Embed Size (px)
Citation preview

Obere ExtremitätSchulter · Ellenbogen
Technical Note
Obere Extremität 2020 · 15:118–121https://doi.org/10.1007/s11678-020-00576-yReceived: 14 March 2020Accepted: 7 May 2020Published online: 20 May 2020© The Author(s) 2020
Michael Dittrich1 · BarbaraWirth1 · Florian Freislederer1 · Frederik Bellmann1 ·Markus Scheibel1,21 Department of Shoulder and Elbow Surgery, Schulthess Clinic Zürich, Zurich, Switzerland2Department of Shoulder and Elbow Surgery, Center for Musculoskeletal Surgery,Charité—UniversitaetsmedizinBerlin, Berlin, Germany
Arthroscopically assistedstabilization of chronicbidirectional acromioclavicularjoint instability using a low-profile implant and a free tendongraftA technical note
Video online
The online version of this article (https://doi.org/10.1007/s11678-020-00576-y)contains the video: “Arthroscopicallyassisted stabilization of chronic bidirectionalacromioclavicular joint instability usinga low-profile implant and a free tendongraft.” You will find the video at the endof the article as “Supplementary material.”Video by courtesy of M. Dittrich, B. Wirth,F. Freislederer, F. Bellmann, Department ofShoulder and Elbow Surgery, SchulthessClinic Zurich, Switzerland; M. Scheibel,Department of Shoulder and Elbow Surgery,Schulthess Clinic Zurich, Switzerland; andthe Department of Shoulder and ElbowSurgery, Center for Musculoskeletal Surgery,Charité—Universitaetsmedizin Berlin,Germany; all rights reserved 2020.
Background
Various surgical techniques have beendescribed to treat chronic acromioclav-icular (AC) joint instability. They canbe divided into three main categories:1. synthetic fixation between the clavicleand the coracoid with suture loops, pul-ley-like implants, or synthetic ligaments;2.biologicalpurchasewithtendonand/orligament transfer such as in theWeaver–-Dunn operation or reconstruction with
allografts or autografts; and 3. a combi-nation of synthetic and biological tech-niques [1].
Fauci et al. showed that biologicalgrafts lead to significantly better clinicaloutcomes as compared to synthetic liga-ment reconstruction in chronic AC jointinstability [2].
Biomechanical studies have high-lighted the importance of including theAC joint for improving horizontal sta-bility. Furthermore, it has been shownthat a combination of coracoclavicularand AC stabilization in the acute settingcan reduce instability of the AC joint inthe horizontal and vertical plains andtherefore lead to good and excellentclinical results [3, 6].
Kraus et al. achieved good clini-cal results for horizontal and verticalstabilization in chronic primary and re-vision AC joint instability using a gracilistendon autograft in combination witha TightRope device (Arthrex, Naples,FL, USA). In the initially describedtechnique, three transclavicular, twotranscoracoidal, and one transacromialdrill hole was made. Postoperative tun-nel widening in the transclavicular graftholes was detected but did not leaddirectly to negative clinical results, al-
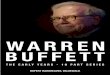
though dynamic posterior translationwas observed in some cases [4]. Mul-tiple drill holes may weaken the boneand lead to fractures of the coracoid andclavicle postoperatively. In addition, thetunnel of the TightRope device showedbone resorption due to frictional dam-age of the high-tensile sutures or tapes.Therefore, the authors present hereina modification of the above-describedtechnique using combined biologicaland synthetic stabilization of chronicbidirectional AC joint instability usinga hamstring tendon graft and a low-profile TightRope implant that reducesbone tunnels through the clavicle andthe coracoid and minimizes soft tissueirritation due to knot stacks, impairedwound healing, and implant irritation([5]; . Fig. 1).
Surgical technique
After administration of perioperative an-tibiotics and under general anesthesia,the patient is placed in the beach chairposition. The shoulder is prepped anddraped in a sterile fashion.
Through a posterior viewing por-tal, diagnostic arthroscopy is performed.Concomitant lesionsof theglenohumeral
118 Obere Extremität 2 · 2020

Fig. 18 Schematic representation of the sur-gical technique showing combined acromio-clavicular and coracoclavicular reconstructionaugmented by a low-profile TightRope device(Arthrex, Naples, Fl, USA)
joint can be detected and treated duringthe same operation.
Ananteroinferiorworkingportal ises-tablished using an outside-in technique,slightly above the tendon of the sub-scapularis muscle. Under arthroscopicview, an anterolateral transtendinousviewing portal is placed approximately1cm posterior of the anterior edge ofthe supraspinatus muscle, parallel tothe tendon fibers. With the help ofa switching stick the camera is placedinto the anterolateral portal. Throughthe anteroinferior working portal, thesubcoracoid space is dissected and thebase of the coracoid is exposed usinga radiofrequency ablation device anda shaver. Debridement of the cora-coid base is important on the one handfor good visualization for drilling andon the other hand for healing of thesubsequently placed graft.
About 2–3cmmedial of the AC joint,a 3-cm sagittal incision is made abovethe clavicle. Under proper hemostasis,the deltotrapezial fascia is opened andthe surface of the clavicle is cleaned ofsoft tissue.
Coracoclavicular drilling
Under arthroscopic visualization andwith the help of an image intensifier,the marking hook of a drill guide is
Fig. 28 a–cArthroscopicviewofthesubcoracoidpositioningofthedrillguideandsubsequentprepa-ration of the coracoclavicular passage for the TightRope device (Arthrex, Naples, Fl, USA).d,eArthro-scopic view showing the passage of themedial and lateral Nitinol suture passingwires that are usedfor subsequent graft transfer. f–iArthroscopic and image-intensifier views showing placement of thelow-profile TightRope, the DogBone button (Arthrex), and themedial and lateral Nitinol suture pass-ingwires that are used for subsequent graft transfer. jArthroscopic view showing the tendon graftpassingunderneath the coracoid.k Image-intensifier viewof the acromioclavicular drilling techniqueandplacement of theNitinol suture passingwire. l Final image-intensifier control shows theanatomicreduction of the acromioclavicular joint
placed through the anteroinferior por-tal close to the base of the coracoid.The drill sleeve is placed about 3cmmedial to the AC joint at the center ofthe clavicle. After x-ray control, a 2.0-mm K-wire is drilled transclavicular–transcoracoidal. In primary cases, thedrill hole is located between the originsof the coracoclavicular ligaments. Inrevision cases tunnel placement might
be slightly more medial or lateral due toprevious drill holes. With a 5.1-mm drillbit the surface of the clavicle is mono-cortically overdrilled using the K-wireas a guide. Thereafter, a 3.5-mm cannu-lated drill bit is used to finalize tunnelplacement for the TightRope device.The K-wire can now be removed anda Nitinol suture passing wire is insertedwith its loop-end up through the drill bit
Obere Extremität 2 · 2020 119

Technical Note
and retrieved through the anteroinferiorportal. The drill bit can now be removed(. Fig. 2a–c).
Preparation of the graft passage
A 2.0-mmK-wire is placedmanually un-der image-intensifier and arthroscopiccontrol posterior to the clavicle and closeto the medial aspect of the coracoid intothe subcoracoid space. A 4.0-mm can-nulated drill bit is placed over the K-wireby hand (without drilling). The K-wireis removed afterwards. A Nitinol suturepassing wire is shuttled through the drillbit with its loop-end up and retrievedthrough the anteroinferior working por-tal. Another Nitinol wire is placed viathe same techniquewith its loop-endfirstfrom anterior to the clavicle and lateral tothe coracoid aspect into the subcoracoidspace (. Fig. 2d, e).
Coracoclavicular stabilization
The inferior sutures of the low-profileTightRope are attached to the eyeletof the central transclavicular–transcora-coidalNitinol suture passingwire. Underarthroscopic visualization, the suturesof the TightRope are pulled through theclavicula and the coracoid and are re-trieved through the anteroinferior portal.A DogBone button (Arthrex) is addedto the inferior sutures and stabilizedwith a clamp. By pulling in reverse, theDogBone button is shuttled through theanteroinferior portal and placed under-neath the coracoid arch. The passingsuturesare removed. Underradiographicand arthroscopic control, the sutures arepulled in an alternating manner untilthe AC joint is reduced and the tophead button reaches its final positioninside the clavicle (. Fig. 2f–i). With theuse of a suture tensioner, 80–100N areapplied for each suture in order to reachperfect tension and correct reductionof the joint. A slight overcorrection of2–3mm is accepted. The sutures tightenthemselves and an additional three knotsper suture are performed for back-upfixation and placed inside the top headbutton. The sutures are cut at the levelof the low-profile button so that no knotstacks appear.
Preparation and placement ofthe graft
A hamstring tendon autograft or allo-graft (e.g., semitendinosus tendon) forbiological reconstruction is used. Thegraft should ideally be 24–26cm long and3–5mm in diameter. The graft is rein-forced on both ends with #2 FiberWires(Arthrex) in a baseball-stitch technique.With the previously placedNitinol suturepassingwires, the inferior part is shuttledfrom retroclavicular proximal paracora-coidal to anteroinferior. From here it isshuttled backwards paracoracoidal lat-eral and anterior to the clavicle, medialof the AC joint. Under arthroscopic vi-sualization one can see that the tendongraft creates a loop around the coracoidarch and lies close to theDogBone button(. Fig. 2i, j).
Acromioclavicular drilling andcerclage
In order to treat the horizontal insta-bility component an additional AC cer-clage is performed. Under image-inten-sifier control, a 1.25-mmK-wire is drilledpercutaneously transacromial from pos-terior and lateral to medial and superior.At the lateral entry point of the K-wire,a small skin incision is needed beforea 3–4-mm cannulated drill bit (depend-ing on the thickness of the graft) canbe used for overdrilling (. Fig. 2k). TheK-wire is removed and a Nitinol suturepassing wire with its loop-end up is in-serted before the drill bit is removed.
The FibreWire of the lateral part ofthe graft is now attached to the loop-endof the transacromial Nitinol suture pass-ing wire. The graft is now pulled later-ally through the transacromial drill hole.Using a clamp the FibreWire is shuttledsubcutaneously backwards to the medialincision above the clavicle. Both ends ofthe tendon graft lie next to each other.The crossed graft ends are additionallysewn together.
The deltotrapezial fascia is closedabove the graft in order to stabilize theAC joint. Final radiographic controlshows correct reduction of the AC joint(. Fig. 2l). The skin incisions can nowbe closed.
Rehabilitation
Postoperative rehabilitation takes placeunder physiotherapeutic supervision.For 8 weeks postoperatively the shoulderis protected in the Ultrasling Quadrant(DJO, Dallas, TX, USA) in the neu-tral “handshake” position. For the first2 weeks, only elbow, wrist, and handmobilization was allowed. In weeks 3and 4, passive flexion and abduction upto 45°, external rotation up to 30°, andinternal rotation as far as the patient’sbelly is possible. During the fifth andsixth weeks, passive flexion, abduction,external rotation up to 60°, and internalrotation to the belly were allowed. Inweeks 7 and 8, actively assisted flexionund abductionup to 90° and free externaland internal rotation is possible. The aimis to regain full range of motion (ROM)after 2 months. Muscle strengtheningexercises start step by step after 12 weeks.
Discussion
Minimally invasive arthroscopically as-sisted techniques for AC joint stabiliza-tion have shown benefits in comparisonto open operations, such as satisfactorycosmetic results, lower infection rates,and the possibility of treating concomi-tant lesions of the glenohumeral joint.The presented technique minimizes thenumber of drill holes in the clavicle andthecoracoid. Thetendongraftiswrappedaround the coracoid. Therefore, we pre-serve the bones of the shoulder girdle andespecially the coracoid from weakeningdue to drill holes, which can cause post-operative fractures, loss of stabilization,and revision surgery. In the describedtechnique the clavicle is in between thetwo ends of the graft, which minimizesdynamic posterior translation and there-fore creates a stable horizontal plane inaddition to the AC reconstruction.
120 Obere Extremität 2 · 2020

Corresponding address
Markus Scheibel, MDDepartment of Shoulderand Elbow Surgery,Center for Muscu-loskeletal Surgery, Char-ité—UniversitaetsmedizinBerlinAugustenburger Platz 1,13353 Berlin, [email protected]
Funding. Open Access funding provided by ProjektDEAL.
Compliance with ethicalguidelines
Conflict of interest. M. Scheibel is a consultantfor Arthrex. M. Dittrich, B.Wirth, F. Freislederer, andF. Bellmanndeclare that theyhave no competinginterests.
For this article, no studieswith humanparticipantsor animalswere performedby anyof the authors. Allstudies performedwere in accordancewith the ethicalstandards indicated in each case.
Open Access. This article is licensedunder a CreativeCommonsAttribution 4.0 International License,whichpermits use, sharing, adaptation, distribution and re-production in anymediumor format, as long as yougive appropriate credit to the original author(s) andthe source, provide a link to the Creative Commons li-cence, and indicate if changesweremade. The imagesor other third partymaterial in this article are includedin the article’s Creative Commons licence, unless in-dicatedotherwise in a credit line to thematerial. Ifmaterial is not included in the article’s Creative Com-mons licence and your intendeduse is not permittedby statutory regulation or exceeds the permitteduse,youwill need toobtain permissiondirectly from thecopyright holder. To viewa copyof this licence, visithttp://creativecommons.org/licenses/by/4.0/.
References
1. Borbas P, Churchill J, Ek ET (2019) Surgical man-agement of chronic high-grade acromioclavicularjoint dislocations: a systematic review. J ShoulderElbowSurg28:2031–2038
2. Fauci F, Merolla G, Paladini P et al (2013)Surgical treatment of chronic acromioclaviculardislocation with biologic graft vs syntheticligament: a prospective randomized comparativestudy. JOrthopTraumatol14:283–290
3. Hann C, Kraus N, Minkus M et al (2018) Com-bined arthroscopically assisted coraco- andacromioclavicular stabilization of acute high-grade acromioclavicular joint separations. KneeSurgSportsTraumatolArthrosc26:212–220
4. Kraus N, Hann C, Minkus M et al (2019) Primaryversus revision arthroscopically-assisted acromio-and coracoclavicular stabilization of chronic AC-
joint instability. Arch Orthop Trauma Surg139:1101–1109
5. Minkus M, Maziak N, Moroder P et al (2019)Arthroscopic low-profile reconstruction for acuteacromioclavicular joint instability. Obere Extrem-ität14:60–65
6. Saier T, Venjakob AJ, Minzlaff P et al (2015)Value of additional acromioclavicular cerclage forhorizontal stability in complete acromioclavicularseparation: a biomechanical study. Knee SurgSportsTraumatolArthrosc23:1498–1505
Obere Extremität 2 · 2020 121
























![Operators AFFE CHAR MECA, AFFE CHAR MECA C and AFF []](https://img.pdfslide.us/doc/110x75/62b271167c6a9a216d034fea/operators-affe-char-meca-affe-char-meca-c-and-aff-.jpg)


