-
290 A E S T H E T I C S U R G E R Y J O U R N A L ~ J u l y / A
u g u s t 2 0 0 3
S e c o n d T h o u g h t s
Arm Contouring
The authors have updated their brachioplasty tech-nique, adding
conservative skin undermining in thetreatment area only and, in
some instances, elbowplasty.Patients are divided into 3 distinct
groups for treatmentplanning on the basis of skin quality and fat
deposits.(Aesthetic Surg J 2003;23:290-292.)
We divide patients undergoing brachioplasty into3 groups,
according to their characteristics.Group 1 comprises patients with
moderate tofirm skin and voluminous upper-arm fat deposits.
Weperform lipoplasty with specic limitations on how muchfat is
removed based on the patients skin turgor. Theseprinciples are the
same as those advocated by Vogt.1
Group 2 comprises patients with abby skin and fatdeposits.
Treatment includes lipoplasty and skin resec-tion in the same
stage. Surgery begins with lipoplasty.We perform skin undermining
superficially, preservingthe subcutaneous tissue to avoid severing
of lymphaticvessels and supercial nerves.
Group 3 comprises patients with accid skin and nofat deposits.
Resection of excess skin is the only indica-tion for this group. In
almost all of these patients, weresect an elliptical or triangular
shaped piece of skin ap,saving the internal brachial sulcus as
reference. We placethe suture and nal scar 1 to 3 cm above or below
thissulcus (Figure 1). The amount of axillary skin resected isbased
simply on redundancy. It is imperative, however,that the scar is
placed at the inner aspect of the upperarm; otherwise it will be
exposed.25
The general preoperative evaluation for any patientundergoing
arm contouring includes the pinch test todetermine the amount of
skin to be resected. When per-forming this test, have the patient
stand with his or herarms abducted.
Surgery is performed under sedation and local anes-thesia; the
patient is prone, with arms abducted at about80 degrees. The specic
technique lipoplasty, surgicalexcision, or both is carried out in
accordance with theplan made before surgery.
Even though we havebeen performing lipoplastysince 1981, it did
notbecome part of our standardapproach to brachioplastyuntil after
1988. Since then,we have routinely usedlipoplasty in
selectedpatients undergoing bra-chioplasty. In the past 6years, we
have also used 2other techniques to improveresults. First, we
performconservative skin undermin-ing only on the area to
beresected to avoid deadspace. Second, patients with redundant skin
in the elbowregion are treated with elbowplasty, which we perform
ina manner similar to the procedure described by Lewis.6
Elbowplasty may be combined with brachioplasty in thesame
surgical stage.
Conservative Skin Undermining
When skin dissection is to be performed, the skin apis stretched
above the superior limit of the incision toestimate the amount of
skin to be resected. Three-zeroisolated intradermal absorbable
stitches are placed allalong the upper nondissected skin edge, and
the dissectedlower limit, to avoid dead space and irregular tension
onthe suture. Then resect the excess skin (Figure 2).
Finish suturing with a running intracuticular 4-0absorbable
material. Straight and zigzag suture lines havedemonstrated similar
scar quality. In long-term follow-up, we have found that suture
tension results in broaden-ing of scars. Scar widening is more
evident in patientswith thin dermis.
Excess elbow skin is common in older patients and inslim
patients with lax skin. In contrast to Lewis proce-dure, which
looks like an elliptical resection, we performa horseshoe-type
resection for excess skin (Figure 3).This has resulted in generally
acceptable scars. The scar
Ricardo Baroudi, MD, SoPaulo, Brazil, is a member ofthe
Brazilian Society of PlasticSurgery.Co-author Carlos Alberto
A.Ferreira, MD, So Paulo.Brazil, is a member of theBrazilian
Society of PlasticSurgery.
-
A E S T H E T I C S U R G E R Y J O U R N A L ~ J u l y / A u g
u s t 2 0 0 3 291Arm Contouring
S e c o n d T h o u g h t s
may resemble one of the remaining elbow-skin folds; abroader and
somewhat less desirable scar may result,depending on individual
healing characteristics. In allpatients, the scar remains reddish
for months.
References1. Vogt PA. Surgery of the upper arm. Lipoplasty
Newsletter 1994;11:24.
2. Baroudi R. Dermatolipectomy of the upper arm. Clin Plast
Surg1975;2:485.
3. Baroudi R. Dermolipectomy of the upper arm. In:
Gonzalez-Ulloa M,Meyer R, Smith JW, Zaoli G, eds. Aesthetic Plastic
Surgery, vol 5.Padua, Italy: Piccin; 1988: 219.
4. Guerrerosantos J. Arm lift. In: Courtiss E, ed. Trouble in
AestheticSurgery. St. Louis, MO: Mosby; 1978:232.
5. Guerrerosantos J. Brachioplasty. Aesth Plast Surg
1979;3:1.
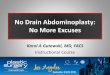
Figure 1. Schematic representation of the triangular and
elliptical incisions for resection of excess skin. XX represents
the internal brachial sulcus. It isimportant to place the nal scar
1 to 3 cm above or below this sulcus so that the scar is hidden
when the arm is adducted.
Figure 2. A, Transoperative aspect of the upper arm, showing the
skin excess undermined up to its resection limits. Estimate the
dissection step by stepto avoid unnecessary undermining. B,
Isolated absorbable 3-0 sutures are applied all along the upper
incision edge to the limits of the underminedskin. C, Excess skin
is resected. D, Routine 4- 0 absorbable running intracuticular skin
suture.
A B
C D
-
292 A e s t h e t i c S u r g e r y J o u r n a l ~ J u l y / A
u g u s t 2 0 0 3 Volume 23, Number 4
S e c o n d T h o u g h t s
6. Lewis JR Jr. Atlas of Aesthetic Surgery. Boston, MA: Little,
Brown;1973:271.
Reprint requests: Ricardo Baroudi, MD, Rua Itabaquara, 48,
01234-020, So Paulo SP, Brazil.
Copyright 2003 by The American Society for Aesthetic Plastic
Surgery, Inc.
1090-820X/2003/$30.00 + 0
doi:10.1067/maj.2003.63
Figure 3. A, Preoperative posterior view of a 46-year-old woman.
B. Postoperative posterior view, demonstrating the skin excess
resection. C,Preoperative anterior view. D, Postoperative anterior
view after 10 months. Upper-arm contour was improved; the scar has
been placed along thebrachial internal sulcus. E, Preoperative view
demonstrates cutis laxa of the elbow. Patient is marked for a
horseshoe-like skin incision similar to thatdescribed in Lewis
procedure.6 F, The pinch test is performed. G, Demonstrates the
dissection and the excess skin to be resected. H, The patient
hasbeen sutured. I, Postoperative view, 10 months after
elbowplasty. The scar remains reddish and broad, possibly because
of the histologic skin structure(cutis laxa). J, Postoperative view
after 8 months demonstrates the nal elbow scar. Posterior view of
the arm shows no evidence of a scar.
A B
C D
E F G H
I J
Arm ContouringConservative Skin UnderminingReferences