Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Array-CGH in children with mild intellectual disability:a population-based study
Charles Coutton & Klaus Dieterich & Véronique Satre &
Gaëlle Vieville & Florence Amblard & Marie David &
Christine Cans & Pierre-Simon Jouk & Francoise Devillard
Received: 30 April 2014 /Revised: 17 June 2014 /Accepted: 19 June 2014# Springer-Verlag Berlin Heidelberg 2014
Abstract Intellectual disability (ID) is characterized by limi-tation in intellectual function and adaptive behavior, withonset in childhood. Frequent identifiable causes of ID origi-nate from chromosomal imbalances. During the last years,array-CGH has successfully contributed to improve the diag-nostic detection rate of genetic abnormalities in patients withID. Most array-CGH studies focused on patients with moder-ate or severe intellectual disability. Studies on genetic etiologyin children with mild intellectual disability (ID) are very rare.We performed array-CGH analysis in 66 children with mildintellectual disability assessed in a population-based study andfor whom no genetic etiology was identified. We found one ormore copy number variations (CNVs) in 20 out of 66 (~30 %)patients with a mild ID. In eight of them (~12 %), the CNVswere certainly responsible for the phenotype and in six theywere potentially pathogenic for ID. Altogether, array-CGHhelped to determine the etiology of ID in 14 patients
(~21 %). Conclusion: Our results underscore the clinical rel-evance of array-CGH to investigate the etiology of isolatedidiopathic mild ID in patients or associated with even subtledysmorphic features or congenital malformations.
Keywords Chromosomal microarray . Array-CGH .Mildintellectual disability . Developmental delay
Abbreviations
AAIDD American Association on Intellectual and De-velopmental Disabilities
AGTR2 Angiotensin II receptor, type 2ARHGAP24 Rho GTPase activating protein 24CDH13 Cadherin 13CGH Comparative genomic hybridizationCNV Copy number variations
Communicated by Beat Steinmann
Electronic supplementary material The online version of this article(doi:10.1007/s00431-014-2367-6) contains supplementary material,which is available to authorized users.
C. Coutton :V. Satre :G. Vieville : F. Amblard : F. DevillardLaboratoire de Génétique Chromosomique, Département deGénétique et Procréation, Hôpital Couple Enfant, CHU Grenoble,38700 Grenoble, France
C. Coutton :V. SatreAGIMCNRS FRE3405, Equipe “Andrologie, Génétique et Cancer”,Université Joseph Fourier, Grenoble, France
K. Dieterich : P.<S. JoukService de Génétique Clinique, Département de Génétique etProcréation, Hôpital Couple Enfant, CHU Grenoble,38700 Grenoble, France
M. DavidRHEOP, Grenoble, Isère, France
K. DieterichInserm U836, Equipe 4, Grenoble Institut des Neurosciences,Université Joseph Fourier, Grenoble, France
C. CansExploitation Units of Medical Information, Grenoble UniversityHospital, Grenoble, Isère, France
C. Coutton (*)Service de Génétique Chromosomique, Hôpital Couple-Enfant,CHU de Grenoble, 38043 Grenoble Cedex 9, Francee-mail: [email protected]
Eur J PediatrDOI 10.1007/s00431-014-2367-6

DECIPHER Database of Chromosomal Imbalance andPhenotype in Humans Using EnsemblResources
DGV Database of genomic variantsEEG ElectroencephalogramFISH Fluorescence in situ hybridizationGPR87 G protein-coupled receptor 87HEPACAM Hepatic and glial cell adhesion moleculeID Intellectual disabilityIQ Intelligence quotientK-ABC Kaufman Assessment Battery for ChildrenMDPH Maison Départementale des Personnes
HandicapéesMED12L Mediator complex subunit 12-likeMED12 Mediator complex subunit 12MED13 Mediator complex subunit 13MED13L Mediator complex subunit 13-likeMED17 Mediator complex subunit 17MED23 Mediator complex subunit 23MLPA Multiplex ligation-dependent probe
amplificationNCBI National center for biotechnology informationOCRL Oculocerebrorenal syndrome of LoweOMIM Online Mendelian Inheritance in ManP2RY Purinergic receptor P2YP2RY12 Purinergic receptor P2Y, G-protein coupled,
12P2RY13 Purinergic receptor P2Y, G-protein coupled,
13P2RY14 Purinergic receptor P2Y, G-protein coupled,
114RHEOP Registre du Handicap Et Observatoire
PérinatalTMEM130 Transmembrane protein 130TRRAP Transformation/transcription domain-
associated proteinUCSC University of California, Santa CruzVUS Variant of unknown significanceWISC Wechsler Intelligence Scale for ChildrenWPPSI-R Wechsler Preschool and Primary Scale of In-
telligence Revised
Introduction
According to The American Association on Intellectual andDevelopmental Disabilities (AAIDD), intellectual disability(ID) is “a condition characterized by significant limitationsboth in intellectual functioning and in adaptive behavior asexpressed in conceptual, social, and practical adaptive skillsoriginating during the developmental period” [32]. Intellectualdisability is one of the most frequent neurological
impairments in school-age children. The prevalence is world-wide estimated to be 3 % [37]. Intellectual disability includesprofound (IQ<20), severe (IQ 20–34), moderate (IQ 35–49),and mild ID (IQ 50–70). Many different causal factors such asgenetic, congenital and developmental, environmental, andsociocultural have been associated with ID. Among them,genetic etiologies remain the most frequent, ranging from 4to 15 % of mild ID and from 20 % to almost 50 % of othercauses of ID [7, 11]. Epidemiological studies of etiologies ofID are rare and difficult to compare because many differentcriteria have been evaluated, different instruments have beenused, and many studies have lumped all the categories ofintellectual disabilities [29, 31]. Whereas ID with IQ <50has been widely investigated, there are very few studies con-ducted on mild ID. The variability in the prevalence of mildID is high from 4 per 1,000 to 20 times higher [6, 13, 29]. Thisis mostly due to the method used to detect these cases. More-over, some children with a mild ID are in regular schoolingeven though they follow specialized educational program,making them difficult to identify. Intellectual disability is notnecessarily a life-long condition and many people with mildID have only intermittent and time-limited contact with intel-lectual disability services [13]. The Registre du Handicap EtObservatoire Périnatal (RHEOP) is a French register whichidentifies all children at the age of 7 with severe motor,sensory, or intellectual disabilities. To better respond to par-ent’s questions on their child’s future, the RHEOP decided toconduct a study on mild ID. The main objectives of this studywere to estimate the prevalence of mild ID, to describe theclinical signs and comorbidities of the children included, andto specify the etiologies of this disability. From the 15,100children born in 1997 in this county, we identified 267 chil-dren with mild ID. Thus, the prevalence was 18/1,000. Prev-alence and epidemiological characteristics of this populationhave been previously reported [6].
In recent years, array-CGH contributes successfully toidentify genomic variations responsible for IDwith an averagedetection rate of 15 to 20 % [3]. Thus, we decided to completethe genetic assessment of the children included in this studyby performing array-CGH when first-line genetic investiga-tions gave a normal result and when no other etiology wasidentified.
Material and methods
Patients
We included in this study 66 children (43 boys and 23girls, sex ratio M/F: 1.87) with a mild ID previouslydescribed in David et al. [6]. All the selected childrenhave an IQ score between 48 and 77 (confidence intervalfor an IQ from 52 to 69) with both index values (verbal
Eur J Pediatr

and performance) less than 85. All the children includedwere born in 1997 and residing in Isère County in 2008,date of the initial recruitment. They presented a mild IDidentified between 9 and 13 years of age. Some of themhave subt le dysmorphic features or congeni ta lmalformations (Table 1). The WISC-IV (69.3 %) wasthe test most frequently used, followed by the WISC-III(27 %). The Kaufman Assessment Battery for Children(K-ABC) and the Wechsler Preschool and Primary Scaleof Intelligence Revised (WPPSI-R) were used for fewcases 3.4 and 0.4 %, respectively. Children were identi-fied using two sources: the Maison Départementale desPersonnes Handicapées (MDPH) (1/3 cases) and the De-partment of Education (2/3 cases). Data on pregnancy,birth, medical and familial history, associated clinicalsigns, as well as any known etiologies and risk factorswere collected from the families.
For all these patients, first-line genetic tests includ-ing peripheral blood karyotypes, fragile X syndromemutation analyses, and subtelomeric studies using mul-tiplex ligation-dependent probe amplification (MLPA)were noncontributory. Other common causes of intel-lectual disability (infectious, traumatic, toxic…) werealso discarded. All samples were obtained from sub-jects after an institutional review board approved in-formed consent (DGS 2004/0341).
Array-CGH
Array-CGH was performed using an 180,000-oligonucleotidemicroarray (Human Genome CGH Microarray Kit 180K,Agilent Technologies, Santa Clara, CA) and following themanufacturer’s instructions. The average spacing of theprobes is 13 kb and the average genomic resolution is about30 kb. DNA from the patient was compared with DNA fromtwo other patients with different diseases, according to theloop model [19]. Genomic Workbench software, standardedition 6.5 (Agilent), was used to interpret the results withthe following parameters: aberration algorithm ADM-2,threshold 6.0, fuzzy zero, centralisation, and moving averagewindow 0.5–1 Mb. A copy number variation (CNV) wasnoted if at least three contiguous oligonucleotides showed anabnormal log2 ratio (> +0.58 or < −1 according to the Alexa 5deviation) with a mirror image. The Database of GenomicVariants (DGV; http://projects.tcag.ca/variation/) andDatabase of Chromosomal Imbalance and Phenotype inHumans Using Ensembl Resources (DECIPHER; http://decipher.sanger.ac.uk) were used to compare findings topreviously reported studies. Coordinates of all variations orprobes are based on the UCSCGRCh37/hg19 assembly http://genome.ucsc.edu/. All CNVs reported in this study weresubsequently submitted to DECIPHER.
Array-CGH confirmation methods
FISH analyses and home-made MLPA kits were used toconfirm the array-CGH results in the proband and to test theparents, if available.
FISH analyses were performed on metaphase chromo-somes with specific FISH probes located in the detectedCNVs.
When FISH analyses could not be performed (smallCNVs, small duplications, no FISH probes available),synthetic custom MLPA probes specific for the genesincluded in the CNVs were designed according to therecommendation of the MRC-Holland synthetic protocol(www.mlpa.com). In addition, four MLPA control probesspecific to the OCRL1 gene were included as controlprobes for a proper copy number quantification (www.omim.org). Information about sequences and ligation sitesof these control probes can be obtained [5]. All MLPAand FISH probes used in this study are listed in theSupplementary Table 1 (online).
Results
A total of 24 nonpolymorphic CNVs were found in 20 of66 patients (~30 %; Table 1). We classified the detectedCNVs into two groups. The first group contains nineCNVs identified in eight patients and have been consid-ered to be clinically relevant and responsible for the ID(Table 2). In one case, two pathogenic CNVs were detect-ed. All these nine pathogenic CNVs were greater than500 kb including eight CNVs over 1 Mb. No CNV waslarger than 3 Mb and more than half were genomic du-plications (6/9, 67 %). In this group, we identified eightknown recurrent rearrangements: deletions 2q13, 15q13.3,22q11.2, and duplications 1q21.1q21.2, 7q11.23, 16p11.2,16p13.11, and 22q11.2.
The second group consists of 15 CNVs of unknownclinical significance (VUS) identified in 13 patients thatare demonstrated to be neither clearly pathogenic norclearly benign (Table 3). Eleven CNVs (73 %) weresmaller than 400 kb and 9 (60 %) were genomic duplica-tions. One patient harbored a VUS coupled with anotherpathogenic CNV and two patients had two VUS. Accord-ing to the American College of Medical Genetics guide-lines [16], VUS were subclassified into three groups:likely pathogenic, likely benign, and undetermined. SevenCNVs were considered to be potentially causative becausethey contain interesting candidate genes that may contrib-ute to the patients’ phenotype and/or were previouslyreported in single cases. Conversely, seven VUS weresubclassified as likely benign variations (not previously
Eur J Pediatr

Tab
le1
Alldetected
CNVs(excluding
well-know
nbenign
CNVs)in
patientsandtheirclinicalfeatures
associated
tomild
intellectuald
isability
Patients
Gender
aCGHresults
(hg19)
Associatedclinicalfeatures
(other
than
mild
ID)
Neuropsychologicald
isturbances
Organic
malform
ations
Dysmorphicfeatures
Other
features
1M
arrXq23q24(115,007,250-116,707,313)
x0,11q24.2(124,452,935-124,909,868)x1
Difficulty
concentrating
–Elongated
face,leftsingle
palm
arcrease
Plagiocephaly
2M
arr15q13.2q13.3(30,943,903-32,438,943)x1
––
–Macrocephaly,esotropia,
myopia,encopresia
3M
arr16q23.3(82,950,213-83,277,559)x1
––
––
4F
arr1p35.3(28,743,173-28,764,436)x1
Selfinjuriousbehavior,
difficulty
concentrating
Preaxialhexadactyly
oftherighth
and
Shortp
hiltrum
,bilateral
clinodactyly
offifthfingers,
smalld
ysplastic
ears,
coarse
facies
Sleepdisturbances;
invitrofertilizatio
n
5F
arr22q11.2(18,894,835-21,464,119)x1
–Sm
allV
SDLarge
nasalroot
Neonatalh
ypocalcemia
6M
arr4q21.23q21.3(86,883,886-86,905,002)x1
Hyperactiv
ity,autistic
behaviors
––
–
7M
arr2q13(111,399,243-113,102,594)x1
Initiallanguage
delay,im
pulsiveness
–Prom
inentfetalpads
–
8F
arr14q23.1(61,316,974-61,430,524)x3
––
––
9M
arr15q13.3(32,021,733-32,438,943)x3
–Ectopialentis
Dow
n-turned
cornersof
mouth,smalld
ysplastic
ears,
evertedlower
lip
Marfandisease
10M
arr16p11.2(29,560,500-30,104,842)x3
Aggressiveness,im
pulsiveness,
difficulty
inestablishing
social
contact,difficulty
concentrating
–Archedeyebrows,malar
hypoplasia
Slim
habitus
11M
arr16p13.11(15,048,751-
16,267,306)x3,16q12.1(49,722,191-
49,812,039)x1
––
Large
incisors
–
12M
arr17q23.3q24.1(62,464,706-62,645,411)x3
––
––
13M
arr1q21.1q21.2(146,506,310-148,936,712)x3
––
Leftsinglepalm
arcrease,
smallh
ands,upturnednose,
flatphiltrum
–
14M
arr1q42.13(228,806,180-228,964,923)x3
Difficulty
concentrating,im
pulsiveness
––
–
15F
arr1q43(239,983,019-242,987,796)x3
Initiallanguage
delay,hyperactivity
–Blepharophimosis,flatp
hiltrum
IUGR,leftn
ystagm
us
16M
arr3q25.1(150,966,686-151,114,133)x3
Initiallanguage
delay
––
–
14F
arr4p13(42,426,912-42,526,844)x3,6q27
(166,340,714-166,704,715)x3
––
––
18M
arr5p15.33(1,842,451-2,916,776)x3
––
Flatphiltrum
Initialmotor
delay
19M
arr7q11.23(72,745,047-74,139,390)
x3,22q11.21(18,894,
835-21,464,119)x3
–Ectopictestis
Cleftpalate,m
idface
hypoplasia,
depressednasalb
ridge,microphtalm
ia,
microstom
ia,thinupperlip
,overfolded
helix
,absentear
lobes
–
20F
arr7q22.1(98,436,870-98,598,685)x3
––
––
IDintellectualdisability,V
SDventricularseptaldefect,IU
GRintrauterine
grow
threstriction,−absentsign,M
male,Ffemale.Coordinates
ofallvariatio
nsarebasedon
theUCSC
GRCh37/hg19
assembly
Eur J Pediatr

associated with ID, reported in a very small number ofcases in databases of variation in the general population,no strong candidate gene evidences, or were inheritedfrom a healthy parent). Last, one CNV was undeterminedbecause CNV is described in contradictory publicationsand databases.
The inheritance status was available only for seven CNVs(21 %): five CNVs were inherited from a healthy parent andtwo were de novo.
Discussion
We found one or more CNVs in 20 out of 66 (~30 %) patientswith a mild ID. In eight of them, the CNVs were certainlyresponsible for the phenotype and in six they were potentially pathogenic for ID. Altogether, array-CGH helped to determine the etiology of ID in 14 patients(~21 %). Very few recent data are available concerning thedetailed genetic etiologies of patients with mild ID. A genetic
Table 2 Detected pathogenic CNVs in patients
Patients Detected pathogenic CNVs
Nature Region Coordinates Size Inheritance MIM or publication(if applicable)
2 Deletion 15q13.2q13.3 chr15:30,943,903-32,438,943 1.5 Mb Mat 612001
5 Deletion 22q11.2 chr22:18,894,835-21,464,119 2.5 Mb Unknown 192430
7 Deletion 2q13 chr2:111,399,243-113,102,594 1.7 Mb Unknown [40]
10 Duplication 16p11.2 chr16:29,560,500-30,104,842 544 kb Unknown 614671
11 Duplication 16p13.11 chr16:15,048,751-16,267,306 1.2 Mb Unknown [24, 33, 34]
13 Duplication 1q21.1q21.2 chr1:146,506,310-148,936,712 1.3 Mb Unknown 612475
15 Duplication 1q43 chr1:239,983,019-242,987,796 3 Mb Unknown
19 Duplication 7q11.23 chr7:72,745,047-74,139,390 1.4 Mb Not mat 609757
Duplication 22q11.2 chr22:18,894,835-21,464,119 2.6 Mb Mat 608363
mat Maternal. Coordinates of all variations are based on the UCSC GRCh37/hg19 assembly
Table 3 Detected variants of unknown signification (VUS) in patients
Patients Detected VUS
Nature Region Coordinates Size Inheritance Genes Classification
1 Deletion Xq23q24 chrX:115,007,250-116,707,313 1.7 Mb De novo AGTR2 Likely pathogenic
Deletion 11q24.2 chr11:124,452,935-124,909,868 457 kb De novo HEPACAM Likely pathogenic
3 Deletion 16q23.3 chr16:82,950,213-83,277,559 327 kb Unknown CDH13 Likely pathogenic
4 Deletion 1p35.3 chr1:28,743,173-28,764,436 21 kb Unknown PHACTR4 Likely benign
6 Deletion 4q21.23q21.3 chr4:86,883,886-86,905,002 21 kb Mat ARHGAP24 Likely pathogenic
8 Duplication 14q23.1 chr14:61,316,974-61,430,524 114 kb Unknown MNAT1 Likely benign
9 Duplication 15q13.3 chr15:32,021,733-32,438,943 417 kb Unknown CHRNA7 Likely pathogenic
11 Deletion 16q12.1 chr16:49,722,191-49,812,039 89 kb Unknown ZNF423 Undetermined
12 Duplication 17q23.3q24.1 chr17:62,464,706-62,645,411 181 kb Unknown POLG2, DDX5,CEP95, SMURF2,MIR3064, MIR5047
Likely benign
14 Duplication 1q42.13 chr1:228,806,180-228,964,923 159 kb Unknown RHOU Likely benign
16 Duplication 3q25.1 chr3:150,966,686-151,114,133 147 kb Unknown MED12L, P2RY12,P2RY13, P2RY14,GPR87
Likely pathogenic
17 Duplication 4p13 chr4:42,426,912-42,526,844 100 kb Mat ATP8A1 Likely benign
Duplication 6q27 chr6:166,340,714-166,704,715 364 kb Mat TFT Likely benign
18 Duplication 5p15.33 chr5:1,842,451-2,916,776 1.05 Mb Unknown IRX2, IRX4, c5orf38 Likely benign
20 Duplication 7q22.1 chr7:98,436,870-98,598,685 162 kb Unknown TMEM130, TRRAP,MIR3609
Likely pathogenic
mat Maternal. Boldface indicates the best candidate genes. Coordinates of all variations are based on the UCSC GRCh37/hg19 assembly
Eur J Pediatr

cause used to be found in about 15 % of patients with mild ID[11]. Our diagnosis rate is similar to the global diagnosis rateof 15–20% obtained in different large array-CGH studies [17,20, 26, 30]. This detection rate reaches 20–25 % in studiesregrouping children with moderate and/or severe intellectualdisability, particularly if associated with dysmorphic features,birth defects, or epilepsy [3]. Our diagnosis rate is surprisingin a cohort of patients with mild ID with subtle associatedclinical features. In fact, the frequency of causative abnormal-ities among these patients is expected to be still significant butcertainly substantially less as compared to the more severephenotypes [3]. One first explanation is the resolution level ofthe array and the retained cut-off to define a CNV. In ourstudy, we have decided to consider a CNV if at least threecontiguous oligonucleotides showed an abnormal log2 ratio.Therefore, we retained nine CNVs smaller than 200 kb in sizeamong which three were classified as potentially pathogenicVUS. A second explanation could be the large clinical spec-trum of different syndromes due to an extreme variable ex-pressivity. Thus, some patients carrying the same pathogenicvariation could present with a mild or more severe ID. On the
other hand, in a large cohort of 256 patients with heteroge-neous severity level for ID, Bartnik et al. [2] found a causativeCNV in about 30 % of the 32 patients with mild ID. Theseheterogeneous results highlight the variability of the patientgroups, the recruitment bias, and the different chromosomalmicroarray technologies. A more consensual methodologywould help to standardize chromosomal microarray studies.
Among all the detected CNVs, 62 % (15/24) wereclassified as a VUS and most of them were small CNVs(73 % lower than 400 kb) and duplications (60 %). Usu-ally, but not uniformly, small CNVs and duplications aremore likely benign than deletions or large CNVs [20].However, we would like to discuss four rare likely path-ogenic CNVs that may contribute in our opinion to thepatients’ phenotypes.
A 327-kb deletion identified in patient 3 includes partiallythe gene CDH13 (4 exons; Fig. 1a). CDH13 codes for T-cadherin belonging to the cadherin family, a group of genesencoding calcium-dependent cell adhesion molecules.CDH13 is highly expressed in the brain and plays, amongother functions, a critical role in the regulation of brain
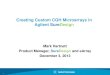
Fig. 1 Array-CGH profiles of selected potential clinical relevant VUSdetected in patient 3, 6, 16, and 20. a Patient 3, showing a 327-kb deletionin 16q23.3 (chr16:82,950,213-83,277,559, NCBI hg19); b patient 6,demonstrating a small 21-kb deletion at 4q21.21q13 (chr4:86,883,886-
86,905,002, NCBI hg19); c patient 16, showing a rare 147-kb duplicationin 3q25.1 (chr3:150,966,686-151,114,133, NCBI hg19); d patient 20,harboring a 162-kb duplication at 7q22.1 (chr7:98,436,870-98,598,685,NCBI hg19)
Eur J Pediatr

network development, plasticity, and function. Linkage stud-ies associated the CDH13 locus with attention deficit/hyperactivity disorder (ADHD) and related neuropsychiatricconditions [9, 18, 25]. The patient 3 presents with ADHD andtherefore we suggest that this deletion in the CDH13 gene isprobably pathogenic for the described clinical features.
In patient 6, we identified a small maternally inheriteddeletion including three exons of the ARHGAP24 gene(Fig. 1b). ARHGAP24 encodes a negative regulator ofRho GTPases, which is implicated in axon and dendriteou tg rowth and b ranch ing [14 , 21 ] . Recen t ly,Wiśniowiecka-Kowalnik et al. [36] identified a de novo1-Mb deletion including only the ARHGAP24 gene in apatient with autism, speech delay, and abnormal EEG. Inaddition to others observations reported in literature anddatabases, authors proposed ARHGAP24 to be a goodcandidate gene for ID and/or autism spectrum disorders.However, some polymorphic deletions including totally orpartially ARHGAP24 are reported in the DGV database[39] and the deletion detected in our patient is inheritedfrom a healthy mother. Although there is some evidencethat ARHGAP24 is a strong candidate gene to explain theID phenotype observed in our patient, further studies arerequired to determine the exact pathogenic effect resultingfrom this deletion.
We also identified a 147-kb duplication at 3q25.1 inpatient 16 presenting with mild ID and language delay(Fig. 1c). This duplication contains five genes: GPR87, acluster of three P2RY genes encoding purinergic P2Yreceptors (P2YR12, P2YR13, and P2YR14) and MED12L(21 exons). The duplication partially includes theMED12L gene, suggesting that the function of the genemay be disrupted. The MED12L gene encodes a subunitof the Mediator complex, which is involved in transcrip-tional coactivation of nearly all RNA polymerase II-dependent genes [27]. Mutations in MED12, the paraloggene of MED12L, are associated with three different IDsyndromes: Lujan-Fryns syndrome (MIM 309520),Opitz–Kaveggia syndrome (FG syndrome, MIM305450), and Ohdo syndrome (MIM 300895). Moreover,other members of the mediator complex like MED13,MED13L, MED17, and MED23 were formally linked toseveral disorders in patients presenting with ID [1, 4, 12,15, 28]. These findings highlight the central key role ofthe mediator complex in the development of the nervoussystem. In DECIPHER, another patient (ID 284908) har-bors a de novo 457-kb duplication in 3q25.1 overlappingalmost all the duplicated region described in our patient.This duplication includes the same five genes and patient284908 presents also with intellectual disability. Overall,these data suggest that our identified aberration is likelypathogenic and that the MED12L gene appears to be themost important candidate gene for the ID in this region.
More patients with a 3q25.1 duplication would strengthenthe genotype-phenotype correlation.
A small 161-kb duplication in 7q22.1 encompassing twogenes, TMEM130 and TRRAP, was identified in patient 20with only mild ID (Fig. 1d). TRRAP gene encodes a largemultidomain protein of the phosphoinositide 3-kinase-relatedkinases family. Germline mutations were associated withASD and schizophrenia [22, 38]. TMEM130 encodes a trans-membrane protein, which contains a polycystic kidneydisease-related domain. In a patient with intellectual disabilityand autism carrying a balanced translocation involving chro-mosomes 6 and 7, Vincent et al. [35] pointed out theTMEM130 as a potential candidate gene at the breakpointson 7q22. Two other larger duplications within this region werereported in patients with intellectual disability (DECIPHERID 254639 and 283603). Although, the phenotype correlationremains unclear, we propose that the duplication identified inthe 7q22.1 region could contribute to the clinical featuresobserved in our patient.
Unfortunately, inheritance status of almost all CNVswas unavailable. This could be mainly explained by themild phenotype, the well-preserved adaptive skills, and bythe fact that parents sometimes are in denial about theirchild’s disability or are not aware of the problems thechild encounters. The information about the inheritancestatus would have been useful to interpret the detectedCNVs and in particular VUS.
We identified four patients carrying multiple CNVs with inparticular the patient 19 harboring two pathogenic CNVs. Infact, in patient 19, we found a maternally inherited 1.4-Mbduplication in 7q11.23 associated to a 2.57-Mb duplication inthe 22q11.21 region. For this second duplication, maternalsample revealed normal result; unfortunately, the paternalsample was unavailable. Some clinical features reported inour patient (Table 1) like cleft palate or malar hypoplasiashould be likely related to the 22q11 duplication [23] whileothers like thin upper lips and ear abnormalities are mostlikely related to the 7q11.23 duplication [8]. This compoundphenotype supports the fact that multiple CNVs contribute toan atypical and complex phenotype [10]. Overall, it empha-sizes the difficulty to precise the genotype phenotype correla-tion in patients with multiple CNVs and in particular theinvolvement of each CNVs in the intellectual disability.
Conclusion
In summary, we present an original study regarding thehomogeneous recruitment of patients based solely on theevidence of a mild ID. We found an unexpectedly highpathogenic CNVs detection rate in this cohort rangingfrom 12 to 21 % including likely pathogenic VUS. Ourresults underscore the clinical relevance of array-CGH to
Eur J Pediatr

investigate the etiology of isolated idiopathic mild ID inpatients or associated with even subtle dysmorphic fea-tures or congenital malformations.
Acknowledgments We thank family members for their interest andcooperation. This study was supported by grants from the French Minis-try (DHOS).
Conflict of interest None
Parental consent Granted
References
1. Asadollahi R, Oneda B, Sheth F, Azzarello-Burri S, Baldinger R,Joset P, Latal B, Knirsch W, Desai S, Baumer A, Houge G, AndrieuxJ, Rauch A (2013) Dosage changes of MED13L further delineate itsrole in congenital heart defects and intellectual disability. Eur J HumGenet 21:1100–1104
2. Bartnik M, Nowakowska B, Derwińska K, Wiśniowiecka-KowalnikB, Kędzior M, Bernaciak J, Ziemkiewicz K, Gambin T, Sykulski M,Bezniakow N, Korniszewski L, Kutkowska-Kaźmierczak A,Klapecki J, Szczałuba K, Shaw CA, Mazurczak T, Gambin A,Obersztyn E, Bocian E, Stankiewicz P (2014) Application of arraycomparative genomic hybridization in 256 patients with develop-mental delay or intellectual disability. J Appl Genet 55:125–144
3. Beaudet AL (2013) The utility of chromosomal microarray analysisin developmental and behavioral pediatrics. Child Dev 84:121–132
4. Boutry-Kryza N, Labalme A, Till M, Schluth-Bolard C, Langue J,Turleau C, Edery P, Sanlaville D (2012) An 800 kb deletion at17q23.2 including the MED13 (THRAP1) gene, revealed by aCGHin a patient with a SMC 17p. Am J Med Genet A 158A:400–405
5. Coutton C, Monnier N, Rendu J, Lunardi J (2010) Development of amultiplex ligation-dependent probe amplification (MLPA) assay forquantification of the OCRL1 gene. Clin Biochem 43:609–614
6. David M, Dieterich K, Billette de Villemeur A, Jouk PS, Counillon J,Larroque B, Bloch J, Cans C (2014) Prevalence and characteristics ofchildrenwith mild intellectual disability in a French county. J IntellectDisabil Res
7. des Portes V, Livet MO, Vallée L, Groupe de travail de la Sociétéfrançaise de neuropédiatrie (SFNP) sur les retards mentaux (2002) Apractical diagnostic approach to mental deficiency in 2002. ArchPediatr 9:709–725
8. Dixit A, McKee S, Mansour S, Mehta SG, Tanteles GA,Anastasiadou V, Patsalis PC, Martin K, McCullough S, Suri M,Sarkar A (2013) 7q11.23 Microduplication: a recognizable pheno-type. Clin Genet 83:155–161
9. FrankeB, Faraone SV,Asherson P, Buitelaar J, BauCH,Ramos-QuirogaJA, Mick E, Grevet EH, Johansson S, Haavik J, Lesch KP, Cormand B,Reif A (2012) International Multicentre persistent ADHDCollaboration.The genetics of attention deficit/hyperactivity disorder in adults, a review.Mol Psychiatry 17:960–987
10. Girirajan S, Rosenfeld JA, Coe BP, Parikh S, Friedman N, GoldsteinA, Filipink RA, McConnell JS, Angle B, Meschino WS, NezaratiMM, Asamoah A, Jackson KE, Gowans GC, Martin JA, CarmanyEP, Stockton DW, Schnur RE, Penney LS, Martin DM, Raskin S,Leppig K, Thiese H, Smith R, Aberg E, Niyazov DM, Escobar LF,El-Khechen D, Johnson KD, Lebel RR, Siefkas K, Ball S, Shur N,McGuire M, Brasington CK, Spence JE, Martin LS, Clericuzio C,Ballif BC, Shaffer LG, Eichler EE (2012) Phenotypic heterogeneityof genomic disorders and rare copy-number variants. N Engl J Med367:1321–1331
11. Hagberg B, Kyllerman M (1983) Epidemiology of mental retarda-tion—a Swedish survey. Brain Dev 5:441–449
12. Hashimoto S, Boissel S, Zarhrate M, Rio M, Munnich A, Egly JM,Colleaux L (2011) MED23 mutation links intellectual disability todysregulation of immediate early gene expression. Science 333:1161–1163
13. Hatton C (2012) Intellectual disabilities – Classification, epidemiol-ogy and causes. Clinical Psychology and People with IntellectualDisabilities, Second Edition, Chapter 1:3–22
14. Katoh Y, Katoh M (2004) Identification and characterization ofARHGAP27 gene in silico. Int J Mol Med 14:943–947
15. Kaufmann R, Straussberg R, Mandel H, Fattal-Valevski A, Ben-ZeevB, Naamati A, Shaag A, Zenvirt S, Konen O, Mimouni-Bloch A,Dobyns WB, Edvardson S, Pines O, Elpeleg O (2010) Infantilecerebral and cerebellar atrophy is associated with a mutation in theMED17 subunit of the transcription preinitiation mediator complex.Am J Hum Genet 87:667–670
16. Kearney HM, Thorland EC, Brown KK, Quintero-Rivera F, SouthST, Working Group of the American College of Medical GeneticsLaboratory Quality Assurance Committee (2011) American Collegeof Medical Genetics standards and guidelines for interpretation andreporting of postnatal constitutional copy number variants. GenetMed 13:680–685
17. Lu XY, Phung MT, Shaw CA, Pham K, Neil SE, Patel A, SahooT, Bacino CA, Stankiewicz P, Kang SH, Lalani S, Chinault AC,Lupski JR, Cheung SW, Beaudet AL (2008) Genomic imbal-ances in neonates with birth defects: high detection rates byusing chromosomal microarray analysis. Pediatrics 122:1310–1318
18. Mavroconstanti T, Johansson S, Winge I, Knappskog PM, Haavik J(2013) Functional properties of rare missense variants of humanCDH13 found in adult attention deficit/hyperactivity disorder(ADHD) patients. PLoS One 8:e71445
19. Menten B, Maas N, Thienpont B, Buysse K, Vandesompele J,Melotte C, de Ravel T, Van Vooren S, Balikova I, Backx L,Janssens S, De Paepe A, De Moor B, Moreau Y, Marynen P, FrynsJP, Mortier G, Devriendt K, Speleman F, Vermeesch JR (2006)Emerging patterns of cryptic chromosomal imbalance in patientswith idiopathic intellectual disability and multiple congenital anom-alies: a new series of 140 patients and review of published reports. JMed Genet 43:625–633
20. Miller DT, Adam MP, Aradhya S, Biesecker LG, Brothman AR,Carter NP, Church DM, Crolla JA, Eichler EE, Epstein CJ, FaucettWA, Feuk L, Friedman JM, Hamosh A, Jackson L, Kaminsky EB,Kok K, Krantz ID, Kuhn RM, Lee C, Ostell JM, Rosenberg C,Scherer SW, Spinner NB, Stavropoulos DJ, Tepperberg JH,Thorland EC, Vermeesch JR, Waggoner DJ, Watson MS, MartinCL, Ledbetter DH (2010) Consensus statement: chromosomal mi-croarray is a first-tier clinical diagnostic test for individuals withdevelopmental disabilities or congenital anomalies. Am J HumGenet 86:749–764
21. Nguyen LS, Jolly L, Shoubridge C, Chan WK, Huang L,Laumonnier F, Raynaud M, Hackett A, Field M, Rodriguez J,Srivastava AK, Lee Y, Long R, Addington AM, Rapoport JL,Suren S, Hahn CN, Gamble J, Wilkinson MF, Corbett MA, Gecz J(2012) Transcriptome profiling of UPF3B/NMD-deficientlymphoblastoid cells from patients with various forms of intellectualdisability. Mol Psychiatry 17:1103–1115
22. O'Roak BJ, Vives L, Girirajan S, Karakoc E, Krumm N, Coe BP,Levy R, Ko A, Lee C, Smith JD, Turner EH, Stanaway IB, Vernot B,Malig M, Baker C, Reilly B, Akey JM, Borenstein E, Rieder MJ,Nickerson DA, Bernier R, Shendure J, Eichler EE (2012) Sporadicautism exomes reveal a highly interconnected protein network of denovo mutations. Nature 485:246–250
23. Portnoï MF (2009) Microduplication 22q11.2: a new chromosomalsyndrome. Eur J Med Genet 52:88–93
Eur J Pediatr

24. Ramalingam A, Zhou XG, Fiedler SD, Brawner SJ, Joyce JM,Liu HY, Yu S (2011) 16p13.11 duplication is a risk factor for awide spectrum of neuropsychiatric disorders. J Hum Genet 56:541–544
25. RiveroO, Sich S, Popp S, Schmitt A, Franke B, LeschKP (2013) Impactof the ADHD-susceptibility gene CDH13 on development and functionof brain networks. Eur Neuropsychopharmacol 23:492–507
26. Sagoo GS, Butterworth AS, Sanderson S, Shaw-Smith C, Higgins JP,Burton H (2009) Array CGH in patients with learning disability(mental retardation) and congenital anomalies: updated systematicreview and meta-analysis of 19 studies and 13,926 subjects. GenetMed 11:139–146
27. Sato S, Tomomori-Sato C, Parmely TJ, Florens L, Zybailov B,Swanson SK, Banks CA, Jin J, Cai Y, Washburn MP, ConawayJW, Conaway RC (2004) A set of consensus mammalian mediatorsubunits identified by multidimensional protein identification tech-nology. Mol Cell 14:685–691
28. Schwartz CE, Tarpey PS, Lubs HA, Verloes A, May MM, Risheg H,Friez MJ, Futreal PA, Edkins S, Teague J, Briault S, Skinner C,Bauer-Carlin A, Simensen RJ, Joseph SM, Jones JR, Gecz J,Stratton MR, Raymond FL, Stevenson RE (2007) The originalLujan syndrome family has a novel missense mutation (p.N1007S)in the MED12 gene. J Med Genet 44:472–477
29. Simonoff E, Pickles A, Chadwick O, Gringras P, Wood N, Higgins S,Maney JA, Karia N, Iqbal H, Moore A (2006) The Croydon assess-ment of learning study: prevalence and educational identification ofmild mental retardation. J Child Psychol Psychiatry 47:828–839
30. Stankiewicz P, Beaudet AL (2007) Use of array CGH in the evalu-ation of dysmorphology, malformations, developmental delay, andidiopathic mental retardation. Curr Opin Genet Dev 17:182–192
31. Stromme P, Valvatne K (1998) Mental retardation in Norway: prev-alence and sub-classification in a cohort of 30037 children bornbetween 1980 and 1985. Acta Paediatr 87:291–296
32. Tassé MJ, Luckasson R, Nygren M (2013) AAIDD proposed recom-mendations for ICD-11 and the condition previously known as men-tal retardation. Intellect Dev Disabil 51:127–131
33. Tropeano M, Ahn JW, Dobson RJ, Breen G, Rucker J, Dixit A, PalDK,McGuffin P, Farmer A,White PS, Andrieux J, Vassos E, OgilvieCM, Curran S, Collier DA (2013) Male-biased autosomal effect of16p13.11 copy number variation in neurodevelopmental disorders.PLoS One 8:e61365
34. Ullmann R, Turner G, Kirchhoff M, ChenW, Tonge B, Rosenberg C,Field M, Vianna-Morgante AM, Christie L, Krepischi-Santos AC,Banna L, Brereton AV, Hill A, Bisgaard AM, Müller I, Hultschig C,Erdogan F, Wieczorek G, Ropers HH (2007) Array CGH identifiesreciprocal 16p13.1 duplications and deletions that predispose toautism and/or mental retardation. Hum Mutat 28:674–682
35. Vincent JB, Choufani S, Horike S, Stachowiak B, Li M, Dill FJ,Marshall C, Hrynchak M, Pewsey E, Ukadike KC, Friedman JM,Srivastava AK, Scherer SW (2008) A translocation t(6;7)(p11-p12;q22) associated with autism and mental retardation: localizationand identification of candidate genes at the breakpoints. PsychiatrGenet 18:101–109
36. Wiśniowiecka-Kowalnik B, Kastory-Bronowska M, Bartnik M,Derwińska K, Dymczak-Domini W, Szumbarska D, Ziemka E,Szczałuba K, Sykulski M, Gambin T, Gambin A, Shaw CA,Mazurczak T, Obersztyn E, Bocian E, Stankiewicz P (2013)Application of custom-designed oligonucleotide array CGH in 145patients with autistic spectrum disorders. Eur J HumGenet 21:620–625
37. World Health Organization (2001) International classification of func-tioning, disability and health. World Health Organization, Geneva
38. Xu B, Ionita-Laza I, Roos JL, Boone B, Woodrick S, Sun Y, Levy S,Gogos JA, Karayiorgou M (2012) De novo gene mutations highlightpatterns of genetic and neural complexity in schizophrenia. Nat Genet44:1365–1369
39. Xu H, PohWT, Sim X, Ong RT, Suo C, TayWT, Khor CC, SeielstadM, Liu J, Aung T, Tai ES, Wong TY, Chia KS, Teo YY (2011) SgD-CNV, a database for common and rare copy number variants in threeAsian populations. Hum Mutat 32:1341–1349
40. YuHE,HawashK, Picker J, Stoler J, UrionD,WuBL, ShenY (2012) Arecurrent 1.71 Mb genomic imbalance at 2q13 increases the risk ofdevelopmental delay and dysmorphism. Clin Genet 81:257–264
Eur J Pediatr