Embed Size (px)
Citation preview

MEDICAL EDUCATION AND RESEARCH IN INDIA SHOULD BE AIMED AT IMPROVING INCLUSIVE
HEALTH EXPECTANCY OF THE BILLION PLUS PEOPLE
HEAD OF VHS DIABETES DEPARTMENT CHAIRMAN – TAG-VHS Diabetes Research Centre, Voluntary Health Services, Chennai, INDIA. EDITOR – INDIAN SUB–CONTINENT – THE JOURNAL OF THE SCIENCE OF HEALING OUTCOMES. FOUNDER CHAIRMAN – HEALTHTRACK INFO SOLUTIONS PVT. LTD.
1
ARE WE GOING IN THE RIGHT DIRECTION?
by
Dr. C.V.Krishnaswami - FRCP(E)., F.A.M.S., D.T.M & H(EDIN)
Medical Education Today
Is it Public or Private?
MCI Scam; Is the replacement – any better?
Is the medical education today really relevantto the needs of our people of this and thefuture generations?
De–schooling and Re–schooling Required.
The Hindu – Monday, April 12th 2010
Dr.Samir K.Brahmachari, Scientist and Director-General of the Councis of Scientific and Industrial Research(CSIR) said “ We need to have a balanced view between health as a right and health as a business. It isbecause there has been imbalance in this view that diseases like TB, with high mortality but lowprofitability, are neglected by the current system of pharmaceutical research”.
“ As virtually no new TB drugs have been developed since the 1960s, the OSDD’s model in particular holdsgreat promise for the scientific community by stimulating the development of better drugs and diagnosticsfor patients” he said.
“ With children and people living with HIV in India and other developing countries bearing the greatestburden of the disease, as well as the emergence and spread of TB that was resistant to treatment by thestandard anti-TB drugs, there was an urgent global, but unanswered, need for new drugs.
“For us, the irony is that with the availability of drugs for HIV and particularly of safe and affordable Indiangenerics, we are living with HIV but dying of TB” (MDR)
Loon Gangte of the Delhi Network of Positive People
Research in Diabetes Mellitus (Type 1, Type 2)
First National Congress on diabetes Mellitus 1969 in INDIA.
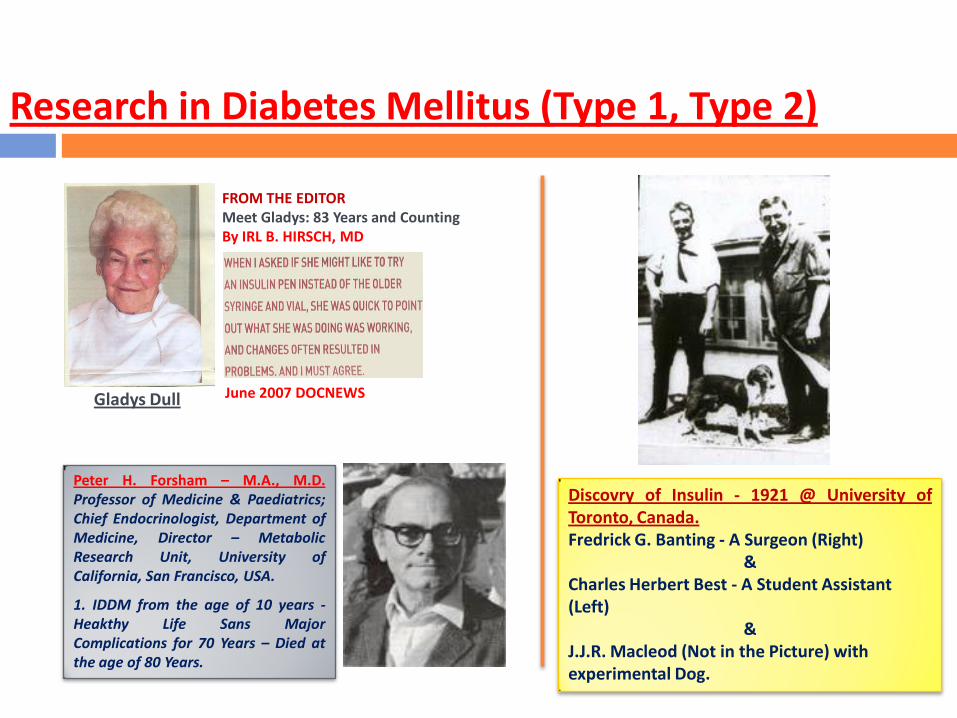
FROM THE EDITORMeet Gladys: 83 Years and CountingBy IRL B. HIRSCH, MD
June 2007 DOCNEWS
Peter H. Forsham – M.A., M.D.Professor of Medicine & Paediatrics;Chief Endocrinologist, Department ofMedicine, Director – MetabolicResearch Unit, University ofCalifornia, San Francisco, USA.
1. IDDM from the age of 10 years -Heakthy Life Sans MajorComplications for 70 Years – Died atthe age of 80 Years.
Research in Diabetes Mellitus (Type 1, Type 2)
Gladys Dull
Discovry of Insulin - 1921 @ University ofToronto, Canada.Fredrick G. Banting - A Surgeon (Right)
& Charles Herbert Best - A Student Assistant (Left)
&J.J.R. Macleod (Not in the Picture) with experimental Dog.
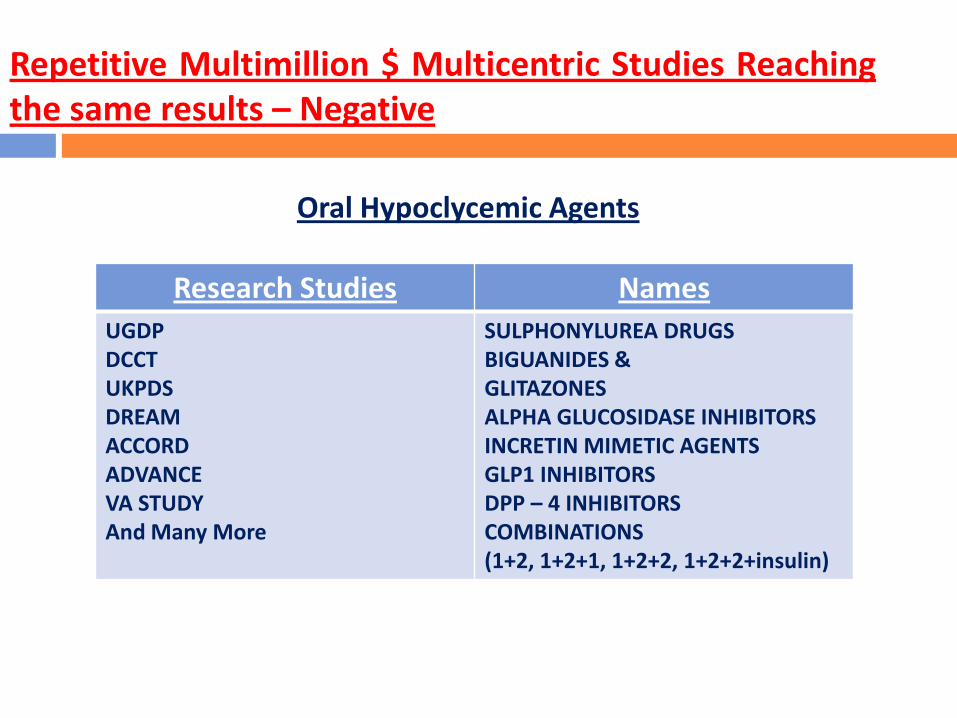
Repetitive Multimillion $ Multicentric Studies Reachingthe same results – Negative
Oral Hypoclycemic Agents
Research Studies Names
UGDPDCCTUKPDSDREAMACCORDADVANCEVA STUDYAnd Many More
SULPHONYLUREA DRUGSBIGUANIDES & GLITAZONESALPHA GLUCOSIDASE INHIBITORSINCRETIN MIMETIC AGENTSGLP1 INHIBITORSDPP – 4 INHIBITORS COMBINATIONS(1+2, 1+2+1, 1+2+2, 1+2+2+insulin)

The Story of Glitazones – (Thiazolidinediones)
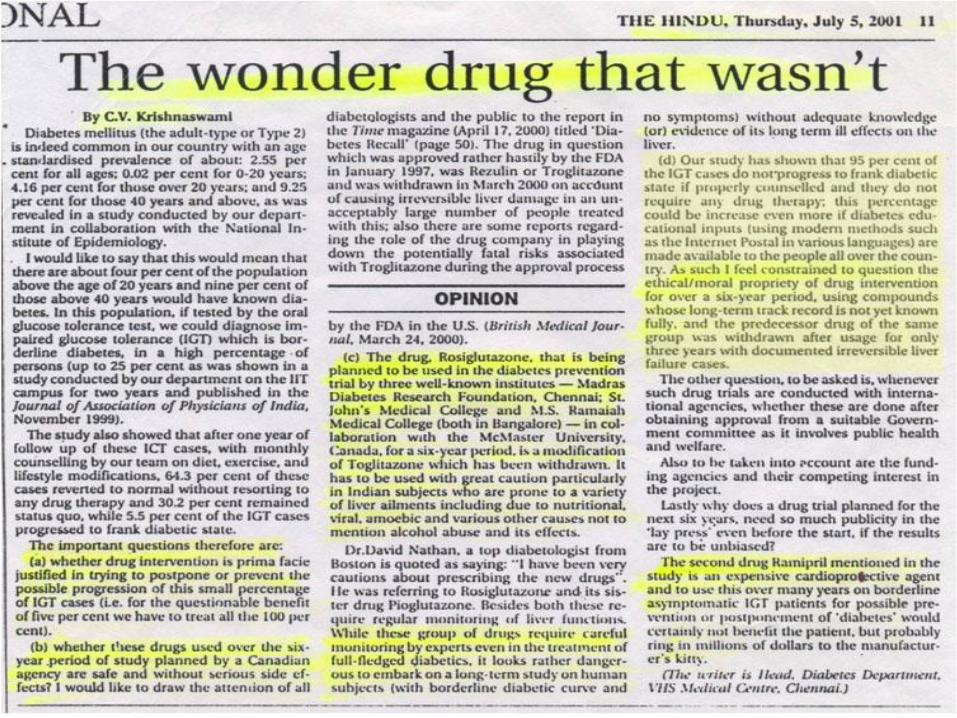
1. Troglitazone (Rezulin):
This exciting PPAR Gamma Activator Agent, was approved by the US FDA andbegan being used clinically in 1997 and after causing irreparable Liver Damageto Significant number of patients, was withdrawn from the market in early 2000.
The US federal Government Healthcarers are still paying for the treatment ofpatients with irreversible liver failure caused due to Troglitazone. The storybehind the story was what happened in the lower / higher echelons of the USFDA (reported in BMJ / NEMJ).

City Institute to take part in diabetes prevention
project
The six-year project - Diabetes Reduction Assessment with the
drugs, Ramipril and Rosiglitazone, is in coordination with the
McMaster University, Canada, with partial funding of the
Canadian Government.
The Hindu, Sunday, July 1 2001 Page 3
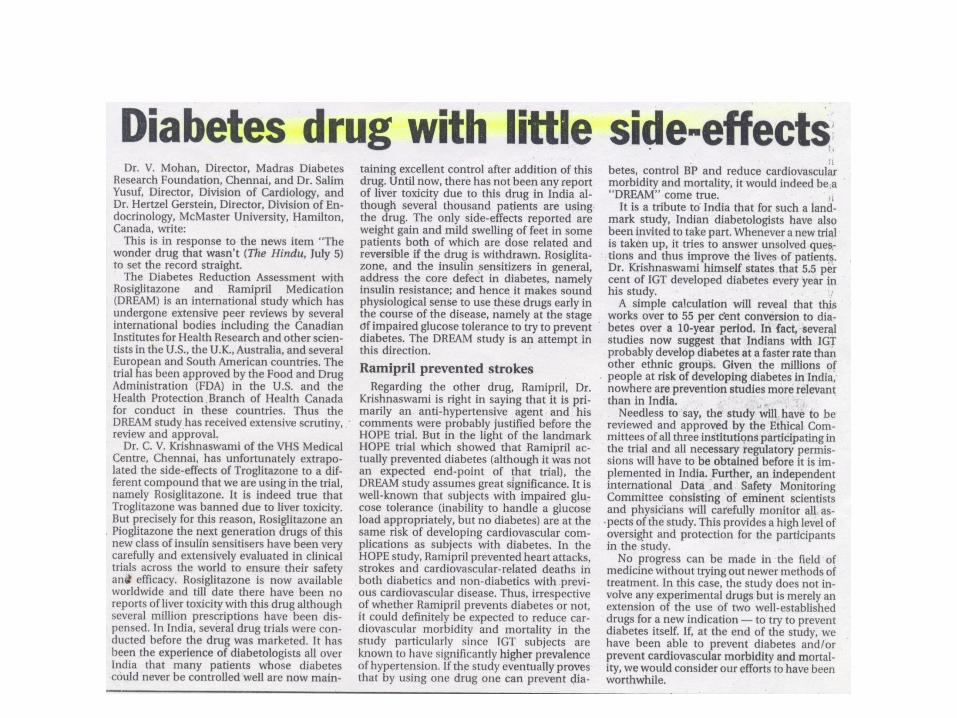


The Story of Glitazones – (Rosiglitazone)
“Rosiglitazone – Useful Drug but has Side Effects”
Before Treatment After Treatment
Mean total cholesterol 188 + 37 212 + 41
Mean LDL cholesterol 108 + 30 126 + 38
Mean Triglycerides 201 + 94 228 + 108
Mean HDL/LDL ratio 4.6 + 1.0 5.3 + 1.2
Mean HDL 42 + 10 41 + 8
The weight gain and adverse lipid profile are
probably secondary to the PPAR gamma
activation. These receptors are highly expressed
in the adipocytes and lead to excess adipose
tissue deposition. In addition, activation of PPAR
gamma increases transcription of certain insulin
sensitive genes influencing adipocyte
differentiation and function.
This results in changes in fat by 10% but increases subcutaneous fat 20-30% with an overall increase in
fat by 10%. This is referred to as the thiazolidinedione paradox as despite overall increase in fat insulin
sensitivity markedly improves because of its effects on the visceral fat. These side effects must be looked
for in all patients on Rosiglitazone. Newer thiazolidinedione compounds with favorable effects on lipid
profile and no other side effects are the urgent need of the hour.
S.Vidya, V.Mohan – MV Diabetes Specialities Centre and Madras Diabetes Research Foundation,
#35, Conran Smith Road, Gopalapuram, Chennai – 600 086, India.JAPI Vol 50, April 2002
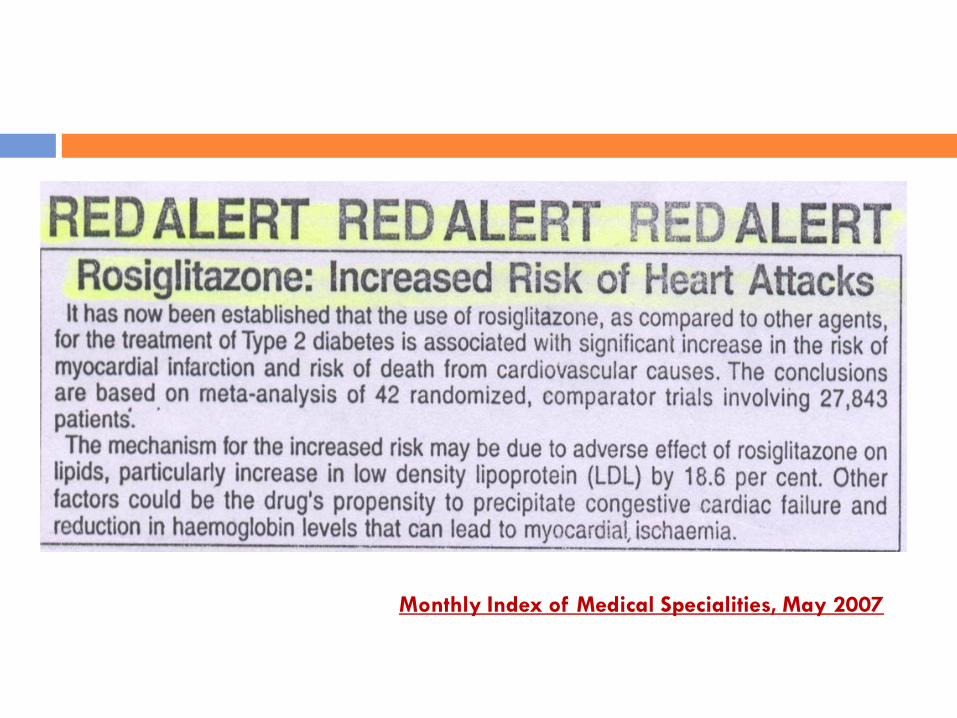
Monthly Index of Medical Specialities, May 2007
Pioglitazone Falls Short of Promise –
Drug’s benefit – to – risk ratio Unclear
by
Joel R. Cooper, Health Behaviour News Service
DOC News, December 2006 (ADA)
The story of rosiglitazone is one of death, greed, and corruption, according to theStaff Report of the United States Senate Committee on Finance, released on Feb20, 2010. The 2-year investigation by Senators Max Baucus, Chuck Grassley, andothers, suggests that excess cardiovascular events in patients taking rosiglitazoneappeared as early as 2004, but that the manufacturer, GlaxoSmithKline(GSK), intimidated researchers and manipulated the scientific process forcommercial advantage. RECORD, one of the studies at the centre of thisstorm, was published by The Lancet in 2009. The Staff Report claims that GSKunblinded the data 2 weeks before approaching the RECORD steering committeeto suggest an interim analysis. GSK maintains that the company has been diligentin investigating rosiglitazone's safety and points to the fact that the drug is stilllicensed by the US Food and Drug Administration. Add to this controversy StevenNissen's account, published on March 24 in the Journal of the American MedicalAssociation, of a manuscript leaked by a peer-reviewer, indiscreet industryemails, and clandestine tape recordings, and one has the ingredients of a JohnGrisham novel.
Strengthening the credibility of clinical research
The Lancet, Volume 375, Issue 9722, Page 1225, 10 April 2010
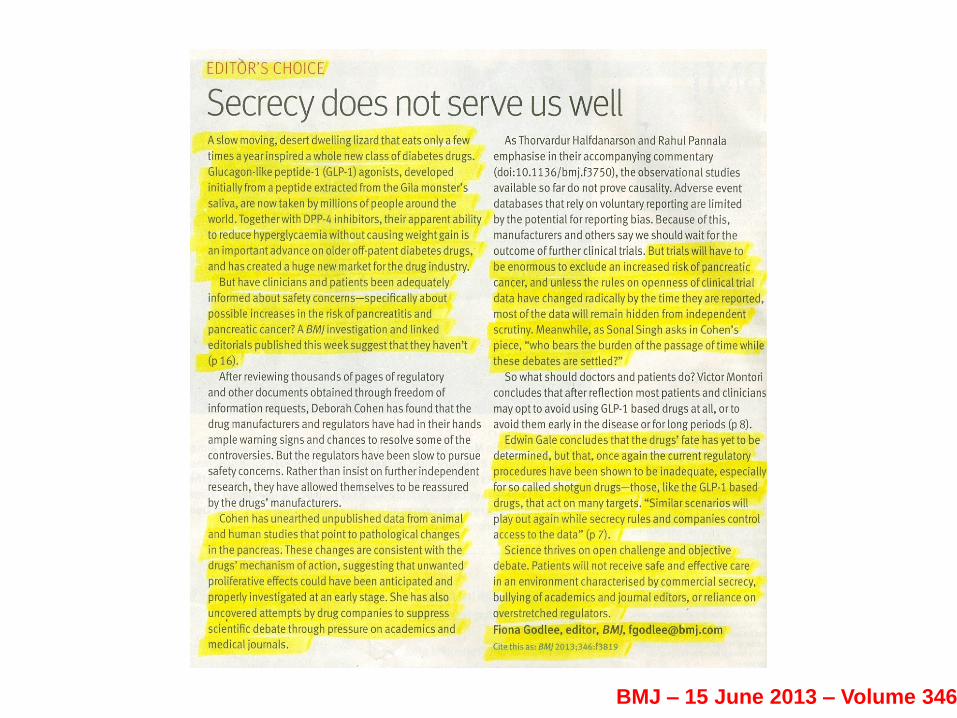
BMJ – 15 June 2013 – Volume 346
10th Congress of The International Diabetes Federation, Vienna, Austria – September 1979
This paper presents the results of computed analysis of 300 randomly sampled cases receiving treatment forMOD in 3 groups: Group A, diet alone; Group B, diet + oral hypoglycaemic agents (OHA), and Group C, diet +insulin. These cases were followed up regularly for 2 years, with periodic assessment of chemical control ofdiabetes. 32% of the cases were in Group A, 44.3% in Group B and the rest in Group C. 75% of the patientscompleted the 2-year follow-up. Successful chemical control was obtained in 95% of Group A (P<0.0002) and in81 + 4.17%(mean) of Group B (P<0.02). Chemical control obtained in Group A was significantly better than inGroup B or C. Group A thus acted as an ‘index group’ in the treatment of the cases under study. The skepticismregarding the hypoglycaemic effects of OHA is perhaps because the studies so far published do not have theresult in the index group, as obtained in this study. Only such a type of diet could be expected to give sustainedgood results in the treatment of MOD, when OHA are indicated.
A feedback study of treatment of maturity-onsetdiabetes (MOD) with regard to various treatment groups– Dr.C.V.KRISHNASWAMI, Madras, India
Research Contributions from VHS Diabetes Department
The Story of Biguanides – Phenformin & Metformin
LACTIC ACIDOSIS FOLLOWING PHENFORMIN THERAPY
(A review of authors’ experience in 25 Indian diabetics)
By
C.V. KRISHNASWAMI* and K.VALMIKINATHAN**
It is difficult to make any definite conclusions based on this limited study. At the same time, it is quite speculative thattheses rather subtle changes in anion gap are perhaps indicative of the early phase of Phenformin effect. This may wellbe a physiological adaptation to possibly a type of drug induced stress leading to sodium retention. This possibly has tobe entertained in view of the report of Phenformin impairing NH4
+ formation which is quite often implicated in sodiumexchange (Rooth and bandman, 1973).
Cohen R.D. and Woods H.F. (1976) : Clinical and biological aspects of Lactic Acidosis, Oxford, Blackwell ScientificPublication London.
Rooth G. and Bandman U.L.F. (1973) : Renal response to acid load after Phenformin, B.M.J., 4 : 256
JOUR. DIAB. ASSO. IND. : VOL XIX. IAN, 1979
Phenformin
Research Contributions from VHS Diabetes Department
Research Contributions from VHS Diabetes Department
KRISHNASWAMI C.V. and CHANDRA, P: ‘The significance of Certain Epidemiological Variants’ in the genesis of Juvenile Insulindependant diabetes Mellitus – the need for a Glbal Program of Co-operation’, Tohoku J., of Exp. Med., 1983, 141 Suppl., pp.161 –170.
Technical Report Series 727: Diabetes Mellitus, Report of a WHO Study Group, Geneva, World Health Organisation, pp.103, 1985.
BINGLEY P.J AND GALE E.A.M. ‘Rising Incidence of I.D.D.M in Europe’, Diabetes Care, 1989, 12, 289, - 95;
ASHA BAI, P.V., KRISHNASWAMI, C.V., CHELLAMARIAPPAN, M., VIJAYAKUMAR, G., and SUBRAMANIAM, J.R; ‘Glycosuria andDiabetes Mellitus in Children and Adolescents in South India’, Diabetes Research and Clinical Practice, 1991, 13, 131 – 136.
STEPHEN G. GARDNER, POLY J BINGLEY, PAMELA, A. SAWTALL, SUZANNE WEEKS, EDWIN A.M. GALE – the Barts’ Oxford StudyGroup : ‘Rising incidence of IDDM in Children aged under 5 years, in the Oxford region: Time Trend Analysis’ B.M.J. 1997, 315. 713– 17;
PV Asha Bai*, CV Krishnaswami**, M Chellamariappan*** Prevalence and Incidence of Type - 2 Diabetes andImpaired Glucose Tolerance in a Selected Indian Urban Population - The I.I.T Study - 1992 - 1993, JAPI 1999,VOL 47, NO 11
ASHA BAI, P.V., B.N.MURTHY, M. CHELLAMARIAPPAN, M.D. GUPTE and C.V.KRISHNASWAMI ‘Prevalance of known Diabetes inCHENNAI CITY, J.A.P.I., 2001, Vol. 49, pp.974 – 81.
ASHA BAI, P.V., CHELLAMARIAPPAN, M., KRISHNASWAMI, C.V., MURTHY B.N., GUPTE, M.D., ‘Magnitude of young Diabetes inIndian Urban Population’, The Antiseptic, 2002, Vol.99, No.8, pp.293 – 98.

‘Bad’ drugs and unethical, unscientific clinical trials
LONE Crusade Against
Statins and risk of incident of diabetes: a collaborative meta-analysis of randomized statin trials
13 statin trials with 91140 participants, of whom 4278 (2226 assigned statins and 2052 assigned control treatment)developed diabetes during a mean of 4 years. Statin therapy was associated with a 9% increased risk for incidentdiabetes (odds ratio [OR] 1.09; 95% CI 1.02-1.17), with little heterogeneity (P Value =11%) between trials.
Lancet 2010; 375:735-42
The story of rosiglitazone is one of death, greed, and corruption, according to the Staff Report of theUnited States Senate Committee on Finance, released on Feb 20, 2010. The 2- year investigation bySenators ax Baucus, Chuck Grassley, and others, suggests that excess cardiovascular events in patientstaking rosiglitazone appeared as early as 2004, but that the manufacturer, Glaxo SmithKline (GSK),intimidated researchers and manipulated the scientific process for commercial advantage.
Add to this controversy Steven Nissen’s account, published on March 24 in the Journal of theAmerican Medical Association, of a manuscript leaked by a pee-reviewer, indiscreet industry emails,and clandestine tape recordings, and one has the ingredients of a John Grisham novel.
The Lancet, Volume 375, Issue 9722, Page 1225, 10 April 2010
“Medicine might be winning the battle of glucose control, but is losing the war against diabetes”
The Lancet, Volume 375, No 9733, June 26-July 2, 2010.
Same issue (P.2193) Editorial: “Type 2 diabetes – time to change our approach”
What is Linear Diabetology?Evolution of Diabetes as a specialty and Linear Diabetology as the ‘goal’ for all ills attributed to Diabetes.
http://www.pubmedinfo.com/pdf/Pitfalls%20in%20Linear%20Diabetology.pdf
Pitfalls in Linear Diabetology – Dr.C.V.Krishnaswami - Keshav Pai MemorialOration, Mangalore, 5th April 2008
Strengthening the credibility of clinical research
Shame: the elephant in the roomManaging shame is important for improving health care
Editorial, BMJ Volume 324, 16th March 2002.
Frank Davidoff – USA.
In 1960’s the results of UGDP showed that Tolbutamide, was associated with a significant increase inmortality in patients who developed Myocardial Infarction. The obvious response from Medical Professionshould have been gratitude: here was an important way to improve the safety of Clinical Practice. But infact the response was doubt, outrage, even legal proceedings against the investigators; the controversywent on for years. Why?
Vindication galore but No Apology or Acceptance of Mistakes
Rosiglitazone StoryPioglitazone StorySitagliptin StoryExenatide Story
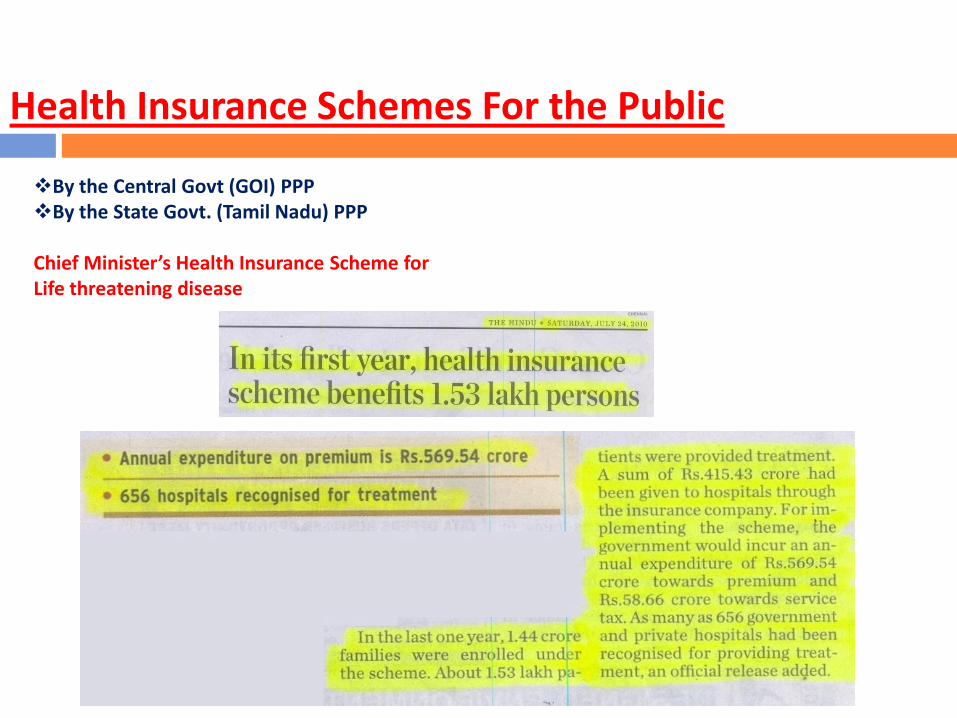
By the Central Govt (GOI) PPPBy the State Govt. (Tamil Nadu) PPP
Chief Minister’s Health Insurance Scheme for Life threatening disease
Health Insurance Schemes For the Public
Dr.Reddy further questioned theviability of public-privatepartnership projects in the
infrastructure space saying "weneed proper institutionalmechanism to support acorporate bond market. Unlesswe put in place properinstitutional and governancemechanisms, public-privatepartnerships in theinfrastructure area can wellbecome private profit at thecost of public expenses," - PTI
Death by Medicineby Gary Null, PhD, Caarolyn Dean, MD, ND Martin Feldman, MD, Debora Rasio, MD, Dorothy Smith, PhD
Ref . http://www.encognitive.com/files/Part%20I--Death%20by%20Medicine.pdf - 2007
Rosuvastatin: Risky in Indians (FDA RED ALERT)Western drug regulators have made it obligatory that prescribers inform all patients that rosuvastatin can cause muscle injury which insevere cases “Can cause kidney damage and other organ failure that are potentially life-threatening.” Hence patients should“promptly report signs and symptoms of muscle pain and weakness, malaise, fever, dark urine, nausea or vomiting” to their doctors.
“OVER MEDICATING SENIORS”
Aspirin Increases Stroke Risk (FDA RED ALERT)
The use of low dose aspirin – a day not only does not reduce but actually increases the risk of heamorrhagic stroke by a whooping 69per cent in males.
There is no beneficial effect on the risk of ischaemic stroke.
These are the results of a meta – analysis of 95,000 patients enrolled in six randmonised controlled clinical trials. (Ref. AM, HeartAssociation)
MIMS May 2007
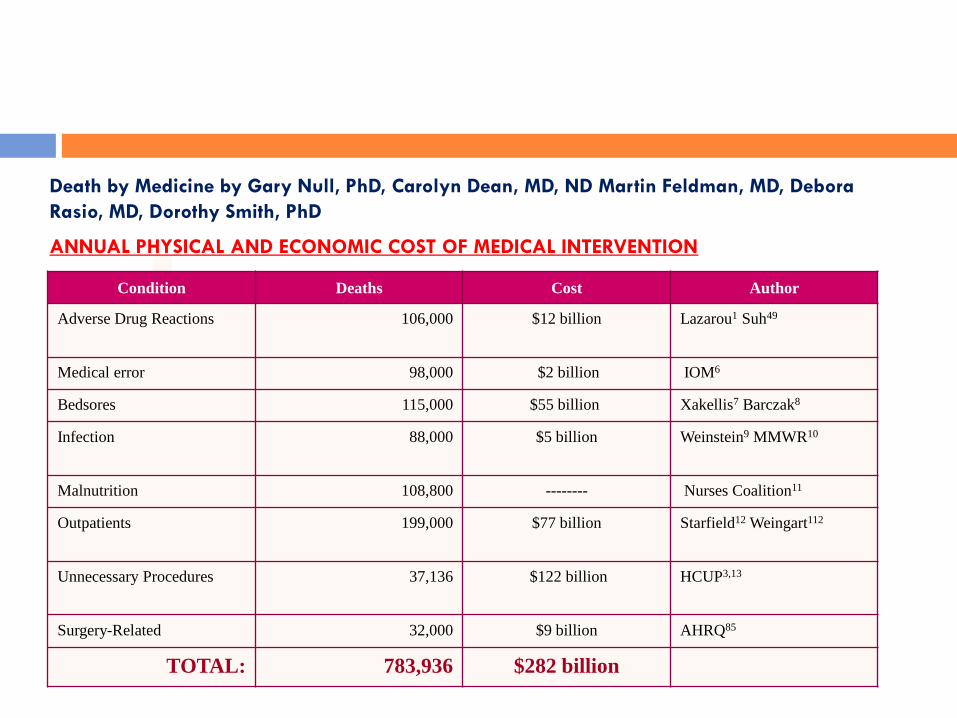
Condition Deaths Cost Author
Adverse Drug Reactions 106,000 $12 billion Lazarou1 Suh49
Medical error 98,000 $2 billion IOM6
Bedsores 115,000 $55 billion Xakellis7 Barczak8
Infection 88,000 $5 billion Weinstein9 MMWR10
Malnutrition 108,800 -------- Nurses Coalition11
Outpatients 199,000 $77 billion Starfield12 Weingart112
Unnecessary Procedures 37,136 $122 billion HCUP3,13
Surgery-Related 32,000 $9 billion AHRQ85
TOTAL: 783,936 $282 billion
Death by Medicine by Gary Null, PhD, Carolyn Dean, MD, ND Martin Feldman, MD, Debora
Rasio, MD, Dorothy Smith, PhD
ANNUAL PHYSICAL AND ECONOMIC COST OF MEDICAL INTERVENTION
Salary / Day`
Salary / Month`
Premium/Day`
% ofIncome
Categories
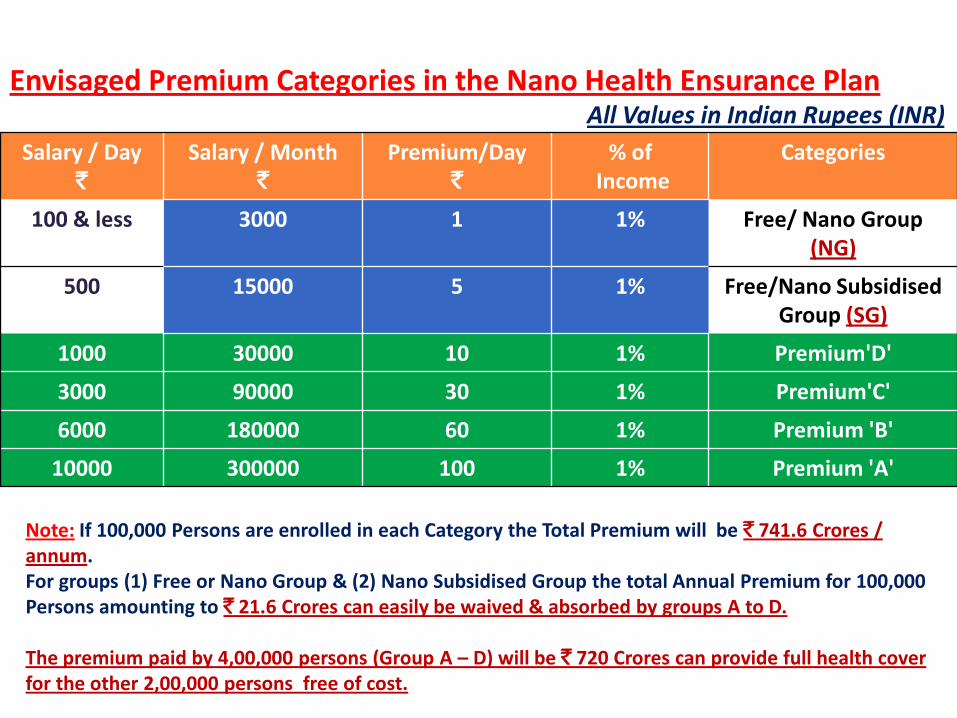
100 & less 3000 1 1% Free/ Nano Group (NG)
500 15000 5 1% Free/Nano Subsidised Group (SG)
1000 30000 10 1% Premium'D'
3000 90000 30 1% Premium'C'
6000 180000 60 1% Premium 'B'
10000 300000 100 1% Premium 'A'
Envisaged Premium Categories in the Nano Health Ensurance PlanAll Values in Indian Rupees (INR)
Note: If 100,000 Persons are enrolled in each Category the Total Premium will be ` 741.6 Crores / annum.For groups (1) Free or Nano Group & (2) Nano Subsidised Group the total Annual Premium for 100,000 Persons amounting to ` 21.6 Crores can easily be waived & absorbed by groups A to D.
The premium paid by 4,00,000 persons (Group A – D) will be ` 720 Crores can provide full health cover for the other 2,00,000 persons free of cost.
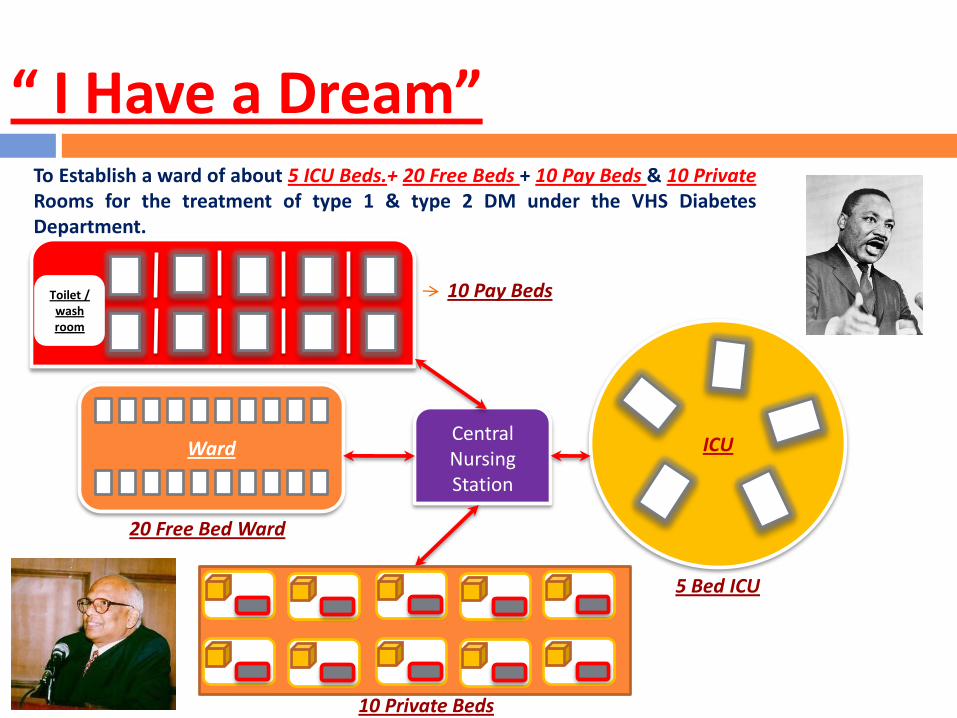
To Establish a ward of about 5 ICU Beds.+ 20 Free Beds + 10 Pay Beds & 10 PrivateRooms for the treatment of type 1 & type 2 DM under the VHS DiabetesDepartment.
“ I Have a Dream”
Toilet / wash room
Ward ICUCentralNursingStation
20 Free Bed Ward
5 Bed ICU
10 Pay Beds
10 Private Beds
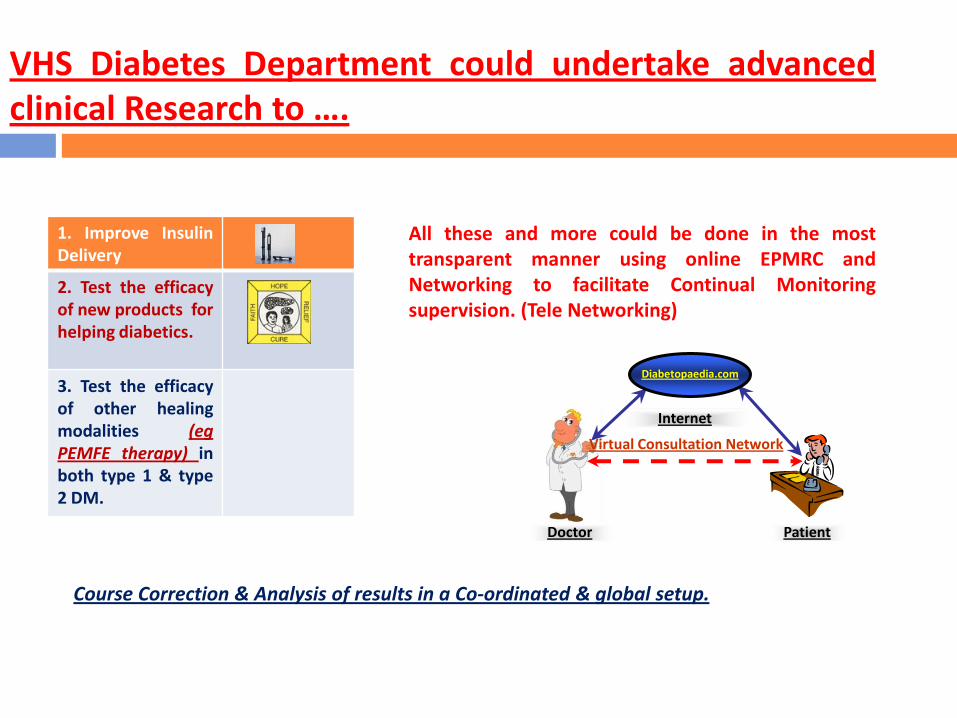
VHS Diabetes Department could undertake advancedclinical Research to ….
1. Improve InsulinDelivery
2. Test the efficacyof new products forhelping diabetics.
3. Test the efficacyof other healingmodalities (egPEMFE therapy) inboth type 1 & type2 DM.
All these and more could be done in the mosttransparent manner using online EPMRC andNetworking to facilitate Continual Monitoringsupervision. (Tele Networking)
Course Correction & Analysis of results in a Co-ordinated & global setup.
Doctor Patient
Internet
Virtual Consultation Network
Diabetopaedia.com
A Completely New Paradigm in Clinical Research
Testing the Efficacy of existing established therapies, approaches and drugs(chemical, plant – based and other forms of drugs in practice around the world,for human healing for centuries).
Authentication using the most up-to date information technology tools forcontinuous Chronological Electronic Case Records (CCECR with secure on-linesystem) for recording all, Clinical, Laboratory, Visual, imaging and all other datathat may be required to diagnose, treat and heal all chronic illnesses. The dataso accrued over the years would be scientifically analysed and the results to bepublish periodically for establishing the best possible treatment modality forevery chronic illness with utmost transparency and truth.
To explore the non-pharmaceutical modes of Pulsed Electro-Magnetic FieldEnergy (PEMFE) and other modes of Energy therapies in promoting healing ofNeuro-cardiac and other serious illnesses that reduce the quality and quantityof life and for which present drug therapies are fraught with more ADR andmortality than the diseases themselves (eg.Diabetes, Hypertension,Cerebrovascular stroke, and Coronary Artery Heart Disease, etc.)
The TAG VHS DIABETES RESEARCH CENTRE
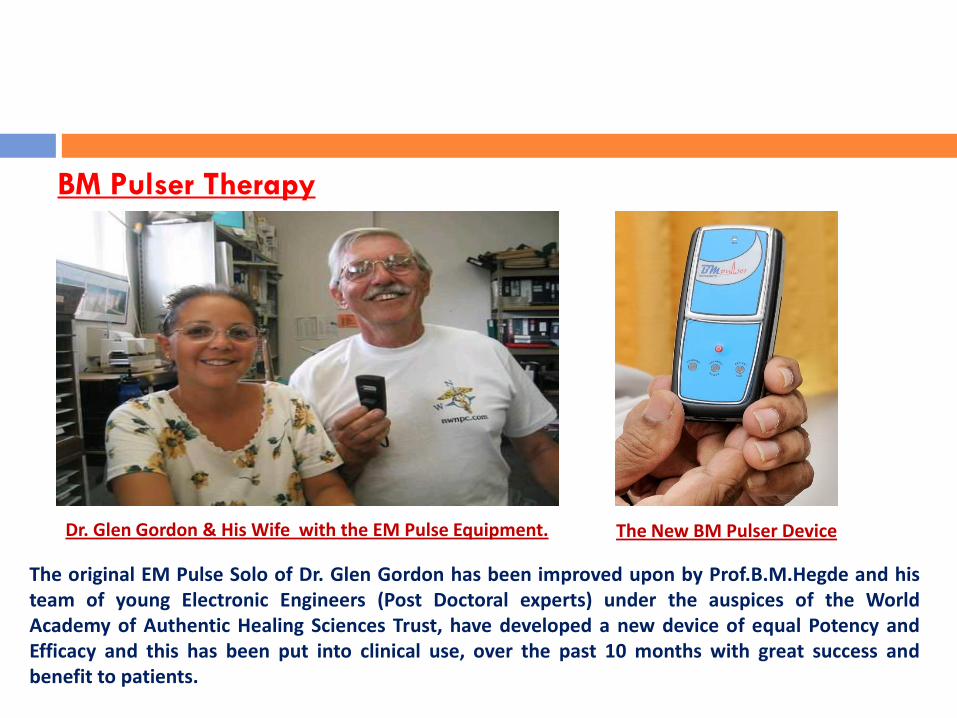
BM Pulser Therapy
The original EM Pulse Solo of Dr. Glen Gordon has been improved upon by Prof.B.M.Hegde and histeam of young Electronic Engineers (Post Doctoral experts) under the auspices of the WorldAcademy of Authentic Healing Sciences Trust, have developed a new device of equal Potency andEfficacy and this has been put into clinical use, over the past 10 months with great success andbenefit to patients.
Dr. Glen Gordon & His Wife with the EM Pulse Equipment. The New BM Pulser Device

Before PEMFE Treatment
Name Mr.VR Sex Male Age 71 Years
AfterPEMFE Treatment
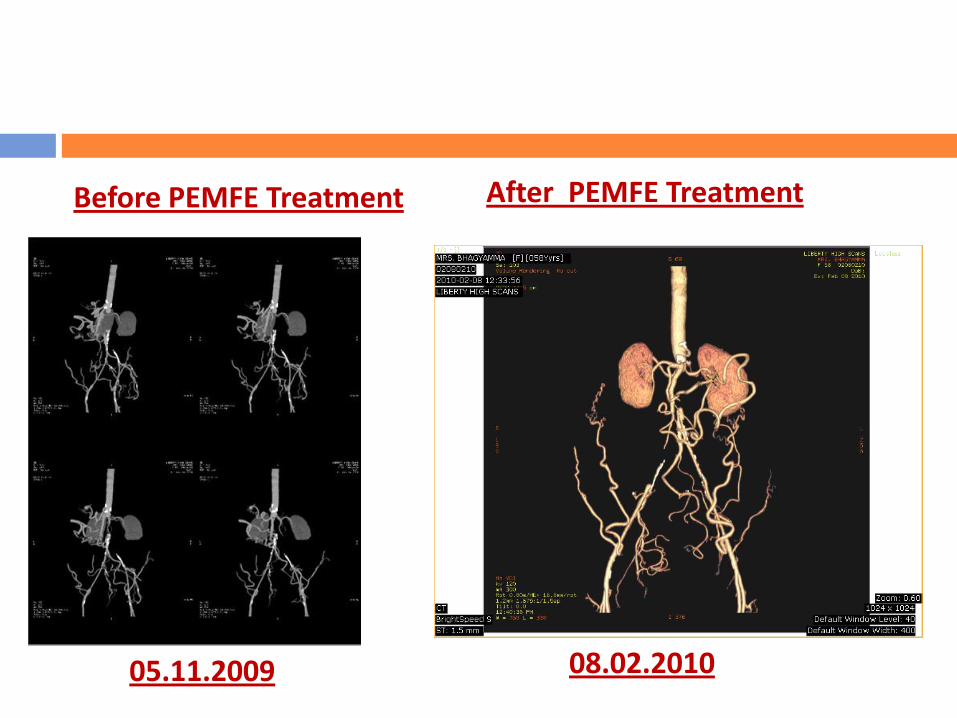
After PEMFE TreatmentBefore PEMFE Treatment
08.02.201005.11.2009
Areas of Collaborative Research between TAG–VHSDIABETES RESEARCH CENTRE & IGCAR.
(I) Effective Insulin Delivery Systems – Wrist Watch Model
Self Administration of Insulin – Using Insulin Pen
Areas of Collaborative Research between TAG–VHS DIABETESRESEARCH CENTRE & IGCAR–Kalpakkam, TAMIL NADU, INDIA
(I) In the field of innovative Electronic Medical Informatics Technology for Providing &Monitoring Unique & Continuous Personalised Multi Modal Medical & Health CareModels with Inbuilt Features of Quality, Security & Cost Effectivity (in Collaboration withM/s. HEALTHTRACK INFO SOLUTIONS). This research Endeavour if done with enthusiasm,intensity & integrity can result in a major breakthrough and may well become a premierexport model for Healthcare Agencies abroad (Western Markets)
(II) Use of PEMFE in the stimulation of endogenous auto stem cell formation for productionof insulin secretion in yours children with type 1 diabetes (who are insulinopenic) anddependant on life-long (several) daily jobs of Insulin!
(III) Research in Biorhythms, Bio-modulation and Bio physical models using space traveltechnology yoga and energy medicine – and nano technology for discovering the anti-degenerative, pro regenerative (auto stem cell) and anti cancer mechanisms in thehuman body.

Nano silver solution. Nanorice solution.Siddha Medicines
(IV) Nanotechnology
Standardization of Metal-Based Herbal Medicines
1Arun Sudha, 2 V.S. Murty and 1T.S. Chandra1Department of Biotechnology, Indian Institute of Technology Madras,Chennai-600 036, India2Department of Physics, Indian Institute of Technology Madras, Chennai-600 036, India
American Journal of Infectious Diseases 5 (3): 200-206, 2009© 2009 Science Publications
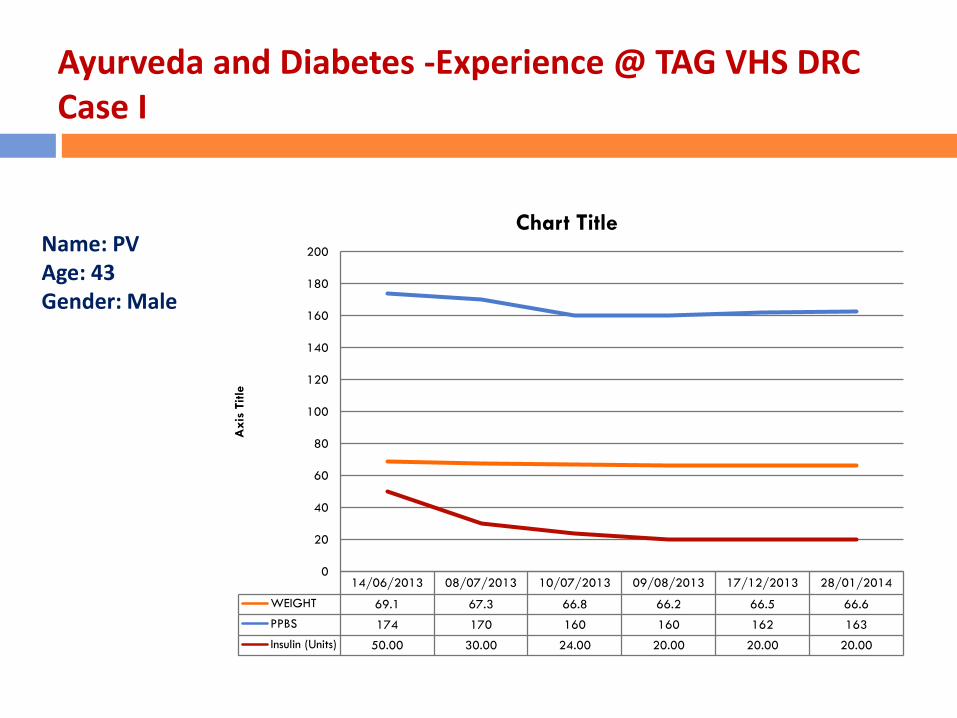
Ayurveda and Diabetes -Experience @ TAG VHS DRC Case I
Name: PV Age: 43Gender: Male
14/06/2013 08/07/2013 10/07/2013 09/08/2013 17/12/2013 28/01/2014
WEIGHT 69.1 67.3 66.8 66.2 66.5 66.6
PPBS 174 170 160 160 162 163
Insulin (Units) 50.00 30.00 24.00 20.00 20.00 20.00
0
20
40
60
80
100
120
140
160
180
200A
xis
Title
Chart Title
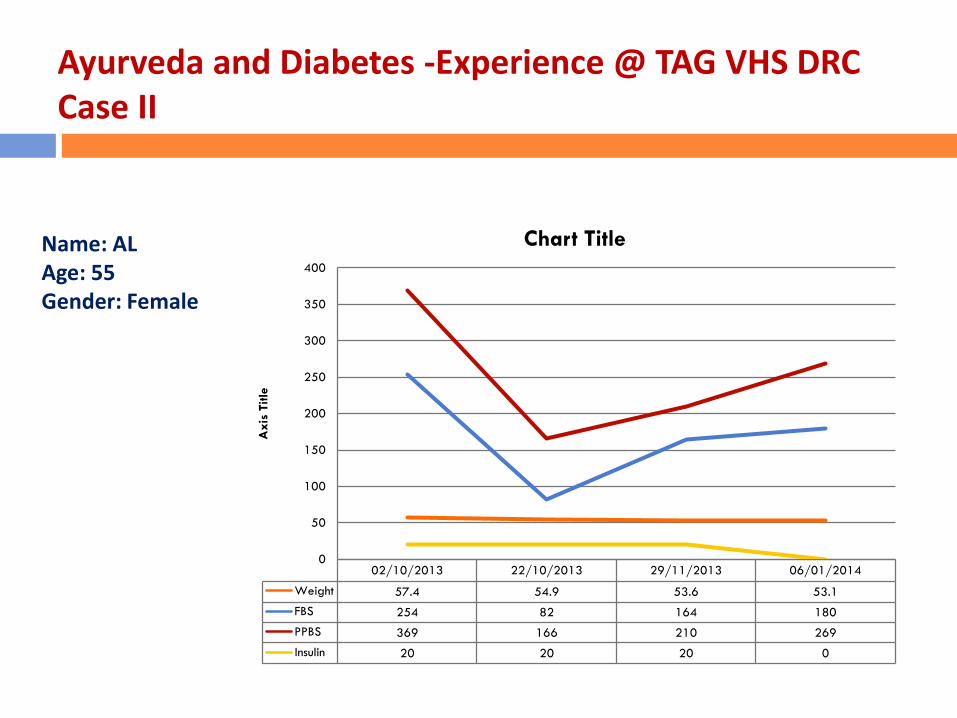
Ayurveda and Diabetes -Experience @ TAG VHS DRC Case II
Name: ALAge: 55Gender: Female
02/10/2013 22/10/2013 29/11/2013 06/01/2014
Weight 57.4 54.9 53.6 53.1
FBS 254 82 164 180
PPBS 369 166 210 269
Insulin 20 20 20 0
0
50
100
150
200
250
300
350
400A
xis
Title
Chart Title
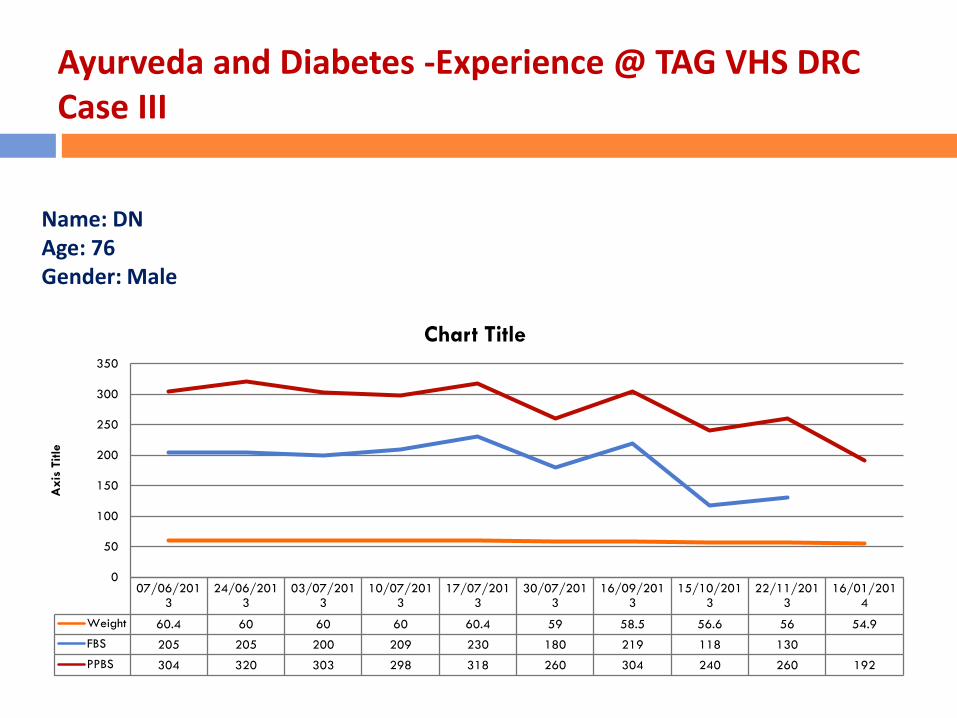
Ayurveda and Diabetes -Experience @ TAG VHS DRC Case III
Name: DNAge: 76Gender: Male
07/06/2013
24/06/2013
03/07/2013
10/07/2013
17/07/2013
30/07/2013
16/09/2013
15/10/2013
22/11/2013
16/01/2014
Weight 60.4 60 60 60 60.4 59 58.5 56.6 56 54.9
FBS 205 205 200 209 230 180 219 118 130
PPBS 304 320 303 298 318 260 304 240 260 192
0
50
100
150
200
250
300
350
Axis
Title
Chart Title
Dynamic Acupuncture Mediated Metaphysical (DAMM) therapy
The new healing modality that being researched at the TAG VHS DRC which we havenamed Dynamic Acupuncture Mediated Metaphysical therapy (DAMM) is anexpression of physical energy of healing, acquired through a rigorous personalunderstanding and divine gift with a tremendous background of practice done by ourtherapist Mr.RajanIyer who has combined all the arts of energy healing (resulting inhis own brand) and customised metaphysical energy release into the human bodythrough a holistic understanding and experience of all modes of healing and transferof macrocosmic energy into the body’s cell (microcosmic level – chi energy).TheDAMM therapy a unique and novel way of infusing and transferring healing energyfrom the therapist to the patient.
These concepts of energy healing are enshrined in the ancient Indian textsofAtharvaveda, which was an off-shoot of the millinea old rig veda – the ancientinscriptions are found in the various temples of north India (Gujarat & Orissa) and inthe south,near Tindivanam&Kanchipuram (Tamil Nadu).Scholars well-versed inAtharvanavedaSastra are very few in the country.
The DAMM therapy a unique and novel way of infusing and transferring healingenergy from the therapist to the patient. This is entirely different from thetraditional Chinese or Japanese acupuncture techniques, but works with lightningspeed in the body of the recipient, to set right the dysfunctional cells that causedisability (? Disease) in the various systems like the Locomotor (Joints, Tendons &muscle), Central, peripheral and autonomic nervous system, cardiovascular system,Alimentary system including Liver, gall bladder, Pancreas, Kidneys and the Genito-urinary systems, Eyes and vision, auditory/hearing/vertigo, Endocrine glands,Haematological disorders and the skin and lymphatic diseases.
Apart from these, DAMM Therapy exerts positive effects, with benefits, in modifyingand improving various conditions like, mental retardation, autism, cerebral palsies,BPD etc. to a great extent especially provided they are started in the early stages ofthe condition. It could be planned and given in tandem with the physicians,psychiatrists and the support team of counselors and social workers.
Dynamic Acupuncture Mediated Metaphysical (DAMM) therapy
The most remarkable observation of this DAMM therapy that has emerged from the pilotstudies done so far at TAG VHS DRC, is the speed with which healing takes place for whatare apparently chronic or long drawn-out disabilities which at present are treated bycomplex, expensive and drug-based therapies which are often replete with side-effectsand are of limited success.
Metaphysical energy therapy which is impressive in getting results with lightning speed isnot based on other esoteric practises like Hypnotism or magic, but is a viable andsustainable healing modality, as has been shown from our experience of over 250 casesduring the past 5 months (since August 2012).
These procedures are all done transparently fully documented in our EMR and whereindicated photographed, and video graphed (with full consent of the patients and withtheir privacy fully protected).
This project is the first of its kind, one of its kind, and incorporates the various novelfeatures mentioned above; it is patient - friendly, highly cost effective, and with virtuallyno side-effects. It is proposed to study in the Phase I of this research project, 100 cases ofall types of Liver ailments and allied intractable digestive disorders, that will be taken upfor treatment, documentation and follow-up at the TAG VHS DRC.
Dynamic Acupuncture Mediated Metaphysical (DAMM) therapy

Mr. DB aged 68 years, right sided bell’s palsy was admitted to TAG VHS DRC with trial ofDynamic Acupuncture Mediated Meta Physical Therapy (DAMM) 2 sittings by Mr. Rajan.He was continued with his previous prescription. His Capillary Blood Sugar Levels weremonitored through-out the day.He improved with the DAMM Therapy and he was discharged on 13/08/2012 with the advice toreview after 1 week to see the clinical progress.
Before Therapy (10-08-2012) After Therapy (13-08-2012)
Case I
Case I
Case I

Case I
Case I
Patient got admitted to a leading corporate Hospital on 27/10/2012, DOD: 19/11/2012 withalleged history of RTA on 26/10/2012 around 9 PM while riding two wheeler. Initially he wastreated at GGH where he was intubated due to low GCS and shifted to its group SpecialityHospital for further care. History of loss of consciousness since the time of accident. History ofvomiting present. No history of ENT bleed or seizures. No comorbids.
CT scan brain showed left high parietal thin SDH and SAH.MRI brain showed lacunar infarct in the right internal capsule with diffuse axonal injury.
He was treated with anti convulsants, analgesics, antibiotics, anti edema measures andother supportive medication.
Opinion was obtained from Faciomaxillary surgeon for multiple facial bone fractures and headvised ORIF for the same once the patient becomes stable.
Opinion was obtained from Ophthalmologist for left eye chemosis and his advice followed. Inview of prolonged airway maintenance and tracheal toileting tracheostomy was done by ENTsurgeon on 30/10/2012.
Case II

Patient was discharged from the corporate Hospital at request and received at 3 pm on19/11/2012 at TAG VHS DRC:
Diagnosis at discharge:Traumatic brain injury withA. Diffuse axonal injuryB. Subarachnoid haemorrhageC. Lacunar infarct in the right internal capsule – left hemiplegiaD. Parafalcine subdural haemorrhage on the left side• Multiple facial bone fractures:• Multiple soft tissue injuries.• Lower respiratory tract infection.• Diabetes Mellitus.
Patient was received in our ICCU. While receiving patient was (E3 M4 VT) T2DM on insulin(Inj.Lantus 16u at night) Patient came for BM Pulser, DAMM therapy, Physiotherapy and forfurther management.He came with Tracheostomy tube, Ryle’s tube feeding and condom drainage.He was treated with Inj. Human Actrapid insulin, Anticonvulsant, Bronchodilators, Antioxidants and vitamins.
Case II

Everyday :He was given Dynamic Acupuncture Mediated Metaphysical (DAMM) therapy by Mr. Rajan Iyer,Pulsed Electro Magnetic Field Energy therapy using BM pulser over the appropriate areas of thescalp and the limbs.And physiotherapy by Mr. Anand Kumar, Physiotherapist .
Gradually :His conscious status improved and became normal.His mentation improved remarkably and he was able to speak normally, follow commands andanswer questions coherently.He is able to walk mostly on his own with little support.Ryle’s tube was removed and he was able to eat on his own.Condom drainage was removed and he was able to void urine on his own.
Under advice from Prof. Mohan Kameshwaran, ENT Specialist, the tracheostomy tube wasremoved on 14/12/2012 and he is able to breathe on his own.
Case II
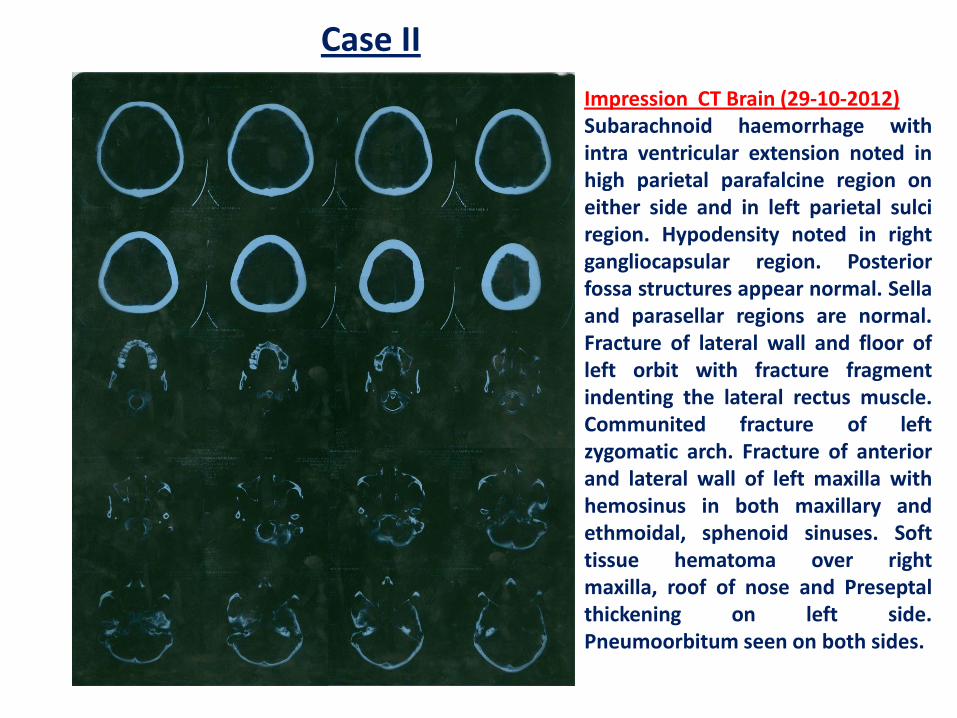
Impression CT Brain (29-10-2012)Subarachnoid haemorrhage withintra ventricular extension noted inhigh parietal parafalcine region oneither side and in left parietal sulciregion. Hypodensity noted in rightgangliocapsular region. Posteriorfossa structures appear normal. Sellaand parasellar regions are normal.Fracture of lateral wall and floor ofleft orbit with fracture fragmentindenting the lateral rectus muscle.Communited fracture of leftzygomatic arch. Fracture of anteriorand lateral wall of left maxilla withhemosinus in both maxillary andethmoidal, sphenoid sinuses. Softtissue hematoma over rightmaxilla, roof of nose and Preseptalthickening on left side.Pneumoorbitum seen on both sides.
Case II

ImpressionCT Brain (28-12-2012)Reduction of axonal hemorrhage inright basal ganglia and centrumsemiovale compared to previousstudy. Complete resolution ofsubarachnoid and subduralhemorrhage. Microbleeds in leftperiventricular white matter andmedial temporal gyrus
Case II
Mr. P.M. J.J aged 65 years, got admitted to TAG VHS DRC on 02/08/2012 with the c/o Severe pain left knee for past 1year, more severe since 4 weeks. Unable to walk, sit, squat. Now right knee also has started paining. On admissionBP: 160/90 mmHg, PR: 74/min, Weight: 117.2 kgs. Afebrile. Left knee swelling +, stiffness +, unable to walkfreely, knee support to walk.
He was started therapy with Chinese volcanic ash with oil application for 6 hours followed by Pulsed ElectromagneticField Energy therapy using BM Pulser 14 hours a day at three strategic areas over the knee for 3 days.
He says there is very minimal relief with the above treatment and on Sunday 05/08/2012 he had very severe pain forwhich he required oral + injectable NSAID’s. After the informed consent he was started on Acupuncture therapy byAcupuncture Specialist Mr. Rajan Iyer.
From 06/08/2012 to 08/08/2012 he had 3 sittings of Acupuncture therapy following which he had significant reliefand he is able to walk freely, bend his knee, climbing stairs which were not possible earlier.
During his stay routine baseline investigations were done 24 hours protein excretion 89.9 mg/day, 24 hrs urinevolume: 2900 ml/day.
His blood sugars were normal throughout and his OHA requirement has come down to 50%.At the time of discharge his knee pain has comedown significantly, no edema, able to walk freely. Weight: 116.2kgs, BP: 130/80 mmHg, PR: 70/min.
He got discharged on 08/08/2012 with the revised prescription and advised to followup with Mr. Rajan IyerAcupuncture therapist for further course and advised to report after 3 weeks with FBS, PPBS and Urine analysis.
Case III
Mr. S.G aged 79 years, a known Hypertension and Parkinsonism admitted to TAG VHS DRC on16/09/2012 to improve his following symptoms.
1. He can't sit and getup without support.2. Unable to walk.3. Excessive salivation.4. Slurred speech.5. Getting started for an activity is very difficult for few minutes.6. Feeding is reduced in amount.7. Typical Parkinson’s gait and mask like face.8. Loss of weight - 18kgs within 2 1/2 yrs.9. Occasionally regurgitation is present.
His vitals on admission were normal but he was non ambulant. Pulsed Electro Magnetic FieldEnergy Therapy using BM Pulser was applied over several strategic areas of the scalp. Also givento him 5 sittings of a new modality called Dynamic Acupuncture Mediated Metaphysical(DAMM) Therapy by Mr. Rajan Iyer.After the 1st session he is started showing all round improvement - his gait improved, he is ableto walk better, excessive salivation & tremors reduced.ECG & Cardiac Echo done both were NAD.
Case IV
His medication were tapered gradually, there was no rebound sequelae.
At the end of 1 week, he showed satisfactory improvement. He was taught to use the BM Pulserat strategic areas over the scalp and he was also given physiotherapy.
He is advised to get discharged on 25/09/2012. On discharged his vitals are stable, he showedsignificant improvement in above said complaints. He was advised to use the PulsedElectromagnetic Field Energy therapy using BM Pulser at strategic areas around 14 to 16 hours aday and continue physiotherapy, Exposure to sunlight 15 minutes per day, Pranayama 15 minutesper day.
Case IV
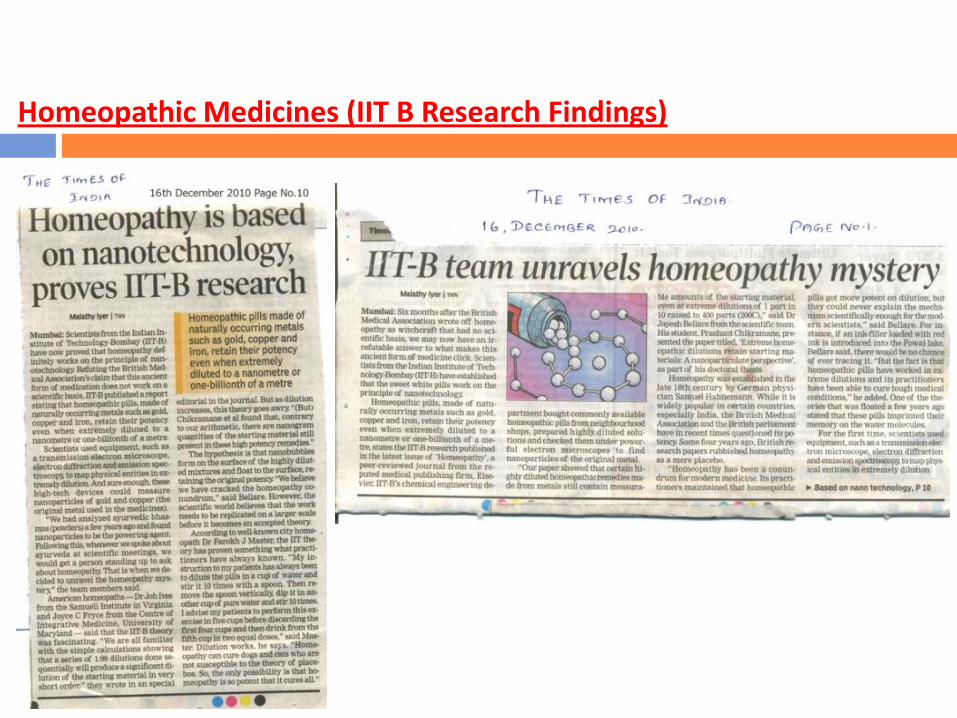
Homeopathic Medicines (IIT B Research Findings)
We have the talent, resources both human, material & economic;Will the Ancient Wisdom of our country unite with Modern Scientific Research for Scripting a new chapter in Future Techno Medical Research?I believe we can! (A-la OBAMA).IGCAR is the Right place, This is the right time, Sir, you are the right person & you are leading a Brilliant Team (A-la-M.S.Dhoni).We can then lay Claim to be leaders of the Scientific World !!
Sarve Jana Sukino Bhavanthu (Sanskrit) (Let all beingsbe healthy and happy) – Vedas.

Thank You All