Embed Size (px)
Citation preview

Arthroscopy: The Journal of Arthroscopic and Related Surgery 1(3):205-209 © 1985 Arthroscopy Association of North America
Arthroscopic Synovectomy for Chronic Hemophilic Synovitis of the Knee
Jerome D. Wiedel, M.D.
Abstract: Synovectomy for chronic hemophilic arthropathy is performed for the main purpose of stopping recurrent hemarthroses. The indications are frequent recurrent bleeds and persistent synovial hypertrophy. Five patients with chronic hemophilic arthropathy of the knee who underwent arthroscopic synovectomy between June 1980 and June 1981 represent the source for this discussion. Two of these patients subsequently developed a stress-induced joint bleed, one persisted in having an effusion bu t no recurrent bleeds, whereas the other patient developed recurrent bleeds and required a second synovectomy 4 years later. Another patient required a second arthroscopic procedure, with posteromedial synovial resection 10 months after the initial synovectomy not including the posteromediai compartment. He has not had a joint bleed since. The remaining two patients have had no recurrence of joint bleeding or synovial hypertrophy. All patients obtained their preoperative mo- tion. No complications occurred as a result of these synovectomies. Subse- quent synovectomies have produced one complication of a severe immediate postoperative hemarthrosis. Key Words: Arthroscopy--Synovial hyper- t rophy-Recurrent hemarthroses-- Synovectomy-- Hemophilia
The most painful experience a patient with he- mophilia must endure occurs as a result of joint bleeds. The most crippling and disabling conditions that a patient with severe hemophilia must endure are the sequelae of joint bleeds. Joint bleeds usually occur once the child begins to walk and reach their peak during adolescence, with spontaneous hemar- throses affecting primarily the knee, elbow, and an- kles. Of all the joints affected, the knee joint ac- counts for the most disability and impairment of function.
The basic cause of progressive joint destruction in the patient with hemophilia is recurrent hemar- throses, which in turn leads to synovial hyperplasia, hemosider in deposi t ion, and fibrosis. Eventual ly , ar t icular cart i lage degenera t ion and subchondra l
From the University of Colorado, Health Sciences Center, Denver, Colorado, U.S.A.
Address correspondence and reprint requests to Dr. Wiedel at the University of Colorado, Health Sciences Center, 4200 E. Ninth Avenue, Denver, CO 80220, U.S.A.
bone involvement lead to severe destruction of the joint.
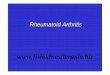
In recent years, with the advent of the Factor VIII concentrate and the emphasis on immediate management of joint bleeds, including home treat- ment programs, fewer severe joint deformities are seen. Desp i te this aggress ive a p p ro a c h to j o in t bleeds, a large number of patients with severe he- mophilia still develop r ecu r ren t jo in t bleeds and chronic synovitis (Fig. 1). The joint affected with chronic synovitis may be managed with joint pro- tection and Factor replacement. Occasionally, how- ever, synovectomy is considered for uncontrollable recurrent joint bleeds.
Synovectomy is performed for the main purpose of stopping recurrent hemarthroses. The indications are those of frequent recurrent bleeds and synovial hypertrophy that persist despite adequate Factor re- p lacement , which may include a several months course of prophylactic Factor replacement.
Synovec tomy of the knee is t radit ionally per-
205

206 J. D. WIEDEL
FIG. 1. Arthroscopic view of chronic hemophilic synovitis. Sy- novium is hypertrophied and pigmented.
formed through parapatellar arthrotomy incisions, providing good exposure to the anterior aspect of the knee joint but not the posterior compartments. Without posteromedial and lateral arthrotomies only a limited (subtotal) synovectomy is accom- plished. An extensive surgical approach, which is necessary to perform a thorough synovectomy of the knee, causes considerable postoperative mor- bidity interfering with the patient's postoperative rehabilitation program and leading to the most fre- quently reported complication following synovec- tomy in the hemophiliac patient--loss of joint mo- tion. Although Storti and coworkers (1) and Dyszy- Laube and coworkers (2) reported improved joint mobility in all their patients following knee syno- vectomy, other authors report a loss of motion in many patients (3-8). Even Storti and Ascari (9), in a later publication, reported that knee mobility re- mained unchanged in 33% of his patients and even worsened in 12%. Other complications reported have been wound healing problems, infection, and fractures associated with manipulation (4) in an at- tempt to gain further motion.
Because of the known low morbidity following arthroscopic surgery, and particularly the ease with which patients with rheumatoid arthritis recovered from arthroscopic synovectomy, this procedure was attempted in the knee joint with chronic hemophilic
arthropathy in the hopes of significantly reducing these recognized complications.
MATERIALS AND METHODS
This discussion is based mainly upon the expe- rience gained from five patients with hemophilia who had arthroscopic synovectomies performed on the knee between June 1980 and June 1981.
Four patients had classic hemophilia (Factor VIII deficiency) and one patient had Factor IX defi- ciency. The stage of knee joint involvement was classified radiographically as stage II in one patient, stage III in two, and stage IV in two patients. All patients had symptoms of frequent recurrent hem- arthroses and findings of persistent joint swelling with marked synovial hypertrophy and effusion. Pain related to activity was a symptom in the pa- tients with stage IV disease. The range of motion demonstrated a slight loss, particularly in flexion in the joints with stage III and IV changes.
All of the patients had a complete preoperative evaluation in a comprehensive hemophilia clinic. At that time, a Factor level and an inhibitor study were performed. The presence of an inhibitor was con- sidered a contraindication to surgery.
One hour before surgery the patient received ap- propriate Factor replacement in the amount to pro- duce a 100% serum Factor level. This was repeated every 12 h for approximately 10 to 14 days, and then the frequency was decreased to a daily dose. More recently, patients have received continuous drip Factor replacement postoperatively. The length of time that a regular dose of Factor replacement was given depended upon the individual case but usual- ly depended upon the intensity of the physical therapy.
By the third to fourth week, Factor replacement was given only on a need basis. Throughout hos- pitalization the Hematology and the Orthopedic ser- vices jointly cared for the patients.
The surgical technique involves a full sterile prep and draping of the extremity and the use of a tour- niquet. Examination of the joint is accomplished through an anterolateral portal using a 30 ° diag- nostic arthroscope. Once inspection of the joint is accomplished, the synovectomy begins using mo- torized instruments. Four anterior insertions sites are routinely used: the standard anteromedial and anterolateral sites plus medial and lateral suprapa- tellar sites. In addition to these four anterior por- tals, a posteromedial approach is used to remove synovium from the posteromedial compartment.
Arthroscopy, Vol. 1, No. 3, 1985

CHRONIC HEMOPHILIC SYNOVITIS 207
The posteromedial approach accommodates the placement of the synovial resector, while the pos- teromedial compartment is visualized, using 30 ° and 70 ° arthroscopes inserted from the anterior ap- proach through the notch. Synovial removal from the posterolateral compartment can usually be ac- complished satisfactorily from an anterolateral ap- proach. Occasionally, a posterolateral approach is necessary to remove fully this synovial tissue.
A large inflow cannula attached to Y-tubing to two overhead 3-L bags of sterile saline provided adequate flow during the synovial resection.
These initial cases were performed using various cartilage and meniscal shavers as there was no sy- novial resector available. Presently, aggressive sy- novial resectors are available with high speeds al- lowing more rapid removal of the synovium. Smaller instruments were used along bony margins of erosions and osteophytes and also underneath the meniscal cartilages adjacent to articular sur- faces and the meniscal synovial reflections.
When starting the synovial resection, one fre- quently must have the resector working until enough of the tissue is cleared to allow direct vi- sualization of the resector. This is necessary be- cause there may be so much synovial hypertrophy that it is impossible to see the tip of the resector until a certain amount of the tissue is removed. Once this is accomplished, one can proceed to a very rapid removal of synovium. The sequence of synovial removal will vary with each case but should follow some pattern so as not to move the instruments around in a haphazard fashion. It is probably best to start the synovial resection pos- teromedially, then proceed anteromedially into the intercondylar notch, next, the anterolateral com- partment, and then the posterolateral compartment. Synovium from the medial and lateral recesses and the suprapatellar pouch are resected last.
Initially, when I performed this procedure with the slower instruments, it took 2 to 3 h to accom- plish the synovectomy. 'Now, with the more rapid synovial resectors, the procedure can be done be- tween 1 and 2 h; however, it still requires meticu- lous technique, patience, and time. If the procedure extends past 90 minutes, I deflate the tourniquet for 10 minutes, then reinflate for a second setting. The joint clears once continuous irrigation is reestab- lished.
Following the completion of the procedures, two 1/8 inch drainage tubes are inserted through the an- teromedial and lateral portals by means of a sharp
trocar exiting superiorly from the suprapatellar pouch through the skin and attached to a suction system. The incisions are closed with either a single subcuticular absorbable suture or steri-strip tapes. A sterile dressing is applied followed by a long-leg compression dressing with medial and lateral splints holding the knee in extension. Since these five cases have been done I have used the continuous passive motion (CPM) machines postoperatively, starting either immediately in the recovery room or the following day. Physical therapy is started im- mediately, with isometric exercises in the first 24 h followed by range of motion exercises shortly there- after. The drains are usually removed in 24 to 48 h. In addition to the CPM machine, whirlpool baths assist in range of motion exercises, usually after 72 h. Electrical stimulation of the quadriceps and ham- strings is instituted early if the patient has not dem- onstrated active muscle contractions.
RESULTS
The hospitalization time for these five patients averaged 17 days. Two of the five patients required manipulation; one with stage III and the other with stage IV disease. Manipulation was considered if the patient was not showing a progressive increase in range of motion and had not passed 60°-70 ° by the fourteenth postoperative day. In follow-up, all patients in this original group completely regained their preoperative range of motion.
Three of the five patients have had a significant decrease in swelling without evidence of recurrent synovial hypertrophy. In one of these patients an effusion persisted but to a much less degree than preoperatively. Of the two remaining patients, one had a persistent posteromedial synovial thickening with a persistent effusion. In this patient a postero- medial compartment synovectomy was not per- formed. Recurrent bleeds persisted, which he could easily identify as beginning in the posteromedial compartment. This patient underwent a repeat arthroscopic examination 10 months after initial synovectomy, at which time the posteromedial compartment synovial tissue was removed. The remainder of the joint in which the previous syno- vectomy was performed demonstrated no recur- rence of synovial hypertrophy. The area of previous resection did, however, show an increased vascu- larity but no pigmented synovial tissue. Since this procedure and 2 years later, the patient has not re- ported a knee joint bleed. The other patient had no
Arthroscopy, Vol. 1, No. 3, 1985

208 J. D. WIEDEL
evidence of synovial hypertrophy and did not report any recurrent bleeds for approximately 2 years, but then sustained an injury to the knee, resulting in an acute hemarthrosis. Since then he has had a persis- tent effusion and subsequently recurrence of sy- novial hypertrophy, mainly in the posterior com- partments. This patient had a repeat synovectomy 4 years later. The other patients have had no re- current bleeds recorded since their synovectomies. No complications occurred as a direct result of the arthroscopic synovectomies in these five patients.
Since these procedures were performed, I have subsequently performed two other synovectomies, and in one of these patients, a severe bleed occurred approximately 7 days postoperatively. This neces- sitated a second arthroscopic procedure for the pur- pose of evacuating the hemarthrosis and blood clots. The patient's postoperative rehabilitation was slowed and he did lose flexion, although 1 year after the procedure he continues to gain gradually with a mild persisting effusion but no reported recurrent hemarthroses.
DISCUSSION
From this small group of patients with short follow-up, it appears that the main objective of syn- ovectomy for chronic hemophilic arthropathy has been accomplished, that is, preventing recurrent hemarthroses. The hope of preventing further de- struction of articular cartilage remains to be seen. Ideally, if one hopes to prevent further joint de- struction, the synovectomy should be performed early before there are irreversible changes within the articular cartilage (10). This probably means stage II, although some authors feel that stage III may be the latest stage at which arthropathy is still reversible by treatment. A consistent finding in these knees when examined arthroscopically was more advanced articular cartilage degeneration than what the preoperative radiographic classification in- dicated.
Two patients in this group had preoperative stage IV involvement with obvious advanced cartilage in- volvement. In addition to their complaints of dis- comfort, probably secondary to the advanced de- generative changes, these patients had documented recurrent bleeds with palpable synovial thickening. Both of these patients felt that the recurrent bleeds interfered enough with their activity that they elected to undergo synovectomy, knowing the risks of possible loss of joint mobility. These individuals
were also highly motivated patients, which is an extremely important preoperative evaluation factor. Without a doubt, the best results have been seen in patients who are cooperative, motivated, and are able to deal maturely with the pain factor. Both of these patients recovered very quickly, although one did require a manipulation. They have both re- gained their preoperative range of motion and the procedure has been successful in that it has stopped the recurrent bleeds. The patients, however, con- tinue to complain of discomfort with activity, which is probably related to the advanced degenerative changes present in the joints.
Although arthroscopic synovectomy in the pa- tient with hemophilia has been shown to be bene- ficial, the ever present threat of a postoperative complication must be taken seriously. Probably the most serious complication likely to occur is post- operative hemarthrosis. This requires immediate at- tention with evacuation of the hemarthrosis and clots, which can be done arthroscopically.
The arthroscopist who plans to perform a pro- cedure on a patient with hemophilia must be fully aware of the potential complications and must be part of the team throughout the course of treatment, which includes pre- and postoperat ive manage- ment. The arthroscopist should not simply perform the surgery and then leave the rest of the manage- ment to the hematologist, therapist, etc. The oper- ation is the easy part, whereas the preoperative evaluation and the postoperative follow-up can be very time-consuming and require input from all the team members. The orthopedist/arthroscopist is an integral part of this team and his or her input, par- ticularly in the postoperative period, is most im- portant.
Although the ideal time to perform a synovec- tomy is probably early during stage II disease, which means doing the procedure in the young pa- tient, I have great concern about the results fol- lowing the performance of arthroscopic synovec- tomy in the child. This is based on the results of two patients, ages 8 and 11, who simply could not cooperate in the immediate postoperative course and in whom knee motion has been compromised.
One must realize that patients with hemophilia have endured great suffering from multiple joint bleeds and this procedure will create an even greater painful experience in the immediate post- operative course.
Ideally, the "mature" adolescent or young adult is the best patient candidate but, unfortunately, the
Arthroscopy, Vol. 1, No. 3, 1985

CHRONIC HEMOPHILIC SYNOVITIS 209
knee may not be because of the advanced changes. Yet, good results can be obtained regardless of the stage of joint involvement.
The best results will come from those patients who have been carefully selected regardless of age and stage of joint involvement. However, the younger and more immature the patient the less pre- dictable will be their response to this procedure.
REFERENCES
1. Storti E, Traldi A, Tosatti E, et al. Synovectomy--a new approach to haemophilic arthropathy. Acta Haematol 1969;41:193 -205.
2. Dyszy-Laube B, Kaminski W, Gizycka I, et al. Synovec- tomy in the treatment of hemophilic arthropathy. J Pediatr Surg 1974;9:123-5.
3. Arnold WD, Hilgartner MW. Hemophilic arthropathy: cur- rent concepts of pathogenesis and management. J Bone Joint Surg 1977;59A:287-305.
4. Bussi L, Silvel[o L, Baudo, et al. Results of synovectomy of the knee in haemophilia. Haematologica (Pavia) 1978; 1:285 -90.
5. Clark MW. Knee synovectomy in hemophilia. Orthopedics 1978; 1:285 -90.
6. McCollough N III, Enis JE, Louih J, et al. Synovectomy or total replacement of the knee in hemophilia. J Bone Joint Surg 1979;61A:69-75.
7. Pietrogrande V, Dioguardi N, Mannucci PM. Short-term evaluation of synovectomy in haemophilia. Br Med J 1972;2:378-81.
8. Greer RB III. Operative management of hemophilic arthrop- athy--an overview. Orthopedics 1980;3:135-8.
9. Storti E, Ascari E. Surgical and chemical synovectomy. Ann N Y Acad Sci 1975;240:316-27.
10. Post M, Teller MC. Surgery in hemophilic patients. J Bone Joint Surg 1975;57A:1136-45.
Arthroscopy, Vol. 1, No. 3, 1985




![Remitting seronegative symmetrical synovitis with … · Remitting seronegative symmetrical synovitis with pitting oedema (RS3PE) is a rare rheumatologic ... [7]. However, cases of](https://img.pdfslide.us/doc/110x75/5adb86477f8b9a4a268b69df/remitting-seronegative-symmetrical-synovitis-with-seronegative-symmetrical-synovitis.jpg)