Embed Size (px)
Citation preview

Arterial and Venous Reconstruction for Free Tissue Transferin Diabetic Ischemic Foot Ulcers
H. Sunar,1* C. A. Aygit,2 Y. Afsar,2 U. Halici1 and E. Duran1
Departments of 1Cardiovascular Surgery and 2Plastic and Reconstructive Surgery, Trakya University MedicalFaculty, Edirne, Turkey
Objective. To review our experience with temporary arteriovenous (AV) fistula followed by free tissue transfer in thetreatment of diabetic foot ulcers associated with peripheral arterial occlusion.Patients and method. From July 1997 to July 2002, 15 lower extremities were operated in 14 patients. An AV loop with itsapex below the medial malleolus was created between popliteal artery and saphenous system. Three weeks later, the loop wasdivided to provide an artery and a vein end. Foot defect was covered with latissimus dorsi muscle flap followed by splitthickness skin grafting.Results. Fistulas were patent in 12 extremities. Free tissue transfer was performed in 13 extremities. Two free flaps failed.After patent temporary arteriovenous fistula, free tissue transfer was successful in 11 of 12 extremities. One patient wasamputated below knee due to ongoing infection despite successful free tissue transfer. Early mortality rate was 7%. Limbsalvage was achieved in 11 of 13 extremities that staged operation was performed. Overall extremity loss was four of 15 lowerextremities in 14 patients. Overall mortality was 21% for mean 20 follow-up period.Conclusion. Temporary AV fistula and free flap may provide stable wound coverage and high rate of limb salvage intreatment of diabetic foot ulcers with large tissue loss.
Key Words: Diabetic foot ulcers; Lower extremity ischemia; Temporary arteriovenous fistula; Free tissue transfer.
Introduction
Diabetic foot ulcers result from varying degrees ofperipheral neuropathy, infection and ischemia,1 the latteroften due to infrapopliteal disease. In patients with largetissue defects, deep space infection, osteomyelitis orexposed tendon, or bone, the limb may be lost despitesuccessful revascularization.2,3 Such patients may benefitfrom additional free tissue transfer.4–8 Furthermore,Atiyeh9 created a temporary arteriovenous J-loop fistulafrom patent popliteal artery to the greater saphenousvein at the ankle level using contralateral saphenous veingraft, followed by free tissue transfer performed bydividing the fistula apex. Here we report our experi-ence with a modification of this technique.
Patients and Method
Fifteen lower extremities in 14 diabetic patients withfoot ulcers were selected for this staged operation from
July 1997 through July 2002 on the basis of theirunderlying lower extremity arterial occlusion andlarge tissue loss of their foot. All patients were male,with an average age of 63 years (range, 47–73 years).
Free flap candidates were evaluated and treated in acollaborative effort of the surgery and plastic surgeryclinics. Patients with diabetic ischemic foot woundsnot healed by transmetatarsal amputation or havinggangrene at the toes and dorsum of the foot withprobable tissue loss at metatarsal level after debride-ment of these lesions, and patients having toegangrene with pus collection along the plantar fasciadue to infection, in whom no healing by local tissueregeneration after debridement and drainage, wereselected for free flap. Prompt surgical drainage of deepspace infection or local debridement of devitalizedtissues were required before the extent of tissue defectcould be determined. All patients underwent pre-operative lower extremity arteriography. As angio-graphic criteria, patients with infrapopliteal occlusion,having no pulses at the ankle level, and patientsexpected to have no pulse at the ankle level afterfemoropopliteal bypass were included into the study.All patients were previously ambulatory and lived
Eur J Vasc Endovasc Surg 27, 210–215 (2004)
doi: 10.1016/j.ejvs.2003.09.013, available online at http://www.sciencedirect.com on
*Corresponding author. H. Sunar, Trakya University MedicalFaculty, Department of Cardiovascular Surgery, GullapogluYerleskesi, 22030 Edirne, Turkey. Email: [email protected]
1078–5884/000210 + 06 $35.00/0 q 2003 Elsevier Ltd. All rights reserved.

independently. Patients excluded from the study weresummarized in Table 1.
In case of angina and electrocardiographic evidenceor history of myocardial infarction cardiac screeningtest, dipyridamole-thallium scanning and subsequentcoronary angiography was done. Three patients wereinvestigated with myocardial perfusion scintigraphyby recommendation of the consultant cardiologist.Two of three patients were done coronary angio-graphy. One patient needed coronary bypass surgerybefore free flap operation.
The posterior tibial artery was explored in allpatients by vertical incision posterior to the medialmalleolus, after inflow artery was prepared. However,no anastomosis was done, if tibial artery wasoccluded. For temporary arteriovenous connection,greater saphenous vein was approached by verticalincision anterior to the medial malleolus or lessersaphenous vein was explored by vertical incisionbehind the lateral malleolus. Distal bypasses andtemporary arteriovenous connections were createdby a vein graft harvested from the contralateral oripsilateral leg. The vein graft was anastomosed in anend-to-side fashion to the inflow artery and wasrouted subfascially to the vertical incision behind themedial malleolus whether or not it was anastomosedin a side-to-side fashion to the tibialis posterior artery.After the graft was passed through inferior to themedial malleolus, venous connection anastomosis wasperformed in an end-to-side fashion to the ipsilateralgreater or lesser saphenous vein (Fig. 1(a) and (b)).
In the last five cases, while using a medial approachto the popliteal artery below the knee, the ipsilateralsaphenous vein was freed through the same incisionmade over it. In these cases, the greater saphenousvein was divided just below the knee, the proximalpart of it was harvested as graft material and the distalpart was immediately anastomosed to the poplitealvein just near the popliteal artery below the knee(Fig. 1(c)). In one case, in situ distal part of greatersaphenous vein was anastomosed to the tibialisposterior vein at the supramalleolar level (Fig. 1(d)).In these cases, all other anastomoses were performed
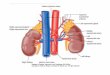
Fig. 1. Creation of temporary arteriovenous connection. (a) wasperformed in patients 1–3, 5, 6–8. (b) was done in patient 4 andthe other leg ofpatient 1. (c)our favor technique,was performedin patients 9–13. (d) was used in patient 14. Anastomosis wasnot performed when a tibialis posterior was occluded. Theseprocedures can be summarized as follows: an arteriovenousloop with its apex at the ankle is prepared. The only material ofthis loop is the saphenous vein. The descending arm of the loopis anastomosed to an inflow site of the artery with sufficientflow and enabling a safe anastomosis. Blood supply to the footwas established by side-to-side anastomosis to arteria tibialisposterior, if it had a suitable lumen in the ankle region. Theascending part of the loop is the last portion of the saphenousvein conduit after surrounding the medial malleolus frombelow. The conduit is anastomosed to the saphenous vein(magna or parva) at the malloeolar region. Main part of theascending arm of the loop is composed of the in situ saphenousvein. This saphena magna ends via an anastomosis to a deepvein (popliteal or posterior tibial vein) or in its naturalconnection (common femoral vein).
Table 1. Exclusion criteria.
Achieving limb salvage by conventional methodsPatients who were not ambulatory before the woundAdvanced sensory loss of at the heelNeuropathic ulcers with at least one distal pulseThrombophlebitis or varicosities at the saphenous veinDeep vein thrombosisForefoot wound or gangrene progressed to the ankleIntractable foot infection progressed to the proximal to the ankleExtensive gangrene in the foot including the heel
Arterial and Venous Reconstruction for Free Flaps 211
Eur J Vasc Endovasc Surg Vol 27, February 2004

afterth
eb
loo
dfl
ow
inth
ecalfp
artofth
eg
reatersap
hen
ou
sv
einw
asd
rained
toth
ep
op
litealv
eino
rits
tribu
tary.
Free
tissue
transfer
Patien
tsw
eread
min
istered2500
IUu
nfractio
nated
hep
arin,
4£
1q
idiv,
un
tilfree
flap
recon
structio
n.
After
2–
3w
eeks
of
ob
servatio
n,
the
paten
tarterio
-v
eno
us
loo
p(F
ig.
2)w
asd
ivid
edo
ver
the
do
rsum
of
the
foo
t,p
rov
idin
gv
esselsfo
rm
icrov
ascu
lartran
sfero
fa
latissimu
sd
orsi
mu
sclefl
apfo
llow
edb
ysp
lit-th
ickn
esssk
ing
raftin
g.
Fo
llow
ing
this
pro
cedu
re,v
ascular
graft
paten
cyw
asco
ntro
lledb
yco
ntin
uo
us
wav
eD
op
pler
exam
inatio
n.
Postop
erative
carean
dfollow
-up
After
freefl
aptran
sfer,all
patien
tsw
eread
min
istered2500
IUh
eparin
qid
intrav
eno
usly
for
on
ew
eek.A
tth
eth
irdw
eeko
fp
osto
perativ
eco
urse,
areh
abilitatio
np
rog
ram
wa
sin
itiated
wh
ichp
rov
ided
pa
tient’s
ph
ysica
la
ctivity.
Pa
tient
surv
iva
lex
pecta
ncy
wa
sassessed
with
Kap
lan–
Meier
meth
od
.
Table 2. Vascular reconstruction characteristics before free tissue transfer.
No. of patients Inflow Sequential anastomosis Foot revascularization Fistula connection Venous drainage Vascular graft material
1 Left proximal PA – ATP VSM – Contralateral VSM2 Left distal PA – ATP VSM – Contralateral VSM3 Right distal PA – – VSM – Contralateral VSM4 Left distal PA – – VSP – Ipsilateral VSM5 Left common FA PA ATP VSP – Ipsilateral VSM6 Left distal PA – – VSM – Contralateral VSM1* Right distal PA – – VSP – Contralateral VSM7 Right proximal PA Distal PA – VSM – Contralateral VSM8 Right distal PA – – VSM – Contralateral VSM9 Right distal PA – – VSM V. poplitea Ipsilateral proximal VSM10 Right distal PA – – VSM V. poplitea Ipsilateral proximal VSM11 Left distal PA – ATP VSM V. poplitea Ipsilateral proximal VSM12 Right distal PA – ATP VSM V. poplitea Ipsilateral proximal VSM13 Left distal PA – – VSM V. poplitea Ipsilateral proximal VSM14 Left distal PA – ATP VSM V. tibialis post. Ipsilateral proximal crural and supragenicular VSM
*Second operation for other leg of same patient after two years. PA popliteal artery, ATP, arteria tibialis posterior, VSM, vena saphena magna, VSP, vena saphena parva.
Fig
.2
.P
op
liteo-v
ena
saph
ena
mag
na
arteriov
eno
us
fistu
laan
gio
gram
.A
scend
ing
and
descen
din
garm
so
nleft,
and
fistu
laap
exo
nrig
ht.
H.
Su
nar
et
al.
212
Eu
rJ
Vasc
En
do
vasc
Su
rgV
ol
27,F
ebru
ary2004

Results
From July 1997 to July 2002, 15 extremities withchronic critical ischemia in grade III, category 6according to SVS/ISCVS criteria10 were operated in14 diabetic patients. Vascular reconstruction charac-teristics of 15 arteriovenous loop fistula procedures areincluded in Table 2.
Twelve of the temporary arteriovenous fistula werepatent in the postoperative waiting period with apatency rate of 80%. Free flap operations wereperformed in these patients after mean 16 days(range 6–35). Free tissue transfer was done in onepatient although arteriovenous fistula was insufficient.Skin defects at the flap border were seen in threepatients. One of them required regrafting.
Two free flaps failed. Flap failures occurred withinthe first 30 days. One of these patients lost his leg, theother’s foot revascularized by tibialis posterior arterywas healed by wound care. One successful flap andgraft required a below knee amputation for ongoinginfection in the surrounding soft tissues. In thispatient, recurrent debridements were also necessary,as the flap did not adhere to the underlying wounddue to ongoing infection and necrosis. And then belowknee amputation was performed since he lost his heel.In this case flap was used for amputation stump tocover it and to aid in the fitting of prosthesis.
After patent temporary arteriovenous fistula, freetissue transfer was successful in 11 (92%) extremities.Mean hospital stay was 46 days (range, 35–78). Meanambulation time was 63 days (range, 54–72). Longterm follow-up was available for an average of 20months (range, 0.1–61 months). Limb salvage andambulation were achieved in 11 (85%) of the 13extremities in which a staged operation was per-formed (Table 3).
One patient died from myocardial infarction on the4th postoperative day, resulting in an in hospitalmortality rate of 7%. Two patients died during follow-up: one from myocardial infarction, and the other fromstroke. The five-year survival rate was 56% accordingto the Kaplan–Meier method.
Discussion
Free flaps provide improved blood supply to compro-mised wounds of diabetic patients with lower extrem-ity occlusive disease and can also provide stablecoverage to larger defects. Although this techniquehas merit in selected patients, there should be noquestion of the patency of vascular inflow11 andvenous return at the time of flap anastomosis.
In free flap transfer, when primary anastomosis isnot possible, interpositional vein grafts are needed toextend the flap pedicle. However, interpositional veingrafts are associated with a 27% thrombosis rate.12 Astaged transfer of a free flap after the primaryestablishment of a temporary arteriovenous fistulagives the best chances for adequate vascularization ofthe flap and reduces the risk of thrombosis.13 Ourattempts to treat complex foot defects, even in theabsence of the distal anastomotic site for footrevascularization grafts, aim to establish arterial andvenous reconstruction for the success of free tissuetransfer in the diabetic patients. Musculus latissimusdorsi is a broad flap with a long pedicle and is usuallynot affected from atherosclerosis.14 In some cases, inspite of a muscle larger than the defect, we preferred touse latissimus dorsi due to its larger vascular outflowcapacity that improves vascular graft patency. How-ever, m. lattisimus dorsi is not the only choice of flap insuch operations.
There are different opinions about the timing of the
Table 3. Results of staged operations and major events in follow-up period.
No. of patients TAVF success Free tissue transfer Flap success Limb salvage Major events
1 þ þ þ þ Contralateral foot wound after 2 years2 þ þ þ þ3 þ þ þ þ Late death4 þ þ þ þ In hospital death5 2 þ 2 2 Late death6 þ þ þ þ Aortocoronary bypass1* 2 2 2 Above knee amputation7 þ þ þ 2 Below knee amputation8 2 2 2 Above knee amputation9 þ þ þ þ10 þ þ þ þ11 þ þ þ þ12 þ þ þ þ13 þ þ þ þ14 þ þ 2 þ
*Second operation for other leg of same patient after two years. TAVF, temporary arteriovenous fistula.
Arterial and Venous Reconstruction for Free Flaps 213
Eur J Vasc Endovasc Surg Vol 27, February 2004

operations. Free flap coverage can be performedsimultaneously,15 or in a week waiting period afterarteriovenous fistula operation.13,16,17 Delaying freeflap operation may have benefits, including assessingof graft patency, and providing optimal wound care.Staged technique also permits a reduction of theoperating time spent on each surgical procedure, anobvious advantage when considering questions ofstaffing and planning.13 However, if the fistula iscreated without performing direct revascularizationbelow the knee, and if two or more minor revisions arerequired after performing the fistula, free tissuetransfer should not be delayed. In such cases, the
need for recurrent revisions may indicate worsening ofischemia due to steal phenomenon. The time elapsewhile waiting for the flap transfer may necessitaterevision. Every new debridement may make criticallyischemic tissue more vulnerable.
The 7% postoperative early mortality rate is similarin which recent series of free flap coverage after bypassgrafting reported operative mortality reaching to 10%of patients.14,18 – 21 Diabetes is the strongest predictorof mortality in combined free tissue transfer andinfrainguinal bypass graft operations. The timing ofbypass grafting relative to flap construction has noeffect on outcome.21
Fig. 3. Nonhealing foot wound. Candidate of temporary arteriovenous fistula and free tissue transfer operations (a).Temporary arteriovenous fistula surrounding inner malleolus was marked for free tissue transfer. Plantar fascia wasdebrided and skin would been incised toward fistula apex (b). Free tissue transfer was performed and covered split thicknessskin grafting (c). Patient could walk with salvaged foot (d).
H. Sunar et al.214
Eur J Vasc Endovasc Surg Vol 27, February 2004

Limb salvage and ambulation are achieved in 11,84.6% of 13 extremities that staged operation wasperformed. In recent series of free flap coverage afterbypass grafting, long-term ambulation is beingachieved in 60–90% of patients.14,18 – 21 The 56%5-year expected survival rate is comparable to therate of combined free tissue transfer and infrainguinalbypass operations21 and to rates commonly acceptedafter bypass grafting alone for limb salvage.22,23 In thediabetic patients, the 5-year mortality rates of lowerextremity major amputation were reported as 39–68%.24,25 It was also reported that after 1 year themajority of amputees had low walking skills andlimited distance.26 Comparable mortality rates afterquick amputation should force improving and makingour technique safer instead of completely leaving it.On the other hand, one can surely not neglect theimportance of walking on own feet after a successfulfree tissue transfer (Fig. 3).
Ulcer recurrence in the same leg reflects thepersistence of the underlying etiology, includingneuropathy, infection or ischemia. However, newulcer was not detected in our series since patientswith severe neuropathy were excluded. Indirectrevascularization via flap was probably successful toremove ischemia whether or not direct foot revascu-larization. Prompt surgical drainage of deep plantarfascia and debridement of devitalized tissues pro-vided to control the infection except one. Anotherproblem during long-term follow-up is the develop-ment of a diabetic ulcer in the other foot. In diabeticpatients undergoing major lower extremity amputa-tion, the expected risk of extremity loss in theremaining leg is around 50% during the following 5years.27 Two results can be concluded from this: itsupports our radical procedure and emphasizes theneed to use the own capacity of a foot for its salvage.
References
1 Akbari CM, LoGerfo FW. Diabetes and peripheral vasculardisease. J Vasc Surg 1999; 30: 373–384.
2 Reichman W, Nichols B, Toner J, Jenvey W, Sobel M. Strategiesin the treatment of major tissue loss and gangrene: results of 100consecutive vascular reconstructions. Ann Vasc Surg 1990; 4(3):233–237.
3 Hobson RW, Lynch TG, Jamil Z, Karanfilian RG, Lee BC,Padberg FT, Long JB. Results of revascularization and amputa-tion in severe lower extremity ischemia: a five-year clinicalexperience. J Vasc Surg 1985; 2(1): 174–185.
4 Cronenwett JL, McDaniel MD, Zwolak RM, Walsh DB,Schneider JR, Reus WF, Colen LB. Limb salvage despiteextensive tissue loss. Arch Surg 1989; 124: 609–615.
5 Greenwald LL, Comerota AJ, Mitra A, Grosh JD, White JV.Free vascularized tissue transfer for limb salvage in peripheralvascular disease. Ann Vasc Surg 1990; 4: 244–254.
6 Chowdary RP, Celani VJ, Goodreau JJ, McCullough JL,McDonald KM, Nicholas GG. Free tissue transfers for limb
salvage utilizing in situ saphenous vein bypass conduit as theinflow. Plast Reconstr Surg 1991; 87: 529–535.
7 Colen LB. Limb salvage in the patient with severe peripheralvascular disease: the role of microsurgical free tissue transfer.Plast Reconstr Surg 1987; 79: 389–395.
8 Oishi SN, Levin LS, Pederson WC. Microsurgical managementof extremity wounds in diabetics with peripheral vasculardisease. Plast Reconstr Surg 1993; 92: 485–492.
9 Atiyeh BS, Sfeir RE, Hussein MM, Husami T. Preliminaryarteriovenous fistula for free flap reconstruction in the diabeticfoot. Plast Reconstr Surg 1995; 95: 1062–1069.
10 Rutherford RB, Baker D, Ernst C, Johnston KW, Porter JM,Ahn S et al. Recommended standards for reports dealing withlower extremity ischemia: revised version. J Vasc Surg 1997; 26:517–538.
11 Feldman DL, Ascer E. Extended techniques for limb salvageusing free flaps. In: Haimovici H, Ascer E, Hollier LH,Strandness DE, Towne JB, eds. Vascular Surgery, 4th ed.Massachusetts: Blackwell Science, 1996: 667–671.
12 Khouri RK, Shaw WW. Reconstruction of the lower extremitywith microvascular free flaps: a 10-year experience with 304consecutive cases. J Trauma 1989; 29: 1086–1094.
13 Sorensen JL, Muchardt O, Reumert T. Temporary arteriove-nous shunt prior to free flap transfer. Scand J Plast Reconstr HandSurg 1990; 24: 43–46.
14 McCarthy WJ, Matsumura JS, Fine NA, Dumanian GA,Pearce WH. Combined arterial reconstruction and free tissuetransfer for limb salvage. J Vasc Surg 1999; 29: 814–820.
15 Freedman AM, Meland NB. Arteriovenous shunts in freevascularized tissue transfer for extremity reconstruction. AnnPlast Surg 1989; 23: 123–128.
16 Atiyeh BS, Khali IM, Hussein MK, Al Am CA, Musharafieh
RS. Temporary arteriovenous fistula and microsurgical free tissuetransfer for reconstruction of complex defects. Plast Reconstr Surg2001; 103: 485–488.
17 Atiyeh BS, Musharafieh RS. Staged arteriovenous fistula andfree flap transfer (Letter). Ann Plast Surg 1997; 38: 193–194.
18 Gooden MA, Gentile AT, Mills JL, Bermann SS, Demas CP,Reinke KR et al. Free tissue transfer to extend the limits of limbsalvage for lower extremity tissue loss. Am J Surg 1997; 174:644–649.
19 Karp NS, Kasabian AK, Siebert JW, Eidelman Y, Colen S.Microvascular free flap salvage of the diabetic foot: a 5-yearexperience. Plast Reconstr Surg 1999; 34: 834–840.
20 Serletti JM, Higgins JP, Moran S, Orlando GS. Factorsaffecting outcome in free tissue transfer in the elderly. PlastReconstr Surg 2000; 106: 66–70.
21 Illig KA, Moran S, Serletti J, Ouriel K, Orlando G, Smith A
et al. Combined free tissue transfer and infrainguinal bypassgraft: an alternative to major amputation in selected patients.J Vasc Surg 2001; 33: 17–23.
22 Whittemore AD, Belkin M. Infrainguinal bypass. In: Ruther-
ford RB, ed. Vascular Surgery, 5th ed. Philadelphia: WB Saunders,2000: 998–1018.
23 Gupta AK, Girishkumar H. Lower extremity revascularization.J Cardiovasc Surg 1993; 34: 229–236.
24 Reiber GE. The epidemiology of diabetic foot problems:proceedings of the Second International Symposium on thediabetic foot. Diabetes Med 1996; 13(Suppl. 1): S6–S11.
25 Lee JS, Lu M, Lee VS, Russell D, Bahr C, Lee ET. Lowerextremity amputation: incidence, risk factors, and mortality inthe Oklahoma Indian Diabetes Study. Diabetes 1993; 42: 876–882.
26 Pernot HF, Winnubst GM, Cluitmans JJ, De Witte LP.Amputees in Limburg: incidence, morbidity and mortality,prosthetic supply, care utilisation and functional level after oneyear. Prosthet Orthot Int 2000; 24: 90–96.
27 Levin ME. Pathogenesis and management of diabetic footlesions. In: Levin ME, O’Neal LW, Bowker JH, eds. The DiabeticFoot, 5th ed. St Louis: Mosby, 1993: 17–60.
Accepted 25 September 2003
Arterial and Venous Reconstruction for Free Flaps 215
Eur J Vasc Endovasc Surg Vol 27, February 2004
























![ABC of Arterial and Venous Disease Www[1].Forumakademi.org](https://img.pdfslide.us/doc/110x75/553f2c4f4a7959b4088b4704/abc-of-arterial-and-venous-disease-www1forumakademiorg.jpg)

