Embed Size (px)
Citation preview

Arthroscopy: The Journal of Arthroscopic and Related Surgery 1(1):68-72 © 1985 Arthroscopy Association of North America
Arthroscopy in Steroid-Induced Osteonecrosis of the Knee
J e r o m e D. W i e d e l
Abstract: Arthroscopic examination and treatment of 10 knees involved with steroid-induced osteonecrosis offered an effective method of thoroughly eval- uating the extent of intraarticular disease and provided a means of debriding the joints with advanced lesions, giving consistent relief of internal derange- ment symptoms and, in some cases, improved functional status. If this pro- vides prolonged relief, which it seems to be accomplishing in some of the longer follow-ups, then, quite likely, we will prevent or at least postpone the next level of t reatment-- joint replacement. Key Words: Arthroscopy--Os- teonecros is - - Steroids.
The first association between osteonecrosis of bone and long-term systemic cortisone treatment was reported in 1957 (1). Since then, numerous cases have been reported. In all cases, there is one common denominator--the use of corticosteroids over a prolonged time in above-physiologic doses.
The most frequent site involved, by far, is the femoral head, followed by the humeral head and the distal femoral condyles. The reported incidence of knee joint involvement in patients who have devel- oped osteonecrosis varies from 4 to 36% (2-6), with our own incidence noted to be 35%.
Although the cause of steroid-induced osteone- crosis is not fully understood, the disease process in the knee, like that described for the femoral (7) and humeral (8) head, is probably initiated by sub- chondral bone necrosis (9), leading eventually to secondary fractures at the site of revascularization (10,11). This eventually results in collapse of the bone beneath the articular cartilage, causing an in- congruity of the articular surfaces and osteochon- dral detachment (12-14).
The clinical presentation in the knee begins with symptoms of pain and swelling. Later, symptoms of internal derangement (impingement) appear,
Address correspondence and reprint requests to Dr. J. D. Wiedel at Department of Orthopedics, University of Colorado School of Medicine, 4200 9th Ave. E, Denver, CO 80220, U.S.A.
characterized by sensations of locking, catching, and popping.
The management of the knee involved with avas- cular necrosis depends primarily on the stage of the disease (15). Early in the disease process, restricted activity, protective weight-bearing, use of cane or crutches, and an exercise program are indicated. Later, when symptoms of internal derangement in- terfere with joint function, exploration and debride- ment may be indicated. Once severe derangement and degenerative changes occur, total joint replace- ment is considered.
Prior to 1976, at the University of Colorado Health Sciences Center, the knee joint involved with steroid-induced osteonecrosis presenting with symptoms of swelling and internal derangement was evaluated by arthrotomy. An open debridement was performed, if indicated. Since 1976, this author has performed arthroscopy for evaluation of the joint, as well as debridement.
This article describes the arthroscopic findings and the results of treatment in 10 knees (eight pa- tients) with steroid-induced avascular necrosis of the knee.
MATERIALS AND METHODS
Arthroscopy was performed in l0 knees (eight pa- tients) during the period of 1976-1982. There were
68

A R T H R O S C O P Y I N S T E R O I D - I N D U C E D O S T E O N E C R O S I S OF K N E E 69
four men and four women, their ages ranging from 18 to 44 years, with an average of 32 years.
The conditions requiring the use of corticoste- roids were renal transplantation in six patients, sys- temic lupus erythematosus in one patient, and asthma in one patient.
The most common complaint, represented in all eight patients, was knee pain. Seven patients, in addition, complained of swelling, and six presented with symptoms of internal derangement.
Physical findings confirmed the presence of an effusion in seven patients, joint crepitation in six patients, and, in all but two patients, a full range of motion. One patient demonstrated a 5 ° and another a 10 ° flexion contracture.
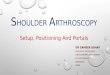
Radiographic evaluation of these 10 knees showed the femoral condyles as the primary site of involvement, with both knees involved in one pa- tient, demonstrating lateral tibial condylar involve- ment as a late finding. One patient showed areas of radiolucency only adjacent to areas of increased ra- diopacity in a patchy pattern located in the medial femoral condylar metaphysis. No subchondral cortex collapse was present. Another patient dem- onstrated a discrete subchondral lesion of radiolu- cency surrounded by sclerosis and an irregular sub- chondral cortex, very much like an osteochondritis dissecans lesion, located on the lateral surface of the medial femoral condyle (Fig. 1).
The other eight knee films demonstrated ad- vanced changes of subchondral bone sclerosis and collapse and destruction of the subchondral cortex, with osteochondral fragmentation. Of these, five showed involvement of only the lateral femoral con- dyles, whereas the other three showed changes in both medial and lateral femoral condyles.
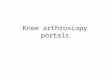
In this group of patients, the routine AP view of the knee failed to demonstrate the advanced nature of the lesion, whereas the lateral and particularly the notch view clearly outlined the site and degree of involvement (Fig. 2).
The indications for arthroscopic evaluation of the knee in these patients were persistent symptoms, in spite of adequate conservative management. The most frequent indication was internal derangement symptoms, causing interference with joint function.
The arthroscopic examination was done, using standard anteromedial and anterolateral portals. The posteromedial and posterolateral compart- ments were also visualized by inserting the arthro- scope through the intercondylar notch and utilizing the 30 ° and 70 ° arthroscopes for viewing the entire
compartment. Posteromedial and posterolateral portals were also utilized to pass surgical instru- ments for the purpose of loose body removal and debridement of the posterior femoral condyles.
RESULTS
The one patient with medial femoral condyle me- taphyseal involvement without collapse underwent arthroscopic examination of his symptomatic left knee. The finding in this knee was normal until the articular cartilage was probed and a discrete area of softening over the lateral area of the medial fem- oral condyle was found. A metaphyseal core de- compression was accomplished in this case. The patient, 2 years postoperatively, reports a decrease in pain, occurring only with strenuous activity like cross-country skiing. He reports no swelling, and no changes have been noted radiographically.
The patient with radiographic evidence of a sub- chondral osteochondritis dissecans-like lesion in the femoral condyle demonstrated a bulging of the articular cartilage in this same area, which was quite soft to probing. Drilling of the subchondral bone beneath this lesion was accomplished arthro- scopically. At 2.5-year follow-up, she continues to have pain with weight-bearing and occasional swelling. No change has been noted radiographi- cally in the bone lesion.
These two patients did not have symptoms of in- ternal derangement.
The remaining six patients (eight knees), in ad- dition to pain and swelling, had symptoms of in- ternal derangement as well as radiographic finding of advanced subchondral bone involvement and loose osteochondral fragments. All eight knees
FIG. 1. Radiograph of both knees in 22-year-old woman who underwent a renal transplant in 1970. She had a 3-year history of bilateral knee pain and mild effusion.
Arthroscopy, Vol. 1, No. 1, 1985

70 J. D. WIEDEL
2 a - c
FIG. 2. AP (a), notch (b), and lateral (c) radiographic views of left knee in 18-year-old woman with systemic lupus erythematosus on long-term steroid management. AP view fails to show extent of involvement, which is best demonstrated on notch view.
demonstrated a moderate synovitis, characterized by increased vasculature and synovial hypertrophy. A full-thickness loss of articular cartilage was ob- served on the lateral femoral condyle in all eight knees. In addition, three knees demonstrated me- dial condylar lesions. The site of these lesions was
typically located over the distal and posterior por- tions of the femoral condyles.
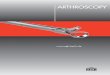
In four patients, a large osteochondral fragment was observed still partially attached at its posterior margin (Fig. 3). In the other knees, the osteochon- dral fragments were completely free. The size of the fragments varied from 5 mm to 2 x 3 cm (Fig. 4).
Articular cartilage lesions were also noted on one medial and three lateral tibial surfaces. These le- sions were characterized by frayed and denuded areas of articular cartilage similar to that observed in a degenerative process.
In the eight knees in which lateral femoral con- dylar lesions were present, the lateral meniscus
FIG. 3. Arthroscopic view of the posterolateral aspect of the left knee joint, demonstrating the free margin of a chondral frag- ment still partially attached to the femoral condyle posteriorly. The anterior margin of the femoral condylar defect is seen, in addition to fraying of the lateral meniscus in front of the popliteal tendon.
FIG. 4. Osteochondral fragment removed from the posterior portion of the lateral femoral condyle.
Arthroscopy, Vol. 1, No. 1, 1985

A R T H R O S C O P Y I N S T E R O I D - I N D U C E D O S T E O N E C R O S I S O F K N E E 71
demonstrated moderate to severe degenerative changes. No significant medial meniscal damage was noted.
Only one knee demonstrated patellofemoral in- volvement. Both articular surfaces of the patella and the patellar groove of the femur showed areas of cartilage loss and marginal osteophytes.
Treatment of the intraarticular lesions, recog- nized at the time of arthroscopy in these eight knees, consisted of loose body removal, including excision of partially attached osteochondral frag- ments and debridement of the subchondral lesions and menisci. The debridement procedure involved trimming the base of these lesions. No attempt was made to remove any remaining island of cartilage. Where bone was exposed, a very light abrading of this surface was done to produce areas of bleeding. Degenerative meniscal tears were trimmed, with preservation of the main body of the meniscus in five knees. However, three knees required partial lateral meniscectomy (Fig. 5).
The postoperative management consisted of a compression dressing, weightbearing as tolerated, with use of crutches initially, followed by a cane until walking could be performed without a limp. Range-of-motion and muscle-strengthening exer- cises were started immediately postoperatively. Cy- cling and swimming were encouraged as forms of exercise.
Follow-up of these six patients ranged from 16 months to 7 years, averaging 40 months. The most consistent finding in follow-up was the relief of im- pingement symptoms. All of the knees (eight) that experienced sensations of locking gained relief from this symptom. Four of these knees continued to have a popping sensation occurring when the knee extended from a flexed position of >60 °. During
FIG. 5. Resected portion of a severely damaged lateral me- niscus.
normal walking, this popping sensation was not ex- perienced.
A sensation of crepitation without pain was re- ported by three patients, involving five knees. Pain was reported as definitely decreased by all patients, although no patient would admit to not experiencing some discomfort some of the time. No joint effusion was reported in four knees, whereas four knees de- veloped an effusion only with activity. All patients regained their preoperative range of motion.
In one patient with bilateral knee involvement, this author performed an arthroscopic debridement of the left knee in July 1981 and of the right knee in October 1982. At the time of the right knee ar- throscopy, he agreed to an arthroscopic examina- tion of the left knee, which still had crepitation and developed an effusion with activity. The original ex- amination of the left knee in July 1981 demonstrated a severe lateral femoral condyle lesion, loose bodies, and severe lateral meniscal degeneration and tear. The loose osteocartilaginous fragments were removed, a partial lateral meniscectomy was performed, and the condylar lesion was lightly abraded and trimmed.
The follow-up examination of the left knee 15 months later demonstrated a discrete lateral fem- oral condylar lesion with smooth margins and a sur- face covered with cartilage, which was uniformly smooth throughout, without any gross degenerative changes. The anterior horn of the lateral meniscus, however, showed considerable fraying. A debride- ment of the lateral meniscus was accomplished at the time of this procedure. No loose bodies were seen.
DISCUSSION
Steroid arthropathy, a term coined by Sweetnam (16), can occur as a result of repeated intraarticular injections of a corticosteroid or secondary to pro- longed systemic corticosteroid usage. The two forms of treatment produce different disease pro- cesses, with the latter causing basically an osteo- necrosis of subchondral bone. The most frequently recognized site of involvement is the femoral head. Osteonecrosis of the humeral head, distal femoral condyles, capitellum, and talus (8), although much less commonly seen, is recognized as a complica- tion of prolonged corticosteroid treatment.
The initial symptom of pain is probably sec- ondary to the subchondral bone fractures that occur
Arlhros('ot~y, Vol. I, No, l, 1985

72 J. D. WIEDEL
at the site of revascularization (17). As the disease progresses, separation of an osteochondral frag- ment results in a mechanical impingement that, in the knee joint, characteristically leads to internal derangement symptoms. This results in the most disabling complaint by a patient who has involve- ment in the knee. To further compound the problem, meniscal cartilage tears occur as a result of the incongruent femoral condylar surface.
The predilection for involvement of the femoral condyles, more specifically, the lateral femoral con- dyle, is not fully understood. A major weight- bearing surface area could be a factor, with the tibial surfaces gaining protection from the menisci.
When tibial articular surface damage was seen, it appeared to be more of a secondary degenerative process than a result of changes recognized as oc- curring from osteonecrosis.
The lo.cation of the femoral condylar lesions, distal and posterior, could also be explained on the basis o f weight-bearing stresses that are created during knee extensions, such as rising from a seated position, stair climbing, walking, and standing.
Radiographic evaluation of the knee joint sus- pected of having steroid-induced osteonecrosis re- quires close interpretation of the lateral view (18) and particularly obtaining a notch view, which best shows the distal and posterior aspects of the fem- oral condyles. It is not uncommon to see minimal changes on a routine AP view but severe changes on a notch view.
Arthroscopic examination of the knee involved with steroid-induced osteonecrosis provided an even better and more thorough evaluation of the articular surfaces, synovium, and menisci.
Furthermore, arthroscopic debridement per- mitted an effective means for removal of loose bodies and trimming of degenerative meniscal tears, including partial meniscectomy, and it allowed de- bridement of the femoral condylar lesions.
The joint debridement consistently provided re- lief of the impingement symptoms, allowing patients to continue relatively symptom-free activities of daily living and, in some cases, to return to recre- ational sports.
Although the patients continued to have discom- fort some of the time, and those with advanced
changes complained of crepitation, these symptoms seemed to be well tolerated.
In the two patients with early or at least minimal involvement, the arthroscopic examination pro- vided a means of identifying a potential area of ar- ticular cartilage involvement. Whether the treat- ment provided these two patients will influence the progression of the disease remains to be seen.
REFERENCES
1. Pietrogrande V, Mastromarino R. Osteopatia da prolongato trattamento cortisonico. Ortop Traumatol 1957;25:791.
2. Briggs WA, Hampers CL, Merill JP, et al. Aseptic necrosis in the femur after renal transplantation. Ann Surg 1972;175:282-9.
3. Cruess RL, Blennerhassett J, MacDonald FR, MacLean LD, Dossetor J. Aseptic necrosis following renal transplan- tation. J Bone Joint Surg [Am] 1968;50:1577-90.
4. Fisher DE, Bickel WH. Corticosteroid-induced avascular necrosis. J Bone Joint Surg [Am] 1971;53:859-73.
5. Ibles LS, Alfrey AC, Huffer WE, Weil R. Aseptic necrosis of bone following renal transplantation: experience in 194 transplant recipients and review of the literature. Medicine 1978;57:25-45.
6. Potter DE, Genant HK, Salvatierra O Jr. Avascular necrosis of bone after renal transplantation. A m J Dis Child 1978;132:1125-9.
7. Cruess RL. Cortisone-induced avascular necrosis of the femoral head. J Bone Joint Surg [Br] 1977;59:308-17.
8. Cruess RL. Steroid-induced avascular necrosis of the head of the humerus. Natural history and management. J Bone Joint Surg [Br] 1976;58:313-7.
9. Evarts CM, Phalen GS. Osseous avascular necrosis asso- ciated with renal transplantation. Clin Orthop 1971;78: 330-5.
10. Aichroth P, Branfoot AC, Huskisson EC, Loughridge LW. Destructive joint changes following kidney transplantation. J Bone Joint Surg [Br] 1971 ;53:488-94.
11. Solomon L. Drug-induced arthropathy and necrosis of the femoral head. J Bone Joint Surg [Br] 1973;55:246-61.
12. Andresen J, Nielsen HE. Osteonecrosis in renal transplant recipients. Acta Orthop Scand 1981;52:475-9.
13. Griffiths HJ, Ennis JT, Bailey G. Skeletal changes following renal transplantation. Diag Radiol 1974;113:621-6.
14. Stern PJ, Watts HG. Osteonecrosis after renal transplanta- tion in children. J Bone Joint Surg [Am] 1979;61:851-6.
15. Harrington KD, Murray WR, Kountz SL, Folkert OB. Avas- cular necrosis of bone after renal transplantation. J Bone Joint Surg [Am] 1971;53:203-15.
16. Sweetnam R. Corticosteroid arthropathy and tendon rup- ture. Editorials and annotations. J Bone Joint Surg [Br] 1969;51:397-8.
17. Bewick M, Stewart PH, Rudge C, et al. Avascular necrosis of bone in patients undergoing renal allotransplantation. Clin Nephrol 1976;5:66-72.
18. Levine E, Erken EH, Price HI, Meyers AM, Solomon L. Osteonecrosis following renal transplantation. Am J Roent- genol 1977;128:985-91.
Arthroscopy, Vol. 1, No. 1, 1985