Embed Size (px)
Citation preview

LETTER TO THE EDITOR
Artifactual severe thrombocytopenia in a pregnant patient
Michael A. Frolich • Alan Tita • Kevin Harris
Received: 17 August 2011 / Accepted: 7 June 2012
� Springer-Verlag 2012
Dear Editor,
We recently treated a 23-year-old patient who presented to
the labor and delivery unit with an extremely low platelet
count. A thorough hematological work up revealed that the
degree of thrombocytopenia was overestimated by the
automated platelet count and that functionally this patient’s
coagulation was not affected. The patient labored for sev-
eral hours but eventually required a cesarean section for
arrested active phase of labor. The differential diagnosis of
thrombocytopenia of pregnancy includes gestational
thrombocytopenia, preeclampsia, idiopathic thrombocyto-
penia purpura (ITP) and pseudo-thrombocytopenia, a lab-
oratory artifact. This case highlights the situation where
pseudo-thrombocytopenia occurred in a patient with ITP
[1, 2].
The patient, a 23-year-old 41 weeks primigravida,
height 157.5 cm, weight 99.3 kg, was transferred to the
university hospital by her primary obstetrician because of a
history of low platelets as a child, presumed to be due to
ITP. The patient did not have any symptoms of pre-
eclampsia or clinical bleeding. The preexisting
thrombocytopenia precluded gestational thrombocytope-
nia, the most common cause in pregnancy.
On admission, her platelet count was 12.7 9 109 L-1
but she did not show any evidence of petechiae or bruising,
her INR was 0.94, prothrombin time 12.7 s and partial
thromboplastin time was 24 s. To verify the extremely low
platelet count, we examined the peripheral blood smear
that confirmed that she had marked thrombocytopenia
without platelet clumps. The few normal sized platelets
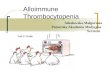
appeared healthy with normal granulation. In addition, her
smear showed frequent giant platelets (Fig. 1), which are
not properly counted by the automated cell counter but are
highly active in hemostasis [1, 2]. As next step in our work
up we ordered a thromboelastogram (TEG) to examine the
patient’s efficiency in clot formation as reported previously
[3, 4]. All TEG parameters were within normal limits
(R-time 7.1 min, alpha angle 67.3�, maximum amplitude
62.3 mm).
Based on the normal TEG and coagulation tests (PTT,
INR) and the expert opinion of the consulting hematologist,
we decided to offer epidural analgesia, also recognizing
there is not a universally acceptable platelet count that is
considered safe for neuraxial blockade [5]. After a thor-
ough risk benefit discussion with the patient, she chose to
proceed with epidural analgesia. The patient’s labor did not
progress beyond 4 cm cervical dilation, necessitating a
low-transverse cesarean section, which was performed
under epidural anesthesia with an uncomplicated postop-
erative course. Her platelet count remained stable around
30–50 9 109 L-1 requiring no therapy such as steroid
therapy or Rho immunoglobulins (RhIG).
Typically, patients with severe thrombocytopenia
undergoing cesarean may be given perioperative platelet
transfusion (typically for levels less than) and a midline
skin incision as opposed to a Pfannenstiel incision may be
M. A. Frolich (&)
Department of Anesthesiology, Center for the Development
of Functional Imaging (CDFI), University of Alabama at
Birmingham (UAB), Jefferson Tower 868C, 619 South
19th Street, Birmingham, AL 35080, USA
e-mail: [email protected]
A. Tita
Department of Obstetrics and Gynecology, UAB,
Birmingham, USA
K. Harris
Division of Hematology, Department of Medicine,
UAB, Birmingham, USA
123
Arch Gynecol Obstet
DOI 10.1007/s00404-012-2422-3

considered in order to avoid cutting into vascular layers.
Vaginal delivery is preferred if feasible, and cesarean
delivery is reserved for usual obstetric indications. This
approach minimizes bleeding complications. Severe fetal
thrombocytopenia is an indication for a cesarean section
since vaginal delivery may be associated with traumatic
cerebral hemorrhage. However, fetal thrombocytopenia is
very rare in the case of ITP because, as in the case pre-
sented here, platelet antibodies are primarily of the IgM
type, which do not cross the placenta in clinically relevant
amounts [6].
Severe thrombocytopenia is also considered a contra-
indication to regional anesthesia. However, the etiology of
this patient’s thrombocytopenia was associated with giant
platelets (GP) that are produced by megakaryocytes in the
bone marrow in response to cytokine-driven up-regulation
of platelet production. The literature indicates that GP have
clinically normal hemostasis, even in the presence of
marked thrombocytopenia [7, 8]. Without recognition of
the misleading nature of the automated platelet count and
our patient’s true coagulation status, both obstetrical and
anaesthesiological management would have been modified.
This could potentially have introduced unwarranted risks to
the patient. Using this case, we hope to illustrate a diag-
nostic and therapeutic approach that may be adopted by
others.
Conflict of interest None.
References
1. Karim R, Sacher RA (2004) Thrombocytopenia in pregnancy. Curr
Hematol Rep 3:128–133
2. Michelson A (2008) The clinical approach to disorder of platelet
number and function, platelets, 2nd edn. In: Oxford AM. Elsevier,
UK, pp 825–830
3. Frolich MA, Gibby G, Mahla ME (2003) Thromboelastography to
assess coagulation in the thrombocytopenic parturient. Can J
Anaesth 50:853
4. Sharma S (2009) Hematologic and coagulation disorders, Chest-
nut’s obstetric anesthesia. In: Chestnut DH, Polley LS, Tsen LC,
Wong CA (eds) Mosby/Elsevier, Philadelphia, pp 943–960
5. van Veen JJ, Nokes TJ, Makris M (2010) The risk of spinal
haematoma following neuraxial anaesthesia or lumbar puncture in
thrombocytopenic individuals. Br J Haematol 148:15–25
6. Ben-Hur H, Gurevich P, Elhayany A, Avinoach I, Schneider DF,
Zusman I (2005) Transport of maternal immunoglobulins through
the human placental barrier in normal pregnancy and during
inflammation. Int J Mol Med 16:401–407
7. Furie B, Furie BC (2007) In vivo thrombus formation. J Thromb
Haemost 5(Suppl 1):12–17
8. Thompson CB, Jakubowski JA, Quinn PG, Deykin D, Valeri CR
(1984) Platelet size and age determine platelet function indepen-
dently. Blood 63:1372–1375
Fig. 1 Blood smear
Arch Gynecol Obstet
123