bridge to Transplant LVADs
The above policy is based on a 1996 BlueCross BlueShield Association Technology
Evaluation Center (TEC) assessment (2), which concluded that left ventricular assist devices
(LVADs) can provide an effective bridge to transplantation. The TEC assessment concluded
that patients receiving a VAD showed both higher survival rates to transplantation and higher
one-year post-transplant survival compared to patients who did not receive the device. In
addition, overall function as reflected by NYHA classification was improved drastically
19
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 20/29
during the period of LVAD support. Although certain adverse effects were more frequent
among LVAD recipients (e.g., thromboembolism, infections), the superior survival to
transplant, post-transplant survival and NYHA status suggest that overall, patients who
receive LVADs have better health outcomes than patients who do not receive them.
Goldstein and colleagues have published a more recent review, confirming the above
analysis. (3) It should be recognized that left ventricular assist devices cannot change the
number of patients undergoing heart transplantation due to the fixed number of donor hearts.
However, the LVAD will categorize its recipient as a high priority heart transplant candidate.
An updated literature search of the MEDLINE database through February 3, 2009 did not
identify any articles that alter the above conclusions regarding LVAD use as a bridge to
transplantation. Published studies continue to report that the use of a LVAD does not
compromise the success of a subsequent heart transplant. In fact, it may improve post-
transplant survival, thus improving the utilization of donor hearts. (4-7) Currently available
LVADs consist of pulsatile devices that require both stiff power vent lines that perforate the
skin and bulky implantable pump chambers. There is considerable research interest in
developing non-pulsatile axial flow systems that have the potential for small size and low-
noise levels.
Publications on children using VADs as a bridge to transplantation have reported positive
outcomes. For example, Davies and colleagues reported that pediatric patients requiring a
pretransplantation VAD had similar long-term survival to those not receiving mechanical
circulatory support.
Bridge to Recovery (Post Cardiotomy) VADs
VAD support was originally indicated for the treatment of postcardiotomy cardiogenic shock
in patients who could not be weaned from cardiopulmonary bypass. VAD use in this setting
is temporary and brief, lasting between 1.4 and 5.7 days. The overall salvage rate for this
indication is low, at approximately 25 percent; however, without VAD support, patients with
refractory postcardiotomy cardiogenic shock would experience 100 percent mortality.
20
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 21/29
LVADs as Destination Therapy
The policy statement regarding LVADs as destination therapy is based on a 2002 TEC
assessment that offered the following observations and conclusions:
• The available evidence comes from a single, well-designed and rigorously conducted
randomized trial, known as the REMATCH study. The study was a cooperative effort
of Thoratec, Columbia University and the National Institutes of Health.
• The randomized trial found that patients with end-stage heart failure who are not
candidates for cardiac transplantation have significantly better survival on an LVAD
compared with treatment by optimal medical therapy. Median survival was improved
by approximately 8.5 months. Serious adverse events were more common in the
LVAD group, but these appear to be outweighed by this group's better outcomes on
function. NYHA Class was significantly improved, as was quality of life among those
living to 12 months.
• LVAD patients spend a greater relative proportion of time inside the hospital than
medical management patients do, but the survival advantage would mean a longer
absolute time outside the hospital.
In 2004, the CardioWest Total Artificial heart received FDA approval for use as a bridge to
transplant. The approval was based on the results of a nonrandomized, prospective study of
81 patients. Patients had failed inotropic therapy and had biventricular failure and thus were
not considered appropriate candidates for an LVAD. The rate of survival to transplant was
79%, which was considered comparable to the experience with LVAD in patients with left
ventricular failure. The mean time from entry into the study until transplantation or death
was 79.1 days.
Like the Cardiowest, the AbioCor is a pulsatile device, but instead of pneumatic drives, the
AbioCor uses an electro hydraulic actuator system. The current AbioCor device weighs
approximately two pounds. In currently available studies, the AbioCor has only been used as
destination therapy for end-stage patients with congestive heart failure. Dowling and
colleagues reported on the first seven patients in the AbioCor clinical trial. The 30-day
survival rate was 71% compared with the predicted survival rate of 13% with only medical
21
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 22/29
therapy. At 60 days, 43% were still alive and as of July 2006 two patients were still alive,
234 and 181 days postoperatively and remain hospitalized. Deaths were due to intraoperative
bleeding at the time of implantation, cerebrovascular accidents, pulmonary embolism, and
multiorgan failure. No reports of serious device malfunction have been reported for the
seven patients. Frazier and colleagues reported information on four additional patients
receiving the AbioCor. Using the same inclusion criteria the device supported three patients
for greater than 100 days, whereas a fourth patient expired at 53 days. There were no device
related problems reported. Abiomed’s initial request in 2005 for humanitarian device
exemption (HDE) status was denied. The Circulatory System Devices Panel note
significant concerns regarding anticoagulation and quality of life. However, in September
2006 Abiomed’s request for HDE status of the AbioCor was approved for use in patients who
are not candidates for heart transplant.
An updated search of the literature through February 3, 2009for clinical trial evidence on
VADs and total artificial hearts did not return any information that would alter the
conclusions of the policy criteria as written.
Abiocorclinicalstudysummar
Since the clinical trials of the AbioCor were initiated in June 2001, 7 patients have been
supported by this system. Four of the 7 patients lived beyond the 60-day study end point,
which is twice their predicted life expectancy. Two patients died within 24 hours of the
implant surgery. Four of the patients who survived beyond the perioperative period were
supported for 151, 142, 56, and 294 days, respectively. One patient continues to be supported
at more than 385 days and is living at home. Two patients have lived outside of the hospital
and 5 patients were ambulatory while supported by the TAH. As with other artificial heart
systems, and despite strict anticoagulation protocols, thromboembolism has been a problem in
patients supported with the AbioCor. Thrombi have been observed on support struts within
the atrial cuffs, which struts have since been removed from the device. Serious device-related
infections have not occurred.
To date, the AbioCor system has demonstrated a high degree of reliability. No pump failures
have been experienced and only minor technical problems have been encountered. The
system has functioned as intended, and hemodynamic stability is easily achieved. The TET
system has functioned reliably with no cases of power interruption. Quality of life was
significantly improved in 4 of 7 patients. The feasibility trial will continue until 15 patients
22
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 23/29
have been enrolled. Detailed results of the feasibility study will be published once the 15
studies are completed.
cardiac surgery. The TET system of the AbioCor helps to reduce device infections by
eliminating the need to penetrate the skin. The relatively small amount of foreign material in
the Jarvik 2000 may also result in fewer infection-related problems. To date, there have been
no reports of colonization of either device. The clinical results so far indicate that the
infectious complications associated with the Jarvik 2000 and the AbioCor are minimal.
9.Care and management issues
The type and the amount of blood flow provided by the axial flow pumps and the TAH differ
substantially. Supportive medical management also differs greatly. The Jarvik 2000 axial
flow pump provides submaximal unloading of the left ventricle, whereas the TAH provides
total circulation to pulmonary and systemic arteries. In TAH-supported patients with normal
intravascular volume and vascular wall tone, blood flow and pressure will be within a normal
range. However, this is not always true in patients supported by an axial flow pump. Because
axial flow pumps cause continuous blood flow throughout the cardiac cycle, diastolic blood
pressure increases, systolic blood pressure
remains unchanged, and the mean blood pressure
increases. The pulse pressure is normally reduced during support with axial flow pumps, but
some pulsatility in the arterial pressure should always be present.
23
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 24/29
Fig 9.1. A representative arterial pressure waveform from a Jarvik 2000-supported
24
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 25/29
The amount of blood flow through an axial flow pump depends primarily on the differential
pressure across the pump. With a relatively constant pump impeller speed and systemic
vascular resistance, the only constantly changing variable is the preload to the pump, which is
the left ventricular pressure. As the left ventricular pressure increases during systole, so, too,
will flow increase through the pump. During the diastolic phase, the pump preload decreases
and blood flow is reduced, but flow continues as blood enters the left ventricle from the left
atrium .The increased pump flow during systole results in a pulsatile pressure, although the
pulse pressure is reduced because of an increased diastolic pressure.
In hypovolemic conditions with high systemic vascular resistance, or when the pump speed
is relatively high, the left ventricle
is completely unloaded and no blood flows through theaortic valve. Some pulsatility may be detected, but the pulse pressure is reduced. In extreme
conditions, there may be no pulse pressure and pump flow, and total cardiac output will be
greatly reduced. Additionally, if the aortic valve remains closed, thrombosis of the aortic root
may occur because of stagnant blood flow.
Serial echocardiogram studies with simultaneous blood pressure measurements are useful to
determine the appropriate Jarvik 2000 pump speed setting. Some ejection of blood is
desirable from the left ventricle out the aortic valve to prevent stasis of blood in the aortic
root. The pump speed is adjusted from 8,000 to 12,000 rpm in 1000-rpm increments while the
aortic valve is observed. A general guideline is that the optimal pump speed setting is 1,000
rpm less than the speed at which the aortic valve remains closed. Another guide for
determining the appropriate pump speed is when the pulse pressure (systolic-diastolic) is
more than 20 mm Hg; the aortic valve will normally be open during systole.
One of the complications that can occur with axial flow pumps is thrombosis within the left
ventricle, adjacent to the device’s inflow conduit, which may lead to inflow obstruction and
recurrent heart failure. Partial or complete obstruction of the inflow can be determined by an
acute increase in the power requirements of the pump motor. The left ventricular thrombus
can be diagnosed or confirmed with echocardiogram studies. This complication has occurred
in 2 of the US bridge-to-transplantation patients supported by the Jarvik 2000. In the cardiac
catheterization laboratory, recombinant tPA is continuously infused into the left ventricle at 1
mg/min. The speed of the LVAD is increased to 11,000 rpm to allow maximal tPA perfusion
of the device. The power readout is observed for a decrease in the power necessary to rotate
25
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 26/29
the impeller, indicating successful thrombolysis. Thrombolytic therapy is often
contraindicated because of recent surgery or gastrointestinal bleeding. In both cases
mentioned above, we were able to treat the thrombus by infusing a thrombolytic agent directly
into the left ventricle. By monitoring the result and administering only as much as of the
thrombolytic agent as necessary to achieve thrombolysis, we were able to achieve a successful
result with a minimal dose.
Because the Jarvik 2000 is a partial assist system, usual heart failure support with inotropic
and vasoactive agents is often necessary. Pacemaker use and electrolyte normalization may be
necessary to maintain an adequate cardiac rhythm. Maintenance of adequate left heart volume
with a low or normal systemic vascular resistance is essential for patients supported by an
axial flow pump. Pulmonary vasodilators, such as prostaglandin
or nitric oxide, are often
needed to keep the pulmonary vascular resistance within a normal range. The right ventricle
should be supported with inotropic agents when the pulmonary vascular resistance is elevated
or if the right ventricular function is poor. Optimal pump flow and cardiac output are usually
achieved when the mean arterial blood pressure is in the range of 65 to 75 mm Hg.
Vasodilator therapy is often necessary for proper blood pressure maintenance.
In contrast, the AbioCor TAH does not normally require strict control of pulmonary and
systemic vascular resistance. The mechanical pumps can generate adequate blood flow
against a high resistance. However, maintaining proper intravascular volume is critical. The
AbioCor system can pump as much as 8 L/min, and it will do so as long as the right and left
atria have sufficient blood volume. Too much intravascular volume may cause severe
pulmonary edema or hepatic congestion; therefore, the left atrial pressure and central venous
pressures should be maintained within normal range. Although hemolysis has not been
observed in patients supported by the AbioCor, frequent hematologic assessments should be
made to monitor for anemia.
All critical care involves the monitoring and maintenance of cardiac rhythm. In the case of
AbioCor recipients, however, there is no electrocardiogram to assess and no need for
medications to support heart function because the natural heart is removed and a mechanical
system is functioning. Inotropic medications are not useful, and the usual cardiac rhythm
problems associated with severe electrolyte imbalance are of no concern. Pulmonary
vasodilator therapy may be used, although this therapy may not always be necessary because
a mechanical right heart pump is present. Hypertension and anticoagulation therapy places
26
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 27/29
these patients at risk for hemorrhagic stroke; therefore, systemic vasoactive agents should be
used as necessary to control the arterial blood pressure.
Anticoagulation therapy is necessary to prevent thrombosis in both the Jarvik 2000 and the
AbioCor. Thrombosis in either of these devices may result in device failure or may cause
infarction in other organs. Typically, a combination of low-molecular-weight dextran,
heparin, warfarin, dipyridamole, and aspirin is used to prolong clotting times and to suppress
platelet function. For all cardiac support systems, with the exception of the HeartMate LVAS,
the initiation of anticoagulation therapy depends on the amount of postoperative bleeding and
the coagulation status of the patient. The partial thromboplastin time is used to assess heparin
dosage, and the prothrombin time and international normalized ratio are used to determine the
dosage of warfarin. The thromboelastogram
is used intermittently to determine the global
efficiency of anticoagulation therapy. The goal is to begin heparin administration at a dose of
10 U · kg-1 · h-1 within the first 3 days and simultaneously start warfarin administration at a
dose of 5 mg/d. The heparin dose is reduced in increments of 200 U/h when the partial
thromboplastin time is longer than 60 seconds, and the warfarin dose is adjusted to achieve an
international normalized ratio in the range of 3.0 to 4.5 by postoperative day 10. Antiplatelet
therapy is also begun at the same time as the anticoagulation therapy. Dextran 40 at a dose of
25 mL/h is continued until the patient can take aspirin
orally. Dipyridamole (100 mg) is givenevery 6 hours, and the dose is increased 100 mg each day until the thromboelastogram
indicates that the patient is not hypercoagulable. Dipyridamole and aspirin are continued
daily.
Nutritional support and exercise are important for all patients supported with a cardiac
support system. Early aggressive physical therapy is necessary for progress toward
ambulation. A key part of the rehabilitation process is proper education of the patient and
family on the operation of the system, since one of the main goals after implantation is to
prepare the patient to live outside the hospital.
Maintenance and care of the Jarvik 2000 and AbioCor systems are different. The external
hardware for the Jarvik 2000 system is small and easily operated. Usually, Jarvik 2000-
supported patients need only to be able to change their batteries and recognize alerts on the
controller. The AbioCor system naturally requires more training, care, and maintenance
because of the increased complexity. Patients need to remove and replace the TET coil,
change batteries, identify multiple alarm conditions, and maintain numerous pieces of
27
Department of ECE
8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 28/29
accessory equipment. Although the AbioCor system is complex, it is designed to be
maintained by patients.
As with all implantable blood pumps, aggressive infection management is necessary to
prevent bacterial colonization of the implanted
foreign material. Chronic infection of these
devices often leads to serious complications and death. Both the AbioCor and the Jarvik 2000
systems are designed to minimize infectious complications. Antimicrobial therapy for
AbioCor and Jarvik 2000 recipients is not unique and is the same as the therapy given to any
patient undergoing
10. Conclusion:
The AbioCor System consists of a set of internal components and
external components. The internal components are those located inside the patient’s body;
they are the thoracic unit (artificial heart), the internal Transcutaneous Energy Transmission
(TET), the implanted controller, and the implanted battery. The external components are
those located outside of the patient’s body; these are the external Transcutaneous Energy
Transmission (TET), the console, the Patient-Carried Electronics (PCE), the PCE battery bag,
the PCE batteries, and the PCE control module. The PCE control module and the console
both serve to provide the whole system with energy. The internal and external TETs work
together to convert this energy into usable energy for all internal components and to transport
that energy from the patient’s exterior to the patient’s interior. Once the energy has reached
the patient’s interior, it is used to maintain the implanted battery charged and to provide
power for the artificial heart and for the implanted controller. All of these components keep
the artificial heart pumping blood and keep sending that blood throughout the patient’s body.
11. References:
Abiomed. Product Details.
<http://www.abiomed.com/products/heart_replacement/product_details.cfm>
28
Department of ECE

8/7/2019 ARTIFICIAL HEART 2
http://slidepdf.com/reader/full/artificial-heart-2 29/29
Bonsor, Kevin. How Artificial Hearts Work. <http://science.howstuffworks.com/artificial-
heart.htm>
Brain, Marshall. How Hydraulic Machines Work.
<http://science.howstuffworks.com/hydraulic.htm>
Cho, B.H., Gyu Bum Joun. “An energy transmission system for an artificial heart using
leakage inductance compensation of transcutaneous transformer”. IEEE. Nov. 1998
< http://ieeexplore.ieee.org/xpl/abs_free.jsp?arNumber=728328>
Factmonster. heart, artificial. <http://www.factmonster.com/ce6/sci/A0823119.html>
Institute of Medicine. The Artificial Heart: Prototypes, Policies, and Patients. Washington,
D.C.: National Academy Press, 1991.



![c3-preview.prosites.com...C] Artificial Heart Valves a Artificial Joints Asthma a Epilepsy Fainting or Dizziness Glaucoma Headaches Heart Murmur Heart Problems Heart Surgery Hepatitis](https://img.pdfslide.us/doc/110x75/5fbb24a8e76ed33c840f5380/c3-c-artificial-heart-valves-a-artificial-joints-asthma-a-epilepsy-fainting.jpg)