Embed Size (px)
Citation preview
Report onReport on
CLINICAL PRACTICE GUIDELINES
The American Urological AssociationProstate Cancer Clinical Guidelines Panel
The Management ofClinically LocalizedProstate Cancer
The Management ofClinically LocalizedProstate CancerArchived Document—
For Reference Only
Richard G. Middleton, MD(Panel Co-Chairman)Department of UrologyThe University of UtahSalt Lake City, Utah
Ian M. Thompson, MD(Panel Co-Chairman)Urology ServiceBrooke Army Medical CenterSan Antonio, Texas
Mark S. Austenfeld, MD(Panel Facilitator)Department of UrologyThe University of Kansas MedicalCenter
Kansas City, Kansas
William H. Cooner, MDDepartment of UrologyEmory UniversityAtlanta, Georgia
Roy J. Correa, Jr., MDDepartment of UrologyThe Virginia Mason ClinicSeattle, Washington
Robert P. Gibbons, MDDepartment of UrologyThe Virginia Mason ClinicSeattle, Washington
Harry C. Miller, Jr., MDDepartment of UrologyThe George Washington UniversityWashington, D.C.
Joseph E. Oesterling, MDDivision of Urology and the MichiganProstate Institute
The University of MichiganAnn Arbor, Michigan
Martin I. Resnick, MDDepartment of UrologyCase Western Reserve UniversityCleveland, Ohio
Stephen R. Smalley, MDTherapeutic Radiologists, Inc.Kansas City, Missouri
John H. Wasson, MDProstate Patient Outcomes ResearchTeam
Dartmouth Medical SchoolHanover, New Hampshire
Claus G. Roehrborn, MD(Facilitator Coordinator)Division of UrologyThe University of Texas SouthwesternMedical Center
Dallas, Texas
Hanan S. Bell, PhD(Consultant in Methodology)Seattle, Washington
Brent Blumenstein, PhD(Consultant in Biostatistics)Fred Hutchinson Cancer CenterSeattle, Washington
Scott Optenberg, Dr. PH(Consultant for Health CareEconomics)
Clinical Investigation ActivityU.S. Army Health Services CommandSan Antonio, Texas
Patrick M. Florer(Database Design and Coordination)Dallas, Texas
Curtis Colby(Editor)Washington, D.C.
Prostate Cancer Clinical Guidelines Panel Members and Consultants
Dedication
This report is dedicated to the memory of William H. Cooner, MD, who lentinvaluable support, time and encouragement to the efforts of the panel.
The Prostate Cancer Clinical Guidelines Panel consists of board-certified urologists and other ex-perts in prostate cancer management. This Report on the Management of Clinically Localized ProstateCancerwas extensively reviewed by nearly 40 urologists throughout the country in early 1995. Thepanel finalized its recommendations for the AUA’s Practice Parameters, Guidelines and StandardsCommittee, chaired by Winston K. Mebust, MD, in June 1995. The AUA Board of Directors approvedthese practice guidelines in July 1995.
The Summary Report also underwent independent scrutiny by the Editorial Board of the Journalof Urology, was accepted for publication in August 1995 and appeared in its December issue. APatient’s Guideand a Technical Supplementhave also been developed; both are available from theAUA.
The American Urological Association expresses its gratitude for the dedication and leadershipdemonstrated by the members of the Prostate Cancer Clinical Guidelines Panel in producing thisguideline.
Members Consultants
ISBN 0-9649702-0-1
Archived Document— For Reference Only
Page iCopyright © 1995 American Urological Association, Inc.
Prostate cancer is the most common nondermatologic malignancy and thesecond most common cause of cancer death among men in the United States.In 1995, an estimated 244,000 new cases were anticipated, and prostate cancerdeaths were estimated at 40,400 (Wingo, Tong and Bolden, 1995). For a whitemale born in 1988-1990, the lifetime risk of developing clinically apparentprostate cancer is 13.34 percent. For an African-American male, the risk is11.27 percent (Miller, Hayes, Potosky, et al., 1993). Lifetime risks of deathfrom prostate cancer in these two groups are 3.18 percent and 3.96 percent, re-spectively. Because of an aging U.S. population, the number of men recog-nized to have prostate cancer will rise dramatically over the next 20 years.During the next 10 years, it is estimated that there will be a 90-percent in-crease in prostate cancer detection and a 37-percent increase in prostate cancerdeaths (Carter and Coffey, 1990).
Enhanced early detection techniques using digital rectal examination (DRE)and prostate specific antigen (PSA), as well as more public awareness of pros-tate cancer, have greatly increased rates of diagnosis. One result has been ashift toward more tumors detected at lower stages. In 1982, an American Col-lege of Surgeons survey found the following percentages, by clinical stage, ofnewly diagnosed prostate tumors: stage T1 (A), 25.9 percent; stage T2 (B),28.9 percent; stages T3-T4 (C), 14.9 percent; stage M1 (D2), 24.9 percent(Murphy, Natarajan, Pontes, et al., 1982). A 1990 survey found that more new-ly diagnosed tumors were organ confined: stage T1 (A), 29.3 percent; stage T2(B), 37.7 percent; stages T3-T4 (C), 12.5 percent; and stage M1 (D2), 20.6percent (Mettlin, Jones and Murphy, 1993). At a number of institutions wherePSA is an integral part of early diagnosis, as many as 99 percent of prostatecancers diagnosed during serial PSA-based screening have been clinically or-gan confined, and 75 percent pathologically organ confined (Catalona, Smith,Ratliff, et al., 1993).
With this growth in numbers of locally confined tumors found through earlydetection efforts has come greater scrutiny of the methods of treatment. A 1988National Institutes of Health (NIH) consensus conference, employing an im-plicit approach to the development of conclusions, compared the efficacy ofsurgical therapy and radiotherapy. It was not possible, based upon available da-ta, to determine the optimal treatment for localized disease (NIH ConsensusDevelopment Panel, National Cancer Institute’s Monograph No. 7, 1988).
Since that time, the publication of a number of series on the management ofclinically localized prostate cancer by surveillance (no treatment) has increasedthe uncertainty as to the optimal treatment for this stage of disease. For low-grade tumors, these series have generally reported cancer-specific survivalswith management by surveillance that do not differ significantly from cancer-
Introduction
Archived Document— For Reference Only
Page ii Copyright © 1995 American Urological Association, Inc.
specific survivals following treatment by surgery or radiotherapy for periods upto 10 years (Johansson, Adami, Andersson, et al., 1992; Whitmore, Warner andThompson, 1991). Pooled analyses and decision analyses employing data fromsurveillance series have further clouded the question of optimal treatment forlocalized disease (Chodak, Thisted, Gerber, et al., 1994; Fleming, Wasson,Albertsen, et al., 1993).
Recognizing the need for a systematic analysis of the literature regardingthe available methods of treatment for localized prostate cancer, and in the ab-sence of a randomized, prospective comparison of these methods, theAmerican Urological Association (AUA) in 1989 convened the Prostate CancerClinical Guidelines Panel to conduct a comprehensive survey and analysis ofpublished data. This document,Report on the Management of Clinically Local-ized Prostate Cancer,is the product of that effort.
This report, as its title indicates, focuses on the treatment of tumors con-fined within the prostate, specifically clinical stage T2 (B) tumors. (“Stage” inthis document means “clinical stage” unless “pathological stage” is specified.)Inevitably discussed in this report are stages other than T2, questions regardingstaging methods and various issues related to the diagnosis as well as treatmentof prostate cancer in general. However, the panel’s analysis and recommenda-tions are intended to apply only to treatment of clinically localized prostatecancer.
The report summarizes the methodology employed by the panel, displaysthe outcomes evidence extracted from the prostate cancer treatment literatureand recommends practice policies for the management of clinical stage T2 (B)prostate cancer insofar as the evidence permits. The report also includes analy-sis of the limitations in the treatment literature regarding outcomes evidenceand makes recommendations for further research.
A summary of this report has been published in the Journal of UrologyDecember 1995: Vol. 154, pgs. 2144 – 2148. A 12-page Patient’s Guidein-cluding illustrations of the progressions of prostate cancer is available to assistthe physician in discussing treatment options with the patient. Also available isa Technical Supplementproviding more detailed displays of the data analysis.
Archived Document— For Reference Only
Page iiiCopyright © 1995 American Urological Association, Inc.
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .iExecutive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1
Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1Treatment alternatives and treatment outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Treatment recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3Literature limitations and recommendations for research . . . . . . . . . . . . . . . . . . . . .6
Chapter 1: Methodology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8Methods and definitions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8Literature search . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Data extraction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Data inadequacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9Data display for survival and disease progression . . . . . . . . . . . . . . . . . . . . . . . . . .10Treatment complications data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .10Literature citations and panel opinions in discussion sections . . . . . . . . . . . . . . . . .10
Chapter 2: Prostate cancer and its management . . . . . . . . . . . . . . . . . . . . . . . . . . .12Background . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12Natural history and grade classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .12Staging . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13Treatment alternatives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .15
Chapter 3: Outcomes of treatments for localized prostate cancer . . . . . . . . . . . . .21Types of outcomes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .21Variability of outcomes data . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22Summary outcomes tables and graphs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .22Analysis of summary outcomes tables . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .32Treatment complications summary outcomes table and graphs . . . . . . . . . . . . . . . .35Analysis of treatment complications summary outcomes table . . . . . . . . . . . . . . . . .36
Chapter 4: Treatment recommendations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37The standard patient . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37Recommendations: Standards . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37Recommendations: Treatment options . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38Advantages and disadvantages of treatment options . . . . . . . . . . . . . . . . . . . . . . . . .38
Chapter 5: Literature limitations and recommendations for research . . . . . . . . . .42Limitations in the prostate cancer treatment literature . . . . . . . . . . . . . . . . . . . . . . .42Recommendations for future research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .43
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .46Appendix A: Data presentation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .A-1Appendix B: Data abstraction form . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .B-1Appendix C: U.S. life expectancy table . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .C-1Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .I-1
Archived Document— For Reference Only
Production and layout by
Lisa EmmonsTracy Kiely
Betty Roberts
Copyright © 1995American Urological Association, Inc.
Archived Document— For Reference Only
Page 1 Executive SummaryCopyright © 1995, American Urological Association, Inc.
In developing recommendations for the manage-ment of clinically localized prostate cancer, theAUA Prostate Cancer Clinical Guidelines Panel ex-tensively reviewed the prostate cancer treatment lit-erature from 1966 to December 1993 and extractedall relevant data to estimate as accurately as possi-ble desirable and undesirable outcomes of the alter-native treatment modalities. The panel followed anexplicit approach to guideline development (Eddy,1992). This approach emphasizes use of scientificevidence in estimating outcomes of interventions.When panel opinion is necessary, the explicit ap-proach calls for explaining why and discussing thefactors considered. For a full description of themethodology, see Chapter 1.
Of the malignant conditions that arise primarilywithin the prostate gland, by far the most frequentlyoccurring type is adenocarcinoma. Because of therarity of other primary neoplasms within the gland,the terms “prostate cancer” and “carcinoma of theprostate” are generally understood to be synony-mous with “adenocarcinoma.”
Adenocarcinoma of the prostate is the most com-monly diagnosed visceral neoplasm in men. The es-timated 244,000 new cases diagnosed in 1995 rep-resent 36 percent of cancers in men, compared with14 percent for lung cancer and 10.4 percent for col-orectal cancer, the next two most frequently diag-nosed cancers (Wingo, Tong and Bolden, 1995).The 40,400 deaths from prostate cancer anticipatedin 1995 represent 14 percent of all cancer deaths inmen, placing prostate cancer second only to lungcancer mortality (33 percent) and ahead of colorec-tal cancer mortality (9.4 percent).
Natural historyProstate cancer has a wide spectrum of growth
rates. Many tumors pursue a relatively indolent
course over many years. Others advance rapidly bylocal extension and/or metastasis. Evaluation of theeffect of active intervention must take into accountthe course the disease would follow if allowed toproceed without interference. Active treatment of aprostatic cancer destined never to present a clinicalproblem would not be expected to improve patientoutcomes over treatment by surveillance alone.Prostate cancer aggressiveness, however, does tendto increase with time (Adolfsson and Tribukait,1990). Given sufficient time, small localized tumorscan be expected to become large, multifocal, nonlo-calized tumors (Whitmore, Warner and Thompson,1991), with decreasing likelihood of cure. “Cure” isdefined in this report as lifetime freedom from dis-ease.
Thus, patient longevity becomes a major consid-eration, especially since techniques to distinguishrapidly growing from slow-growing tumors are stillevolving. Treatment of prostate cancer depends to asignificant degree upon the patient’s age, functionallevel and medical status. Factors such as tumor vol-ume (stage) and grade, along with evaluation of nu-clear chromatin content and nuclear roundness, al-low some prediction of a tumor’s biologic potential.However, at present, such factors are not all fullyapplicable to individual patients because of themany exceptions to these predictive indices.
StagingAccurate determination of tumor stage is impor-
tant, in that therapy is highly dependent upon theknowledge of whether the tumor is localized to thegland. Several staging systems for prostate cancerhave been described. The two most often used arethe Jewett-Whitmore (ABCD) system and theAmerican Joint Committee (TNM) system. Theyare shown in Table 1 on page 13. A new clinicalstage has been designated primarily for PSA-detect-ed prostate cancers. In the TNM staging system,these tumors are categorized as stage T1c and in theJewett-Whitmore staging system as stage B0.
Clinical staging has improved in recent years,but considerable inaccuracy remains. The result canbe understaging or, to a lesser extent, overstaging ascompared with surgical or pathologic staging. This
Background
Methodology
Executive summary:Report on the management of clinically localized prostate cancer
Archived Document— For Reference Only
Page 2 Executive Summary Copyright © 1995, American Urological Association, Inc.
has confounded accurate evaluation of treatmentmodalities based solely upon clinical staging.
Methods available for the staging of clinicallylocalized prostate cancer include digital rectal ex-amination (DRE), serum prostate specific antigen(PSA), serum acid phosphatase, transrectal ultra-sonography (TRUS), computerized tomography(CT) scan and magnetic resonance imaging (MRI).For determination of distant metastases, stagingmethods include CT scan, MRI and radioisotopicbone scan. In the panel’s opinion and based ongrowing evidence from recent studies, many of themethods available do not necessarily provide usefulinformation and may not be required for patientswith clinically localized prostate cancer.
Regarding clinical staging, several conclusionscan be drawn from the medical literature that affectclinical practice:
(1) CT scan and MRI may not be required in thestaging evaluation of patients with clinically local-ized prostate cancer. These tests can often detectgross extraprostatic disease, but that degree ofspread can usually be predicted by the serum PSAconcentration, DRE or TRUS at time of biopsy.Capsular perforation, seminal vesicle invasion andpelvic lymph node involvement most often are mi-croscopic phenomena and cannot be diagnosed byeither CT scan or MRI.
(2) Evidence is mounting that the majority ofpatients who are candidates for a radical prostatec-tomy or radiotherapy have a very low risk of havingpositive pelvic lymph nodes. When the serum PSAconcentration, tumor grade and local clinical stageused together are below certain levels, a pelviclymph node dissection may not be necessary be-cause, as noted on page 15, the probability of posi-tive lymph nodes is extremely low.
(3) From the results of two large clinical studies(Chybowski, Larson-Keller, Bergstralh, et al., 1991;Oesterling, Martin, Bergstralh, et al., 1993), it ap-pears that a staging radionuclide bone scan may notbe necessary for patients with newly diagnosed, un-treated prostate cancer who have no skeletal symp-toms and a serum PSA of 10 ng/ml or less.
The following treatment alternatives in currentuse for managing localized prostate cancer, eitheralone or in various combinations, were analyzed bythe AUA Prostate Cancer Clinical Guidelines Panel:
radical prostatectomy, external beam radiotherapy,brachytherapy (interstitial radiotherapy) and sur-veillance (also known as expectant management,watchful waiting or observation). Treatment meth-ods considered investigational are thermotherapy,cryotherapy, androgen deprivation and chemothera-py. The panel categorized a treatment method as in-vestigational if the number of patients treated hasbeen inadequate for evaluation and/or if follow-uphas been inadequate to provide sufficiently preciseoutcome estimates.
Treatment outcomesFor assessing the benefits and harms of treatment
interventions for stage T2 (B) prostate malignancy,the panel considered the following outcomes asmost important to the patient:
(1) Survival at 5, 10 and 15 years (overall sur-vival, disease-specific survival, progression-freesurvival and metastasis-free survival);
(2) Progression rates at 5, 10 and 15 years(metastatic, local and biochemical); and
(3) Complications of treatment. Although allcomplications were evaluated, the most importantare: death from treatment, incontinence, impotence(erectile dysfunction), cystitis, proctitis, majorbleeding, pulmonary embolism, rectal injury andbladder neck contracture/urethral stricture.
Survival at 5, 10 and 15 years
Clinically localized prostate cancer (stages T1and T2) is rarely lethal within the first 5 years afterdiagnosis. The overall death rate during this periodis low and usually secondary to comorbid process-es. Almost any treatment for localized prostate can-cer would appear to have an excellent survival re-sult at 5 years. Survival at 10 years and 15 years al-lows a more accurate assessment of the influence ofprostate cancer treatment on patient survival.
It is not enough to assess survival independentlyof tumor progression status. Comorbid processesassociated with advanced age will often determinesurvival. However, morbidity from cancer progres-sion may occur for years prior to death. It is there-fore reasonable to inform patients not only aboutthe risk of dying from prostate cancer, but alsoabout the risk of developing metastatic disease orany evidence of tumor recurrence during follow-up.Thus, outcomes of cancer-specific metastasis-freeand tumor-free survival should be assessed in addi-tion to overall survival rates.
Treatment alternativesand treatment outcomes
Archived Document— For Reference Only
Page 3 Executive SummaryCopyright © 1995, American Urological Association, Inc.
Progression rates at 5, 10 and 15 years
After surgery or radiotherapy, most recurrence orprogression of adenocarcinoma of the prostate willbecome biochemically (PSA) apparent by 5 years,but a few patients may have lengthy delays beforethe progression becomes clinically apparent. It istherefore important to continue to assess progres-sion rates to 10 years and beyond. Progression ratesmay or may not influence the patient directly. Manytimes progression will be defined as the develop-ment of any evidence of tumor. This recurrence isoften asymptomatic and found only through sur-veillance examinations.
Obviously, either local recurrence or sympto-matic metastatic prostate cancer is of extreme im-portance to patients diagnosed with localized dis-ease. However, biochemical failures, usually in theform of rising serum PSA, may also negatively im-pact patients from a psychologic standpoint. Menwith prostate cancer understand that a rising serumPSA often precedes eventual symptomatic recur-rence.
Complications and harms of treatment
Treatment-related death, the most serious ad-verse outcome from treatment of prostate cancer, isuncommon. Other adverse outcomes from treat-ment, such as incontinence, impotence (erectiledysfunction), cystitis, rectal injury and bleeding, aremore common and have variable degrees of nega-tive impact on patient well-being. The reported in-cidences and estimates of these adverse outcomesare important to a patient making decisions regard-ing treatment. Some of the complications are muchless common today than in older reports because ofnewer technology and advancements in technique.It is important to stratify the complications relativeto era of treatment. (See Appendix A, Figures A-7to A-31.)
Analysis of outcomes data fromthe literature
The panel was impressed by the massive amountof literature available on prostate cancer, but thevast bulk of the literature is not usable for extract-ing and combining data to assess treatment out-comes and develop practice recommendations. Of12,501 papers reviewed, the panel was able to re-trieve only 165 with acceptable data on outcomesfrom treatment of localized prostate cancer. (Seepage 9 for an explanation of the review process.)Moreover, in these 165 articles, there are significantdifferences among treatment series regarding such
characteristics as patient age, tumor grade and pel-vic lymph node status. For example, patients under-going radical prostatectomy are on average 3 yearsyounger than those undergoing external beam ra-diotherapy and 7 years younger than those reportedto have been followed with surveillance.
It is striking that only about one in seven patientsreported in the literature was followed even for 5years and that a very small fraction was followedfor 10 or 15 years. Estimates of important out-comes—notably survival and progression rates at 5,10 and 15 years—are likely to be inaccurate if suchsmall numbers of patients are available for analysis.
Tumor grades are relatively comparable in pa-tients treated actively (with surgery or radiation);but for patients followed with surveillance, thereare data on very few patients who have high-gradetumors. Also, there is scant information on pelviclymph node status in patients receiving externalbeam radiotherapy or followed with surveillance,leaving open the possibility of dramatic differencesin the stages of patients’ tumors.
Because of the significant differences amongtreatment series and the consequent inability tomake meaningful estimates from data available forthe treatment outcomes of patient survival and tu-mor progression, the panel concluded that it wouldbe methodologically unsound to compare treatmentmodalities directly with regard to these outcomes.Nevertheless, the panel did decide to present dataresults in the form of summary outcomes tables 3–4 (pages 25-26), as well as graphically in Figures 1–13 (pages 28-31), to show the range of outcomesdata reported for the different modalities. Theranges of frequency reported for the 25 most com-mon treatment complications are shown in Table 5(page 27). Frequency rates for the most importantof these complications are depicted graphically aswell in Figures 14–16 (page 31).
The panel generated its practice policy recom-mendations based on the outcome estimates avail-able and on panel opinion. The recommendationswere graded according to levels of flexibility basedon the strength of the evidence and the panel’s as-sessment of patient needs and preferences. Threelevels—standards, guidelines and options—are de-fined on page 8. A standard has the least flexibility.A guideline has significantly more flexibility, and
Treatment recommendations
(Continues on page 6)
Archived Document— For Reference Only
Page 4 Executive Summary Copyright © 1995, American Urological Association, Inc.
Recommendations: Standards
• As a standard, an assessment of the patient’s life expectancy, overallhealth status and tumor characteristics is necessary before any treatment deci-sions can be made.
Life expectancy:Life expectancy, rather than patient age, should be the fac-tor considered in treatment selection. Therefore, the panel did not set a specificchronological cutoff point. When a man’s life expectancy is relatively long,prostate cancer can be a cause of morbidity and mortality. On the other hand,at an advanced patient age, or when life expectancy is relatively short, compet-ing hazards for mortality reduce the chance that a man will suffer from diseaseprogression or die from prostate cancer. (See U.S. Life Expectancy Table inAppendix C.)
Health status:The patient’s overall health status is the sum of all condi-tions and includes both patient and family history as well as the present stateof the patient’s well-being and the degree of any coexistent disease. There aretwo reasons to evaluate the overall health status prior to deciding on an inter-vention: (1) Overall health status influences life expectancy; (2) overall healthstatus may affect patient response to adverse events resulting from particularinterventions.
Tumor characteristics: The histologic grade and stage of the tumor shouldbe considered when assessing the potential natural history and treatment op-tions for prostate cancer. Small, well-differentiated cancers progress moreslowly and are less likely to be life threatening than large, poorly differentiatedtumors which have a greater potential to be biologically aggressive and clini-cally significant.
• As a standard, a patient with clinically localized prostate cancer should beinformed about the commonly accepted initial interventions including, at aminimum, radical prostatectomy, radiotherapy and surveillance. A discussionof the estimates for benefits and harms of each intervention should be offeredto the patient.
The panel defines radical prostatectomy to include complete removal of theprostate, vasal ampullae and seminal vesicles. The panel defines radiotherapyto include external beam and/or interstitial (brachytherapy) treatments.Surveillance is defined as periodic monitoring of the patient’s prostate cancerand its effects.
The patient should be informed that depending on his condition and initialchoice, subsequent interventions may be appropriate.
• As a standard, the patient’s preference, based on his attitude toward thecourse of the disease and the benefits and harms of the different interventions,should be considered in determining his treatment.
Archived Document— For Reference Only
Page 5 Executive SummaryCopyright © 1995, American Urological Association, Inc.
Recommendations: Treatment options
Options for management of localized prostate cancer include radicalprostatectomy, radiotherapy and surveillance. Radiotherapy includes ex-ternal beam and interstitial (brachytherapy) treatments. The panel consid-ers these interventions to be options because data from the literature donot provide clear-cut evidence for the superiority of any one treatment.Provided for each option, however, are a description of the patient mostlikely to benefit from the intervention and a brief summary of the inter-vention’s advantages and disadvantages.
• Radical prostatectomy:Based on the panel’s interpretation of theliterature and panel opinion, the patient most likely to benefit from radi-cal prostatectomy would have a relatively long life expectancy, no signifi-cant surgical risk factors and a preference to undergo surgery.
The major advantage of radical prostatectomy is its potential for totalremoval of the cancer and “cure” in properly selected patients. “Cure” isdefined as lifetime freedom from disease. Potential harms include urinaryincontinence and erectile dysfunction. Because the cancer may not becompletely eradicated, disease progression may occur.
• Radiotherapy: Based on the panel’s interpretation of the literatureand panel opinion, the patient most likely to benefit from radiotherapywould have a relatively long life expectancy, no significant risk factorsfor radiation toxicity and a preference for radiotherapy.
The advantages of radiotherapy are that it has a potential for cure andthat it is well tolerated in the majority of men when modern techniquesare used. Its principal potential harms include radiation cystitis and proc-titis and erectile dysfunction. Because the prostate remains in place, per-sistence and progression of the disease may occur.
• Surveillance:Based on the panel’s interpretation of the literatureand panel opinion, patients most likely to benefit from surveillance arethose with a shorter life expectancy and/or a low-grade tumor.
Benefits of surveillance for low- or intermediate-grade, localized pros-tate cancer include a lack of treatment-related morbidity with only mar-ginal compromise of disease-specific survival at 5 to 10 years of follow-up. Because the prostate is neither removed nor irradiated, progression ofthe disease is more likely to occur.
Archived Document— For Reference Only
Page 6 Executive Summary Copyright © 1995, American Urological Association, Inc.
an option is the most flexible. None of the panel’srecommendations, however, fits the guideline cate-gory defined on page 8.
The standard patientThe panel’s recommendations apply to the stan-
dard patient, defined as a man who has clinically lo-calized prostate cancer (adenocarcinoma of theprostate). For this report, the panel focused on clini-cal stage T2 (B) disease. Based on the opinion ofthe panel, recommendations may also be applied topatients diagnosed with stage cT1c disease (detect-ed by elevated PSA). The recommendations werenot developed for patients with stage T1a/b (A1/A2)or clinical T3-T4 (C) disease. For a detailed discus-sion of prostate cancer staging, see pages 13-15.
Limitations in the literatureThe medical literature for stage T2 prostate can-
cer is, overall, clearly deficient in usable data onwhich to base comparable estimates for outcomesof treatments and to make practice policy recom-mendations. The deficiencies are such that the Pros-tate Cancer Clinical Guidelines Panel was unable todevelop, based on evidence from the literature,treatment-comparable outcome estimates for themost important outcomes: patient survival and tum-or progression at 5, 10 and 15 years. Major limita-tions can be summarized as follows:
• Few randomized controlled trials:Most ofthe data come from case series not subjected to therigors of a carefully performed, prospective, central-ly controlled clinical trial. Indeed, most of the stud-ies the panel reviewed in its literature search wereclinical series based on “convenience samples,” pa-tients available in the clinical setting where the re-search was done. The majority of the other limita-tions summarized on this page stem from the pau-city of randomized controlled trials.
• Insufficient data: Many articles do not reportall outcomes (such as cancer-specific, metastasis-free and tumor-free survival). Also, there are fewdata on high-grade tumors in patients managed bysurveillance, or on pelvic lymph node status in pa-tients managed by external beam radiotherapy aswell as surveillance. In another very important ex-ample, many articles do not specify ages of patients
despite the effect of age on survival and the signifi-cant differences in average patient age for differenttreatment modalities. In still another example, manyarticles reporting complications from treatment donot report “zero complications.” For instance, an ar-ticle may not refer to incontinence in its list of treat-ment-related complications. Readers are left towonder whether the complication did not occur or ifit was omitted from the report.
• Data variability: Examples of variabilityabound in the literature. For instance, staging meth-odology often varies between studies, not only withregard to clinical staging versus surgical staging,but with regard to differences in types of lymphnode dissections (not all of which are comparable).Patient populations differ greatly in the literature, asdo such important factors as means and length offollow-up.
• Publication bias:Because not all physicianspublish, case-study results may not be generallyrepresentative. Moreover, studies with negative orequivocal results are less likely to be submitted forpublication and less likely to be published if sub-mitted.
Recommendations for futureresearch
Most research needs can be grouped in three cat-egories: (1) new and better methods to diagnose andmanage localized prostate cancer; (2) prospective,randomized, controlled studies of the issues con-cerning prostate cancer, especially controlled stud-ies of competing treatments for the management oflocalized prostate cancer; and (3) studies of howprostate cancer and its treatments affect patientquality of life.
❶ In the first category,needs for new methodsof cancer diagnosis and monitoringinclude theneed for a more sensitive, more specific tumor indi-cator. As clinically useful as serum PSA values havebecome, they lack important properties such asprostate-cancer specificity.
Needed also are biochemical, radiographic and/orgenetic methods to assist in staging and to deter-mine reliably which cancers are biologically aggres-sive and which are clinically insignificant. For de-tecting potentially life-threatening cancers whilestill localized, it would be useful to have a geneticmarker that can identify men likely to develop sucha tumor in their lifetimes.
❷ In the second category,randomized, prospec-tive, controlled studiesof competing treatments formanaging localized prostate cancer are clearly a
Literature limitations andrecommendations for research
Archived Document— For Reference Only
Page 7 Executive SummaryCopyright © 1995, American Urological Association, Inc.
pressing need, especially comparative studies inves-tigating surveillance vis-à-vis active treatments.
Properly designed efficacy studies of treatmentmodalities will provide reliable descriptive data forthe patients studied. The descriptive factors shouldinclude age, tumor stage, tumor grade, ploidy, PSA,performance status and comorbidity, as well as costfactors and validated measures of quality of lifeover the course of a trial.
End points measured in a trial should includerisk of local recurrence, risk of disease progression(including objective measures of symptoms associ-ated with progression), risk of metastatic diseaseand risk of prostate cancer death.
Following are additional suggested study topicsand issues for each of the three major modalities:
• Radical prostatectomy:Methods of improv-ing preoperative staging, reducing the numberof patients with extraprostatic disease and re-ducing treatment complications; strategies toreduce the cost of the procedure; better waysto disseminate advances in surgical techniqueto the urologic community; treatments for pa-tients with pathologically proven (pT3) ex-traprostatic disease; and treatments for patientswith evidence of serologic (PSA) failure.
• Radiotherapy: Ways to reduce treatment mor-bidity; ways to standardize treatment; the roleof three-dimensional conformal therapy and ofradiosensitizers; strategies to reduce the costof treatment; optimal treatment at progression;mature data on long-term follow-up of existingradiotherapy patients; stage-specific complica-tions data on existing series; and PSA andbiopsy data.
• Surveillance:Optimal schedule of follow-upand optimal interventions at evidence of pro-gression.
Among the other topics and issues that need tobe addressed in rigorously designed clinical trialsare:
• New technologies for the treatment of clinical-ly localized prostate cancer;
• Trade-offs between survival and quality oflife—including analysis of methods by whichpatients make treatment choices and the roleplayed by quality-of-life factors in thosechoices;
• Opportunities for chemoprevention of prostatecancer including dietary interventions, hor-monal therapy and retinoid therapy;
• New strategies for the use of hormonal treat-ments;
• Combined therapies for prostate cancer;• Development and validation of surrogate mea-
sures of long-term prostate cancer outcomes(e.g.,validation of PSA failure as a surrogatefor cancer survival).
❸ Finally, the third category of research needsconsists of research into how prostate cancer andits treatments affect patient quality of life. Suchresearch would include the second topic in theabove list: analysis of trade-offs between survivaland quality of life and of the role played by quality-of-life factors in patients’ treatment choices.Needed as well are improved methods for involvingthe patient in a meaningful and efficient decision-making process and for providing unbiased infor-mation to patients and physicians about emergingprocesses and outcomes of care.
Archived Document— For Reference Only
Page 8 Copyright © 1995 American Urological Association, Inc.
The AUA Prostate Cancer Clinical GuidelinesPanel developed the recommendations in thisReport on the Management of Clinically LocalizedProstate Cancerfollowing an explicit approach todevelopment of practice policies (Eddy, 1992). Theexplicit approach attempts to arrive at recommenda-tions through mechanisms that take into account therelevant factors for making selections from alterna-tive interventions. Such factors include estimationof outcomes from the interventions, considerationof patient preferences regarding those outcomes(including costs engendered by the interventions)and assessing when possible the relative priority ofthe interventions for a share of limited health careresources. Emphasized is the use of scientific evi-dence in estimating the outcomes of interventions.When panel opinion is necessary, the explicit ap-proach calls for an explanation of why it is neces-sary and discussion of the factors considered.
To develop recommendations for this report, thepanel made an extensive effort to review the litera-ture on stage T2 (B) prostate cancer from 1966-1993 and to estimate outcomes from the alternativetreatment modalities as accurately as possible.Unfortunately, the paucity of randomized, con-trolled trials and lack of comparability among treat-ment series regarding the most important outcomes,survival and disease progression, made method-ologically sound estimations impossible for com-paring alternative treatment modalities.
The review of the evidence began with a litera-ture search and extraction of data as described onpage 9. The data available in the literature were dis-played in evidence tables. From these tables, thepanel attempted to develop estimates of outcomesfor major treatment alternatives (radical prostatec-tomy, radiotherapy and surveillance). In Chapter 3,outcomes are analyzed in detail.
The panel generated its practice policy recom-mendations based on the outcome estimates avail-able and on expert opinion. The recommendationswere graded according to three levels of flexibilitybased on the strength of the evidence and the pan-el’s assessment of patient needs and preferences.
Levels of flexibility are defined as follows (Eddy,1992; American Academy of Family Physicians,1995):
• Standard: A policy is considered a standardif the health and economic outcomes of the al-ternative interventions are sufficiently well-known to permit meaningful decisions andthere is virtual unanimity about which inter-vention is preferred.
• Guideline: A policy is considered a guidelineif the health and economic outcomes of the in-terventions are sufficiently well-known to per-mit meaningful decisions and an appreciablebut not unanimous majority agree on which in-tervention is preferred.
• Option: A policy is considered an option if(1) the health and economic outcomes of theinterventions are not sufficiently well-knownto permit meaningful decisions, (2) prefer-ences among the outcomes are not known, (3)patients’ preferences are divided among alter-native interventions and/or (4) patients are in-different about the alternative interventions.
Standards obviously have the least flexibility.Guidelines have considerably more flexibility, andoptions are the most flexible. In this report, theterms are used to indicate the strength of the rec-ommendations. A recommendation was labeled astandard if the panel concluded that it should befollowed by virtually all health care providers forvirtually all patients. A recommendation would belabeled a guideline if the panel thought it appropri-ate not for all, but for a significant majority of pa-tients. None of the recommendations in this report,however, fits the guideline category.
Recommendations in this report regarding treat-ment choices were labeled options mostly becauseof the inability to estimate outcomes meaningfullyfrom the evidence available. Because the evidencedoes not permit direct comparison of the most im-portant outcomes among alternative treatmentmodalities, the comparative recommendations forthese modalities are presented as treatment optionsrather than as guidelines or standards (page 38).
Another reason for labeling a recommenda-tion an option is that patient preferences may be
Methods and definitions
Chapter 1: Methodology
Archived Document— For Reference Only
Page 9Copyright © 1995 American Urological Association, Inc.
unknown or divided because of complications fromthe treatment, in which case it is particularly impor-tant to consider preferences of individual patients inselecting from among alternative interventions.
To extract scientific evidence about the outcomesfrom alternative interventions for treating stage T2(B) prostate cancer, the panel performed a literaturesearch utilizing the MEDLINE database. The data-base was searched several times up to December1993, using the MESH subject heading “prostaticneoplasms.” All citations recovered were importedinto a bibliographic database software system(Papyrus Bibliography System; Research SoftwareDesign, Portland, Oregon).
Members of the panel reviewed abstracts for12,501 articles on prostate cancer published from1966 to 1993. Each abstract was independently re-viewed by two panel members. If either memberthought the article appeared relevant, it was re-trieved. On the basis of abstract review, 1,453 arti-cles were retrieved. After a summary review ofthese articles, the panel found 926 of the 1,453 arti-cles (64 percent) acceptable for detailed review. Ofthe 926 articles, 396 were found relevant to stageT2 (B) prostate cancer and were accepted for ex-traction of outcomes data.
Figure A-1 in Appendix A of this report showsgraphically, by year, the number of articles the pan-el retrieved on the basis of abstract review. Evidentin this graph is the dramatic increase over time inthe number of papers published. Figure A-2 showssources of articles from the English-language litera-ture. Also see Appendix A for the bibliography inTable A-1 of sources of articles from which out-comes data were extracted. (Articles cited in thetext of this report, for referencing particular pointsdiscussed, were not necessarily among articles thepanel reviewed to extract outcomes data.)
A comprehensive data-extraction form was de-vised by the panel and staff to capture as much per-tinent information as possible from each article. Asample of the form is in Appendix B. The selectedarticles were divided among the panel members,who extracted the data to complete the form.
During the finely detailed data-extraction pro-cess, 231 of the 396 stage T2 articles were rejectedfor the following reasons: 6 percent because infor-mation on patients could not be separated accordingto treatment used; 8 percent because of updated da-ta available in a later paper; 12 percent because in-formation on patients’ cancers could not be separat-ed according to stage; 16 percent because of absentdata; 27 percent because of irrelevant data; and 31percent for other, miscellaneous reasons. The netresult was 165 articles with stage T2 outcomes dataextracted (see Appendix A, Figures A-5 and A-6).
Each of the 165 articles was reviewed and thedata extracted separately by two panel members,who then met to resolve any differences. Their re-sult was entered into a database software system(PARADOX) by staff, who also verified all data en-tries. The data were entered by series. Series in thisreport are groups of patients stratified by parame-ters such as primary treatment modality.
Subsequent to data extraction, the panel attempt-ed to follow a process in which the extracted datawould be combined by meta-analysis to yield out-come estimates for alternative treatment modalities.The meta-analytically derived estimates would thenbe arrayed in an outcomes table to compare themodalities.
Meta-analysis is a term that has been used in avariety of contexts in the medical literature. In itsmost general definition, meta-analysis is any pro-cess of utilizing the results of multiple studies todetermine a final estimate for a given parameter.For this report, the definition was restricted to in-clude only formal mathematical methods of com-bining the results of multiple studies. Various meth-ods can be used. The techniques employed dependupon the nature of the studies to be combined, thedegree to which the studies are similar and thetypes of data available. In its most restrictive defini-tion, meta-analysis includes only the classical (non-Bayesian) techniques used to combine randomizedcontrolled trials.
As noted previously (page 8), after examining atlength the data on management of localized prostatecancer, the panel had to conclude that these data donot provide sufficient evidence to allow valid com-parisons of treatments. Therefore, meta-analyticcombination by any method is inappropriate.
A major reason is that the data are from clinicalseries, and data from clinical series are frequently
Data inadequacy
Data extraction
Literature search
Archived Document— For Reference Only
Page 10 Copyright © 1995 American Urological Association, Inc.
not comparable. Pooling such data can lead tolarge, uncharacterizable biases. In the case of pros-tate cancer, the differences between series are espe-cially significant. For example, it is known that pa-tients who are older are more likely to be found inseries on treatment by surveillance or radiation.Many studies, however, do not specify ages of thepatients. In another example, patients in nonran-domized studies will likely have different grades ofdisease. Yet, grade data are frequently not available.In still another example, stage data are sometimesbased on clinical staging and sometimes on surgicalstaging. For patients not undergoing surgery, clini-cal staging is generally used, whereas authors ofsurgical series frequently reclassify patients basedon surgical stage. This implies that nonsurgical se-ries may include more higher-stage patients.
Particularly problematic are survival and disease-recurrence data (including overall survival, disease-specific survival, recurrence-free survival and timeto recurrence). The problems include differences inreporting of follow-up, differences in methods ofreporting survival and biases in losses to follow-up.
Having determined that combining the outcomesdata from different series is inappropriate, the paneldebated several methods for displaying the data.These methods included crude combinations in anoutcomes table, graphs with outcomes and sizes ofeach study shown or simply graphs with the out-comes from each study. All of these methods havethe disadvantage that the reader might infer differ-ences for alternative treatments that cannot be justi-fied.
The panel chose the simplest forms of display(pages 25-26, 28-31). In the graphical displays, thecircles indicate the rate reported by each series foroverall survival, progression-free survival, metasta-sis-free survival or disease-specific survival. Thedata are also shown in tabular form with the mini-mum and maximum percentages reported but nomean or median estimates. The tables indicatewhether reported results are based upon actuarialcalculations (life tables or Kaplan-Meier) or wheth-er they are “actual” (observed, nonactuarial), thatis, representing a ratio of an actual number of sur-vivors over a denominator that may have some re-duction for dropouts. As noted on page 23, becausemany patients are lost to follow-up, die of unknowncauses or fail to have consistent testing or to have
the data recorded, “actual” rates might not accurate-ly represent the impact of the disease or its treat-ment in the general population. For this reason, theword “actual” when used to denote such data ap-pears in quotes.
The problems that exist with regard to data forsurvival and disease progression also exist with re-gard to data for complications of treatment. Thelack of randomized trials and differences in patientpopulations and treatment techniques frequently re-sult in data not generalizable across studies. Dif-ferences in reporting data add to the problems. Forexample, many investigators do not list all compli-cations in the results sections of their studies. Theymay list only the complications that occur. Uncom-mon complications like perioperative death are thusnot included in many studies. To use such studies ina meta-analysis combining results of multiple stud-ies, a zero rate must be assumed for complicationsnot reported. Otherwise, if data were combined on-ly from those studies where a complication occurs,the estimate of frequency of occurrence would beartificially high.
Because of the various problems with regard tothe complications data, the panel chose not to com-bine these data from the different studies in order toestimate frequency of occurrence for alternativetherapies. The panel elected instead to display thecomplications data using the same method as forsurvival and progression data. For each of the mostimportant complications, such as perioperativedeath, impotence (erectile dysfunction), rectal in-jury and incontinence, a graph indicates the report-ed frequency rates for that complication (see Fig-ures 14–16, page 31). The data are shown in tabu-lar form as well (page 27), with reported high andlow rates to indicate a range but with no mean ormedian estimates. In Chapter 3, tables and graphsare explained in detail.
The discussion sections in Chapter 2 provide pri-marily descriptive and explanatory informationabout the natural history of prostate cancer, theGleason grading system and systems and methods
Literature citations and panelopinions in discussion sections
Treatment complications data
Data display for survivaland disease progression
Archived Document— For Reference Only
Page 11Copyright © 1995 American Urological Association, Inc.
used for clinical staging. Also provided in Chap-ter 2 are individual overview discussions of thetreatment alternatives analyzed by the AUAProstate Cancer Clinical Guidelines Panel: radicalprostatectomy, external beam radiotherapy, brachy-therapy (interstitial radiotherapy) and surveillance.Advantages and disadvantages of each of thesetreatment options are discussed on pages 38-41 ofChapter 4, following the panel’s treatment recom-mendations.
Some of the studies cited in the discussion sec-tions in Chapters 2 and 4 are in addition to articlesreviewed by the panel for data extraction and analy-sis. Among the additional articles are papers pub-lished after December 1993. As noted on page 9,December 1993 was the cutoff date in the literaturesearch to obtain articles for the purpose of extract-ing outcomes data. However, the discussion sec-
tions also include information from more recentstudies published in 1994.
Although these discussion sections contain pri-marily descriptive and explanatory information,some sections also contain panel opinions based onevidence from studies cited in the text of the dis-cussion. In particular, the section in Chapter 2 onstaging methods (pages 13–15) contains panel opin-ions questioning the need to use methods such ascomputerized tomography (CT) scan and magneticresonance imaging (MRI) for patients with clinical-ly localized prostate cancer. Reasons for panelopinions are stated explicitly in this and other sec-tions, but it should be recognized that no attemptwas made to subject the evidence cited to a rigor-ous review process like that described on pages 9-10 of this chapter.
Archived Document— For Reference Only
Page 12 Copyright © 1995 American Urological Association, Inc.
Chapter 2: Prostate cancer and its management
Prostate cancer is the most commonly diagnosedvisceral neoplasm in men. The estimated 244,000new cases diagnosed in the United States in 1995represent 36 percent of cancers in men, comparedto 14 percent for lung cancer and 10.4 percent forcolorectal cancer, the next two most frequently di-agnosed cancers (Wingo, Tong and Bolden, 1995).The 40,400 deaths from prostate cancer anticipatedin 1995 represent 14 percent of all cancer deaths inmen, placing prostate cancer second only to lungcancer mortality (33 percent) and ahead of colorec-tal cancer mortality (9.4 percent).
Of the malignant conditions that arise primarilywithin the prostate gland, by far the most frequentlyoccurring type is adenocarcinoma. Because of therarity of other primary neoplasms within the gland,the terms “prostate cancer” and “carcinoma of theprostate” are generally understood to be synony-mous with “adenocarcinoma.”
Anatomically, four glandular prostatic regionsare recognized: (1) the transition zone, a bilobararea lying on each side of the distal two-thirds ofthe supramontanal prostatic urethra in the unen-larged state, but which can, following the develop-ment of benign prostatic hyperplasia, occupy asmuch as 95 percent of the entire gland volume; (2)the central zone, which occupies the major portionof the cephalad half of the prostate; (3) the periph-eral zone, which occupies most of the distal half ofthe gland and (4) the periurethral glands lining theurethra.
Approximately 75 percent of prostatic carcino-mas arise in the outer gland (a combination of thecentral and peripheral zones), and many of thesecancers are multifocal. The remaining 25 percentarise in the transition zone. The volume of thelargest area of involvement, if in the peripheral orcentral zones, correlates with overall tumor stage.The periurethral glands are rarely involved in ma-lignant change.
A nonglandular area, the fibromuscular stroma,lying on the anterior gland surface as well as com-prising the internal and external urethral sphincters,
is devoid of carcinomatous change as its compo-nents do not include glandular tissue.
Prostate cancer has a wide spectrum of growthrates. Many tumors pursue a relatively indolentcourse over a number of years. Others advance rap-idly by local extension and/or metastasis. Evalu-ation of the effect of active intervention must takeinto account the course the disease would follow ifit were allowed to proceed without interference.Active treatment of a prostatic cancer that is des-tined never to present a clinical problem to the pa-tient would not be expected to improve patient out-comes over treatment by surveillance alone. Pros-tate cancer aggressiveness, however, does tend toincrease with time (Adolfsson and Tribukait, 1990).Given sufficient time, small localized tumors can beexpected to become large, multifocal, nonlocalizedtumors (Whitmore, Warner and Thompson, 1991),with decreasing likelihood of cure. “Cure” is de-fined in this report as lifetime freedom from dis-ease.
Thus, because techniques for distinguishingrapidly growing from slow growing tumors are stillevolving, patient longevity becomes a major factorin determining treatment. Treatment of prostatecancer depends to a significant degree upon the pa-tient’s age, functional level and medical status.Because a younger, healthier patient may be ex-posed to a longer period of risk for disease progres-sion, metastases and death, consideration of inter-vention rather than management by surveillancemay be more compelling in this patient. Risks fordeath from untreated disease are presented in thisreport (pages 40-41), but long-term results arepoorly understood. Of concern is a recent articlesuggesting that even low-grade tumors may have ashigh as a 55 percent likelihood of resulting in can-cer death within 15 years of follow-up (Aus, Hugo-sson and Norlén, 1994). The older patient with ashorter period at risk may have a lesser chance ofprostate cancer death. The age at which the risk of
Natural history andgrade classification
Background
Archived Document— For Reference Only
Page 13Copyright © 1995 American Urological Association, Inc.
cancer death reaches an “acceptable” level, so thattreatment is unnecessary, is not known.
Histologic grade is currently one of the mostcommon methods for classifying tumor aggressionlevels, and the most common system currently inuse is the Gleason grading system based on archi-tectural criteria (Gleason, 1977). A primary gradefrom 1 to 5, with 5 being the most aggressive, is as-signed to the pattern occupying the greatest area ofthe specimen. A secondary grade is assigned to thepattern occupying the second largest area. Thesetwo grades are then added to get a Gleason score,which ranges from 2 to 10. It is generally agreedthat tumors with a Gleason score ≤ 6 have lower bi-ologic aggressiveness and those with a Gleasonscore ≥ 7 are biologically aggressive tumors.
Pathologists can have difficulty, however, distin-guishing grade 3 histologic patterns from grade 4histologic patterns for assigning primary or sec-ondary grades. The distinction is important. Studiesrelating component grades to spread of cancer haveshown that metastases almost never occur withgrade 3, but occur often with grades 4 and 5 (Mc-Neal, Villers, Redwine, et al., 1990). Consequently,whereas 3 + 3 = 6 is a favorable Gleason score, 4 +2 = 6 or 2 + 4 = 6 is not. Certainly not favorableare 4 + 3 = 7, 3 + 4 = 7, 5 + 2 = 7 and 2 + 5 = 7.The value of the Gleason system may thus depend,in some cases, on the pathologist’s proper catego-rization of grade 3. Still, the system is a vast im-provement over earlier, purely descriptive attemptsat classification.
Factors such as tumor grade and volume (stage),along with evaluation of nuclear chromatin contentand nuclear roundness, allow some prediction of atumor’s biologic potential. However, at the presenttime, such factors are not fully applicable to indi-vidual patients because of the many exceptions thatexist to these predictive indices.
The natural history of untreated prostate canceris discussed in detail on pages 18-19 of this chapterin the description of surveillance as a treatment al-ternative.
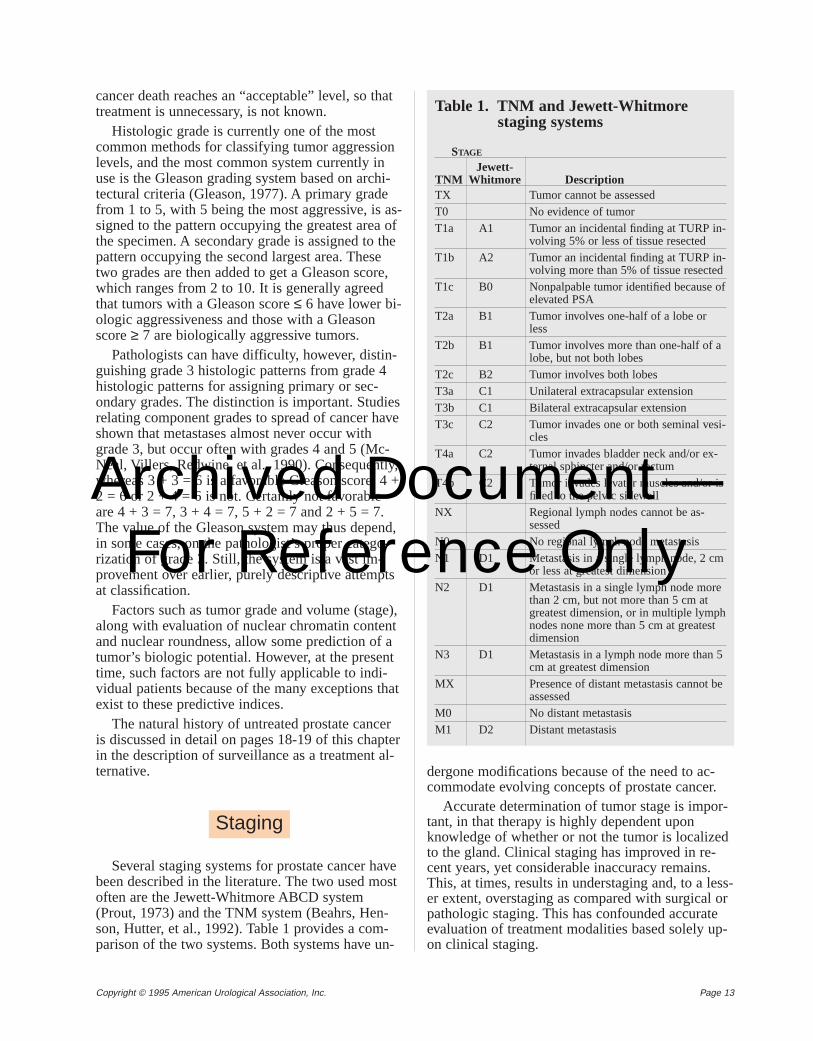
Several staging systems for prostate cancer havebeen described in the literature. The two used mostoften are the Jewett-Whitmore ABCD system(Prout, 1973) and the TNM system (Beahrs, Hen-son, Hutter, et al., 1992). Table 1 provides a com-parison of the two systems. Both systems have un-
dergone modifications because of the need to ac-commodate evolving concepts of prostate cancer.
Accurate determination of tumor stage is impor-tant, in that therapy is highly dependent uponknowledge of whether or not the tumor is localizedto the gland. Clinical staging has improved in re-cent years, yet considerable inaccuracy remains.This, at times, results in understaging and, to a less-er extent, overstaging as compared with surgical orpathologic staging. This has confounded accurateevaluation of treatment modalities based solely up-on clinical staging.
Staging
Table 1. TNM and Jewett-Whitmorestaging systems
STAGE
Jewett-TNM Whitmore DescriptionTX Tumor cannot be assessedT0 No evidence of tumorT1a A1 Tumor an incidental finding at TURP in-
volving 5% or less of tissue resectedT1b A2 Tumor an incidental finding at TURP in-
volving more than 5% of tissue resectedT1c B0 Nonpalpable tumor identified because of
elevated PSAT2a B1 Tumor involves one-half of a lobe or
lessT2b B1 Tumor involves more than one-half of a
lobe, but not both lobesT2c B2 Tumor involves both lobesT3a C1 Unilateral extracapsular extensionT3b C1 Bilateral extracapsular extensionT3c C2 Tumor invades one or both seminal vesi-
clesT4a C2 Tumor invades bladder neck and/or ex-
ternal sphincter and/or rectumT4b C2 Tumor invades levator muscles and/or is
fixed to the pelvic sidewallNX Regional lymph nodes cannot be as-
sessedN0 No regional lymph node metastasisN1 D1 Metastasis in a single lymph node, 2 cm
or less at greatest dimensionN2 D1 Metastasis in a single lymph node more
than 2 cm, but not more than 5 cm atgreatest dimension, or in multiple lymphnodes none more than 5 cm at greatestdimension
N3 D1 Metastasis in a lymph node more than 5cm at greatest dimension
MX Presence of distant metastasis cannot beassessed
M0 No distant metastasisM1 D2 Distant metastasis
Archived Document— For Reference Only
Page 14 Copyright © 1995 American Urological Association, Inc.
Methods used in clinical stagingof prostate cancer
Methods available for staging of clinically local-ized prostate cancer include digital rectal examina-tion (DRE), serum prostate specific antigen (PSA),serum acid phosphatase, transrectal ultrasonogra-phy (TRUS), computerized tomography (CT) scanand both body and endorectal magnetic resonanceimaging (MRI). For determination of distant metas-tases, staging methods include CT scan, MRI andradioisotopic bone scan. In the panel’s opinion,based on growing evidence from recent studies,many of the methods available do not necessarilyprovide useful information and may not be requiredfor patients with clinically localized prostate can-cer.
CT scan and MRI
Approximately 50 percent of patients with newlydiagnosed prostate cancer undergo a CT scanand/or MRI to assess locoregional spread (Stameyand McNeal, 1992). Yet, for most patients, thesestaging modalities provide little useful informationand may not be necessary. Capsular perforation,seminal vesicle invasion and pelvic lymph node in-volvement most often are microscopic phenomenaand, if so, cannot be diagnosed by either CT orMRI (Rifkin, Zerhouni, Gatsonis, et al., 1990).These tests can often detect gross extraprostatic dis-ease, but that degree of spread can usually be deter-mined from the serum PSA concentration, DRE orTRUS at time of biopsy. For these reasons, CT andMRI may not be required in the staging evaluationof patients with clinically localized prostate cancer.
Prostate cancer detected by PSA
Beginning in 1987, PSA has gradually achievedwidespread clinical use, initially as a tumor markerfor monitoring response to treatment, and more re-cently as an indicator of early, potentially curableprostate cancer (Brawer, Chetner, Beatie, et al.,1992; Catalona, Smith, Ratliff, et al., 1991; Cooner,Mosley, Rutherford, et al., 1990; Labrie, Dupont,Suburu, et al., 1992).
It is well established that serum PSA can identi-fy patients with prostate cancers not detectable byDRE, thus increasing the number of nonpalpableprostate cancers being diagnosed. As shown inTable 1 in the TNM staging system, “PSA-detect-ed” cancers are classified as stage T1c; in theJewett-Whitmore staging system, they are referredto as stage B0 (Stormont, Farrow, Myers, et al.,1993).
Studies indicate that most nonpalpable, PSA-de-tected prostate cancers are of sufficient volume toclassify them as clinically important (Brendler,Carmichael, Walsh, et al., 1993; Epstein, Walsh,Carmichael, et al., 1994; Oesterling, Suman,Zincke, et al., 1993; Scaletscky, Koch, Eckstein, etal., 1993). There is no evidence that PSA-detectedprostate cancers are different from small DRE-de-tected tumors.
Pelvic lymph node dissection
Pelvic lymph node dissection (PLND) has longbeen considered the gold standard in evaluation ofregional metastases from prostate cancer. AlthoughPLND can provide staging information obtainableby no other method, the procedure increases time insurgery and can increase patient morbidity. Poten-tial complications include hemorrhage, lymphocele,infection and vascular and neurologic injurieswhich occur in as many as 20 percent of those pa-tients undergoing PLND (Donohue, Mani, White-sel, et al., 1990; Kavoussi, Sosa, Chandhoke, et al.,1993).
Evidence is mounting that most patients who arecandidates for a radical prostatectomy or radiother-apy have very low risk for positive pelvic lymphnodes. One study found that patients with a primarytumor volume less than 4 cc (1.5-2.0 cm in diame-ter) do not have lymph node metastases (Stamey,McNeal, Freiha, et al., 1988). Another study notedthat only 6 of 274 patients (2 percent) with palpabledisease in one lobe (clinical stage T2a/T2b) hadpositive pelvic lymph nodes, in contrast to 23 per-cent of 84 patients with palpable disease in bothlobes (clinical stage T2c) (Walsh, 1988). The Stan-ford group found in patients with clinical stageT2a/T2b disease that no patients having sextantneedle biopsy specimens positive in only one lobehad positive lymph nodes, and only 8 percent of pa-tients having biopsy specimens positive in bothlobes had lymph node metastases (Daniels, McNealand Stamey, 1992). In two other large contempo-rary series of almost 600 patients, in which thecancers were detected using PSA screening, the in-cidence of positive pelvic lymph nodes was approx-imately 5 percent (Danella, deKernion, Smith, etal., 1993; Petros and Catalona, 1992).
In a study reviewing 1,632 patients with clinical-ly localized prostate cancer who had undergone bi-lateral pelvic lymphadenectomy at the Mayo Clinic,the overall incidence of positive pelvic lymphnodes was 12 percent (Bluestein, Bostwick, Berg-stralh, et al., 1994). Using logistic regression analy-sis, serum PSA was found to be the best predictorof pelvic lymph node metastases.
Archived Document— For Reference Only
Page 15Copyright © 1995 American Urological Association, Inc.
However, the predictive power of serum PSAcould be enhanced considerably by taking into ac-count the tumor grade and clinical stage. Using allthree clinical parameters together, a statistical mod-el was generated that allows the practicing urologistto accurately estimate the probability of pelviclymph node involvement. The model indicates thatwhen the serum PSA concentration, tumor gradeand local clinical stage are below certain levels, theprobability of positive lymph nodes is extremelylow. A pelvic lymph node dissection may not benecessary (Bluestein, Bostwick, Bergstralh, et al.,1994).
Radionuclide bone scan
The most sensitive method to detect bony metas-tases is radionuclide bone scan. Of late, evidencehas accumulated suggesting that bone scans may beeliminated for selected patients. Based on twolarge-scale clinical studies, Oesterling and col-leagues have determined that serum PSA concentra-tion can be used to reliably predict bone scan find-ings in patients with newly diagnosed prostate can-cer.
In the first clinical study, the investigators evalu-ated, retrospectively, 521 randomly selected pa-tients who presented with newly diagnosed, untreat-ed prostate cancer (Chybowski, Larson-Keller,Bergstralh, et al., 1991). All were evaluated with re-gard to local clinical stage as determined by DRE,biopsy tumor grade, serum acid phosphatase, pro-static acid phosphatase concentration, serum PSAand bone scan findings. Of all the clinical parame-ters available to predict the presence of skeletalmetastases, PSA was the best in predicting the re-sults of a radionuclide bone scan. For a serum PSAconcentration of 10 ng/ml or less, the probability ofskeletal metastases (positive bone scan) is extreme-ly low—less than 1.5 percent.
In order to confirm these initial findings, a sec-ond investigation was conducted to assess the abili-ty of serum PSA to predict bone scan findings(Oesterling, Martin, Bergstralh, et al., 1993).Medical records of 2,064 consecutive patients withprostate cancer were reviewed. Patients with priortreatment (androgen deprivation therapy, radicalprostatectomy or radiotherapy) were excluded. Aswith the previous study, irrespective of the tumorgrade and local clinical stage, the serum PSA valuewas the best predictor of the bone scan results.Combining tumor grade, local clinical stage or bothwith PSA did not enhance the predictive power ofPSA. This second investigation also confirmed theobservation that patients with a low serum PSA
concentration (less than 10 ng/ml) rarely haveskeletal metastases.
From the results of these two large clinical stud-ies, it appears that a staging radionuclide bone scanmay no longer be necessary for the patient withnewly diagnosed, untreated prostate cancer who hasno skeletal symptoms and a serum PSA concentra-tion of 10 ng/ml or less.
The evolution of therapeutic modalities for treat-ment of prostate cancer has been continuous overthe past several decades, making it difficult to as-sess the comparative value of each modality. Also,the treatment options for a particular patient aresubject to a number of constraints. First is an as-sessment of the patient’s life expectancy based up-on actuarial and comorbidity information, his func-tional status and his own wishes regarding therapy.Another important concern is whether the malig-nancy is believed to be confined within the gland orwhether it has spread either regionally or distantly.
The following treatment alternatives in currentuse for managing localized prostate cancer, eitheralone or in various combinations, were analyzed bythe AUA Prostate Cancer Clinical Guidelines Panel:radical prostatectomy, external beam radiotherapy,brachytherapy (interstitial radiotherapy) and sur-veillance (also known as expectant management,watchful waiting or observation).
Treatment methods that the panel considered in-vestigational are thermotherapy, cryotherapy, andro-gen deprivation and chemotherapy. A treatmentmethod was categorized as investigational if thepanel found the number of patients treated inade-quate for evaluation and/or if follow-up has beeninadequate to provide sufficiently precise outcomeestimates.
Treatment alternative: Radical(total) prostatectomy
Patient selection
Surgical removal of the prostate gland is “cura-tive” only if all the tumor is removed. “Cure” is de-fined as lifetime freedom from disease. Therefore,the appropriate patient for radical prostatectomyhas the disease clinically confined to the prostate,with no area of extension beyond the capsule or fix-ation of the gland and no evidence of regional or
Treatment alternatives
Archived Document— For Reference Only
Page 16 Copyright © 1995 American Urological Association, Inc.
distant disease. This would include selected patientswith clinical stage T1 or T2 biopsy-proven tumors.Evidence suggests that not all of these patients needto undergo a pelvic lymph node dissection or a ra-dionuclide bone scan before radical prostatectomy(see pages 14-15).
The appropriate patient also has these character-istics: (1) an expected longevity longer than the ex-pected morbidity of his cancer if left untreated; (2)no significant surgical risk factors; and (3) a will-ingness to undergo surgery following a discussionof risks, postoperative side effects, natural historyand options (Gibbons, 1993).
Life expectancy of the patient
Although relentless, the growth pattern of inter-mediate- and low-grade prostate cancers (Gleasonscore ≤ 6) is such that the cancer might not repre-sent a significant threat to the patient in his lifetime.An assessment of the patient’s overall health statusis therefore mandatory before any treatment recom-mendations can be made. This should include infor-mation regarding age and cause of death of parents,familial longevity and diseases (for example, hyper-tension, cardiovascular, metabolic), and past andcurrent health problems.
Patients with localized prostate cancer might becandidates for treatment by surveillance or delayedtherapy if they have a low-grade tumor and a lifeexpectancy of 10 years or less (Whitmore, 1993),whereas patients with a greater life expectancymight be considered candidates for radical prosta-tectomy.
Performance of radical prostatectomy
Radical prostatectomy is performed using eitherthe retropubic or perineal approach. Walsh and as-sociates have provided considerable insight into theperiprostatic anatomy over the last 10 years, whichhas reduced the complications associated with theretropubic procedure (Walsh, 1992). Techniques in-clude precise control of bleeding from the dorsalvein complex, to allow a more precise anatomicdissection of the apex, and identifying the branchesof the pelvic plexus that innervate the corpora cav-ernosa so that they can be preserved and sexualfunction can be maintained. These “nerve-sparing”techniques have subsequently been incorporated in-to the perineal procedure (Weldon and Tavel, 1988).
The goal of both the retropubic and perineal ap-proaches is to remove the entire prostate gland,both seminal vesicles, both ampullae of the vas andthe surrounding tissues including the bladder neck.
The bladder neck opening is then contoured as nec-essary to the size of the urethral stump where anend-to-end anastomosis is performed. The princi-ples of the operations are well established, withusual operating times of 2 to 4 hours. Hospitaliza-tions of 3 to 6 days are the rule, and the patient hasan indwelling catheter for 10 to 21 days.
Treatment alternative: Externalbeam radiotherapy
Technological improvements
Advances in radiation oncology over the last sev-eral years have substantially improved externalbeam radiotherapy for prostate cancer. Technologi-cal improvements allow the radiation beam to bemore precisely targeted to the prostate and seminalvesicles, sparing normal tissues to a greater degreefrom harmful effects of radiation. Computer tech-nology now permits accurate three-dimensional de-lineation not only of the prostate and seminal vesi-cles, but of the normal rectum, bladder and otherstructures (conformal therapy). This facilitates indi-vidually customized therapeutic blocks, sharply fo-cusing the radiation beam on the target volume.
Moreover, recent advances in clinicopathologicunderstanding of the likelihood of seminal vesicleextension, the location of the prostatic apex, the im-portance of day-to-day prostate motion and thetherapeutic efficacy of lymph node irradiation haveall contributed to improvements in external beamradiotherapy. The full effects of these advances in atherapeutic context will become clearer over thenext several years as data from long-term follow-upbecome available.
Patient selection
Patients selected for external beam radiotherapyshould have a relatively long life expectancy and nosignificant factors for radiation toxicity. For in-stance, bilateral femoral hip replacements can sig-nificantly interfere with the delivery of radiothera-py. In addition, patients with systemic lupus erythe-matosis, other unusual collagen vascular diseasesand inflammatory bowel diseases such as ulcerativecolitis are candidates for an alternative therapy.
Known pelvic nodal metastasis is a strong con-traindication to external beam radiotherapy. Stud-ies by both Memorial Sloan-Kettering (Fuks,Leibel, Wallner, et al., 1991) and the RadiationTherapy Oncology Group (Hanks, Krall, Pilepich,et al., 1992) reported that only about 10 percent ofpatients with node-positive disease at presentation
Archived Document— For Reference Only
Page 17Copyright © 1995 American Urological Association, Inc.
remain free of disease at 10 years, and there is noindication of a plateau in the disease-free survivalcurve. This indicates that node-positive patients,with perhaps rare exceptions, cannot be cured us-ing current radiotherapy techniques and may re-quire an alternative therapy.
Patients likely to benefit most and have the bestresults from external beam radiotherapy are gener-ally those who are also ideal candidates for radicalprostatectomy. Patients with T2a tumors will havemuch better long-term disease-free survival thanpatients with T2b or T2c tumors (Glick, Philput, El-Mahdi, et al., 1990; Kaplan, Prestidge, Bagshaw, etal., 1992; Kuban, El-Mahdi and Schellhammer,1989b; Schellhammer, Whitmore, Kuban, et al.,1989). Patients with well-differentiated tumors, nor-mal acid phosphatases and PSA values ≤ 10-15ng/ml have markedly improved outcomes comparedto patients with either higher-grade tumors or high-er PSA values at time of presentation. This hasbeen well documented (Asbell, Martz, Pilepich, etal., 1989; Duncan, Warde, Catton, et al, 1993; For-man, Zinreich, Lee, et al., 1985; Landmann andHunig, 1989; Perez, Garcia, Simpson, et al., 1989;Pisansky, Cha, Earle, et al., 1993; Russell, Dunatov,Hafermann, et al., 1991).
Target volume
Historically, pelvic lymph nodes were includedin the radiation treatment volume as they wereknown to be positive in a significant percentage ofpatients. Some reports showed improved survivalwhen the lymph nodes were treated, versus historiccontrols (Bagshaw, 1984; Epstein and Hanks, 1993;McGowan, 1981); and regional nodal radiotherapywas known to be effective in other types of cancers.
However, there are many who now doubt the im-portance or efficacy of regional pelvic radiotherapy.As noted previously, the most mature reports of pa-tients with involved lymph nodes clearly indicatethat, at 10 years, the overwhelming majority willhave developed metastatic disease (Fuks, Leibel,Wallner, et al., 1991; Hanks, Krall, Pilepich, et al.,1992). Moreover, there is no evidence of a plateauin the disease-free survival curves, suggesting thatradiation to involved pelvic nodes is incapable ofcuring a meaningful number of patients. Finally,prospective randomized trials have demonstrated noadvantage to pelvic nodal radiation when comparedwith the results of prostate radiotherapy alone(Asbell, Krall, Pilepich, et al., 1988; Asbell, Martz,Pilepich, et al., 1989; Pilepich, Krall, Johnson, etal., 1986).
Whether to include seminal vesicles in targetvolume is also uncertain. Depending upon the pre-cise characteristics of the stage T2 prostate cancer,the risk of seminal vesicle invasion can vary from 5to 40 percent (Marks and Anscher, 1992; Mukamel,deKernion, Hannah, et al., 1987; Oesterling, Brend-ler, Epstein, et al., 1987). Most patients with semi-nal vesicle invasion will have minimal involvement(less than 16 percent of the gland). Yet, even in themost favorable subsets of T2 disease, it is not rarefor seminal vesicles to be significantly infiltrated bytumor.
For the majority of patients with T2 tumors, theseminal vesicles can be included in the target vol-ume with minimal added morbidity. However, thevolume of irradiated rectum will definitely increase.Also, in occasional patients, the seminal vesiclesextend laterally and posteriorly for a significant dis-tance, with consequently greater risk of morbidity.It is reasonable in such cases to carefully weigh theincreased risk of morbidity against the benefits oftreating the seminal vesicles, especially if the tumoris classified in the most favorable substages of T2disease.
Treatment alternative: Brachytherapy(interstitial radiotherapy)
Patient selection
Patient selection criteria for brachytherapy aresimilar to those for external beam radiotherapy. Ingeneral, operative mortality is low, but complica-tions are not infrequent (see Table 5, page 27). Fortransperineal ultrasound-guided implantation ap-proaches, widely variable complications have beenreported (Blasko, Ragde and Grimm, 1991; Iversen,Bak, Juul, et al., 1989; Smalley and Noble, 1992).Although some reports show negligible complica-tions, longer follow-up and other corroborative se-ries are needed (Bertermann, et al., 1991; Blasko,Ragde and Grimm, 1991; Bosch, Forbes, Prassvin-ichai, et al., 1986; Carey, Lippert, Constable, et al.,1988; Fowler, Barzell, Hilaris, et al., 1979; Iversen,Bak, Juul, et al., 1989).
Prior transurethral resection of the prostate(TURP) is a relative contraindication to prostatebrachytherapy. Because patients with prior TURPhave a much higher incidence of late urinary com-plications (Blasko, Ragde and Grimm, 1991), ex-treme caution in minimizing urethral dose is impor-tant. Extensive corpora amylacea also present a the-oretical contraindication to implantation withlow-energy radionuclides (125I and 103Pd). The high
Archived Document— For Reference Only
Page 18 Copyright © 1995 American Urological Association, Inc.
electron density of the corpora amylacea may ab-sorb the radiation emitted from these low-energysources.
Finally, patients with high-grade tumors or withlarge tumor volume (expressed either as a volumet-ric estimate or as advanced clinical stage) are notwell suited for brachytherapy. No widely utilizedbrachytherapy techniques implant either the semi-nal vesicles or extracapsular tissue.
Techniques
Brachytherapy techniques involve two separatechoices: which type of radionuclide and whichmethod of administration. Isotopes can be chosenfrom a variety of radionuclides, taking into accountsuch factors as dosimetry scheme, half-life, type ofemission and tissue penetration. Brachytherapy mayalso be augmented by external beam radiotherapy,as well as by high-technology modifications thatare still investigational.
There are two methods of administration. In theearlier approach (1965 – 1985), the prostate was ex-posed retropubically. Then the radionuclide “seeds”were inserted by means of hand-positioning the car-rier needles, attempting to encompass the entireprostate mass by gross estimation. Several draw-backs to this method have been reported. One is in-ferior control of localized disease when comparedwith external beam radiotherapy (Kuban, El-Mahdiand Schellhammer, 1989a; Morton and Peschel,1988; Schellhammer, El-Mahdi, Higgins, et al.,1987; Schellhammer, Whitmore, Kuban, et al.,1989; Smalley and Noble, 1992).
Errors have also been documented in evaluatingprostate size, and thus in the numbering and spac-ing of seeds (Stone, Forman, Sogani, et al., 1988).Because distribution of seeds was difficult, the radi-ation dose was nonhomogeneous (Gore and Moss,1983; Kandzari, Belis, Kim, et al., 1982; Sogani,DeCosse, Montie, et al., 1979). Seeds migrated andwere usually passed out through the urethra (Som-merkamp, Rupprecht and Wannenmacher, 1988;Steinfeld, Donahue and Plaine, 1991). Finally,some authors have been concerned about the lowdoses delivered by 125I and 103Pd (Anderson andLing, 1991; Dale, 1985; Fowler, 1989, 1991; Small-ey and Noble, 1992). Data the panel extracted oncomplications of brachytherapy were based on thisearlier, retropubic approach.
The newer method of administering the radiation(1984-present) places the seeds much more precise-ly via the perineal percutaneous route. This ap-proach uses a perforated template on the perineumto position the carrying needles and transrectal ul-
trasound to monitor accurate distribution of theseeds. Anesthesia may be used, but no open surgeryis necessary. The transperineal method providesmore homogeneous delivery of the radiation dose tothe prostate, but some concern has been expressedabout adequately accessing the prostate base andseminal vesicles. More important, this method hasnot yet produced outcome results with long enoughfollow-up to be able to evaluate the potential advan-tages and risks. In the panel’s opinion, however,there is no evidence that results from the transperi-neal method are inferior to those from the retropu-bic method.
Treatment alternative: Surveillance
Basis for management by surveillance
The notion that no active treatment can be usedfor a disease process is not unusual. A classic ex-ample is the common cold. However, for such apolicy of “no active treatment” or “surveillance” tobe used for a neoplasm in which morbidity or mor-tality can occur, one or more of the following crite-ria must be met: (1) The neoplasm must have a lowrisk of morbidity and mortality; (2) The impact oftreatment upon morbidity or mortality must be neg-ligible, minimal or of unknown effect; and (3) Theharms of treatment must outweigh the benefits.
With regard to the first criterion, evidence sug-gests that low-grade, low-stage prostate canceruntreated may not produce any symptoms for pro-longed periods. Only in some patients will morbidi-ty or death from the disease ensue. Autopsies ofmen who died from other causes reveal a substan-tial number with occult prostate cancer. The rate isas high as 80 percent in older men (Franks, 1954).A study using assiduous sectioning techniques toinvestigate young men found carcinoma present in9 percent, 16 percent and 26 percent of men in theirthird, fourth and fifth decades, respectively (Sakr,Haas, Cassin, et al., 1993).
Of men with untreated prostate cancer followedup to 10 years, most series suggest that the majoritydo not die of prostate cancer but with it. Most ofthese series included older men at a higher risk ofdeath from other causes and men with less lethalforms of prostate cancer (well differentiated, lowstage). In one series (George, 1988), although 5 pa-tients died of prostate cancer, 48 died of other caus-es (4 percent versus 40 percent of the study popula-tion). In another series (Adolfsson, Carstensen andLowhagen, 1992), of the 38 percent of patients whodied, 7 percent died of prostate cancer and 31 per-cent of other causes.
Archived Document— For Reference Only
Page 19Copyright © 1995 American Urological Association, Inc.
In regard to the second criterion—that the impactof treatment on prostate cancer may be minor—three bodies of evidence support this contention.First, using contemporary measures of treatment ef-ficacy, many patients with clinically localized pros-tate cancer when treated for cure have been shownto be at risk for disease recurrence. In the case ofradical prostatectomy, a guiding principle holds thatif the tumor is confined to the prostate and the pros-tate is removed, likelihood of “cure” (lifetime free-dom from disease) is high. Unfortunately, the dis-ease may not, in fact, be organ confined. In theUnited States, as many as 50 percent of patients un-dergoing radical prostatectomy will be found tohave disease outside the prostate capsule or in theseminal vesicles or to have a positive surgical mar-gin (Morton, Steiner and Walsh, 1991; Wahle,Reznicek, Fallon, et al., 1990). These patients havea higher risk of disease recurrence than do patientswith organ-confined tumors (Paulson, Moul andWalther, 1990).
Some patients will be found to have a measur-able PSA following radical prostatectomy, indicat-ing persistent disease (Stein, deKernion, Smith, etal., 1992). Using PSA as an indicator of failure, pa-tients treated with radiotherapy have also been not-ed to have a high risk of relapse. One article re-ported that as many as 80 percent of patients treat-ed with radiotherapy have a rising PSA within arelatively short period of follow-up (Stamey, Ferrariand Schmid, 1993). Another article reported that ifPSA and clinical relapse are combined, the risk ofdisease relapse within 4 years following radiothera-py is 40 percent (Zagars and von Eschenbach,1993).
The second body of evidence indicates that apolicy of surveillance alone is often associated withprolonged, morbidity-free survivals. A number ofinvestigators have presented the results of a surveil-lance policy for localized prostate cancer (Adolfs-son and Carstensen, 1991; George, 1988; Johans-son, Adami, Andersson, et al., 1992; Jones, 1992;Madsen, Graversen, Gasser, et al., 1988; Rana,Chisholm, Christodoulou, et al., 1993; Stenzl andStuder, 1993; Waaler and Stenwig, 1993; Whit-more, Warner and Thompson, 1991). It must benoted that many of the patients were older and that,in many series, patients with focal disease detectedon transurethral resection of the prostate (TURP)were included (stage T1a). Nevertheless, it is in-structive to recognize that 10-year disease-specificsurvivals of between 40 and 92 percent were real-ized, with most studies in the 80 to 90 percentrange.
Finally, in a recent decision analysis, treatmentof localized prostate cancer for “cure” was calculat-ed to result in only minimal improvements in quali-ty-adjusted life expectancy (Fleming, Wasson, Al-bertsen, et al., 1993). The authors stratified patientsby age and tumor grade and made estimates oftreatment efficacy and risk of metastatic disease.Using the highest estimate of a positive effect oftreatment on life expectancy as well as the highestrisk of developing metastatic disease, the resultantincrease in quality-adjusted life expectancy was nomore than 4 years in the youngest patients studied.Using the median estimate for the risk of metastaticdisease and the highest efficacy of treatment, theauthors found that improvement of quality-adjustedlife expectancy was less than 1 year. With virtuallyall other estimates, treatment had a negative effecton quality-adjusted life expectancy.
Another study (Beck, Kattan and Miles, 1994),using more recent data from Chodak, Thisted, Ger-ber, et al. (1994), concluded that improvement inquality-adjusted life expectancy for radical prosta-tectomy compared with surveillance was 1.01, 2.41and 2.68 years for well-differentiated, moderatelywell-differentiated and poorly differentiated tumors,respectively.
The candidate for surveillance
There are two general principles in selecting theideal patient for surveillance: (1) a tumor of low bi-ologic activity (which poses the lowest threat ofmetastasis); and (2) a relatively short period of timeat risk for disease progression.
With regard to low biologic activity, tumor char-acteristics thought to be associated with the longestdisease-free survival include: low grade, low stage,low volume and (because it is often associated withtumor volume) low PSA.
As to short period at risk, because tumor pro-gression will occur in most patients with untreatedprostate cancer, given sufficient time, the ideal pa-tient for surveillance has a relatively short life ex-pectancy. Methods to estimate life expectancyinclude age (see U.S. Life Expectancy Table in Ap-pendix C), as well as information on other diseaseprocesses that the patient may have. These data canbe integrated to establish the period of time at riskfor disease progression and thereby determinewhether surveillance is an appropriate treatment op-tion.
Finally, a patient may choose surveillance formanagement of prostate cancer because of a desireto avoid or defer the side effects of other forms oftherapy.
Archived Document— For Reference Only
Page 20 Copyright © 1995 American Urological Association, Inc.
Surveillance in practice
Following the diagnosis of prostate cancer andappropriate staging to assure that metastatic diseaseis not present, treatment alternatives are discussedwith the patient. Surveillance is presented as one ofthese treatment options. If the patient elects a pro-gram of surveillance, he is informed that the statusof his prostate tumor will be monitored periodical-ly. Monitoring may take any number of forms, butwill generally include, as a minimum, DRE andPSA. The frequency of monitoring is often basedupon a number of factors including measures of thetumor’s biologic activity (stage, grade, volume,PSA) and the age and medical status of the patient.Patients may be informed that periodic monitoringshould also include a close relationship with their
physician, including an understanding that shouldsymptoms or signs develop which the patient feelsmay be related to the tumor, he should contact thephysician at that time.
One principle of surveillance as a managementmodality for localized prostate cancer is that otherforms of intervention may be employed at any time.For example, if evidence suggests that there is aneed for further treatment, then radical prostatec-tomy, radiotherapy or other forms of therapy maybe undertaken. (The patient is then no longer a“surveillance patient.”) However, the patient mustunderstand at the outset that the delay inherent insurveillance may compromise the effectiveness ofany subsequent treatment, if any should becomenecessary.
Archived Document— For Reference Only
Page 21Copyright © 1995 American Urological Association, Inc.
Outcomes of therapeutic medical interventionsmay be direct or indirect. Direct outcomes affectpatients’ lives directly and are experienced directly.Some direct outcomes, such as pain from treatment,occur immediately and are short-term. Others, suchas impotence (erectile dysfunction), may occur on acontinuing basis over a period of time. Still others,such as the effect of treatment on life expectancy,can be considered future outcomes. Patient prefer-ences may differ as to relative benefits/harms be-tween different types of direct outcomes, for exam-ple, the risk of erectile dysfunction compared withthe future benefit of longer life expectancy as a re-sult of the same treatment.
Indirect outcomes are measures, such as the levelof serum PSA, that are affected by treatment butnot experienced by patients directly. Such measuresmay provide data about the probability of futureoutcomes. For example, rising PSA can be of greatimportance when assessing the effectiveness of can-cer treatment and the probability of future progres-sion of the disease.
In treating prostate cancer, differences betweendirect and indirect outcomes are less important thanin treating many other diseases. The major consid-eration is where patients place the emphasis withregard to impact on their lives. Some patients areconcerned with adverse direct outcomes such asurinary incontinence or erectile dysfunction to thepoint that they may opt for a less morbid treatment,even if the probability of “cure” (lifetime freedomfrom disease) is notably less than for the rejectedtreatment (Singer, Tasch, Stocking, et al., 1991).
However, for many men with adenocarcinoma ofthe prostate, the most compelling reason for seek-ing treatment is the hope of “cure.” Given thechoice, these men may choose the risk of inconti-nence or erectile dysfunction for an improvedchance of “cure.” They are usually well informedand recognize the prognostic implications of indi-rect measures such as rising PSA.
For assessing benefits and harms of interventionfor stage T2 (B) prostate malignancy, the AUAProstate Cancer Clinical Guidelines Panel consid-ered the following outcomes the most important tothe patient: (1) survival at 5, 10 and 15 years(overall survival, disease-specific survival, progres-sion-free survival and metastasis-free survival); (2)progression rates at 5, 10 and 15 years(metastat-ic, local and biochemical); and (3) complicationsof treatment. Although all treatment complicationswere evaluated, the most important are: death fromtreatment, incontinence, impotence (erectile dys-function), cystitis, proctitis, major bleeding, pul-monary embolism, rectal injury and bladder neckcontracture/urethral stricture.
Survival at 5, 10 and 15 yearsClinically localized prostate cancer (stages T1
and T2) is rarely lethal within the first 5 years afterdiagnosis. The overall death rate during this periodis low and usually secondary to comorbid process-es. Almost any treatment for localized prostate can-cer would appear to have an excellent survival re-sult at 5 years. Survival at 10 years and 15 years al-lows a more accurate assessment of the influence ofprostate cancer and its treatment on patient sur-vival.
It is not sufficient to assess survival independent-ly of tumor progression status. Comorbid processesassociated with advanced age will often determineoverall survival. However, morbidity from cancerprogression may occur for years prior to death. It istherefore reasonable to inform patients not onlyabout the risk of dying from prostate cancer, but al-so about the risk of developing metastatic diseaseor evidence of tumor recurrence. Outcomes of dis-ease-specific, progression-free and metastasis-freesurvival should be assessed in addition to overallsurvival rates.
Progression rates at 5, 10 and15 years
After surgery or radiotherapy, most recurrence orprogression of adenocarcinoma of the prostate will
Types of outcomes
Chapter 3:Outcomes of treatments for localized prostate cancer
Archived Document— For Reference Only
Page 22 Copyright © 1995 American Urological Association, Inc.
become biochemically (PSA) apparent by 5 years,but a few patients may have lengthy delays beforethe progression becomes clinically apparent. Thus,it is important to continue to assess progressionrates to 10 years and beyond. Progression rates mayor may not influence the patient directly. Manytimes progression will be defined as the develop-ment of any evidence of tumor. This recurrence isoften asymptomatic and found only through sur-veillance examinations.
Obviously, either local recurrence or sympto-matic metastatic prostate cancer is of extreme im-portance to patients diagnosed with localized dis-ease. However, biochemical failures, usually in theform of rising serum PSA, will also negatively im-pact patients from a psychologic standpoint. Menwith prostate cancer understand that a rising serumPSA often precedes eventual symptomatic recur-rence.
Complications and harms oftreatment
Death from treatment is the most serious (thoughuncommon) immediate adverse outcome for a pa-tient diagnosed with prostate cancer. Other adverseoutcomes from treatment, such as incontinence, im-potence (erectile dysfunction), cystitis, rectal injuryand bleeding, are much more common and havevariable degrees of negative impact on patient well-being. The reported incidences and estimates ofthese adverse outcomes are important to a patientmaking decisions regarding treatment. Some of thecomplications are much less common today than inolder reports because of newer technology and ad-vancements in technique. It is therefore importantto stratify the complications relative to era of treat-ment. (See Appendix A, Figures A-7 to A-31.)
Cost, inconvenience and indirectquality-of-life issues
Although such issues as cost and inconvenienceare important, no meaningful data are readily avail-able from the literature. These are areas in need offuture research (see Chapter 5, page 45).
The panel was impressed by the massive amountof literature available on the topic of prostate can-cer. However, as discussed in Chapter 1 and in theLimitations section (page 42) of Chapter 5, the vast
bulk of the literature is not usable for extracting andcombining data to assess treatment outcomes anddevelop comparative estimates for these outcomes.
Of 12,501 papers reviewed, the panel was able toretrieve only 165 with acceptable data on outcomesfrom treatment of localized prostate cancer. (Seepage 9 for a discussion of the review process.)Moreover, in these 165 articles, there are significantdifferences among treatment series regarding suchcharacteristics as patient age, tumor grade andpelvic lymph node status. The differences are sum-marized in Table 2 (page 23).
Table 2 makes clear that patients receiving thevarious forms of treatment are not similar. For ex-ample, patients undergoing radical prostatectomyare on average 3 years younger than those undergo-ing external beam radiotherapy and approximately7 years younger than those reported to have beenfollowed with surveillance.
It is also striking that only about one in sevenpatients reported in the literature was followed evenfor 5 years and that a very small fraction was fol-lowed for 10 or 15 years. Estimates of importantoutcomes, particularly of survival and progressionrates at 5, 10 and 15 years, are likely to be inaccu-rate if such small numbers of patients are availablefor analysis.
Tumor grades are relatively comparable in pa-tients treated actively (by surgery or radiotherapy);but for patients followed with surveillance, thereare data on very few patients who have high-gradetumors. In addition, there is scant information onpelvic lymph node status in patients receiving ex-ternal beam radiotherapy or followed with surveil-lance, which leaves open the possibility of dramaticdifferences in the stages of patients’ tumors.
Because of the significant differences in the liter-ature among treatment series and the consequent in-ability to make meaningful estimates from availabledata for the most important outcomes, those of pa-tient survival and tumor progression, the panel con-cluded that it would be methodologically unsoundto compare treatment modalities directly with re-gard to survival and progression.
Nevertheless, in order to show the range of out-comes data reported for the different modalities, thepanel decided to display results of the data extract-ed. Results are displayed in summary outcomes
Summary outcomestables and graphs
Variability of outcomes data
Archived Document— For Reference Only
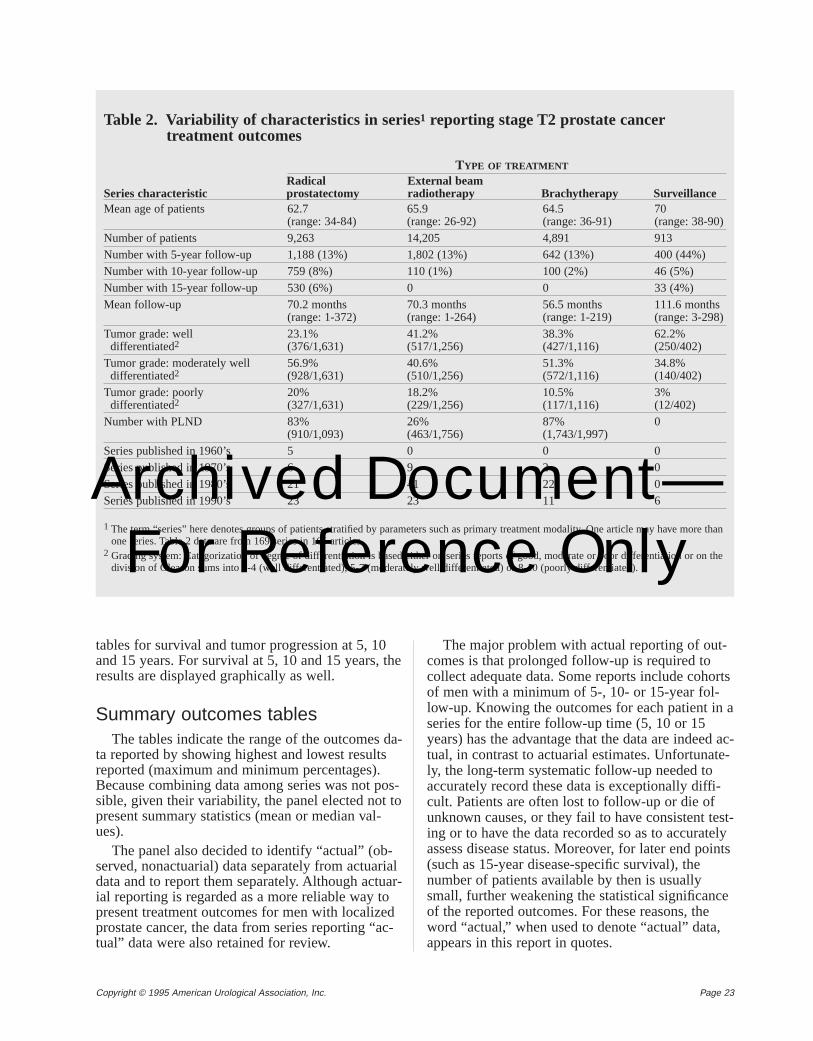
Page 23Copyright © 1995 American Urological Association, Inc.
tables for survival and tumor progression at 5, 10and 15 years. For survival at 5, 10 and 15 years, theresults are displayed graphically as well.
Summary outcomes tablesThe tables indicate the range of the outcomes da-
ta reported by showing highest and lowest resultsreported (maximum and minimum percentages).Because combining data among series was not pos-sible, given their variability, the panel elected not topresent summary statistics (mean or median val-ues).
The panel also decided to identify “actual” (ob-served, nonactuarial) data separately from actuarialdata and to report them separately. Although actuar-ial reporting is regarded as a more reliable way topresent treatment outcomes for men with localizedprostate cancer, the data from series reporting “ac-tual” data were also retained for review.
The major problem with actual reporting of out-comes is that prolonged follow-up is required tocollect adequate data. Some reports include cohortsof men with a minimum of 5-, 10- or 15-year fol-low-up. Knowing the outcomes for each patient in aseries for the entire follow-up time (5, 10 or 15years) has the advantage that the data are indeed ac-tual, in contrast to actuarial estimates. Unfortunate-ly, the long-term systematic follow-up needed toaccurately record these data is exceptionally diffi-cult. Patients are often lost to follow-up or die ofunknown causes, or they fail to have consistent test-ing or to have the data recorded so as to accuratelyassess disease status. Moreover, for later end points(such as 15-year disease-specific survival), thenumber of patients available by then is usuallysmall, further weakening the statistical significanceof the reported outcomes. For these reasons, theword “actual,” when used to denote “actual” data,appears in this report in quotes.
Table 2. Variability of characteristics in series1 reporting stage T2 prostate cancertreatment outcomes
TYPE OF TREATMENT
Radical External beamSeries characteristic prostatectomy radiotherapy Brachytherapy SurveillanceMean age of patients 62.7 65.9 64.5 70
(range: 34-84) (range: 26-92) (range: 36-91) (range: 38-90)Number of patients 9,263 14,205 4,891 913Number with 5-year follow-up 1,188 (13%) 1,802 (13%) 642 (13%) 400 (44%)Number with 10-year follow-up 759 (8%) 110 (1%) 100 (2%) 46 (5%)Number with 15-year follow-up 530 (6%) 0 0 33 (4%)Mean follow-up 70.2 months 70.3 months 56.5 months 111.6 months
(range: 1-372) (range: 1-264) (range: 1-219) (range: 3-298)Tumor grade: well 23.1% 41.2% 38.3% 62.2%differentiated2 (376/1,631) (517/1,256) (427/1,116) (250/402)
Tumor grade: moderately well 56.9% 40.6% 51.3% 34.8%differentiated2 (928/1,631) (510/1,256) (572/1,116) (140/402)
Tumor grade: poorly 20% 18.2% 10.5% 3%differentiated2 (327/1,631) (229/1,256) (117/1,116) (12/402)
Number with PLND 83% 26% 87% 0(910/1,093) (463/1,756) (1,743/1,997)
Series published in 1960’s 5 0 0 0Series published in 1970’s 6 9 2 0Series published in 1980’s 21 41 22 0Series published in 1990’s 23 23 11 6
1 The term “series” here denotes groups of patients stratified by parameters such as primary treatment modality. One article may have more thanone series. Table 2 data are from 169 series in 165 articles.
2 Grading system: Categorization of degree of differentiation is based either on series reports of good, moderate or poor differentiation or on thedivision of Gleason sums into 2-4 (well differentiated), 5-7 (moderately well differentiated) or 8-10 (poorly differentiated).
Archived Document— For Reference Only
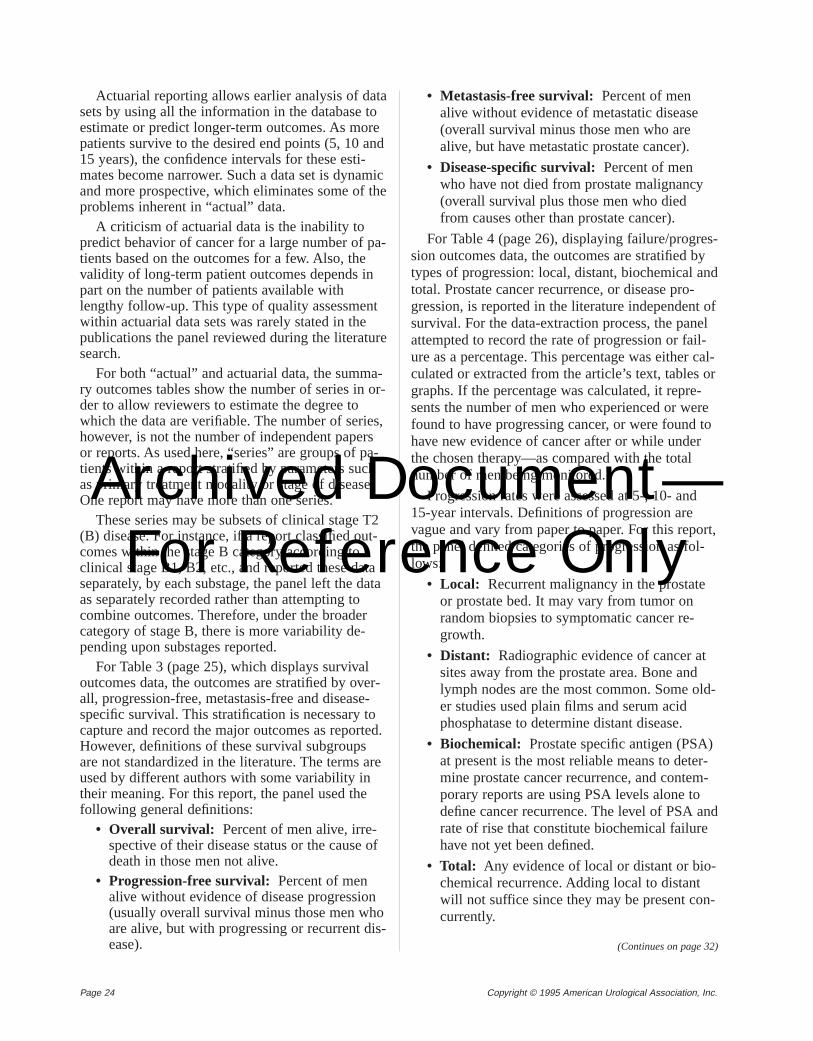
Page 24 Copyright © 1995 American Urological Association, Inc.
Actuarial reporting allows earlier analysis of datasets by using all the information in the database toestimate or predict longer-term outcomes. As morepatients survive to the desired end points (5, 10 and15 years), the confidence intervals for these esti-mates become narrower. Such a data set is dynamicand more prospective, which eliminates some of theproblems inherent in “actual” data.
A criticism of actuarial data is the inability topredict behavior of cancer for a large number of pa-tients based on the outcomes for a few. Also, thevalidity of long-term patient outcomes depends inpart on the number of patients available withlengthy follow-up. This type of quality assessmentwithin actuarial data sets was rarely stated in thepublications the panel reviewed during the literaturesearch.
For both “actual” and actuarial data, the summa-ry outcomes tables show the number of series in or-der to allow reviewers to estimate the degree towhich the data are verifiable. The number of series,however, is not the number of independent papersor reports. As used here, “series” are groups of pa-tients within a report stratified by parameters suchas primary treatment modality or stage of disease.One report may have more than one series.
These series may be subsets of clinical stage T2(B) disease. For instance, if a report classified out-comes within the stage B category according toclinical stage B1, B2, etc., and reported these dataseparately, by each substage, the panel left the dataas separately recorded rather than attempting tocombine outcomes. Therefore, under the broadercategory of stage B, there is more variability de-pending upon substages reported.
For Table 3 (page 25), which displays survivaloutcomes data, the outcomes are stratified by over-all, progression-free, metastasis-free and disease-specific survival. This stratification is necessary tocapture and record the major outcomes as reported.However, definitions of these survival subgroupsare not standardized in the literature. The terms areused by different authors with some variability intheir meaning. For this report, the panel used thefollowing general definitions:
• Overall survival: Percent of men alive, irre-spective of their disease status or the cause ofdeath in those men not alive.
• Progression-free survival: Percent of menalive without evidence of disease progression(usually overall survival minus those men whoare alive, but with progressing or recurrent dis-ease).
• Metastasis-free survival: Percent of menalive without evidence of metastatic disease(overall survival minus those men who arealive, but have metastatic prostate cancer).
• Disease-specific survival:Percent of menwho have not died from prostate malignancy(overall survival plus those men who diedfrom causes other than prostate cancer).
For Table 4 (page 26), displaying failure/progres-sion outcomes data, the outcomes are stratified bytypes of progression: local, distant, biochemical andtotal. Prostate cancer recurrence, or disease pro-gression, is reported in the literature independent ofsurvival. For the data-extraction process, the panelattempted to record the rate of progression or fail-ure as a percentage. This percentage was either cal-culated or extracted from the article’s text, tables orgraphs. If the percentage was calculated, it repre-sents the number of men who experienced or werefound to have progressing cancer, or were found tohave new evidence of cancer after or while underthe chosen therapy—as compared with the totalnumber of men being monitored.
Progression rates were assessed at 5-, 10- and15-year intervals. Definitions of progression arevague and vary from paper to paper. For this report,the panel defined categories of progression as fol-lows:
• Local: Recurrent malignancy in the prostateor prostate bed. It may vary from tumor onrandom biopsies to symptomatic cancer re-growth.
• Distant: Radiographic evidence of cancer atsites away from the prostate area. Bone andlymph nodes are the most common. Some old-er studies used plain films and serum acidphosphatase to determine distant disease.
• Biochemical: Prostate specific antigen (PSA)at present is the most reliable means to deter-mine prostate cancer recurrence, and contem-porary reports are using PSA levels alone todefine cancer recurrence. The level of PSA andrate of rise that constitute biochemical failurehave not yet been defined.
• Total: Any evidence of local or distant or bio-chemical recurrence. Adding local to distantwill not suffice since they may be present con-currently.
(Continues on page 32)
Archived Document— For Reference Only
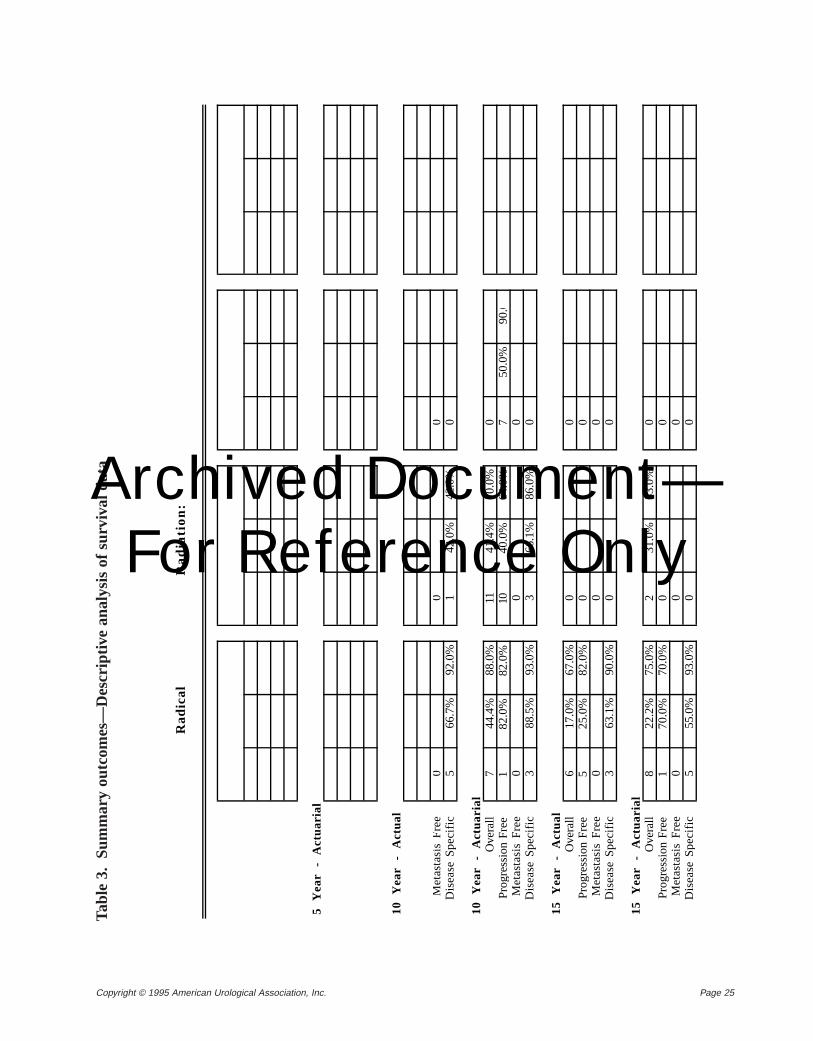
Page 25Copyright © 1995 American Urological Association, Inc.
R
ad
ica
lR
ad
iati
on
:
5
Ye
ar
- A
ctu
ari
al
10
Y
ea
r -
Act
ua
l
Me
tast
asi
s F
ree
00
0D
ise
ase
Sp
eci
fic5
66.7
%92
.0%
142
.0%
42.0
%0
10
Y
ea
r -
Act
ua
ria
lO
vera
ll7
44.4
%88
.0%
1141
.4%
70.0
%0
Pro
gres
sion
Fre
e1
82.0
%82
.0%
1040
.0%
64.0
%7
50.0
%90
.0M
eta
sta
sis
Fre
e0
00
Dis
ea
se S
pe
cific
388
.5%
93.0
%3
66.1
%86
.0%
0
15
Y
ea
r -
Act
ua
lO
vera
ll6
17.0
%67
.0%
00
Pro
gres
sion
Fre
e5
25.0
%82
.0%
00
Me
tast
asi
s F
ree
00
0D
ise
ase
Sp
eci
fic3
63.1
%90
.0%
00
15
Y
ea
r -
Act
ua
ria
lO
vera
ll8
22.2
%75
.0%
231
.0%
33.0
%0
Pro
gres
sion
Fre
e1
70.0
%70
.0%
00
Me
tast
asi
s F
ree
00
0D
ise
ase
Sp
eci
fic5
55.0
%93
.0%
00
Tabl
e 3.
S
umm
ary
outc
omes
—D
escr
iptiv
e an
alys
is o
f su
rviv
al d
ata
Archived Document— For Reference Only
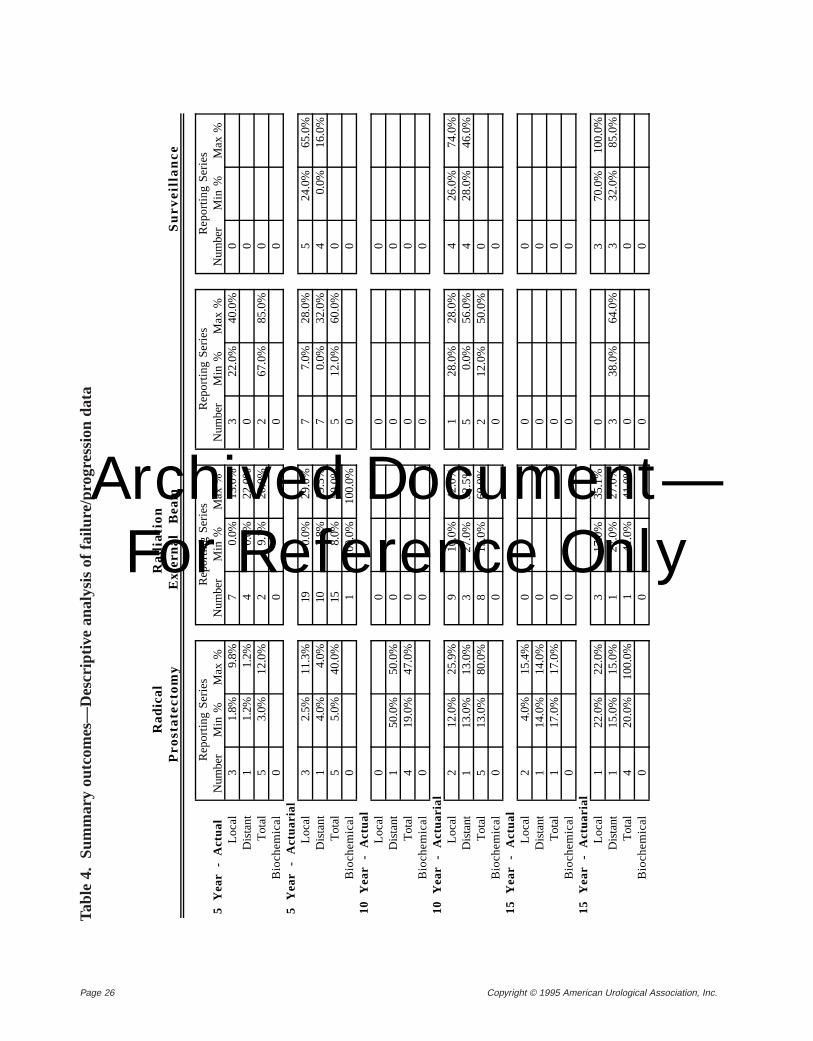
Page 26 Copyright © 1995 American Urological Association, Inc.
Tabl
e 4.
S
umm
ary
outc
omes
—D
escr
iptiv
e an
alys
is o
f fa
ilure
/pro
gres
sion
dat
a
R
ad
ica
lR
ad
iati
on
Pro
sta
tec
tom
yE
xte
rna
l B
ea
mS
urv
eil
lan
ce
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
5
Ye
ar
- A
ctu
al
Num
ber
Min
%M
ax
%N
umbe
rM
in %
Ma
x %
Num
ber
Min
%M
ax
%N
umbe
rM
in %
Ma
x %
Lo
cal
31.
8%9.
8%7
0.0%
13.0
%3
22.0
%40
.0%
0D
ista
nt1
1.2%
1.2%
40.
0%22
.0%
00
Tot
al5
3.0%
12.0
%2
9.1%
20.0
%2
67.0
%85
.0%
0B
ioch
em
ica
l0
00
05
Y
ea
r -
Act
ua
ria
lL
oca
l3
2.5%
11.3
%19
0.0%
29.0
%7
7.0%
28.0
%5
24.0
%65
.0%
Dis
tant
14.
0%4.
0%10
3.8%
19.5
%7
0.0%
32.0
%4
0.0%
16.0
%T
otal
55.
0%40
.0%
158.
0%50
.0%
512
.0%
60.0
%0
Bio
che
mic
al
01
100.
0%10
0.0%
00
10
Y
ea
r -
Act
ua
lL
oca
l0
00
0D
ista
nt1
50.0
%50
.0%
00
0T
otal
419
.0%
47.0
%0
00
Bio
che
mic
al
00
00
10
Y
ea
r -
Act
ua
ria
lL
oca
l2
12.0
%25
.9%
910
.0%
42.0
%1
28.0
%28
.0%
426
.0%
74.0
%D
ista
nt1
13.0
%13
.0%
327
.0%
32.5
%5
0.0%
56.0
%4
28.0
%46
.0%
Tot
al5
13.0
%80
.0%
815
.0%
60.0
%2
12.0
%50
.0%
0B
ioch
em
ica
l0
00
01
5
Ye
ar
- A
ctu
al
Lo
cal
24.
0%15
.4%
00
0D
ista
nt1
14.0
%14
.0%
00
0T
otal
117
.0%
17.0
%0
00
Bio
che
mic
al
00
00
15
Y
ea
r -
Act
ua
ria
lL
oca
l1
22.0
%22
.0%
317
.0%
35.1
%0
370
.0%
100.
0%D
ista
nt1
15.0
%15
.0%
127
.0%
27.0
%3
38.0
%64
.0%
332
.0%
85.0
%T
otal
420
.0%
100.
0%1
41.0
%41
.0%
00
Bio
che
mic
al
00
00
Archived Document— For Reference Only
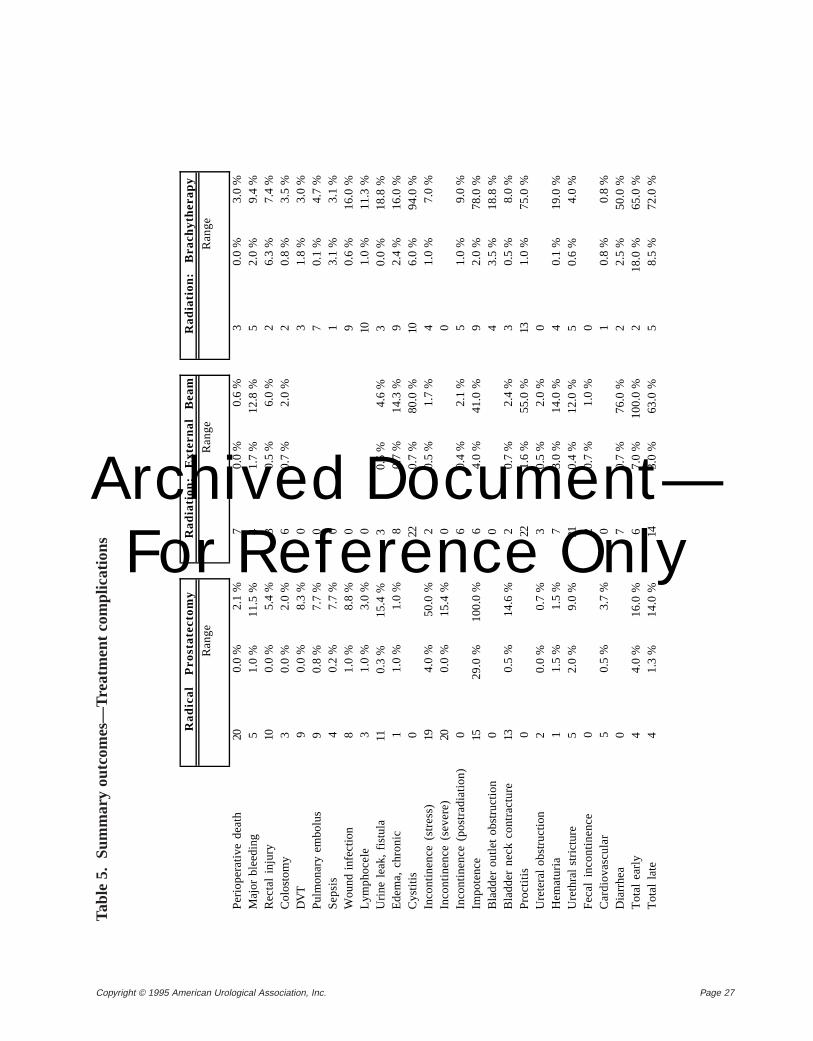
Page 27Copyright © 1995 American Urological Association, Inc.
Ra
dic
al
Pro
sta
tect
om
yR
ad
iati
on
: E
xte
rna
l B
ea
mR
ad
iati
on
: B
rach
yth
era
py
Ra
ng
eR
an
ge
Ra
ng
e
Pe
rio
pe
rativ
e d
ea
th20
0.0
%2.
1 %
70.
0 %
0.6
%3
0.0
%3.
0 %
Ma
jor
ble
ed
ing
51
.0 %
11
.5 %
41
.7 %
12
.8 %
52
.0 %
9.4
%R
ect
al
inju
ry10
0.0
%5.
4 %
30.
5 %
6.0
%2
6.3
%7.
4 %
Co
lost
om
y3
0.0
%2
.0 %
60
.7 %
2.0
%2
0.8
%3
.5 %
DV
T9
0.0
%8.
3 %
03
1.8
%3.
0 %
Pu
lmo
na
ry e
mb
olu
s9
0.8
%7
.7 %
07
0.1
%4
.7 %
Se
psi
s4
0.2
%7.
7 %
01
3.1
%3.
1 %
Wo
un
d i
nfe
ctio
n8
1.0
%8
.8 %
09
0.6
%1
6.0
%L
ymp
ho
cele
31.
0 %
3.0
%0
101.
0 %
11.3
%U
rin
e l
ea
k, f
istu
la11
0.3
%1
5.4
%3
0.5
%4
.6 %
30
.0 %
18
.8 %
Ed
em
a,
chro
nic
11.
0 %
1.0
%8
0.7
%14
.3 %
92.
4 %
16.0
%C
ystit
is0
220
.7 %
80
.0 %
106
.0 %
94
.0 %
Inco
ntin
en
ce (
stre
ss)
194.
0 %
50.0
%2
0.5
%1.
7 %
41.
0 %
7.0
%In
con
tine
nce
(se
vere
)20
0.0
%1
5.4
%0
0In
con
tine
nce
(p
ost
rad
iatio
n)
06
0.4
%2.
1 %
51.
0 %
9.0
%Im
po
ten
ce15
29
.0 %
100.
0 %
64.
0 %
41.0
%9
2.0
%78
.0 %
Bla
dd
er
ou
tlet
ob
stru
ctio
n0
04
3.5
%1
8.8
%B
lad
de
r n
eck
co
ntr
act
ure
130.
5 %
14.6
%2
0.7
%2.
4 %
30.
5 %
8.0
%P
roct
itis
022
1.6
%5
5.0
%13
1.0
%7
5.0
%U
rete
ral
ob
stru
ctio
n2
0.0
%0
.7 %
30
.5 %
2.0
%0
He
ma
turi
a1
1.5
%1.
5 %
73.
0 %
14.0
%4
0.1
%19
.0 %
Ure
thra
l str
ictu
re5
2.0
%9
.0 %
210
.4 %
12
.0 %
50
.6 %
4.0
%F
eca
l in
con
tine
nce
02
0.7
%1.
0 %
0C
ard
iova
scu
lar
50.
5 %
3.7
%0
10.
8 %
0.8
%D
iarr
he
a0
70
.7 %
76
.0 %
22
.5 %
50
.0 %
To
tal
ea
rly
44
.0 %
16
.0 %
67
.0 %
10
0.0
%2
18
.0 %
65
.0 %
To
tal
late
41
.3 %
14
.0 %
143
.0 %
63
.0 %
58
.5 %
72
.0 %
Tabl
e 5.
S
umm
ary
outc
omes
—Tr
eatm
ent
com
plic
atio
ns
Archived Document— For Reference Only
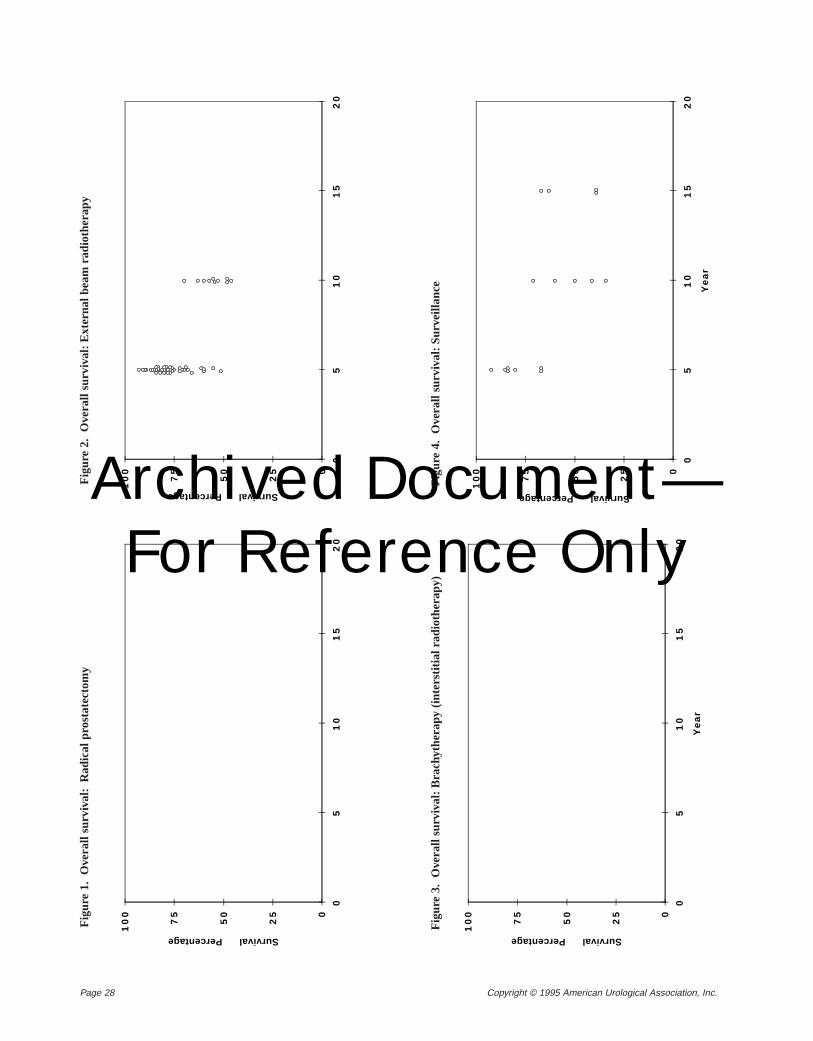
Page 28 Copyright © 1995 American Urological Association, Inc.
Fig
ure
1.
Ove
rall
surv
ival
:R
adic
al p
rost
atec
tom
yF
igur
e 2.
O
vera
ll su
rviv
al:E
xter
nal b
eam
rad
ioth
erap
y
0
25
50
75
10
0
05
10
15
20
Survival Percentage
0
25
50
75
10
0
05
10
15
20
Survival Percentage
Fig
ure
3.
Ove
rall
surv
ival
:Bra
chyt
hera
py (
inte
rstit
ial r
adio
ther
apy)
0
25
50
75
10
0
05
10
15
20
Ye
ar
Survival Percentage
0
25
50
75
10
0
05
10
15
20
Ye
ar
Survival Percentage
Fig
ure
4.
Ove
rall
surv
ival
:Sur
veill
ance
Archived Document— For Reference Only
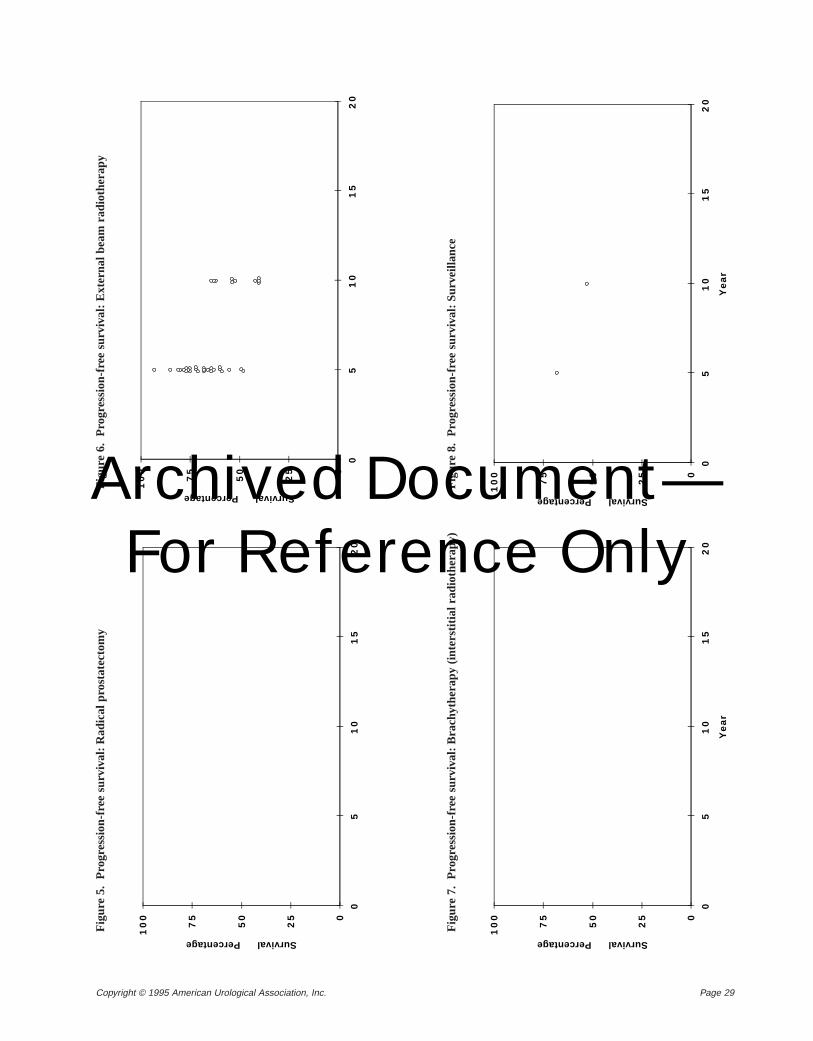
Page 29Copyright © 1995 American Urological Association, Inc.
Fig
ure
5.
Pro
gres
sion
-fre
e su
rviv
al:R
adic
al p
rost
atec
tom
yF
igur
e 6.
P
rogr
essi
on-f
ree
surv
ival
:Ext
erna
l bea
m r
adio
ther
apy
0
25
50
75
10
0
05
10
15
20
Survival Percentage
0
25
50
75
10
0
05
10
15
20
Survival Percentage
Fig
ure
7.
Pro
gres
sion
-fre
e su
rviv
al:B
rach
ythe
rapy
(in
ters
titia
l rad
ioth
erap
y)
0
25
50
75
10
0
05
10
15
20
Ye
ar
Survival Percentage
0
25
50
75
10
0
05
10
15
20
Ye
ar
Survival Percentage
Fig
ure
8.
Pro
gres
sion
-fre
e su
rviv
al:S
urve
illan
ce
Archived Document— For Reference Only
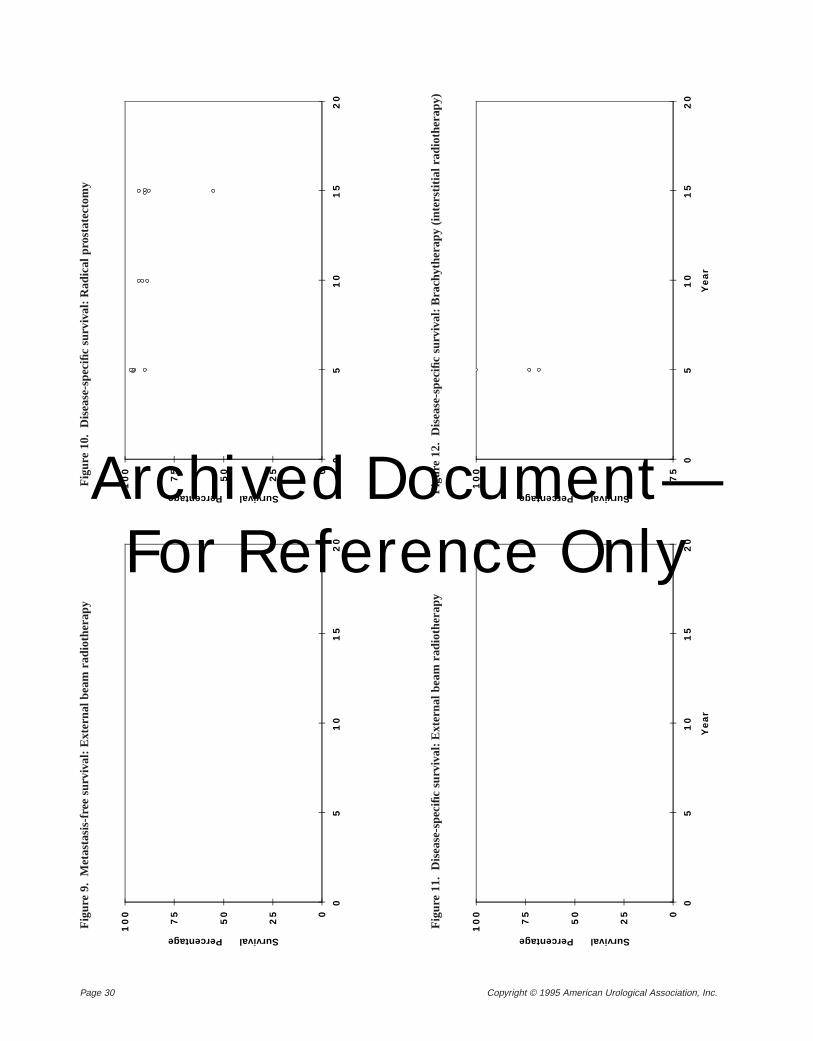
Page 30 Copyright © 1995 American Urological Association, Inc.
Fig
ure
9.
Met
asta
sis-
free
sur
viva
l:E
xter
nal b
eam
rad
ioth
erap
yF
igur
e 10
. D
isea
se-s
peci
fic s
urvi
val:
Rad
ical
pro
stat
ecto
my
0
25
50
75
10
0
05
10
15
20
Survival Percentage
0
25
50
75
10
0
05
10
15
20
Survival Percentage
Fig
ure
11.
Dis
ease
-spe
cific
sur
viva
l:E
xter
nal b
eam
rad
ioth
erap
y
0
25
50
75
10
0
05
10
15
20
Ye
ar
Survival Percentage
75
10
0
05
10
15
20
Ye
ar
Survival PercentageFig
ure
12.
Dis
ease
-spe
cific
sur
viva
l:B
rach
ythe
rapy
(in
ters
titia
l rad
ioth
erap
y)
Archived Document— For Reference Only
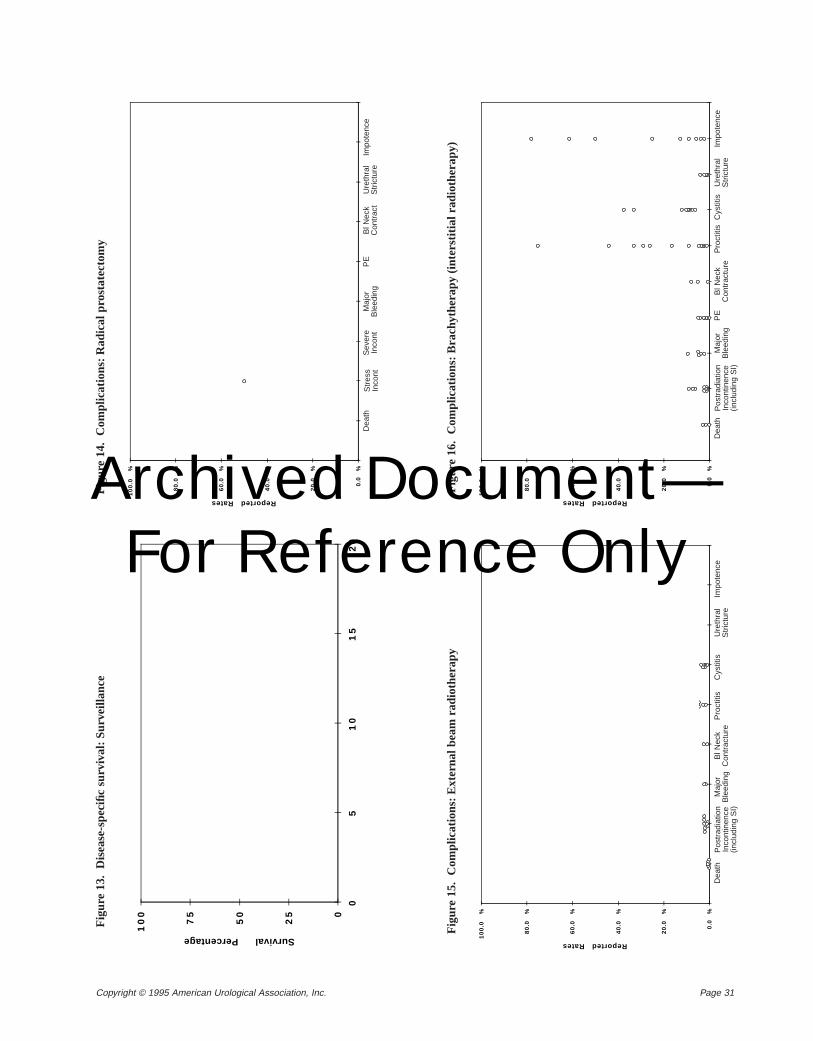
Page 31Copyright © 1995 American Urological Association, Inc.
Fig
ure
13.
Dis
ease
-spe
cific
sur
viva
l:S
urve
illan
ceF
igur
e 14
. C
ompl
icat
ions
:Rad
ical
pro
stat
ecto
my
0
25
50
75
10
0
05
10
15
20
Survival Percentage
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
%
Reported Rates
Fig
ure
15.
Com
plic
atio
ns:E
xter
nal b
eam
rad
ioth
erap
y
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
%
Reported Rates
De
ath
Ma
jor
Ble
ed
ing
Po
str
ad
iati
on
Inc
on
tin
en
ce
(in
clu
din
g
SI)
Bl
Ne
ckC
on
tra
ct
Pro
cti
tis
Cy
st
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
%
Reported Rates
De
ath
Ma
jor
Ble
ed
ing
Po
str
ad
iati
on
Inc
on
tin
en
ce
(in
clu
din
g
SI)
Ure
thra
lS
tric
ture
Imp
ote
nc
eB
l N
eck
Co
ntr
ac
tP
roc
titi
sC
ys
titi
sP
E
Fig
ure
16.
Com
plic
atio
ns:B
rach
ythe
rapy
(inte
rstit
ial r
adio
ther
apy)
Str
ess
Inco
ntIm
pote
nce
Ure
thra
lS
tric
ture
Bl N
eck
Con
trac
tP
EM
ajor
Ble
edin
gS
ever
eIn
cont
Dea
th
Pos
trad
iatio
nIn
cont
inen
ce(in
clud
ing
SI)
Ure
thra
lS
tric
ture
Cys
titis
Pro
ctiti
sB
l Nec
kC
ontr
actu
reP
EM
ajor
Ble
edin
gD
eath
Impo
tenc
eP
ostr
adia
tion
Inco
ntin
ence
(incl
udin
g S
I)
Impo
tenc
eU
reth
ral
Str
ictu
reC
ystit
isP
roct
itis
Bl N
eck
Con
trac
ture
Maj
orB
leed
ing
Dea
th
Archived Document— For Reference Only
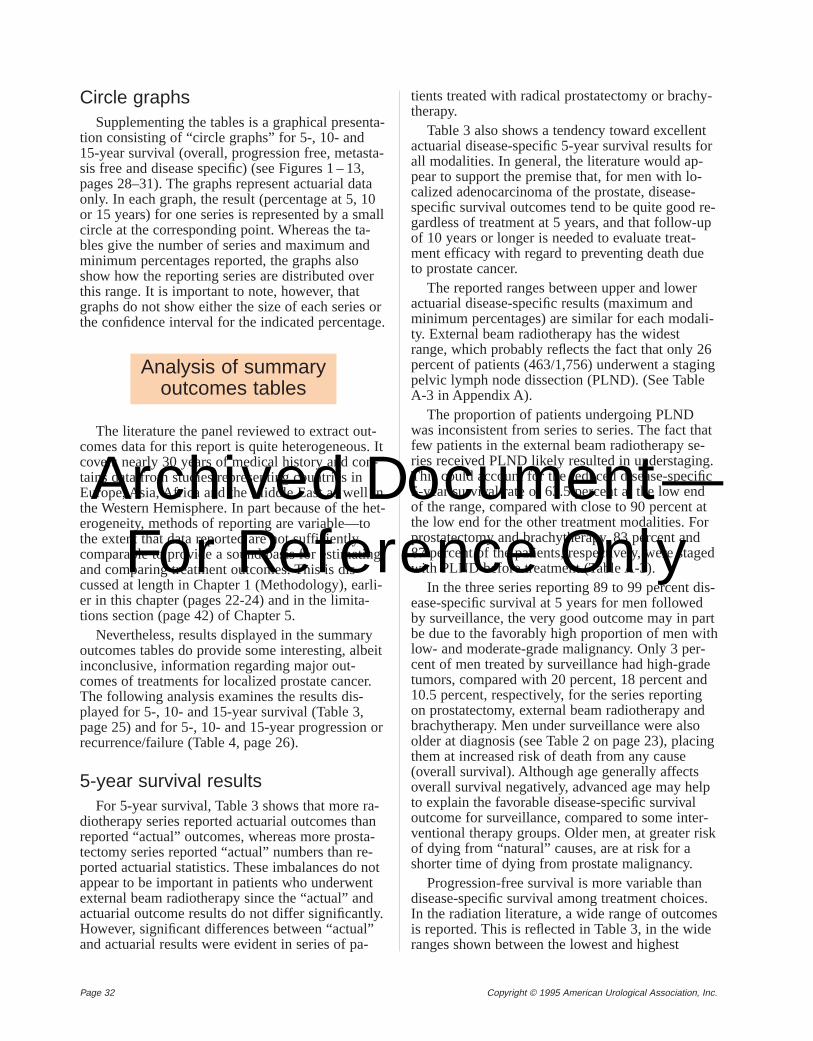
Page 32 Copyright © 1995 American Urological Association, Inc.
Circle graphsSupplementing the tables is a graphical presenta-
tion consisting of “circle graphs” for 5-, 10- and15-year survival (overall, progression free, metasta-sis free and disease specific) (see Figures 1 – 13,pages 28–31). The graphs represent actuarial dataonly. In each graph, the result (percentage at 5, 10or 15 years) for one series is represented by a smallcircle at the corresponding point. Whereas the ta-bles give the number of series and maximum andminimum percentages reported, the graphs alsoshow how the reporting series are distributed overthis range. It is important to note, however, thatgraphs do not show either the size of each series orthe confidence interval for the indicated percentage.
The literature the panel reviewed to extract out-comes data for this report is quite heterogeneous. Itcovers nearly 30 years of medical history and con-tains data from studies representing countries inEurope, Asia, Africa and the Middle East as well inthe Western Hemisphere. In part because of the het-erogeneity, methods of reporting are variable—tothe extent that data reported are not sufficientlycomparable to provide a sound basis for estimatingand comparing treatment outcomes. This is dis-cussed at length in Chapter 1 (Methodology), earli-er in this chapter (pages 22-24) and in the limita-tions section (page 42) of Chapter 5.
Nevertheless, results displayed in the summaryoutcomes tables do provide some interesting, albeitinconclusive, information regarding major out-comes of treatments for localized prostate cancer.The following analysis examines the results dis-played for 5-, 10- and 15-year survival (Table 3,page 25) and for 5-, 10- and 15-year progression orrecurrence/failure (Table 4, page 26).
5-year survival resultsFor 5-year survival, Table 3 shows that more ra-
diotherapy series reported actuarial outcomes thanreported “actual” outcomes, whereas more prosta-tectomy series reported “actual” numbers than re-ported actuarial statistics. These imbalances do notappear to be important in patients who underwentexternal beam radiotherapy since the “actual” andactuarial outcome results do not differ significantly.However, significant differences between “actual”and actuarial results were evident in series of pa-
tients treated with radical prostatectomy or brachy-therapy.
Table 3 also shows a tendency toward excellentactuarial disease-specific 5-year survival results forall modalities. In general, the literature would ap-pear to support the premise that, for men with lo-calized adenocarcinoma of the prostate, disease-specific survival outcomes tend to be quite good re-gardless of treatment at 5 years, and that follow-upof 10 years or longer is needed to evaluate treat-ment efficacy with regard to preventing death dueto prostate cancer.
The reported ranges between upper and loweractuarial disease-specific results (maximum andminimum percentages) are similar for each modali-ty. External beam radiotherapy has the widestrange, which probably reflects the fact that only 26percent of patients (463/1,756) underwent a stagingpelvic lymph node dissection (PLND). (See TableA-3 in Appendix A).
The proportion of patients undergoing PLNDwas inconsistent from series to series. The fact thatfew patients in the external beam radiotherapy se-ries received PLND likely resulted in understaging.This could account for the reduced disease-specific5-year survival rate of 63.5 percent at the low endof the range, compared with close to 90 percent atthe low end for the other treatment modalities. Forprostatectomy and brachytherapy, 83 percent and87 percent of the patients, respectively, were stagedwith PLND before treatment (Table A-3).
In the three series reporting 89 to 99 percent dis-ease-specific survival at 5 years for men followedby surveillance, the very good outcome may in partbe due to the favorably high proportion of men withlow- and moderate-grade malignancy. Only 3 per-cent of men treated by surveillance had high-gradetumors, compared with 20 percent, 18 percent and10.5 percent, respectively, for the series reportingon prostatectomy, external beam radiotherapy andbrachytherapy. Men under surveillance were alsoolder at diagnosis (see Table 2 on page 23), placingthem at increased risk of death from any cause(overall survival). Although age generally affectsoverall survival negatively, advanced age may helpto explain the favorable disease-specific survivaloutcome for surveillance, compared to some inter-ventional therapy groups. Older men, at greater riskof dying from “natural” causes, are at risk for ashorter time of dying from prostate malignancy.
Progression-free survival is more variable thandisease-specific survival among treatment choices.In the radiation literature, a wide range of outcomesis reported. This is reflected in Table 3, in the wideranges shown between the lowest and highest
Analysis of summaryoutcomes tables
Archived Document— For Reference Only
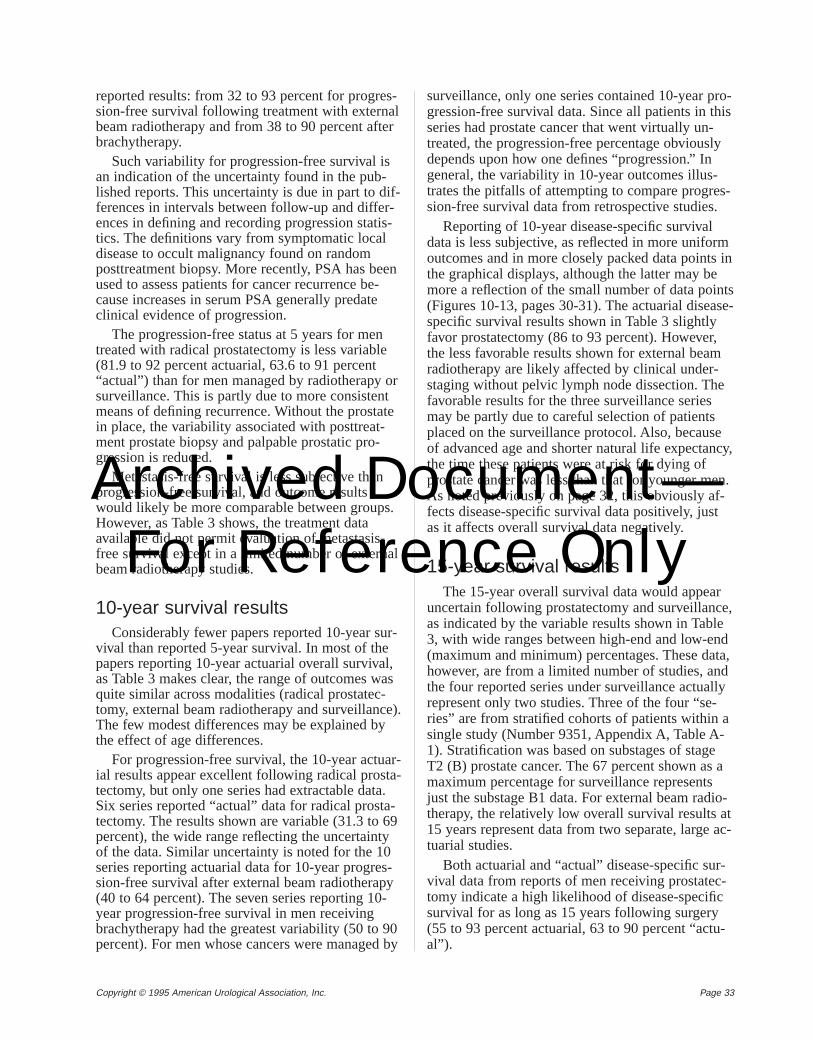
Page 33Copyright © 1995 American Urological Association, Inc.
reported results: from 32 to 93 percent for progres-sion-free survival following treatment with externalbeam radiotherapy and from 38 to 90 percent afterbrachytherapy.
Such variability for progression-free survival isan indication of the uncertainty found in the pub-lished reports. This uncertainty is due in part to dif-ferences in intervals between follow-up and differ-ences in defining and recording progression statis-tics. The definitions vary from symptomatic localdisease to occult malignancy found on randomposttreatment biopsy. More recently, PSA has beenused to assess patients for cancer recurrence be-cause increases in serum PSA generally predateclinical evidence of progression.
The progression-free status at 5 years for mentreated with radical prostatectomy is less variable(81.9 to 92 percent actuarial, 63.6 to 91 percent“actual”) than for men managed by radiotherapy orsurveillance. This is partly due to more consistentmeans of defining recurrence. Without the prostatein place, the variability associated with posttreat-ment prostate biopsy and palpable prostatic pro-gression is reduced.
Metastasis-free survival is less subjective thanprogression-free survival, and outcome resultswould likely be more comparable between groups.However, as Table 3 shows, the treatment dataavailable did not permit evaluation of metastasis-free survival except in a limited number of externalbeam radiotherapy studies.
10-year survival resultsConsiderably fewer papers reported 10-year sur-
vival than reported 5-year survival. In most of thepapers reporting 10-year actuarial overall survival,as Table 3 makes clear, the range of outcomes wasquite similar across modalities (radical prostatec-tomy, external beam radiotherapy and surveillance).The few modest differences may be explained bythe effect of age differences.
For progression-free survival, the 10-year actuar-ial results appear excellent following radical prosta-tectomy, but only one series had extractable data.Six series reported “actual” data for radical prosta-tectomy. The results shown are variable (31.3 to 69percent), the wide range reflecting the uncertaintyof the data. Similar uncertainty is noted for the 10series reporting actuarial data for 10-year progres-sion-free survival after external beam radiotherapy(40 to 64 percent). The seven series reporting 10-year progression-free survival in men receivingbrachytherapy had the greatest variability (50 to 90percent). For men whose cancers were managed by
surveillance, only one series contained 10-year pro-gression-free survival data. Since all patients in thisseries had prostate cancer that went virtually un-treated, the progression-free percentage obviouslydepends upon how one defines “progression.” Ingeneral, the variability in 10-year outcomes illus-trates the pitfalls of attempting to compare progres-sion-free survival data from retrospective studies.
Reporting of 10-year disease-specific survivaldata is less subjective, as reflected in more uniformoutcomes and in more closely packed data points inthe graphical displays, although the latter may bemore a reflection of the small number of data points(Figures 10-13, pages 30-31). The actuarial disease-specific survival results shown in Table 3 slightlyfavor prostatectomy (86 to 93 percent). However,the less favorable results shown for external beamradiotherapy are likely affected by clinical under-staging without pelvic lymph node dissection. Thefavorable results for the three surveillance seriesmay be partly due to careful selection of patientsplaced on the surveillance protocol. Also, becauseof advanced age and shorter natural life expectancy,the time these patients were at risk for dying ofprostate cancer was less than that for younger men.As noted previously on page 32, this obviously af-fects disease-specific survival data positively, justas it affects overall survival data negatively.
15-year survival resultsThe 15-year overall survival data would appear
uncertain following prostatectomy and surveillance,as indicated by the variable results shown in Table3, with wide ranges between high-end and low-end(maximum and minimum) percentages. These data,however, are from a limited number of studies, andthe four reported series under surveillance actuallyrepresent only two studies. Three of the four “se-ries” are from stratified cohorts of patients within asingle study (Number 9351, Appendix A, Table A-1). Stratification was based on substages of stageT2 (B) prostate cancer. The 67 percent shown as amaximum percentage for surveillance representsjust the substage B1 data. For external beam radio-therapy, the relatively low overall survival results at15 years represent data from two separate, large ac-tuarial studies.
Both actuarial and “actual” disease-specific sur-vival data from reports of men receiving prostatec-tomy indicate a high likelihood of disease-specificsurvival for as long as 15 years following surgery(55 to 93 percent actuarial, 63 to 90 percent “actu-al”).
Archived Document— For Reference Only
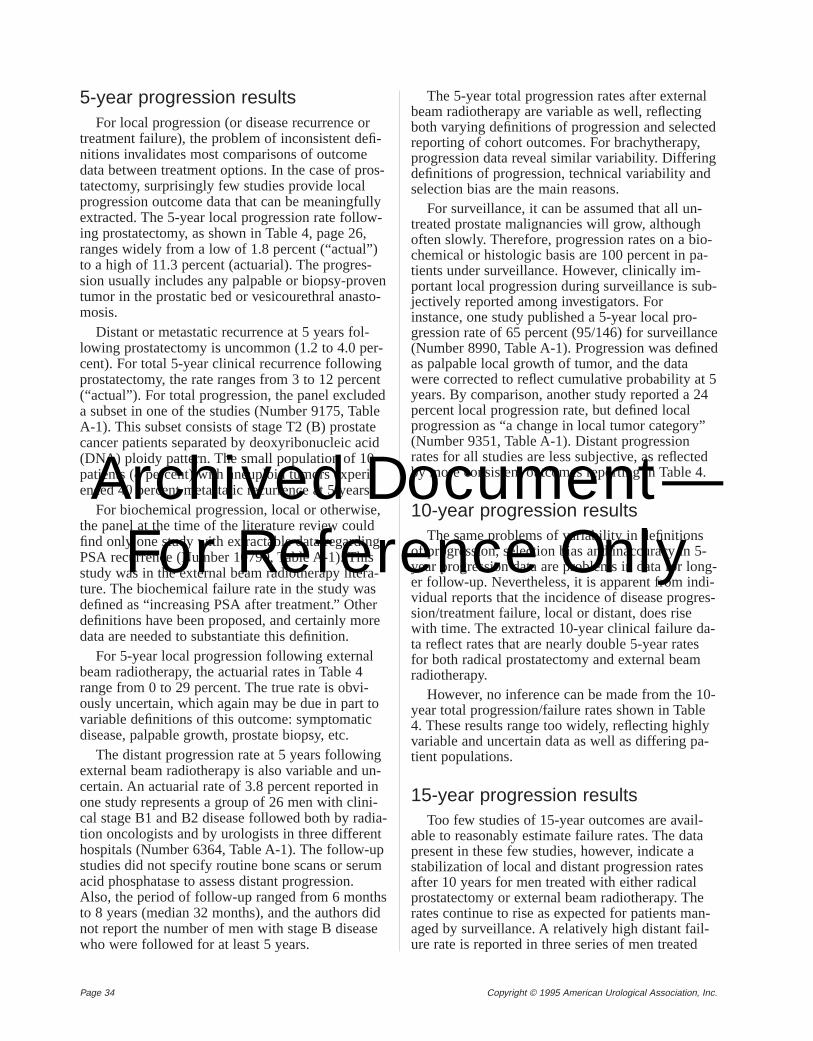
Page 34 Copyright © 1995 American Urological Association, Inc.
5-year progression resultsFor local progression (or disease recurrence or
treatment failure), the problem of inconsistent defi-nitions invalidates most comparisons of outcomedata between treatment options. In the case of pros-tatectomy, surprisingly few studies provide localprogression outcome data that can be meaningfullyextracted. The 5-year local progression rate follow-ing prostatectomy, as shown in Table 4, page 26,ranges widely from a low of 1.8 percent (“actual”)to a high of 11.3 percent (actuarial). The progres-sion usually includes any palpable or biopsy-proventumor in the prostatic bed or vesicourethral anasto-mosis.
Distant or metastatic recurrence at 5 years fol-lowing prostatectomy is uncommon (1.2 to 4.0 per-cent). For total 5-year clinical recurrence followingprostatectomy, the rate ranges from 3 to 12 percent(“actual”). For total progression, the panel excludeda subset in one of the studies (Number 9175, TableA-1). This subset consists of stage T2 (B) prostatecancer patients separated by deoxyribonucleic acid(DNA) ploidy pattern. The small population of 10patients (4 percent) with aneuploid tumors experi-enced 40 percent metastatic recurrence at 5 years.
For biochemical progression, local or otherwise,the panel at the time of the literature review couldfind only one study with extractable data regardingPSA recurrence (Number 10790, Table A-1). Thisstudy was in the external beam radiotherapy litera-ture. The biochemical failure rate in the study wasdefined as “increasing PSA after treatment.” Otherdefinitions have been proposed, and certainly moredata are needed to substantiate this definition.
For 5-year local progression following externalbeam radiotherapy, the actuarial rates in Table 4range from 0 to 29 percent. The true rate is obvi-ously uncertain, which again may be due in part tovariable definitions of this outcome: symptomaticdisease, palpable growth, prostate biopsy, etc.
The distant progression rate at 5 years followingexternal beam radiotherapy is also variable and un-certain. An actuarial rate of 3.8 percent reported inone study represents a group of 26 men with clini-cal stage B1 and B2 disease followed both by radia-tion oncologists and by urologists in three differenthospitals (Number 6364, Table A-1). The follow-upstudies did not specify routine bone scans or serumacid phosphatase to assess distant progression.Also, the period of follow-up ranged from 6 monthsto 8 years (median 32 months), and the authors didnot report the number of men with stage B diseasewho were followed for at least 5 years.
The 5-year total progression rates after externalbeam radiotherapy are variable as well, reflectingboth varying definitions of progression and selectedreporting of cohort outcomes. For brachytherapy,progression data reveal similar variability. Differingdefinitions of progression, technical variability andselection bias are the main reasons.
For surveillance, it can be assumed that all un-treated prostate malignancies will grow, althoughoften slowly. Therefore, progression rates on a bio-chemical or histologic basis are 100 percent in pa-tients under surveillance. However, clinically im-portant local progression during surveillance is sub-jectively reported among investigators. Forinstance, one study published a 5-year local pro-gression rate of 65 percent (95/146) for surveillance(Number 8990, Table A-1). Progression was definedas palpable local growth of tumor, and the datawere corrected to reflect cumulative probability at 5years. By comparison, another study reported a 24percent local progression rate, but defined localprogression as “a change in local tumor category”(Number 9351, Table A-1). Distant progressionrates for all studies are less subjective, as reflectedby more consistent outcomes reporting in Table 4.
10-year progression resultsThe same problems of variability in definitions
of progression, selection bias and inaccuracy in 5-year progression data are problems in data for long-er follow-up. Nevertheless, it is apparent from indi-vidual reports that the incidence of disease progres-sion/treatment failure, local or distant, does risewith time. The extracted 10-year clinical failure da-ta reflect rates that are nearly double 5-year ratesfor both radical prostatectomy and external beamradiotherapy.
However, no inference can be made from the 10-year total progression/failure rates shown in Table4. These results range too widely, reflecting highlyvariable and uncertain data as well as differing pa-tient populations.
15-year progression resultsToo few studies of 15-year outcomes are avail-
able to reasonably estimate failure rates. The datapresent in these few studies, however, indicate astabilization of local and distant progression ratesafter 10 years for men treated with either radicalprostatectomy or external beam radiotherapy. Therates continue to rise as expected for patients man-aged by surveillance. A relatively high distant fail-ure rate is reported in three series of men treated
Archived Document— For Reference Only
Page 35Copyright © 1995 American Urological Association, Inc.
with brachytherapy. The three series are from thesame report (Number 9879, Table A-1) and repre-sent substages of stage T2 (B) prostate cancer. Pro-gression/failure of 64 percent was found in menwith substage B3 prostate malignancy. It is obviousthat the 15-year progression data are sparse, vari-able and uncertain.
The variability in the prostate cancer treatmentliterature in reporting factors such as grade, stageand age of the patient—which has a confoundingeffect on reported data for survival and progres-sion—has a similar confounding effect on reporteddata for complications from surgery or radiationtreatment. The panel chose therefore to display re-sults of the extracted data on treatment complica-tions in the same manner as for the survival andprogression data.
The complications summary outcomes table(Table 5) on page 27 lists the 25 most commonlyreported complications. Under each treatment mod-ality to which a particular complication applies,Table 5 displays the number of series reporting thecomplication and the lowest and highest reportedfrequencies of occurrence (minimum/maximumpercentages). The table does not show mean or me-dian estimates of frequency.
Graphical displays visually represent the report-ed frequency rates for the most important complica-tions (Figures 14 - 16, page 31). Each circle on agraph represents one series reporting the complica-tion. As in the graphs representing survival out-comes, these graphs are a useful supplement toTable 5 in that they show how the reporting seriesare distributed along the range between the mini-mum and maximum percentages. Again, however, itmust be noted that the graphs show neither the sizeof each series nor the confidence interval for the in-dicated percentage.
It should also be noted that the data displayed inTable 5 and Figures 14– 16, in addition to beingsubject to problems of variability mentioned previ-ously, may be subject to publication bias. The pos-sibility exists that those centers publishing their re-sults are mainly centers having low complicationrates. The data could also be biased in the other di-rection because many of the series may not be re-cent enough for reported complications to reflect
improvements in modern surgical and radiologicaltechniques.
Some of the complications in Table 5 apply to allthree treatment modalities, but not necessarily tothe same extent. Stress incontinence, for example,is reported by 19 series as a complication of radicalprostatectomy, but by only two series as a compli-cation of external beam radiotherapy. To a consider-able degree, each form of therapy has its own spec-trum of complications. In an obvious example,wound infection is a potential complication of pros-tatectomy, but is reported by zero series under thenoninvasive external beam radiotherapy. For procti-tis, a potential complication of radiotherapy, Table5 shows a zero under prostatectomy. The panel wasunable to determine that any one therapy has amore significant cumulative risk of complications.
In the case of complications from external beamradiotherapy, the data shown in Table 5 may over-state the frequency of some complications follow-ing this treatment, such as proctitis and other rectaltoxicity. The reason is that, in abstracting the com-plications data for external beam radiotherapy, thepanel found very little information specific to stageT2 (B) disease. The panel faced a choice: either in-clude only series that purely address T2 patients, inwhich case there would essentially be no data, orinclude radiotherapy series that describe complica-tions in all stages of disease. The panel chose to in-clude all radiotherapy series that describe toxicityin order to provide at least rough indications of riskfrom therapy.
However, toxicity from radiotherapy is muchmore likely in advanced stages of disease, becausepatients reported with stages T3-T4 (C) or M1 (D2)tumors are much more likely to have received ra-diotherapy to regional lymph nodes. Radiation tothe entire pelvis and in some cases the para-aorticregion is often administered in those with higher-stage disease. Moreover, these patients are oftentreated with significantly greater doses of radiationto significantly larger amounts of normal tissue,which markedly increases toxicity (Green, Gold-berg, Goldman, et al., 1984; Lawton, Won, Pile-pich, et al., 1991; Mameghan, Fisher, Mameghan,et al., 1990; Pilepich, Krall, Sause, et al., 1987;Smit, Helle, van Putten, et al., 1990).
If the panel had been able to include only thecomplications data for external beam treatment ofstage T2 disease, the frequency rates would verylikely have been less than what Table 5 shows.Patients clinically judged as having T2 disease (as agroup) will generally receive a lower dose of radia-tion to a smaller volume of tissue.
Treatment complicationssummary outcomes table
and graphs
Archived Document— For Reference Only
Page 36 Copyright © 1995 American Urological Association, Inc.
Of the complications listed in Table 5 for treat-ments of stage T2 prostate cancer, the panel consid-ered the most important to be perioperative death,major bleeding, pulmonary embolism, inconti-nence, impotence (erectile dysfunction), rectal in-jury, cystitis, proctitis, bladder neck contracture andurethral stricture. Most often reported are rates ofdeath, incontinence, rectal injury and impotence.Some surgical series also comment on adverse post-operative events such as bleeding and pulmonaryembolism.
A structured review of the literature (Wasson,Cushman, Bruskewitz, et al., 1993) found reportedcomplication rates within the ranges reported inTable 5. Also, patient attitudes about the impor-tance of such adverse events are now under activeinvestigation. One study used standardized data col-lection instruments to examine patient attitudes re-garding complications following radical prostatec-tomy (Fowler, Barry, Lu-Yao, et al., 1993). Reportsby these patients indicated higher rates of strictureand incontinence than in most reported series.Moreover, complete incontinence, bladder neckcontracture and stricture formation may result fromadditional interventions to ameliorate the originalproblem. Patient interviews in the Fowler study in-dicate that treatment of these urinary complications,with associated symptoms such as frequent urina-tion, wetness and difficulty in voiding, is often notvery successful. (Age was not related to postsurgi-cal incontinence in this study.)
Table 5 shows that both obstruction and inconti-nence may be more common following surgery.Cystitis, which most often results in the symptomof urinary frequency, is a potential complication ofradiotherapy. Radiotherapy is also more likely thansurgery to cause bowel/rectal injury. Diarrhea asso-ciated with radiotherapy is usually transient.
With regard to the important complication of im-potence (erectile dysfunction) following activetreatment for prostate cancer, the reports are diffi-cult to interpret because of patient selection. This isan instance in which a patient-related factor, age,may affect the complications data. The youngest(and presumably most potent) patients tend to un-dergo surgery. The oldest patients tend to receiveradiotherapy. Few reports have carefully comparedpretreatment and posttreatment potency. For treat-ment of erectile dysfunction, patients report favor-ably on treatment with pharmacologic erection ther-apy, penile implantation or vacuum devices (Fowl-er, Barry, Lu-Yao, et al., 1993).
With regard to perioperative mortality, deathfrom treatment is relatively rare following externalbeam radiotherapy. Death following surgery, al-though shown to increase with age, is generally lessthan 1 percent in men under age 75 (Lu-Yao,McLerran, Wasson, et al., 1993).
Significant bleeding may be expected to occurfollowing radical prostatectomy with a frequencybetween 1.0 and 11.5 percent. The perineal ap-proach may have the lowest incidence of this com-plication. Finally, pulmonary embolism and sepsisare risks of any operative intervention. Medicaredata suggest that the incidence of cardiopulmonarycomplications following radical prostatectomy in-creases to more than 7 percent in men over age 75(Lu-Yao, McLerran, Wasson, et al., 1993).
Analysis of treatmentcomplications summary
outcomes table
Archived Document— For Reference Only
Page 37Copyright © 1995 American Urological Association, Inc.
The AUA Prostate Cancer Clinical GuidelinesPanel generated its practice policy recommenda-tions based on the outcome estimates available andon panel opinion. As explained in Chapter 1, therecommendations were graded according to threelevels of flexibility based on strength of evidenceand the panel’s assessment of patient needs andpreferences. The definitions of these three levels arerepeated below from Chapter 1:
• Standard: A policy is considered a standardif the health and economic outcomes of the al-ternative interventions are sufficiently well-known to permit meaningful decisions andthere is virtual unanimity about which inter-vention is preferred.
• Guideline: A policy is considered a guidelineif the health and economic outcomes of the in-terventions are sufficiently well-known to per-mit meaningful decisions and an appreciablebut not unanimous majority agree on which in-tervention is preferred.
• Option: A policy is considered an option if(1) the health and economic outcomes of theinterventions are not sufficiently well-knownto permit meaningful decisions, (2) prefer-ences among the outcomes are not known, (3)patients’ preferences are divided among alter-native interventions and/or (4) patients are in-different about the alternative interventions.
Obviously, a standard has the least flexibility. Aguideline has significantly more flexibility, and anoption is the most flexible. As noted in the defini-tions, options can exist because of insufficient evi-dence or because patient preferences are divided orunknown. In the following panel recommendations,those regarding treatment choices were labeled op-tions mostly because of insufficient evidence. Noneof the following panel recommendations fits theabove definition of a guideline.
The panel’s recommendations apply to the stan-dard patient, defined as a man who has clinicallylocalized prostate cancer (adenocarcinoma of the
prostate). For this report, the panel focused on clin-ical stage T2 (B) disease. Based on the opinion ofthe panel, recommendations may also be applied topatients diagnosed with stage cT1c disease (detect-ed by elevated PSA). The recommendations werenot developed for patients with stage T1a/b(A1/A2) or clinical T3-T4 (C) disease. For a de-tailed discussion of prostate cancer staging, seepages 13-15.
As a standard, an assessment of the patient’s lifeexpectancy, overall health status and tumor charac-teristics is necessary before any treatment decisionscan be made.
Life expectancy:Life expectancy, rather than pa-tient age, should be the factor considered in treat-ment selection. Therefore, the panel did not set aspecific chronological cutoff point. When a man’slife expectancy is relatively long, prostate cancercan be a cause of morbidity and mortality. On theother hand, at an advanced patient age, or when lifeexpectancy is relatively short, competing hazardsfor mortality reduce the chance that a man will suf-fer from disease progression or die from prostatecancer. (See U.S. Life Expectancy Table in Appen-dix C.)
Health status:The patient’s overall health statusis the sum of all conditions and includes both pa-tient and family history as well as the present stateof the patient’s well-being and the degree of anycoexistent disease. There are two reasons to evalu-ate the overall health status prior to deciding on anintervention: (1) Overall health status influenceslife expectancy; (2) overall health status may affectpatient response to adverse events resulting fromparticular interventions.
Tumor characteristics:The histologic grade andstage of the tumor should be considered when as-sessing the potential natural history and treatmentoptions for prostate cancer. Small, well-differentiat-ed cancers progress more slowly and are less likelyto be life threatening than large, poorly differentiat-
Recommendations: Standards
The standard patient
Chapter 4: Treatment recommendations
Archived Document— For Reference Only
Page 38 Copyright © 1995 American Urological Association, Inc.
ed tumors which have a greater potential to be bio-logically aggressive and clinically significant.
As a standard, a patient with clinically localizedprostate cancer should be informed about the com-monly accepted initial interventions including, at aminimum, radical prostatectomy, radiotherapy andsurveillance. A discussion of the estimates for bene-fits and harms of each intervention should be of-fered to the patient.
The panel defines radical prostatectomy to in-clude complete removal of the prostate, vasalampullae and seminal vesicles. The panel definesradiotherapy to include external beam and/or inter-stitial (brachytherapy) treatments. Surveillance isdefined as periodic monitoring of the patient’s pros-tate cancer and its effects.
The patient should be informed that dependingon his condition and initial choice, subsequent in-terventions may be appropriate.
As a standard, the patient’s preference, based onhis attitude toward the course of the disease and thebenefits and harms of the different interventions,should be considered in determining his treatment.
Options for management of localized prostatecancer include radical prostatectomy, radiotherapyand surveillance. Radiotherapy includes externalbeam and interstitial (brachytherapy) treatments.The panel considers these interventions to be op-tions because data from the literature do not pro-vide clear-cut evidence for the superiority of anyone treatment. Described for each option is the pa-tient most likely to benefit from the intervention.
Radical prostatectomy:Based on the panel’sinterpretation of the literature and panel opinion,the patient most likely to benefit from radical pros-tatectomy would have a relatively long life ex-pectancy, no significant surgical risk factors and apreference to undergo surgery.
Radiotherapy: Based on the panel’s interpreta-tion of the literature and panel opinion, the patientmost likely to benefit from radiotherapy would havea relatively long life expectancy, no significant riskfactors for radiation toxicity and a preference forradiotherapy.
Surveillance: Based on the panel’s interpretationof the literature and panel opinion, patients mostlikely to benefit from surveillance are those with ashorter life expectancy and/or a low-grade tumor.
Radical prostatectomyThe major advantage of radical (total) prostatec-
tomy is its potential for “cure” by removing all ofthe tumor. “Cure” is defined as lifetime freedomfrom disease. Total prostatectomy in the properlyselected patient will provide disease-free survivalrates comparable to the expected survival in simi-larly aged men for up to 30 years of observation(Gibbons, Correa, Brannen, et al., 1989).
The major disadvantage is potential morbidity.Possible operative morbidity includes the follow-ing: bleeding, which can require a transfusion; dif-ficulty with anastomosis of the bladder neck to ure-thra; and rectal injury. These problems will varywith the size and anatomy of the patient’s pelvic or-gans and the experience of the surgeon. Postoperat-ive morbidity includes problems with indwellingcatheters, lymphocele, anastomotic stricture, uri-nary incontinence and impotence (erectile dysfunc-tion).
With regard to impotence, some authors have re-ported postoperative potency rates in the 70-percentrange in patients who were potent preoperatively(Catalona and Bigg, 1990). If impotence occursafter surgery (or radiotherapy or hormone therapy),what is lost is erectile function. The sensation oforgasm may remain intact. In these patients, phar-macologically induced erections (using self-admin-istered penile injections) or use of vacuum constric-tion devices or penile prostheses can provide effect-ive treatment (Lue, Carroll and Moore, 1989).
A number of articles have reported stress urinaryincontinence and/or severe urinary incontinence (re-quiring intervention) following radical prostatec-tomy. The complications summary outcomes table(Table 5) on page 27 shows a reported low of 4 per-cent and a high of 50 percent for stress inconti-nence and a range from 0 percent to 15.4 percentfor severe incontinence. The complications graphfor prostatectomy (Figure 14, page 31) shows howthe reporting series are distributed along these low-high ranges.
For mortality following radical prostatectomy,Table 5 shows a range from 0 percent to 2.1 per-cent. More than half the series reported 0 percent.However, the risk of death from radical prostatec-tomy increases with patient age and was found tobe 1.4 percent in men aged 75 to 80 and 4.6 percent
Advantages and disadvantagesof treatment options
Recommendations:Treatment options
Archived Document— For Reference Only
Page 39Copyright © 1995 American Urological Association, Inc.
for age 80 and older (Lu-Yao, McLerran, Wasson,et al., 1993).
Pulmonary embolism, in the panel’s review ofthe literature, occurred in 0.8 percent to 7.7 percentof patients after radical prostatectomy. In a reportof Medicare patients (Lu-Yao, McLerran, Wasson,et al., 1993), investigators found cardiopulmonarycomplications in 4 percent of men 65 to 69 years ofage and in 7.4 percent of men 75 to 79 years ofage. Other potential complications, such as anasto-motic stricture, fistula and bowel injuries, occur in-frequently.
Recent developments in the technique of radicalprostatectomy may have reduced the risks of com-plications. Refinements in the understanding of thesurgical anatomy of the prostate have made possi-ble a more meticulous operation, improved opera-tive visualization, reduction in blood loss and im-proved sexual function and urinary continence ratespostoperatively.
Length of hospitalization has also been signifi-cantly reduced in many patients to 3 – 6 days, butthe total cost for radical prostatectomy has not beenwell described and remains a “moving target”(Koch, Smith, Hodge, et al., 1994).
RadiotherapyThe advantage of radiotherapy (external beam
radiotherapy and brachytherapy) is that it not onlyhas a potential for cure, but is well tolerated in themajority of men when modern techniques are used.Its principal potential harms include radiation cysti-tis, proctitis, and erectile dysfunction. Also, becausethe prostate remains in place, persistence and pro-gression of the disease may occur.
External beam radiotherapy
External beam radiotherapy can be an effectivetreatment in the appropriate standard patient afflict-ed with stage T2 prostate cancer. Notwithstandingcaveats regarding survival and disease progressiondata (pages 32-33, 33-34), the results reported inthe literature for external beam radiotherapy appearreasonably favorable. Although some selected se-ries have reported extremely high PSA failures(noted in Hanks, 1994), others have demonstratedextremely favorable PSA control with long-termfollow-up (Hanks, 1994; Hanks, Perez, Kozar, etal., 1993; Pisansky, Cha, Earle, et al., 1993).
However, an accurate characterization of the trueincidence of PSA failure in an unbiased cohort isurgently needed. There is also evidence that clinicallack of local tumor progression may underestimate
the true incidence of cancer remaining in the pros-tate gland. Biopsies of the radiated gland have re-vealed persistent malignancy in at least 30 percentof patients (Kabalin, Hodge, McNeal, et al., 1989;Kaplan, Prestidge, Bagshaw, et al., 1992; Kiesling,McAninch, Goebel, et al., 1980). Recently, TRUS-guided biopsy series in selected patients suggestthat the true incidence of residual cancer may bemuch higher than previously reported.
Regarding toxicity, external beam radiotherapy,as employed in state-of-the-art radiotherapy centers,has the advantage of having become a very well-tolerated treatment. Improvements include higher-energy radiation beams that can be more preciselyfocused, thus sparing larger amounts of normal tis-sue from therapy; improved computer technologythat calculates with greater precision the absorbeddose of radiation and helps optimize treatmentplanning; and more sophisticated planning proce-dures that precisely localize both the tumor volumeand normal tissues, allowing maximal sparing ofnormal tissues and ensuring adequate delivery ofdose to the tumor.
However, there remain many potential complica-tions. The actual incidence of erectile dysfunctionfor patients receiving radiotherapy (as in series ofpatients receiving other forms of therapy) may beunderreported. Diarrhea is a potential problem forthose patients who receive radiation to regionallymphatics. Other potential significant complica-tions include rectal toxicity (proctitis, rectal ulcera-tion, need for colostomy) as well as bladder com-plications (hematuria, cystitis, dysfunctional void-ing).
Brachytherapy
Mature data are only available for the olderretropubic brachytherapy techniques. Althoughproblems have been reported in these mature brach-ytherapy series (page 18), several groups have doc-umented reasonably satisfactory survival results.The 5-year survival data are not yet available forthe newer ultrasound-guided transperineal tech-niques. However, as the outcomes analysis on pages32-33 indicates, the 5-year survival results wouldbe expected to be quite good. In general, eventhough sufficiently mature data are not yet availableto establish superiority of the newer techniques, thepanel knows of no evidence that the results fromthese techniques are inferior to results from the old-er techniques.
One clear advantage of the current brachytherapymethods is patient convenience. Several series ofTRUS-guided transperineal techniques report that
Archived Document— For Reference Only
Page 40 Copyright © 1995 American Urological Association, Inc.
the procedures are usually performed with hospitalstays of 2 days or less. When permanent radionu-clides are implanted, there is usually only a moder-ate amount of postimplantation discomfort, con-trolled in the overwhelming majority of patients byoral pain medications.
Disadvantages of brachytherapy can include in-ferior control of localized tumors. Similar to allprostate cancer treatment modalities, brachytherapyproduces markedly improved local control in low-stage and low- to moderate-grade disease (Carey,Lippert, Constable, et al., 1988; Fuks, Leibel, Wall-ner, et al., 1991; Giles and Brady, 1986; Kuban, El-Mahdi and Schellhammer, 1989a; Morton and Pes-chel, 1988; Smalley and Noble, 1992).
Additionally, the importance of long-term fol-low-up cannot be overemphasized. Several serieshave reported that the mean time to local failure inbrachytherapy-treated patients is in the range of 5to 10 years (Fuks, Leibel, Wallner, et al., 1991;Kuban, El-Mahdi and Schellhammer, 1989a; Small-ey and Noble, 1992). The exceedingly long time tolocal recurrence seen in series that have adequatefollow-up emphasizes both the indolent natural his-tory of the disease and the tentative nature of anyconclusion reached in studies without follow-up of10 to 15 years.
The ability of brachytherapy to control local dis-ease must, therefore, be evaluated on the basis ofseries that have sufficient follow-up. Four differentreports have compared local tumor control withbrachytherapy versus control with alternative thera-pies. Three reported that brachytherapy producedinferior local tumor control when compared witheither external beam radiotherapy or radical prosta-tectomy (Kuban, El-Mahdi and Schellhammer,1989a; Morton and Peschel, 1988; Schellhammer,Whitmore, Kuban, et al., 1989; Smalley and Noble,1992). However, differences in other factors such aspatient selection, rather than the treatment itself,may explain the differences in outcomes.
With regard to complications, those reported inpresent brachytherapy series are remarkably hetero-geneous. They include impotence (erectile dysfunc-tion), with no convincing evidence of less risk thanwith external beam radiotherapy (Smalley andNoble, 1992). For the newer, TRUS-guided trans-perineal techniques, rates for the complications re-ported to date vary widely (Blasko, Ragde andGrimm, 1991; Iversen, Bak, Juul, et al., 1989).
In some stage T2 patients, higher complicationshave been reported for brachytherapy as comparedwith external beam radiotherapy. Also, patients witha previous transurethral resection or significant oth-
er uropathy have a much greater risk of developingsubsequent urinary complications.
SurveillanceOne advantage of surveillance therapy as a treat-
ment option for localized carcinoma of the prostateis its low initial cost. Because most patients can befollowed with DRE and PSA alone, if disease pro-gression does not develop during the patient’s life-time, the cost of such follow-up may be very low.This advantage is dependent upon the assumptionthat most patients will not develop symptomatic ormetastatic disease during their lifetimes. If this as-sumption is incorrect, the cost advantage may dis-appear as it has been estimated that the cost oftreatment for one new case of metastatic prostatecancer is $70,000 (Littrup, Goodman and Mettlin,1993).
Another major advantage of surveillance for lo-calized prostate cancer is its avoidance of morbidityassociated with treatment. Most patients with newlydiagnosed prostate cancer, because of the currentpolicy of early detection and treatment, have nocancer-related symptoms at diagnosis. Surveillancewould allow these men to preserve their quality oflife. Conversely, radiotherapy and radical prostatec-tomy are associated with potential complicationsincluding erectile dysfunction, incontinence and in-jury to various organs from treatment (Fleming,Wasson, Albertsen, et al., 1993).
Finally, survival outcomes for at least 10 yearsare generally good. As summarized on page 19,available data suggest that the risk of metastaticdisease and prostate cancer death in patients man-aged with surveillance alone is not substantiallydifferent from the risk in patients treated for “cure.”A recent pooled analysis of six series of patients sotreated found excellent 10-year disease-specific sur-vivals for patients with well-differentiated andmoderately well-differentiated tumors (Chodak,Thisted, Gerber, et al., 1994). On the other hand,one study reported that the majority of patients onsurveillance who survive more than 10 years ulti-mately die of prostate cancer (Aus, Hugosson andNorlén, 1994).
Among the disadvantages of surveillance is therisk of subsequent, possibly incurable disease. Invirtually every series of patients managed by sur-veillance, some percentage of patients was reportedto have died of the disease and an additional groupwas reported to have suffered from disease-relatedmorbidity. In a pooled analysis, at 10 years of fol-low-up, 6 percent, 6.5 percent and 42 percent ofpatients with well-differentiated, moderately well-
Archived Document— For Reference Only
Page 41Copyright © 1995 American Urological Association, Inc.
differentiated and poorly differentiated tumors, re-spectively, died of their disease (Chodak, Thisted,Gerber, et al., 1994). Another study reported on 61patients with stages T1-T2 disease managed by sur-veillance. Of 8 who died during the period of ob-servation, 4 died of prostate cancer (Adolfsson andCarstensen, 1991).
Then there is the risk of developing disease-re-lated morbidity. The premise of “curative” treat-ment of carcinoma of the prostate is that it will pre-vent not only cancer-related death, but those com-plications related to the tumor that reduce thepatient’s quality of life. Patients managed with sur-veillance may be at a higher risk for such cancer-re-lated morbidities. Among these complications,spinal cord compression is a major concern. Thisevent can occur in as many as 12 percent of pa-tients with metastatic disease and can lead to deathas well as severe reductions in the patient’s qualityof life (Rubin, Lome and Presman, 1974). Whetherintervention at the time of diagnosis might preventsuch an outcome could not be predicted.
Other disease-related complications include pain,obstructive voiding symptoms, bone fracture ane-mia, ureteral obstruction, uremia, deep venousthrombosis and pulmonary embolism. In one paper,26 of 223 patients followed on a program of sur-veillance developed metastases (Johansson, Adami,Andersson, et al., 1992). Of these 26 patients, 23had a reduction in performance status. Of 19 pa-tients who died of prostate cancer, their perfor-mance status decreased for more than 6 months in12, and 13 patients required hospital care for 1month or more prior to death. Fourteen patients inthis series required hospital care for local problemsdue to their tumors. Of 152 patients who did notdevelop disease progression, 30 had mild or moder-ate local problems and 14 required transurethral re-section of the prostate. Of 71 patients who did de-velop local progression, 60 had local problems(which generally disappeared after treatment withhormone therapy). Twenty-eight of these 71 had re-current local problems during the course of theirdisease.
In summary, using surveillance as the primarymanagement of patients with locally confined pros-tate cancer may place a number of patients at risk
for various complications related to progression ofthe tumor.
As pointed out on page 20, patients who elect topursue a policy of surveillance are free to choose a“curative” intervention at any time during follow-up. However, if the goal for subsequent interventionis to time its application prior to the development ofextraprostatic disease, evidence indicates that thewindow of opportunity is very narrow. Data fromone report suggest that if serum PSA is measuredduring surveillance, once the value exceeds 5 ng/mlthe risk exceeds 50 percent that the disease is ex-traprostatic (Thompson, Zeidman, Crawford, et al.,1993).
Additional treatment may be needed. In virtuallyevery series of patients treated with surveillance forlocalized prostate cancer, the term “surveillance”included a variety of additional forms of treatment.Examples include a series of 122 patients (Adolfs-son, Carstensen and Lowhagen, 1992). Of these, 45percent received endocrine therapy (36 patients),external beam irradiation (12 patients),125I implan-tation (3 patients) or radical prostatectomy (4 pa-tients). In another series, treatment for local pro-gression was required for 23 of 120 patients(George, 1988).
It can be seen then that patients followed withsurveillance may be at risk for deferring treatmentto a later age and, by doing so, either deferring theside effects of treatment or, alternatively, losing theopportunity of disease control as well as undergo-ing invasive therapy at an age when comorbiditiesincrease.
A major unmeasured disadvantage to a policy ofsurveillance is the patient’s possible anxiety, hisfeeling that “nothing is being done about my pros-tate cancer.” Although the patient may intellectuallyunderstand the often confusing data supporting thevalidity of surveillance therapy, considerable anxi-ety can be generated in many patients and theirfamilies by a lack of intervention. The psychologicconsequences of cancer risk or diagnosis awarenessare well recognized, and clinicians practicing in thisfield are well aware of the overpowering dread thatcan be induced by worry about prostate cancer(Lerman, Miller, Scarborough, et al., 1991; Lerman,Rimer and Engstrom, 1991).
Archived Document— For Reference Only
Page 42 Copyright © 1995 American Urological Association, Inc.
The explicit methodology the AUA ProstateCancer Clinical Guidelines Panel used in its analy-sis for this Report on the Management of ClinicallyLocalized Prostate Cancerrequired careful reviewand interpretation of published reports in the peer-reviewed literature. As discussed in Chapter 1,many articles were reviewed and most were reject-ed for a variety of reasons, including inaccurate re-porting of data, limited time of follow-up, incom-plete description of treatments utilized and poorlydefined patient populations. Moreover, the studiesfinally selected for data extraction were not by anymeans free of deficiencies.
Data not based on randomizedcontrolled trials
All the studies finally selected by the panel pro-vided useful information, but most were case seriesnot subjected to the rigors of a carefully performed,prospective, centrally controlled clinical trial. Manyof the patient populations were “convenience sam-ples” selected mainly because they were availablein the clinical settings in which the research wasconducted.
The lack of randomized, controlled trials is aproblem inherent in the medical literature.Although it can be addressed and responded to, itcannot be avoided. Neither can it be dismissed. Thedifficulties this problem creates for developing evi-dence-based practice policy recommendations areespecially severe with regard to localized prostatecancer. Because of the particular attributes of thisdisease, such as high histologic prevalence, yetvariable natural history, treatment outcomes datafrom uncontrolled trials can be even less reliablethan usual.
Insufficient dataMany of the limitations in the literature stem di-
rectly from the previously mentioned plethora of
case series and lack of randomized controlled trials.These limitations include the large gaps that exist inthe literature regarding data reported. For example,many articles do not report all outcomes (such ascancer-specific survival, metastasis-free survivaland tumor-free survival). There are also few data onhigh-grade tumors in patients managed by surveil-lance, or on pelvic lymph node status in patientsmanaged by external beam radiotherapy as well assurveillance. In another very important example,many articles do not specify ages of patients not-withstanding the effect of age on survival and thesignificant differences in average patient age fordifferent treatment modalities. In still another ex-ample, many articles reporting complications fromtreatment do not report “zero complications.” Forinstance, an article may not refer to incontinence inits list of treatment-related complications. Readersare left to wonder whether the complication did notoccur or if it was omitted from the report.
Data variabilityData variability is one of the most frequent limi-
tations encountered when attempting to combineevidence from multiple studies. This variabilitytakes many forms with many causes. Variations be-tween studies because of differences in stagingmethods are one example. Some articles reviewedby the panel reported outcomes according to clini-cal stage, others according to surgical stage. Out-comes data from these two classes of articles arenot comparable.
Lymph node dissections performed for stagingvary between studies. Lymphadenectomy is typical-ly performed, but the panel could not substantiatethat all procedures reported in the literature werecomparable. Both extensive and limited dissectionswere carried out by different surgeons. In addition,although laparoscopic dissections are becomingmore commonplace, they were not included in thearticles selected.
Imaging studies are frequently utilized and arelimited not only by the state-of-the-art technology,but by the abilities of radiologists and urologists tointerpret a particular study. Laboratories vary aswell. Similar studies performed in different facilities,
Limitations in the prostatecancer treatment literature
Chapter 5:Literature limitations and recommendations for research
Archived Document— For Reference Only
Page 43Copyright © 1995 American Urological Association, Inc.
using different assays, could yield very different re-sults. Urologists and radiologists also differ. It can-not be assumed that a radiation technique or surgicalprocedure performed by one clinician is comparableto that performed by another.
As laboratories and imaging studies vary, so dopathology reports. Controlled trials often utilize acentral pathology facility, but comparing case seriesmeans comparing varied facilities. Differences existin preparation of histologic material, especiallywith the current emphasis on whole mount prostatepreparations. Yet, interpretations of extent of in-volvement and margin status are highly dependenton tissue preparation and subsequent pathologic in-terpretation, which makes comparisions betweenstudies problematic. Similar variations exist in theabilities of pathologists to grade malignancies. Al-though standards have been established, the subjec-tive component of these interpretations cannot beignored.
Patient populations differ as do the methods bywhich patients are selected for review. For instance,some clinical reports include consecutive patients,whereas many others are based upon informal se-lection factors such as availability for follow-up, re-ferral patterns and logistic concerns. Controlledstudies, because of strict inclusion and exclusioncriteria, may be preferable but may not be general-izable because of the carefully selected patients en-rolled. Means and ranges of follow-up often vary aswell. Such variations will not only have an impacton outcomes, but will influence any conclusions de-rived from the studies.
Because selection criteria between studies maydiffer, with variations in patient population, studiesperformed and methods of follow-up, comparisonsof studies may not be reliable. A common problemwith prostate cancer case series, for example, is thereporting of endocrine therapy for patients develop-ing recurrence after surgery or radiotherapy. Thetiming of administration, the form of therapy uti-lized and the method of reporting may not be clear-ly detailed, thus limiting the value of the report.Controlled prospective trials, by contrast, usuallyspecify from the outset the approach to be utilized.
Publication biasPublication bias is a problem affecting the avail-
able data to which there may be no immediate solu-tion. Very simply, because not all physicians pub-lish, case-study results may not be generally repre-
sentative. Moreover, studies with negative or equiv-ocal results are less likely to be submitted for publi-cation and less likely to be published if submitted.
Data limitations in reflectingcurrent techniques
The data available do not always reflect themany changes in treatment modalities that have oc-curred over the past two decades. For instance, ear-ly brachytherapy experience utilizing retropubicimplantation techniques with 131I and 198Au hadhigh failure rates. Newer methods, utilizing differ-ent isotopes (such as iridium) implanted perineallyunder ultrasound guidance, are being used with in-creasing frequency, but too few data are currentlyavailable to make efficacy comparisons.
Similarly, nerve-sparing techniques are being in-creasingly applied to radical prostatectomy. Yet, itmust be assumed that this modification has not hadany impact on survival or progression. In addition,the use of PSA to detect disease recurrence has al-tered the definition of treatment failure. Whetherconcepts regarding success and failure will nowchange because of the availability of this relativelyreliable marker is not known. Many questions re-main: Does PSA failure following radical prostatec-tomy or radiotherapy always indicate treatment fail-ure? What numeric criteria should be used to estab-lish PSA failure? What is its impact on survival?
Finally, new forms of therapy continue to evolve.Cryotherapy and other ablative techniques are beingdeveloped, but too few data are available to appro-priately assess success and failure in order to makemeaningful comparisons with other treatmentmodalities.
Most research needs can be grouped in three cat-egories: (1) new and better methods to diagnoseand manage localized prostate cancer; (2) prospec-tive, randomized, controlled studies of the issuesconcerning prostate cancer, especially controlledstudies of competing treatments for the manage-ment of localized prostate cancer; and (3) studies ofhow prostate cancer and its treatments affect patientquality of life.
Recommendations forfuture research
Archived Document— For Reference Only
Page 44 Copyright © 1995 American Urological Association, Inc.
Needs for new assessment andmanagement methods
Needs for new methods of cancer diagnosis andmonitoring include a more sensitive, more specifictumor indicator. As clinically useful as serum PSAvalues have now become, PSA is not prostate-can-cer specific. As a result, it lacks sufficient sensitivi-ty and specificity to be the ideal screening test forprostate cancer. In addition, although serum PSAconcentration correlates strongly with tumor vol-ume (r = 0.70), it cannot reliably predict tumorstage on an individual basis. Moreover, PSA afterandrogen deprivation therapy may not always be areliable indicator of the true tumor status becausethe cell’s ability to express PSA is under hormonalregulation, and androgen-insensitive cells do notproduce and secrete PSA to the same degree as an-drogen-sensitive cells. Patients with progressivedisease after androgen deprivation therapy may infact have a low or stable serum PSA concentration.
Needed also are biochemical, radiographicand/or genetic methods to reliably determine whichcancers are biologically aggressive and which areclinically insignificant, so that focused treatmentstrategies can be developed such that treatment isinitiated only in those patients with life-threateningprostate tumors.
For detecting potentially life-threatening cancerswhile still localized, it would be useful to have agenetic marker that can identify men likely to de-velop such a tumor in their lifetimes. These mencould then be monitored with appropriate, compre-hensive screening programs. Knowing who is atrisk for developing a clinically significant prostatecancer has tremendous potential not only to in-crease the probability of detecting prostate cancerwhile still organ confined, but to markedly decreasethe health care costs associated with unfocused ef-forts at prostate cancer detection.
Finally, with only 50 to 60 percent of newly di-agnosed prostate cancers currently organ confined,there is an overwhelming need for an effective sys-temic therapy for this disease. At the present time,no curative treatment exists for advanced prostatecancer. None of the currently available chemothera-peutic agents is effective, and androgen deprivationtherapy remains a palliative treatment for most pa-tients. New and creative approaches, such as genetherapy, need to be pursued both at the basic sci-ence level and in prospective clinical trials.
Recommendations for randomizedcontrolled trials
It is clear, from the discussions in this report oflimitations in the prostate cancer treatment litera-ture, that a pressing need exists for properly de-signed and controlled, prospective, randomizedclinical trials to study effectiveness of competingtreatment modalities for localized disease. In partic-ular, randomized, controlled trials are needed tocompare surveillance with the accepted active treat-ments.
Properly designed efficacy studies of treatmentmodalities will provide reliable descriptive data forthe patients studied. The descriptive factors shouldinclude age, tumor stage, tumor grade, ploidy, PSA,performance status and comorbidity, as well as costfactors and validated measures of quality of lifeover the course of a trial. End points measured in atrial should include risk of local recurrence, risk ofdisease progression (including objective measuresof symptoms associated with progression), risk ofmetastatic disease and risk of prostate cancer death.
Following are additional suggested study topicsfor each of the three major modalities:
• Radical prostatectomy: Methods of improv-ing preoperative staging, reducing the numberof patients with extraprostatic disease and re-ducing treatment complications; strategies toreduce the cost of the procedure; better waysto disseminate advances in surgical techniquesto the urologic community; treatments for pa-tients with pathologically proven (pT3) ex-traprostatic disease; and treatments for patientswith evidence of serologic (PSA) failure.
• Radiotherapy: Ways to reduce treatmentmorbidity; ways to standardize treatment; therole of conformal therapy and of radiosensitiz-ers; strategies to reduce the cost of treatment;optimal treatment at progression; mature dataon long-term follow-up of existing radiothera-py patients; stage-specific complications dataon existing series; and PSA and biopsy data.
• Surveillance: Optimal schedule of follow-upand optimal interventions at evidence of pro-gression.
Among the other topics and issues that need tobe addressed in rigorously designed clinical trialsare:
• New technologies for the treatment of clini-cally localized prostate cancer.
Archived Document— For Reference Only
Page 45Copyright © 1995 American Urological Association, Inc.
• Trade-offs between survival and quality oflife—including analysis of methods by whichpatients make treatment choices and the roleplayed by quality-of-life factors in thosechoices.
• Opportunities for chemoprevention of pros-tate cancer and dietary interventions, hor-monal therapy and retinoid therapy.
• New strategies for the use of hormonal treat-ments.
• Combined therapies for prostate cancer.• Development and validation of surrogate
measures of long-term prostate cancer out-comes (e.g.,validation of PSA failure as asurrogate for cancer survival).
Patient quality of lifeResearch is needed for determining how prostate
cancer and its treatments affect patient quality oflife. Such research would include the second topicin the foregoing list: analysis of trade-offs betweensurvival and quality of life and how quality-of-lifefactors affect patients’ treatment choices. Neededalso are improved methods for enhancing patient
involvement in a meaningful and efficient decision-making process and improved methods for provid-ing unbiased information to patients and physiciansabout emerging processes and outcomes of care.
Further research needsWith the increasing emphasis on efficient alloca-
tion of health care resources, it will be necessary todevelop methods to assess the costs related to treat-ment of prostate cancer. These include the costs ofearly detection, of treatment and of complicationsfrom treatment. It would be useful as well to beable to assess the financial impact of interventionon productive longevity and the costs related to dis-ability, long-term care and management of metasta-tic disease, and to compare these data with similardata regarding the financial impact of the disease it-self.
It would also be helpful for future research tohave a prostate cancer registry established for allprostate cancer cases in the United States. Informa-tion is now available from the Surveillance, Epi-demiology and End Results Program registry, butonly for a limited number of locations around thecountry.Archived Document—
For Reference Only
Page 46 Copyright © 1995 American Urological Association, Inc.
Adolfsson J, Carstensen J. Natural course of clinically local-ized prostate adenocarcinoma in men less than 70 years old. JUrol 1991;146:96-8.
Adolfsson J, Carstensen J, Lowhagen T. Deferred treatment inclinically localised carcinoma. Br J Urol 1992;69:183-7.
Adolfsson J, Tribukait B. Evaluation of tumor progression byrepeated fine needle biopsies in prostate adenocarcinoma:modal deoxyribonucleic acid value and cytological differenti-ation. J Urol 1990;144:1408-10.
American Academy of Family Physicians. AAFP Positions onthe Clinical Aspects of Medical Practice. Kansas City: Ameri-can Academy of Family Physicians, 1995.
Anderson L, Ling C. Radiobiophysical considerations in brach-ytherapy: temporal and spatial aspects (abstract). Presented atprostate symposium, prostate cancer: the role of interstitialimplantation. Seattle, Washington, 1991.
Asbell SO, Krall JM, Pilepich MV, Baerwald H, Sause WT,Hanks GE, Perez CA. Elective pelvic irradiation in stage A2,B carcinoma of the prostate: analysis of RTOG 77-06. Int JRadiat Oncol Biol Phys 1988; 15:1307-16.
Asbell SO, Martz KL, Pilepich MV, Baerwald HH, Sause WT,Doggett RL, Perez CA. Impact of surgical staging in evaluat-ing the radiotherapeutic outcome in RTOG phase III study forA2 and B prostate carcinoma. Int J Radiat Oncol Biol Phys1989;17:945-51.
Aus G, Hugosson J, Norlén L. Risk of dying of prostate cancerin different stages, grades and age at diagnosis. J Urol 1994;151:278A.
Bagshaw MA. Radiotherapeutic treatment of prostatic carcino-ma with pelvic node involvement. Urol Clin N Amer 1984;11:297-304.
Beahrs OH, Henson DE, Hutter RVP, Kennedy BJ, eds.Manual for staging of cancer, 4th ed. American JointCommittee on Cancer. Philadelphia: J.B. Lippincott, 1992.280 p.
Beck JR, Kattan MW, Miles BJ. A critique of the decisionanalysis for clinically localized prostate cancer. J Urol 1994;152:1894-9.
Bertermann H, et al. Iridium-192: Five years experience withinterstitial high dose brachy- and external teletherapy in lo-cally confined prostate cancer. Presented at prostate sympo-sium, prostate cancer: the role of interstitial implantation,Seattle, Washington, 1991.
Blasko JC, Ragde H, Grimm PD. Transperineal ultrasound-guided implantation of the prostate: morbidity and complica-tions. Scand J Urol Nephrol Suppl 1991;137:113-8.
Bluestein DL, Bostwick DG, Bergstralh EJ, Oesterling JE.Eliminating the need for bilateral pelvic lymphadenectomy inselect patients with prostate cancer. J Urol 1994;151:1315-20.
Bosch PC, Forbes KA, Prassvinichai S, Miller JB, Golji H,Martin DC. Preliminary observations on the results of com-bined temporary 192Iridium implantation and external beamirradiation for carcinoma of the prostate. J Urol1986;135:722-5.
Brawer MK, Chetner MP, Beatie J, Buchner DM, Vessella RL,Lange PH. Screening for prostatic carcinoma with prostatespecific antigen. J Urol 1992;147:841-5.
Brendler CB, Carmichael M, Walsh PC, Epstein JI. Radicalprostatectomy (RP) for non-palpable prostate cancer diag-nosed by needle biopsy: pathologic and clinical findings. JUrol 1993;149:378A.
Carey PO, Lippert MC, Constable WC, Jones D, Talton BM.Combined gold seed implantation and external radiotherapyfor stage B2 or C prostate cancer. J Urol 1988;139:989-94.
Carter HB, Coffey DS. The prostate: an increasing medicalproblem. Prostate 1990;16:39-48.
Catalona WJ, Bigg SW. Nerve-sparing radical prostatectomy:evaluation of results after 250 patients. J Urol 1990;143:538-44.
Catalona WJ, Smith DS, Ratliff TL, Basler JW. Detection oforgan-confined prostate cancer is increased through prostate-specific antigen-based screening. JAMA 1993;270:948-54.
Catalona WJ, Smith DS, Ratliff TL, Dodds KM, Coplen DE,Yuan JJ, Petros JA, Andriole GL. Measurement of prostate-specific antigen in serum as a screening test for prostate can-cer. N Engl J Med 1991; 324:1156-61.
Chodak GW, Thisted RA, Gerber GS, Johansson J-E,Adolfsson J, Jones GW, Chisholm GD, Moskovitz B, LivnePM, Warner J. Results of conservative management of clini-cally localized prostate cancer. N Engl J Med 1994;330:242-8.
Chybowski FM, Larson-Keller JJ, Bergstralh EJ, Oesterling JE.Predicting radionuclide bone scan findings in patients withnewly diagnosed, untreated prostate cancer: prostate-specificantigen is superior to all other clinical parameters. J Urol1991;145:313-8.
Cooner WH, Mosley BR, Rutherford CL Jr, Beard JH, PondHS, Terry WJ, Igel TC, Kidd DD. Prostate cancer detection ina clinical urological practice by ultrasonography, digital rectalexamination and prostate specific antigen. J Urol 1990;143:1146-54.
Dale RG. The application of the linear-quadratic dose-effectequation to fractionated and protracted radiotherapy. Br JRadiol 1985;58:515-28.
Danella JF, deKernion JB, Smith RB, Steckel J. The contempo-rary incidence of lymph nodes metastases in prostate cancer:implications for laparoscopic lymph node dissection. J Urol1993;149:1488-91.
References*
_________________*Includes articles cited in text. See Table A-1 in Appendix A for a complete listing of articles extracted for analysis.
Archived Document— For Reference Only
Page 47Copyright © 1995 American Urological Association, Inc.
Daniels GF Jr, McNeal JE, Stamey TA. Predicted value of con-tralateral biopsies in unilaterally palpable prostate cancer. JUrol 1992;147:870-4.
Donohue RE, Mani JH, Whitesel JA, Augspurger RR, WilliamsG, Fauver HE. Intraoperative and early complications of stag-ing pelvic lymph node dissection in prostatic adenocarcino-ma. Urology 1990; 35:223-7.
Duncan W, Warde P, Catton CN, Munro AJ, Lakier R, GadallaT, Gospodarowicz MK. Carcinoma of the prostate: results ofradical radiotherapy (1970-1985). Int J Radiat Oncol BiolPhys 1993;26:203-10.
Eddy DM. A manual for assessing health practices & designingpractice policies: the explicit approach. Philadelphia:American College of Physicians, 1992. 126 p.
Epstein BE, Hanks GE. Radiation therapy techniques and doseselection in the treatment of prostate cancer. Semin RadiatOncol 1993;3:179-86.
Epstein JI, Walsh PC, Carmichael M, Brendler CB. Pathologicand clinical findings to predict tumor extent of nonpalpable(stage T1c) prostate cancer. JAMA 1994;271:368-74.
Fleming C, Wasson JH, Albertsen PC, Barry MJ, Wennberg JE,for the Prostate Patient Outcomes Research Team. A decisionanalysis of alternative treatment strategies for clinically local-ized prostate cancer. JAMA 1993;269:2650-8.
Forman JD, Zinreich E, Lee D-J, Wharam MD, BaumgardnerRA, Order SE. Improving the therapeutic ratio of externalbeam irradiation for carcinoma of the prostate. Int J RadiatOncol Biol Phys 1985;11:2073-80.
Fowler FJ, Barry MJ, Lu-Yao G, Roman A, Wasson J, Wenn-berg JE. Patient-reported complications and follow-up treat-ment after radical prostatectomy. Urology 1993;42:622-9.
Fowler J. The linear-quadratic formula and progress in frac-tionated radiotherapy. Br J Radiol 1989;62:679-94.
Fowler J. The radiobiology of brachytherapy: dose rate effectsof iodine palladium and iridium (abstract). Presented at pros-tate symposium, prostate cancer: the role of interstitial im-plantation, Seattle, Washington, 1991.
Fowler JE, Barzell W, Hilaris BS, Whitmore WF.Complications of 125Iodine implantation and pelvic lym-phadenectomy in the treatment of prostatic cancer. J Urol1979;121:447-51.
Franks LM. Latent carcinoma of the prostate. J Path Bact1954; 68:603-16.
Fuks Z, Leibel SA, Wallner KE, Begg CB, Fair WR, AndersonLL, Hilaris BS, Whitmore WF. The effect of local control onmetastatic dissemination in carcinoma of the prostate: long-term results in patients treated with 125I implantation. Int JRadiat Oncol Biol Phys 1991; 21:537-47.
George NJR. Natural history of localised prostatic cancer man-aged by conservative therapy alone. Lancet 1988;1:494-7.
Gibbons RP. Localized prostate carcinoma: surgical manage-ment. Cancer 1993;72:2865-72.
Gibbons RP, Correa RJ Jr, Brannen GE, Weissman RM. Totalprostatectomy for clinically localized prostate cancer: long-term results. J Urol 1989;141:564-6.
Giles GM, Brady LW. 125Iodine implantation after lymphaden-ectomy in early carcinoma of the prostate. Int J Radiat OncolBiol Phys 1986; 12:2117-25.
Gleason DF. Veterans Administration Cooperative UrologicalResearch Group. Histologic grading and staging of prostaticcarcinoma. In: Tannenbaum M, ed. Urologic pathology: theprostate. Philadelphia: Lea and Febiger, 1977:171-98.
Glick AJ, Philput CB, El-Mahdi AM, Ladaga LE, Schell-hammer PF. Are three substages of clinical B prostate carci-noma useful in predicting disease-free survival? Urology1990; 36:483-7.
Gore RM, Moss AA. Value of computed tomography in inter-stitial 125I brachytherapy of prostatic carcinoma. Radiology1983;146:453-8.
Green N, Goldberg H, Goldman H, Lombardo L, Skaist L.Severe rectal injury following radiation for prostatic cancer. JUrol 1984;131:701-4.
Hanks GE. Treatment of early stage prostate cancer: radiother-apy. American Society for Therapeutic Radiology andOncology spring program, refresher course, 1994.
Hanks GE, Krall JM, Pilepich MV, Asbell SO, Perez CA,Rubin P, Sause WT, Doggett RLS. Comparison of pathologicand clinical evaluation of lymph nodes in prostate cancer: im-plications of RTOG data for patient management and trial de-sign and stratification. Int J Radiat Oncol Biol Phys1992;23:293-8.
Hanks GE, Perez CA, Kozar MB, et al. Prostatic specific anti-gen confirmation of long-term cure of prostate cancer treatedby external beam radiation in the RTOG. Proc 35th Ann AS-TRO Meeting 1993;27:192.
Iversen P, Bak M, Juul N, Laursen F, von der Maase H, NielsenL, Rasmussen F, Torp-Pedersen S, Holm HH. Ultrasonicallyguided 125Iodine seed implantation with external radiation inmanagement of localized prostatic carcinoma. Urology 1989;34:181-6.
Johansson J-E, Adami HO, Andersson SO, Bergstrom R,Holmberg L, Krusemo UB. High 10-year survival rate in pa-tients with early, untreated prostatic cancer. JAMA 1992;267:2191-6.
Jones GW. Prospective, conservative management of localizedprostate cancer. Cancer 1992;70:Suppl:307-10.
Kabalin JN, Hodge KK, McNeal JE, Freiha FS, Stamey TA.Identification of residual cancer in the prostate following ra-diation therapy: role of transrectal ultrasound guided biopsyand prostate specific antigen. J Urol 1989;142:326-31.
Kandzari SJ, Belis JA, Kim J-C, Gnepp DR, Riley RS. Clinicalresults of early stage prostatic cancer treated by pelviclymphadenectomy and 125Iodine implants. J Urol1982;127:923-7.
Kaplan ID, Prestidge BR, Bagshaw MA, Cox RS. The impor-tance of local control in the treatment of prostatic cancer. JUrol 1992;147:917-21.
Kavoussi LR, Sosa E, Chandhoke P, Chodak G, Clayman RV,Hadley HR, Loughlin KR, Ruckle HC, Rukstalis D,Schuessler W, Segura J, Vancaille T, Winfield HN.Complications of laparoscopic pelvic lymph node dissection.J Urol 1993;149:322-5.
Kiesling VJ, McAninch JW, Goebel JL, Agee RE. Externalbeam radiotherapy for adenocarcinoma of the prostate: a clin-ical follow-up. J Urol 1980;124:851-4.
Koch MO, Smith JA Jr, Hodge EM, Brandell RA. Prospectivedevelopment of a cost-efficient program for radical retropubicprostatectomy. Urology 1994;44:311-8.
Archived Document— For Reference Only
Page 48 Copyright © 1995 American Urological Association, Inc.
Kuban DA, El-Mahdi AM, Schellhammer PF. 125I interstitialimplantation for prostate cancer: what have we learned 10years later? Cancer 1989a;63:2415-20.
Kuban DA, El-Mahdi AM, Schellhammer PF. Prognosis in pa-tients with local recurrence after definitive irradiation for pro-static carcinoma. Cancer 1989b;63:2421-5.
Labrie F, Dupont A, Suburu R, Cusan L, Tremblay M, GomezJL, Emond J. Serum prostate specific antigen as a pre-screen-ing test for prostate cancer. J Urol 1992;147:846-52.
Landmann C, Hunig R. Prostatic specific antigen as an indica-tor of response to radiotherapy in prostate cancer. Int J RadiatOncol Biol Phys 1989;17:1073-6.
Lawton CA, Won M, Pilepich MV, Asbell SO, Shipley WU,Hanks GE, Cox JD, Perez CA, Sause WT, Doggett SR, RubinP. Long-term treatment sequelae following external beam ir-radiation for adenocarcinoma of the prostate: analysis ofRTOG studies 7506 and 7706. Int J Radiat Oncol Biol Phys1991; 21:935-9.
Lerman C, Miller SM, Scarborough R, Hanjani P, Nolte S,Smith D. Adverse psychologic consequences of positive cyto-logic cervical screening. Am J Obstet Gynecol 1991;165:658-62.
Lerman C, Rimer BK, Engstrom PF. Cancer risk notification:psychosocial and ethical implications. J Clin Oncol 1991;9:1275-82.
Littrup PJ, Goodman AC, Mettlin CJ. The benefit and cost ofprostate cancer early detection. The Investigators of theAmerican Cancer Society-National Prostate Cancer DetectionProject. CA Cancer J Clin 1993;43:134-49.
Lue TF, Carroll PR, Moore C. Treatment of impotence in can-cer patients. In Important Advances in Oncology. DeVita VTJr, Hellman S, Rosenberg SA, eds. Philadelphia: J.B.Lippincott, 1989: 193-203.
Lu-Yao GL, McLerran D, Wasson J, Wennberg JE, for theProstate Patient Outcomes Research Team. An assessment ofradical prostatectomy: time trends, geographic variation, andoutcomes. JAMA 1993;269:2633-6.
Madsen PO, Graversen PH, Gasser TC, Corle DK. Treatmentof localized prostatic cancer: radical prostatectomy versusplacebo: a 15-year follow-up. Scand J Urol Nephrol Suppl1988; 110:95-100.
Mameghan H, Fisher R, Mameghan J, Watt WH, Tynan A.Bowel complications after radiotherapy for carcinoma of theprostate: the volume effect. Int J Radiat Oncol Biol Phys1990; 18:315-20.
Marks LB, Anscher MS. Radiotherapy for prostate cancer:should the seminal vesicles be considered target? Int J RadiatOncol Biol Phys 1992;24:435-40.
McGowan DG. The value of extended field radiation therapy incarcinoma of the prostate. Int J Radiat Oncol Biol Phys 1981;7:1333-9.
McNeal JE, Villers AA, Redwine EA, Freiha FS, Stamey TA.Histologic differentiation, cancer volume, and pelvic lymphnode metastasis in adenocarcinoma of the prostate. Cancer1990; 66:1225-33.
Mettlin C, Jones GW, Murphy GP. Trends in prostate cancercare in the United States, 1974-1990: observations from thepatient care evaluation studies of the American College ofSurgeons Commission on Cancer. CA Cancer J Clin 1993;43:83-91.
Miller BA, Hayes RB, Potosky AL, Brawley O, Kaplan R.Prostate. In SEER Cancer Statistics Review, 1973-1990. Na-tional Institutes of Health, National Cancer Institute, NIHPublication No. 93-2789, 1993:XXII,1-15.
Morton JD, Peschel RE. Iodine-125 implants versus externalbeam therapy for stages A2, B, and C prostate cancer. Int JRadiat Oncol Biol Phys 1988;14:1153-7.
Morton RA, Steiner MS, Walsh PC. Cancer control followinganatomical radical prostatectomy: an interim report. J Urol1991;145:1197-200.
Mukamel E, deKernion JB, Hannah J, Smith RB, Skinner DG,Goodwin WE. The incidence and significance of seminalvesicle invasion in patients with adenocarcinoma of the pros-tate. Cancer 1987;59:1535-8.
Murphy GP, Natarajan N, Pontes JE, Schmitz RL, Smart CR,Schmidt JD, Mettlin C. The national survey of prostate can-cer in the United States by the American College ofSurgeons. J Urol 1982;127:928-34.
National Institutes of Health Consensus Development Panel.Consensus development conference on the management ofclinically localized prostate cancer. National Cancer InstituteMonographs, No 7. NIH Publication No. 88-3005, 1988:1-183.
Oesterling JE, Brendler CB, Epstein JI, Kimball AW, WalshPC. Correlation of clinical stage, serum prostatic acid phos-phatase and preoperative Gleason grade with final pathologi-cal stage in 275 patients with clinically localized adenocarci-noma of the prostate. J Urol 1987; 138:92-8.
Oesterling JE, Martin SK, Bergstralh EJ, Lowe FC. The use ofprostate-specific antigen in staging patients with newly diag-nosed prostate cancer. JAMA 1993;269:57-60.
Oesterling JE, Suman VJ, Zincke H, Bostwick DG. PSA-de-tected (clinical stage T1c or B0) prostate cancer.Pathologically significant tumors. Urol Clin N Am1993;20:687-93.
Paulson DF, Moul JW, Walther PJ. Radical prostatectomy forclinical stage T1-2NOMO prostatic adenocarcinoma: long-term results. J Urol 1990;144;1180-4.
Perez CA, Garcia D, Simpson JR, Zivnuska F, Lockett MA.Factors influencing outcome of definitive radiotherapy for lo-calized carcinoma of the prostate. Radiother Oncol1989;16:1-21.
Petros JA, Catalona WJ. Lower incidence of unsuspectedlymph node metastases in 521 consecutive patients with clini-cally localized prostate cancer. J Urol 1992;147:1574-5.
Pilepich MV, Krall JM, Johnson RJ, Sause WT, Perez CA,Zinninger M, Martz K. Extended field (periaortic) irradiationin carcinoma of the prostate: analysis of RTOG 75-06. Int JRadiat Oncol Biol Phys 1986; 12:345-51.
Pilepich MV, Krall JM, Sause WT, Johnson RJ, Russ HH,Hanks GE, Perez CA, Zinninger M, Martz KL, Gardner P.Correlation of radiotherapeutic parameters and treatment re-lated morbidity in carcinoma of the prostate: analysis ofRTOG study 75-06. Int J Radiat Oncol Biol Phys1987;13:351-7.
Pisansky TM, Cha SS, Earle JD, Durr ED, Kozelsky TF,Wieand HS, Oesterling JE. Prostate-specific antigen as a pre-therapy prognostic factor in patients treated with radiationtherapy for clinically localized prostate cancer. J Clin Oncol1993;11:2158-66.
Archived Document— For Reference Only
Page 49Copyright © 1995 American Urological Association, Inc.
Prout GR Jr. Diagnosis and staging of prostatic carcinoma.Cancer 1973;32:1096-103.
Rana A, Chisholm GD, Christodoulou S, McIntyre MA, EltonRA. Audit and its impact in the management of early prostat-ic cancer. Br J Urol 1993;71:721-7.
Rifkin MD, Zerhouni EA, Gatsonis CA, Quint LE, PaushterDM, Epstein JI, Hamper U, Walsh PC, McNeil BJ. Compari-son of magnetic resonance imaging and ultrasonography instaging early prostate cancer. Results of multi-institutionalcooperative trial. N Engl J Med 1990;323:621-6.
Rubin H, Lome LG, Presman D. Neurological manifestation ofmetastatic prostatic carcinoma. J Urol 1974;111:799-802.
Russell KJ, Dunatov C, Hafermann MD, Griffeth JT, PolissarL, Pelton J, Cole SB, Taylor EW, Wiens LW, Koh WJ,Austin-Seymour MM, Griffin BR, Russell AH, Laramore GE,Griffin TW. Prostate specific antigen in the management ofpatients with localized adenocarcinoma of the prostate treatedwith primary radiation therapy. J Urol 1991; 146:1046-52.
Sakr WA, Haas GP, Cassin BF, Pontes JE, Crissman JD. Thefrequency of carcinoma and intraepithelial neoplasia of theprostate in young male patients. J Urol 1993;150:379-85.
Scaletscky R, Koch MO, Eckstein CW, Smith JA Jr. Pathologicfindings in prostate cancer detected because of PSA eleva-tion. J Urol 1993; 149:303A.
Schellhammer PF, El-Mahdi AM, Higgins EM, Schultheiss TE,Ladaga LE, Babb TJ. Prostate biopsy after definitive treat-ment by interstitial 125Iodine implant or external beam radia-tion therapy. J Urol 1987; 137:897-901.
Schellhammer PF, Whitmore RB III, Kuban DA, El-MahdiAM, Ladaga LA. Morbidity and mortality of local failure af-ter definitive therapy for prostate cancer. J Urol1989;141:567-71.
Singer PA, Tasch ES, Stocking C, Rubin S, Siegler M,Weichselbaum R. Sex or survival: trade-offs between qualityand quantity of life. J Clin Oncol 1991;9:328-34.
Smalley SR, Noble MJ. Prostate brachytherapy. Part I: tech-nique, radiophysical considerations, and biology. Part II: clin-ical results complications, and salvage therapy. AUA UpdateSeries; 1992: 258-72.
Smit WGJM, Helle PA, van Putten WLJ, Wijnmaalen AJ, Sel-denrath JJ, van der Werf Messing BHP. Late radiation dam-age in prostate cancer patients treated by high dose externalradiotherapy in relation to rectal dose. Int J Radiat Oncol BiolPhys 1990;18:23-9.
Sogani PC, DeCosse JJ, Montie J, Whitmore WF, Grabstald H,Hilaris BS. Carcinoma of the prostate: treatment with pelviclymphadenectomy and iodine-125 implants. Clin Bull1979;9:24-31.
Sommerkamp H, Rupprecht M, Wannenmacher M. Seed loss ininterstitial radiotherapy of prostatic carcinoma with I-125. IntJ Radiat Oncol Biol Phys 1988;14:389-92.
Stamey TA, Ferrari MK, Schmid HP. The value of serial pros-tate specific antigen determinations 5 years after radiothera-py: steeply increasing values characterize 80% of patients. JUrol 1993;150:1856-9.
Stamey TA, McNeal JE. Adenocarcinoma of the prostate. InCampbell’s Urology, 6th ed. Walsh PC, Retik AB, StameyTA, Vaughan ED Jr, eds. Philadelphia: W.B. SaundersCompany; 1992:Chapter 29,1159-221.
Stamey TA, McNeal JE, Freiha FS, Redwine E. Morphometricand clinical studies on 68 consecutive radical prostatec-tomies. J Urol 1988;139:1235-41.
Stein A, deKernion JB, Smith RB, Dorey F, Patel H. Prostatespecific antigen levels after radical prostatectomy in patientswith organ confined and locally extensive prostate cancer. JUrol 1992;147:942-6.
Steinfeld AD, Donahue BR, Plaine L. Pulmonary embolizationof iodine-125 seeds following prostate implantation. Urology1991;37:149-50.
Stenzl A, Studer UE. Outcome of patients with untreated can-cer of the prostate. Eur Urol 1993;24:1-6.
Stone NN, Forman JD, Sogani PC, Hilaris BS, Whitmore WF,Fair WR. Transrectal ultrasonography and 125I implantation inpatients with prostate cancer. J Urol 1988;139:313A.
Stormont TJ, Farrow GM, Myers RP, Blute ML, Zincke H,Wilson TM, Oesterling JE. Clinical stage Bo or T1c prostatecancer: nonpalpable disease identified by elevated serumprostate-specific antigen concentration. Urology 1993;41:3-8.
Thompson IM, Zeidman EJ, Crawford ED, Sagalowsky AI,Schellhammer PF, deVere White RW, Grossman HB, Klein E,Lowe BA, Bueschen AJ, Scardino PT, Flanigan RC. In theera of prostate specific antigen (PSA), is prostate acid phos-phatase (PAP) necessary for staging prostate cancer? ASouthwest Oncology Group (SWOG) study. J Urol 1993;149:303A.
Waaler G, Stenwig AE. Prognosis of localised prostatic cancermanaged by “watch and wait” policy. Br J Urol 1993;72:214-9.
Wahle S, Reznicek M, Fallon B, Platz C, Williams R.Incidence of surgical margin involvement in various forms ofradical prostatectomy. Urology 1990;36:23-6.
Walsh PC. Radical retropubic prostatectomy. In Campbell’sUrology, 6th ed. Walsh PC, Retik AB, Stamey TA, VaughanED Jr, eds. Philadelphia: WB Saunders Company; 1992:Chapter 78,2865-86.
Walsh PC. Radical retropubic prostatectomy with reduced mor-bidity: an anatomic approach. NCI Monographs No. 7 1988:133-7.
Wasson J, Cushman C, Bruskewitz RC, Littenberg B, MulleyAG, Wennberg JE, for the Prostate Patient OutcomesResearch Team. A structured literature review of treatmentfor localized prostate cancer. Arch Fam Med 1993;2:487-93.
Weldon VE, Tavel FR. Potency-sparing radical perineal prosta-tectomy: anatomy, surgical technique, and initial results. JUrol 1988;140:559-62.
Whitmore WF Jr. Conservative approaches to the managementof localized prostatic cancer. Cancer 1993;71:970-5.
Whitmore WF Jr, Warner JA, Thompson IM Jr. Expectant man-agement of localized prostate cancer. Cancer 1991;67:1091-6.
Wingo PA, Tong T, Bolden S. Cancer Statistics, 1995. CACancer J Clin 1995;45:8-30.
Zagars GK, von Eschenbach AC. Prostate-specific antigen: animportant marker for prostate cancer treated by external beamradiation therapy. Cancer 1993;72:538-48.
Archived Document— For Reference Only
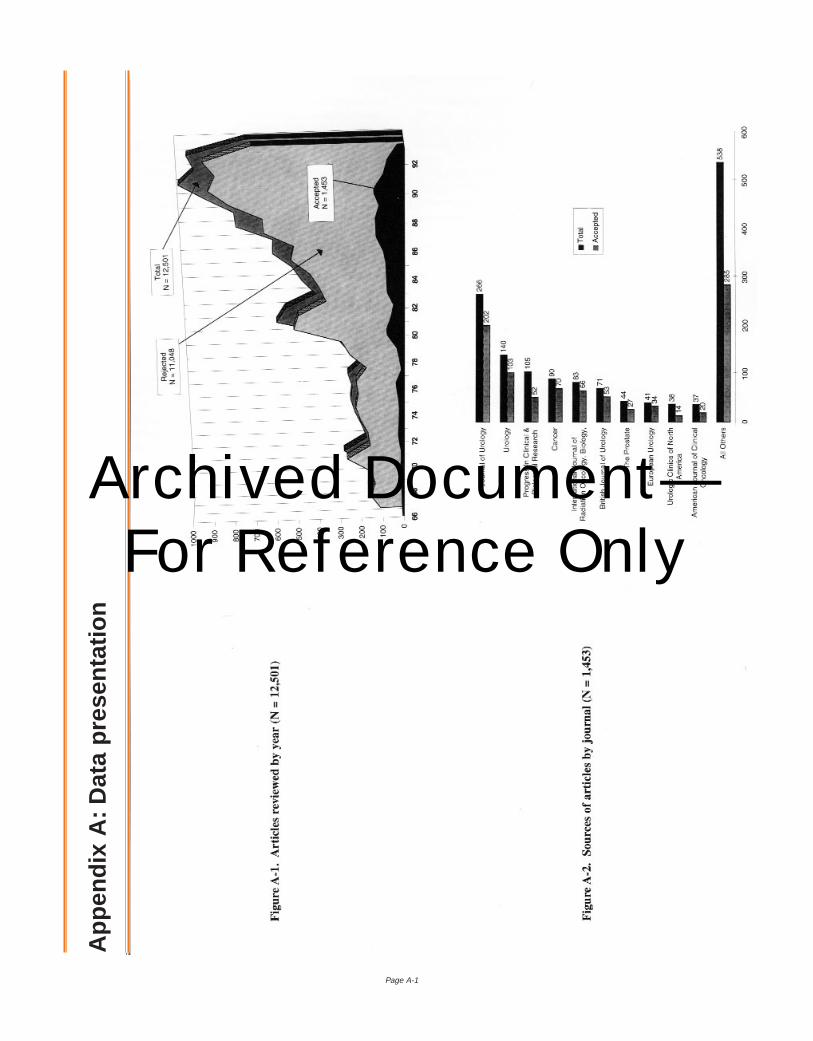
Page A-1
App
endi
x A
:Dat
a pr
esen
tatio
n
Archived Document— For Reference Only
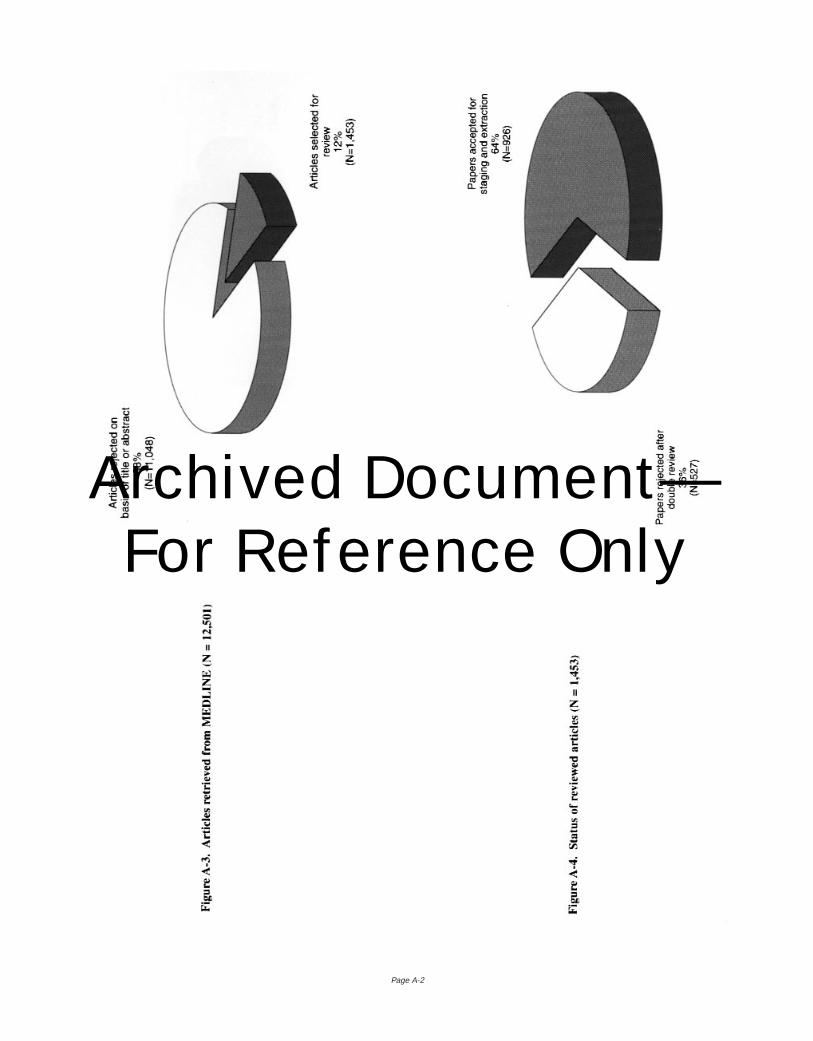
Page A-2
Archived Document— For Reference Only
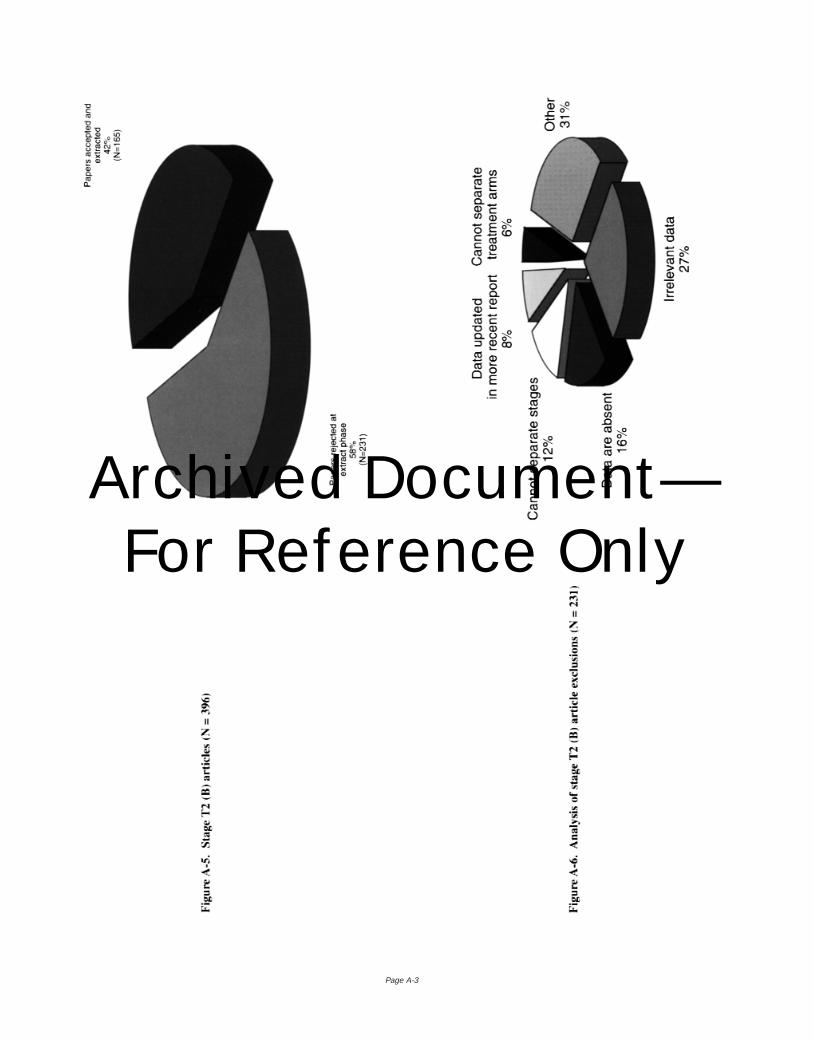
Page A-3
Archived Document— For Reference Only
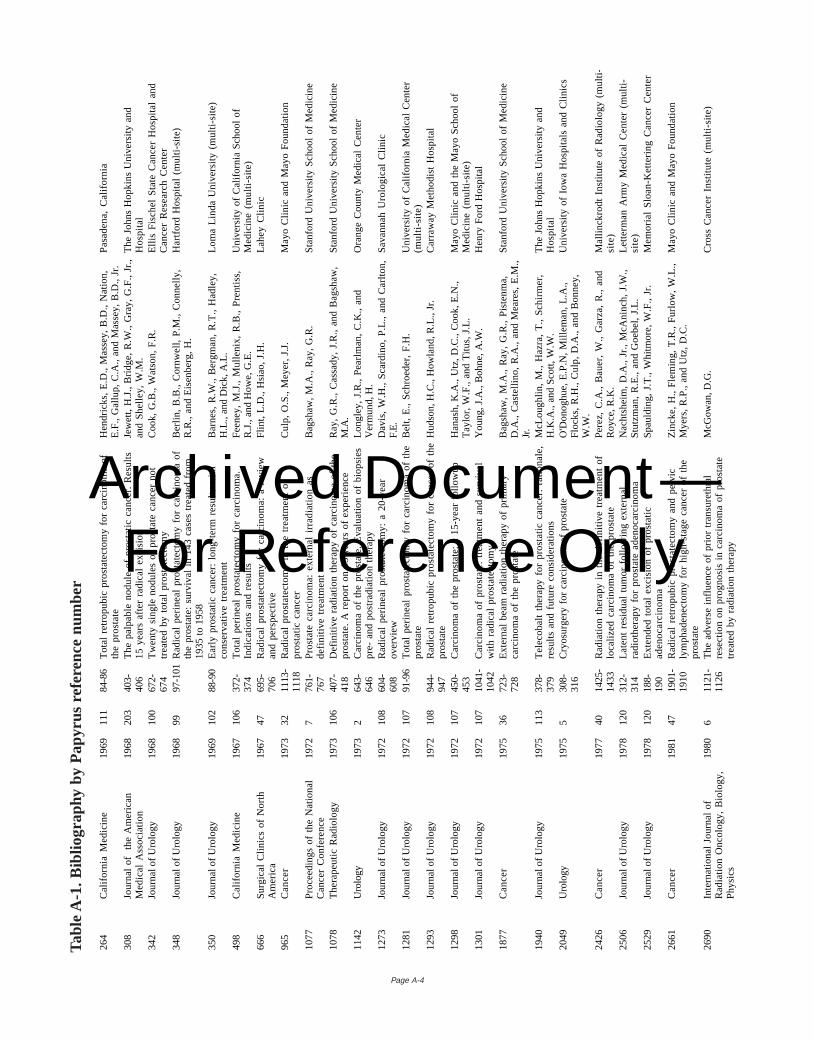
Page A-4
264
Ca
lifo
rnia
Me
dic
ine
1969
111
84-8
6T
ota
l re
tro
pu
bic
pro
sta
tect
om
y fo
r ca
rcin
om
a o
fth
e p
rost
ate
He
nd
rick
s, E
.D.,
Ma
sse
y, B
.D.,
Na
tion
,E
.F.,
Ga
llup
, C
.A.,
an
d M
ass
ey,
B.D
., J
r.Pa
sad
en
a,
Ca
lifo
rnia
308
Jou
rna
l o
f t
he
Am
eri
can
Me
dic
al
Ass
oci
atio
n19
6820
340
3-40
6T
he
pa
lpa
ble
no
du
le o
f p
rost
atic
ca
nce
r. R
esu
lts1
5 y
ea
rs a
fte
r ra
dic
al
exc
isio
nJe
we
tt,
H.J
., B
rid
ge
, R
.W.,
Gra
y, G
.F.,
Jr.
,a
nd
Sh
elle
y, W
.M.
Th
e J
oh
ns
Ho
pki
ns
Un
ive
rsity
an
dH
osp
ital
342
Jour
nal o
f U
rolo
gy19
6810
067
2-67
4T
we
nty
sin
gle
no
du
les
of
pro
sta
te c
an
cer
no
ttr
ea
ted
by
tota
l p
rost
ate
cto
my
Co
ok,
G.B
., W
ats
on
, F
.R.
Elli
s F
isch
el
Sta
te C
an
cer
Ho
spita
l a
nd
Ca
nce
r R
ese
arc
h C
en
ter
348
Jour
nal o
f U
rolo
gy19
6899
97-1
01R
ad
ica
l p
eri
ne
al
pro
sta
tect
om
y fo
r ca
rcin
om
a o
fth
e p
rost
ate
: su
rviv
al
in 1
43
ca
ses
tre
ate
d f
rom
19
35
to
19
58
Be
rlin
, B
.B.,
Co
rnw
ell,
P.M
., C
on
ne
lly,
R.R
., a
nd
Eis
en
be
rg,
H.
Ha
rtfo
rd H
osp
ital
(mu
lti-s
ite)
350
Jour
nal o
f U
rolo
gy19
6910
288
-90
Ea
rly
pro
sta
tic c
an
cer:
lo
ng
-te
rm r
esu
lts w
ithco
nse
rva
tive
tre
atm
en
tB
arn
es,
R.W
., B
erg
ma
n,
R.T
., H
ad
ley,
H.L
., an
d D
ick,
A.L
.L
om
a L
ind
a U
niv
ers
ity (
mu
lti-s
ite)
498
Ca
lifo
rnia
Me
dic
ine
1967
106
372-
374
To
tal
pe
rin
ea
l p
rost
ate
cto
my
for
carc
ino
ma
.In
dic
atio
ns
an
d r
esu
ltsF
ee
ne
y, M
.J.,
Mu
llen
ix,
R.B
., P
ren
tiss,
R.J
., an
d H
owe,
G.E
.U
niv
ers
ity o
f C
alif
orn
ia S
cho
ol
of
Me
dic
ine
(m
ulti
-site
)66
6S
urg
ica
l C
linic
s o
f N
ort
hA
me
rica
1967
4769
5-70
6R
ad
ica
l p
rost
ate
cto
my
for
carc
ino
ma
: a
re
vie
wa
nd
pe
rsp
ect
ive
Flin
t, L
.D.,
Hsi
ao
, J.
H.
La
he
y C
linic
965
Ca
nce
r19
7332
1113
-11
18R
ad
ica
l p
rost
ate
cto
my
in t
he
tre
atm
en
t o
fp
rost
atic
ca
nce
rC
ulp
, O
.S.,
Me
yer,
J.J
.M
ayo
Clin
ic a
nd
Ma
yo F
ou
nd
atio
n
1077
Pro
cee
din
gs
of
the
Na
tion
al
Ca
nce
r C
on
fere
nce
1972
776
1-76
7P
rost
ate
ca
rcin
om
a:
ext
ern
al
irra
dia
tion
as
de
finiti
ve t
rea
tme
nt
Ba
gsh
aw
, M
.A.,
Ra
y, G
.R.
Sta
nfo
rd U
niv
ers
ity S
cho
ol
of
Me
dic
ine
1078
Th
era
pe
utic
Ra
dio
log
y19
7310
640
7-41
8D
efin
itive
ra
dia
tion
th
era
py
of
carc
ino
ma
of
the
pro
sta
te.
A r
ep
ort
on
15
ye
ars
of
exp
eri
en
ceR
ay,
G.R
., C
ass
ad
y, J
.R.,
an
d B
ag
sha
w,
M.A
.S
tan
ford
Un
ive
rsity
Sch
oo
l o
f M
ed
icin
e
1142
Uro
logy
1973
264
3-64
6C
arc
ino
ma
of
the
pro
sta
te.
Eva
lua
tion
of
bio
psi
es
pre
- a
nd
po
stra
dia
tion
th
era
py
Lo
ng
ley,
J.R
., P
ea
rlm
an
, C
.K.,
an
dV
erm
und,
H.
Ora
ng
e C
ou
nty
Me
dic
al
Ce
nte
r
1273
Jour
nal o
f U
rolo
gy19
7210
860
4-60
8R
ad
ica
l p
eri
ne
al
pro
sta
tect
om
y: a
20
-ye
ar
ove
rvie
wD
avi
s, W
.H.,
Sca
rdin
o,
P.L
., a
nd
Ca
rlto
n,
F.E
.S
ava
nn
ah
Uro
log
ica
l C
linic
1281
Jour
nal o
f U
rolo
gy19
7210
791
-96
To
tal
pe
rin
ea
l p
rost
ate
cto
my
for
carc
ino
ma
of
the
pro
sta
teB
elt,
E.,
Sch
roe
de
r, F
.H.
Un
ive
rsity
of
Ca
lifo
rnia
Me
dic
al
Ce
nte
r(m
ulti
-site
)12
93Jo
urna
l of
Uro
logy
1972
108
944-
947
Ra
dic
al
retr
op
ub
ic p
rost
ate
cto
my
for
can
cer
of
the
pro
sta
teH
udso
n, H
.C.,
How
land
, R
.L.,
Jr.
Ca
rra
wa
y M
eth
od
ist
Ho
spita
l
1298
Jour
nal o
f U
rolo
gy19
7210
745
0-45
3C
arc
ino
ma
of
the
pro
sta
te:
a 1
5-y
ea
r fo
llow
up
Ha
na
sh,
K.A
., U
tz,
D.C
., C
oo
k, E
.N.,
Ta
ylo
r, W
.F.,
an
d T
itus,
J.L
.M
ayo
Clin
ic a
nd
th
e M
ayo
Sch
oo
l o
fM
ed
icin
e (
mu
lti-s
ite)
1301
Jour
nal o
f U
rolo
gy19
7210
710
41-
1042
Ca
rcin
om
a o
f p
rost
ate
: tr
ea
tme
nt
an
d s
urv
iva
lw
ith r
ad
ica
l p
rost
ate
cto
my
Yo
un
g,
J.A
., B
oh
ne
, A
.W.
He
nry
Fo
rd H
osp
ital
1877
Ca
nce
r19
7536
723-
728
Ext
ern
al
be
am
ra
dia
tion
th
era
py
of
pri
ma
ryca
rcin
om
a o
f th
e p
rost
ate
Ba
gsh
aw
, M
.A.,
Ra
y, G
.R.,
Pis
ten
ma
,D
.A.,
Ca
ste
llin
o,
R.A
., a
nd
Me
are
s, E
.M.,
Jr.
Sta
nfo
rd U
niv
ers
ity S
cho
ol
of
Me
dic
ine
1940
Jour
nal o
f U
rolo
gy19
7511
337
8-37
9T
ele
cob
alt
the
rap
y fo
r p
rost
atic
ca
nce
r: r
atio
na
le,
resu
lts a
nd
fu
ture
co
nsi
de
ratio
ns
McL
ou
gh
lin,
M.,
Ha
zra
, T
., S
chir
me
r,H
.K.A
., a
nd
Sco
tt,
W.W
.T
he
Jo
hn
s H
op
kin
s U
niv
ers
ity a
nd
Ho
spita
l20
49U
rolo
gy19
755
308-
316
Cry
osu
rge
ry f
or
carc
ino
ma
of
pro
sta
teO
'Do
no
gh
ue
, E
.P.N
, M
ille
ma
n,
L.A
.,F
lock
s, R
.H.,
Cu
lp,
D.A
., a
nd
Bo
nn
ey,
W.W
.
Un
ive
rsity
of
Iow
a H
osp
itals
an
d C
linic
s
2426
Ca
nce
r19
7740
1425
-14
33R
ad
iatio
n t
he
rap
y in
th
e d
efin
itive
tre
atm
en
t o
flo
caliz
ed
ca
rcin
om
a o
f th
e p
rost
ate
Pe
rez,
C.A
., B
au
er,
W.,
Ga
rza
, R
., a
nd
Ro
yce
, R
.K.
Ma
llin
ckro
dt
Inst
itute
of
Ra
dio
log
y (m
ulti
-si
te)
2506
Jour
nal o
f U
rolo
gy19
7812
031
2-31
4L
ate
nt
resi
du
al
tum
or
follo
win
g e
xte
rna
lra
dio
the
rap
y fo
r p
rost
ate
ad
en
oca
rcin
om
aN
ach
tsh
eim
, D
.A.,
Jr.
, M
cAn
inch
, J.
W.,
Stu
tzm
an
, R
.E.,
an
d G
oe
be
l, J.
L.
Le
tte
rma
n A
rmy
Me
dic
al
Ce
nte
r (m
ulti
-si
te)
2529
Jour
nal o
f U
rolo
gy19
7812
018
8-19
0E
xte
nd
ed
to
tal
exc
isio
n o
f p
rost
atic
ad
en
oca
rcin
om
aS
pa
uld
ing
, J.
T.,
Wh
itmo
re,
W.F
., J
r.M
em
ori
al
Slo
an
-Ke
tte
rin
g C
an
cer
Ce
nte
r
2661
Ca
nce
r19
8147
1901
-19
10R
ad
ica
l re
tro
pu
bic
pro
sta
tect
om
y a
nd
pe
lvic
lym
ph
ad
en
ect
om
y fo
r h
igh
-sta
ge
ca
nce
r o
f th
ep
rost
ate
Zin
cke
, H
., F
lem
ing
, T
.R.,
Fu
rlo
w,
W.L
.,M
yers
, R
.P.,
an
d U
tz,
D.C
.M
ayo
Clin
ic a
nd
Ma
yo F
ou
nd
atio
n
2690
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1980
611
21-
1126
Th
e a
dve
rse
in
flue
nce
of
pri
or
tra
nsu
reth
ral
rese
ctio
n o
n p
rog
no
sis
in c
arc
ino
ma
of
pro
sta
tetr
ea
ted
by
rad
iatio
n t
he
rap
y
McG
owan
, D.G
.C
ross
Ca
nce
r In
stitu
te (
mu
lti-s
ite)
Tabl
e A
-1.
Bib
liogr
aphy
by
Pap
yrus
ref
eren
ce n
umbe
r
Archived Document— For Reference Only
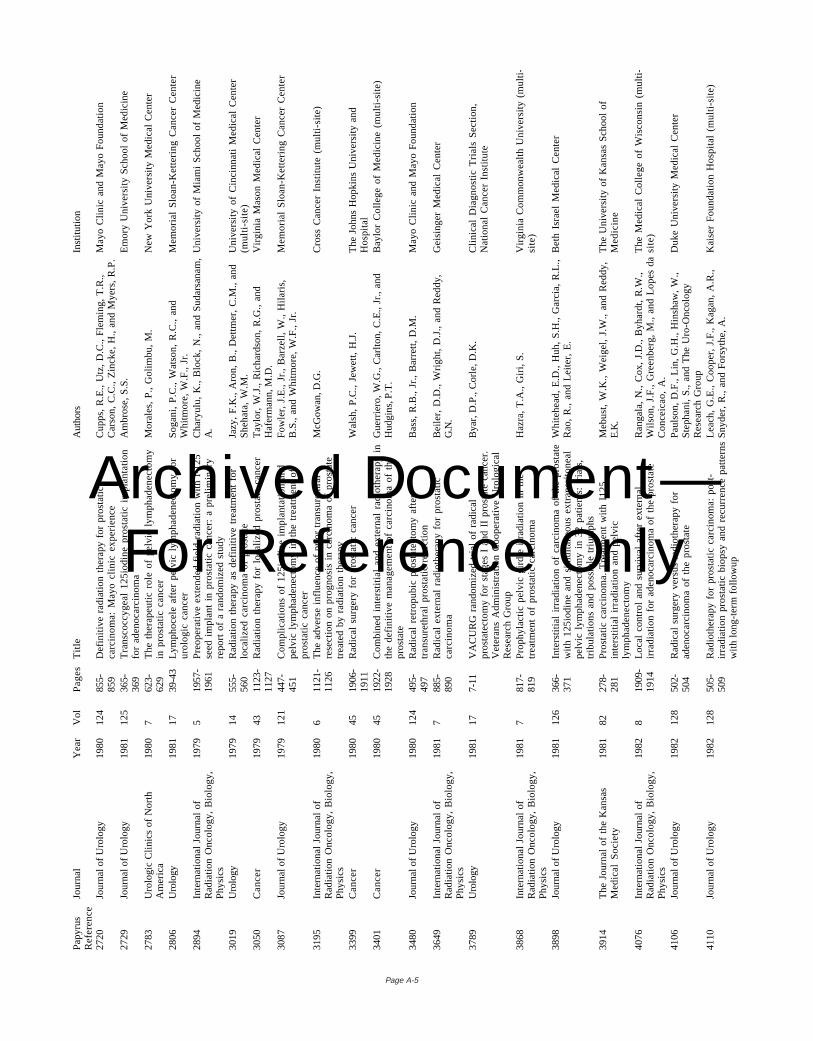
Page A-5
Pa
pyr
us
Re
fere
nce
Jou
rna
lY
ea
rV
olP
ag
es
Titl
eA
utho
rsIn
stitu
tion
2720
Jour
nal o
f U
rolo
gy19
8012
485
5-85
9D
efin
itive
ra
dia
tion
th
era
py
for
pro
sta
ticca
rcin
om
a:
Ma
yo c
linic
exp
eri
en
ceC
up
ps,
R.E
., U
tz,
D.C
., F
lem
ing
, T
.R.,
Ca
rso
n,
C.C
., Z
inck
e,
H.,
an
d M
yers
, R
.P.
Ma
yo C
linic
an
d M
ayo
Fo
un
da
tion
2729
Jour
nal o
f U
rolo
gy19
8112
536
5-36
9T
ran
sco
ccyg
ea
l 1
25
iod
ine
pro
sta
tic i
mp
lan
tatio
nfo
r a
de
no
carc
ino
ma
Am
bro
se,
S.S
.E
mo
ry U
niv
ers
ity S
cho
ol
of
Me
dic
ine
2783
Uro
log
ic C
linic
s o
f N
ort
hA
me
rica
1980
762
3-62
9T
he
th
era
pe
utic
ro
le o
f p
elv
ic l
ymp
ha
de
ne
cto
my
in p
rost
atic
ca
nce
rM
ora
les,
P.,
Go
limb
u,
M.
Ne
w Y
ork
Un
ive
rsity
Me
dic
al
Ce
nte
r
2806
Uro
logy
1981
1739
-43
Lym
ph
oce
le a
fte
r p
elv
ic l
ymp
ha
de
ne
cto
my
for
uro
log
ic c
an
cer
So
ga
ni,
P.C
., W
ats
on
, R
.C.,
an
dW
hitm
ore
, W
.F.,
Jr.
Me
mo
ria
l S
loa
n-K
ett
eri
ng
Ca
nce
r C
en
ter
2894
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1979
519
57-
1961
Pre
op
era
tive
ext
en
de
d f
ield
ra
dia
tion
with
I-1
25
see
d i
mp
lan
t in
pro
sta
tic c
an
cer:
a p
relim
ina
ryre
po
rt o
f a
ra
nd
om
ize
d s
tud
y
Ch
ary
ulu
, K
., B
lock
, N
., a
nd
Su
da
rsa
na
m,
A.
Un
ive
rsity
of
Mia
mi
Sch
oo
l o
f M
ed
icin
e
3019
Uro
logy
1979
1455
5-56
0R
ad
iatio
n t
he
rap
y a
s d
efin
itive
tre
atm
en
t fo
rlo
caliz
ed
ca
rcin
om
a o
f p
rost
ate
Jazy
, F
.K.,
Aro
n,
B.,
De
ttm
er,
C.M
., a
nd
Sh
eh
ata
, W
.M.
Un
ive
rsity
of
Cin
cin
na
ti M
ed
ica
l C
en
ter
(mu
lti-s
ite)
3050
Ca
nce
r19
7943
1123
-11
27R
ad
iatio
n t
he
rap
y fo
r lo
caliz
ed
pro
sta
te c
an
cerT
ayl
or,
W.J
., R
ich
ard
son
, R
.G.,
an
dH
afer
man
n, M
.D.
Vir
gin
ia M
aso
n M
ed
ica
l C
en
ter
3087
Jour
nal o
f U
rolo
gy19
7912
144
7-45
1C
om
plic
atio
ns
of
12
5io
din
e i
mp
lan
tatio
n a
nd
pe
lvic
lym
ph
ad
en
ect
om
y in
th
e t
rea
tme
nt
of
pro
sta
tic c
an
cer
Fo
wle
r, J
.E.,
Jr.
, B
arz
ell,
W.,
Hila
ris,
B.S
., a
nd
Wh
itmo
re,
W.F
., J
r.M
em
ori
al
Slo
an
-Ke
tte
rin
g C
an
cer
Ce
nte
r
3195
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1980
611
21-
1126
Th
e a
dve
rse
in
flue
nce
of
pri
or
tra
nsu
reth
ral
rese
ctio
n o
n p
rog
no
sis
in c
arc
ino
ma
of
pro
sta
tetr
ea
ted
by
rad
iatio
n t
he
rap
y
McG
owan
, D.G
.C
ross
Ca
nce
r In
stitu
te (
mu
lti-s
ite)
3399
Ca
nce
r19
8045
1906
-19
11R
ad
ica
l su
rge
ry f
or
pro
sta
tic c
an
cer
Wa
lsh
, P
.C.,
Je
we
tt,
H.J
.T
he
Jo
hn
s H
op
kin
s U
niv
ers
ity a
nd
Ho
spita
l34
01C
an
cer
1980
4519
22-
1928
Co
mb
ine
d i
nte
rstit
ial
an
d e
xte
rna
l ra
dio
the
rap
y in
the
de
finiti
ve m
an
ag
em
en
t o
f ca
rcin
om
a o
f th
ep
rost
ate
Gu
err
iero
, W
.G.,
Ca
rlto
n,
C.E
., J
r.,
an
dH
udgi
ns, P
.T.
Ba
ylo
r C
olle
ge
of
Me
dic
ine
(m
ulti
-site
)
3480
Jour
nal o
f U
rolo
gy19
8012
449
5-49
7R
ad
ica
l re
tro
pu
bic
pro
sta
tect
om
y a
fte
rtr
an
sure
thra
l p
rost
atic
re
sect
ion
Ba
ss,
R.B
., J
r.,
Ba
rre
tt,
D.M
.M
ayo
Clin
ic a
nd
Ma
yo F
ou
nd
atio
n
3649
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1981
788
5-89
0R
ad
ica
l e
xte
rna
l ra
dio
the
rap
y fo
r p
rost
atic
carc
ino
ma
Be
iler,
D.D
., W
rig
ht,
D.J
., a
nd
Re
dd
y,G
.N.
Ge
isin
ge
r M
ed
ica
l C
en
ter
3789
Uro
logy
1981
177-
11V
AC
UR
G r
an
do
miz
ed
tri
al
of
rad
ica
lp
rost
ate
cto
my
for
sta
ge
s I
an
d I
I p
rost
ate
ca
nce
r.V
ete
ran
s A
dm
inis
tra
tion
Co
op
era
tive
Uro
log
ica
lR
ese
arc
h G
rou
p
Bya
r, D
.P.,
Co
rle
, D
.K.
Clin
ica
l D
iag
no
stic
Tri
als
Se
ctio
n,
Na
tion
al
Ca
nce
r In
stitu
te
3868
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1981
781
7-81
9P
rop
hyl
act
ic p
elv
ic g
ird
le i
rra
dia
tion
in
th
etr
ea
tme
nt
of
pro
sta
tic c
arc
ino
ma
Ha
zra
, T
.A.,
Gir
i, S
.V
irg
inia
Co
mm
on
we
alth
Un
ive
rsity
(m
ulti
-si
te)
3898
Jour
nal o
f U
rolo
gy19
8112
636
6-37
1In
ters
titia
l ir
rad
iatio
n o
f ca
rcin
om
a o
f th
e p
rost
ate
with
12
5io
din
e a
nd
sim
ulta
ne
ou
s e
xtra
pe
rito
ne
al
pe
lvic
lym
ph
ad
en
ect
om
y in
32
pa
tien
ts:
tria
ls,
trib
ula
tion
s a
nd
po
ssib
le t
riu
mp
hs
Wh
iteh
ea
d,
E.D
., H
uh
, S
.H.,
Ga
rcia
, R
.L.,
Ra
o,
R.,
an
d L
eite
r, E
.B
eth
Isr
ae
l M
ed
ica
l C
en
ter
3914
Th
e J
ou
rna
l o
f th
e K
an
sas
Me
dic
al
So
cie
ty19
8182
278-
281
Pro
sta
tic c
arc
ino
ma
. T
rea
tme
nt
with
I1
25
inte
rstit
ial
irra
dia
tion
an
d p
elv
icly
mp
ha
de
ne
cto
my
Me
bu
st,
W.K
., W
eig
el,
J.W
., a
nd
Re
dd
y,E
.K.
Th
e U
niv
ers
ity o
f K
an
sas
Sch
oo
l o
fM
ed
icin
e
4076
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1982
819
09-
1914
Lo
cal
con
tro
l a
nd
su
rviv
al
aft
er
ext
ern
al
irra
dia
tion
fo
r a
de
no
carc
ino
ma
of
the
pro
sta
teR
an
ga
la,
N.,
Co
x, J
.D.,
Byh
ard
t, R
.W.,
Wils
on
, J.
F.,
Gre
en
be
rg,
M.,
an
d L
op
es
da
Co
nce
ica
o,
A.
Th
e M
ed
ica
l C
olle
ge
of
Wis
con
sin
(m
ulti
-si
te)
4106
Jour
nal o
f U
rolo
gy19
8212
850
2-50
4R
ad
ica
l su
rge
ry v
ers
us
rad
ioth
era
py
for
ad
en
oca
rcin
om
a o
f th
e p
rost
ate
Pa
uls
on
, D
.F.,
Lin
, G
.H.,
Hin
sha
w,
W.,
Ste
ph
an
i, S
., a
nd
Th
e U
ro-O
nco
log
yR
ese
arc
h G
rou
p
Du
ke U
niv
ers
ity M
ed
ica
l C
en
ter
4110
Jour
nal o
f U
rolo
gy19
8212
850
5-50
9R
ad
ioth
era
py
for
pro
sta
tic c
arc
ino
ma
: p
ost
-ir
rad
iatio
n p
rost
atic
bio
psy
an
d r
ecu
rre
nce
pa
tte
rns
with
lon
g-t
erm
fo
llow
up
Le
ach
, G
.E.,
Co
op
er,
J.F
., K
ag
an
, A
.R.,
Sn
yde
r, R
., a
nd
Fo
rsyt
he
, A
.K
ais
er
Fo
un
da
tion
Ho
spita
l (m
ulti
-site
)
Archived Document— For Reference Only
Page A-6
4208
Uro
logy
1982
2059
1-59
81
25
I im
pla
nta
tion
fo
r ca
rcin
om
a o
f p
rost
ate
.F
urt
he
r fo
llow
-up
of
first
10
0 c
ase
sG
ross
ma
n,
H.B
., B
ata
ta,
M.,
Hila
ris,
B.,
an
d W
hitm
ore
, W
.F.,
Jr.
Me
mo
ria
l S
loa
n-K
ett
eri
ng
Ca
nce
r C
en
ter
4280
Jour
nal o
f U
rolo
gy19
8212
792
3-92
7C
linic
al
resu
lts o
f e
arl
y st
ag
e p
rost
atic
ca
nce
rtr
ea
ted
by
pe
lvic
lym
ph
ad
en
ect
om
y a
nd
12
5io
din
eim
pla
nts
Ka
nd
zari
, S
.J.,
Be
lis,
J.A
., K
im,
J.C
.,G
ne
pp
, D
.R.,
an
d R
iley,
R.S
.W
est
Vir
gin
ia U
niv
ers
ity M
ed
ica
l C
en
ter
4285
Jour
nal o
f U
rolo
gy19
8212
770
4-70
6R
ad
ica
l p
eri
ne
al
pro
sta
tect
om
y fo
r cl
inic
al
sta
ge
B2
ca
rcin
om
a o
f th
e p
rost
ate
Eld
er,
J.S
., J
ew
ett
, H
.J.,
an
d W
als
h,
P.C
.Th
e J
oh
ns
Ho
pki
ns
Un
ive
rsity
an
dH
osp
ital
4287
Jour
nal o
f U
rolo
gy19
8212
769
9-70
1P
relim
ina
ry o
bse
rva
tion
s o
n t
he
re
sults
of
com
bin
ed
12
5io
din
e s
ee
d i
mp
lan
tatio
n a
nd
ext
ern
al
irra
dia
tion
fo
r ca
rcin
om
a o
f th
e p
rost
ateR
oss
, G
., J
r.,
Bo
rko
n,
W.D
., L
an
dry
, L
.J.,
Ed
wa
rds,
F.M
., W
ein
ste
in,
S.H
., a
nd
Ab
ad
ir,
R.
Un
ive
rsity
of
Mis
sou
ri S
cho
ol o
fM
ed
icin
e
4345
Uro
logy
1982
1937
-42
Cry
osu
rge
ry i
n p
rost
atic
ca
nce
r: s
urv
iva
lB
on
ne
y, W
.W.,
Fa
llon
, B
., G
erb
er,
W.L
.,H
aw
tre
y, C
.E.,
Lo
en
ing
, S
.A.,
Na
raya
na
,A
.S.,
Pla
tz,
C.E
., R
ose
E.F
., S
all,
J.C
.,S
chm
idt,
J.D
., a
nd
Cu
lp,
D.A
.
Un
ive
rsity
of
Iow
a (
mu
lti-s
ite)
4383
Au
stra
lian
& N
ew
Ze
ala
nd
Jour
nal o
f S
urge
ry19
8353
561-
565
Ra
dic
al
rad
ioth
era
py
for
carc
ino
ma
of
the
pro
sta
te:
loca
lize
d a
nd
ext
en
de
d f
ield
tre
atm
en
tNa
cey,
J.N
.D
un
ed
in H
osp
ital
4401
Ca
nce
r19
8351
1599
-16
04P
roto
ns
or
me
ga
volta
ge
X-r
ays
as
bo
ost
th
era
py
for
pa
tien
ts i
rra
dia
ted
fo
r lo
caliz
ed
pro
sta
ticca
rcin
om
a.
An
ea
rly
ph
ase
I/I
I co
mp
ari
son
Du
tte
nh
ave
r, J
.R.,
Sh
iple
y, W
.U.,
Pe
rro
ne
,T
., V
erh
ey,
L.J
., G
oite
in,
M.,
Mu
nze
nri
de
r, J
.E.,
Pro
ut,
G.R
., P
ark
hu
rst,
E.C
., a
nd
Su
it, H
.D.
Ma
ssa
chu
sett
s G
en
era
l H
osp
ital
(mu
lti-
site
)
4639
Th
e C
an
ad
ian
Jo
urn
al
of
Sur
gery
1983
2636
3-36
5In
ters
titia
l ra
dio
the
rap
y fo
r lo
caliz
ed
ca
rcin
om
a o
fth
e p
rost
ate
Wils
on
, J.
W.L
., M
ora
les,
A.,
Bru
ce,
A.W
.,a
nd
Fro
ud
, P
.Q
ue
en
's U
niv
ers
ity
4897
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1984
1018
61-
1867
Tre
atm
en
t-re
late
d m
orb
idity
in
ph
ase
III
RT
OG
stu
die
s o
f e
xte
nd
ed
-fie
ld i
rra
dia
tion
fo
r ca
rcin
om
ao
f th
e p
rost
ate
Pile
pic
h,
M.V
., K
rall,
J.,
Ge
org
e,
F.W
.,A
sbe
ll, S
.O.,
Ple
nk,
H.D
., J
oh
nso
n,
R.J
.,S
tetz
, J.
, Z
inn
ing
er,
M.,
an
d W
alz
, B
.J.W
ash
ing
ton
Un
ive
rsity
Sch
oo
l o
fM
ed
icin
e (
mu
lti-s
ite)
4922
Jou
rna
l o
f th
e M
issi
ssip
pi
Sta
teM
ed
ica
l A
sso
cia
tion
1984
2532
4-32
7E
xte
rna
l b
ea
m i
rra
dia
tion
fo
r p
rost
ate
ca
nce
r: t
he
MB
MC
exp
eri
en
ce a
nd
a l
itera
ture
re
vie
wR
ea
ga
n,
M.T
., S
mith
, R
.A.,
an
dS
tea
dh
am
, R
.E.
Mis
siss
ipp
i B
ap
tist
Me
dic
al
Ce
nte
r
5077
Ca
nce
r19
8453
1857
-18
63R
ela
tion
ship
of
pre
tre
atm
en
t tr
an
sure
thra
lre
sect
ion
of
the
pro
sta
te t
o s
urv
iva
l w
itho
ut
dis
tan
tm
eta
sta
ses
in p
atie
nts
tre
ate
d w
ith 1
25
I-im
pla
nta
tion
fo
r lo
caliz
ed
pro
sta
tic c
an
cer
Fo
wle
r, J
.E.,
Jr.
, F
ish
er,
H.A
.G.,
Ka
ise
r,D
.L.,
an
d W
hitm
ore
, W
.F.,
Jr.
Me
mo
ria
l S
loa
n-K
ett
eri
ng
Ca
nce
rIn
stitu
te
52
05
Th
e P
rost
ate
19
84
519
-25
Ca
rcin
om
a o
f th
e p
rost
ate
: re
sults
of
po
st-
irra
dia
tion
bio
psy
Fre
iha
, F
.S.,
Ba
gsh
aw
, M
.A.
Sta
nfo
rd U
niv
ers
ity S
cho
ol
of
Me
dic
ine
52
19
Ra
dio
the
rap
y a
nd
On
colo
gy
19
84
130
9-31
5E
xte
rna
l b
ea
m r
ad
ioth
era
py
in c
an
cer
of
the
pro
sta
te.
Th
e U
niv
ers
ity o
f A
rizo
na
exp
eri
en
ceA
rist
iza
ba
l, S
.A.,
Ste
inb
ron
n,
D.,
an
dH
eu
sin
kve
ld,
R.S
.U
niv
ers
ity o
f A
rizo
na
He
alth
Sci
en
ces
Ce
nte
r52
65C
an
cer
1984
5337
-43
Ext
ern
al
be
am
irr
ad
iatio
n o
f p
rost
ate
ca
nce
r.E
xpe
rie
nce
in
16
3 p
atie
nts
Ku
rup
, P
., K
ram
er,
T.S
., L
ee
, M
.S.,
an
dP
hill
ips,
R.
Ru
sh-P
resb
yte
ria
n-S
t. L
uke
's M
ed
ica
lC
en
ter
(mu
lti-s
ite)
5610
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1985
1117
77-
1781
Iod
ine
-12
5 i
mp
lan
ts f
or
carc
ino
ma
of
the
pro
sta
tePe
sch
el,
R.E
., F
og
el,
T.D
., K
aci
nsk
i,B
.M.,
Ke
lly,
K.,
an
d M
ate
, T
.P.
Ya
le U
niv
ers
ity S
cho
ol
of
Me
dic
ine
5631
Jour
nal o
f U
rolo
gy19
8513
411
49-
1151
Ne
rve
-sp
ari
ng
ra
dic
al
pro
sta
tect
om
y:e
xtra
pro
sta
tic t
um
or
ext
en
sio
n a
nd
pre
serv
atio
n o
fe
rect
ile f
un
ctio
n
Ca
talo
na
, W
.J.,
Dre
sne
r, S
.M.
Wa
shin
gto
n U
niv
ers
ity S
cho
ol
of
Me
dic
ine
5642
Jour
nal o
f U
rolo
gy19
8513
411
40-
1145
12
5Io
din
e i
mp
lan
tatio
n f
or
carc
ino
ma
of
the
pro
sta
te:
5-y
ea
r su
rviv
al
fre
e o
f d
ise
ase
an
din
cid
en
ce o
f lo
cal
failu
re
Sch
ellh
am
me
r, P
.F.,
El-
Ma
hd
i, A
.E.,
La
da
ga
, L
.E.,
an
d S
chu
lthe
iss,
T.
Ea
ste
rn V
irg
inia
Me
dic
al
Sch
oo
l
5732
Uro
logy
1985
261-
3R
ad
ica
l p
rost
ate
cto
my
for
sta
ge
A2
an
d B
pro
sta
tic c
arc
ino
ma
. O
pe
rativ
e e
xpe
rie
nce
Fo
wle
r, J
.E.,
Jr.
Un
ive
rsity
of
Vir
gin
ia S
cho
ol
of
Me
dic
ine
5813
Uro
logy
1985
2522
8-23
2P
rost
ate
ca
nce
r: e
xpe
rie
nce
with
de
finiti
veir
rad
iatio
n i
n t
he
ag
ed
Gre
en
, N
., B
od
ne
r, H
., a
nd
Bro
th,
E.
LA
C/U
SC
Me
dic
al
Ce
nte
r (m
ulti
-site
)
6141
Clin
ica
l R
ad
iolo
gy
1986
3747
3-47
7R
ad
ica
l tr
ea
tme
nt
of
pro
sta
tic c
arc
ino
ma
by
me
ga
volta
ge
X-r
ay
the
rap
yP
rest
on
, C
.I.,
Du
nca
n,
W.,
an
d K
err
, G
.R.
We
ste
rn G
en
era
l H
osp
ital
6163
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1986
1217
21-
1727
Cu
rre
nt
con
flict
s in
th
e m
an
ag
em
en
t o
f p
rost
atic
can
cer
Ba
gsh
aw
, M
.A.
Sta
nfo
rd U
niv
ers
ity S
cho
ol
of
Me
dic
ine
Archived Document— For Reference Only
Page A-7
Pa
pyr
us
Re
fere
nce
Jou
rna
lY
ea
rV
olP
ag
es
Titl
eA
utho
rsIn
stitu
tion
6191
Jour
nal o
f U
rolo
gy19
8613
642
2-42
4P
atie
nt
surv
iva
l a
nd
lo
cal
recu
rre
nce
ra
tefo
llow
ing
ra
dic
al
pro
sta
tect
om
y fo
r p
rost
atic
carc
ino
ma
Mid
dle
ton
, R
.G.,
Sm
ith,
J.A
., J
r.,
Me
lze
r,R
.B.,
an
d H
am
ilto
n,
P.E
.U
niv
ers
ity o
f U
tah
Sch
oo
l o
f M
ed
icin
e
6215
Th
e M
ed
ica
l Jo
urn
al
of
Au
stra
lia19
8614
462
4-62
8H
igh
-do
se r
ad
ioth
era
py
for
loca
lize
d p
rost
atic
can
cer.
An
an
aly
sis
of
tre
atm
en
t re
sults
an
d e
arl
yco
mp
lica
tion
s
Ke
ars
ley,
J.H
.Q
ue
en
sla
nd
Ra
diu
m I
nst
itute
(m
ulti
-site
)
6331
Jour
nal o
f U
rolo
gy19
8613
551
7-51
9P
rost
atic
ca
rcin
om
a:
5-y
ea
r fo
llow
up
of
pa
tien
tsw
ith s
urg
ica
lly s
tag
ed
dis
ea
se u
nd
erg
oin
ge
xte
nd
ed
fie
ld r
ad
iatio
n
Sa
use
, W
.T.,
Ric
ha
rds,
R.S
., a
nd
Ple
nk,
H.P
.L
DS
Ho
spita
l (m
ulti
-site
)
6344
Jour
nal o
f U
rolo
gy19
8613
572
2-72
5P
relim
ina
ry o
bse
rva
tion
s o
n t
he
re
sults
of
com
bin
ed
te
mp
ora
ry 1
92
irid
ium
im
pla
nta
tion
an
de
xte
rna
l b
ea
m i
rra
dia
tion
fo
r ca
rcin
om
a o
f th
ep
rost
ate
Bo
sch
, P
.C.,
Fo
rbe
s, K
.A.,
Pra
ssvi
nic
ha
i,S
., M
ille
r, J
.B.,
Go
lji,
H.,
an
d M
art
in,
D.C
.
Lo
ng
Be
ach
Ve
tera
ns
Ad
min
istr
atio
nM
ed
ica
l C
en
ter
(mu
lti-s
ite)
6364
Uro
logy
1986
2710
-16
Co
mp
ari
son
of
wh
ole
pe
lvis
ve
rsu
s sm
all-
field
rad
iatio
n t
he
rap
y fo
r ca
rcin
om
a o
f p
rost
ate
Plo
yso
ng
san
g,
S.,
Aro
n,
B.S
., S
he
ha
ta,
W.M
., J
azy
, F
.K.,
Sco
tt,
R.M
., H
o,
P.Y
.,a
nd
Mo
ran
d,
T.M
.
Ch
rist
Ho
spita
l (m
ulti
-site
)
6601
Uro
log
ic C
linic
s o
f N
ort
hA
me
rica
1987
1467
5-68
4R
ad
ioth
era
py
vers
us
surg
ery
fo
r lo
caliz
ed
pro
sta
ticca
nce
rP
au
lso
n,
D.F
.D
uke
Un
ive
rsity
Me
dic
al
Ce
nte
r
6732
Pro
gre
ss i
n C
linic
al
&B
iolo
gic
al
Re
sea
rch
1987
243B
379-
386
Ra
dio
the
rap
y o
f st
ag
e B
2 l
esi
on
s o
f th
e p
rost
ateB
ag
sha
w,
M.A
.S
tan
ford
Un
ive
rsity
Sch
oo
l o
f M
ed
icin
e
6813
Ra
dio
the
rap
y a
nd
On
colo
gy
1987
107-
15R
ad
ioth
era
py
of
pro
sta
te c
arc
ino
ma
: re
sults
of
tre
atm
en
t a
nd
co
mp
lica
tion
sS
ack
, H
., N
osb
ue
sch
, H
., a
nd
Stu
etz
er,
H.
Un
ive
rsity
of
Co
log
ne
6860
An
tica
nce
r R
ese
arc
h19
877
395-
399
Pre
tre
atm
en
t tr
an
sure
thra
l re
sect
ion
of
pro
sta
teca
nce
r a
nd
dis
ea
se-f
ree
su
rviv
al
Na
tara
jan
, N
., M
ett
lin,
C.,
Mu
rph
y, G
.P.,
an
d S
chm
idt,
J.
Ro
swe
ll P
ark
Me
mo
ria
l In
stitu
te (
mu
lti-
site
)69
35In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1987
1349
9-50
5A
te
n y
ea
r fo
llow
-up
of
68
2 p
atie
nts
tre
ate
d f
or
pro
sta
te c
an
cer
with
ra
dia
tion
th
era
py
in t
he
Un
ited
Sta
tes
Ha
nks
, G
.E.,
Dia
mo
nd
, J.
J.,
Kra
ll, J
.M.,
Ma
rtz,
K.L
., a
nd
Kra
me
r, S
.U
niv
ers
ity o
f P
en
nsy
lva
nia
/Fo
x C
ha
seC
an
cer
Ce
nte
r (m
ulti
-site
)
6937
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1987
1310
13-
1020
Pro
sta
tic c
arc
ino
ma
: lim
ited
fie
ld i
rra
dia
tion
Ro
un
savi
lle,
M.C
., G
ree
n,
J.P
., V
ae
th,
J.M
., P
urd
on
, R
.P.,
an
d H
eltz
el,
M.M
.C
hild
ren
's H
osp
ital
(mu
lti-s
ite)
7164
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1988
1513
07-
1316
Ele
ctiv
e p
elv
ic i
rra
dia
tion
in
sta
ge
A2
, B
carc
ino
ma
of
the
pro
sta
te:
an
aly
sis
of
RT
OG
77
06
Asb
ell,
S.O
., K
rall,
J.M
., P
ilep
ich
, M
.V.,
Ba
erw
ald
, H
., S
au
se,
W.T
., H
an
ks,
G.E
.,a
nd
Pe
rez,
C.A
.
Alb
ert
Ein
ste
in M
ed
ica
l C
en
ter
(mu
lti-
site
)
7419
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1988
1513
17-
1322
Ad
en
oca
rcin
om
a o
f th
e p
rost
ate
: ra
dio
act
ive
go
ldse
ed
im
pla
nt
plu
s e
xte
rna
l ir
rad
iatio
nG
utie
rre
z, A
.E.,
Me
rin
o,
O.R
.R
ad
iatio
n O
nco
log
y S
ect
ion
, S
t. J
ose
ph
Ho
spita
l
7519
Sca
nd
ina
via
n J
ou
rna
l o
fU
rolo
gy &
Nep
hrol
ogy
-S
up
ple
me
ntu
m
1988
110
95-1
00T
rea
tme
nt
of
loca
lize
d p
rost
atic
ca
nce
r. R
ad
ica
lp
rost
ate
cto
my
vers
us
pla
ceb
o.
A 1
5-y
ea
r fo
llow
-up
Ma
dse
n,
P.O
., G
rave
rse
n,
P.H
., G
ass
er,
T.C
., a
nd
Co
rle
, D
.K.
Will
iam
S.
Mid
dle
ton
Me
mo
ria
l V
ete
ran
sH
osp
ital
(mu
lti-s
ite)
7522
Sca
nd
ina
via
n J
ou
rna
l o
fU
rolo
gy &
Nep
hrol
ogy
-S
up
ple
me
ntu
m
1988
110
89-9
4R
ad
iatio
n t
he
rap
y fo
r p
rost
atic
ca
rcin
om
aB
erg
ma
n,
B.,
Mo
dig
, H
.D
ep
art
me
nts
of
Uro
log
y &
An
dro
log
y a
nd
On
colo
gy,
Un
vers
ity o
f U
me
a
7644
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1988
1411
53-
1157
Iod
ine
-12
5 i
mp
lan
ts v
ers
us
ext
ern
al
be
am
th
era
py
for
sta
ge
s A
2,
B,
an
d C
pro
sta
te c
an
cer
Mo
rto
n,
J.D
., P
esc
he
l, R
.E.
Ya
le U
niv
ers
ity S
cho
ol
of
Me
dic
ine
7670
Jour
nal o
f U
rolo
gy19
8813
998
5-98
8In
ters
titia
l g
old
an
d e
xte
rna
l b
ea
m i
rra
dia
tion
fo
rp
rost
ate
ca
nce
rB
oile
au
, M
.A.,
Do
wlin
g,
R.A
., G
on
zale
s,M
., H
an
de
l, P
.H.,
Be
nso
n,
G.S
., a
nd
Co
rrie
re,
J.N
., J
r.
Un
ive
rsity
of
Te
xas
Me
dic
al
Sch
oo
l
7671
Jour
nal o
f U
rolo
gy19
8813
998
9-99
4C
om
bin
ed
go
ld s
ee
d i
mp
lan
tatio
n a
nd
ext
ern
al
rad
ioth
era
py
for
sta
ge
B2
or
C p
rost
ate
ca
nce
rCa
rey,
P.O
., L
ipp
ert
, M
.C.,
Co
nst
ab
le,
W.C
., J
on
es,
D.,
an
d T
alto
n,
B.M
.U
niv
ers
ity o
f V
irg
inia
Me
dic
al
Sch
oo
l(m
ulti
-site
)77
65A
me
rica
n J
ou
rna
l o
f C
linic
al
On
colo
gy
1988
1116
6-17
1R
ad
iatio
n-t
rea
ted
ca
rcin
om
a o
f p
rost
ate
.C
om
pa
riso
n o
f su
rviv
al
of
bla
ck a
nd
wh
itep
atie
nts
by
Gle
aso
n's
gra
din
g s
yste
m
Azi
z, H
., R
otm
an
, M
., T
he
lmo
, W
., C
he
n,
P.,
Ch
oi,
K.N
., K
hil,
S.U
., L
au
ng
an
i, G
.B.,
Bra
nd
ys,
M.,
Ayr
, G
., a
nd
Ma
cch
ia,
R.J
.Sta
te U
niv
ers
ity o
f N
ew
Yo
rk-H
ea
lthS
cie
nce
Ce
nte
r a
t B
roo
klyn
Archived Document— For Reference Only
Page A-8
7796
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1988
1470
1-70
9T
he
ro
le o
f ra
dia
tion
th
era
py
in s
tag
es
A2
an
d B
ad
en
oca
rcin
om
a o
f th
e p
rost
ate
Za
ga
rs,
G.K
., v
on
Esc
he
nb
ach
, A
.C.,
Joh
nso
n,
D.E
., a
nd
Osw
ald
, M
.J.
Th
e U
niv
ers
ity o
f T
exa
s M
.D.
An
de
rso
nH
osp
ital
(mu
lti-s
ite)
7832
Uro
logy
1988
3119
1-19
7R
ad
ica
l p
rost
ate
cto
my.
Pa
tte
rns
of
loca
l fa
ilure
an
d s
urv
iva
l in
67
pa
tien
tsS
che
llha
mm
er,
P.F
.E
ast
ern
Vir
gin
ia M
ed
ica
l S
cho
ol
8161
Inte
rna
tion
al
Uro
log
y &
Nep
hrol
ogy
1989
2132
5-33
2E
xpe
rie
nce
in
th
e t
rea
tme
nt
of
loca
lize
dca
rcin
om
a o
f th
e p
rost
ate
by
de
finiti
ve e
xte
rna
lir
rad
iatio
n
Ku
ten
, A
., N
itetz
ky,
S.,
Ta
tch
er,
M.,
Co
he
n,
Y.,
an
d R
ob
inso
n,
E.
Te
chn
ion
-Isr
ae
l In
stitu
te o
f T
ech
no
log
y(m
ulti
-site
)
8182
Jour
nal o
f U
rolo
gy19
8914
212
62-
1265
Pa
tte
rn o
f fa
ilure
aft
er
rad
ica
l re
tro
pu
bic
pro
sta
tect
om
y fo
r cl
inic
ally
an
d p
ath
olo
gic
ally
loca
lize
d a
de
no
carc
ino
ma
of
the
pro
sta
te:
influ
en
ce o
f tu
mo
r d
eo
xyri
bo
nu
cle
ic a
cid
plo
idy
Blu
te,
M.L
., N
ativ
, O
., Z
inck
e,
H.,
Fa
rro
w,
G.M
., T
he
rne
au
, T
., a
nd
Lie
be
r,M
.M.
Ma
yo C
linic
82
57
Ra
dio
the
rap
y a
nd
On
colo
gy
19
89
16
1-21
Fa
cto
rs i
nflu
en
cin
g o
utc
om
e o
f d
efin
itive
rad
ioth
era
py
for
loca
lize
d c
arc
ino
ma
of
the
pro
sta
te
Pe
rez,
C.A
., G
arc
ia,
D.,
Sim
pso
n,
J.R
.,Z
ivn
usk
a,
F.,
an
d L
ock
ett
, M
.A.
Ma
llin
ckro
dt
Inst
itute
of
Ra
dio
log
y (m
ulti
-si
te)
8280
Uro
logy
1989
3317
-20
Pa
tien
t se
lect
ion
fo
r ra
dic
al
pro
sta
tect
om
yS
mith
, J.
A.,
Jr.
Un
ive
rsity
of
Uta
h C
en
ter
for
He
alth
Sci
en
ces
83
18
Bri
tish
Jo
urn
al o
f U
rolo
gy
19
89
63
191-
195
Re
tro
spe
ctiv
e s
tud
y o
f ra
dio
the
rap
y in
ea
rly
carc
ino
ma
of
the
pro
sta
teR
ea
d,
G.,
Po
into
n,
R.C
.S.
Ch
rist
ie H
osp
ital
(mu
lti-s
ite)
8331
Ca
nce
r19
8963
2468
-24
74E
xte
rna
l b
ea
m r
ad
ioth
era
py
for
carc
ino
ma
of
the
pro
sta
teS
ag
erm
an
, R
.H.,
Ch
un
, H
.C.,
Kin
g,
G.A
.,C
hu
ng
, C
.T.,
an
d D
ala
l, P
.S.
Ma
llin
ckro
dt
Inst
itute
of
Ra
dio
log
y (m
ulti
-si
te)
8332
Ca
nce
r19
8963
2421
-24
25P
rog
no
sis
in p
atie
nts
with
lo
cal
recu
rre
nce
aft
er
de
finiti
ve i
rra
dia
tion
fo
r p
rost
atic
ca
rcin
om
aK
ub
an
, D
.A.,
El-
Ma
hd
i, A
.M.,
an
dS
che
llha
mm
er,
P.F
.E
ast
ern
Vir
gin
ia M
ed
ica
l S
cho
ol
8333
Ca
nce
r19
8963
2415
-24
20I-
12
5 i
nte
rstit
ial
imp
lan
tatio
n f
or
pro
sta
te c
an
cer.
Wh
at
ha
ve w
e l
ea
rne
d 1
0 y
ea
rs l
ate
r?K
ub
an
, D
.A.,
El-
Ma
hd
i, A
.M.,
an
dS
che
llha
mm
er,
P.F
.E
ast
ern
Vir
gin
ia M
ed
ica
l S
cho
ol
8411
Jour
nal o
f U
rolo
gy19
8914
182
-84
Ca
use
-sp
eci
fic a
ctu
ari
al
surv
iva
l a
na
lysi
s: a
use
ful
me
tho
d f
or
rep
ort
ing
su
rviv
al
da
ta i
n m
en
with
clin
ica
lly l
oca
lize
d c
arc
ino
ma
of
the
pro
sta
teLe
po
r, H
., K
imb
all,
A.W
., a
nd
Wa
lsh
,P
.C.
Th
e J
oh
ns
Ho
pki
ns
Un
ive
rsity
an
dH
osp
ital
8428
Jour
nal o
f U
rolo
gy19
8914
156
4-56
6T
ota
l p
rost
ate
cto
my
for
clin
ica
lly l
oca
lize
dp
rost
atic
ca
nce
r: l
on
g-t
erm
re
sults
Gib
bo
ns,
R.P
., C
orr
ea
, R
.J.,
Jr.
, B
ran
ne
n,
G.E
., a
nd
We
issm
an
, R
.M.
Th
e V
irg
inia
Ma
son
Clin
ic
8493
Uro
logy
1989
3336
1-36
6P
rog
no
stic
sig
nifi
can
ce o
f D
NA
plo
idy
inca
rcin
om
a o
f p
rost
ate
De
jter,
S.W
., J
r.,
Cu
nn
ing
ha
m,
R.E
.,N
og
uch
i, P
.D.,
Jo
ne
s, R
.V.,
Mo
ul,
J.W
.,M
cLe
od
, D
.G.,
an
d L
ynch
, J.
H.
Ge
org
eto
wn
Un
ive
rsity
Ho
spita
l (m
ulti
-si
te)
8615
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1990
1913
83-
1388
Th
e r
ole
of
seru
m p
rost
atic
aci
d p
ho
sph
ata
se i
nth
e m
an
ag
em
en
t o
f a
de
no
carc
ino
ma
of
the
pro
sta
te w
ith r
ad
ioth
era
py
Ca
rlto
n,
J.C
., Z
ag
ars
, G
.K.,
an
d O
swa
ld,
M.J
.T
he
Un
ive
rsity
of
Te
xas
M.D
. A
nd
ers
on
Ca
nce
r C
en
ter
8616
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1990
1913
77-
1382
Th
e e
ffe
ct o
f o
vera
ll tr
ea
tme
nt
time
on
lo
cal
con
tro
l in
pa
tien
ts w
ith a
de
no
carc
ino
ma
of
the
pro
sta
te t
rea
ted
with
ra
dia
tion
th
era
py
Am
du
r, R
.J.,
Pa
rso
ns,
J.T
., F
itzg
era
ld,
L.T
., a
nd
Mill
ion
, R
.R.
Un
ive
rsity
of
Flo
rid
a C
olle
ge
of
Me
dic
ine
8717
Uro
logy
1990
3649
3-49
8R
ad
ica
l p
rost
ate
cto
my
vers
us
exp
ect
an
t p
rim
ary
tre
atm
en
t in
sta
ge
s I
an
d I
I p
rost
atic
ca
nce
r. A
fifte
en
-ye
ar
follo
w-u
p
Gra
vers
en
, P
.H.,
Nie
lse
n,
K.T
., G
ass
er,
T.C
., C
orl
e,
D.K
., a
nd
Ma
dse
n,
P.O
.V
ete
ran
s A
dm
inis
tra
tion
Ho
spita
l (m
ulti
-si
te)
8798
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1990
1956
1-56
8C
arc
ino
ma
of
the
pro
sta
te s
tag
e B
an
d C
: la
ck o
fin
flue
nce
of
du
ratio
n o
f ra
dio
the
rap
y o
n t
um
or
con
tro
l a
nd
tre
atm
en
t m
orb
idity
La
i, P
.P.,
Pe
rez,
C.A
., S
ha
pir
o,
S.J
., a
nd
Lo
cke
tt,
M.A
.M
alli
nck
rod
t In
stitu
te o
f R
ad
iolo
gy
(mu
lti-
site
)
8823
Jour
nal o
f U
rolo
gy19
9014
411
80-
1184
Ra
dic
al
pro
sta
tect
om
y fo
r cl
inic
al
sta
ge
T1
-2
N0
M0
pro
sta
tic a
de
no
carc
ino
ma
: lo
ng
-te
rmre
sults
Pa
uls
on
, D
.F.,
Mo
ul,
J.W
., a
nd
Wa
lthe
r,P
.J.
Du
ke U
niv
ers
ity M
ed
ica
l C
en
ter
8827
Jour
nal o
f U
rolo
gy19
9014
414
20-
1424
Ro
le o
f n
erv
e-s
pa
rin
g r
ad
ica
l p
rost
ate
cto
my
for
clin
ica
l st
ag
e B
2 p
rost
ate
ca
nce
rB
igg
, S
.W.,
Ka
vou
ssi,
L.R
., a
nd
Ca
talo
na
,W
.J.
Wa
shin
gto
n U
niv
ers
ity S
cho
ol
of
Me
dic
ine
89
02
Ra
dio
the
rap
y a
nd
On
colo
gy
19
90
18
235-
246
Ad
en
oca
rcin
om
a o
f th
e p
rost
ate
tre
ate
d w
ithe
xte
rna
l-b
ea
m r
ad
iatio
n t
he
rap
y: 5
-ye
ar
min
imu
mfo
llow
-up
Am
du
r, R
.J.,
Pa
rso
ns,
J.T
., F
itzg
era
ld,
L.T
., a
nd
Mill
ion
, R
.R.
Un
ive
rsity
of
Flo
rid
a C
olle
ge
of
Me
dic
ine
8925
Uro
log
ic C
linic
s o
f N
ort
hA
me
rica
1990
1777
9-78
5S
ele
ctio
n o
f p
atie
nts
with
sta
ge
B p
rost
ate
ca
nce
rfo
r ra
dic
al
pro
sta
tect
om
yM
idd
leto
n,
R.G
., L
ars
en
, R
.H.
Un
ive
rsity
of
Uta
h C
en
ter
for
the
He
alth
Sci
en
ces
Archived Document— For Reference Only
Page A-9
Pa
pyr
us
Re
fere
nce
Jou
rna
lY
ea
rV
olP
ag
es
Titl
eA
utho
rsIn
stitu
tion
8990
Bri
tish
Jo
urn
al o
f U
rolo
gy
1990
6561
1-61
4T
he
na
tura
l co
urs
e o
f lo
w g
rad
e,
no
n-m
eta
sta
ticp
rost
atic
ca
rcin
om
aA
do
lfsso
n,
J.,
Ro
nst
rom
, L
., C
ars
ten
sen
,J.
, L
ow
ha
ge
n,
T.,
an
d H
ed
lun
d,
P.O
.K
aro
linsk
a H
osp
ital
(mu
lti-s
ite)
9175
Arc
hiv
es
of
Su
rge
ry19
9012
532
7-33
1S
tag
e B
pro
sta
te a
de
no
carc
ino
ma
. F
low
cyto
me
tric
nu
cle
ar
DN
A p
loid
y a
na
lysi
sM
on
tgo
me
ry,
B.T
., N
ativ
, O
., B
lute
, M
.L.,
Fa
rro
w,
G.M
., M
yers
, R
.P.,
Zin
cke
, H
.,T
he
rne
au
, T
.M.,
an
d L
ieb
er,
M.M
.
Ma
yo C
linic
9194
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1990
1831
5-32
0B
ow
el
com
plic
atio
ns
aft
er
rad
ioth
era
py
for
carc
ino
ma
of
the
pro
sta
te:
the
vo
lum
e e
ffe
ctM
am
eg
ha
n,
H.,
Fis
he
r, R
., M
am
eg
ha
n,
J.,
Wa
tt,
W.H
., a
nd
Tyn
an
, A
.In
stitu
te o
f R
ad
ioth
era
py
(mu
lti-s
ite)
9219
Uro
logy
1990
3522
3-22
7In
tra
op
era
tive
an
d e
arl
y co
mp
lica
tion
s o
f st
ag
ing
pe
lvic
lym
ph
no
de
dis
sect
ion
in
pro
sta
tica
de
no
carc
ino
ma
Do
no
hu
e,
R.E
., M
an
i, J.
H.,
Wh
itese
l, J.
A.,
Au
gsp
urg
er,
R.R
., W
illia
ms,
G.,
an
dF
auve
r, H
.E.
Un
ive
rsity
of
Co
lora
do
He
alth
Sci
en
ces
Ce
nte
r (m
ulti
-site
)
9265
Au
stra
lian
& N
ew
Ze
ala
nd
Jour
nal o
f S
urge
ry19
9161
658-
662
Ra
dia
tion
th
era
py
for
the
ma
na
ge
me
nt
of
loca
lize
d p
rost
ate
ca
rcin
om
aB
urm
eis
ter,
B.H
., P
rob
ert
, J.
C.
Au
ckla
nd
Ho
spita
l
9351
Ca
nce
r19
9167
1091
-10
96E
xpe
cta
nt
ma
na
ge
me
nt
of
loca
lize
d p
rost
atic
can
cer
Wh
itmo
re,
W.F
., J
r.,
Wa
rne
r, J
.A.,
an
dT
hom
pson
, I.M
., Jr
.M
em
ori
al
Slo
an
-Ke
tte
rin
g C
an
cer
Ce
nte
r
9407
Jour
nal o
f U
rolo
gy19
9114
551
2-51
4Im
pa
ct o
f a
na
tom
ica
l ra
dic
al
pro
sta
tect
om
y o
nu
rin
ary
co
ntin
en
ceS
tein
er,
M.S
., M
ort
on
, R
.A.,
an
d W
als
h,
P.C
.T
he
Jo
hn
s H
op
kin
s U
niv
ers
ity a
nd
Ho
spita
l95
72In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1985
1120
73-
2080
Imp
rovi
ng
th
e t
he
rap
eu
tic r
atio
of
ext
ern
al
be
am
irra
dia
tion
fo
r ca
rcin
om
a o
f th
e p
rost
ate
Fo
rma
n,
J.D
., Z
inre
ich
, E
., L
ee
, D
.J.,
Wh
ara
m,
M.D
., B
au
mg
ard
ne
r, R
.A.,
an
dO
rder
, S.E
.
Th
e J
oh
ns
Ho
pki
ns
Un
ive
rsity
an
dH
osp
ital
9580
Jour
nal o
f U
rolo
gy19
8513
349
-52
Op
era
ble
pro
sta
tic c
arc
ino
ma
: co
rre
latio
ns
am
on
gcl
inic
al
sta
ge
, p
ath
olo
gic
al
sta
ge
, G
lea
son
his
tolo
gic
al
sco
re a
nd
ea
rly
dis
ea
se-f
ree
su
rviv
al
Fo
wle
r, J
.E.,
Jr.
, M
ills,
S.E
.U
niv
ers
ity o
f V
irg
inia
Sch
oo
l o
f M
ed
icin
e
9717
Uro
logy
1983
2145
1-45
7P
elv
ic c
om
plic
atio
ns
aft
er
de
finiti
ve t
rea
tme
nt
of
pro
sta
te c
an
cer
by
inte
rstit
ial
or
ext
ern
al
be
am
rad
iatio
n
Sch
ellh
am
me
r, P
.F.,
El-
Ma
hd
i, A
.M.
Ea
ste
rn V
irg
inia
Me
dic
al
Sch
oo
l
9733
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1984
1054
1-54
8T
rip
le c
ou
rse
ext
ern
al
be
am
ra
dio
the
rap
y fo
rca
rcin
om
a o
f th
e p
rost
ate
El-
Ma
hd
i, A
.M.,
Tu
ralb
a,
C.I
.C.,
Sch
ellh
am
me
r, P
.F.,
an
d P
ee
ple
s, W
.J.E
ast
ern
Vir
gin
ia M
ed
ica
l S
cho
ol/M
ed
ica
lC
en
ter
Ho
spita
ls
9737
Jou
rna
l o
f th
e N
atio
na
l M
ed
ica
lA
sso
cia
tion
1984
7661
-66
Ext
ern
al
rad
iatio
n t
he
rap
y o
f lo
caliz
ed
pro
sta
ticca
nce
rR
ed
dy,
E.K
., G
iri,
S.,
an
d M
an
sfie
ld,
C.M
.U
niv
ers
ity o
f K
an
sas
Me
dic
al
Ce
nte
r(m
ulti
-site
)98
79In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1991
2153
7-54
7T
he
eff
ect
of
loca
l co
ntr
ol
on
me
tast
atic
dis
sem
ina
tion
in
ca
rcin
om
a o
f th
e p
rost
ate
: lo
ng
-te
rm r
esu
lts i
n p
atie
nts
tre
ate
d w
ith 1
25
Iim
pla
nta
tion
Fu
ks,
Z.,
Le
ibe
l, S
.A.,
Wa
llne
r, K
.E.,
Be
gg
, C
.B.,
Fa
ir,
W.R
., A
nd
ers
on
, L
.L.,
Hila
ris,
B.S
., a
nd
Wh
itmo
re,
W.F
.
Me
mo
ria
l S
loa
n-K
ett
eri
ng
Ca
nce
r C
en
ter
9895
Jour
nal o
f U
rolo
gy19
9114
511
97-
1200
Ca
nce
r co
ntr
ol
follo
win
g a
na
tom
ica
l ra
dic
al
pro
sta
tect
om
y: a
n i
nte
rim
re
po
rtM
ort
on
, R
.A.,
Ste
ine
r, M
.S.,
an
d W
als
h,
P.C
.T
he
Jo
hn
s H
op
kin
s U
niv
ers
ity a
nd
Ho
spita
l98
99Jo
urna
l of
Uro
logy
1991
146
798-
802
Co
mp
lica
tion
s fo
llow
ing
ext
ern
al
be
am
ra
dia
tion
the
rap
y fo
r p
rost
ate
ca
nce
r: a
n a
na
lysi
s o
f p
atie
nts
tre
ate
d w
ith a
nd
with
ou
t st
ag
ing
pe
lvic
lym
ph
ad
en
ect
om
y
Gre
sko
vich
, F
.J.,
Za
ga
rs,
G.K
., S
he
rma
n,
N.E
., an
d Jo
hnso
n, D
.E.
Un
ive
rsity
of
Te
xas
M.D
. A
nd
ers
on
Ca
nce
r C
en
ter
1003
9B
ritis
h J
ou
rna
l of
Uro
log
y19
9269
183-
187
De
ferr
ed
tre
atm
en
t in
clin
ica
lly l
oca
lise
d p
rost
atic
carc
ino
ma
Ad
olfs
son
, J.
, C
ars
ten
sen
, J.
, a
nd
Lo
wh
ag
en
, T
.K
aro
linsk
a H
osp
ital
(mu
lti-s
ite)
1007
6In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1992
2256
5-56
8T
he
eff
ica
cy o
f p
ha
rma
coki
ne
tic m
on
itori
ng
an
dd
ose
mo
difi
catio
n o
f e
tan
ida
zole
on
th
e i
nci
de
nce
of
ne
uro
toxi
city
: re
sults
fro
m a
ph
ase
II
tria
l o
fe
tan
ida
zole
an
d r
ad
iatio
n t
he
rap
y in
lo
cally
ad
van
ced
pro
sta
te c
an
cer
Co
lem
an
, C
.N.,
Bu
swe
ll, L
., N
oll,
L.,
Rie
se,
N.,
an
d R
ose
, M
.A.
Join
t C
en
ter
for
Ra
dia
tion
Th
era
py
(mu
lti-
site
)
1010
4Jo
urna
l of
Uro
logy
1992
147
905-
907
Th
e m
an
ag
em
en
t o
f re
cta
l in
jury
du
rin
g r
ad
ica
lre
tro
pu
bic
pro
sta
tect
om
yB
orl
an
d,
R.N
., W
als
h,
P.C
.T
he
Jo
hn
s H
op
kin
s U
niv
ers
ity a
nd
Ho
spita
l10
107
Jour
nal o
f U
rolo
gy19
9214
791
7-92
1T
he
im
po
rta
nce
of
loca
l co
ntr
ol
in t
he
tre
atm
en
to
f p
rost
atic
ca
nce
rK
ap
lan
, I.
D.,
Pre
stid
ge
, B
.R.,
Ba
gsh
aw
,M
.A.,
an
d C
ox,
R.S
.S
tan
ford
Un
ive
rsity
Sch
oo
l o
f M
ed
icin
e(m
ulti
-site
)10
108
Jour
nal o
f U
rolo
gy19
9214
788
8-89
0R
ad
ica
l p
rost
ate
cto
my:
th
e p
ros
an
d c
on
s o
f th
ep
eri
ne
al
vers
us
retr
op
ub
ic a
pp
roa
chF
razi
er,
H.A
., R
ob
ert
son
, J.
E.,
an
dP
au
lso
n,
D.F
.D
uke
Un
ive
rsity
Me
dic
al
Ce
nte
r
Archived Document— For Reference Only
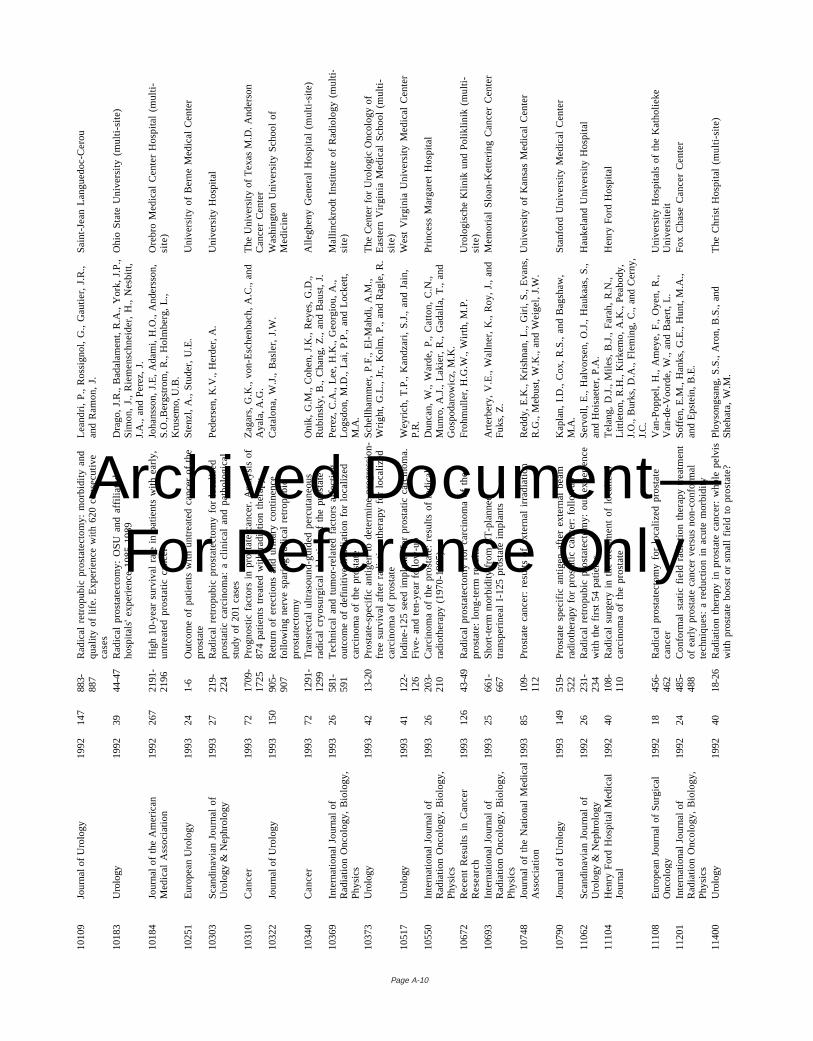
Page A-10
1010
9Jo
urna
l of
Uro
logy
1992
147
883-
887
Ra
dic
al
retr
op
ub
ic p
rost
ate
cto
my:
mo
rbid
ity a
nd
qu
alit
y o
f lif
e.
Exp
eri
en
ce w
ith 6
20
co
nse
cutiv
eca
ses
Le
an
dri
, P
., R
oss
ign
ol,
G.,
Ga
utie
r, J
.R.,
an
d R
am
on
, J.
Sa
int-
Jea
n L
an
gu
ed
oc-
Ce
rou
1018
3U
rolo
gy19
9239
44-4
7R
ad
ica
l p
rost
ate
cto
my:
OS
U a
nd
aff
ilia
ted
ho
spita
ls'
exp
eri
en
ce 1
98
5-1
98
9D
rag
o,
J.R
., B
ad
ala
me
nt,
R.A
., Y
ork
, J.
P.,
Sim
on
, J.
, R
iem
en
sch
ne
ide
r, H
., N
esb
itt,
J.A
., a
nd
Pe
rez,
J.
Oh
io S
tate
Un
ive
rsity
(m
ulti
-site
)
1018
4Jo
urn
al
of
the
Am
eri
can
Me
dic
al
Ass
oci
atio
n19
9226
721
91-
2196
Hig
h 1
0-y
ea
r su
rviv
al
rate
in
pa
tien
ts w
ith e
arl
y,u
ntr
ea
ted
pro
sta
tic c
an
cer
Joh
an
sso
n,
J.E
, A
da
mi,
H.O
., A
nd
ers
son
,S
.O.,
Be
rgst
rom
, R
., H
olm
be
rg,
L.,
Kru
sem
o, U
.B.
Ore
bro
Me
dic
al
Ce
nte
r H
osp
ital
(mu
lti-
site
)
10
25
1E
uro
pe
an
Uro
log
y1
99
32
41-
6O
utc
om
e o
f p
atie
nts
with
un
tre
ate
d c
an
cer
of
the
pro
sta
teS
ten
zl,
A.,
Stu
de
r, U
.E.
Un
ive
rsity
of
Be
rne
Me
dic
al
Ce
nte
r
1030
3S
can
din
avi
an
Jo
urn
al
of
Uro
log
y &
Ne
ph
rolo
gy
1993
2721
9-22
4R
ad
ica
l re
tro
pu
bic
pro
sta
tect
om
y fo
r lo
calis
ed
pro
sta
tic c
arc
ino
ma
: a
clin
ica
l a
nd
pa
tho
log
ica
lst
ud
y o
f 2
01
ca
ses
Pe
de
rse
n,
K.V
., H
erd
er,
A.
Un
ive
rsity
Ho
spita
l
1031
0C
an
cer
1993
7217
09-
1725
Pro
gn
ost
ic f
act
ors
in
pro
sta
te c
an
cer.
An
aly
sis
of
87
4 p
atie
nts
tre
ate
d w
ith r
ad
iatio
n t
he
rap
yZ
ag
ars
, G
.K.,
vo
n-E
sch
en
ba
ch,
A.C
., a
nd
Aya
la,
A.G
.T
he
Un
ive
rsity
of
Te
xas
M.D
. A
nd
ers
on
Ca
nce
r C
en
ter
1032
2Jo
urna
l of
Uro
logy
1993
150
905-
907
Re
turn
of
ere
ctio
ns
an
d u
rin
ary
co
ntin
en
cefo
llow
ing
ne
rve
sp
ari
ng
ra
dic
al
retr
op
ub
icp
rost
ate
cto
my
Ca
talo
na
, W
.J.,
Ba
sle
r, J
.W.
Wa
shin
gto
n U
niv
ers
ity S
cho
ol
of
Me
dic
ine
1034
0C
an
cer
1993
7212
91-
1299
Tra
nsr
ect
al
ultr
aso
un
d-g
uid
ed
pe
rcu
tan
eo
us
rad
ica
l cr
yosu
rgic
al
ab
latio
n o
f th
e p
rost
ate
On
ik,
G.M
., C
oh
en
, J.
K.,
Re
yes,
G.D
.,R
ub
insk
y, B
., C
ha
ng
, Z
., a
nd
Ba
ust
, J.
Alle
gh
en
y G
en
era
l H
osp
ital
(mu
lti-s
ite)
1036
9In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1993
2658
1-59
1T
ech
nic
al
an
d t
um
or-
rela
ted
fa
cto
rs a
ffe
ctin
go
utc
om
e o
f d
efin
itive
irr
ad
iatio
n f
or
loca
lize
dca
rcin
om
a o
f th
e p
rost
ate
Pe
rez,
C.A
., L
ee
, H
.K.,
Ge
org
iou
, A
.,L
og
sdo
n,
M.D
., L
ai,
P.P
., a
nd
Lo
cke
tt,
M.A
.
Ma
llin
ckro
dt
Inst
itute
of
Ra
dio
log
y (m
ulti
-si
te)
1037
3U
rolo
gy19
9342
13-2
0P
rost
ate
-sp
eci
fic a
ntig
en
to
de
term
ine
pro
gre
ssio
n-
fre
e s
urv
iva
l a
fte
r ra
dia
tion
th
era
py
for
loca
lize
dca
rcin
om
a o
f p
rost
ate
Sch
ellh
am
me
r, P
.F.,
El-
Ma
hd
i, A
.M.,
Wri
gh
t, G
.L.,
Jr.
, K
olm
, P
., a
nd
Ra
gle
, R
.Th
e C
en
ter
for
Uro
log
ic O
nco
log
y o
fE
ast
ern
Vir
gin
ia M
ed
ica
l S
cho
ol
(mu
lti-
site
)10
517
Uro
logy
1993
4112
2-12
6Io
din
e-1
25
se
ed
im
pla
nts
fo
r p
rost
atic
ca
rcin
om
a.
Fiv
e-
an
d t
en
-ye
ar
follo
w-u
pW
eyr
ich
, T
.P.,
Ka
nd
zari
, S
.J.,
an
d J
ain
,P
.R.
We
st V
irg
inia
Un
ive
rsity
Me
dic
al
Ce
nte
r
1055
0In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1993
2620
3-21
0C
arc
ino
ma
of
the
pro
sta
te:
resu
lts o
f ra
dic
al
rad
ioth
era
py
(19
70
-19
85
)D
un
can
, W
., W
ard
e,
P.,
Ca
tto
n,
C.N
.,M
un
ro,
A.J
., L
aki
er,
R.,
Ga
da
lla,
T.,
an
dG
osp
od
aro
wic
z, M
.K.
Pri
nce
ss M
arg
are
t H
osp
ital
1067
2R
ece
nt
Re
sults
in
Ca
nce
rR
ese
arc
h19
9312
643
-49
Ra
dic
al
pro
sta
tect
om
y fo
r ca
rcin
om
a o
f th
ep
rost
ate
: lo
ng
-te
rm r
esu
ltsF
roh
mu
ller,
H.G
.W.,
Wir
th,
M.P
.U
rolo
gis
che
Klin
ik u
nd
Po
liklin
ik (
mu
lti-
site
)10
693
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1993
2566
1-66
7S
ho
rt-t
erm
mo
rbid
ity f
rom
CT
-pla
nn
ed
tra
nsp
eri
ne
al
I-1
25
pro
sta
te i
mp
lan
tsA
rte
rbe
ry,
V.E
., W
alln
er,
K.,
Ro
y, J
., a
nd
Fu
ks,
Z.
Me
mo
ria
l S
loa
n-K
ett
eri
ng
Ca
nce
r C
en
ter
1074
8Jo
urn
al
of
the
Na
tion
al
Me
dic
al
Ass
oci
atio
n19
9385
109-
112
Pro
sta
te c
an
cer:
re
sults
of
ext
ern
al
irra
dia
tion
Re
dd
y, E
.K.,
Kri
shn
an
, L
., G
iri,
S.,
Eva
ns,
R.G
., M
eb
ust
, W
.K.,
an
d W
eig
el,
J.W
.U
niv
ers
ity o
f K
an
sas
Me
dic
al
Ce
nte
r
1079
0Jo
urna
l of
Uro
logy
1993
149
519-
522
Pro
sta
te s
pe
cific
an
tige
n a
fte
r e
xte
rna
l b
ea
mra
dio
the
rap
y fo
r p
rost
atic
ca
nce
r: f
ollo
wu
pK
ap
lan
, I.
D.,
Co
x, R
.S.,
an
d B
ag
sha
w,
M.A
.S
tan
ford
Un
ive
rsity
Me
dic
al
Ce
nte
r
1106
2S
can
din
avi
an
Jo
urn
al
of
Uro
log
y &
Ne
ph
rolo
gy
1992
2623
1-23
4R
ad
ica
l re
tro
pu
bic
pro
sta
tect
om
y: o
ur
exp
eri
en
cew
ith t
he
fir
st 5
4 p
atie
nts
Se
rvo
ll, E
., H
alv
ors
en
, O
.J.,
Ha
uka
as,
S.,
an
d H
ois
ae
ter,
P.A
.H
au
kela
nd
Un
ive
rsity
Ho
spita
l
1110
4H
en
ry F
ord
Ho
spita
l M
ed
ica
lJo
urn
al
1992
4010
8-11
0R
ad
ica
l su
rge
ry i
n t
he
tre
atm
en
t o
f lo
caliz
ed
carc
ino
ma
of
the
pro
sta
teT
ela
ng
, D
.J.,
Mile
s, B
.J.,
Fa
rah
, R
.N.,
Litt
leto
n,
R.H
., K
irke
mo
, A
.K.,
Pe
ab
od
y,J.
O.,
Bu
rks,
D.A
., F
lem
ing
, C
., a
nd
Ce
rny,
J.C
.
He
nry
Fo
rd H
osp
ital
1110
8E
uro
pe
an
Jo
urn
al
of
Su
rgic
al
On
colo
gy
1992
1845
6-46
2R
ad
ica
l p
rost
ate
cto
my
for
loca
lize
d p
rost
ate
can
cer
Va
n-P
op
pe
l, H
., A
me
ye,
F.,
Oye
n,
R.,
Va
n-d
e-V
oo
rde
, W
., a
nd
Ba
ert
, L
.U
niv
ers
ity H
osp
itals
of
the
Ka
tho
lieke
Un
ive
rsite
it11
201
Inte
rna
tion
al
Jou
rna
l o
fR
ad
iatio
n O
nco
log
y, B
iolo
gy,
Ph
ysic
s
1992
2448
5-48
8C
on
form
al
sta
tic f
ield
ra
dia
tion
th
era
py
tre
atm
en
to
f e
arl
y p
rost
ate
ca
nce
r ve
rsu
s n
on
-co
nfo
rma
lte
chn
iqu
es:
a r
ed
uct
ion
in
acu
te m
orb
idity
So
ffe
n,
E.M
., H
an
ks,
G.E
., H
un
t, M
.A.,
an
d E
pst
ein
, B
.E.
Fo
x C
ha
se C
an
cer
Ce
nte
r
1140
0U
rolo
gy19
9240
18-2
6R
ad
iatio
n t
he
rap
y in
pro
sta
te c
an
cer:
wh
ole
pe
lvis
with
pro
sta
te b
oo
st o
r sm
all
field
to
pro
sta
te?
Plo
yso
ng
san
g,
S.S
., A
ron
, B
.S.,
an
dS
he
ha
ta,
W.M
.T
he
Ch
rist
Ho
spita
l (m
ulti
-site
)
Archived Document— For Reference Only
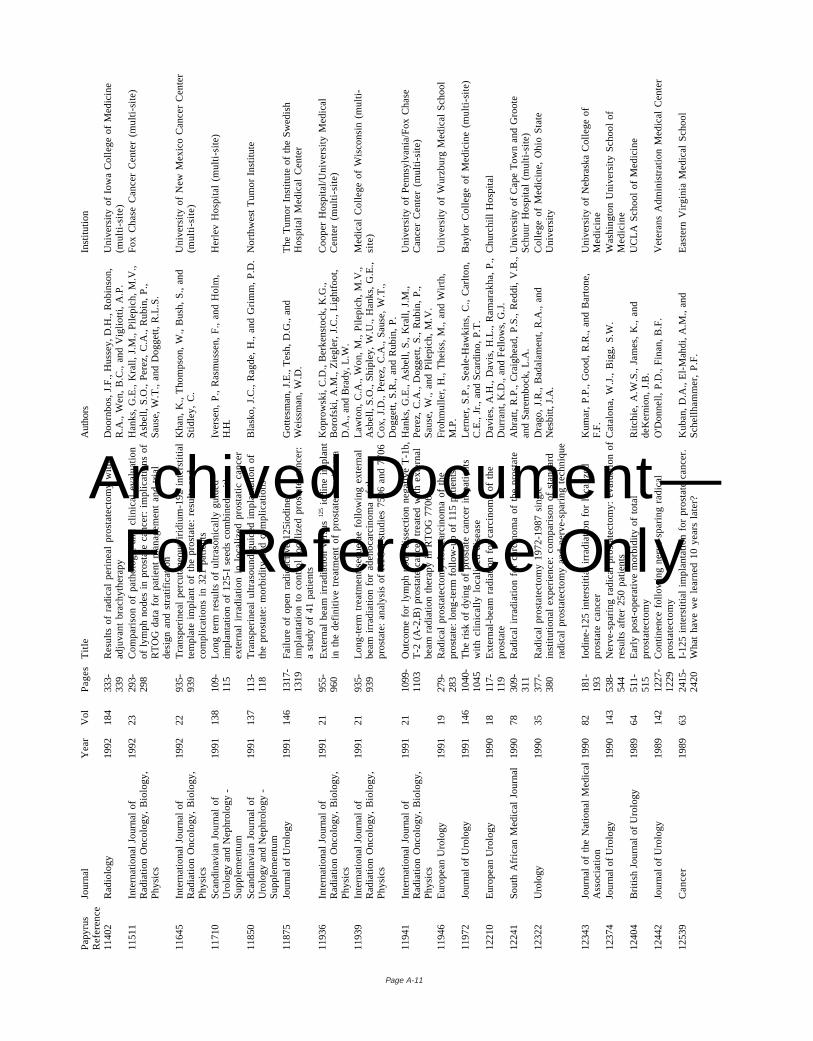
Page A-11
Pa
pyr
us
Re
fere
nce
Jou
rna
lY
ea
rV
olP
ag
es
Titl
eA
utho
rsIn
stitu
tion
1140
2R
ad
iolo
gy
1992
184
333-
339
Re
sults
of
rad
ica
l p
eri
ne
al
pro
sta
tect
om
y w
itha
dju
van
t b
rach
yth
era
py
Do
orn
bo
s, J
.F.,
Hu
sse
y, D
.H.,
Ro
bin
son
,R
.A.,
We
n,
B.C
., a
nd
Vig
liott
i, A
.P.
Un
ive
rsity
of
Iow
a C
olle
ge
of
Me
dic
ine
(mu
lti-s
ite)
1151
1In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1992
2329
3-29
8C
om
pa
riso
n o
f p
ath
olo
gic
an
d c
linic
al
eva
lua
tion
of
lym
ph
no
de
s in
pro
sta
te c
an
cer:
im
plic
atio
ns
of
RT
OG
da
ta f
or
pa
tien
t m
an
ag
em
en
t a
nd
tri
al
de
sig
n a
nd
str
atif
ica
tion
Ha
nks
, G
.E.,
Kra
ll, J
.M.,
Pile
pic
h,
M.V
.,A
sbe
ll, S
.O.,
Pe
rez,
C.A
., R
ub
in,
P.,
Sa
use
, W
.T.,
an
d D
og
ge
tt,
R.L
.S.
Fo
x C
ha
se C
an
cer
Ce
nte
r (m
ulti
-site
)
1164
5In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1992
2293
5-93
9T
ran
spe
rin
ea
l p
erc
uta
ne
ou
s ir
idiu
m-1
92
in
ters
titia
lte
mp
late
im
pla
nt
of
the
pro
sta
te:
resu
lts a
nd
com
plic
atio
ns
in 3
21
pa
tien
ts
Kh
an
, K
., T
ho
mp
son
, W
., B
ush
, S
., a
nd
Stid
ley,
C.
Un
ive
rsity
of
Ne
w M
exi
co C
an
cer
Ce
nte
r(m
ulti
-site
)
1171
0S
can
din
avi
an
Jo
urn
al
of
Uro
log
y a
nd
Ne
ph
rolo
gy
-S
up
ple
me
ntu
m
1991
138
109-
115
Lo
ng
te
rm r
esu
lts o
f u
ltra
son
ica
lly g
uid
ed
imp
lan
tatio
n o
f 1
25
-I s
ee
ds
com
bin
ed
with
ext
ern
al
irra
dia
tion
in
lo
caliz
ed
pro
sta
tic c
an
cerIv
ers
en
, P
., R
asm
uss
en
, F
., a
nd
Ho
lm,
H.H
.H
erl
ev
Ho
spita
l (m
ulti
-site
)
1185
0S
can
din
avi
an
Jo
urn
al
of
Uro
log
y a
nd
Ne
ph
rolo
gy
-S
up
ple
me
ntu
m
1991
137
113-
118
Tra
nsp
eri
ne
al
ultr
aso
un
d-g
uid
ed
im
pla
nta
tion
of
the
pro
sta
te:
mo
rbid
ity a
nd
co
mp
lica
tion
sB
lask
o,
J.C
., R
ag
de
, H
., a
nd
Gri
mm
, P
.D.
No
rth
we
st T
um
or
Inst
itute
1187
5Jo
urna
l of
Uro
logy
1991
146
1317
-13
19F
ailu
re o
f o
pe
n r
ad
ioa
ctiv
e 1
25
iod
ine
imp
lan
tatio
n t
o c
on
tro
l lo
caliz
ed
pro
sta
te c
an
cer:
a s
tud
y o
f 4
1 p
atie
nts
Go
tte
sma
n,
J.E
., T
esh
, D
.G.,
an
dW
eis
sma
n,
W.D
.T
he
Tu
mo
r In
stitu
te o
f th
e S
we
dis
hH
osp
ital
Me
dic
al
Ce
nte
r
1193
6In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1991
2195
5-96
0E
xte
rna
l b
ea
m i
rra
dia
tion
ve
rsu
s12
5 io
din
e i
mp
lan
tin
th
e d
efin
itive
tre
atm
en
t o
f p
rost
ate
ca
rcin
om
aKo
pro
wsk
i, C
.D.,
Be
rke
nst
ock
, K
.G.,
Bo
rofs
ki,
A.M
., Z
ieg
ler,
J.C
., L
igh
tfo
ot,
D.A
., a
nd
Bra
dy,
L.W
.
Co
op
er
Ho
spita
l/Un
ive
rsity
Me
dic
al
Ce
nte
r (m
ulti
-site
)
1193
9In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1991
2193
5-93
9L
on
g-t
erm
tre
atm
en
t se
qu
ela
e f
ollo
win
g e
xte
rna
lb
ea
m i
rra
dia
tion
fo
r a
de
no
carc
ino
ma
of
the
pro
sta
te:
an
aly
sis
of
RT
OG
stu
die
s 7
50
6 a
nd
77
06
La
wto
n,
C.A
., W
on
, M
., P
ilep
ich
, M
.V.,
Asb
ell,
S.O
., S
hip
ley,
W.U
., H
an
ks,
G.E
.,C
ox,
J.D
., P
ere
z, C
.A.,
Sa
use
, W
.T.,
Do
gg
ett
, S
.R.,
an
d R
ub
in,
P.
Me
dic
al
Co
lleg
e o
f W
isco
nsi
n (
mu
lti-
site
)
1194
1In
tern
atio
na
l Jo
urn
al
of
Ra
dia
tion
On
colo
gy,
Bio
log
y,P
hys
ics
1991
2110
99-
1103
Ou
tco
me
fo
r ly
mp
h n
od
e d
isse
ctio
n n
eg
ativ
e T
-1b
,T
-2 (
A-2
,B)
pro
sta
te c
an
cer
tre
ate
d w
ith e
xte
rna
lb
ea
m r
ad
iatio
n t
he
rap
y in
RT
OG
77
06
Ha
nks
, G
.E.,
Asb
ell,
S.,
Kra
ll, J
.M.,
Pe
rez,
C.A
., D
og
ge
tt,
S.,
Ru
bin
, P
.,S
au
se,
W.,
an
d P
ilep
ich
, M
.V.
Un
ive
rsity
of
Pe
nn
sylv
an
ia/F
ox
Ch
ase
Ca
nce
r C
en
ter
(mu
lti-s
ite)
1194
6E
uro
pe
an
Uro
log
y19
9119
279-
283
Ra
dic
al
pro
sta
tect
om
y fo
r ca
rcin
om
a o
f th
ep
rost
ate
: lo
ng
-te
rm f
ollo
w-u
p o
f 1
15
pa
tien
tsF
roh
mu
ller,
H.,
Th
eis
s, M
., a
nd
Wir
th,
M.P
.U
niv
ers
ity o
f W
urz
bu
rg M
ed
ica
l S
cho
ol
1197
2Jo
urna
l of
Uro
logy
1991
146
1040
-10
45T
he
ris
k o
f d
yin
g o
f p
rost
ate
ca
nce
r in
pa
tien
tsw
ith c
linic
ally
lo
caliz
ed
dis
ea
seL
ern
er,
S.P
., S
ea
le-H
aw
kin
s, C
., C
arl
ton
,C
.E.,
Jr.
, a
nd
Sca
rdin
o,
P.T
.B
ayl
or
Co
lleg
e o
f M
ed
icin
e (
mu
lti-s
ite)
1221
0E
uro
pe
an
Uro
log
y19
9018
117-
119
Ext
ern
al-
be
am
ra
dia
tion
fo
r ca
rcin
om
a o
f th
ep
rost
ate
Da
vie
s, A
.H.,
Da
vis,
H.L
., R
am
ara
kha
, P
.,D
urr
an
t, K
.D.,
an
d F
ello
ws,
G.J
.C
hu
rch
ill H
osp
ital
1224
1S
ou
th A
fric
an
Me
dic
al
Jou
rna
l199
078
309-
311
Ra
dic
al
irra
dia
tion
fo
r ca
rcin
om
a o
f th
e p
rost
ateA
bra
tt,
R.P
., C
raig
he
ad
, P
.S.,
Re
dd
i, V
.B.,
an
d S
are
mb
ock
, L
.A.
Un
ive
rsity
of
Ca
pe
To
wn
an
d G
roo
teS
chu
ur
Ho
spita
l (m
ulti
-site
)12
322
Uro
logy
1990
3537
7-38
0R
ad
ica
l p
rost
ate
cto
my
19
72
-19
87
sin
gle
inst
itutio
na
l e
xpe
rie
nce
: co
mp
ari
son
of
sta
nd
ard
rad
ica
l p
rost
ate
cto
my
an
d n
erv
e-s
pa
rin
g t
ech
niq
ue
Dra
go
, J.
R.,
Ba
da
lam
en
t, R
.A.,
an
dN
esbi
tt, J
.A.
Co
lleg
e o
f M
ed
icin
e,
Oh
io S
tate
Un
ive
rsity
1234
3Jo
urn
al
of
the
Na
tion
al
Me
dic
al
Ass
oci
atio
n19
9082
181-
193
Iod
ine
-12
5 i
nte
rstit
ial
irra
dia
tion
fo
r lo
caliz
ed
pro
sta
te c
an
cer
Ku
ma
r, P
.P.,
Go
od
, R
.R.,
an
d B
art
on
e,
F.F
.U
niv
ers
ity o
f N
eb
rask
a C
olle
ge
of
Me
dic
ine
1237
4Jo
urna
l of
Uro
logy
1990
143
538-
544
Ne
rve
-sp
ari
ng
ra
dic
al
pro
sta
tect
om
y: e
valu
atio
n o
fre
sults
aft
er
25
0 p
atie
nts
Ca
talo
na
, W
.J.,
Big
g,
S.W
.W
ash
ing
ton
Un
ive
rsity
Sch
oo
l o
fM
ed
icin
e12
404
Bri
tish
Jo
urn
al o
f U
rolo
gy
1989
6451
1-51
5E
arl
y p
ost
-op
era
tive
mo
rbid
ity o
f to
tal
pro
sta
tect
om
yR
itch
ie,
A.W
.S.,
Ja
me
s, K
., a
nd
de
Ke
rnio
n,
J.B
.U
CL
A S
cho
ol
of
Me
dic
ine
1244
2Jo
urna
l of
Uro
logy
1989
142
1227
-12
29C
on
tine
nce
fo
llow
ing
ne
rve
-sp
ari
ng
ra
dic
al
pro
sta
tect
om
yO
'Do
nn
ell,
P.D
., F
ina
n,
B.F
.V
ete
ran
s A
dm
inis
tra
tion
Me
dic
al
Ce
nte
r
1253
9C
an
cer
1989
6324
15-
2420
I-1
25
in
ters
titia
l im
pla
nta
tion
fo
r p
rost
ate
ca
nce
r.W
ha
t h
ave
we
le
arn
ed
10
ye
ars
la
ter?
Ku
ba
n,
D.A
., E
l-M
ah
di,
A.M
., a
nd
Sch
ellh
am
me
r, P
.F.
Ea
ste
rn V
irg
inia
Me
dic
al
Sch
oo
l
Archived Document— For Reference Only
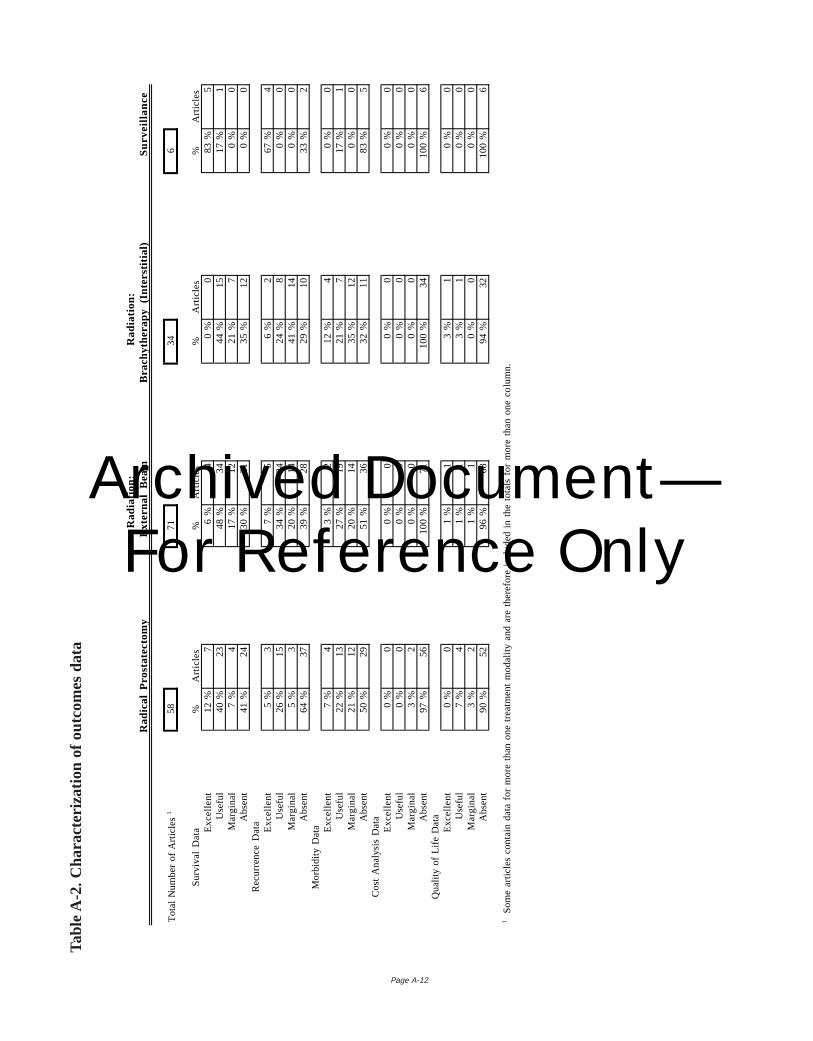
Page A-12
Ra
dia
tion
:R
ad
iatio
n:
R
ad
ica
l P
rost
ate
cto
my
Ext
ern
al
Be
am
Bra
chyt
he
rap
y (I
nte
rstit
ial)
Su
rve
illa
nce
To
tal
Nu
mb
er
of
Art
icle
s158
7134
6
Su
rviv
al
Da
ta%
Art
icle
s%
Art
icle
s%
Art
icle
s%
Art
icle
sE
xce
llen
t1
2 %
76
%4
0 %
08
3 %
5U
sefu
l4
0 %
234
8 %
344
4 %
151
7 %
1M
arg
ina
l7
%4
17
%12
21
%7
0 %
0A
bse
nt
41
%24
30
%21
35
%12
0 %
0R
ecu
rre
nce
Da
taE
xce
llen
t5
%3
7 %
56
%2
67
%4
Use
ful
26
%15
34
%24
24
%8
0 %
0M
arg
ina
l5
%3
20
%14
41
%14
0 %
0A
bse
nt
64
%37
39
%28
29
%10
33
%2
Mo
rbid
ity D
ata E
xce
llen
t7
%4
3 %
21
2 %
40
%0
Use
ful
22
%13
27
%19
21
%7
17
%1
Ma
rgin
al
21
%12
20
%14
35
%12
0 %
0A
bse
nt
50
%29
51
%36
32
%11
83
%5
Co
st A
na
lysi
s D
ata
Exc
elle
nt
0 %
00
%0
0 %
00
%0
Use
ful
0 %
00
%0
0 %
00
%0
Ma
rgin
al
3 %
20
%0
0 %
00
%0
Ab
sen
t9
7 %
561
00
%71
10
0 %
341
00
%6
Qu
alit
y o
f L
ife D
ata
Exc
elle
nt
0 %
01
%1
3 %
10
%0
Use
ful
7 %
41
%1
3 %
10
%0
Ma
rgin
al
3 %
21
%1
0 %
00
%0
Ab
sen
t9
0 %
529
6 %
689
4 %
321
00
%6
1 S
om
e a
rtic
les
con
tain
da
ta f
or
mo
re t
ha
n o
ne
tre
atm
en
t m
od
alit
y a
nd
are
th
ere
fore
in
clu
de
d i
n t
he
to
tals
fo
r m
ore
th
an
on
e c
olu
mn
.
Tabl
e A
-2.
Cha
ract
eriz
atio
n of
out
com
es d
ata
Archived Document— For Reference Only
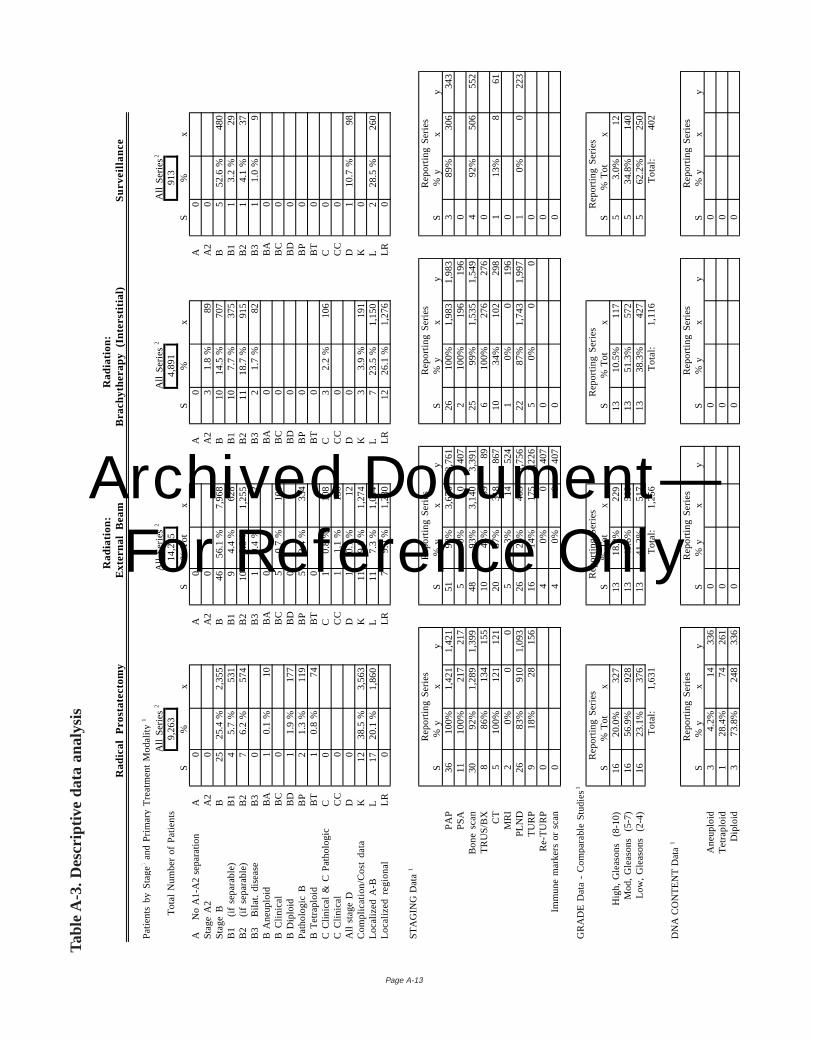
Ra
dia
tion
:R
ad
iatio
n:
Ra
dic
al
Pro
sta
tect
om
yE
xte
rna
l B
ea
mB
rach
yth
era
py
(In
ters
titia
l)S
urv
eill
an
ce
Pa
tien
ts b
y S
tag
e3 a
nd
Pri
ma
ry T
rea
tme
nt
Mo
da
lity1
All
Se
rie
s2
All
Se
rie
s2
All
Se
rie
s2
All
Se
rie
s 2
To
tal
Nu
mb
er
of
Pa
tien
ts9
,26
31
4,2
05
4,8
91
913
S%
xS
% T
ot
xS
%x
S%
xA
No
A1
-A2
se
pa
ratio
nA
0A
0A
0A
0S
tag
e A
2A
20
A2
0A
23
1.8
%89
A2
0S
tag
e B
B25
25
.4 %
2,3
55
B46
56
.1 %
7,9
68
B10
14
.5 %
707
B5
52
.6 %
480
B1
(
if se
pa
rab
le)
B1
45
.7 %
531
B1
94
.4 %
628
B1
107
.7 %
375
B1
13
.2 %
29B
2
(if
sep
ara
ble
)B
27
6.2
%57
4B
210
8.8
%1
,25
5B
211
18
.7 %
915
B2
14
.1 %
37B
3
Bila
t. d
ise
ase
B3
0B
31
0.4
%52
B3
21
.7 %
82B
31
1.0
%9
B A
ne
up
loid
BA
10
.1 %
10B
A0
BA
0B
A0
B C
linic
al
BC
0B
C5
0.7
%1
00
BC
0B
C0
B D
iplo
idB
D1
1.9
%1
77
BD
0B
D0
BD
0P
ath
olo
gic
BB
P2
1.3
%11
9B
P5
2.4
%33
4B
P0
BP
0B
Te
tra
plo
idB
T1
0.8
%74
BT
0B
T0
BT
0C
Clin
ica
l &
C P
ath
olo
gic
C0
C1
0.8
%10
8C
32
.2 %
106
C0
C C
linic
al
CC
0C
C1
1.1
%1
50
CC
0C
C0
All
sta
ge
DD
0D
10
.1 %
12D
0D
11
0.7
%98
Co
mp
lica
tion
/Co
st d
ata
K12
38
.5 %
3,5
63
K11
9.0
%1
,27
4K
33
.9 %
191
K0
Lo
caliz
ed
A-B
L17
20
.1 %
1,8
60
L11
7.3
%1
,04
4L
72
3.5
%1
,15
0L
22
8.5
%26
0L
oca
lize
d r
eg
ion
al
LR
0L
R7
9.0
%1
,28
0L
R12
26
.1 %
1,2
76
LR
0
ST
AG
ING
Da
ta1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
yx
yS
% y
xy
S%
yx
yS
% y
xy
PA
P36
10
0%
1,4
21
1,4
21
519
8%
3,6
76
3,7
61
261
00
%1
,98
31
,98
33
89
%30
634
3P
SA
111
00
%21
721
75
0%
040
72
10
0%
196
196
0B
on
e s
can
309
2%
1,2
89
1,3
99
489
3%
3,1
40
3,3
91
259
9%
1,5
35
1,5
49
49
2%
506
552
TR
US
/BX
88
6%
134
155
104
4%
3989
61
00
%27
627
60
CT
51
00
%12
112
120
37
%31
886
710
34
%10
229
81
13
%8
61M
RI
20
%0
05
3%
1452
41
0%
019
60
PLN
D26
83
%91
01
,09
326
26
%46
31
,75
622
87
%1
,74
31
,99
71
0%
022
3T
UR
P9
18
%28
156
161
4%
175
1,2
26
50
%0
00
Re
-TU
RP
04
0%
040
70
0Im
mu
ne
ma
rke
rs o
r sc
an
04
0%
040
70
0
GR
AD
E D
ata
- C
om
pa
rab
le S
tud
ies
1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
To
tx
S%
To
tx
S%
To
tx
S%
To
tx
Hig
h,
Gle
aso
ns
(8
-10
)1
62
0.0
%3
27
13
18
.2%
22
91
31
0.5
%1
17
53
.0%
12
Mo
d,
Gle
aso
ns
(5
-7)
165
6.9
%92
813
40
.6%
510
135
1.3
%57
25
34
.8%
140
Lo
w,
Gle
aso
ns
(2
-4)
16
23
.1%
37
61
34
1.2
%5
17
13
38
.3%
42
75
62
.2%
25
0T
ota
l:1
,63
1T
ota
l:1
,25
6T
ota
l:1
,11
6T
ota
l:40
2
DN
A C
ON
TE
NT
Da
ta1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
yx
yS
% y
xy
S%
yx
yS
% y
xy
An
eu
plo
id3
4.2
%14
336
00
0T
etr
ap
loid
12
8.4
%74
261
00
0D
iplo
id3
73
.8%
24
83
36
00
0
Page A-13
Tabl
e A
-3.
Des
crip
tive
data
ana
lysi
s
Archived Document— For Reference Only
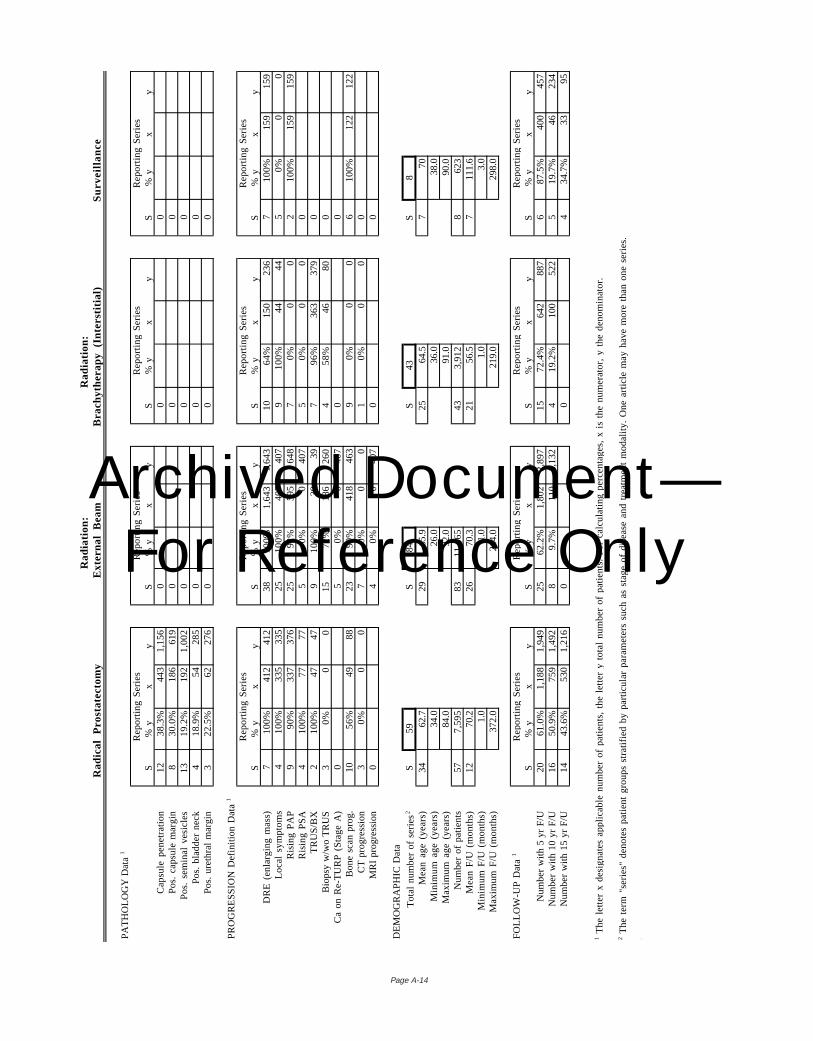
Page A-14
Ra
dia
tion
:R
ad
iatio
n:
Ra
dic
al
Pro
sta
tect
om
yE
xte
rna
l B
ea
mB
rach
yth
era
py
(In
ters
titia
l)S
urv
eill
an
ce
PA
TH
OL
OG
Y D
ata
1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
yx
yS
% y
xy
S%
yx
yS
% y
xy
Ca
psu
le p
en
etr
atio
n12
38
.3%
443
1,1
56
00
0P
os.
ca
psu
le m
arg
in8
30
.0%
186
619
00
0P
os.
se
min
al
vesi
cle
s13
19
.2%
192
1,0
02
00
0P
os.
bla
dd
er
ne
ck4
18
.9%
5428
50
00
Po
s. u
reth
ral
ma
rgin
32
2.5
%6
22
76
00
0
PR
OG
RE
SS
ION
De
finiti
on
Da
ta1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
yx
yS
% y
xy
S%
yx
yS
% y
xy
DR
E (
en
larg
ing
ma
ss)
71
00
%41
241
238
10
0%
1,6
43
1,6
43
106
4%
150
236
71
00
%15
915
9L
oca
l sy
mp
tom
s4
10
0%
335
335
251
00
%40
740
79
10
0%
4444
50
%0
0R
isin
g P
AP
99
0%
337
376
259
2%
595
648
70
%0
02
10
0%
159
159
Ris
ing
PS
A4
10
0%
7777
50
%0
407
50
%0
00
TR
US
/BX
21
00
%47
479
10
0%
3939
79
6%
363
379
0B
iop
sy w
/wo
TR
US
30
%0
015
72
%1
86
26
04
58
%4
68
00
Ca
on
Re
-TU
RP
(S
tag
e A
)0
50
%0
407
00
Bo
ne
sca
n p
rog
.10
56
%49
8823
90
%41
846
39
0%
00
61
00
%12
212
2C
T p
rog
ress
ion
30
%0
07
0%
00
10
%0
00
MR
I p
rog
ress
ion
04
0%
04
07
00
DE
MO
GR
AP
HIC
Da
ta
To
tal
nu
mb
er
of
seri
es
2S
59S
84S
43S
8M
ea
n a
ge
(ye
ars
)34
62.7
2965
.925
64.5
770
Min
imu
m a
ge
(ye
ars
)34
.026
.036
.038
.0M
axi
mu
m a
ge
(ye
ars
)84
.092
.091
.090
.0N
um
be
r o
f p
atie
nts
577
,59
583
11
,46
543
3,9
12
862
3M
ea
n F
/U (
mo
nth
s)12
70.2
2670
.321
56.5
711
1.6
Min
imu
m F
/U (
mo
nth
s)1.
01.
01.
03.
0M
axi
mu
m F
/U (
mo
nth
s)37
2.0
264.
021
9.0
298.
0
FO
LL
OW
-UP
Da
ta1
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
Re
po
rtin
g S
eri
es
S%
yx
yS
% y
xy
S%
yx
yS
% y
xy
Nu
mb
er
with
5 y
r F
/U20
61
.0%
1,1
88
1,9
49
256
2.2
%1
,80
22
,89
715
72
.4%
642
887
68
7.5
%40
045
7N
um
be
r w
ith 1
0 y
r F
/U16
50
.9%
759
1,4
92
89
.7%
110
1,1
32
41
9.2
%10
052
25
19
.7%
4623
4N
um
be
r w
ith 1
5 y
r F
/U14
43
.6%
530
1,2
16
00
43
4.7
%33
95
1 Th
e l
ett
er
x d
esi
gn
ate
s a
pp
lica
ble
nu
mb
er
of
pa
tien
ts,
the
le
tte
r y
tota
l n
um
be
r o
f p
atie
nts
. F
or
calc
ula
ting
pe
rce
nta
ge
s, x
is
the
nu
me
rato
r, y
th
e d
en
om
ina
tor.
2 Th
e t
erm
"se
rie
s" d
en
ote
s p
atie
nt
gro
up
s st
ratif
ied
by
pa
rtic
ula
r p
ara
me
ters
su
ch a
s st
ag
e o
f d
ise
ase
an
d t
rea
tme
nt
mo
da
lity.
On
e a
rtic
le m
ay
ha
ve m
ore
th
an
on
e s
eri
es.
3 Th
e s
tag
e c
od
es
for
this
da
tab
ase
are
:A
A (
No
A1
-A2
se
pa
ratio
n)
B3
B3
(B
ilat.
dis
ea
se)
BT
(B
Te
tra
plo
id)
L (
Lo
caliz
ed
A-B
)A
2 (
Sta
ge
A2
)B
A B
(A
ne
up
loid
)C
(C
Clin
ica
l &
C P
ath
olo
gic
)L
R (
Lo
caliz
ed
re
gio
na
l)B
(S
tag
e B
)B
C (
B C
linic
al)
CC
(C
Clin
ica
l)O
Oth
er,
de
fine
:B
1 B
1 (
if se
pa
rab
le)
BD
(B
Dip
loid
)D
(A
ll st
ag
e D
)R
Re
curr
en
ce-e
.g.,
fo
llow
ing
tre
atm
en
t b
y R
RP
or
RT
B2
B2
(if
sep
ara
ble
)B
P (
Pa
tho
log
ic B
)K
(C
om
plic
atio
n/C
ost
da
ta)
U U
nkno
wn
Archived Document— For Reference Only
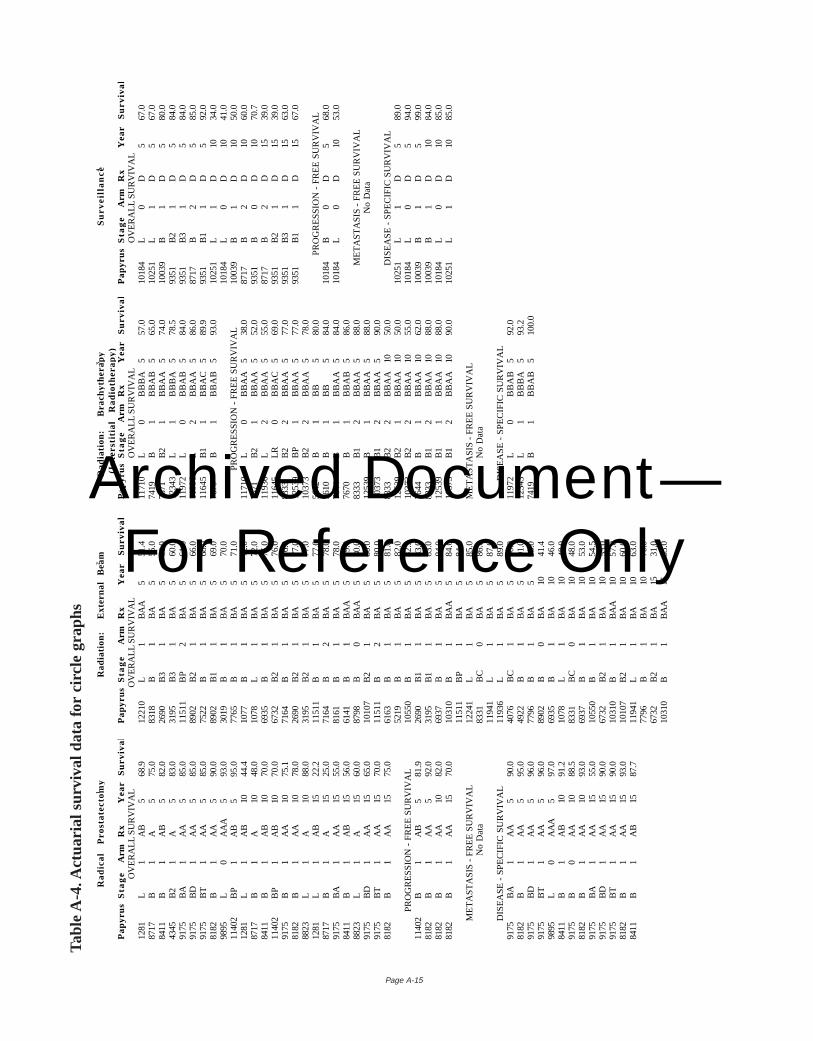
Page A-15
Ra
dic
al
Pro
sta
tect
om
y 1
Ra
dia
tio
n:
E
xte
rna
l B
ea
m2
Ra
dia
tio
n:
B
rach
yth
era
py
3S
urv
eil
lan
ce4
(In
ters
titi
al
Ra
dio
the
rap
y)P
ap
yru
sS
tag
eA
rmR
xY
ea
rS
urv
iva
lP
ap
yru
sS
tag
eA
rmR
xY
ea
rS
urv
iva
lP
ap
yru
sS
tag
eA
rmR
xY
ea
rS
urv
iva
lP
ap
yru
sS
tag
eA
rmR
xY
ea
rS
urv
iva
lO
VE
RA
LL S
UR
VIV
AL
OV
ER
ALL
SU
RV
IVA
LO
VE
RA
LL S
UR
VIV
AL
OV
ER
ALL
SU
RV
IVA
L12
81L
1A
B5
68.9
1221
0L
1B
AA
551
.411
710
L0
BB
BA
557
.010
184
L0
D5
67.0
8717
B1
A5
75.0
8318
B1
BA
555
.074
19B
1B
BA
B5
65.0
1025
1L
1D
567
.084
11B
1A
B5
82.0
2690
B3
1B
A5
60.0
7671
B2
1B
BA
A5
74.0
1003
9B
1D
580
.043
45B
21
A5
83.0
3195
B3
1B
A5
60.0
1234
3L
1B
BB
A5
78.5
9351
B2
1D
584
.091
75B
A1
AA
585
.011
511
BP
2B
A5
61.0
1197
2L
0B
BA
B5
84.0
9351
B3
1D
584
.091
75B
D1
AA
585
.089
02B
21
BA
566
.011
936
L2
BB
AA
586
.087
17B
2D
585
.091
75B
T1
AA
585
.075
22B
1B
A5
68.0
1164
5B
11
BB
AC
589
.993
51B
11
D5
92.0
8182
B1
AA
590
.089
02B
11
BA
569
.076
70B
1B
BA
B5
93.0
1025
1L
1D
1034
.098
95L
0A
AA
593
.030
19B
1B
A5
70.0
1018
4L
0D
1041
.011
402
BP
1A
B5
95.0
7765
B1
BA
571
.0P
RO
GR
ES
SIO
N -
FR
EE
SU
RV
IVA
L10
039
B1
D10
50.0
1281
L1
AB
1044
.410
77B
1B
A5
72.0
1171
0L
0B
BA
A5
38.0
8717
B2
D10
60.0
8717
B1
A10
48.0
1078
L1
BA
572
.076
71B
21
BB
AA
552
.093
51B
0D
1070
.784
11B
1A
B10
70.0
6935
B1
BA
575
.011
936
L2
BB
AA
555
.087
17B
2D
1539
.011
402
BP
1A
B10
70.0
6732
B2
1B
A5
76.0
1164
5LR
0B
BA
C5
69.0
9351
B2
1D
1539
.091
75B
1A
A10
75.1
7164
B1
BA
576
.083
33B
22
BB
AA
577
.093
51B
31
D15
63.0
8182
B1
AA
1078
.026
90B
21
BA
577
.012
539
BP
1B
BA
A5
77.0
9351
B1
1D
1567
.088
23L
1A
1088
.031
95B
21
BA
577
.010
373
B2
2B
BA
A5
78.0
1281
L1
AB
1522
.211
511
B1
BA
577
.056
42B
1B
B5
80.0
PR
OG
RE
SS
ION
- F
RE
E S
UR
VIV
AL
8717
B1
A15
25.0
7164
B2
BA
578
.056
10B
1B
B5
84.0
1018
4B
0D
568
.091
75B
A1
AA
1555
.081
61B
1B
A5
78.0
7644
B1
BB
AA
584
.010
184
L0
D10
53.0
8411
B1
AB
1556
.061
41B
1B
AA
579
.076
70B
1B
BA
B5
86.0
8823
L1
A15
60.0
8798
B0
BA
A5
80.0
8333
B1
2B
BA
A5
88.0
ME
TA
ST
AS
IS -
FR
EE
SU
RV
IVA
L91
75B
D1
AA
1565
.010
107
B2
1B
A5
80.0
1253
9B
1B
BA
A5
88.0
No
Da
ta91
75B
T1
AA
1570
.011
511
B2
BA
580
.010
373
B1
2B
BA
A5
90.0
8182
B1
AA
1575
.061
63B
1B
A5
81.0
8333
B2
2B
BA
A10
50.0
DIS
EA
SE
- S
PE
CIF
IC S
UR
VIV
AL
5219
B1
BA
582
.012
539
B2
1B
BA
A10
50.0
1025
1L
1D
589
.0P
RO
GR
ES
SIO
N -
FR
EE
SU
RV
IVA
L10
550
B1
BA
582
.910
373
B2
2B
BA
A10
55.0
1018
4L
0D
594
.011
402
B1
AB
581
.926
90B
11
BA
583
.076
44B
1B
BA
A10
62.0
1003
9B
1D
599
.081
82B
1A
A5
92.0
3195
B1
1B
A5
83.0
8333
B1
2B
BA
A10
88.0
1003
9B
1D
1084
.081
82B
1A
A10
82.0
6937
B1
BA
584
.012
539
B1
1B
BA
A10
88.0
1018
4L
0D
1085
.081
82B
1A
A15
70.0
1031
0B
1B
AA
584
.010
373
B1
2B
BA
A10
90.0
1025
1L
1D
1085
.011
511
BP
1B
A5
84.0
ME
TA
ST
AS
IS -
FR
EE
SU
RV
IVA
L12
241
L1
BA
585
.0M
ET
AS
TA
SIS
- F
RE
E S
UR
VIV
AL
No
Da
ta83
31B
C0
BA
586
.0N
o Da
ta11
941
L1
BA
587
.0D
ISE
AS
E -
SP
EC
IFIC
SU
RV
IVA
L11
936
L1
BA
589
.0D
ISE
AS
E -
SP
EC
IFIC
SU
RV
IVA
L91
75B
A1
AA
590
.040
76B
C1
BA
590
.011
972
L0
BB
AB
592
.081
82B
1A
A5
95.0
4922
B1
BA
591
.012
343
L1
BB
BA
593
.291
75B
D1
AA
596
.077
96B
1B
A5
93.0
7419
B1
BB
AB
510
0.0
9175
BT
1A
A5
96.0
8902
B0
BA
1041
.498
95L
0A
AA
597
.069
35B
1B
A10
46.0
8411
B1
AB
1091
.210
78L
1B
A10
48.0
9175
B0
AA
1088
.583
31B
C0
BA
1048
.081
82B
1A
A10
93.0
6937
B1
BA
1053
.091
75B
A1
AA
1555
.010
550
B1
BA
1054
.591
75B
D1
AA
1590
.067
32B
21
BA
1055
.091
75B
T1
AA
1590
.010
310
B1
BA
A10
57.0
8182
B1
AA
1593
.010
107
B2
1B
A10
60.0
8411
B1
AB
1587
.711
941
L1
BA
1063
.077
96B
1B
A10
70.0
6732
B2
1B
A15
31.0
1031
0B
1B
AA
1533
.0
Tabl
e A
-4. A
ctua
rial s
urvi
val d
ata
for
circ
le g
raph
s
Archived Document— For Reference Only
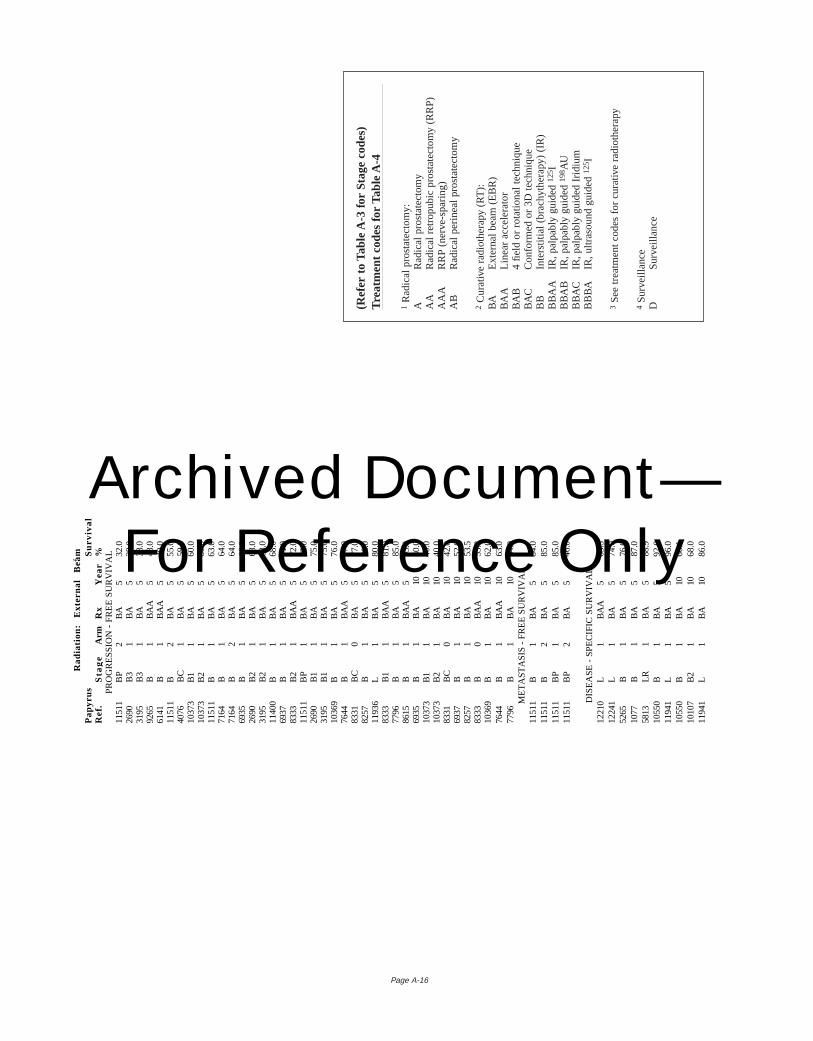
Page A-16
Ra
dia
tio
n:
Ext
ern
al
Be
am
2
Pa
pyr
us
Re
f.S
tag
eA
rmR
xY
ea
rS
urv
iva
l%
PR
OG
RE
SS
ION
- F
RE
E S
UR
VIV
AL
1151
1B
P2
BA
532
.026
90B
31
BA
538
.031
95B
31
BA
538
.092
65B
1B
AA
548
.061
41B
1B
AA
549
.011
511
B2
BA
555
.040
76B
C1
BA
559
.010
373
B1
1B
A5
60.0
1037
3B
21
BA
560
.011
511
B1
BA
563
.071
64B
1B
A5
64.0
7164
B2
BA
564
.069
35B
1B
A5
66.0
2690
B2
1B
A5
68.0
3195
B2
1B
A5
68.0
1140
0B
1B
A5
68.0
6937
B1
BA
571
.083
33B
21
BA
A5
72.0
1151
1B
P1
BA
572
.026
90B
11
BA
575
.031
95B
11
BA
575
.010
369
B1
BA
576
.076
44B
1B
AA
577
.083
31B
C0
BA
577
.082
57B
1B
A5
78.0
1193
6L
1B
A5
80.0
8333
B1
1B
AA
581
.077
96B
1B
A5
85.0
8615
B1
BA
A5
93.0
6935
B1
BA
1040
.010
373
B1
1B
A10
40.0
1037
3B
21
BA
1040
.083
31B
C0
BA
1042
.069
37B
1B
A10
52.0
8257
B1
BA
1053
.583
33B
0B
AA
1053
.810
369
B1
BA
1062
.076
44B
1B
AA
1063
.077
96B
1B
A10
64.0
ME
TA
ST
AS
IS -
FR
EE
SU
RV
IVA
L11
511
B1
BA
584
.011
511
B2
BA
585
.011
511
BP
1B
A5
85.0
1151
1B
P2
BA
546
.0
DIS
EA
SE
- S
PE
CIF
IC S
UR
VIV
AL
1221
0L
1B
AA
563
.512
241
L1
BA
574
.052
65B
1B
A5
76.0
1077
B1
BA
587
.058
13LR
1B
A5
88.9
1055
0B
1B
A5
92.0
1194
1L
1B
A5
96.0
1055
0B
1B
A10
66.1
1010
7B
21
BA
1068
.011
941
L1
BA
1086
.0
(Ref
er t
o Ta
ble
A-3
for
Sta
ge c
odes
)Tr
eatm
ent
code
s fo
r Ta
ble
A-4
1R
adic
al p
rost
atec
tom
y:A
Rad
ical
pro
stat
ecto
my
AA
Rad
ical
ret
ropu
bic
pros
tate
ctom
y (R
RP
)A
AA
RR
P(n
erve
-spa
ring)
AB
Rad
ical
per
inea
l pro
stat
ecto
my
2C
urat
ive
radi
othe
rapy
(RT
):B
AE
xter
nal b
eam
(E
BR
)B
AA
Line
ar a
ccel
erat
orB
AB
4 fie
ld o
r ro
tatio
nal t
echn
ique
BA
CC
onfo
rmed
or
3D t
echn
ique
BB
Inte
rstit
ial (
brac
hyth
erap
y) (
IR)
BB
AA
IR,p
alpa
bly
guid
ed 12
5 IB
BA
BIR
,pal
pabl
y gu
ided
198 A
UB
BA
CIR
,pal
pabl
y gu
ided
Irid
ium
BB
BA
IR,u
ltras
ound
gui
ded 12
5 I
3S
ee t
reat
men
t co
des
for
cura
tive
radi
othe
rapy
4S
urve
illan
ceD
Sur
veill
ance
Archived Document— For Reference Only
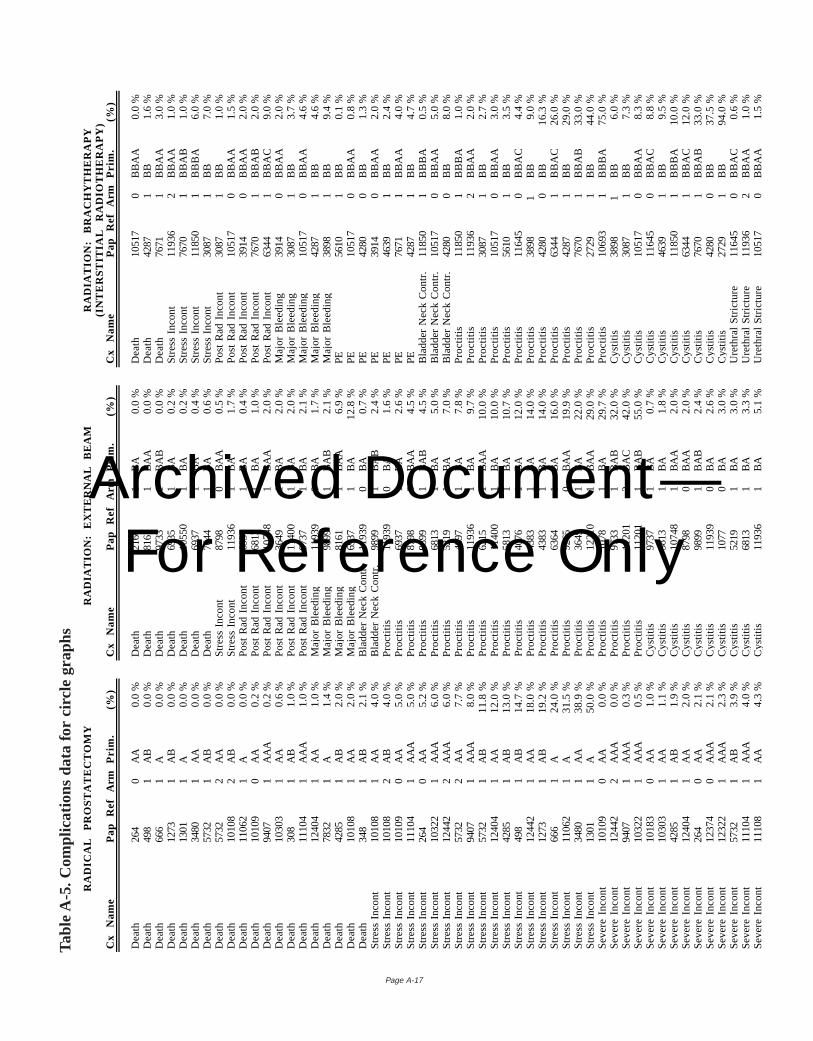
Page A-17
RA
DIC
AL
P
RO
ST
AT
EC
TO
MY
RA
DIA
TIO
N:
EX
TE
RN
AL
B
EA
MR
AD
IAT
ION
: B
RA
CH
YT
HE
RA
PY
(IN
TE
RS
TIT
IAL
R
AD
IOT
HE
RA
PY
)C
x N
am
eP
ap
R
ef
Arm
Pri
m.
(%)
Cx
Na
me
Pa
p
Re
fA
rmP
rim
.(%
)C
x N
am
eP
ap
R
ef
Arm
Pri
m.
(%)
De
ath
264
0A
A0.
0 %
De
ath
2160
1B
A0.
0 %
De
ath
1051
70
BB
AA
0.0
%D
ea
th49
81
AB
0.0
%D
ea
th81
611
BA
A0.
0 %
De
ath
4287
1B
B1.
6 %
De
ath
666
1A
0.0
%D
ea
th97
331
BA
B0.
0 %
De
ath
7671
1B
BA
A3.
0 %
De
ath
1273
1A
B0.
0 %
De
ath
6935
1B
A0
.2 %
Str
ess
In
con
t11
936
2B
BA
A1.
0 %
De
ath
1301
1A
0.0
%D
ea
th10
550
1B
A0
.2 %
Str
ess
In
con
t76
701
BB
AB
1.0
%D
ea
th34
801
AA
0.0
%D
ea
th69
371
BA
0.4
%S
tre
ss I
nco
nt
1185
01
BB
BA
6.0
%D
ea
th57
321
AB
0.0
%D
ea
th76
441
BA
0.6
%S
tre
ss I
nco
nt
3087
1B
B7.
0 %
De
ath
5732
2A
A0
.0 %
Str
ess
In
con
t87
980
BA
A0
.5 %
Po
st R
ad
In
con
t30
871
BB
1.0
%D
ea
th10
108
2A
B0
.0 %
Str
ess
In
con
t11
936
1B
A1
.7 %
Po
st R
ad
In
con
t10
517
0B
BA
A1.
5 %
De
ath
1106
21
A0
.0 %
Po
st R
ad
In
con
t69
371
BA
0.4
%P
ost
Ra
d I
nco
nt
3914
0B
BA
A2.
0 %
De
ath
1010
90
AA
0.2
%P
ost
Ra
d I
nco
nt
6813
1B
A1
.0 %
Po
st R
ad
In
con
t76
701
BB
AB
2.0
%D
ea
th94
071
AA
A0
.2 %
Po
st R
ad
In
con
t10
748
1B
AA
2.0
%P
ost
Ra
d I
nco
nt
6344
1B
BA
C9.
0 %
De
ath
1030
31
AA
0.6
%P
ost
Ra
d I
nco
nt
3649
1B
A2
.0 %
Ma
jor
Ble
ed
ing
3914
0B
BA
A2.
0 %
De
ath
308
1A
B1
.0 %
Po
st R
ad
In
con
t11
400
1B
A2
.0 %
Ma
jor
Ble
ed
ing
3087
1B
B3.
7 %
De
ath
1110
41
AA
A1
.0 %
Po
st R
ad
In
con
t97
371
BA
2.1
%M
ajo
r B
lee
din
g10
517
0B
BA
A4.
6 %
De
ath
1240
41
AA
1.0
%M
ajo
r B
lee
din
g11
939
0B
A1
.7 %
Ma
jor
Ble
ed
ing
4287
1B
B4.
6 %
De
ath
7832
1A
1.4
%M
ajo
r B
lee
din
g98
991
BA
B2
.1 %
Ma
jor
Ble
ed
ing
3898
1B
B9.
4 %
De
ath
4285
1A
B2
.0 %
Ma
jor
Ble
ed
ing
8161
1B
AA
6.9
%P
E56
101
BB
0.1
%D
ea
th10
108
1A
A2
.0 %
Ma
jor
Ble
ed
ing
6937
1B
A1
2.8
%P
E10
517
0B
BA
A0.
8 %
De
ath
348
1A
B2
.1 %
Bla
dd
er
Ne
ck C
on
tr.
1193
90
BA
0.7
%P
E42
800
BB
1.3
%S
tre
ss I
nco
nt
1010
81
AA
4.0
%B
lad
de
r N
eck
Co
ntr
.98
991
BA
B2.
4 %
PE
3914
0B
BA
A2.
0 %
Str
ess
In
con
t10
108
2A
B4.
0 %
Pro
ctiti
s11
939
0B
A1.
6 %
PE
4639
1B
B2.
4 %
Str
ess
In
con
t10
109
0A
A5.
0 %
Pro
ctiti
s69
371
BA
2.6
%P
E76
711
BB
AA
4.0
%S
tre
ss I
nco
nt
1110
41
AA
A5.
0 %
Pro
ctiti
s87
980
BA
A4.
5 %
PE
4287
1B
B4.
7 %
Str
ess
In
con
t26
40
AA
5.2
%P
roct
itis
9899
1B
AB
4.5
%B
lad
de
r N
eck
Co
ntr
.11
850
1B
BB
A0.
5 %
Str
ess
In
con
t10
322
1A
AA
6.0
%P
roct
itis
6813
1B
A5
.0 %
Bla
dd
er
Ne
ck C
on
tr.
1051
70
BB
AA
5.0
%S
tre
ss I
nco
nt
1244
22
AA
A6.
0 %
Pro
ctiti
s52
191
BA
7.0
%B
lad
de
r N
eck
Co
ntr
.42
800
BB
8.0
%S
tre
ss I
nco
nt
5732
2A
A7.
7 %
Pro
ctiti
s48
971
BA
7.8
%P
roct
itis
1185
01
BB
BA
1.0
%S
tre
ss I
nco
nt
9407
1A
AA
8.0
%P
roct
itis
1193
61
BA
9.7
%P
roct
itis
1193
62
BB
AA
2.0
%S
tre
ss I
nco
nt
5732
1A
B1
1.8
%P
roct
itis
6215
1B
AA
10
.0 %
Pro
ctiti
s30
871
BB
2.7
%S
tre
ss I
nco
nt
1240
41
AA
12
.0 %
Pro
ctiti
s11
400
1B
A1
0.0
%P
roct
itis
1051
70
BB
AA
3.0
%S
tre
ss I
nco
nt
4285
1A
B1
3.0
%P
roct
itis
5813
1B
A1
0.7
%P
roct
itis
5610
1B
B3.
5 %
Str
ess
In
con
t49
81
AB
14
.7 %
Pro
ctiti
s40
761
BA
12
.0 %
Pro
ctiti
s11
645
0B
BA
C4.
4 %
Str
ess
In
con
t12
442
1A
A1
8.0
%P
roct
itis
4383
1B
A1
4.0
%P
roct
itis
3898
1B
B9.
0 %
Str
ess
In
con
t12
731
AB
19
.2 %
Pro
ctiti
s43
831
BA
14
.0 %
Pro
ctiti
s42
800
BB
16
.3 %
Str
ess
In
con
t66
61
A2
4.0
%P
roct
itis
6364
1B
A1
6.0
%P
roct
itis
6344
1B
BA
C2
6.0
%S
tre
ss I
nco
nt
1106
21
A3
1.5
%P
roct
itis
9265
0B
AA
19
.9 %
Pro
ctiti
s42
871
BB
29
.0 %
Str
ess
In
con
t34
801
AA
38
.9 %
Pro
ctiti
s36
491
BA
22
.0 %
Pro
ctiti
s76
701
BB
AB
33
.0 %
Str
ess
In
con
t13
011
A5
0.0
%P
roct
itis
1221
01
BA
A2
9.0
%P
roct
itis
2729
1B
B4
4.0
%S
eve
re I
nco
nt
1010
90
AA
0.0
%P
roct
itis
1078
1B
A2
9.7
%P
roct
itis
1069
31
BB
BA
75
.0 %
Se
vere
In
con
t12
442
2A
AA
0.0
%P
roct
itis
9733
1B
AB
32
.0 %
Cys
titis
3898
1B
B6.
0 %
Se
vere
In
con
t94
071
AA
A0.
3 %
Pro
ctiti
s11
201
2B
AC
42
.0 %
Cys
titis
3087
1B
B7.
3 %
Se
vere
In
con
t10
322
1A
AA
0.5
%P
roct
itis
1120
11
BA
B5
5.0
%C
ystit
is10
517
0B
BA
A8.
3 %
Se
vere
In
con
t10
183
0A
A1
.0 %
Cys
titis
9737
1B
A0
.7 %
Cys
titis
1164
50
BB
AC
8.8
%S
eve
re I
nco
nt
1030
31
AA
1.1
%C
ystit
is58
131
BA
1.8
%C
ystit
is46
391
BB
9.5
%S
eve
re I
nco
nt
4285
1A
B1
.9 %
Cys
titis
1074
81
BA
A2
.0 %
Cys
titis
1185
01
BB
BA
10
.0 %
Se
vere
In
con
t12
404
1A
A2
.0 %
Cys
titis
8798
0B
AA
2.0
%C
ystit
is63
441
BB
AC
12
.0 %
Se
vere
In
con
t26
40
AA
2.1
%C
ystit
is98
991
BA
B2
.4 %
Cys
titis
7670
1B
BA
B3
3.0
%S
eve
re I
nco
nt
1237
40
AA
A2
.1 %
Cys
titis
1193
90
BA
2.6
%C
ystit
is42
800
BB
37
.5 %
Se
vere
In
con
t12
322
1A
AA
2.3
%C
ystit
is10
770
BA
3.0
%C
ystit
is27
291
BB
94
.0 %
Se
vere
In
con
t57
321
AB
3.9
%C
ystit
is52
191
BA
3.0
%U
reth
ral
Str
ictu
re11
645
0B
BA
C0.
6 %
Se
vere
In
con
t11
104
1A
AA
4.0
%C
ystit
is68
131
BA
3.3
%U
reth
ral
Str
ictu
re11
936
2B
BA
A1.
0 %
Se
vere
In
con
t11
108
1A
A4
.3 %
Cys
titis
1193
61
BA
5.1
%U
reth
ral
Str
ictu
re10
517
0B
BA
A1.
5 %
Tabl
e A
-5.
Com
plic
atio
ns d
ata
for
circ
le g
raph
s
Archived Document— For Reference Only
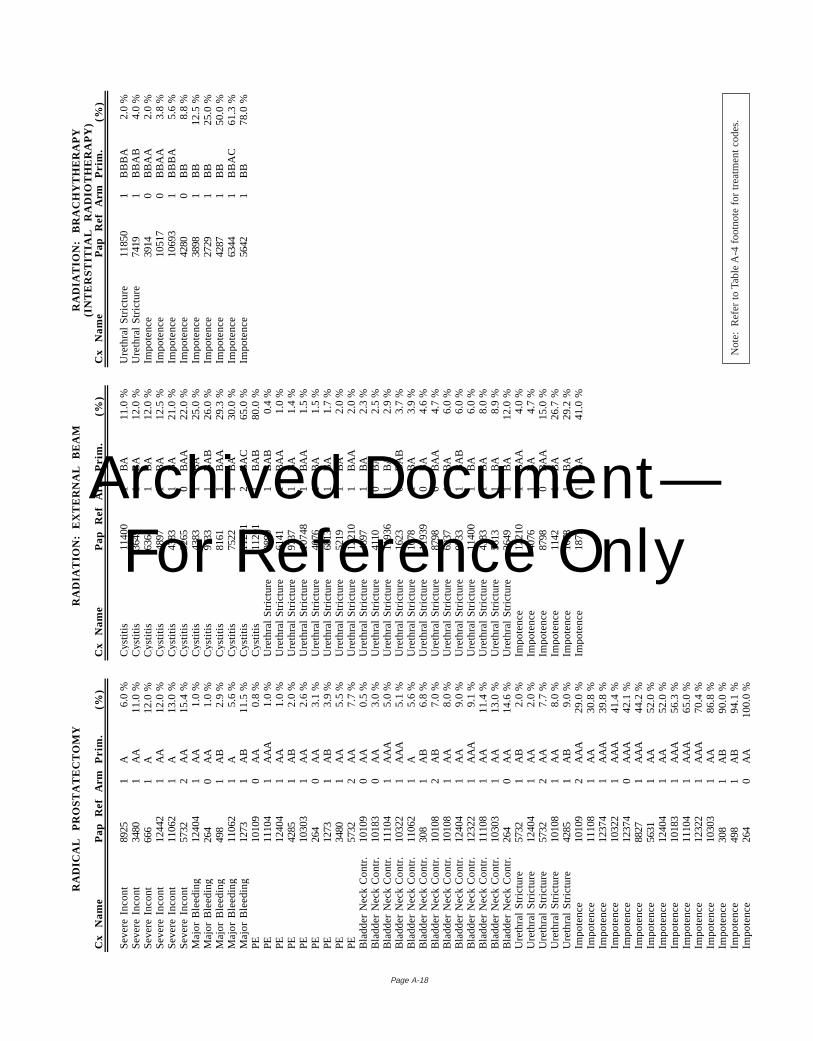
Page A-18
RA
DIC
AL
P
RO
ST
AT
EC
TO
MY
RA
DIA
TIO
N:
EX
TE
RN
AL
B
EA
MR
AD
IAT
ION
: B
RA
CH
YT
HE
RA
PY
(IN
TE
RS
TIT
IAL
R
AD
IOT
HE
RA
PY
)C
x N
am
eP
ap
R
ef
Arm
Pri
m.
(%)
Cx
Na
me
Pa
p
Re
fA
rmP
rim
.(%
)C
x N
am
eP
ap
R
ef
Arm
Pri
m.
(%)
Se
vere
In
con
t89
251
A6
.0 %
Cys
titis
1140
01
BA
11
.0 %
Ure
thra
l S
tric
ture
1185
01
BB
BA
2.0
%S
eve
re I
nco
nt
3480
1A
A1
1.0
%C
ystit
is36
491
BA
12
.0 %
Ure
thra
l S
tric
ture
7419
1B
BA
B4.
0 %
Se
vere
In
con
t66
61
A1
2.0
%C
ystit
is63
641
BA
12
.0 %
Imp
ote
nce
3914
0B
BA
A2.
0 %
Se
vere
In
con
t12
442
1A
A1
2.0
%C
ystit
is48
971
BA
12
.5 %
Imp
ote
nce
1051
70
BB
AA
3.8
%S
eve
re I
nco
nt
1106
21
A1
3.0
%C
ystit
is43
831
BA
21
.0 %
Imp
ote
nce
1069
31
BB
BA
5.6
%S
eve
re I
nco
nt
5732
2A
A1
5.4
%C
ystit
is92
650
BA
A2
2.0
%Im
po
ten
ce42
800
BB
8.8
%M
ajo
r B
lee
din
g12
404
1A
A1
.0 %
Cys
titis
4383
1B
A2
5.0
%Im
po
ten
ce38
981
BB
12
.5 %
Ma
jor
Ble
ed
ing
264
0A
A1
.0 %
Cys
titis
9733
1B
AB
26
.0 %
Imp
ote
nce
2729
1B
B2
5.0
%M
ajo
r B
lee
din
g49
81
AB
2.9
%C
ystit
is81
611
BA
A2
9.3
%Im
po
ten
ce42
871
BB
50
.0 %
Ma
jor
Ble
ed
ing
1106
21
A5
.6 %
Cys
titis
7522
1B
A3
0.0
%Im
po
ten
ce63
441
BB
AC
61
.3 %
Ma
jor
Ble
ed
ing
1273
1A
B1
1.5
%C
ystit
is11
201
2B
AC
65
.0 %
Impo
ten
ce56
421
BB
78
.0 %
PE
1010
90
AA
0.8
%C
ystit
is11
201
1B
AB
80
.0 %
PE
1110
41
AA
A1
.0 %
Ure
thra
l S
tric
ture
9899
1B
AB
0.4
%P
E12
404
1A
A1
.0 %
Ure
thra
l S
tric
ture
6141
1B
AA
1.0
%P
E42
851
AB
2.0
%U
reth
ral
Str
ictu
re97
371
BA
1.4
%P
E10
303
1A
A2
.6 %
Ure
thra
l S
tric
ture
1074
81
BA
A1.
5 %
PE
264
0A
A3
.1 %
Ure
thra
l S
tric
ture
4076
1B
A1.
5 %
PE
1273
1A
B3
.9 %
Ure
thra
l S
tric
ture
6813
1B
A1.
7 %
PE
3480
1A
A5
.5 %
Ure
thra
l S
tric
ture
5219
1B
A2.
0 %
PE
5732
2A
A7
.7 %
Ure
thra
l S
tric
ture
1221
01
BA
A2.
0 %
Bla
dd
er
Ne
ck C
on
tr.
1010
90
AA
0.5
%U
reth
ral
Str
ictu
re48
971
BA
2.3
%B
lad
de
r N
eck
Co
ntr
.10
183
0A
A3
.0 %
Ure
thra
l S
tric
ture
4110
0B
A2.
5 %
Bla
dd
er
Ne
ck C
on
tr.
1110
41
AA
A5
.0 %
Ure
thra
l S
tric
ture
1193
61
BA
2.9
%B
lad
de
r N
eck
Co
ntr
.10
322
1A
AA
5.1
%U
reth
ral
Str
ictu
re16
230
BA
B3.
7 %
Bla
dd
er
Ne
ck C
on
tr.
1106
21
A5
.6 %
Ure
thra
l S
tric
ture
1078
1B
A3.
9 %
Bla
dd
er
Ne
ck C
on
tr.
308
1A
B6
.8 %
Ure
thra
l S
tric
ture
1193
90
BA
4.6
%B
lad
de
r N
eck
Co
ntr
.10
108
2A
B7
.0 %
Ure
thra
l S
tric
ture
8798
0B
AA
4.7
%B
lad
de
r N
eck
Co
ntr
.10
108
1A
A8
.0 %
Ure
thra
l S
tric
ture
6937
1B
A6.
0 %
Bla
dd
er
Ne
ck C
on
tr.
1240
41
AA
9.0
%U
reth
ral
Str
ictu
re97
331
BA
B6.
0 %
Bla
dd
er
Ne
ck C
on
tr.
1232
21
AA
A9
.1 %
Ure
thra
l S
tric
ture
1140
01
BA
6.0
%B
lad
de
r N
eck
Co
ntr
.11
108
1A
A1
1.4
%U
reth
ral
Str
ictu
re43
831
BA
8.0
%B
lad
de
r N
eck
Co
ntr
.10
303
1A
A1
3.0
%U
reth
ral
Str
ictu
re58
131
BA
8.9
%B
lad
de
r N
eck
Co
ntr
.26
40
AA
14
.6 %
Ure
thra
l S
tric
ture
3649
1B
A1
2.0
%U
reth
ral
Str
ictu
re57
321
AB
2.0
%Im
po
ten
ce12
210
1B
AA
4.0
%U
reth
ral
Str
ictu
re12
404
1A
A2.
0 %
Imp
ote
nce
4076
1B
A4.
7 %
Ure
thra
l S
tric
ture
5732
2A
A7.
7 %
Imp
ote
nce
8798
0B
AA
15
.0 %
Ure
thra
l S
tric
ture
1010
81
AA
8.0
%Im
po
ten
ce11
421
BA
26
.7 %
Ure
thra
l S
tric
ture
4285
1A
B9.
0 %
Imp
ote
nce
1078
1B
A2
9.2
%Im
po
ten
ce10
109
2A
AA
29
.0 %
Imp
ote
nce
1877
1B
A4
1.0
%Im
po
ten
ce11
108
1A
A3
0.8
%Im
po
ten
ce12
374
1A
AA
39
.8 %
Imp
ote
nce
1032
21
AA
A4
1.4
%Im
po
ten
ce12
374
0A
AA
42
.1 %
Imp
ote
nce
8827
1A
AA
44
.2 %
Imp
ote
nce
5631
1A
A5
2.0
%Im
po
ten
ce12
404
1A
A5
2.0
%Im
po
ten
ce10
183
1A
AA
56
.3 %
Imp
ote
nce
1110
41
AA
A6
5.0
%Im
po
ten
ce12
322
1A
AA
70
.4 %
Imp
ote
nce
1030
31
AA
86
.8 %
Imp
ote
nce
308
1A
B9
0.0
%Im
po
ten
ce49
81
AB
94
.1 %
Imp
ote
nce
264
0A
A10
0.0
%N
ote:
Ref
er t
o Ta
ble
A-4
foo
tnot
e fo
r tr
eatm
ent
code
s.
Archived Document— For Reference Only
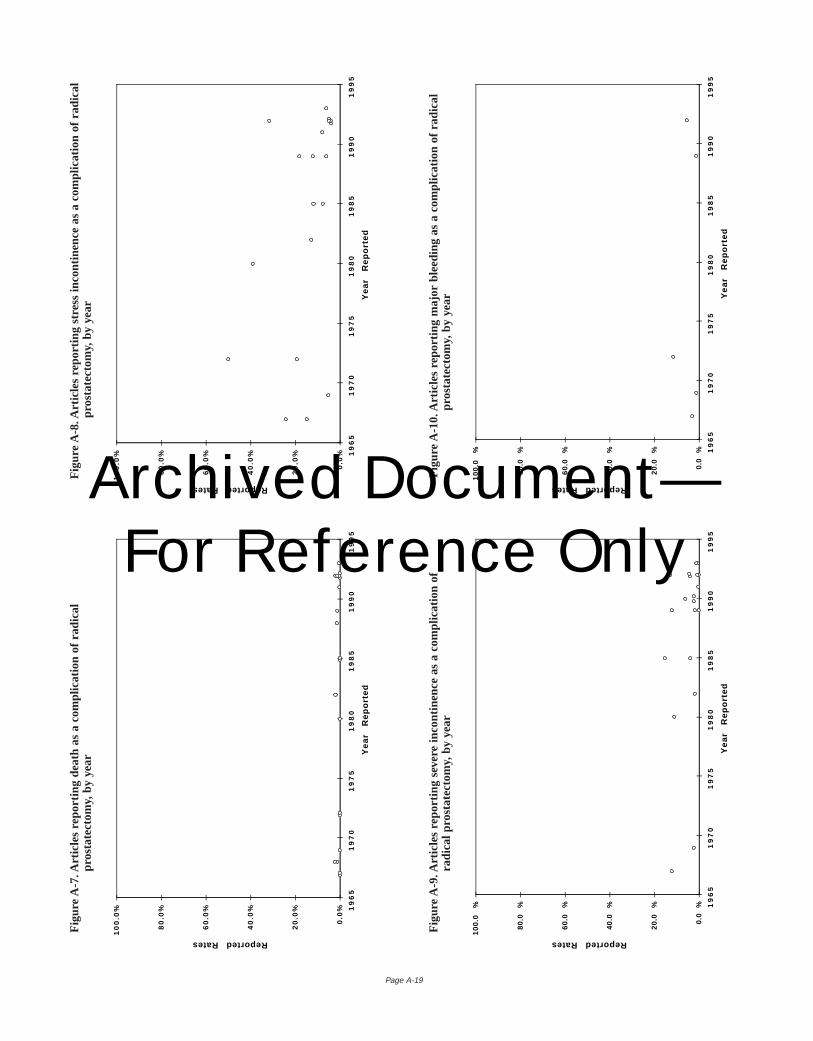
Page A-19
Fig
ure
A-9
. Art
icle
s re
port
ing
seve
re in
cont
inen
ce a
s a
com
plic
atio
n of
radi
cal p
rost
atec
tom
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
0. A
rtic
les
repo
rtin
g m
ajor
ble
edin
g as
a c
ompl
icat
ion
of r
adic
alpr
osta
tect
omy,
by y
ear
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-8
. Art
icle
s re
port
ing
stre
ss in
cont
inen
ce a
s a
com
plic
atio
n of
rad
ical
pros
tate
ctom
y,by
yea
r
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-7
. Art
icle
s re
port
ing
deat
h as
a c
ompl
icat
ion
of r
adic
alpr
osta
tect
omy,
by y
ear
Archived Document— For Reference Only
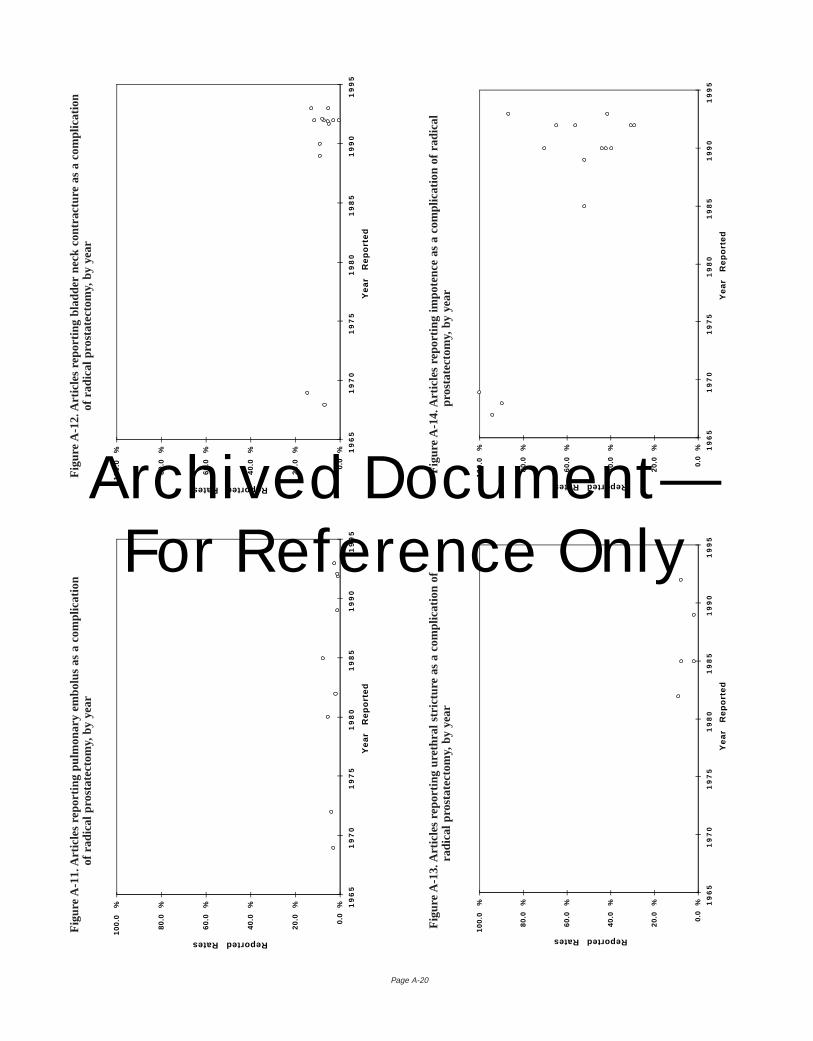
Page A-20
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
2. A
rtic
les
repo
rtin
g bl
adde
r ne
ck c
ontr
actu
re a
s a
com
plic
atio
nof
rad
ical
pro
stat
ecto
my,
by y
ear
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
1. A
rtic
les
repo
rtin
g pu
lmon
ary
embo
lus
as a
com
plic
atio
nof
rad
ical
pro
stat
ecto
my,
by y
ear
Fig
ure
A-1
3. A
rtic
les
repo
rtin
g ur
ethr
al s
tric
ture
as
a co
mpl
icat
ion
ofra
dica
l pro
stat
ecto
my,
by y
ear
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
4. A
rtic
les
repo
rtin
g im
pote
nce
as a
com
plic
atio
n of
rad
ical
pros
tate
ctom
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported RatesArchived Document— For Reference Only
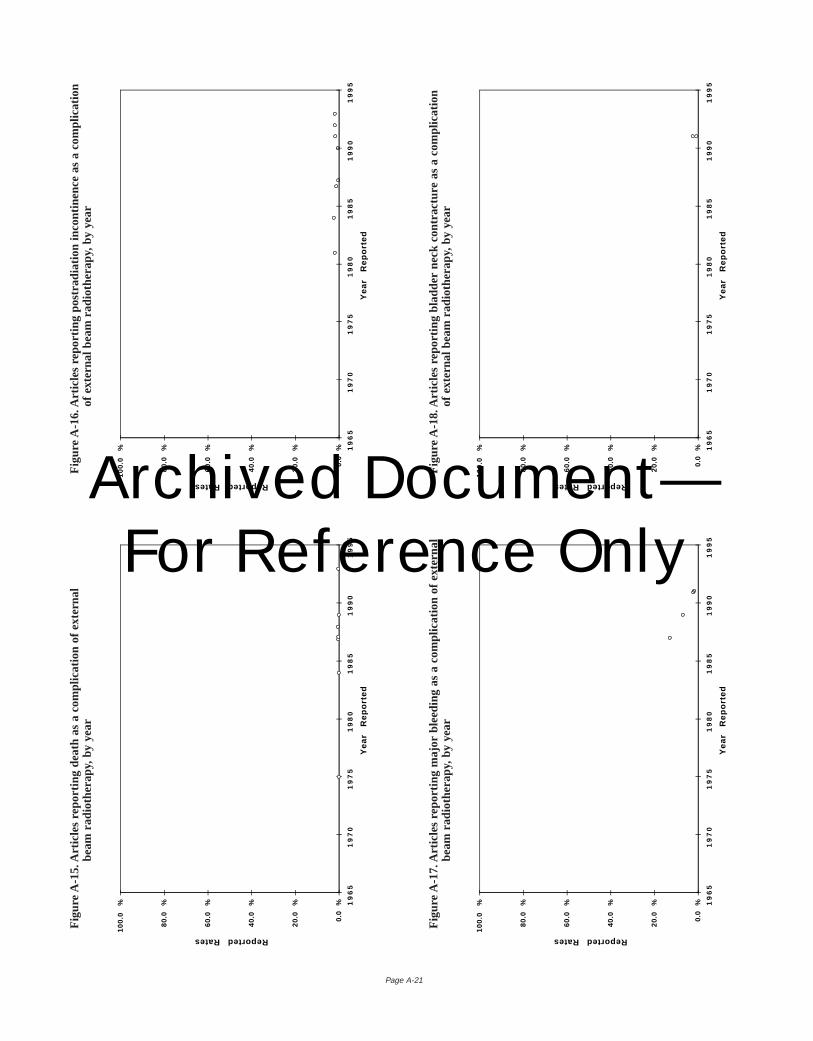
Page A-21
Fig
ure
A-1
7. A
rtic
les
repo
rtin
g m
ajor
ble
edin
g as
a c
ompl
icat
ion
of e
xter
nal
beam
rad
ioth
erap
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
8. A
rtic
les
repo
rtin
g bl
adde
r ne
ck c
ontr
actu
re a
s a
com
plic
atio
nof
ext
erna
l bea
m r
adio
ther
apy,
by y
ear
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
6. A
rtic
les
repo
rtin
g po
stra
diat
ion
inco
ntin
ence
as
a co
mpl
icat
ion
of e
xter
nal b
eam
rad
ioth
erap
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
5. A
rtic
les
repo
rtin
g de
ath
as a
com
plic
atio
n of
ext
erna
lbe
am r
adio
ther
apy,
by y
ear
Archived Document— For Reference Only
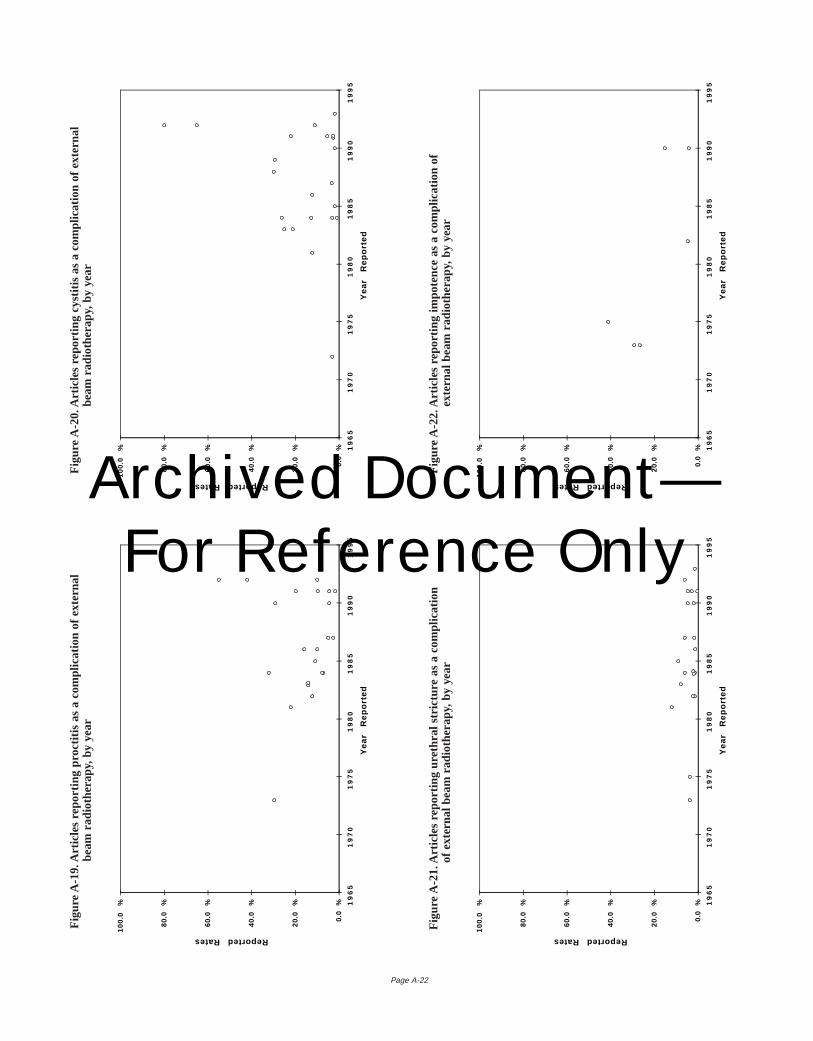
Page A-22
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
0. A
rtic
les
repo
rtin
g cy
stiti
s as
a c
ompl
icat
ion
of e
xter
nal
beam
rad
ioth
erap
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-1
9. A
rtic
les
repo
rtin
g pr
octit
is a
s a
com
plic
atio
n of
ext
erna
lbe
am r
adio
ther
apy,
by y
ear
Fig
ure
A-2
1. A
rtic
les
repo
rtin
g ur
ethr
al s
tric
ture
as
a co
mpl
icat
ion
of e
xter
nal b
eam
rad
ioth
erap
y,by
yea
r
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
2. A
rtic
les
repo
rtin
g im
pote
nce
as a
com
plic
atio
n of
exte
rnal
bea
m r
adio
ther
apy,
by y
ear
0.0
%
20
.0
%
40
.0
%
60
.0
%
80
.0
%
10
0.0
% 1
96
51
97
01
97
51
98
01
98
51
99
01
99
5
Ye
ar
Re
po
rte
d
Reported RatesArchived Document— For Reference Only
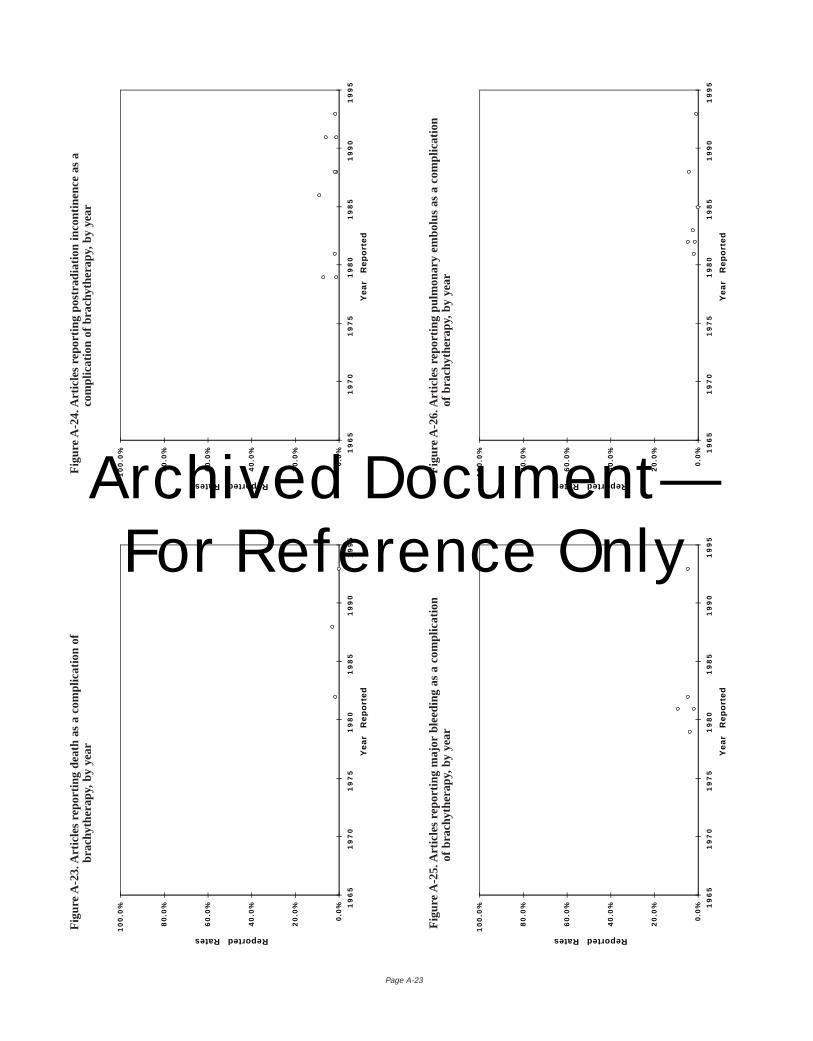
Page A-23
Fig
ure
A-2
5. A
rtic
les
repo
rtin
g m
ajor
ble
edin
g as
a c
ompl
icat
ion
of b
rach
ythe
rapy
,by
year
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
6. A
rtic
les
repo
rtin
g pu
lmon
ary
embo
lus
as a
com
plic
atio
nof
bra
chyt
hera
py,b
y ye
ar
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
4. A
rtic
les
repo
rtin
g po
stra
diat
ion
inco
ntin
ence
as
aco
mpl
icat
ion
of b
rach
ythe
rapy
,by
year
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
3. A
rtic
les
repo
rtin
g de
ath
as a
com
plic
atio
n of
brac
hyth
erap
y,by
yea
r
Archived Document— For Reference Only
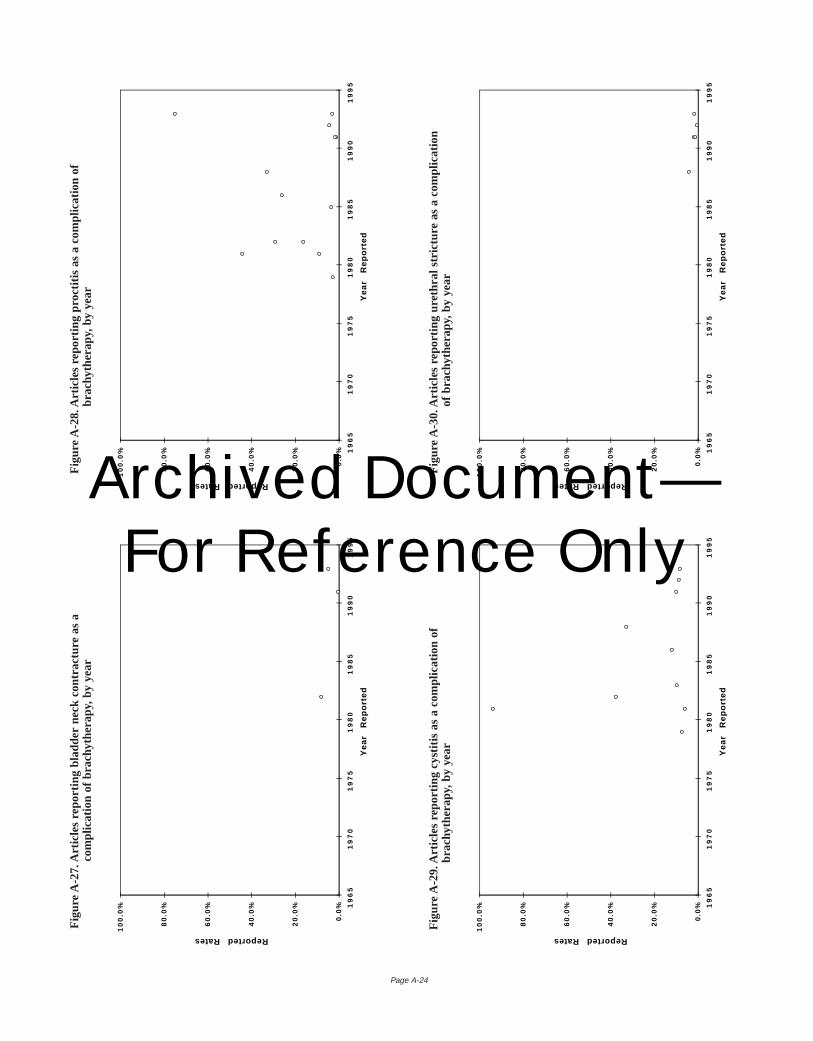
Page A-24
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
8. A
rtic
les
repo
rtin
g pr
octit
is a
s a
com
plic
atio
n of
brac
hyth
erap
y,by
yea
r
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-2
7. A
rtic
les
repo
rtin
g bl
adde
r ne
ck c
ontr
actu
re a
s a
com
plic
atio
n of
bra
chyt
hera
py,b
y ye
ar
Fig
ure
A-2
9. A
rtic
les
repo
rtin
g cy
stiti
s as
a c
ompl
icat
ion
ofbr
achy
ther
apy,
by y
ear
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-3
0. A
rtic
les
repo
rtin
g ur
ethr
al s
tric
ture
as
a co
mpl
icat
ion
of b
rach
ythe
rapy
,by
year
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported RatesArchived Document— For Reference Only
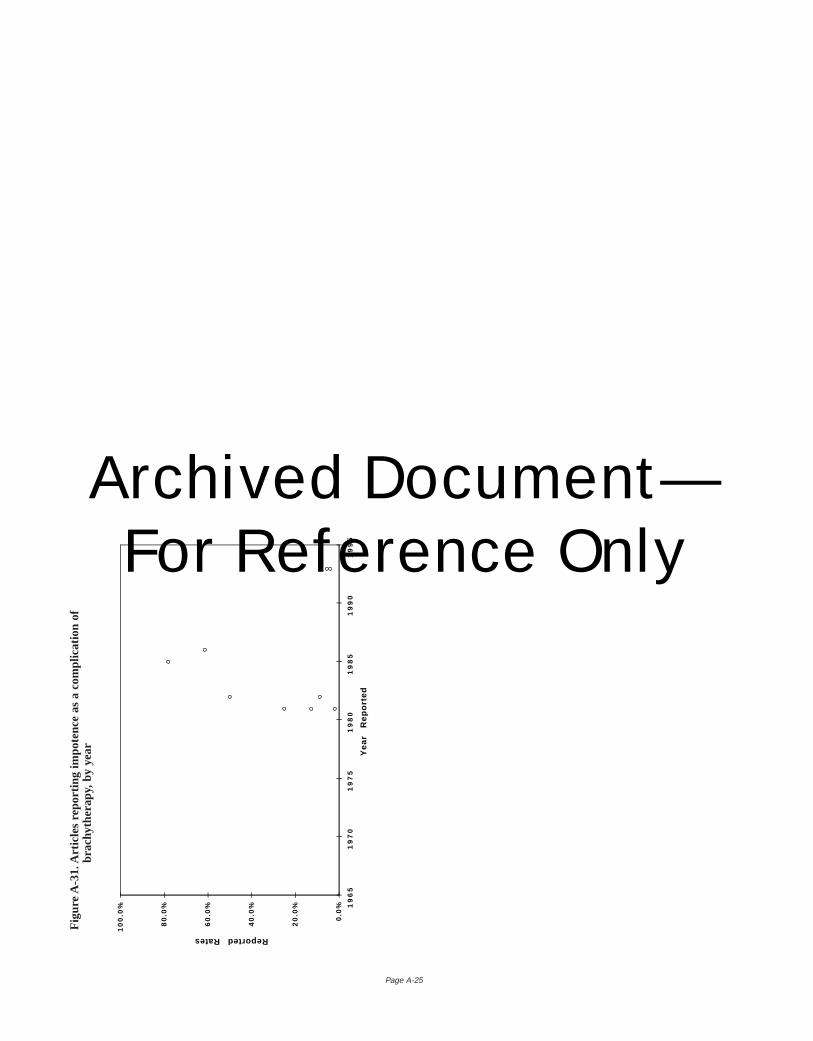
Page A-25
0.0
%
20
.0%
40
.0%
60
.0%
80
.0%
10
0.0
% 19
65
19
70
19
75
19
80
19
85
19
90
19
95
Ye
ar
Re
po
rte
d
Reported Rates
Fig
ure
A-3
1. A
rtic
les
repo
rtin
g im
pote
nce
as a
com
plic
atio
n of
brac
hyth
erap
y,by
yea
r
Archived Document— For Reference Only
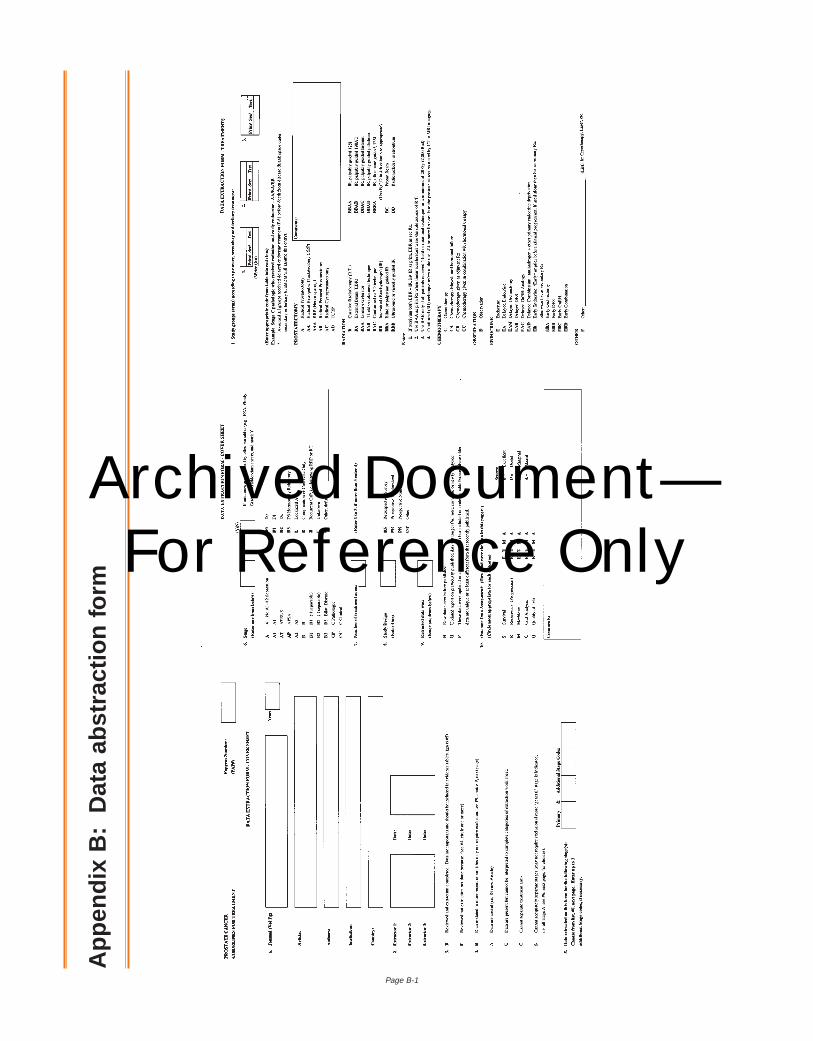
Page B-1
App
endi
x B
:D
ata
abst
ract
ion
form
Archived Document— For Reference Only
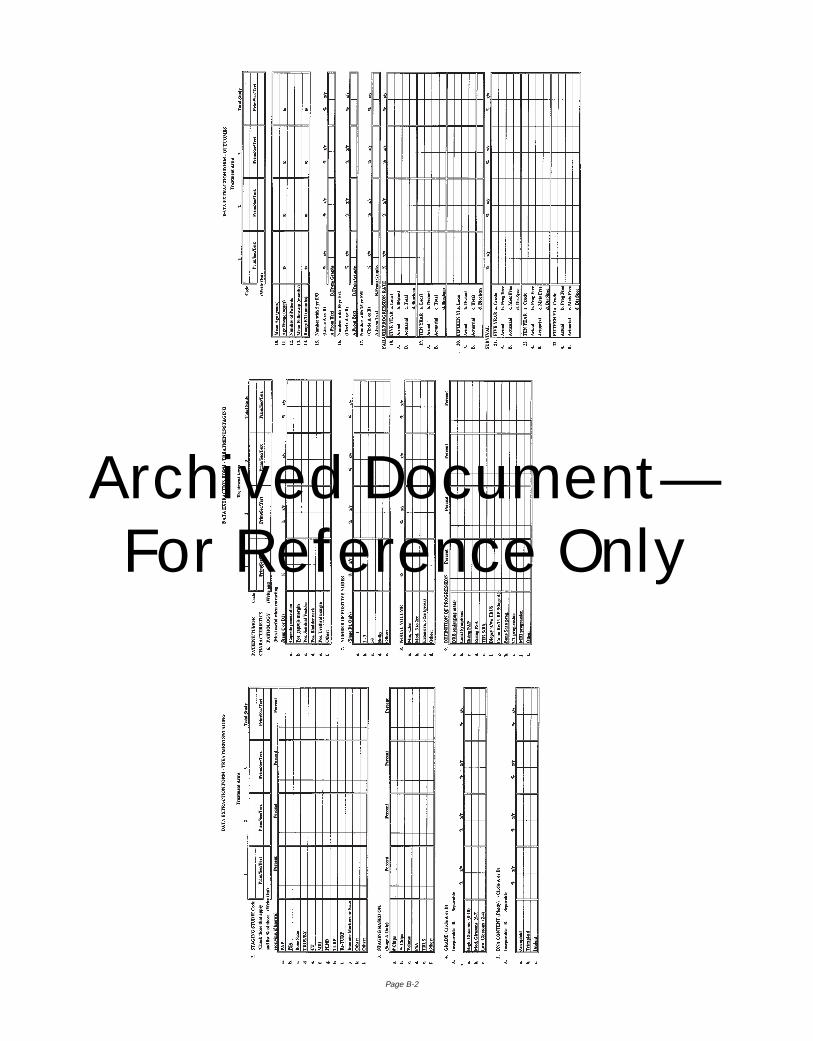
Page B-2
Archived Document— For Reference Only
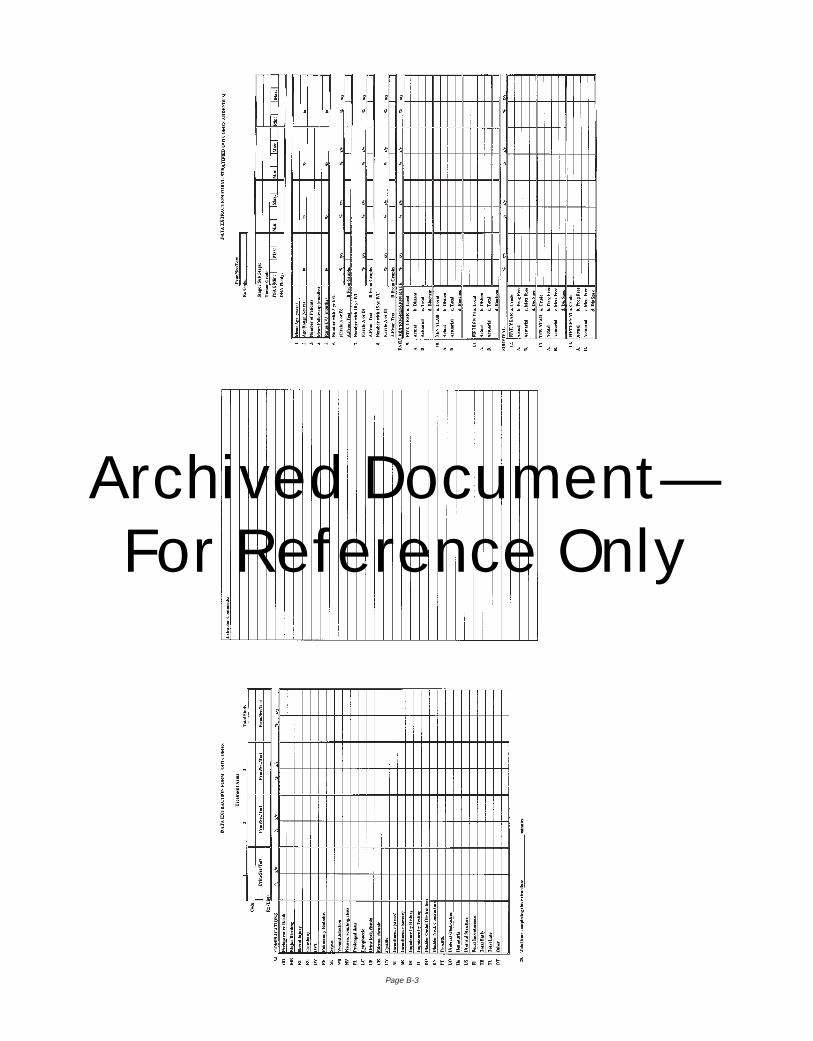
Page B-3
Archived Document— For Reference Only
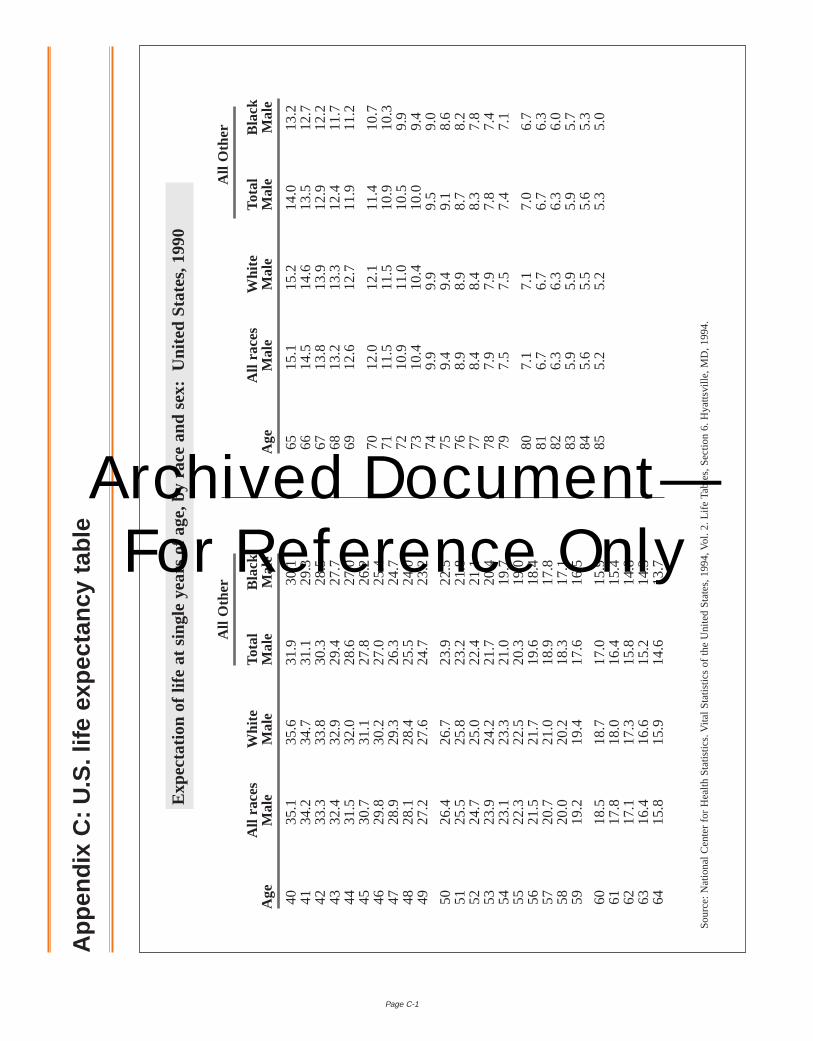
Page C-1
6515
.115
.214
.013
.266
14.5
14.6
13.5
12.7
6713
.813
.912
.912
.268
13.2
13.3
12.4
11.7
6912
.612
.711
.911
.2
7012
.012
.111
.410
.771
11.5
11.5
10.9
10.3
7210
.911
.010
.59.
973
10.4
10.4
10.0
9.4
749.
99.
99.
59.
075
9.4
9.4
9.1
8.6
768.
98.
98.
78.
277
8.4
8.4
8.3
7.8
787.
97.
97.
87.
479
7.5
7.5
7.4
7.1
807.
17.
17.
06.
781
6.7
6.7
6.7
6.3
826.
36.
36.
36.
083
5.9
5.9
5.9
5.7
845.
65.
55.
65.
385
5.2
5.2
5.3
5.0
App
endi
x C
:U.S
.life
exp
ecta
ncy
tabl
e
Sou
rce:
Nat
iona
l Cen
ter
for
Hea
lth S
tatis
tics.
Vita
l Sta
tistic
s of
the
Uni
ted
Sta
tes,
1994
,Vol
. 2.
Life
Tab
les,
Sec
tion
6. H
yatts
ville
,MD
,199
4.
Exp
ecta
tion
of li
fe a
t si
ngle
yea
rs o
f ag
e,by
rac
e an
d se
x:U
nite
d S
tate
s,19
90
All
Oth
er
All
race
s W
hite
Tota
lB
lack
Age
Mal
eM
ale
Mal
eM
ale
All
Oth
er
All
race
s W
hite
Tota
lB
lack
Age
Mal
eM
ale
Mal
eM
ale
4035
.135
.631
.930
.141
34.2
34.7
31.1
29.3
4233
.333
.830
.328
.543
32.4
32.9
29.4
27.7
4431
.532
.028
.627
.045
30.7
31.1
27.8
26.2
4629
.830
.227
.025
.447
28.9
29.3
26.3
24.7
4828
.128
.425
.524
.049
27.2
27.6
24.7
23.2
5026
.426
.723
.922
.551
25.5
25.8
23.2
21.8
5224
.725
.022
.421
.153
23.9
24.2
21.7
20.4
5423
.123
.321
.019
.755
22.3
22.5
20.3
19.0
5621
.521
.719
.618
.457
20.7
21.0
18.9
17.8
5820
.020
.218
.317
.159
19.2
19.4
17.6
16.5
6018
.518
.717
.015
.961
17.8
18.0
16.4
15.4
6217
.117
.315
.814
.863
16.4
16.6
15.2
14.3
6415
.815
.914
.613
.7
Archived Document— For Reference Only
Page I-1
Index
AActual and actuarial data, use of, 10, 23–24Adenocarcinoma, 1, 12. See alsoProstate cancerAmerican Joint Committee (TNM) staging system, 1, 13, 14Androgen deprivation, 2, 15, 44
BBiochemical markers, 6, 44. See alsoProstate specific antigen
(PSA)Bladder neck contracture, 2, 21, 27, 31, 36, 38Bleeding (major), 2, 3, 21, 22, 27, 31, 36, 38, 39Brachytherapy. See alsoRadiotherapy
advantages and disadvantages of, 5, 39–40complications from, 5, 17, 27, 31, 40patient selection for, 5, 17–18, 38progression data for, 26, 34–35survival data for, 25, 28–30, 32techniques for, 18, 43as treatment alternative, 2, 5, 15, 38–40
CChemotherapy, 2, 15, 44Clinical staging. SeeStagingClinically localized prostate cancer. See alsoProstate cancer;
Stage T2 (B)background information for, 1–2, 12detection rate for, ilimitations of research on, 6, 9–10, 42–43recommendations for future research on, 6–7, 43–45
Colorectal cancer, 1, 12Complications. Seespecific complications; Treatment complica-
tionsComputerized tomography (CT) scans, 2, 14Cost factors, 22, 40, 45Cryotherapy, 2, 15, 43Cystitis, 2, 3, 5, 21, 22, 27, 31, 36, 38, 39
DDeath. SeeMortalityDiarrhea, 27, 36, 39Digital rectal examination (DRE)
clinical staging using, 2, 14detection using, imonitoring with, 20, 40
Disease-specific survival. SeeSurvival
EErectile dysfunction, 2, 3, 5, 21, 22, 27, 31, 36, 38, 39, 40External beam radiotherapy. See alsoRadiotherapy
advantages and disadvantages of, 5, 39complications from, 5, 17, 27, 35, 36, 39conformal therapy and, 7, 16, 44patient selection for, 5, 16–17, 38progression data for, 26, 34survival data for, 25, 28–30, 32, 33target volume and, 17technological improvements in, 7, 16, 44as treatment alternative, 2, 5, 15, 38, 39
GGleason grading system, 13
HHealth status, treatment selection based on, 4, 37
IImpotence. SeeErectile dysfunctionIncontinence. SeeUrinary incontinenceInterstitial radiotherapy. SeeBrachytherapy
JJewett-Whitmore (ABCD) staging system, 1, 13, 14
LLife expectancy, 21
estimation of, 19treatment selection based on, 4, 12–13, 16, 37
Lung cancer, 1, 12Lymph node dissection, 42. See alsoPelvic lymph node dissection
(PLND)Lymph nodes as target volume (radiotherapy), 16–17
MMagnetic resonance imaging (MRI), 2, 14Meta-analysis, definition of, 9Metastasis-free survival. SeeSurvivalMortality
from prostate cancer, i, 1, 4, 12, 37, 40, 41treatment related, 2, 3, 21, 22, 27, 31, 36, 38–39
NNational Institutes of Health (NIH), i
OOutcomes. SeeTreatment outcomesOverall survival. SeeSurvival
PPelvic lymph node dissection (PLND), 2, 14, 32, 42Proctitis, 5, 21, 27, 31, 35, 36, 39Progression, 3, 8, 21, 33, 40
analysis of data, 26, 34–35categories (local, distant, biochemical, total), definitions of, 24rates, 3, 21–22, 26, 34–35
Progression-free survival. SeeSurvivalProstate cancer. See alsoClinically localized prostate cancer; spe-
cific stagesbackground of, 1–2, 12detection of, igrowth rate of, 1, 12–13mortality from, i, 1, 4, 12, 37, 40, 41natural history of, 1, 12–13staging of, 1–2, 13–15
Prostate Cancer Clinical Guidelinesdata display for survival and disease progression and, 10data extraction for, 9data inadequacies and, 9–10
Archived Document— For Reference Only
Page I-2
literature citations and panel opinions in discussion sections in,10–11
literature searches used in, 9methods and definitions of, 8–9treatment complications data and, 10
Prostate specific antigen (PSA)clinical staging using, 1, 2, 13, 14, 15, 44detection using, i, 14, 43, 44to determine recurrence, 3, 19, 24, 33, 43monitoring progression with, 20, 24, 33, 40, 45as predictor of pelvic lymph node metastases, 14–15
Prostatectomy. SeeRadical prostatectomyPsychological factors, 3, 21, 41Pulmonary embolism, 2, 21, 27, 31, 36, 39
QQuality of life, 7, 22, 41, 45
RRadiation cystitis, 2, 3, 5, 21, 22, 27, 31, 36, 38, 39Radical prostatectomy, 4, 38
advantages and disadvantages of, 5, 38–39complications from, 27, 31, 35, 36, 38–40definition of, 4, 38life expectancy and decision for, 16nerve-sparing techniques, 16, 39, 43overall survival rates for, 28patient age and, 3patient selection for, 15–16, 38performance of, 16, 43progression data for, 26, 34recommendations for research on, 7, 43, 44survival data for, 25, 28–29, 32, 33as treatment alternative, 2, 5, 15, 38–39
Radionuclide bone scan, 2, 15, 16Radiotherapy. See alsoBrachytherapy; External beam
radiotherapyadvantages and disadvantages of, 5, 39–40complications from, 5, 17, 27, 31, 35, 36, 39, 40definition of, 4, 38patient selection for, 5, 16–18, 38progression data for, 26, 34–35recommendations for research on, 7, 44survival data for, 25, 28–30, 32, 33as treatment alternative, 2, 5, 15, 38–40
Rectal injury, 2, 3, 21, 22, 27, 35, 36, 39Recurrence of disease, 3, 19, 21, 22, 24, 26, 33, 34, 40, 43. See
alsoProgression
SSeminal vesicles, 4, 16–18, 38Serum acid phosphatase, 2, 14, 15, 17, 24Spinal cord compression, 41Stage BO. SeeStage T1cStage M1 (D2), i, 35Stage T1 (A)
detection rate at, isurvival rate and, 2, 17treatment outcomes for, 2
Stage T2 (B)detection rate at, ilimitations in literature for, 6progression and, 34, 35review of literature on, 8, 9survival rate and, 2, 17, 33treatment complications of, 36
treatment outcomes for, 2, 23
Stage T2 (C), 17
Stage T1c, 1, 6, 14
Stage T3-T4 (C), i, 35, 37
Staging. See alsospecific stages
improvements needed, 1, 2, 7, 13, 44
methods used for, 1–2, 14–15
Standard patient, 6, 37
Stress urinary incontinence. SeeUrinary incontinence
Surveillance
advantages and disadvantages of, 5, 40–41
basis for management by, 18–19
patient selection for, 19, 38
progression data for, 26, 34
recommendations for research on, 7, 44
survival data for, 25, 28–31, 32, 33, 40
as treatment alternative, 2, 5, 15, 38, 40–41
Survival, 3, 8, 10, 21, 40
analysis of, 25, 32–33
categories (overall, progression free, metastasis free, diseasespecific), definitions of, 24
rates, 2, 3, 21, 25, 28–33
TThermotherapy, 2, 15
TNM staging system, 1, 13, 14
Toxicity from radiotherapy. SeeRadiotherapy, complications from
Transrectal ultrasonography (TRUS), 2, 14, 17, 39–40
Transurethral resection of the prostate (TURP), 17, 19, 40
Treatment complications, 2, 3, 5, 21, 22, 27, 31, 35–36, 38, 39, 40,41
outcomes data for, 10, 27, 31, 35–36
problems with data for, 10, 35
Treatment outcomes
analysis of summary tables of, 32–35
from available literature, 3, 22
tables and graphs summarizing, 22–32
types of, 2, 3, 21, 22
variability of data on, 9–10, 22, 32, 42–43
Treatment recommendations
alternatives, 5
levels of, 3, 6, 37
standards, 4, 37–38
Tumors. See alsoClinically localized prostate cancer
grading, 13
growth rate of, 1, 12–13
stage determination of, 1–2, 13–15
treatment selection based on characteristics of, 17, 37–38
UUrethral stricture, 2, 21, 27, 31, 36, 38
Urinary incontinence, 2, 3, 5, 21, 22, 27, 31, 35, 36, 38, 39, 40
Archived Document— For Reference Only
American Urological Association, Inc.
This Report on the Management of Clinically Localized Prostate Cancerwas developed by theProstate Cancer Clinical Guidelines Panel of the American Urological Association, Inc.
This Report is intended to furnish to the skilled practitioner a consensus of clear principles andstrategies for quality patient care, based on current professional literature, clinical experience andexpert opinion. It does not establish a fixed set of rules or define the legal standard of care, pre-empting physician judgment in individual cases.
An attempt has been made to recommend a range of generally acceptable modalities of treat-ment, taking into account variations in resources and in patient needs and preferences. It is recom-mended that the practitioner articulate and document the basis for any significant deviation fromthese parameters.
Finally, it is recognized that conformance with these guidelines cannot ensure a successfulresult. The parameters should not stifle innovation, but will, themselves, be updated and willchange with both scientific knowledge and technological advances.
Board of Directors (1995 – 1996)
Practice Parameters, Guidelines and Standards Committee (1995 – 1996)
Health Policy Department Staff and Consultants
Charles F. McKiel, Jr., MD*Jack W. McAninch, MD*C. Eugene Carlton, Jr., MD*William R. Turner, Jr., MD*Roy J. Correa, Jr., MD*Harry C. Miller, Jr., MD*Dennis J. Card, MD*E. Darracott Vaughan, Jr., MD*Joseph C. Cerny, MD*
Gerald Sufrin, MD*Thomas P. Ball, Jr., MD*Lloyd H. Harrison, MD*Lawrence W. Jones, MD*Harry E. Lichtwardt, MDAbraham T. K. Cockett, MDH. Logan Holtgrewe, MDWinston K. Mebust, MDMartin I. Resnick, MD
Joseph N. Corriere, Jr., MDDavid M. Drylie, MDG. James GallagherRichard J. HanniganThomas D. Brockman Melanie H. Younger
*Voting member
Stephanie MenshDirector
Suzanne Boland PopeGuidelines Coordinator
Julie BowersAdministrative Assistant
Kim HagedornHealth Policy Projects Coordinator
Robin HudsonSecretary
Lisa EmmonsHealth Policy Manager
Tracy KielyHealth Policy Information Assistant
Betty RobertsHealth Policy Assistant
Megan CohenGovernment Relations Coordinator
Roger WoodsGovernment Relations Assistant
Randolph B. FenningerWashington Liaison
Justine GermannLegislative Associate
William GlitzPublic Relations Consultant
Karen CostanzoUniversity of Texas,Southwestern Medical School
Winston K. Mebust, MD, ChairJoseph W. Segura, MD, Vice-ChairReginald C. Bruskewitz, MDJack S. Elder, MDThomas C. Fenter, MDJohn B. Forrest, MD
Drogo K. Montague, MDGlenn M. Preminger, MDJoseph A. Smith, MDIan M. Thompson, Jr., MDCharles E. Hawtrey, MD, ConsultantJohn D. McConnell, MD, Consultant
Linda D. Shortliffe, MD, ConsultantEdward S. Tank, MD, ConsultantClaus G. Roehrborn, MD, FacilitatorRoy J. Correa, Jr., MD, Ex-officioCharles F. McKiel, Jr., MD, Ex-officioWilliam R. Turner, Jr., MD, Ex-officio
Archived Document— For Reference Only
American Urological Association, Inc.1000 Corporate BoulevardLinthicum, Maryland 21090
ISBN 0-9649702-0-1
Decem
ber 1995R
eport on the Managem
ent of Localized Prostate C
ancerArchived Document— For Reference Only


















