-
ti
Foad Abd-Allah c, Mohammad A. FGamaleldin Osman b, Shady S. Geoa
HealthPartners Clinics and Services Department of Neuroscb Ain
Shams University Department of Neurology, Cairo, Egyc Cairo
University, Kasralainy School of Medicine, Neurologyd Cedars-Sinai
Department of Neurology, Los Angeles, CA, Un
ed in 1994 [4]. It hasials and practice [57].
Journal of the Neurological Sciences xxx (2015) xxxxxx
JNS-13921; No of Pages 5
Contents lists available at ScienceDirect
Journal of the Neur
j ourna l homepage: www.e1. Introduction trial [3]. The current
version was rst publishsince become an integral part of stroke
clinical trResults: In 6months, 137 patientswere recruited (mean
age standard deviation 6212 years; 48women). Forinterrater
agreement, weighted kappa value ranged from 0.36 to 0.66 and
intraclass correlation coefcient (ICC)for the whole scale was
excellent at 0.95 (95% condence interval [CI] 0.940.97). For
intrarater agreement,weighted kappa ranged from 0.52 to 1.0 and the
ICC was 0.94 (95% CI 0.870.98). The construct validity ofthe
arNIHSS is demonstrated by its correlation with the DWI-ASPECT and
the 3 months mRS score (Spearmancorrelation0.46 and 0.58
respectively; P b 0.001 for both).Conclusion: We developed and
validated a culturally adapted Arabic version of the NIHSS. Further
validation inother Arab countries is recommended.
2015 Elsevier B.V. All rights reserved.The original NIH Stroke
Scale (NIHSS) wassity of Cincinnati [1,2] and subsequently mod
Funding source: None. Corresponding author at: HealthPartners
Clinics a
St. Paul, MN 55130, United States.E-mail address:
[email protected]
http://dx.doi.org/10.1016/j.jns.2015.07.0220022-510X/ 2015
Elsevier B.V. All rights reserved.
Please cite this article as: H.M. Hussein, et aNeurol Sci
(2015), http://dx.doi.org/10.1016evaluated by correlating the
arNIHSS on admission with the infarct volume on initial the
diffusion weightedimaging (DWI) using the Alberta Stroke Program
Early CT score (DWI-ASPECTS) and the functional outcomeat 3 months
assessed by the modied Rankin Scale (mRS).Stroke severityArticle
history:Received 5 March 2015Received in revised form 20 June
2015Accepted 10 July 2015Available online xxxx
Keywords:NIHSSCross-culturalTranslationArabicIschemic
strokeNeurological examinationStroke scale
Introduction: The National Institutes of Health Stroke Scale
(NIHSS), the most commonly used tool to quantifyneurological decit
in acute stroke, was initially developed in English. We present our
experience in developingand validating an Arabic version of the
NIHSS (arNIHSS).Methods:
A) Scale development phase: 6 bilingual neurologists translated
the scale to Arabic. Items 9 and 10 weremodied to suit the Arabic
language and culture. A panel of 11 Arab neurologists reviewed the
nal productand an Arabic language expert did nal editing.
B) Scale validation phase: 10 examiners (four neurology
residents and six nurses), who had no experiencewith the NIHSS,
were trained to use the arNIHSS. Patients with acute stroke were
recruited at two academicinstitutions in Egypt. Each patient was
examined on admission by 3 examiners using the arNIHSS and at24
hours by one of the three examiners. The agreement between the rst
three examinations was used tocalculate the interrater agreement.
The agreement between the admission and the 24-hour arNIHSS
per-formed by the same examiner was used to calculate the
intrarater agreement. Construct validity wasa b s t r a c ta r t i
c l e i n f ol Moneim b, Tamer Emara b, Yousry A. Abd-elhamid b,
Haitham H. Salem b,arrag c, M. Amir Tork b, Ali S. Shalash b,
Khaled H. Ezz el dein b,rgy b, Peter G. Ghali b, Patrick D. Lyden
d, Ramez R. Moustafa b
iences, St Paul, MN, United StatesptDepartment, Cairo, Egyptited
StatesHaitham M. Hussein a,, Amr Abdeof Health Stroke Scale
Arabic cross cultural adaptation and validadeveloped at the
Univer-ied for the NINDS rtPA
nd Services, 401 Phalen Blvd.,
om (H.M. Hussein).
l., Arabic cross cultural adapta/j.jns.2015.07.022on of the
National Institutes
ological Sciences
l sev ie r .com/ locate / jnsUtilization of the NIHSS in
non-English-speaking countries is chal-lenging. The difference in
language may impair the examiner's abilityto understand the
instructions. The objects used to test aphasia initem 9 may not be
familiar in other cultures and the syllables used initem 10 maybe
foreign or inadequate to test for dysarthria in languagesother than
English. Several cross-cultural adaptations of the NIHSS
haveaddressed these issues in their respective cultures [814].
tion and validation of the National Institutes of Health Stroke
Scale, J
-
2 H.M. Hussein et al. / Journal of the Neurological Sciences xxx
(2015) xxxxxxThe aim of this study was to develop an Arabic version
of the NIHSS(arNIHSS). A culturally adapted Arabic version of the
NIHSS is neededto serve more than 200 million Arabic native
speakers; most of themdo not speak any other languages [15]. It
will be particularly usefulin standardizing acute stroke care
(initial assessment and monitoringof clinical progression)
performed by neurologists as well as non-neurologists (other
specialty physicians and non-physician providers).The
non-neurologists group is important given the rarity of
neurologistsin the Arab world, which has one neurologist per
100,000500,000population (much less than Europe and USAwhich have
approximately4 per 100,000 population) [16].
2. Methods
The study was performed in 2 phases. Phase 1 was to develop
thearNIHSS according to standard methods of cross-cultural
adaptation[17,18], and phase 2 was to validate it in an Arabic
speaking clinicalsetting.
2.1. Phase 1: arNIHSS scale development
Four bilingual neurologists translated the NIHSS to Arabic,
creatingthe rst draft of the arNIHSS by consensus. A fth bilingual
neurologistindependently back-translated the draft to English.
Another investiga-tor compared theNIHSSwith the back translation
andmade correctionsto the Arabic draft to reconcile discrepancies.
The following changeswere made to items 9, aphasia, and 10,
dysarthria (see online Supple-mentary material):
Cookie jar card: the word cookie on the jar was replaced by
itsArabic equivalentObject naming card: the original cardwas
replaced by the one devel-oped for the Spanish version of the NIHSS
[10] because it has objectsthat are more familiar to natives of the
Arabic world.Sentence reading card: except for minor modication in
the order ofwords to fulll the proper Arabic grammar, the original
sentenceswere translated word for word to maintain the meaning and
theincremental complexity of the original version.Word reading
card: we chose 6 words that would: a) test labial,lingual and
glottal sounds, b) include the phonemes that are uniqueto the
Arabic language, and c) be devoid of any cultural, social,
orreligious insinuations.
To ensure that the scale was comprehensible and acceptable in
thevarious Arab-speaking countries, the draft scale was sent to a
panel ofeleven bilingual Arab neurologists from eight different
Arab countries.Each neurologist independently reviewed and edited
the draft. Thesechangeswere incorporated into one draft. Finally,
an Arabic language ex-pert proofread the draft for spelling and
grammar mistakes, producingthe nal version of the arNIHSS (online
supplementarymaterial 1 and 2).
2.2. Phase 2: scale validation:
The goal of this phase was to assess a) the feasibility of
trainingArabic speaking examiners to use the arNIHSS and b) the
psychometriccharacteristics of the scale.
2.2.1. Training of examinersNeurology residents and nurses were
approached to participate
in the study. Those who had previous experience with the NIHSS
wereexcluded. Both study sites were allowed to design their own
trainingprogram provided that they follow these guidelines: a) the
trainingwould be provided by in Arabic by senior neurologists with
exten-sive experience in NIHSS, and b) the training would consist
of three
phases. Phase 1 involved explaining the purpose and use of the
NIHSS,
Please cite this article as: H.M. Hussein, et al., Arabic cross
cultural adaptaNeurol Sci (2015),
http://dx.doi.org/10.1016/j.jns.2015.07.022examination techniques
and scoring rules. Phase 2 focused on practic-ing the arNIHSS in
groups and individually on actors with real timefeedback and
discussion. Phase 3 allowed examiners to independentlypractice
arNIHSS on actual stroke patients. Scores were reviewed
andcorrected by the trainers. Examiners were admitted to the study
whenat least 75% of their score was correct.
2.2.2. Study subjectsPatients 18 years or older who were
admitted with ischemic stroke
to the stroke units of two academic institutions in Cairo, Egypt
(AinShams University Hospital and Cairo University Hospital) were
identi-ed. We excluded patients with hemorrhagic strokes,
thrombolytictreatment, and onset N48 hours from presentation.
2.2.3. Study protocolEach patientwas examined on admission three
separate times using
the arNIHSS by three different examiners. Each examinerwas
blinded tothe scores given by the other examiners. A fourth
examinationwas per-formed 24 hours later by one of those three
examiners.
For patients with anterior circulation stroke, recruited at Ain
ShamsUniversity Hospital, the diffusion weighted imaging (DWI)
sequenceof the admission brain magnetic resonance imaging (MRI) was
used tocalculate the infarct volume using themodication of the
Alberta StrokeProgram Early CT score (DWI-ASPECTS) [19,20]. Modied
Rankin Scale(mRS) was assessed through telephone interview at 3
months [21,22]by study investigators unaware of initial assessment.
The proceduresfollowed in this study were in accordance of
institutional guidelinesand the research authority at both academic
institutions and hospitalsapproved the study. All patients (or
their caregivers) consented to par-ticipate in the study.
2.2.4. Statistical analysisBaseline population characteristics
were reported using frequency
for categorical variables, mean standard deviation (SD) for
continu-ous variables, and median (interquartile range IQR) for
nonparamet-ric variables. The initial three examinations were used
to calculatethe interrater agreement. Weighted Kappa statistic was
calculatedfor individual arNIHSS items, and was categorized as
follows: poor ifb0.40, moderate if 0.40.75, and excellent if N0.75.
If the kappa ofNIHSS item is included within the 95% CI of its
corresponding item onthe arNIHSS, then the two kappaswere
considered to be not statisticallydifferent. The two examinations
done by the same examiner 24 hoursapart were used to calculate the
intrarater agreement. The intraclasscorrelation coefcient (ICC) was
also calculated but for the total scores.
To assess the construct validity of the arNIHSS, Spearman's
correla-tion was calculated between arNIHSS (total and individual
items) andDWI-ASPECTS, and between arNIHSS (total and individual
items) andmRS. For the construct validity correlations, we
calculated the averageof the initial three arNIHSS scores instead
of choosing the scores givenby one examiner, since none of the
initial scores represent the referenceor the gold standard.
All analytical procedureswere conducted using SPSS statistical
pack-ages version 18 (SPSS Inc.) and SAS (PC SAS 9.2, SAS Institute
Inc., Cary,North Carolina).
3. Results
3.1. Subjects' characteristics
A total of 137 patients were recruited into the study (mean
age62 12 years; 48 women). Ain ShamsUniversity Hospital
contributed117 patients and Cairo University Hospital contributed
20 patients(Table e-1). The median (IQR) arNIHSS score at admission
and at24 hours was the same 5 (8). Median (IQR) DWI-ASPECTS (n =
68)was 7 (410). The median (IQR) mRS at 3 months (n = 117) was
2 (05).
tion and validation of the National Institutes of Health Stroke
Scale, J
-
agreement (Table 2). In comparison with the NIHSS, which had
a
score was 0.94 (95% CI 0.870.98; Table 3) with no difference
betweennurses 0.94 (95% CI 0.861.0) and physicians 0.91 (95% CI
0.810.99).
outcome at 3 months as measured by mRS (Spearman correlation
0.58;P b 0.001; Fig. 2).
Table 3Intrarater agreement of the arNIHSS.
Component Kappa(median)
Interquartilerange
Agreementbeyond chance
LOC (1a) 0.52 0.030.93 ModerateLOC questions (1b) 0.81 0.711.00
ExcellentLOC command (1c) 1.00 0.731.00 ExcellentGaze (2) 1.00
1.001.00 ExcellentVisual Fields (3) 0.63 0.420.95 ModerateFacial
Weakness (4) 0.68 0.471.00 ModerateMotor left arm (5a) 0.79
0.620.85 ExcellentMotor right arm (5b) 0.65 0.450.95 ModerateMotor
left leg (6a) 0.76 0.550.97 ExcellentMotor right leg (6b) 0.90
0.631.00 ExcellentAtaxia (7) 0.77 0.511.00 ExcellentSensory (8)
0.56 0.140.68 ModerateAphasia (9) 1.00 0.681.00 ExcellentDysarthria
(10) 0.72 0.621.00 ModerateExtinction (11) 0.81 0.451.00
Excellent
ICC, Median Interquartile rangeTotal score 0.94 0.921.00
Excellent
arNIHSS: Arabic version of the NIH Stroke Scale; LOC: level of
consciousness.
Table 1Distribution of responses for arNIHSS components by the
initial three examinations.
Components Total responses(max = 411)
0 1 2 3 4
LOC (1a) 411 87.4 9.3 3.4 0 LOC questions (1b) 411 68.1 14.4
17.5 LOC Command (1c) 411 90.3 4.9 4.9 Gaze (2) 411 91.2 5.6 3.2
Visual Fields (3) 411 78.8 10.7 9.5 1 Facial Weakness (4) 411 34.1
45.3 18.2 1.5 Motor left arm (5a) 411 67.2 10.2 5.4 8.5 8.8Motor
right arm (5b) 411 75.9 11.7 3.7 3.4 5.4Motor left leg (6a) 411
61.1 11 11.7 11 5.4Motor right leg (6b) 411 65.5 13.6 10.7 7.1
3.2Ataxia (7) 411 68.9 23.6 7.5 Sensory (8) 411 52.6 44 3.4 Aphasia
(9) 408a 80.6 6.4 7.8 5.2 Dysarthria (10) 411 51.8 38.9 9.3
Extinction (11) 411 91.2 6.1 2.7
arNIHSS: Arabic version of the National Institutes of Health
Stroke Scale; LOC: level ofconsciousness.
a Item was untestable in 3 patients.
3H.M. Hussein et al. / Journal of the Neurological Sciences xxx
(2015) xxxxxxbroader distribution of agreement (2 excellent, 2
poor, and 11moderateagreement) the 95% CI of the kappa of all but
three items of the arNIHSSoverlapped with the Kappa of the NIHSS:
level of consciousnesscommands (item 1c) and visual eld (item 3)
better interrater agree-ment in favor of NIHSS [23], and ataxia
(item 7) in favor of arNIHSS.The ICC for the whole scale was
excellent at 0.95 (95% CI 0.940.97),which is similar to the NIHSS
ICC of 0.94 (95% CI 0.841.00) [23].Six nurses and four neurology
residents were recruited to the study(Table e-2). There were 411
responses recorded for each of the scaleitems on admission (137
patients 3 examiners) except for item9 (aphasia) for which only 408
responses were recorded because ofintubation of one patient.
Responses distributed throughout all possiblelevels for all items
except level 3 for item 1a (see Table 1). At 24 hours,110 responses
were available for each item.
3.2. Interrater agreement
The three independent examinations performed on the rst dayof
admission, had kappa value for interrater agreement ranging
from0.36 to 0.66. One itemwas categorized as poor agreement (facial
weak-ness), and the rest of the fourteen items were categorized as
moderateTable 2Interrater agreement of the arNIHSS compared with
NIHSS.
Kappa (95%CI)
Components arNIHSS (95% CI) Agreement ca
LOC (1a) 0.61 (0.53, 0.69) ModerateLOC questions (1b) 0.64
(0.56, 0.72) ModerateLOC Command (1c) 0.58 (0.50, 0.66)
ModerateGaze (2) 0.42 (0.34, 0.49) ModerateVisual Fields (3) 0.44
(0.36, 0.52) ModerateFacial Weakness (4) 0.36 (0.28, 0.44)
PoorMotor left arm (5a) 0.57 (0.51, 0.63) ModerateMotor right arm
(5b) 0.66 (0.60, 0.72) ModerateMotor left leg (6a) 0.61 (0.55,
0.67) ModerateMotor right leg (6b) 0.56 (0.50, 0.62) ModerateAtaxia
(7) 0.41 (0.33, 0.49) ModerateSensory (8) 0.51 (0.43, 0.59)
ModerateAphasia (9) 0.64 (0.58, 0.70) ModerateDysarthria (10) 0.53
(0.45, 0.61) ModerateExtinction (11) 0.55 (0.47, 0.63) Moderate
ICC (95%)Total scores 0.95 (0.94, 0.97) Excellent
arNIHSS: Arabic version of the NIH Stroke Scale; CI: condence
interval; LOC: level of consciou
Please cite this article as: H.M. Hussein, et al., Arabic cross
cultural adaptaNeurol Sci (2015),
http://dx.doi.org/10.1016/j.jns.2015.07.022We performed a
comparison of individual items and total score by spe-cialty
(physician versus nurses) and even compared individual exam-iners;
however, we did not nd statistically signicant differences.
3.4. Construct validity
The construct validity of the arNIHSS is demonstrated by
thecorrelation between the average of the three initial arNIHSS
assess-ments with the infarct volume on MRI using the DWI-ASPECTS
(Spear-man correlation 0.46; P b 0.001; Fig. 1) and with the
functional3.3. Intrarater agreement
One hundred and ten patients were examined a second time by
thesame examiner, 24 hours after the initial examination. Kappa
forintrarater agreement ranged from0.52 to 1.0. The agreementwas
excel-lent for nine items and moderate for six items. The ICC of
the overalltegory NIHSS (95% CI) [23] Agreement category
0.46 (0.39, 0.53) Moderate0.77 (0.64, 0.90) Excellent0.92 (0.75,
1.0) Excellent0.70 (0.39, 1.0) Moderate0.72 (0.57, 0.87)
Moderate0.38 (0.27, 0.49) Poor0.65 (0.51, 0.79) Moderate0.72 (0.54,
0.79) Moderate0.64 (0.53, 0.72) Moderate0.64 (0.53, 0.72)
Moderate0.21 (0.12, 0.30) Poor0.73 (0.53, 0.93) Moderate0.64 (0.53,
0.75) Moderate0.56 (0.39, 0.73) Moderate0.57 (0.40, 0.74)
Moderate
0.94 (0.84, 1.00) Excellent
sness.
tion and validation of the National Institutes of Health Stroke
Scale, J
-
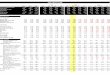
Fig. 1. arNIHSS according to DWI-ASPECTS. The construct validity
of the arNIHSS is dem-onstrated by the incremental increase in the
median of the average of the three baselineassessments, indicating
more severe neurologic decit, as the DWI-ASPECTS scoredecreases,
indicating larger infarct volume. arNIHSS: Arabic version of the
NationalInstitutes of Health Stroke Scale; DWI: diffusion weighted
imaging; ASPECTS: AlbertaStroke Program Early CT score.
4 H.M. Hussein et al. / Journal of the Neurological Sciences xxx
(2015) xxxxxx4. Discussion
Our study design is similar to the Thai version of the NIHSS
[11]in which the examiners were practicing nurses and physicians
(notneurologists with long clinical experience as in the Spanish
version[10]) and the patients were actual patients of those
examiners (versusvideotaped cases as in the NIHSS [23] and the
Italian version [13]).This design makes our study more
representative of real life trainingand patient care encounters
rather than ideal educational conditions.
The difference in methods probably accounts for some of the
differ-ences in results when our study is compared to previous
studies. Whilethe NIHSS items analysis used unweighted kappa, we
did use weightedkappa since it is the more suitable to compare
ordinal variables. All theitems in which interrater agreement was
categorized as moderate bythe NIHSS were similarly categorized as
moderate by the arNIHSS. Thedifference between the two scales is in
three items that were catego-rized as moderate by the arNIHSS,
while categorized as excellent(items 1b and 1c) or poor (item 7) by
the NIHSS. The random patientselection and the variablemixes of
examiners (every patient was exam-ined by any 3 out of the 10
examiners, but not all examiners examinedeach patient) may have
brought the agreement to a realistic middlerather than extreme
values. Another contributing factor is the acuityof the cases, as
the patients had suffered an acute stroke 48 hoursprior to study
participation. In this acute stage, patients' neurologicalstate,
particularly the level of consciousness, may uctuate for a
varietyof medical reasons. This is in contrast to the NIHSS in
which 26 patientswere selected from stroke clinics andwere sent to
a professional TV stu-dio to optimize videotaping quality and then
the interrater agreement isFig. 2. arNIHSS according tomRS. The
construct validity of the arNIHSS is demonstrated bythe incremental
increase in the median of the average of the three baseline
assessments,indicatingmore severe neurologic decit, as the
3-monthsmRS score increases, indicatingmore severe disability.
arNIHSS: Arabic version of the National Institutes of Health
StrokeScale; mRS: modied Rankin Scale.
Please cite this article as: H.M. Hussein, et al., Arabic cross
cultural adaptaNeurol Sci (2015),
http://dx.doi.org/10.1016/j.jns.2015.07.022derived from all
examiners who reviewed the same video clip of theitem examined
[23]. In developing the Spanish version NIHSS, onlytwo examiners
examined the patients and the statistical analysis wasbased on the
score values obtained by them.
Comparing the current study to other NIHSS-validation
studies,this study used dual indicators for construct validity
while other studiesused only functional outcome scales. The
construct validity of thearNIHSS has a signicant correlation for
both DWI-ASPECTS and func-tional outcome at 3 months as measured by
mRS. Its correlation withboth radiological and clinical marker
indicates that arNIHSS versionfunctioned as it was
hypothesized.
The NIHSS itself has well recognized limitations, which led to
thedevelopment of the modied NIHSS (mNHISS) trying to eliminate
theitems with low reliability: level of consciousness, facial
palsy, limbataxia, and dysarthria [24]. The arNIHSS shares the same
limitationsfor facial palsy and limb ataxia, and dysarthria,
performs better thanNIHSS in level of consciousness, and worse in
visual eld and gazeitems. An exploration into a modied arNIHSS is
warranted to assesswhether it will increase the reliability. The
intrarater reliability in thisstudy was undertaken by comparing
individual rater's arNIHSS exami-nation of the same patient on
admission and at 24 hours. The assump-tion was that the change in
neurological state would not cause asignicant change in the arNIHSS
score over this time period for thevastmajority of patients.
Tominimize the chance of a signicant changein the arNIHSS, we
excluded patients whowere treated with thrombol-ysis and we limited
the time period between the rst and the secondexamination to 24
hours. This method was used in the validation ofthe Spanish version
of the NIHSS [10].
In the Arab world, NIHSS has always been taught in English and
leftto the individual to create his/her own Arabic version for
their practice.We are aware of several attempts by individuals and
institutions tocreate an Arabic version of the NIHSS, yet these
versions were not vali-dated and remained local. The arNIHSS is an
opportunity to standardizethe utilization of the NIHSS among
Arabic-speaking populations. Theinclusion of a panel of
neurologists from all over the Arab world in thedevelopment of the
scale aimed at this pan-Arab goal. However, thevalidation phase was
implemented only in Egypt on Egyptian patients.Future validation in
other Arabic-speaking countries is needed to ensurethat the current
arNIHSS version is universally pertinent. Anotherpotential
limitation is the lack of a unied training program, whichcan
potentially improve the interrater agreement. Creating a
certica-tion process will ensure the standardization of
instructions and therigor of training. Further work should be
directed at new training strat-egies using in-print and online
materials to increase the utilization ofarNIHSS.
5. Conclusion
A culturally adaptedArabic version of theNIHSS has
beendeveloped.The proposed version has been found to be valid and
reliable using acohort in Egypt. Validation in other Arab countries
is recommended.
Acknowledgment
Panel of bilingual Arab Neurologists by country of
origin:Tunisia: Senda Ajroud-Driss MD (Chicago, IL), Nizar Souayah
MD
(Newark, NJ)Sudan: Khalafallah Bushara, MD (Minneapolis,
MN)Lebanon: Mustapha Ezzeddine MD (Minneapolis, MN), Gamil
Fteeh
MD (Houston, TX)Syria: Yousef Hennawi MD (Houston, TX), Amrou
Serajj MD
(Houston, TX)Palestine: Akram Shehadeh MD (Milwaukee, WI)Saudi
Arabia: Amer Zahrallayalli MD (Houston, TX)Jordan: Osama Zaidat MD
(Milwaukee, WI)
Iraq: Saef Ahmed MD (Boston, MA)
tion and validation of the National Institutes of Health Stroke
Scale, J
-
Professional ArabicEnglish TranslatorMr Suhaib Alrawi (Houston,
TX)
Appendix A. Supplementary data
Supplementary data to this article can be found online at
http://dx.doi.org/10.1016/j.jns.2015.07.022.
References
[1] T. Brott, H.P. Adams Jr., C.P. Olinger, et al., Measurements
of acute cerebral infarction:a clinical examination scale, Stroke
20 (1989) 864870.
[2] P.D. Lyden, G.T. Lau, A critical appraisal of stroke
evaluation and rating scales, Stroke22 (1991) 13451352.
[3] Tissue plasminogen activator for acute ischemic stroke. The
National Institute ofNeurological Disorders and Stroke rt-PA Stroke
Study Group, N. Engl. J. Med. 333(1995) 15811587.
[4] P. Lyden, T. Brott, B. Tilley, et al., Improved reliability
of the NIH Stroke Scale usingvideo training. NINDS TPA Stroke Study
Group, Stroke 25 (1994) 22202226.
[5] M.J. Alberts, G. Hademenos, R.E. Latchaw, et al.,
Recommendations for the estab-lishment of primary stroke centers.
Brain Attack Coalition, JAMA 283 (2000)31023109.
[6] J.S. McKinney, Y. Deng, S.E. Kasner, J.B. Kostis, Myocardial
Infarction Data AcquisitionSystem Study G, Comprehensive stroke
centers overcome the weekend versusweekday gap in stroke treatment
and mortality, Stroke 42 (2011) 24032409.
[7] E.C. Jauch, J.L. Saver, H.P. Adams Jr., et al., Guidelines
for the early management ofpatients with acute ischemic stroke: a
guideline for healthcare professionals fromthe American Heart
Association/American Stroke Association, Stroke 44
(2013)870947.
[8] R.T. Cheung, P.D. Lyden, T.H. Tsoi, et al., Production and
validation of Putonghuaand CantoneseChinese language National
Institutes of Health Stroke Scale trainingand certication videos,
Int. J. Stroke 5 (2010) 7479.
[9] C. Cincura, O.M. Pontes-Neto, I.S. Neville, et al.,
Validation of the National Institutesof Health Stroke Scale, modied
Rankin Scale and Barthel Index in Brazil: the roleof cultural
adaptation and structured interviewing, Cerebrovasc. Dis. 27
(2009)119122.
[10] R. Dominguez, J.F. Vila, F. Augustovski, et al., Spanish
cross-cultural adaptation andvalidation of the National Institutes
of Health Stroke Scale, Mayo Clin. Proc. 81(2006) 476480.
[11] Y. Nilanont, S. Phattharayuttawat, P. Chiewit, et al.,
Establishment of the Thai versionof National Institute of Health
Stroke Scale (NIHSS) and a validation study, J. Med.Assoc. Thai. 93
(Suppl. 1) (2010) S171S178.
[12] M.S. Oh, K.H. Yu, J.H. Lee, et al., Validity and
reliability of a Korean version of theNational Institutes of Health
Stroke Scale, J. Clin. Neurol. 8 (2012) 177183.
[13] F.R. Pezzella, O. Picconi, A. De Luca, P.D. Lyden, M.
Fiorelli, Development of the Italianversion of the National
Institutes of Health Stroke Scale: It-NIHSS, Stroke 40
(2009)25572559.
[14] K. Prasad, D. Dash, A. Kumar, Validation of the Hindi
version of National Institute ofHealth Stroke Scale, Neurol. India
60 (2012) 4044.
[15] SIL Ethnologue, 17th, 2015.
http://www.ethnologue.com/statistics/size. AccessedNovember 2014
[online].
[16] H.T. Benamer, R.A. Shakir, The neurology map of the Arab
world, J. Neurol. Sci. 285(2009) 1012.
[17] M. Bullinger, J. Alonso, G. Apolone, et al., Translating
health status questionnairesand evaluating their quality: the IQOLA
Project approach. International Quality ofLife Assessment, J. Clin.
Epidemiol. 51 (1998) 913923.
[18] B. Gandek, J.E. Ware Jr., Methods for validating and
norming translations of healthstatus questionnaires: the IQOLA
Project approach. International Quality of LifeAssessment, J. Clin.
Epidemiol. 51 (1998) 953959.
[19] P.A. Barber, M.D. Hill, M. Eliasziw, et al., Imaging of the
brain in acute ischaemicstroke: comparison of computed tomography
and magnetic resonance diffusion-weighted imaging, J. Neurol.
Neurosurg. Psychiatry 76 (2005) 15281533.
[20] C. de Margerie-Mellon, G. Turc, M. Tisserand, et al., Can
DWI-ASPECTS substitute forlesion volume in acute stroke? Stroke 44
(2013) 35653567.
[21] R. Bonita, R. Beaglehole, Recovery of motor function after
stroke, Stroke 19 (1988)14971500.
[22] P.M. Janssen, N.A. Visser, S.M. Dorhout Mees, C.J. Klijn,
A. Algra, G.J. Rinkel, Compar-ison of telephone and face-to-face
assessment of the modied Rankin Scale,Cerebrovasc. Dis. 29 (2010)
137139.
[23] P. Lyden, R. Raman, L. Liu, et al., NIHSS training and
certication using a new digitalvideo disk is reliable, Stroke 36
(2005) 24462449.
[24] B.C. Meyer, P.D. Lyden, The modied National Institutes of
Health Stroke Scale: itstime has come, Int. J. Stroke 4 (2009)
267273.
5H.M. Hussein et al. / Journal of the Neurological Sciences xxx
(2015) xxxxxxPlease cite this article as: H.M. Hussein, et al.,
Arabic cross cultural adaptaNeurol Sci (2015),
http://dx.doi.org/10.1016/j.jns.2015.07.022tion and validation of
the National Institutes of Health Stroke Scale, J
Arabic cross cultural adaptation and validation of the National
Institutes of Health Stroke Scale1. Introduction2. Methods2.1.
Phase 1: arNIHSS scale development2.2. Phase 2: scale
validation:2.2.1. Training of examiners2.2.2. Study subjects2.2.3.
Study protocol2.2.4. Statistical analysis
3. Results3.1. Subjects' characteristics3.2. Interrater
agreement3.3. Intrarater agreement3.4. Construct validity
4. Discussion5. ConclusionAcknowledgmentAppendix A.
Supplementary dataReferences