Embed Size (px)
Citation preview
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
AQUATIC PHYSIOTHERAPY IN THE INPATIENT SETTING
SARAH GUILLE
[sarah_guillehotmailcom]
RESEARCH QUESTION
What evidence is there to support the use of aquatic physiotherapy in the inpatient setting
ABSTRACT
Background The purpose of this literature review was to search for and appraise the quality
of all research evidence supporting the use of aquatic physiotherapy in the inpatient setting
There is growing evidence for the use of aquatic physiotherapy in outpatient populations By
contrast aquatic rehabilitation in the inpatient setting remains largely understudied Method
Ten medical and allied health databases were systematically searched and relevant trials were
critically appraised using recognised critical review protocols Results 7 trials were
appropriate for inclusion and their methodological quality was analysed Moderate to high
quality evidence exists to support the use of aquatic physiotherapy in early post-operative
lower limb joint arthroplasty for benefit in muscle strength and self-reported functional
measures There is low level evidence for the application of aquatic physiotherapy in
neurological populations to reduce spasticity and medication use While three case studies
involving patients with orthopaedic and neuromuscular debility offer poor research merit they
indicate positive outcome trends for the use of aquatic physiotherapy in complex conditions
Conclusion More evidence is required to investigate the specific benefits of aquatic
physiotherapy as compared to land based treatment or general water exercise in acute patient
populations
INTRODUCTION
Use of aquatic physiotherapy in the management of musculoskeletal and orthopaedic
conditions is widespread There is growing evidence to support the use of aquatic
physiotherapy in chronic conditions including rheumatoid arthritis hip and knee osteoarthritis
(OA) chronic low back pain fibromyalgia and chronic regional pain syndrome (Geytenbeek
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
2002 Geytenbeek 2008 Bartels et al 2009) In osteoarthritis gold level evidence supports
the use of aquatic therapy for short term slight improvement in pain and function (Bartels et al
2007) while benefits in disability strength range of motion pain flexibility balance well-
being cost-effectiveness heath status and quality of life are also demonstrated (Geytenbeek
2002 Geytenbeek 2008) Scientific grounds and evidence from outpatient studies support the
use of aquatic physiotherapy in post-surgical rehabilitation and orthopaedic injury (Ahlqvist
2002 Fappiano and Gangaway 2008 Watts and Gangaway 2007) It has been demonstrated
that aquatic intervention can facilitate early initiation of exercise improve self-reported pain
and function and contribute to greater range of motion strength proprioception and decreased
risk of further injury (Fappiano and Gangaway 2008 Watts and Gangaway 2007 McAvoy
2009) In anterior cruciate ligament (ACL) rehabilitation aquatic physiotherapy has been
attributed to reduced joint effusion and earlier gains in range of motion (McClintock and
Kirkley 1995 Tovin et al 1994) In a reduced weight bearing environment which minimises
joint stress it is likely that the physiological and thermal properties of water including
hydrostatic pressure and buoyancy effect enable early initiation of exercise and increased
activity tolerance
Limited evidence exists to support the use of aquatic physiotherapy in inpatient populations
including acute orthopaedic rehabilitation (Geytenbeek 2008) Land-based studies of
intensive rehabilitation programmes and additional physiotherapy in the hospital setting
clearly demonstrate a positive relationship between physiotherapy service and positive patient
outcomes Increased intensity and frequency of physiotherapy intervention has been shown to
benefit parameters of functional mobility and total hospital cost including discharge
destination and reduced length of stay (Boxall 2004 Freburger 2000 Kirk-Sanchez 2001
Lawson 2006 Moffet 2004 and Roach 1998 Weigl 2003) In the post-operative recovery of
high risk patients undergoing elective hip or knee arthroplasty early inpatient rehabilitation
(day 3 instead of 7) was well tolerated and contributed to earlier obtainment of functional
goals at less overall cost (Munin et al 1998) Considering that aquatic physiotherapy is
indicated where land based activity is contraindicated due to pain or acute injury (Babb and
Simelson-Warr 1994) it is possible that aquatic physiotherapy could be used as a substitute
for land-based rehabilitation The inpatient setting provides a unique opportunity to explore
the use of aquatic physiotherapy in hospital patients recovering from surgery injury illness or
disease This review of the literature aims to investigate what evidence exists to support the
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
use of aquatic physiotherapy in the inpatient setting across the orthopaedic neurological and
general medical disciplines
METHODSSELECTION OF ARTICLES
Inclusion criteria All studies describing aquatic physiotherapy as an inpatient intervention
were included There was no limitation on the type of studies participants nor outcomes
selected for inclusion
Search Strategy The following search terms were used with various truncations
ldquohydrotherapyldquo ldquoaquatic therapyldquo ldquoaquatic physiotherapyldquo ldquoaquatic physical therapyrdquo
ldquowater therapyrdquo and ldquowater exerciserdquo combined with ldquoinpatientldquo ldquoin-patientldquo ldquomedical
patientldquo ldquosurgical patientldquo ldquohospital patientldquo ldquorehabilitationldquo or ldquolength of stayldquo The
reference lists of all relevant articles were also searched
Database searched The following databases were searched for English language abstracts
from the year 2000-September 2010 CINAHL MEDLINE PUBMED PEDro Cochrane
Library TrIP Database Up to Date Scopus Best Practise MD Consult
Exclusion Criteria Articles were excluded that described aquatic-based rehabilitation in an
outpatient setting Inpatient physiotherapy not specific to aquatic physiotherapy nor able to be
differentiated from concurrent land based therapy or where the nature of water exercise was
not described (including Kneipp Hydrotherapy Spa therapy and Balneotherapy unrelated to
physiotherapy intervention) were excluded
Full-text articles for all relevant abstracts were sourced and selection criteria were applied
Methodological quality was assessed by one reviewer using three separate assessment tools to
reflect the breadth and variety of studies sourced The Oxford Centre for Evidence-based
Medicine Levels of Evidence (OCEBM 2009) where level 1a (systematic reviews of
randomized controlled trials) represents the highest level of evidence or that which is least
flawed and level 5 (expert opinion) represents the most flawed or lowest level of evidence
the PEDro Scale (CEBP 1999) for Randomized Controlled Trials (to help identify which of
the known or suspected randomised clinical trials are likely to be internally valid (criteria 2-
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
9) and could have sufficient statistical information to make their results interpretable (criteria
10-11) and Law et al‟s (1998) Critical Review Form- Quantitative Studies
RESULTS
The search strategy yielded over 100 papers Abstracts sourced from more than one database
were removed On closer review of full text articles many did not meet the inclusion criteria
and were excluded based on aquatic-based rehabilitation occurring in an outpatient setting or
being poorly described and unable to be distinguished from land therapy Four articles were
sourced that described inpatient orthopaedic rehabilitation after hip or knee joint arthroplasty
(THA or TKA) These included one high quality randomized controlled trial (RCT)
(Rahmann et al 2009) and two moderate quality prospective cohort randomized design studies
(Giaquinto et al 2009(a) Giaquinto et al 2009(b) scoring 1b to 2b on the OEBM scale A low
quality single case study describing a cardiopulmonary compromised elderly patient
recovering from THA was also included (Costa et al 2004) From these four studies benefit
in lower limb strength self-reported pain and functional measures and trends in range of
motion limb girth and improved patient satisfaction were attributed to the adjunct of aquatic
physiotherapy to routine care (Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al
2009(b) Costa et al 2004) Particularly in a geriatric population the authors suggest aquatic
physiotherapy be considered after joint arthroplasty surgery as a safe and effective alternative
to routine or additional land-based therapy The benefit of aquatic physiotherapy post joint
arthroplasty as a stand-alone treatment remains unclear
One control case matched study was sourced that investigated an inpatient neurological
population post spinal cord injury (SCI) (Kesiktas et al 2004) Hydrotherapy was added as an
adjunct to the rehabilitation programme of participants who had not reached their functional
targets due to spasticity Compared to a control group patients participating in hydrotherapy
had a statistically significant reduction in spasticity severity and decreased medication use
OEBM scoring is 3b and the study is of low quality due to the small convenience sample size
(n=20) and non-randomization
Representing the lowest level of available evidence (OEBM 4-5) two further case studies
were sourced for clinical interest and completeness One study described the post-operative
spinal surgery rehabilitation in a patient with significant comorbidities and orthopaedic
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
weight-bearing restriction (Fragala-Pinkham et al 2009) The authors concluded that the
integration of an aquatic programme positively impacted on client participation and
motivation level of activity and general body function There was no statistical analysis and
overall quality was low a reflection of single case study design Taylor (2003) undertook a
retrospective case study of a ventilated Guillain Barre Syndrome patient undergoing aquatic
physiotherapy in the acute setting Despite anecdotal improvements in muscle size and
strength lack of structured methodology and valid and reliable outcomes means we are unable
to draw clear recommendations for the application of hydrotherapy in the wider critical care
population
As evidence of further methodological and quality assessment for all of the above studies
Table 2 indicates the yesno response to sixteen short answer questions from Law et al‟s
(1998) Critical Review Form- Quantitative Studies A ldquoyesrdquo answer indicates the study met
the domain criteria with a higher overall number of ldquoyesrdquo answers reflecting stronger
methodological quality Where applicable PEDro scores for Randomised Control Trials
(CEBP 1999) are presented in Table 3
A summary of each study‟s main findings including outcome measures assessment and
details of the aquatic program are included in Table 4
DISCUSSION
Aquatic physiotherapy in the early stages after surgery injury illness neurological event or
disease is largely understudied Conducting research in an inpatient rehabilitation setting may
be confounded by difficulty in sourcing large numbers of homogenous patient groups and
complex interventions often not suitable for application in the generic group setting
(Geytenbeek 2008) Potential constraints to study recruitment and retention include medical
unsuitability or short hospital length of stay meaning descriptive and comparative case studies
may be more readily undertaken than high quality research trials
Despite physiotherapy and aquatic intervention being treatments of choice by clinicians the
acute phase following joint arthroplasty is one of the most understudied aspects in the
literature with wide variance in the modes of service delivery (Harmer et al 2009 Lawson
2009 Naylor et al 2006 Roos 2003) With growing disability from osteoarthritis contributing
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
2002 Geytenbeek 2008 Bartels et al 2009) In osteoarthritis gold level evidence supports
the use of aquatic therapy for short term slight improvement in pain and function (Bartels et al
2007) while benefits in disability strength range of motion pain flexibility balance well-
being cost-effectiveness heath status and quality of life are also demonstrated (Geytenbeek
2002 Geytenbeek 2008) Scientific grounds and evidence from outpatient studies support the
use of aquatic physiotherapy in post-surgical rehabilitation and orthopaedic injury (Ahlqvist
2002 Fappiano and Gangaway 2008 Watts and Gangaway 2007) It has been demonstrated
that aquatic intervention can facilitate early initiation of exercise improve self-reported pain
and function and contribute to greater range of motion strength proprioception and decreased
risk of further injury (Fappiano and Gangaway 2008 Watts and Gangaway 2007 McAvoy
2009) In anterior cruciate ligament (ACL) rehabilitation aquatic physiotherapy has been
attributed to reduced joint effusion and earlier gains in range of motion (McClintock and
Kirkley 1995 Tovin et al 1994) In a reduced weight bearing environment which minimises
joint stress it is likely that the physiological and thermal properties of water including
hydrostatic pressure and buoyancy effect enable early initiation of exercise and increased
activity tolerance
Limited evidence exists to support the use of aquatic physiotherapy in inpatient populations
including acute orthopaedic rehabilitation (Geytenbeek 2008) Land-based studies of
intensive rehabilitation programmes and additional physiotherapy in the hospital setting
clearly demonstrate a positive relationship between physiotherapy service and positive patient
outcomes Increased intensity and frequency of physiotherapy intervention has been shown to
benefit parameters of functional mobility and total hospital cost including discharge
destination and reduced length of stay (Boxall 2004 Freburger 2000 Kirk-Sanchez 2001
Lawson 2006 Moffet 2004 and Roach 1998 Weigl 2003) In the post-operative recovery of
high risk patients undergoing elective hip or knee arthroplasty early inpatient rehabilitation
(day 3 instead of 7) was well tolerated and contributed to earlier obtainment of functional
goals at less overall cost (Munin et al 1998) Considering that aquatic physiotherapy is
indicated where land based activity is contraindicated due to pain or acute injury (Babb and
Simelson-Warr 1994) it is possible that aquatic physiotherapy could be used as a substitute
for land-based rehabilitation The inpatient setting provides a unique opportunity to explore
the use of aquatic physiotherapy in hospital patients recovering from surgery injury illness or
disease This review of the literature aims to investigate what evidence exists to support the
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
use of aquatic physiotherapy in the inpatient setting across the orthopaedic neurological and
general medical disciplines
METHODSSELECTION OF ARTICLES
Inclusion criteria All studies describing aquatic physiotherapy as an inpatient intervention
were included There was no limitation on the type of studies participants nor outcomes
selected for inclusion
Search Strategy The following search terms were used with various truncations
ldquohydrotherapyldquo ldquoaquatic therapyldquo ldquoaquatic physiotherapyldquo ldquoaquatic physical therapyrdquo
ldquowater therapyrdquo and ldquowater exerciserdquo combined with ldquoinpatientldquo ldquoin-patientldquo ldquomedical
patientldquo ldquosurgical patientldquo ldquohospital patientldquo ldquorehabilitationldquo or ldquolength of stayldquo The
reference lists of all relevant articles were also searched
Database searched The following databases were searched for English language abstracts
from the year 2000-September 2010 CINAHL MEDLINE PUBMED PEDro Cochrane
Library TrIP Database Up to Date Scopus Best Practise MD Consult
Exclusion Criteria Articles were excluded that described aquatic-based rehabilitation in an
outpatient setting Inpatient physiotherapy not specific to aquatic physiotherapy nor able to be
differentiated from concurrent land based therapy or where the nature of water exercise was
not described (including Kneipp Hydrotherapy Spa therapy and Balneotherapy unrelated to
physiotherapy intervention) were excluded
Full-text articles for all relevant abstracts were sourced and selection criteria were applied
Methodological quality was assessed by one reviewer using three separate assessment tools to
reflect the breadth and variety of studies sourced The Oxford Centre for Evidence-based
Medicine Levels of Evidence (OCEBM 2009) where level 1a (systematic reviews of
randomized controlled trials) represents the highest level of evidence or that which is least
flawed and level 5 (expert opinion) represents the most flawed or lowest level of evidence
the PEDro Scale (CEBP 1999) for Randomized Controlled Trials (to help identify which of
the known or suspected randomised clinical trials are likely to be internally valid (criteria 2-
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
9) and could have sufficient statistical information to make their results interpretable (criteria
10-11) and Law et al‟s (1998) Critical Review Form- Quantitative Studies
RESULTS
The search strategy yielded over 100 papers Abstracts sourced from more than one database
were removed On closer review of full text articles many did not meet the inclusion criteria
and were excluded based on aquatic-based rehabilitation occurring in an outpatient setting or
being poorly described and unable to be distinguished from land therapy Four articles were
sourced that described inpatient orthopaedic rehabilitation after hip or knee joint arthroplasty
(THA or TKA) These included one high quality randomized controlled trial (RCT)
(Rahmann et al 2009) and two moderate quality prospective cohort randomized design studies
(Giaquinto et al 2009(a) Giaquinto et al 2009(b) scoring 1b to 2b on the OEBM scale A low
quality single case study describing a cardiopulmonary compromised elderly patient
recovering from THA was also included (Costa et al 2004) From these four studies benefit
in lower limb strength self-reported pain and functional measures and trends in range of
motion limb girth and improved patient satisfaction were attributed to the adjunct of aquatic
physiotherapy to routine care (Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al
2009(b) Costa et al 2004) Particularly in a geriatric population the authors suggest aquatic
physiotherapy be considered after joint arthroplasty surgery as a safe and effective alternative
to routine or additional land-based therapy The benefit of aquatic physiotherapy post joint
arthroplasty as a stand-alone treatment remains unclear
One control case matched study was sourced that investigated an inpatient neurological
population post spinal cord injury (SCI) (Kesiktas et al 2004) Hydrotherapy was added as an
adjunct to the rehabilitation programme of participants who had not reached their functional
targets due to spasticity Compared to a control group patients participating in hydrotherapy
had a statistically significant reduction in spasticity severity and decreased medication use
OEBM scoring is 3b and the study is of low quality due to the small convenience sample size
(n=20) and non-randomization
Representing the lowest level of available evidence (OEBM 4-5) two further case studies
were sourced for clinical interest and completeness One study described the post-operative
spinal surgery rehabilitation in a patient with significant comorbidities and orthopaedic
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
weight-bearing restriction (Fragala-Pinkham et al 2009) The authors concluded that the
integration of an aquatic programme positively impacted on client participation and
motivation level of activity and general body function There was no statistical analysis and
overall quality was low a reflection of single case study design Taylor (2003) undertook a
retrospective case study of a ventilated Guillain Barre Syndrome patient undergoing aquatic
physiotherapy in the acute setting Despite anecdotal improvements in muscle size and
strength lack of structured methodology and valid and reliable outcomes means we are unable
to draw clear recommendations for the application of hydrotherapy in the wider critical care
population
As evidence of further methodological and quality assessment for all of the above studies
Table 2 indicates the yesno response to sixteen short answer questions from Law et al‟s
(1998) Critical Review Form- Quantitative Studies A ldquoyesrdquo answer indicates the study met
the domain criteria with a higher overall number of ldquoyesrdquo answers reflecting stronger
methodological quality Where applicable PEDro scores for Randomised Control Trials
(CEBP 1999) are presented in Table 3
A summary of each study‟s main findings including outcome measures assessment and
details of the aquatic program are included in Table 4
DISCUSSION
Aquatic physiotherapy in the early stages after surgery injury illness neurological event or
disease is largely understudied Conducting research in an inpatient rehabilitation setting may
be confounded by difficulty in sourcing large numbers of homogenous patient groups and
complex interventions often not suitable for application in the generic group setting
(Geytenbeek 2008) Potential constraints to study recruitment and retention include medical
unsuitability or short hospital length of stay meaning descriptive and comparative case studies
may be more readily undertaken than high quality research trials
Despite physiotherapy and aquatic intervention being treatments of choice by clinicians the
acute phase following joint arthroplasty is one of the most understudied aspects in the
literature with wide variance in the modes of service delivery (Harmer et al 2009 Lawson
2009 Naylor et al 2006 Roos 2003) With growing disability from osteoarthritis contributing
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
use of aquatic physiotherapy in the inpatient setting across the orthopaedic neurological and
general medical disciplines
METHODSSELECTION OF ARTICLES
Inclusion criteria All studies describing aquatic physiotherapy as an inpatient intervention
were included There was no limitation on the type of studies participants nor outcomes
selected for inclusion
Search Strategy The following search terms were used with various truncations
ldquohydrotherapyldquo ldquoaquatic therapyldquo ldquoaquatic physiotherapyldquo ldquoaquatic physical therapyrdquo
ldquowater therapyrdquo and ldquowater exerciserdquo combined with ldquoinpatientldquo ldquoin-patientldquo ldquomedical
patientldquo ldquosurgical patientldquo ldquohospital patientldquo ldquorehabilitationldquo or ldquolength of stayldquo The
reference lists of all relevant articles were also searched
Database searched The following databases were searched for English language abstracts
from the year 2000-September 2010 CINAHL MEDLINE PUBMED PEDro Cochrane
Library TrIP Database Up to Date Scopus Best Practise MD Consult
Exclusion Criteria Articles were excluded that described aquatic-based rehabilitation in an
outpatient setting Inpatient physiotherapy not specific to aquatic physiotherapy nor able to be
differentiated from concurrent land based therapy or where the nature of water exercise was
not described (including Kneipp Hydrotherapy Spa therapy and Balneotherapy unrelated to
physiotherapy intervention) were excluded
Full-text articles for all relevant abstracts were sourced and selection criteria were applied
Methodological quality was assessed by one reviewer using three separate assessment tools to
reflect the breadth and variety of studies sourced The Oxford Centre for Evidence-based
Medicine Levels of Evidence (OCEBM 2009) where level 1a (systematic reviews of
randomized controlled trials) represents the highest level of evidence or that which is least
flawed and level 5 (expert opinion) represents the most flawed or lowest level of evidence
the PEDro Scale (CEBP 1999) for Randomized Controlled Trials (to help identify which of
the known or suspected randomised clinical trials are likely to be internally valid (criteria 2-
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
9) and could have sufficient statistical information to make their results interpretable (criteria
10-11) and Law et al‟s (1998) Critical Review Form- Quantitative Studies
RESULTS
The search strategy yielded over 100 papers Abstracts sourced from more than one database
were removed On closer review of full text articles many did not meet the inclusion criteria
and were excluded based on aquatic-based rehabilitation occurring in an outpatient setting or
being poorly described and unable to be distinguished from land therapy Four articles were
sourced that described inpatient orthopaedic rehabilitation after hip or knee joint arthroplasty
(THA or TKA) These included one high quality randomized controlled trial (RCT)
(Rahmann et al 2009) and two moderate quality prospective cohort randomized design studies
(Giaquinto et al 2009(a) Giaquinto et al 2009(b) scoring 1b to 2b on the OEBM scale A low
quality single case study describing a cardiopulmonary compromised elderly patient
recovering from THA was also included (Costa et al 2004) From these four studies benefit
in lower limb strength self-reported pain and functional measures and trends in range of
motion limb girth and improved patient satisfaction were attributed to the adjunct of aquatic
physiotherapy to routine care (Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al
2009(b) Costa et al 2004) Particularly in a geriatric population the authors suggest aquatic
physiotherapy be considered after joint arthroplasty surgery as a safe and effective alternative
to routine or additional land-based therapy The benefit of aquatic physiotherapy post joint
arthroplasty as a stand-alone treatment remains unclear
One control case matched study was sourced that investigated an inpatient neurological
population post spinal cord injury (SCI) (Kesiktas et al 2004) Hydrotherapy was added as an
adjunct to the rehabilitation programme of participants who had not reached their functional
targets due to spasticity Compared to a control group patients participating in hydrotherapy
had a statistically significant reduction in spasticity severity and decreased medication use
OEBM scoring is 3b and the study is of low quality due to the small convenience sample size
(n=20) and non-randomization
Representing the lowest level of available evidence (OEBM 4-5) two further case studies
were sourced for clinical interest and completeness One study described the post-operative
spinal surgery rehabilitation in a patient with significant comorbidities and orthopaedic
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
weight-bearing restriction (Fragala-Pinkham et al 2009) The authors concluded that the
integration of an aquatic programme positively impacted on client participation and
motivation level of activity and general body function There was no statistical analysis and
overall quality was low a reflection of single case study design Taylor (2003) undertook a
retrospective case study of a ventilated Guillain Barre Syndrome patient undergoing aquatic
physiotherapy in the acute setting Despite anecdotal improvements in muscle size and
strength lack of structured methodology and valid and reliable outcomes means we are unable
to draw clear recommendations for the application of hydrotherapy in the wider critical care
population
As evidence of further methodological and quality assessment for all of the above studies
Table 2 indicates the yesno response to sixteen short answer questions from Law et al‟s
(1998) Critical Review Form- Quantitative Studies A ldquoyesrdquo answer indicates the study met
the domain criteria with a higher overall number of ldquoyesrdquo answers reflecting stronger
methodological quality Where applicable PEDro scores for Randomised Control Trials
(CEBP 1999) are presented in Table 3
A summary of each study‟s main findings including outcome measures assessment and
details of the aquatic program are included in Table 4
DISCUSSION
Aquatic physiotherapy in the early stages after surgery injury illness neurological event or
disease is largely understudied Conducting research in an inpatient rehabilitation setting may
be confounded by difficulty in sourcing large numbers of homogenous patient groups and
complex interventions often not suitable for application in the generic group setting
(Geytenbeek 2008) Potential constraints to study recruitment and retention include medical
unsuitability or short hospital length of stay meaning descriptive and comparative case studies
may be more readily undertaken than high quality research trials
Despite physiotherapy and aquatic intervention being treatments of choice by clinicians the
acute phase following joint arthroplasty is one of the most understudied aspects in the
literature with wide variance in the modes of service delivery (Harmer et al 2009 Lawson
2009 Naylor et al 2006 Roos 2003) With growing disability from osteoarthritis contributing
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
9) and could have sufficient statistical information to make their results interpretable (criteria
10-11) and Law et al‟s (1998) Critical Review Form- Quantitative Studies
RESULTS
The search strategy yielded over 100 papers Abstracts sourced from more than one database
were removed On closer review of full text articles many did not meet the inclusion criteria
and were excluded based on aquatic-based rehabilitation occurring in an outpatient setting or
being poorly described and unable to be distinguished from land therapy Four articles were
sourced that described inpatient orthopaedic rehabilitation after hip or knee joint arthroplasty
(THA or TKA) These included one high quality randomized controlled trial (RCT)
(Rahmann et al 2009) and two moderate quality prospective cohort randomized design studies
(Giaquinto et al 2009(a) Giaquinto et al 2009(b) scoring 1b to 2b on the OEBM scale A low
quality single case study describing a cardiopulmonary compromised elderly patient
recovering from THA was also included (Costa et al 2004) From these four studies benefit
in lower limb strength self-reported pain and functional measures and trends in range of
motion limb girth and improved patient satisfaction were attributed to the adjunct of aquatic
physiotherapy to routine care (Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al
2009(b) Costa et al 2004) Particularly in a geriatric population the authors suggest aquatic
physiotherapy be considered after joint arthroplasty surgery as a safe and effective alternative
to routine or additional land-based therapy The benefit of aquatic physiotherapy post joint
arthroplasty as a stand-alone treatment remains unclear
One control case matched study was sourced that investigated an inpatient neurological
population post spinal cord injury (SCI) (Kesiktas et al 2004) Hydrotherapy was added as an
adjunct to the rehabilitation programme of participants who had not reached their functional
targets due to spasticity Compared to a control group patients participating in hydrotherapy
had a statistically significant reduction in spasticity severity and decreased medication use
OEBM scoring is 3b and the study is of low quality due to the small convenience sample size
(n=20) and non-randomization
Representing the lowest level of available evidence (OEBM 4-5) two further case studies
were sourced for clinical interest and completeness One study described the post-operative
spinal surgery rehabilitation in a patient with significant comorbidities and orthopaedic
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
weight-bearing restriction (Fragala-Pinkham et al 2009) The authors concluded that the
integration of an aquatic programme positively impacted on client participation and
motivation level of activity and general body function There was no statistical analysis and
overall quality was low a reflection of single case study design Taylor (2003) undertook a
retrospective case study of a ventilated Guillain Barre Syndrome patient undergoing aquatic
physiotherapy in the acute setting Despite anecdotal improvements in muscle size and
strength lack of structured methodology and valid and reliable outcomes means we are unable
to draw clear recommendations for the application of hydrotherapy in the wider critical care
population
As evidence of further methodological and quality assessment for all of the above studies
Table 2 indicates the yesno response to sixteen short answer questions from Law et al‟s
(1998) Critical Review Form- Quantitative Studies A ldquoyesrdquo answer indicates the study met
the domain criteria with a higher overall number of ldquoyesrdquo answers reflecting stronger
methodological quality Where applicable PEDro scores for Randomised Control Trials
(CEBP 1999) are presented in Table 3
A summary of each study‟s main findings including outcome measures assessment and
details of the aquatic program are included in Table 4
DISCUSSION
Aquatic physiotherapy in the early stages after surgery injury illness neurological event or
disease is largely understudied Conducting research in an inpatient rehabilitation setting may
be confounded by difficulty in sourcing large numbers of homogenous patient groups and
complex interventions often not suitable for application in the generic group setting
(Geytenbeek 2008) Potential constraints to study recruitment and retention include medical
unsuitability or short hospital length of stay meaning descriptive and comparative case studies
may be more readily undertaken than high quality research trials
Despite physiotherapy and aquatic intervention being treatments of choice by clinicians the
acute phase following joint arthroplasty is one of the most understudied aspects in the
literature with wide variance in the modes of service delivery (Harmer et al 2009 Lawson
2009 Naylor et al 2006 Roos 2003) With growing disability from osteoarthritis contributing
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
weight-bearing restriction (Fragala-Pinkham et al 2009) The authors concluded that the
integration of an aquatic programme positively impacted on client participation and
motivation level of activity and general body function There was no statistical analysis and
overall quality was low a reflection of single case study design Taylor (2003) undertook a
retrospective case study of a ventilated Guillain Barre Syndrome patient undergoing aquatic
physiotherapy in the acute setting Despite anecdotal improvements in muscle size and
strength lack of structured methodology and valid and reliable outcomes means we are unable
to draw clear recommendations for the application of hydrotherapy in the wider critical care
population
As evidence of further methodological and quality assessment for all of the above studies
Table 2 indicates the yesno response to sixteen short answer questions from Law et al‟s
(1998) Critical Review Form- Quantitative Studies A ldquoyesrdquo answer indicates the study met
the domain criteria with a higher overall number of ldquoyesrdquo answers reflecting stronger
methodological quality Where applicable PEDro scores for Randomised Control Trials
(CEBP 1999) are presented in Table 3
A summary of each study‟s main findings including outcome measures assessment and
details of the aquatic program are included in Table 4
DISCUSSION
Aquatic physiotherapy in the early stages after surgery injury illness neurological event or
disease is largely understudied Conducting research in an inpatient rehabilitation setting may
be confounded by difficulty in sourcing large numbers of homogenous patient groups and
complex interventions often not suitable for application in the generic group setting
(Geytenbeek 2008) Potential constraints to study recruitment and retention include medical
unsuitability or short hospital length of stay meaning descriptive and comparative case studies
may be more readily undertaken than high quality research trials
Despite physiotherapy and aquatic intervention being treatments of choice by clinicians the
acute phase following joint arthroplasty is one of the most understudied aspects in the
literature with wide variance in the modes of service delivery (Harmer et al 2009 Lawson
2009 Naylor et al 2006 Roos 2003) With growing disability from osteoarthritis contributing
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
to increasing incidence of joint replacement surgery in Australia and worldwide there is
increasing pressure to contain costs reduce hospital length of stay and establish the most
efficient and effective clinical pathways for patients recovering from joint replacement
surgery in the inpatient setting (Rahmann et al 2009)
Rahmann et al (2009) designed a prospective randomised controlled trial to evaluate the
effect of inpatient aquatic physiotherapy in addition to usual ward physiotherapy Outcome
measures were evaluated relating to strength function and gait speed at baseline and at day
14 90 and 180 after total hip or knee replacement surgery The number of different and
validreliable outcome measurements assessor blinding and use of a general ldquowater exerciserdquo
control contributes methodological strength to this article Main findings were a significant
increase in hip abductor strength at day 14 after aquatic physiotherapy compared to additional
ward treatment or water exercise This is clinically significant in the context that hip abductor
weakness was the most common muscle weakness post THA that can result in ipsilateral
trunk flexion during stance phase and a Trendelenberg gait (Bhave et al 2007 in Costa et al
2009) Secondary outcome measures of length of stay and occasions of physiotherapy service
were analysed without significant difference when comparing the aquatic with the ward or
water exercise groups No adverse events occurred with early aquatic intervention There
was a trend towards reduced swelling and knee circumference that was not statistically
different A justified sample of 65 patients were recruited for this study yet small group
numbers (n=20-24) and an increasing loss to follow-up of 26 by day 180 may lessen the
power calculation and quality of this article
Giaquinto et al (2009) in two separate studies(a)(b) used a prospective randomised design to
follow up of a cohort of patients who underwent TKA and THA Using the same
methodology patients were randomly allocated to a conventional gym treatment or
hydrotherapy group and interviewed with Western-Ontario McMasters Universities
Osteoarthritis Index (WOMAC) the gold standard for self-perceived functional status in OA
and total joint arthroplasty (Bellamy et al 2005 in Giaquinto et al 2009(a) Scores were
obtained at admission to a rehabilitation unit at discharge and 6 months later Both studies
reported subjective improvement in pain stiffness and function in both intervention groups
with WOMAC sub-scales significantly lower for all patients undergoing hydrotherapy
Benefits gained at discharge still remained at the 6 month follow-up mark
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Weaknesses of both Rahmann et al‟s (2009) and Giaquinto et al‟s (2009) two studies is the
lack of control for confounding factors in the 6 month period post discharge In Giaquinto et
al (2009) there was no intention-to-treat analysis and a loss to follow up of 17 (1270) in
study(b) compared to 9 (674) in study(a) casting doubt on the internal validity of the TKA
trial(b) in particular using PEDro‟s (CEBP 1999) scoring criteria Assessor blinding and
group randomisation lends strength to these studies however unlike Rahmann et al‟s (2009)
comprehensive physiotherapy exercise prescription there was a lack of clear description of
either water or land therapy in Giaquinto et al‟s (2009) two studies making the intervention
difficult to replicate in a clinical setting Participants in Giaquinto et al‟s (2009) hydrotherapy
groups received 20 minutes of passive joint motion followed by 40 minutes of treatment in
water The control groups received land therapy followed by a bdquoneutral‟ massage on the hip
or knee scar for 20 minutes The inclusion of massage and joint mobilisation could be seen as
a source of co-intervention which may confound results Yoshida et al (2008) cited in
Rahmann et al (2009) suggest that the multi-faceted disability from osteoarthritis means a
single outcome measure or domain is likely to be inadequate for measuring the true nature of
post-operative recovery The use of only a single qualitative outcome measure and no
physical measures is a limitation to interpretation and wider application of the findings in
Giaquinto et al‟s (2009) randomised cohort trials and a potential source of measurement bias
(Law et al 1998)
While providing low quality evidence as far as research methodology and widespread
application case studies give an insight into the role of aquatic therapy in often complex
clinical scenarios Costa et al‟s (2009) single case study of a cardiopulmonary compromised
patient who underwent THA supports the use of early aquatic intervention in the acute
rehabilitation setting Improvement was demonstrated in range of motion strength girth and
pain The authors conclude that in the geriatric population with comorbidities aquatic
intervention may be well tolerated less painful than land therapy and can lead to earlier
functional improvements and patient satisfaction As cited in Costa et al (2009) their findings
are consistent with Hall and Brody‟s (1999) assertion that aquatic therapy as an alternative to
land-based therapy may be more tolerable in post-operative patients who are deconditioned
The lack of cardiopulmonary complication on immersion is supported by Perk et al‟s (1996)
study of a cohort of non-hypoxaemic normotensive chronic obstructive pulmonary disease
patients who were able to exercise sub-maximally in a hydrotherapy environment safely and
without desaturation arrhythmia or discomfort that was deemed clinically relevant In Costa
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
et al‟s (2009) case study there was an attempt to use reliable and valid outcome measures
although no statistical analysis was performed and there was no intention to control for
confounding factors High motivation and high pre-morbid activity may also have
contributed to patientbdquos improvement A conclusion cannot be drawn as to the benefit of land
versus aquatic intervention
Aquatic exercise is often recommended as an adjunct to land based therapy as part of an
integrated rehabilitation programme A review of lower limb orthopaedic literature found that
when used together water and land based interventions are more effective in treating lower
extremity injuries than land based treatment alone (Fappiano and Gangaway 2008) Findings
of improved strength (Rahmann et al 2009) and functional measures (Giaquinto et al 2009(a)
Giaquinto et al 2009(b) Costa et al 2009) with the addition of aquatic physiotherapy is a
finding not always consistent with orthopaedic and musculoskeletal literature Investigations
of aquatic exercise compared to land based intervention in outpatient studies often yield
similar results or no added benefit raising doubt about the cost-effectiveness of offering
particularly in-house aquatic intervention (Geytenbeek 2008 Harmer et al 2009) While
aquatic intervention may be better tolerated in TKR and OA it has also been demonstrated
that exercise in water compared to land may not be as effective in regaining maximal muscle
performance in ACL rehabilitation (Tovin et al 1994) or in improving strength and pain in
knee OA (Lund et al 2008) Variable expert opinion means it is increasingly necessary to
justify aquatic intervention with sound clinical reasoning and improve the specificity and
intensity of exercises using the unique properties of water to replicate the strength gains
achievable on land Improving reporting quality of aquatic exercise in the literature is a
promising trend that will aid replication in the clinical setting
A case series by Fragala-Pinkham et al (2009) investigated the effect of inpatient orthopaedic
aquatic rehabilitation and the feasibility of treating a participant with a complex history A 19
year old obese participant had undergone L1sacrum spinal fusion on a background of Prader-
Willi Syndrome and a history of multiple spinal surgeries and complications After a period
of bed-rest due to orthopaedic non-weight-bearing (NWB) restriction the patient was cleared
to participate in upright standing activities in water and an intensive aquatic programme was
initiated A variety of valid and reliable outcome measures were used and reported in
measures of Minimal Important Difference (MID) and Mean Detectable Change (MDC)
Intervention was well described and resulted in a clinically significant improvement in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
functional mobility as well as improved walking endurance pain scores and lower extremity
strength on manual muscle testing Obvious limitations of the study were lack of statistical
analysis and co-intervention of land and aquatic therapy from 12 weeks post-operatively
meaning no conclusions could be drawn as to the relative benefit of either intervention
Single case studies have inherently very poor applicability to wider populations and offer low
quality evidence to the research pool
Despite having a vital role in functional recovery in the neurological population (Kesiktas
2004) Geytenbeek (2008) highlights that this is one area where there is a need for quality
aquatic physiotherapy research Single case studies in SCI and traumatic brain injury have
demonstrated that aquatic physiotherapy contributes to improvement in long term functional
outcomes as part of neurological rehabilitation (Degano et al 2009 Stowell et al 2001) Noh
et al (2007) found that when compared to conventional therapy outpatient stroke survivors
participating in aquatic physiotherapy participants showed improved balance and strength in
the hemi-paretic leg With the bulk of neurological aquatic research conducted in outpatient
post-acute rehabilitation settings only 2 studies were found describing aquatic intervention in
the inpatient setting in this current review
Kesiktas et al (2004) conducted a control case matched study to compare the effects of
hydrotherapy on spasticity and functional independence measures (FIM) in twenty patients
with SCI While both control and hydrotherapy intervention groups made significant
improvement in functional scores the hydrotherapy group made a larger improvement
(plt00001) and demonstrated a significant decrease in oral baclofen use and muscle spasm
severity (plt002) Both groups gained significant improved in spasticity as measured by the
Ashworth Scale Lack of blinding and randomisation through bdquoconvenience sampling‟ as well
as the small number of participants make it difficult to generalise findings to the wider SCI
population although reduced medication use is a positive trend consistent with previous SCI
literature (Giesecke 1997)
In a Single Case Study Taylor (2003) described a detailed protocol requiring combined
medical nursing and physiotherapy staff cooperation to facilitate the treatment of an intensive
care ventilated Guillain Barre Syndrome patient in the water 2-3 times per week for 7 months
The purpose of the intervention was to benefit morale facilitate graduated weight bearing and
improve muscle strength and range of motion in an otherwise highly physically dependent
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
patient A lack of valid or reliable outcomes measures makes it difficult to draw conclusions
and wider recommendations from this study Furthermore costbenefit analysis would assist
in determining whether the benefit of reducing Intensive Critical Care Unit (ICCU) length of
stay is offset by the intensive staff requirements to allow treatment to take place Interestingly
the author purports that due to the high per patient costs in an ICCU environment facilitating
early ventilator weaning so as to reduce length of stay by only 1-2 weeks could be seen as cost
effective compared to long-term ventilator dependence
CONCLUSION
A comprehensive database search yielded 7 studies describing aquatic physiotherapy taking
place in an inpatient population Level 1b to 2b moderate to high quality evidence from three
randomised control trials supports the use of aquatic physiotherapy in the early post-operative
phase after lower limb joint arthroplasty as a safe and effective modality for consideration
(Rahmann et al 2009 Giaquinto et al 2009(a) Giaquinto et al 2009(b) Early improvement in
lower limb strength compared to land based or general water exercise has been demonstrated
on physical measures (Rahmann et al 2009) Qualitative self-reported data of pain stiffness
and function can be positively influenced in geriatric patients who underwent total hip or knee
joint arthroplasty compared to land based (Giaquinto et al 2009(a) Giaquinto et al 2009(b)
Aquatic intervention contributes to less post exercise soreness improved pain and functional
measures and a reduction in swelling and lower limb girth in the orthopaedic population
(Costa et al 2009 Fappiano and Gangaway 2008 Giaquinto et al 2009(a) Giaquinto et al
2009(b) McClintock 1995 Rahmann et al 2009 Tovin et al 2009) It may be a preferred
mode of treatment where pain comorbidities severe debility or weight-bearing restriction
make it difficult for a patient to exercise on land (Babb and Simelson-Warr 1994 Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003)
Low level 3b evidence supports the use of aquatic physiotherapy to reduce spasticity severity
decrease medication use and improve functional independence scores in SCI (Kesiktas et al
2004) Very low quality evidence from case studies investigate the application of aquatic
intervention in a cardiopulmonary individual status post THA a young orthopaedic patient
with bilateral weight bearing restrictions post spinal fusion surgery and a ventilated patient
with severe neuromuscular weakness secondary to Guillain Barre Syndrome (Costa et al
2009 Fragala-Pinkham et al 2009 Taylor 2003) These individual studies are important in
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
their capacity to describe complex clinical scenarios in detail with good aquatic exercise
specificity and description Individual case studies demonstrate that even in an acute
population recovering from orthopaedic surgery neuromuscular insult or with
cardiorespiratory compromise aquatic physiotherapy can be a safe and effective mode of
treatment There is particular scope for application in functional rehabilitation of geriatric
deconditioned patients with benefit in strength range of movement and morale paving the
way for further research into the area (Costa et al 2009 Giaquinto et al 2009(a) Giaquinto et
al 2009(b)
To my knowledge there are no studies to date that investigate the cost effectiveness of
operating an in-house hydrotherapy pool for inpatient use There is little investigation and no
significant findings on the potential for inpatient aquatic rehabilitation to contribute to earlier
obtainment of functional goals less physiotherapy occasions of service or reduced length of
hospital stay More high quality studies are needed comparing land versus aquatic therapy in
the inpatient setting in a wide population of patients Attention to true randomisation
increased patient numbers assessor blinding using general water exercise as a control and
the use of a battery of tests for reliable and valid outcome measures will improve the quality
of available evidence in this area
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
REFERENCES
Ahlqvist J (2002) Hydrotherapy has had and has a rationale Rheumatology (Oxford) 41 p
1070-1071
Babb R Simelson-Warr A (1994) Manual techniques of the lower extremities in aquatic
physical therapy Journal of Aquatic Physical Therapy 74710-19
Bartels EM Lund H Hagen K B Dagfinrud H Christensen R Danneskiold-Samsoe B (2009)
Aquatic exercise for the treatment of knee and hip osteoarthritis Cochrane Database of
Systematic Reviews 2007 Issue 4 art No CD005523
Boxall A Sayers A Kaplan GA (2004) A cohort study of 7 day a week physiotherapy on an
acute orthopedic ward Journal of Orthopedic Nursing 8(2) 96-102
Costa B Wilmarth MA Glynn PE (2009) Rehabilitation of a cardiopulmonary compromised
individual status-post total hip arthroplasty utilizing a combined land and aquatic based
program a case report Journal of Aquatic Physical Therapy 17(2) 12-19
Degano AC Geigle PR (2009) Use of aquatic physical therapy in the treatment of balance and
gait impairments following traumatic brain injury A case report Journal of Aquatic Physical
Therapy 17(1) 16-21
Fappiano M Gangaway JMK (2008) Aquatic physical therapy improves joint mobility
strength and edema in lower extremity orthopedic injuries The ournal of Aquatic Physical
Therapy 16(1) 10-15
Fragala-Pinkham MA Dumas HM Barlow CA Pasternak A (2009) An aquatic physical
therapy program at a pediatric rehabilitation hospital a case series Pediatric Physical Therapy
21(1) 68-78
Freburger JK (2000) An analysis of the relationship between the utilization of physical
therapy services and outcomes of care for patients after total hip arthroplasty Physical
Therapy 80(5) 448-58
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Geytenbeek J (2002) Evidence for effective hydrotherapy Physiotherapy 88(9)514-529
Geytenbeek J (2008) Aquatic Physiotherapy Evidence-Based Practice Guide National
Aquatic Physiotherapy Group Australian Physiotherapy Association
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(a) Hydrotherapy after total hip
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5092-95
Giaquinto S Ciatola E Dall‟Armi V Margutti F (2009)(b) Hydrotherapy after total knee
arthroplasty A follow-up study Archives of Gerontology and Geriatrics 5159-63
Giaquinto S Ferdinando M (2004) A special pool project for rehabilitation of hip and knee
arthroprosthesis Franco Romano Disability amp Rehabilitation 26(19) 1158-1162
Giesecke C (1997) Aquatic rehabilitation of clients with spinal cord injury In Ruoti RG
Morris DM Cole J eds Aquatic Rehabilitation Hagerstown MD Lippincott Williams and
Wilkins pp 125-50
Kesiktas N Paker N Erdogen N Gulsen G Bicki D and Yilmaz H (2004) The Use of
Hydrotherapy for the Management of Spasticity Neurorehabilitation and Repair 18(4) 268-
273
Kirk-Sanchez NJ Roach KE (2001) Relationship between duration of therapy services in a
comprehensive rehabilitation program and mobility at discharge in patients with orthopedic
problems Physical Therapy 81(3) 888-95
Law M Stewart D Pollicj N Letts L Bosch J Westmorland M (1998) Critical Review Form-
Quantitative Studies McMaster University
httpfhsmcmastercarehabebppdfquanreviewpdf [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Lawson D (2009) Comparing outcomes of patients following total knee replacement does
frequency of physical therapy treatment affect outcomes in the acute care setting A case
study Acute Care Perspectives June 2009
Lund H Weile U Christensen R Rostock B Downey A Bartels EM Danneskiod-Samsoe B
Bliddal H (2008) A Randomized Controlled Trial of Aquatic and land based exercise in
participants with knee osteoarthritis J Rehabil Med 40 137-144
McAvoy R (2009) Aquatic and Land Based Therapy vs Land Therapy on the Outcome of
Total Knee Arthroplasty A Pilot Randomized Clinical Trial Journal of Aquatic Physical
Therapy 17(1) 8-15
McClintock A Kirkley PJ (1995) Prospective randomized clinical trial of standard
physiotherapy versus aquatic therapy for early rehabilitation of the ACL reconstructed knee
Clinical Journal of Sports Medicine 5(4)
Moffet H Collet J-P Shapiro SH Paradis G Marquis F Roy L (2004) Effectiveness of
intensive rehabilitation on functional ability and quality of life after first total knee
arthroplasty a single-blind randomized controlled trial Archives of Physical Medicine amp
Rehabilitation 85546-56
Munin MC Rudy TE Glynn NW Crossett LS Rubash HE (1998) Early inpatient
rehabilitation after elective hip and knee arthroplasty JAMA Mar 18279(11)847-52
Naylor J Harmer A Fransen M Crosbie J Innes L (2006) Status of physiotherapy
rehabilitation after total knee replacement in Australia
Physiotherapy Research International 11(1)35-47
Noh DK Lim JY Shin HI Paik NJ (2008) The effect of aquatic therapy on postural balance
and muscle strength in stroke survivors--a randomized controlled pilot trial Clinical
Rehabilitation 22(10-11)966-76
OCEBM (2001) Oxford Centre for Evidence-based Medicine Levels of Evidence (May 2001)
httpwwwcebmnetindexaspxo=1025 [Accessed October-November 2010]
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Oldmeadow LB McBurney H and Robertson VJ (2002) Hospital stay and discharge
outcomes after knee arthroplasty Implications for physiotherapy practice Australian Journal
of Physiotherapy 48 117-121
PEDro Scale (Updated 1999) Centre for Evidence-Based Physiotherapy Musculoskeletal
Division The George Institute for Global Health Affiliated with the University of Sydney
Available httpwwwpedroorgauenglishdownloadspedro-scale [Accessed October-
November 2010]
Perk J Perk L and Boden C (1996) Cardiorespiratory adaptation of COPD patients to physical
training on land and in water European Respiratory Journal 9 248-252
Rahmann AE Brauer SG Nitz JC (2009) A specific inpatient aquatic physiotherapy program
improves strength after total hip or knee replacement surgery a randomized controlled trial
Archives of Physical Medicine amp Rehabilitation 90(5)745-55
Roach KE Ally D Finnerty B Watkins D et al (1998) The relationship between duration of
physical therapy services in the acute care setting and change in functional status in patients
with lower-extremity orthopedic problems Physical Therapy 78(1) 19-24
Roos EM (2003) Effectiveness and practice variation of rehabilitation after joint replacement
Current Opinion in Rheumatology Rehabilitation medicine in rheumatic diseases 15(2)160-
162
Stalzer S Wahoff M Scanlan M (2006) Rehabilitation Following Hip Arthroscopy Clinics in
Sports Medicine 25(2)337-57
Stowell T Fuller R Fulk G (2001) An Aquatic and Land-Based Physical Therapy
Intervention to Improve Functional Mobility for an Individual After an Incomplete C6 Spinal
Cord Lesion Journal of Aquatic Physical Therapy 9(1)27-32
Taylor S (2003) The ventilated patient undergoing hydrotherapy a case study Australian
Critical Care 16(3)111-5
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
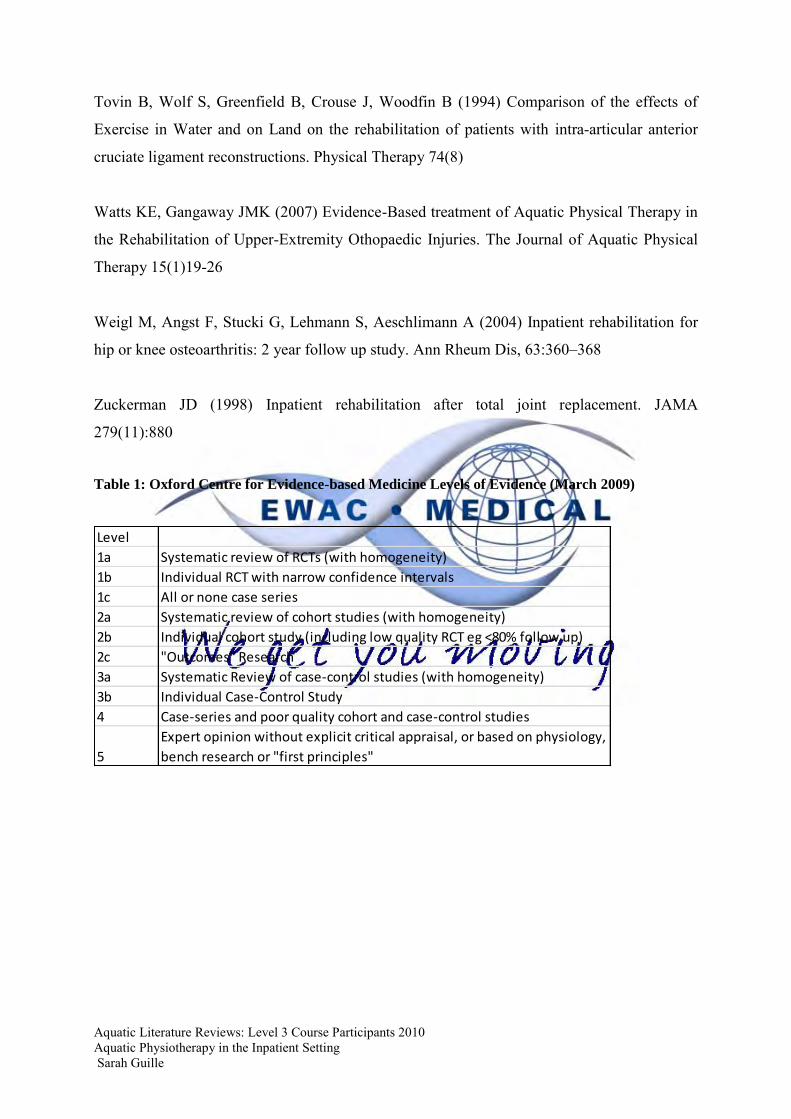
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Tovin B Wolf S Greenfield B Crouse J Woodfin B (1994) Comparison of the effects of
Exercise in Water and on Land on the rehabilitation of patients with intra-articular anterior
cruciate ligament reconstructions Physical Therapy 74(8)
Watts KE Gangaway JMK (2007) Evidence-Based treatment of Aquatic Physical Therapy in
the Rehabilitation of Upper-Extremity Othopaedic Injuries The Journal of Aquatic Physical
Therapy 15(1)19-26
Weigl M Angst F Stucki G Lehmann S Aeschlimann A (2004) Inpatient rehabilitation for
hip or knee osteoarthritis 2 year follow up study Ann Rheum Dis 63360ndash368
Zuckerman JD (1998) Inpatient rehabilitation after total joint replacement JAMA
279(11)880
Table 1 Oxford Centre for Evidence-based Medicine Levels of Evidence (March 2009)
Level
1a Systematic review of RCTs (with homogeneity)
1b Individual RCT with narrow confidence intervals
1c All or none case series
2a Systematic review of cohort studies (with homogeneity)
2b Individual cohort study (including low quality RCT eg lt80 follow up)
2c Outcomes Research
3a Systematic Review of case-control studies (with homogeneity)
3b Individual Case-Control Study
4 Case-series and poor quality cohort and case-control studies
5
Expert opinion without explicit critical appraisal or based on physiology
bench research or first principles
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
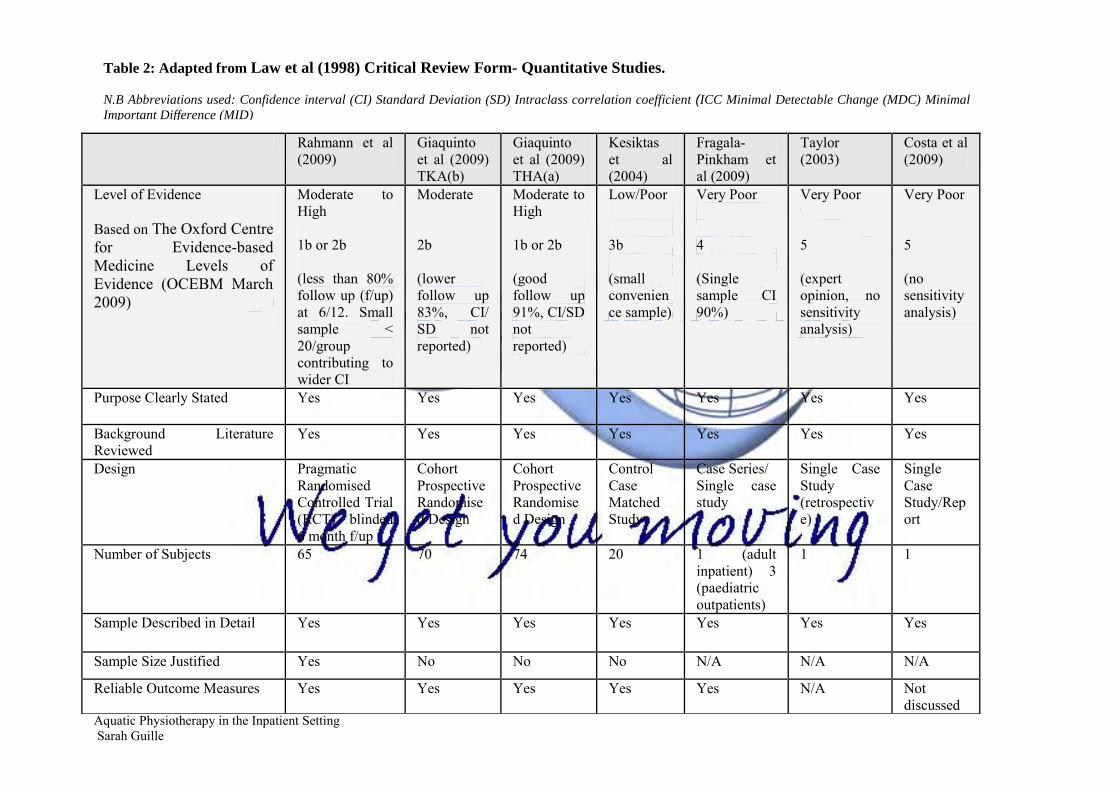
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
nothing
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Level of Evidence Based on The Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM March 2009)
Moderate to High 1b or 2b (less than 80 follow up (fup) at 612 Small sample lt 20group contributing to wider CI
Moderate 2b (lower follow up 83 CI SD not reported)
Moderate to High 1b or 2b (good follow up 91 CISD not reported)
LowPoor 3b (small convenience sample)
Very Poor 4 (Single sample CI 90)
Very Poor 5 (expert opinion no sensitivity analysis)
Very Poor 5 (no sensitivity analysis)
Purpose Clearly Stated Yes Yes Yes Yes Yes Yes Yes
Background Literature Reviewed
Yes Yes Yes Yes Yes Yes Yes
Design Pragmatic Randomised Controlled Trial (RCT) blinded 6 month fup
Cohort Prospective Randomised Design
Cohort Prospective Randomised Design
Control Case Matched Study
Case Series Single case study
Single Case Study (retrospective)
Single Case StudyReport
Number of Subjects 65 70 74 20 1 (adult inpatient) 3 (paediatric outpatients)
1 1
Sample Described in Detail Yes Yes
Yes
Yes Yes Yes Yes
Sample Size Justified Yes No No No NA NA NA
Reliable Outcome Measures Yes Yes Yes Yes Yes NA
Not discussed
Table 2 Adapted from Law et al (1998) Critical Review Form- Quantitative Studies
NB Abbreviations used Confidence interval (CI) Standard Deviation (SD) Intraclass correlation coefficient (ICC Minimal Detectable Change (MDC) Minimal
Important Difference (MID)
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
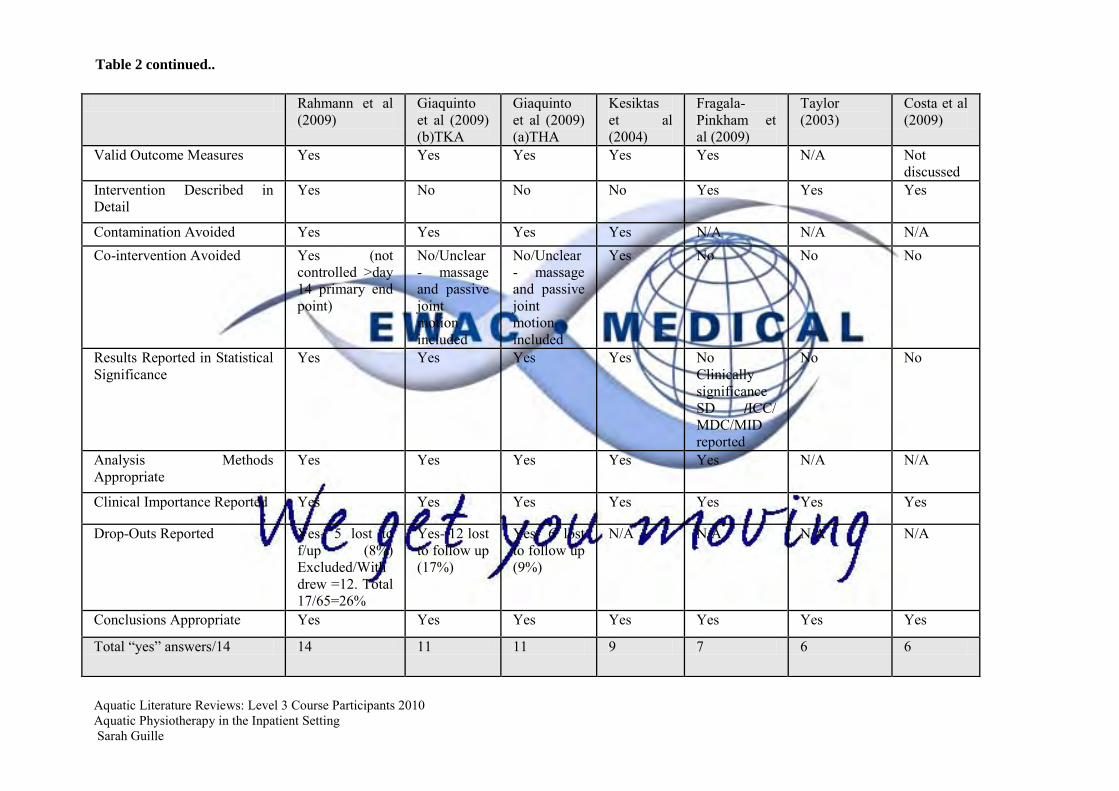
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009) (b)TKA
Giaquinto et al (2009) (a)THA
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003)
Costa et al (2009)
Valid Outcome Measures Yes Yes Yes Yes Yes NA Not discussed
Intervention Described in Detail
Yes No No No Yes Yes Yes
Contamination Avoided Yes Yes Yes Yes NA NA NA Co-intervention Avoided Yes (not
controlled gtday 14 primary end point)
NoUnclear- massage and passive joint motion included
NoUnclear- massage and passive joint motion included
Yes No No No
Results Reported in Statistical Significance
Yes Yes Yes Yes No Clinically significance SD ICC MDCMID reported
No No
Analysis Methods Appropriate
Yes Yes Yes Yes Yes NA NA
Clinical Importance Reported Yes Yes Yes Yes Yes Yes Yes
Drop-Outs Reported Yes- 5 lost to fup (8) ExcludedWithdrew =12 Total 1765=26
Yes- 12 lost to follow up (17)
Yes- 6 lost to follow up (9)
NA NA NA NA
Conclusions Appropriate Yes Yes Yes Yes Yes Yes Yes
Total ldquoyesrdquo answers14 14 11 11 9 7 6 6
Table 2 continued
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy

Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
PEDro SCALE 10
Rahmann et al (2009)
Giaquinto et al (2009) TKA(b)
Giaquinto et al (2009) THA(a)
Kesiktas et al (2004)
1 eligibility criteria were specified Yes Yes Yes Yes
2 subjects were randomly allocated to groups (in a crossover study subjects were randomly allocated an order in which treatments were received)
Yes Yes Yes No included for comparison only
3 allocation was concealed Yes Yes Yes No
4 the groups were similar at baseline regarding the most important prognostic indicators NB Abbreviation used for The
Western Ontario and McMaster
Universities Arthritis Index
(WOMAC)
Yes Yes Yes WOMAC= functionpainstiffness Significant difference in stiffness plt001
Yes
5 there was blinding of all subjects No No No No
6 there was blinding of all therapists who administered the therapy
No No No No
7 there was blinding of all assessors who measured at least one key outcome
Yes Yes Yes No
8 measures of at least one key outcome were obtained from more than 85 of the subjects initially allocated to groups
No No Yes Yes
9 all subjects for whom outcome measures were available received the treatment or control condition as allocated or where this was not the case data for at least one key outcome was analysed by ldquointention to treatrdquo
Yes No No Yes
10 the results of between-group statistical comparisons are reported for at least one key outcome
Yes Yes Yes Yes
11 the study provides both point measures and measures of variability for at least one key outcome
Yes No Confidence Interval (CI) reported No point measure
No CI reported No point measure
Yes
SCORE 710 510 610 510
Table 3 PEDro SCALE 10 (CEBP 1999) for Randomized Controlled Trials
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
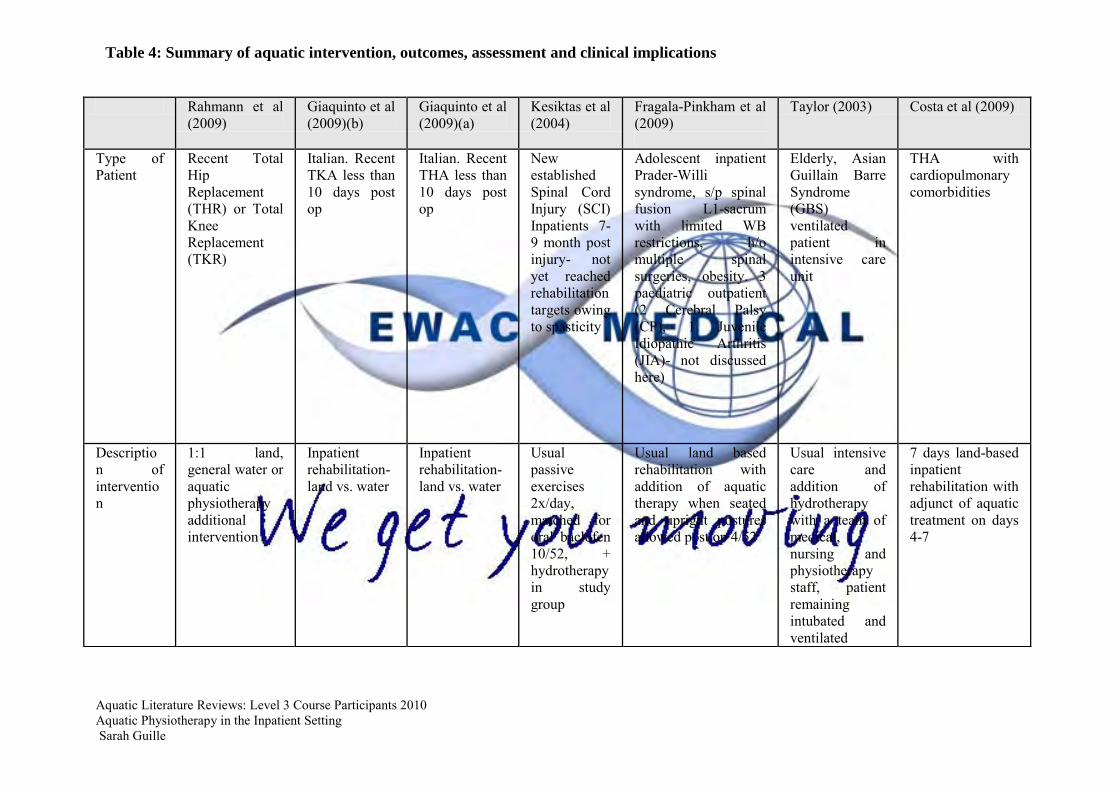
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of Patient
Recent Total Hip Replacement (THR) or Total Knee Replacement (TKR)
Italian Recent TKA less than 10 days post op
Italian Recent THA less than 10 days post op
New established Spinal Cord Injury (SCI) Inpatients 7-9 month post injury- not yet reached rehabilitation targets owing to spasticity
Adolescent inpatient Prader-Willi syndrome sp spinal fusion L1-sacrum with limited WB restrictions ho multiple spinal surgeries obesity 3 paediatric outpatient (2 Cerebral Palsy (CP) 1 Juvenile Idiopathic Arthritis (JIA)- not discussed here)
Elderly Asian Guillain Barre Syndrome (GBS) ventilated patient in intensive care unit
THA with cardiopulmonary comorbidities
Description of intervention
11 land general water or aquatic physiotherapy additional intervention
Inpatient rehabilitation- land vs water
Inpatient rehabilitation- land vs water
Usual passive exercises 2xday matched for oral baclofen 1052 + hydrotherapy in study group
Usual land based rehabilitation with addition of aquatic therapy when seated and upright postures allowed post op 452
Usual intensive care and addition of hydrotherapy with a team of medical nursing and physiotherapy staff patient remaining intubated and ventilated
7 days land-based inpatient rehabilitation with adjunct of aquatic treatment on days 4-7
Table 4 Summary of aquatic intervention outcomes assessment and clinical implications
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
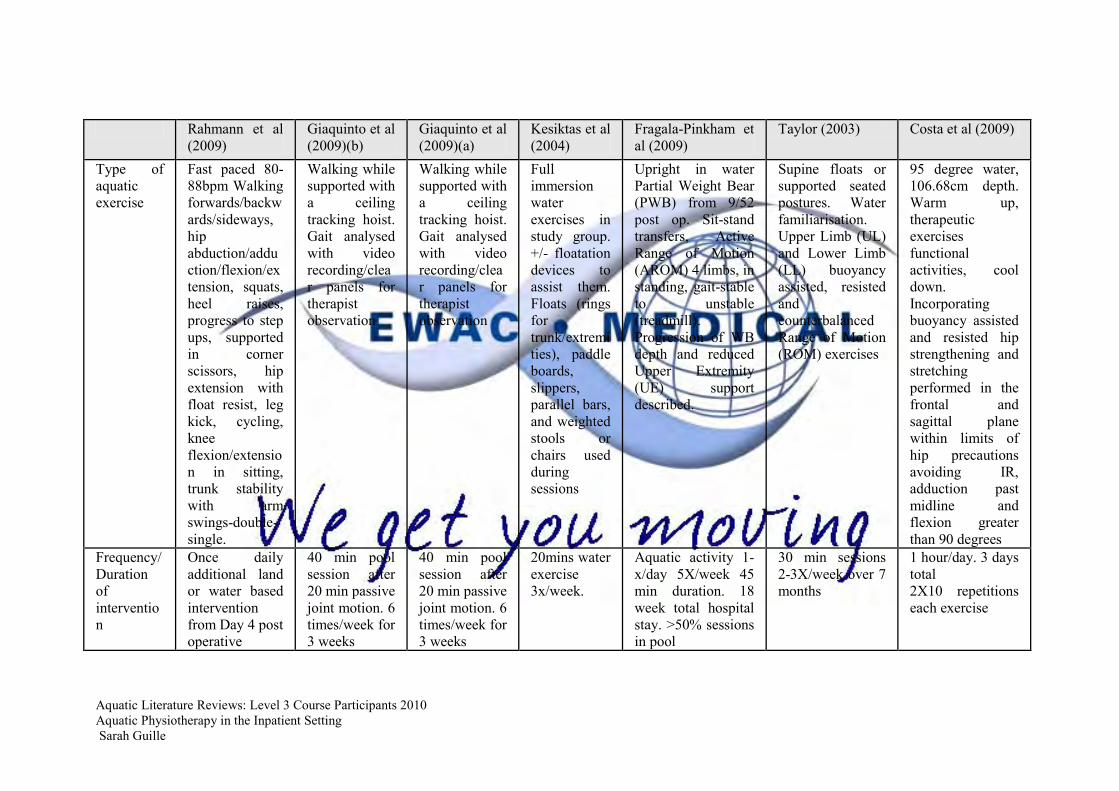
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009)(a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Type of aquatic exercise
Fast paced 80-88bpm Walking forwardsbackwardssideways hip abductionadductionflexionextension squats heel raises progress to step ups supported in corner scissors hip extension with float resist leg kick cycling knee flexionextension in sitting trunk stability with arm swings-double-single
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Walking while supported with a ceiling tracking hoist Gait analysed with video recordingclear panels for therapist observation
Full immersion water exercises in study group +- floatation devices to assist them Floats (rings for trunkextremities) paddle boards slippers parallel bars and weighted stools or chairs used during sessions
Upright in water Partial Weight Bear (PWB) from 952 post op Sit-stand transfers Active Range of Motion (AROM) 4 limbs in standing gait-stable to unstable (treadmill) Progression of WB depth and reduced Upper Extremity (UE) support described
Supine floats or supported seated postures Water familiarisation Upper Limb (UL) and Lower Limb (LL) buoyancy assisted resisted and counterbalanced Range of Motion (ROM) exercises
95 degree water 10668cm depth Warm up therapeutic exercises functional activities cool down Incorporating buoyancy assisted and resisted hip strengthening and stretching performed in the frontal and sagittal plane within limits of hip precautions avoiding IR adduction past midline and flexion greater than 90 degrees
Frequency Duration of intervention
Once daily additional land or water based intervention from Day 4 post operative
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
40 min pool session after 20 min passive joint motion 6 timesweek for 3 weeks
20mins water exercise 3xweek
Aquatic activity 1-xday 5Xweek 45 min duration 18 week total hospital stay gt50 sessions in pool
30 min sessions 2-3Xweek over 7 months
1 hourday 3 days total 2X10 repetitions each exercise
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
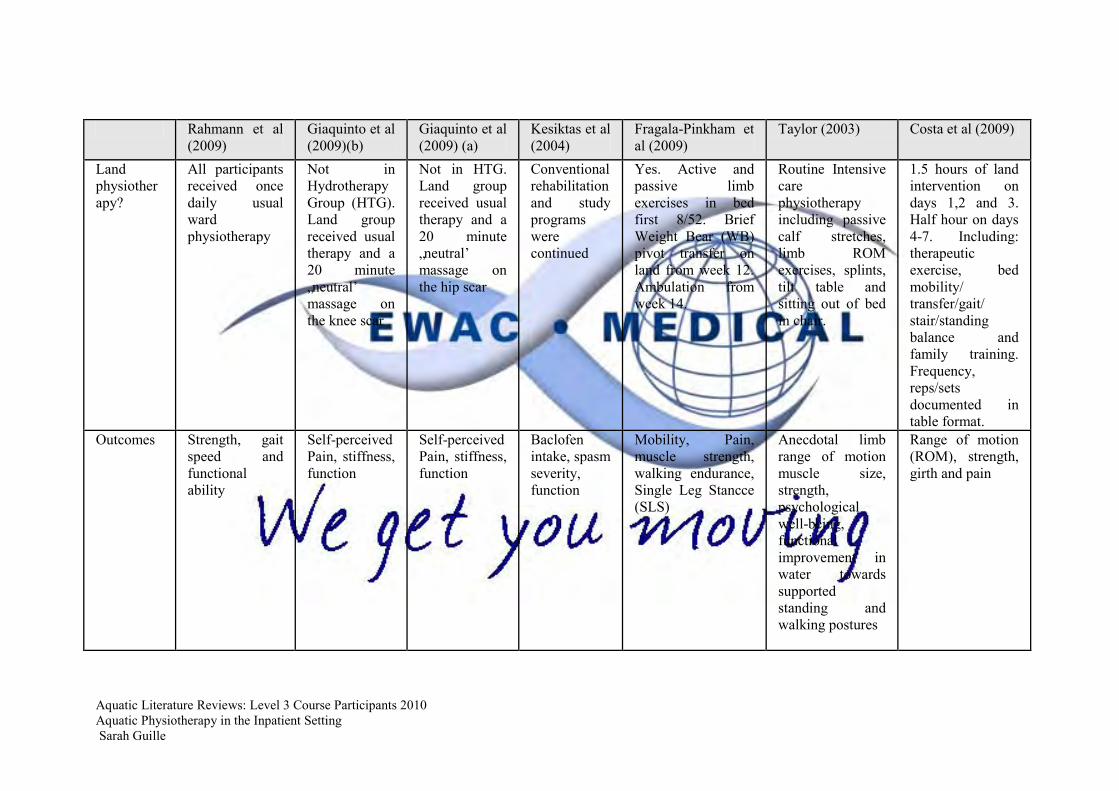
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Land physiotherapy
All participants received once daily usual ward physiotherapy
Not in Hydrotherapy Group (HTG) Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the knee scar
Not in HTG Land group received usual therapy and a 20 minute bdquoneutral‟ massage on the hip scar
Conventional rehabilitation and study programs were continued
Yes Active and passive limb exercises in bed first 852 Brief Weight Bear (WB) pivot transfer on land from week 12 Ambulation from week 14
Routine Intensive care physiotherapy including passive calf stretches limb ROM exercises splints tilt table and sitting out of bed in chair
15 hours of land intervention on days 12 and 3 Half hour on days 4-7 Including therapeutic exercise bed mobility transfergait stairstanding balance and family training Frequency repssets documented in table format
Outcomes Strength gait speed and functional ability
Self-perceived Pain stiffness function
Self-perceived Pain stiffness function
Baclofen intake spasm severity function
Mobility Pain muscle strength walking endurance Single Leg Stancce (SLS)
Anecdotal limb range of motion muscle size strength psychological well-being functional improvement in water towards supported standing and walking postures
Range of motion (ROM) strength girth and pain
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
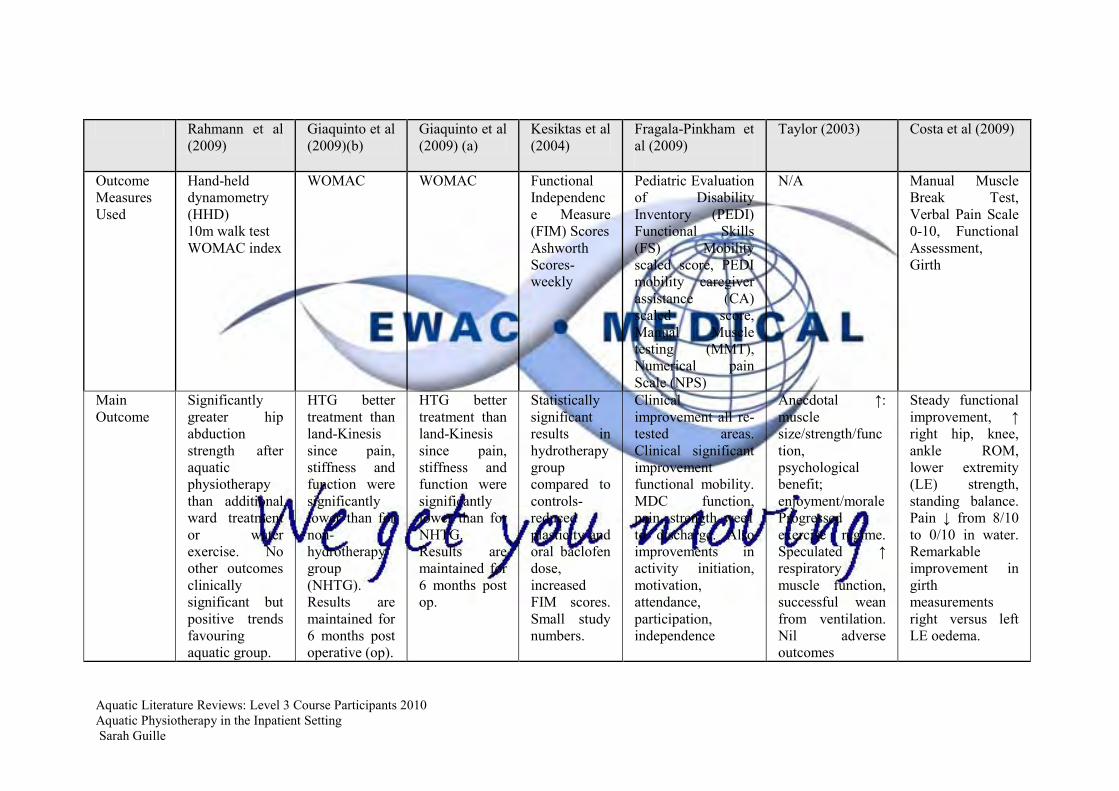
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Outcome Measures Used
Hand-held dynamometry (HHD) 10m walk test WOMAC index
WOMAC WOMAC Functional Independence Measure (FIM) Scores Ashworth Scores-weekly
Pediatric Evaluation of Disability Inventory (PEDI) Functional Skills (FS) Mobility scaled score PEDI mobility caregiver assistance (CA) scaled score Manual Muscle testing (MMT) Numerical pain Scale (NPS)
NA Manual Muscle Break Test Verbal Pain Scale 0-10 Functional Assessment Girth
Main Outcome
Significantly greater hip abduction strength after aquatic physiotherapy than additional ward treatment or water exercise No other outcomes clinically significant but positive trends favouring aquatic group
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for non-hydrotherapy group (NHTG) Results are maintained for 6 months post operative (op)
HTG better treatment than land-Kinesis since pain stiffness and function were significantly lower than for NHTG Results are maintained for 6 months post op
Statistically significant results in hydrotherapy group compared to controls- reduced plasticity and oral baclofen dose increased FIM scores Small study numbers
Clinical improvement all re-tested areas Clinical significant improvement functional mobility MDC function pain strength wee1 to discharge Also improvements in activity initiation motivation attendance participation independence
Anecdotal uarr muscle sizestrengthfunction psychological benefit enjoymentmorale Progressed exercise regime Speculated uarr respiratory muscle function successful wean from ventilation Nil adverse outcomes
Steady functional improvement uarr right hip knee ankle ROM lower extremity (LE) strength standing balance Pain darr from 810 to 010 in water Remarkable improvement in girth measurements right versus left LE oedema
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy
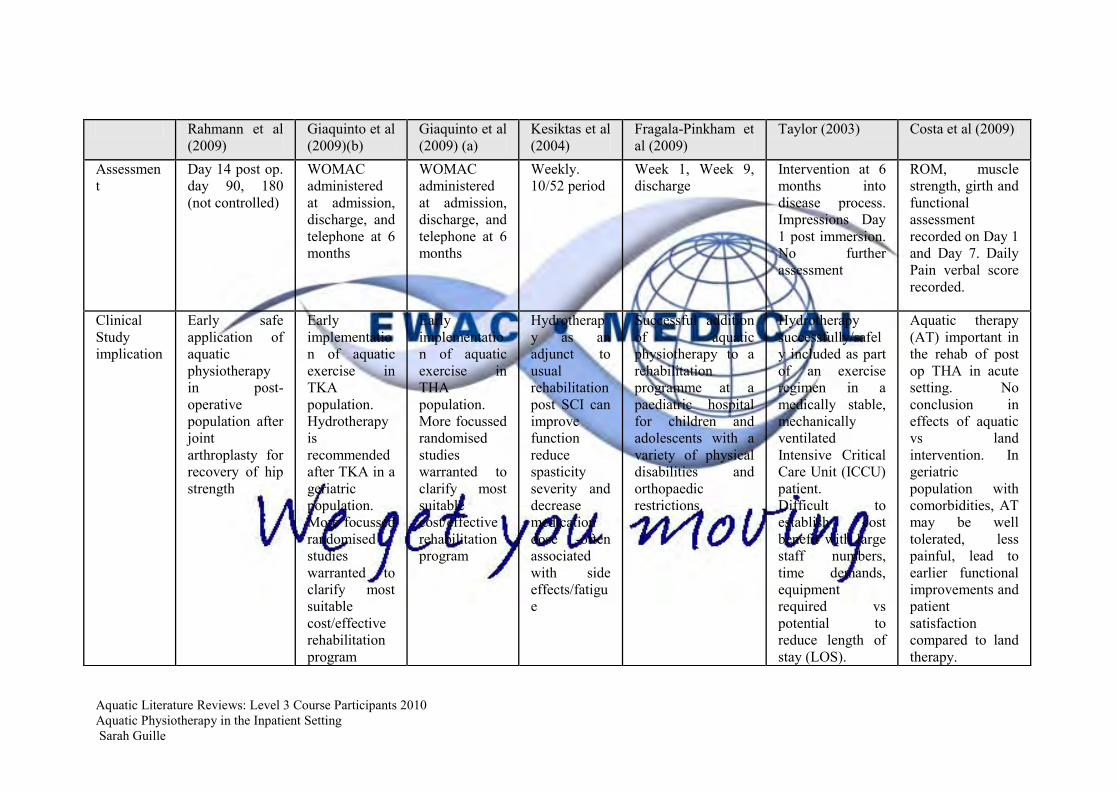
Aquatic Literature Reviews Level 3 Course Participants 2010 Aquatic Physiotherapy in the Inpatient Setting Sarah Guille
Rahmann et al (2009)
Giaquinto et al (2009)(b)
Giaquinto et al (2009) (a)
Kesiktas et al (2004)
Fragala-Pinkham et al (2009)
Taylor (2003) Costa et al (2009)
Assessment
Day 14 post op day 90 180 (not controlled)
WOMAC administered at admission discharge and telephone at 6 months
WOMAC administered at admission discharge and telephone at 6 months
Weekly 1052 period
Week 1 Week 9 discharge
Intervention at 6 months into disease process Impressions Day 1 post immersion No further assessment
ROM muscle strength girth and functional assessment recorded on Day 1 and Day 7 Daily Pain verbal score recorded
Clinical Study implication
Early safe application of aquatic physiotherapy in post-operative population after joint arthroplasty for recovery of hip strength
Early implementation of aquatic exercise in TKA population Hydrotherapy is recommended after TKA in a geriatric population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Early implementation of aquatic exercise in THA population More focussed randomised studies warranted to clarify most suitable costeffective rehabilitation program
Hydrotherapy as an adjunct to usual rehabilitation post SCI can improve function reduce spasticity severity and decrease medication dose -often associated with side effectsfatigue
Successful addition of aquatic physiotherapy to a rehabilitation programme at a paediatric hospital for children and adolescents with a variety of physical disabilities and orthopaedic restrictions
Hydrotherapy successfullysafely included as part of an exercise regimen in a medically stable mechanically ventilated Intensive Critical Care Unit (ICCU) patient Difficult to establish cost benefit with large staff numbers time demands equipment required vs potential to reduce length of stay (LOS)
Aquatic therapy (AT) important in the rehab of post op THA in acute setting No conclusion in effects of aquatic vs land intervention In geriatric population with comorbidities AT may be well tolerated less painful lead to earlier functional improvements and patient satisfaction compared to land therapy








![Chest physiotherapy compared to no chest physiotherapy for ... · [Intervention Review] Chest physiotherapy compared to no chest physiotherapy for cystic fibrosis Cees P van der](https://img.pdfslide.us/doc/110x75/5cc2dd0188c99389538bb642/chest-physiotherapy-compared-to-no-chest-physiotherapy-for-intervention.jpg)