Embed Size (px)
Citation preview
April Procedure Code Review Updates Now Available Information posted February 19, 2010
Effective for dates of service on or after April 1, 2010, to align with the Centers for Medicare & Medicaid Services (CMS) requirements for easy access to all Texas Medicaid fees, provider type, place-of-service (POS), and type-of-service (TOS) changes will be applied to a number of services.
Abatacept (Orencia) The following benefit changes apply to procedure code J0129 as indicated:
Procedure Code Changes J0129 Will no longer be reimbursed to podiatrist, certified nurse midwife (CNM),
and hospital-based rural health clinic (RHC) providers in the office setting. Will no longer be reimbursed in the home or extended care facility (ECF) setting. Will no longer be reimbursed to hospital-based RHC providers in the outpatient hospital setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement.
Aerosol Treatments – Outpatient Setting The following aerosol treatment procedure codes will be made benefits of Texas Medicaid and may be reimbursed as indicated:
Procedure Code Changes J7605, J7608, J7622, J7626, J7631, J7633, J7639, J7644, J7682
May be reimbursed to nurse practitioner (NP), clinical nurse specialist (CNS), physician assistant (PA), physician, portable X-ray supplier, and radiological and physiological laboratory providers in the office setting. May be reimbursed to hospitals in the outpatient hospital setting.
These new aerosol treatment procedure codes may be reimbursed when submitted with any of the following diagnosis codes:
Diagnosis Codes 0115 27702 46611 46619 4801 48242 486 4880 4881 4910 4911 49120 49121 49122 4918 4919 4920 4928 49300 49301 49302 49310 49311 49312 49320 49321 49322 49381 49382 49390 49391 49392 4940 4941 4950
Diagnosis Codes 4951 4952 4953 4954 4955 4956 4957 4958 4959 496 500 501 502 503 504 505 5060 5061 5062 5063 5064 5069 5070 5071 5078 5080 5081 5088 5089 51911 51919 7864 74861
Additional diagnosis codes may be considered with prior authorization. Documentation must support medical necessity.
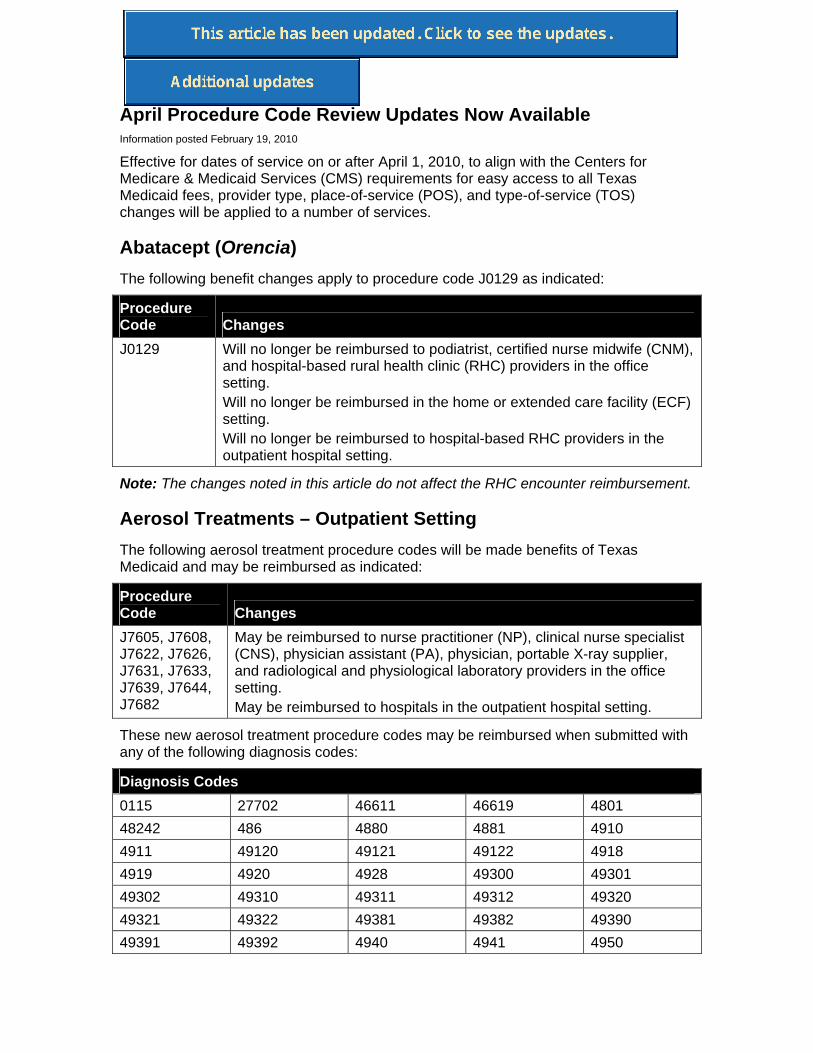
The following changes will be applied to the medical procedure codes indicated:
Procedure Code Changes 94640 Medical component: Will no longer be reimbursed to independent
laboratory and CNM providers in the office setting. May be reimbursed to portable X-ray suppliers and radiological and physiological laboratories in the office setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the outpatient hospital setting.
94642 Medical component: Will no longer be reimbursed to CNM providers in the office setting Will no longer be reimbursed to NP, CNS, PA, physician, CNM, radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting.
94644 Medical component: Will no longer be reimbursed to independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), and renal dialysis facility providers in the office setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, and radiological and physiological laboratory providers in the outpatient hospital setting.
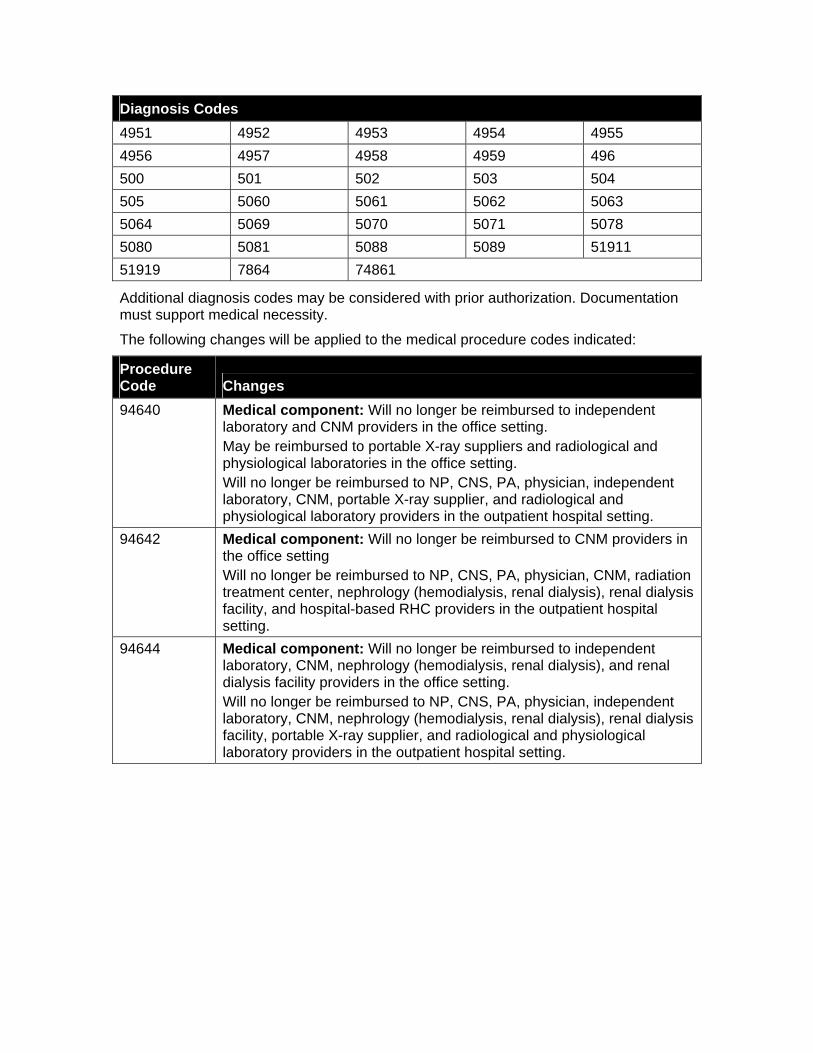
Procedure Code Changes 94760, 94761
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, durable medical equipment (DME) medical supplier, Coordinated Care Program (CCP), hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the home setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, DME medical supplier, CCP provider, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Note: Pulse oximetry (procedure codes 94760 or 94761) is considered part of an evaluation and management visit and will not be reimbursed separately.
J2545 Medical component: Will no longer be reimbursed to CNM providers in the office setting. Will no longer be reimbursed in the home, skilled nursing facility (SNF), intermediary care facility (ICF), or ECF setting. Will no longer be reimbursed to NP, CNS, PA, physician, CNM, radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement or the hospital diagnosis-related group (DRG) reimbursement.
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 25.3.3.1, “Aerosol Treatment,” on page 25-28, and section 36.4.1, “Aerosol Treatment,” on page 36-11, for more information.
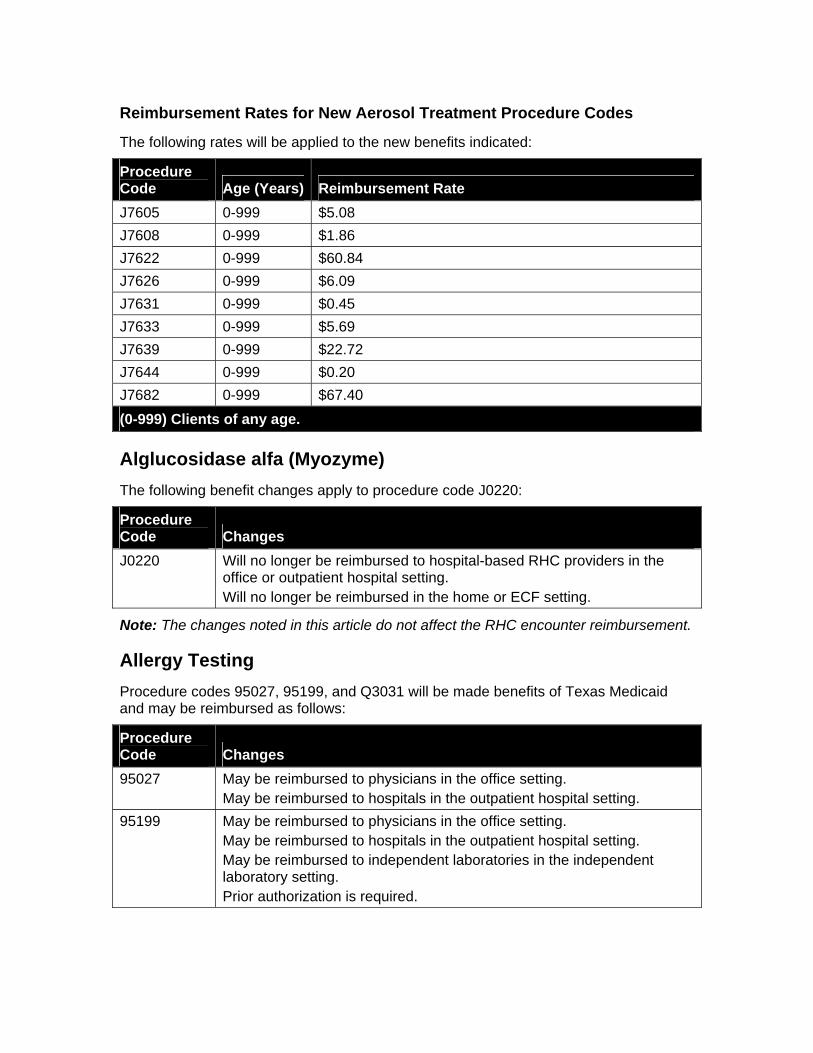
Reimbursement Rates for New Aerosol Treatment Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate J7605 0-999 $5.08 J7608 0-999 $1.86 J7622 0-999 $60.84 J7626 0-999 $6.09 J7631 0-999 $0.45 J7633 0-999 $5.69 J7639 0-999 $22.72 J7644 0-999 $0.20 J7682 0-999 $67.40 (0-999) Clients of any age.
Alglucosidase alfa (Myozyme) The following benefit changes apply to procedure code J0220:
Procedure Code Changes J0220 Will no longer be reimbursed to hospital-based RHC providers in the
office or outpatient hospital setting. Will no longer be reimbursed in the home or ECF setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement.
Allergy Testing Procedure codes 95027, 95199, and Q3031 will be made benefits of Texas Medicaid and may be reimbursed as follows:
Procedure Code Changes 95027 May be reimbursed to physicians in the office setting.
May be reimbursed to hospitals in the outpatient hospital setting. 95199 May be reimbursed to physicians in the office setting.
May be reimbursed to hospitals in the outpatient hospital setting. May be reimbursed to independent laboratories in the independent laboratory setting. Prior authorization is required.
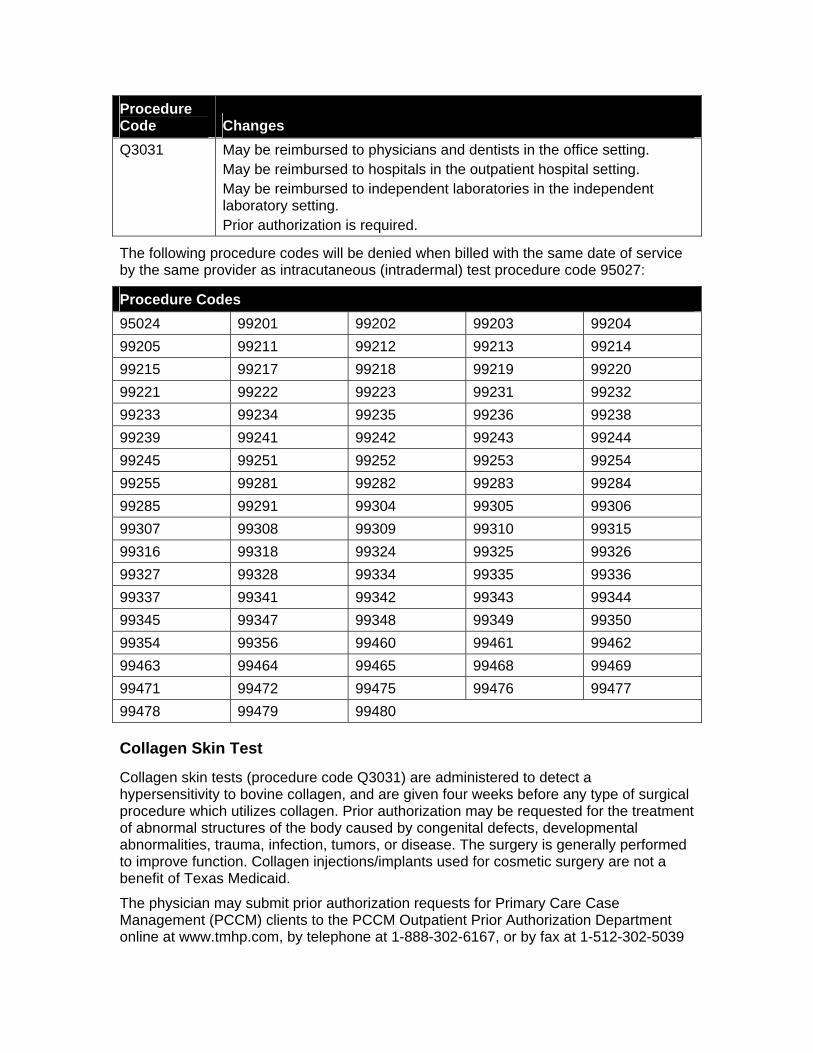
Procedure Code Changes Q3031 May be reimbursed to physicians and dentists in the office setting.
May be reimbursed to hospitals in the outpatient hospital setting. May be reimbursed to independent laboratories in the independent laboratory setting. Prior authorization is required.
The following procedure codes will be denied when billed with the same date of service by the same provider as intracutaneous (intradermal) test procedure code 95027:
Procedure Codes 95024 99201 99202 99203 99204 99205 99211 99212 99213 99214 99215 99217 99218 99219 99220 99221 99222 99223 99231 99232 99233 99234 99235 99236 99238 99239 99241 99242 99243 99244 99245 99251 99252 99253 99254 99255 99281 99282 99283 99284 99285 99291 99304 99305 99306 99307 99308 99309 99310 99315 99316 99318 99324 99325 99326 99327 99328 99334 99335 99336 99337 99341 99342 99343 99344 99345 99347 99348 99349 99350 99354 99356 99460 99461 99462 99463 99464 99465 99468 99469 99471 99472 99475 99476 99477 99478 99479 99480
Collagen Skin Test
Collagen skin tests (procedure code Q3031) are administered to detect a hypersensitivity to bovine collagen, and are given four weeks before any type of surgical procedure which utilizes collagen. Prior authorization may be requested for the treatment of abnormal structures of the body caused by congenital defects, developmental abnormalities, trauma, infection, tumors, or disease. The surgery is generally performed to improve function. Collagen injections/implants used for cosmetic surgery are not a benefit of Texas Medicaid.
The physician may submit prior authorization requests for Primary Care Case Management (PCCM) clients to the PCCM Outpatient Prior Authorization Department online at www.tmhp.com, by telephone at 1-888-302-6167, or by fax at 1-512-302-5039
using the Primary Care Case Management (PCCM) Inpatient/Outpatient Authorization Form.
The physician may submit prior authorization requests for fee-for-service clients to the Special Medical Prior Authorization (SMPA) department online at www.tmhp.com, by fax at 1-512-514-4213, or by mail to:
Texas Medicaid & Healthcare Partnership Special Medical Prior Authorization Department
12357-B Riata Trace Parkway, Suite 150 Austin TX 78727
Documentation that supports medical necessity for the requested device, service, or supply must be submitted to the SMPA Department with the prior authorization request. Prior authorization is a condition for reimbursement; it is not a guarantee of payment.
Unlisted Procedure Code
Procedure code 95199 is for an unlisted allergy or clinical immunologic services or procedures and may be used if there is no specific procedure code that describes the service performed. Every effort should be made to bill with the appropriate procedure code that describes the procedure being performed. If a code does not exist to describe the service performed, prior authorization may be requested using unlisted procedure code 95199 and with appropriate documentation to assist in determining coverage.
The documentation submitted with the prior authorization request must include all of the following:
• The client's diagnosis
• Medical records indicating prior treatment for this diagnosis and the medical necessity of the requested procedure
• A clear, concise description of the procedure to be performed
• Reason for recommending this particular procedure
• A procedure code that is comparable to the procedure being requested
• Documentation that this procedure is not investigational or experimental
• Place of service the procedure is to be performed
• The physician's intended fee for this procedure
The physician may submit prior authorization requests for PCCM clients to the PCCM Outpatient Prior Authorization Department online at www.tmhp.com, by telephone at 1-888-302-6167, or by fax at 1-512-302-5039 using the Primary Care Case Management (PCCM) Inpatient/Outpatient Authorization Form. The physician may submit prior authorization requests for fee-for-service clients to the Special Medical Prior Authorization (SMPA) department online at www.tmhp.com, by fax at 1-512-514-4213, or by mail at:
Texas Medicaid & Healthcare Partnership Special Medical Prior Authorization Department
12357-B Riata Trace Parkway, Suite 150 Austin TX 78727
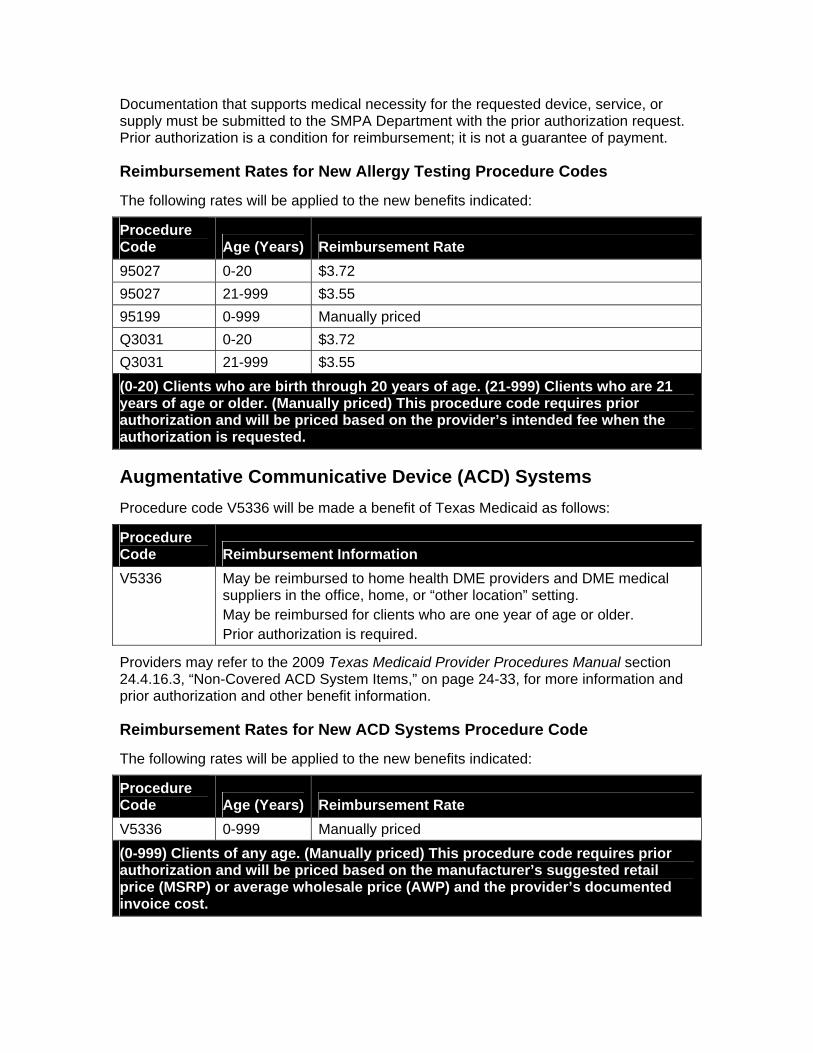
Documentation that supports medical necessity for the requested device, service, or supply must be submitted to the SMPA Department with the prior authorization request. Prior authorization is a condition for reimbursement; it is not a guarantee of payment.
Reimbursement Rates for New Allergy Testing Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 95027 0-20 $3.72 95027 21-999 $3.55 95199 0-999 Manually priced Q3031 0-20 $3.72 Q3031 21-999 $3.55 (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older. (Manually priced) This procedure code requires prior authorization and will be priced based on the provider’s intended fee when the authorization is requested.
Augmentative Communicative Device (ACD) Systems Procedure code V5336 will be made a benefit of Texas Medicaid as follows:
Procedure Code Reimbursement Information V5336 May be reimbursed to home health DME providers and DME medical
suppliers in the office, home, or “other location” setting. May be reimbursed for clients who are one year of age or older. Prior authorization is required.
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 24.4.16.3, “Non-Covered ACD System Items,” on page 24-33, for more information and prior authorization and other benefit information.
Reimbursement Rates for New ACD Systems Procedure Code
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate V5336 0-999 Manually priced (0-999) Clients of any age. (Manually priced) This procedure code requires prior authorization and will be priced based on the manufacturer’s suggested retail price (MSRP) or average wholesale price (AWP) and the provider’s documented invoice cost.
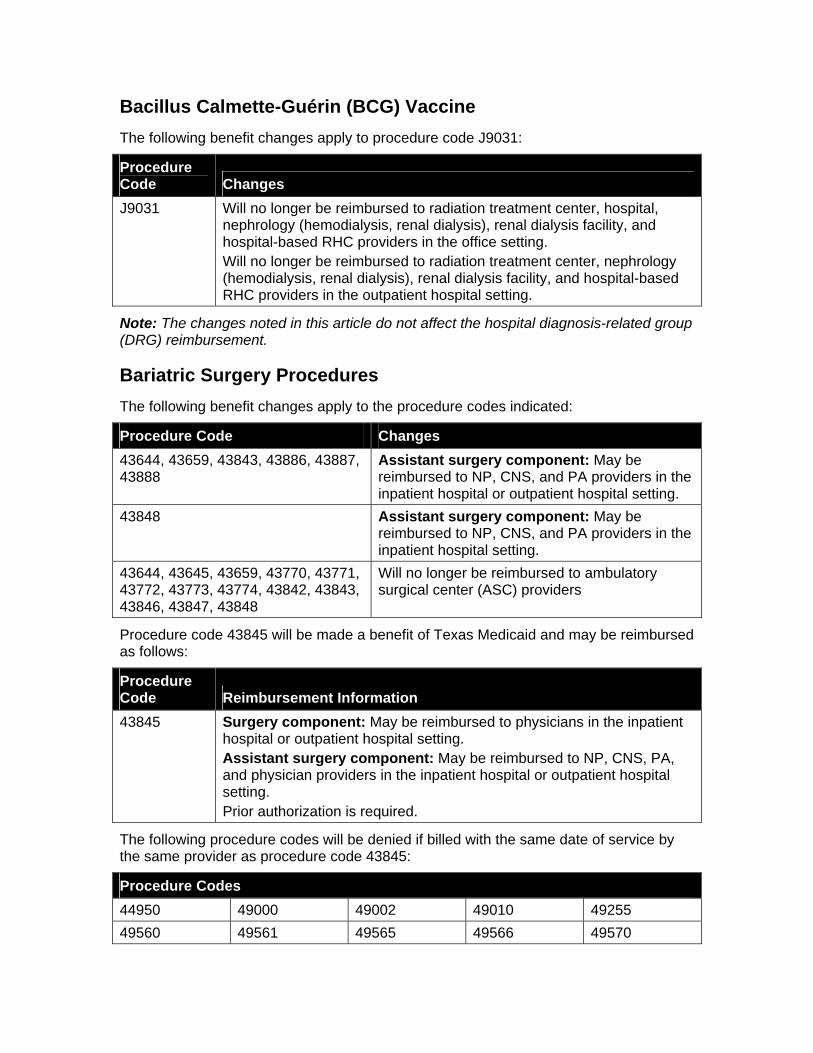
Bacillus Calmette-Guérin (BCG) Vaccine The following benefit changes apply to procedure code J9031:
Procedure Code Changes J9031 Will no longer be reimbursed to radiation treatment center, hospital,
nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting.
Note: The changes noted in this article do not affect the hospital diagnosis-related group (DRG) reimbursement.
Bariatric Surgery Procedures The following benefit changes apply to the procedure codes indicated:
Procedure Code Changes 43644, 43659, 43843, 43886, 43887, 43888
Assistant surgery component: May be reimbursed to NP, CNS, and PA providers in the inpatient hospital or outpatient hospital setting.
43848 Assistant surgery component: May be reimbursed to NP, CNS, and PA providers in the inpatient hospital setting.
43644, 43645, 43659, 43770, 43771, 43772, 43773, 43774, 43842, 43843, 43846, 43847, 43848
Will no longer be reimbursed to ambulatory surgical center (ASC) providers
Procedure code 43845 will be made a benefit of Texas Medicaid and may be reimbursed as follows:
Procedure Code Reimbursement Information 43845 Surgery component: May be reimbursed to physicians in the inpatient
hospital or outpatient hospital setting. Assistant surgery component: May be reimbursed to NP, CNS, PA, and physician providers in the inpatient hospital or outpatient hospital setting. Prior authorization is required.
The following procedure codes will be denied if billed with the same date of service by the same provider as procedure code 43845:
Procedure Codes 44950 49000 49002 49010 49255 49560 49561 49565 49566 49570
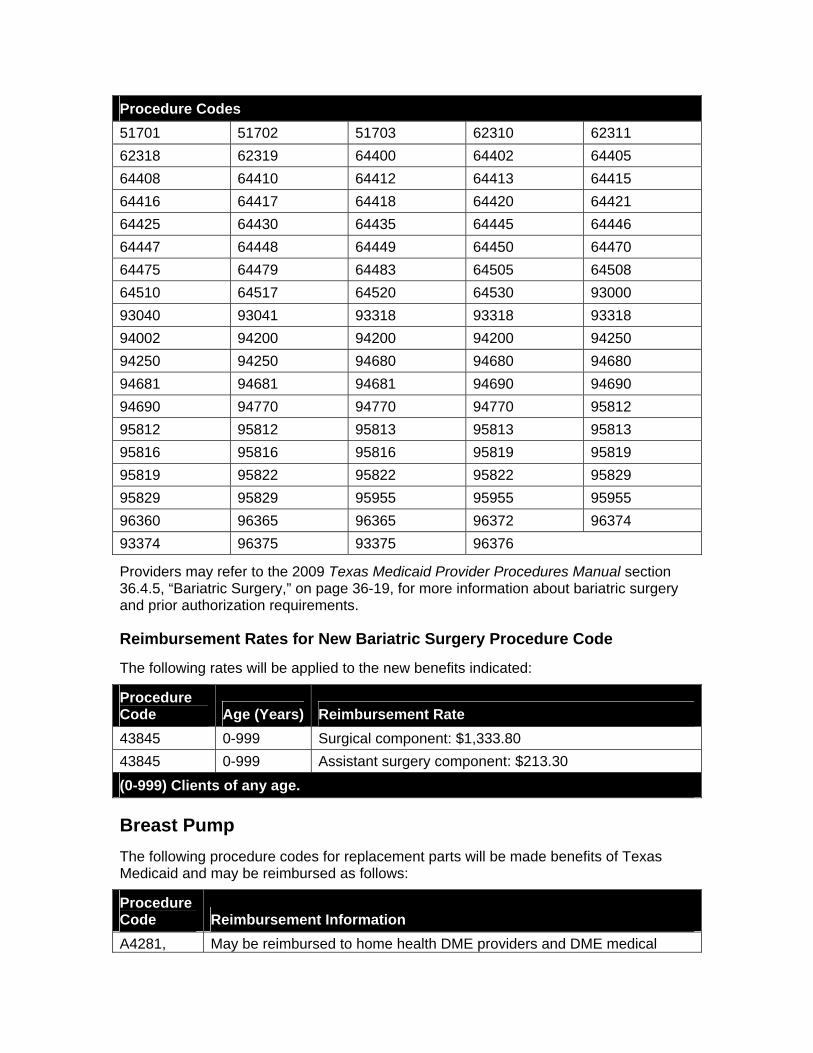
Procedure Codes 51701 51702 51703 62310 62311 62318 62319 64400 64402 64405 64408 64410 64412 64413 64415 64416 64417 64418 64420 64421 64425 64430 64435 64445 64446 64447 64448 64449 64450 64470 64475 64479 64483 64505 64508 64510 64517 64520 64530 93000 93040 93041 93318 93318 93318 94002 94200 94200 94200 94250 94250 94250 94680 94680 94680 94681 94681 94681 94690 94690 94690 94770 94770 94770 95812 95812 95812 95813 95813 95813 95816 95816 95816 95819 95819 95819 95822 95822 95822 95829 95829 95829 95955 95955 95955 96360 96365 96365 96372 96374 93374 96375 93375 96376
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 36.4.5, “Bariatric Surgery,” on page 36-19, for more information about bariatric surgery and prior authorization requirements.
Reimbursement Rates for New Bariatric Surgery Procedure Code
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 43845 0-999 Surgical component: $1,333.80 43845 0-999 Assistant surgery component: $213.30 (0-999) Clients of any age.
Breast Pump The following procedure codes for replacement parts will be made benefits of Texas Medicaid and may be reimbursed as follows:
Procedure Code Reimbursement Information A4281, May be reimbursed to home health DME providers and DME medical
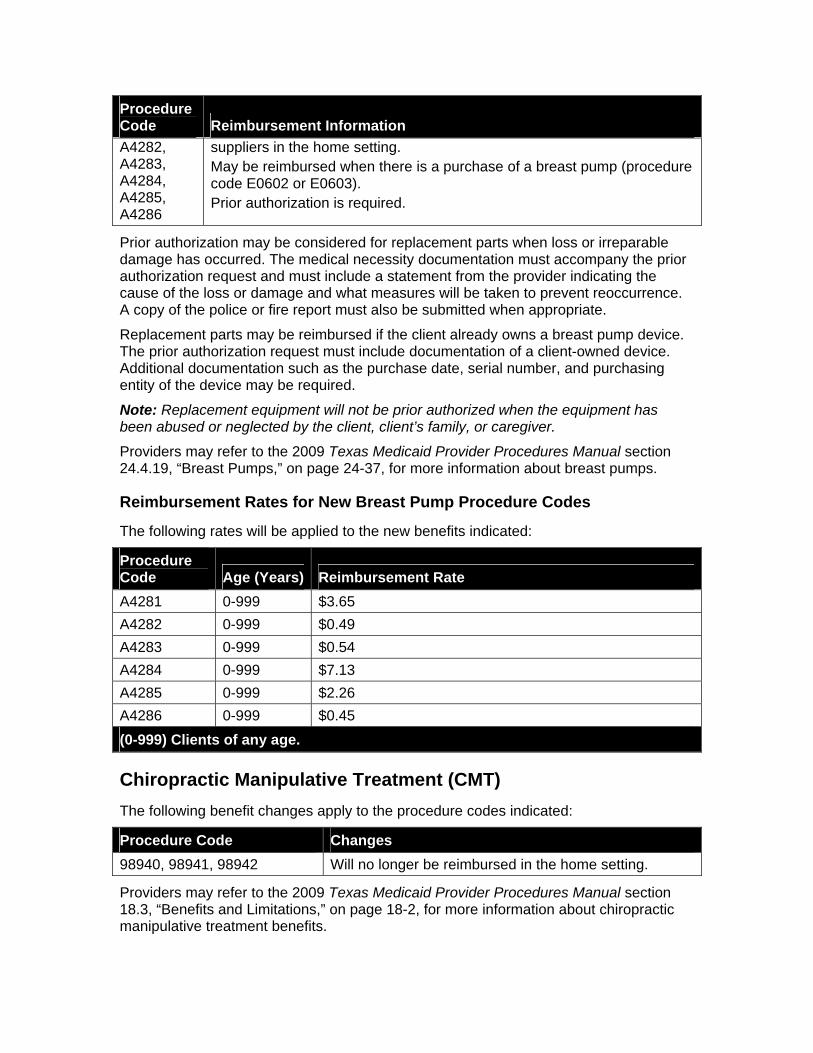
Procedure Code Reimbursement Information A4282, A4283, A4284, A4285, A4286
suppliers in the home setting. May be reimbursed when there is a purchase of a breast pump (procedure code E0602 or E0603). Prior authorization is required.
Prior authorization may be considered for replacement parts when loss or irreparable damage has occurred. The medical necessity documentation must accompany the prior authorization request and must include a statement from the provider indicating the cause of the loss or damage and what measures will be taken to prevent reoccurrence. A copy of the police or fire report must also be submitted when appropriate.
Replacement parts may be reimbursed if the client already owns a breast pump device. The prior authorization request must include documentation of a client-owned device. Additional documentation such as the purchase date, serial number, and purchasing entity of the device may be required.
Note: Replacement equipment will not be prior authorized when the equipment has been abused or neglected by the client, client’s family, or caregiver.
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 24.4.19, “Breast Pumps,” on page 24-37, for more information about breast pumps.
Reimbursement Rates for New Breast Pump Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate A4281 0-999 $3.65 A4282 0-999 $0.49 A4283 0-999 $0.54 A4284 0-999 $7.13 A4285 0-999 $2.26 A4286 0-999 $0.45 (0-999) Clients of any age.
Chiropractic Manipulative Treatment (CMT) The following benefit changes apply to the procedure codes indicated:
Procedure Code Changes 98940, 98941, 98942 Will no longer be reimbursed in the home setting.
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 18.3, “Benefits and Limitations,” on page 18-2, for more information about chiropractic manipulative treatment benefits.
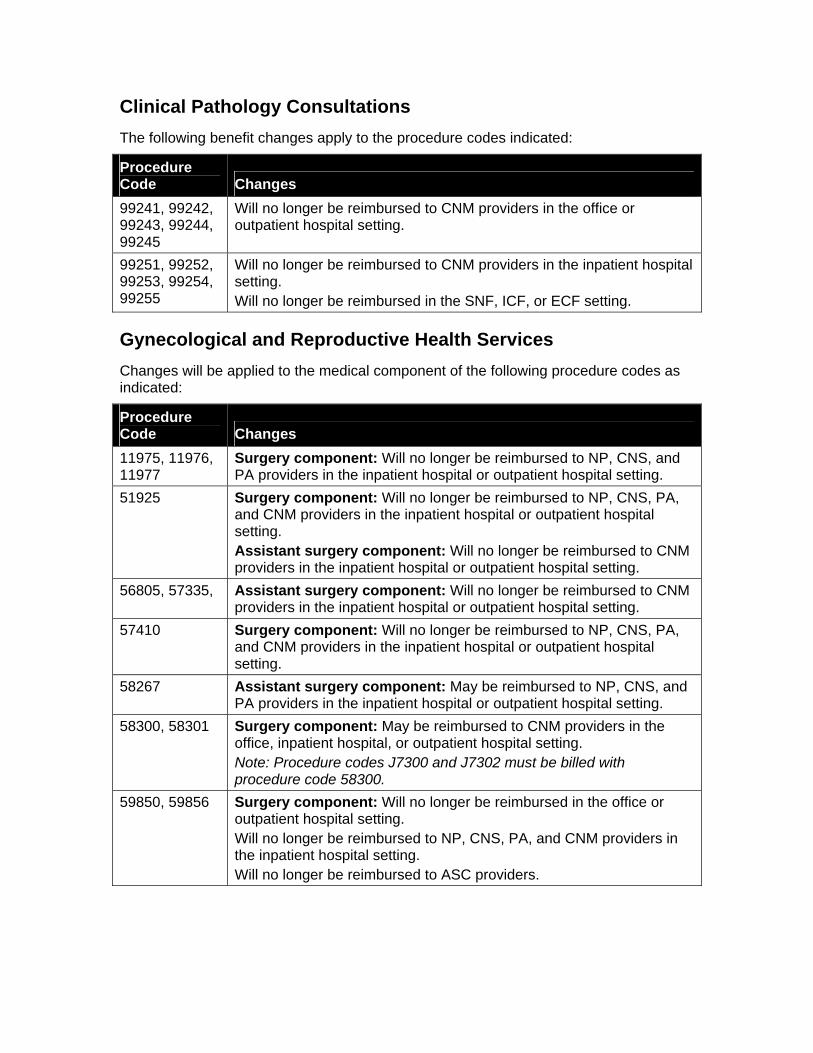
Clinical Pathology Consultations The following benefit changes apply to the procedure codes indicated:
Procedure Code Changes 99241, 99242, 99243, 99244, 99245
Will no longer be reimbursed to CNM providers in the office or outpatient hospital setting.
99251, 99252, 99253, 99254, 99255
Will no longer be reimbursed to CNM providers in the inpatient hospital setting. Will no longer be reimbursed in the SNF, ICF, or ECF setting.
Gynecological and Reproductive Health Services Changes will be applied to the medical component of the following procedure codes as indicated:
Procedure Code Changes 11975, 11976, 11977
Surgery component: Will no longer be reimbursed to NP, CNS, and PA providers in the inpatient hospital or outpatient hospital setting.
51925 Surgery component: Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
56805, 57335, Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
57410 Surgery component: Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting.
58267 Assistant surgery component: May be reimbursed to NP, CNS, and PA providers in the inpatient hospital or outpatient hospital setting.
58300, 58301 Surgery component: May be reimbursed to CNM providers in the office, inpatient hospital, or outpatient hospital setting. Note: Procedure codes J7300 and J7302 must be billed with procedure code 58300.
59850, 59856 Surgery component: Will no longer be reimbursed in the office or outpatient hospital setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital setting. Will no longer be reimbursed to ASC providers.
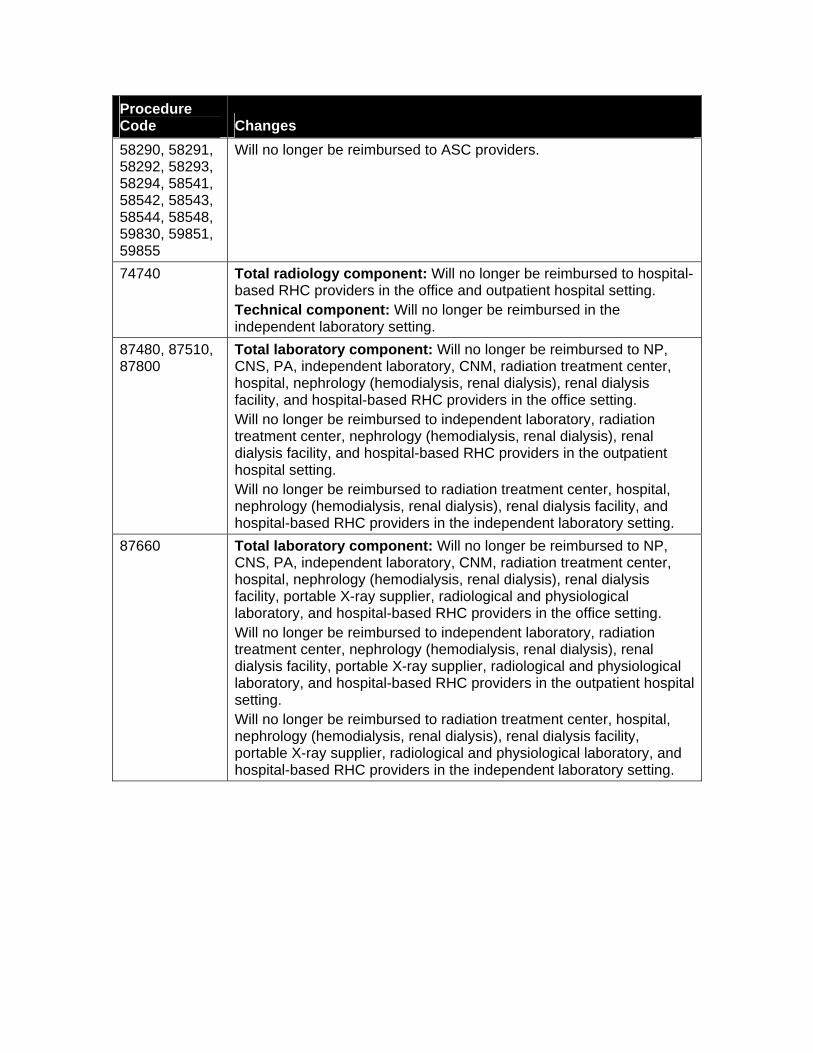
Procedure Code Changes 58290, 58291, 58292, 58293, 58294, 58541, 58542, 58543, 58544, 58548, 59830, 59851, 59855
Will no longer be reimbursed to ASC providers.
74740 Total radiology component: Will no longer be reimbursed to hospital-based RHC providers in the office and outpatient hospital setting. Technical component: Will no longer be reimbursed in the independent laboratory setting.
87480, 87510, 87800
Total laboratory component: Will no longer be reimbursed to NP, CNS, PA, independent laboratory, CNM, radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to independent laboratory, radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting. Will no longer be reimbursed to radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the independent laboratory setting.
87660 Total laboratory component: Will no longer be reimbursed to NP, CNS, PA, independent laboratory, CNM, radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to independent laboratory, radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Will no longer be reimbursed to radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the independent laboratory setting.
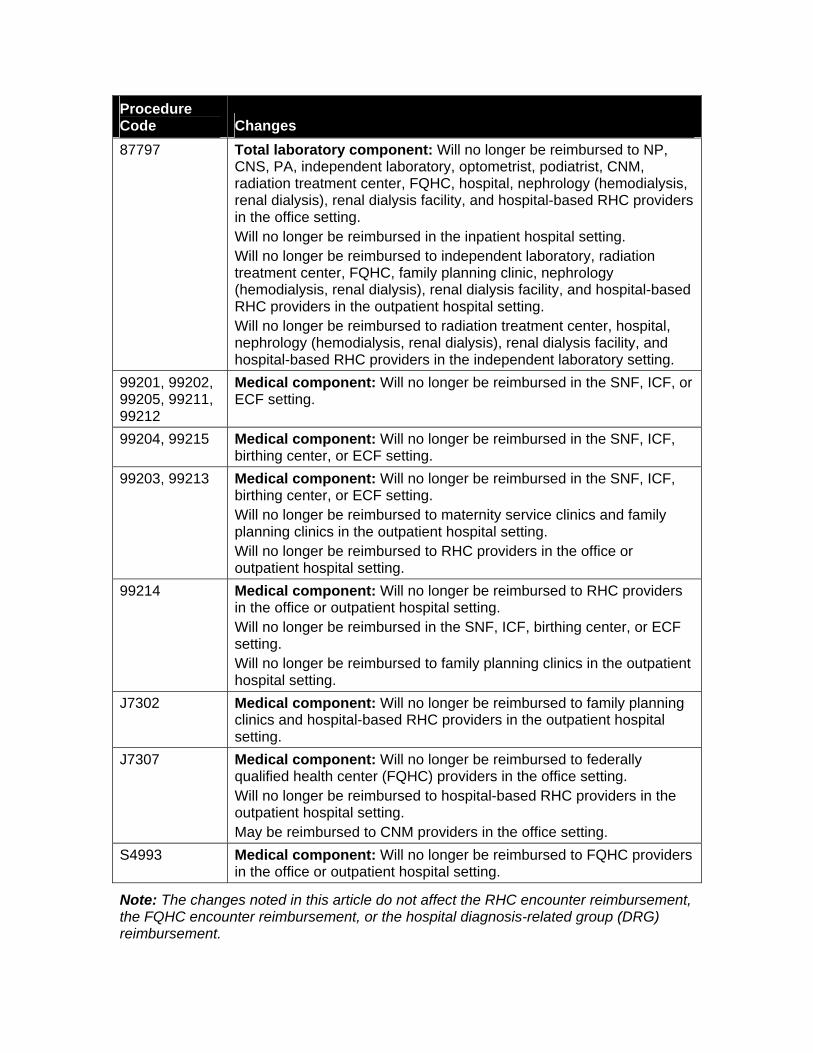
Procedure Code Changes 87797 Total laboratory component: Will no longer be reimbursed to NP,
CNS, PA, independent laboratory, optometrist, podiatrist, CNM, radiation treatment center, FQHC, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital setting. Will no longer be reimbursed to independent laboratory, radiation treatment center, FQHC, family planning clinic, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting. Will no longer be reimbursed to radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the independent laboratory setting.
99201, 99202, 99205, 99211, 99212
Medical component: Will no longer be reimbursed in the SNF, ICF, or ECF setting.
99204, 99215 Medical component: Will no longer be reimbursed in the SNF, ICF, birthing center, or ECF setting.
99203, 99213 Medical component: Will no longer be reimbursed in the SNF, ICF, birthing center, or ECF setting. Will no longer be reimbursed to maternity service clinics and family planning clinics in the outpatient hospital setting. Will no longer be reimbursed to RHC providers in the office or outpatient hospital setting.
99214 Medical component: Will no longer be reimbursed to RHC providers in the office or outpatient hospital setting. Will no longer be reimbursed in the SNF, ICF, birthing center, or ECF setting. Will no longer be reimbursed to family planning clinics in the outpatient hospital setting.
J7302 Medical component: Will no longer be reimbursed to family planning clinics and hospital-based RHC providers in the outpatient hospital setting.
J7307 Medical component: Will no longer be reimbursed to federally qualified health center (FQHC) providers in the office setting. Will no longer be reimbursed to hospital-based RHC providers in the outpatient hospital setting. May be reimbursed to CNM providers in the office setting.
S4993 Medical component: Will no longer be reimbursed to FQHC providers in the office or outpatient hospital setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement, the FQHC encounter reimbursement, or the hospital diagnosis-related group (DRG) reimbursement.
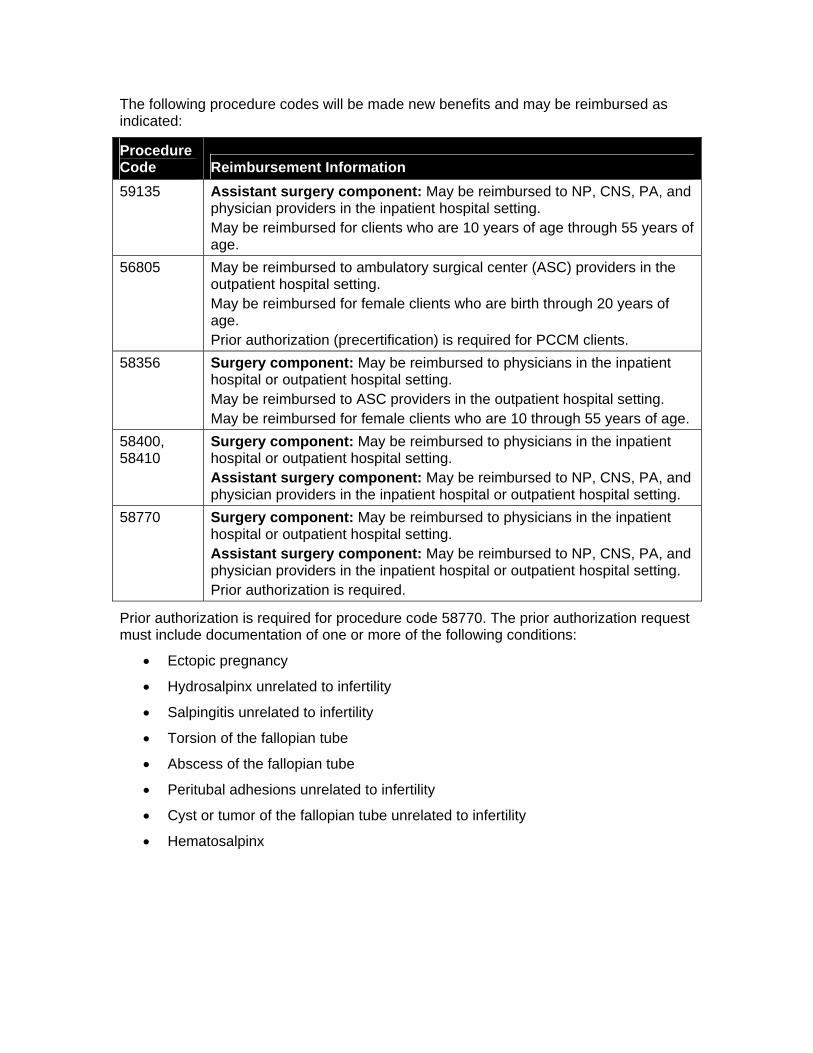
The following procedure codes will be made new benefits and may be reimbursed as indicated:
Procedure Code Reimbursement Information 59135 Assistant surgery component: May be reimbursed to NP, CNS, PA, and
physician providers in the inpatient hospital setting. May be reimbursed for clients who are 10 years of age through 55 years of age.
56805 May be reimbursed to ambulatory surgical center (ASC) providers in the outpatient hospital setting. May be reimbursed for female clients who are birth through 20 years of age. Prior authorization (precertification) is required for PCCM clients.
58356 Surgery component: May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting. May be reimbursed to ASC providers in the outpatient hospital setting. May be reimbursed for female clients who are 10 through 55 years of age.
58400, 58410
Surgery component: May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting. Assistant surgery component: May be reimbursed to NP, CNS, PA, and physician providers in the inpatient hospital or outpatient hospital setting.
58770 Surgery component: May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting. Assistant surgery component: May be reimbursed to NP, CNS, PA, and physician providers in the inpatient hospital or outpatient hospital setting. Prior authorization is required.
Prior authorization is required for procedure code 58770. The prior authorization request must include documentation of one or more of the following conditions:
• Ectopic pregnancy
• Hydrosalpinx unrelated to infertility
• Salpingitis unrelated to infertility
• Torsion of the fallopian tube
• Abscess of the fallopian tube
• Peritubal adhesions unrelated to infertility
• Cyst or tumor of the fallopian tube unrelated to infertility
• Hematosalpinx
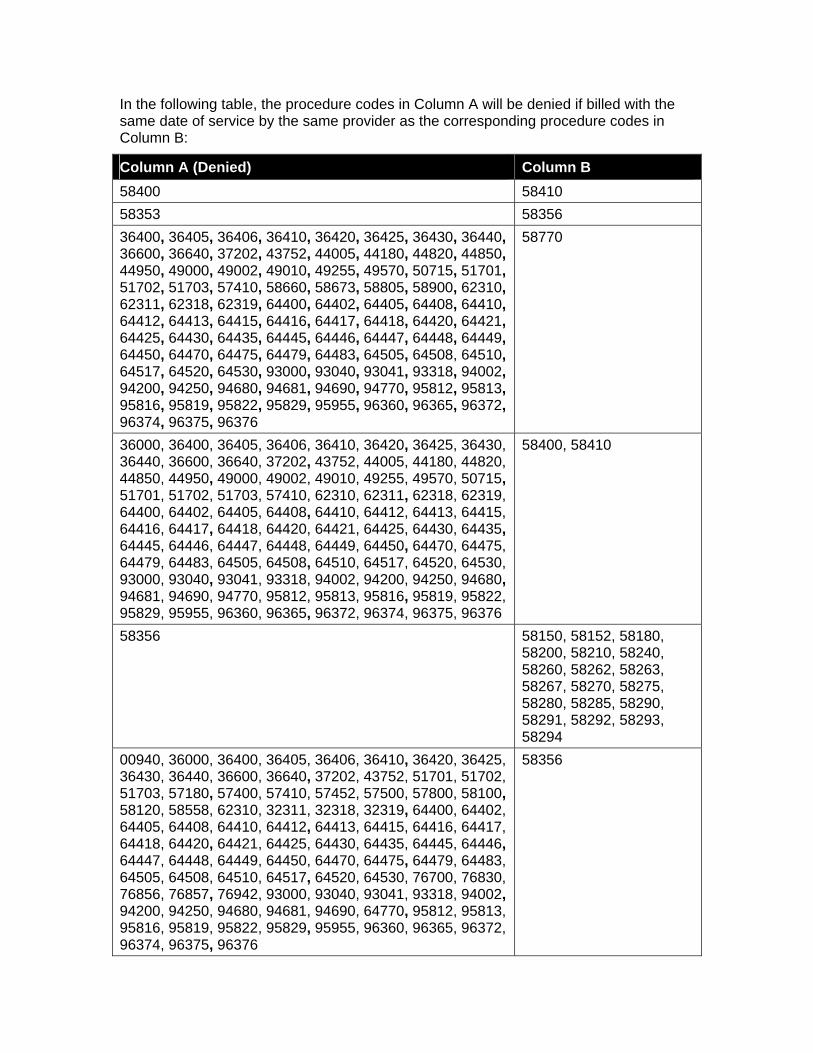
In the following table, the procedure codes in Column A will be denied if billed with the same date of service by the same provider as the corresponding procedure codes in Column B:
Column A (Denied) Column B 58400 58410 58353 58356 36400, 36405, 36406, 36410, 36420, 36425, 36430, 36440, 36600, 36640, 37202, 43752, 44005, 44180, 44820, 44850, 44950, 49000, 49002, 49010, 49255, 49570, 50715, 51701, 51702, 51703, 57410, 58660, 58673, 58805, 58900, 62310, 62311, 62318, 62319, 64400, 64402, 64405, 64408, 64410, 64412, 64413, 64415, 64416, 64417, 64418, 64420, 64421, 64425, 64430, 64435, 64445, 64446, 64447, 64448, 64449, 64450, 64470, 64475, 64479, 64483, 64505, 64508, 64510, 64517, 64520, 64530, 93000, 93040, 93041, 93318, 94002, 94200, 94250, 94680, 94681, 94690, 94770, 95812, 95813, 95816, 95819, 95822, 95829, 95955, 96360, 96365, 96372, 96374, 96375, 96376
58770
36000, 36400, 36405, 36406, 36410, 36420, 36425, 36430, 36440, 36600, 36640, 37202, 43752, 44005, 44180, 44820, 44850, 44950, 49000, 49002, 49010, 49255, 49570, 50715, 51701, 51702, 51703, 57410, 62310, 62311, 62318, 62319, 64400, 64402, 64405, 64408, 64410, 64412, 64413, 64415, 64416, 64417, 64418, 64420, 64421, 64425, 64430, 64435, 64445, 64446, 64447, 64448, 64449, 64450, 64470, 64475, 64479, 64483, 64505, 64508, 64510, 64517, 64520, 64530, 93000, 93040, 93041, 93318, 94002, 94200, 94250, 94680, 94681, 94690, 94770, 95812, 95813, 95816, 95819, 95822, 95829, 95955, 96360, 96365, 96372, 96374, 96375, 96376
58400, 58410
58356 58150, 58152, 58180, 58200, 58210, 58240, 58260, 58262, 58263, 58267, 58270, 58275, 58280, 58285, 58290, 58291, 58292, 58293, 58294
00940, 36000, 36400, 36405, 36406, 36410, 36420, 36425, 36430, 36440, 36600, 36640, 37202, 43752, 51701, 51702, 51703, 57180, 57400, 57410, 57452, 57500, 57800, 58100, 58120, 58558, 62310, 32311, 32318, 32319, 64400, 64402, 64405, 64408, 64410, 64412, 64413, 64415, 64416, 64417, 64418, 64420, 64421, 64425, 64430, 64435, 64445, 64446, 64447, 64448, 64449, 64450, 64470, 64475, 64479, 64483, 64505, 64508, 64510, 64517, 64520, 64530, 76700, 76830, 76856, 76857, 76942, 93000, 93040, 93041, 93318, 94002, 94200, 94250, 94680, 94681, 94690, 64770, 95812, 95813, 95816, 95819, 95822, 95829, 95955, 96360, 96365, 96372, 96374, 96375, 96376
58356
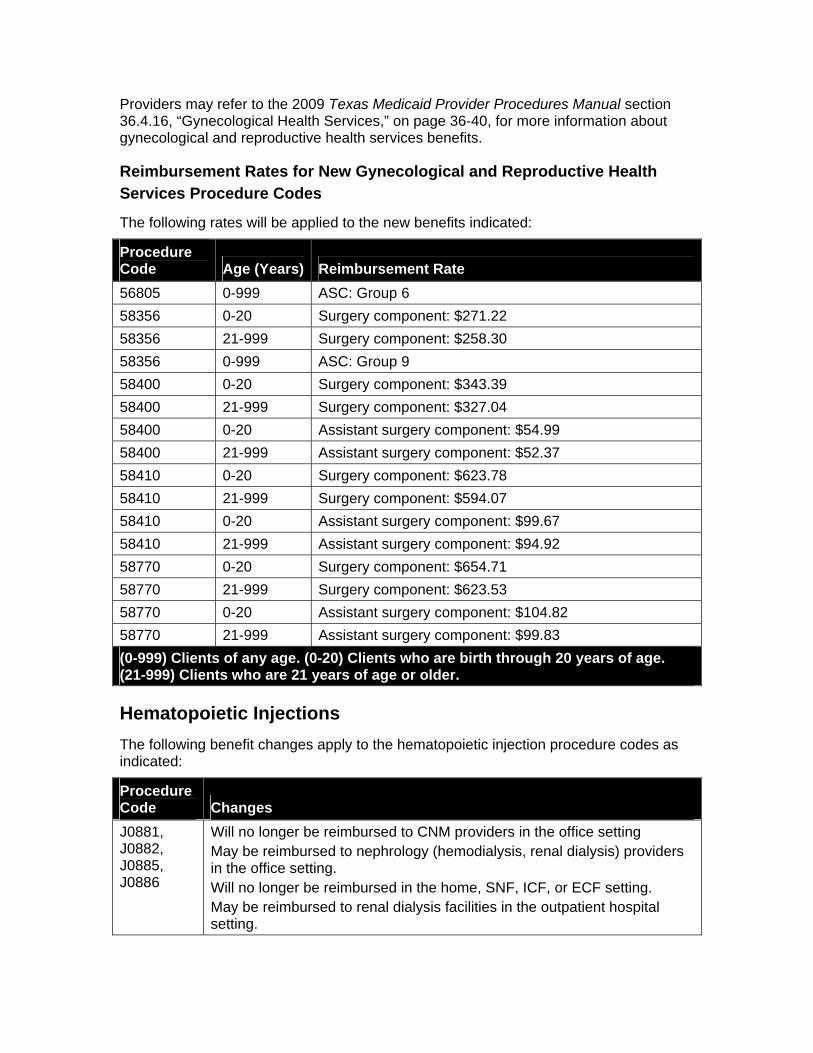
Providers may refer to the 2009 Texas Medicaid Provider Procedures Manual section 36.4.16, “Gynecological Health Services,” on page 36-40, for more information about gynecological and reproductive health services benefits.
Reimbursement Rates for New Gynecological and Reproductive Health Services Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 56805 0-999 ASC: Group 6 58356 0-20 Surgery component: $271.22 58356 21-999 Surgery component: $258.30 58356 0-999 ASC: Group 9 58400 0-20 Surgery component: $343.39 58400 21-999 Surgery component: $327.04 58400 0-20 Assistant surgery component: $54.99 58400 21-999 Assistant surgery component: $52.37 58410 0-20 Surgery component: $623.78 58410 21-999 Surgery component: $594.07 58410 0-20 Assistant surgery component: $99.67 58410 21-999 Assistant surgery component: $94.92 58770 0-20 Surgery component: $654.71 58770 21-999 Surgery component: $623.53 58770 0-20 Assistant surgery component: $104.82 58770 21-999 Assistant surgery component: $99.83 (0-999) Clients of any age. (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older.
Hematopoietic Injections The following benefit changes apply to the hematopoietic injection procedure codes as indicated:
Procedure Code Changes J0881, J0882, J0885, J0886
Will no longer be reimbursed to CNM providers in the office setting May be reimbursed to nephrology (hemodialysis, renal dialysis) providers in the office setting. Will no longer be reimbursed in the home, SNF, ICF, or ECF setting. May be reimbursed to renal dialysis facilities in the outpatient hospital setting.
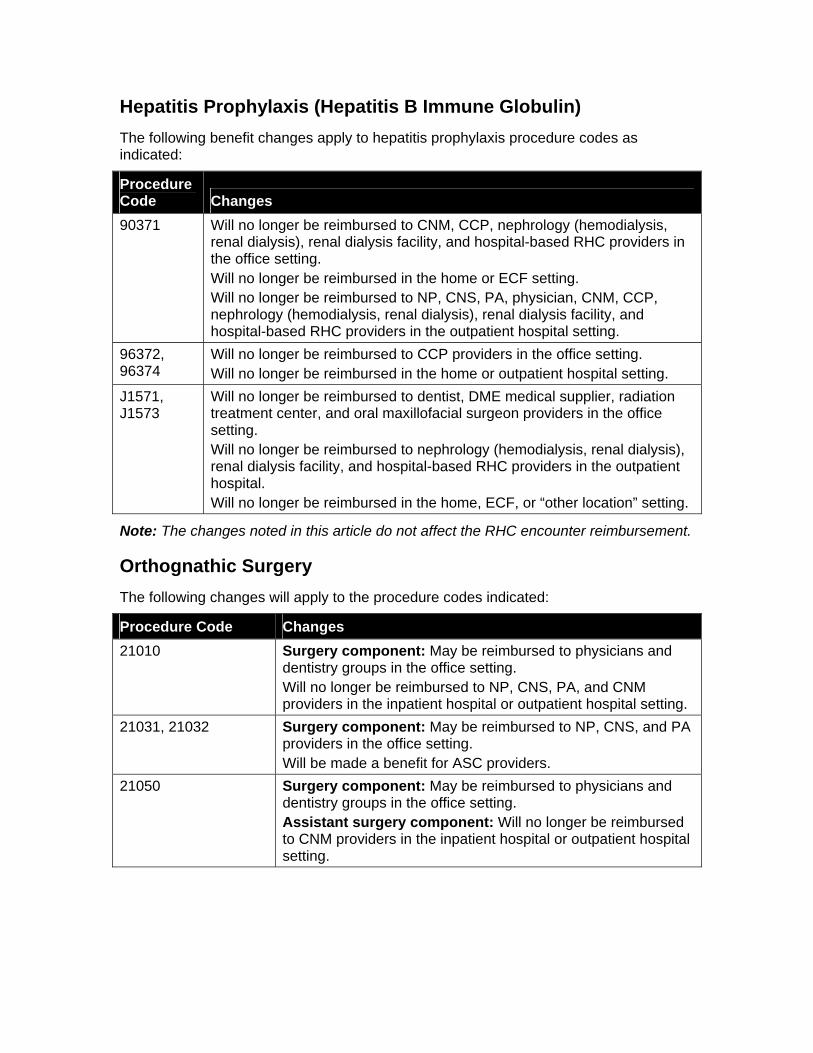
Hepatitis Prophylaxis (Hepatitis B Immune Globulin) The following benefit changes apply to hepatitis prophylaxis procedure codes as indicated:
Procedure Code Changes 90371 Will no longer be reimbursed to CNM, CCP, nephrology (hemodialysis,
renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the home or ECF setting. Will no longer be reimbursed to NP, CNS, PA, physician, CNM, CCP, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting.
96372, 96374
Will no longer be reimbursed to CCP providers in the office setting. Will no longer be reimbursed in the home or outpatient hospital setting.
J1571, J1573
Will no longer be reimbursed to dentist, DME medical supplier, radiation treatment center, and oral maxillofacial surgeon providers in the office setting. Will no longer be reimbursed to nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital. Will no longer be reimbursed in the home, ECF, or “other location” setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement.
Orthognathic Surgery The following changes will apply to the procedure codes indicated:
Procedure Code Changes 21010 Surgery component: May be reimbursed to physicians and
dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting.
21031, 21032 Surgery component: May be reimbursed to NP, CNS, and PA providers in the office setting. Will be made a benefit for ASC providers.
21050 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
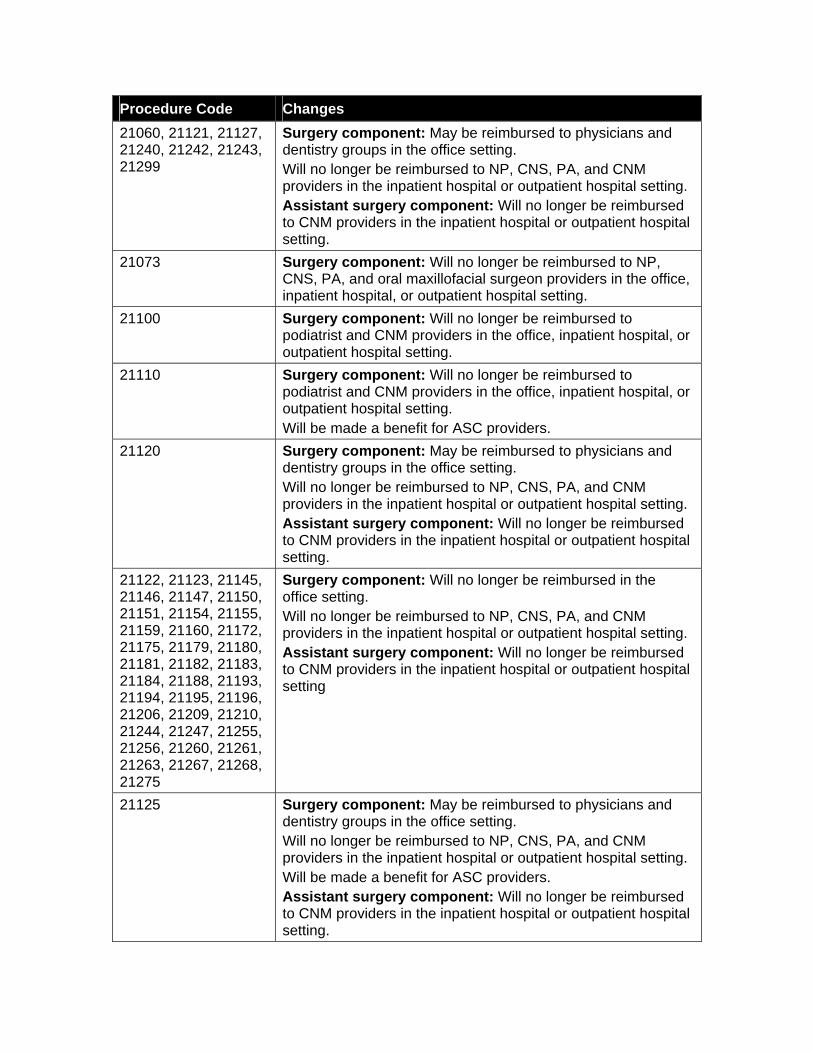
Procedure Code Changes 21060, 21121, 21127, 21240, 21242, 21243, 21299
Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
21073 Surgery component: Will no longer be reimbursed to NP, CNS, PA, and oral maxillofacial surgeon providers in the office, inpatient hospital, or outpatient hospital setting.
21100 Surgery component: Will no longer be reimbursed to podiatrist and CNM providers in the office, inpatient hospital, or outpatient hospital setting.
21110 Surgery component: Will no longer be reimbursed to podiatrist and CNM providers in the office, inpatient hospital, or outpatient hospital setting. Will be made a benefit for ASC providers.
21120 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
21122, 21123, 21145, 21146, 21147, 21150, 21151, 21154, 21155, 21159, 21160, 21172, 21175, 21179, 21180, 21181, 21182, 21183, 21184, 21188, 21193, 21194, 21195, 21196, 21206, 21209, 21210, 21244, 21247, 21255, 21256, 21260, 21261, 21263, 21267, 21268, 21275
Surgery component: Will no longer be reimbursed in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting
21125 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Will be made a benefit for ASC providers. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
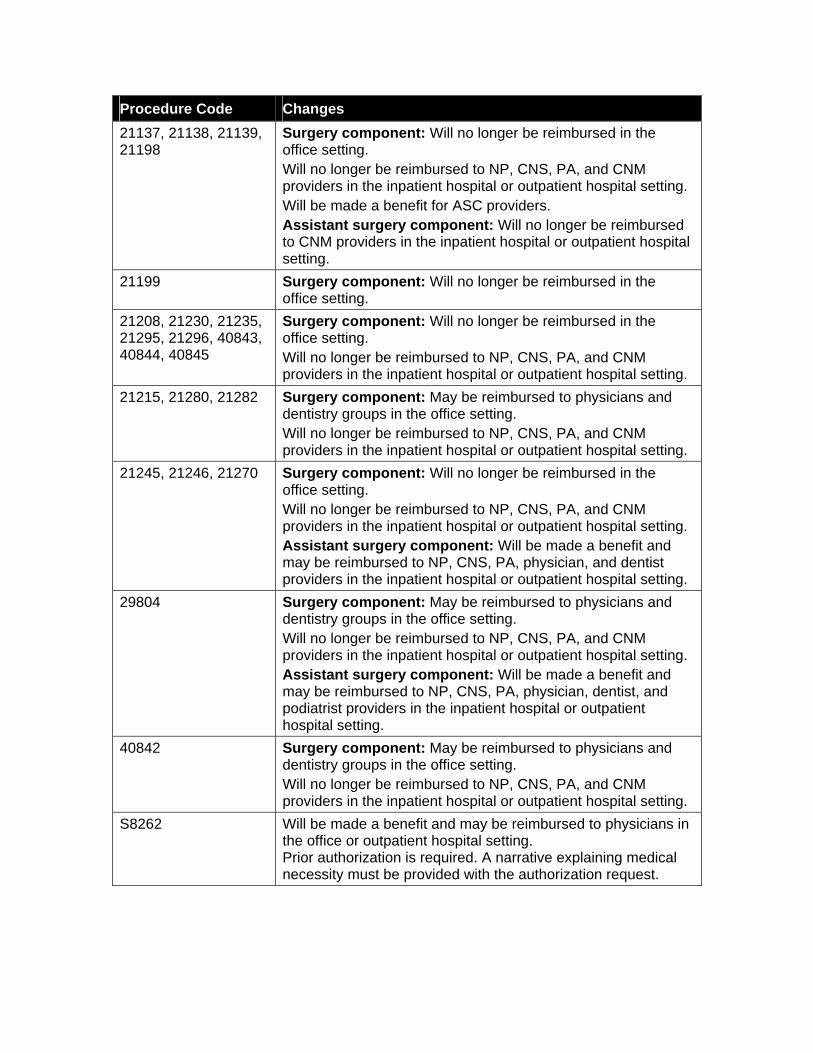
Procedure Code Changes 21137, 21138, 21139, 21198
Surgery component: Will no longer be reimbursed in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Will be made a benefit for ASC providers. Assistant surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
21199 Surgery component: Will no longer be reimbursed in the office setting.
21208, 21230, 21235, 21295, 21296, 40843, 40844, 40845
Surgery component: Will no longer be reimbursed in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting.
21215, 21280, 21282 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting.
21245, 21246, 21270 Surgery component: Will no longer be reimbursed in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will be made a benefit and may be reimbursed to NP, CNS, PA, physician, and dentist providers in the inpatient hospital or outpatient hospital setting.
29804 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. Assistant surgery component: Will be made a benefit and may be reimbursed to NP, CNS, PA, physician, dentist, and podiatrist providers in the inpatient hospital or outpatient hospital setting.
40842 Surgery component: May be reimbursed to physicians and dentistry groups in the office setting. Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting.
S8262 Will be made a benefit and may be reimbursed to physicians in the office or outpatient hospital setting. Prior authorization is required. A narrative explaining medical necessity must be provided with the authorization request.
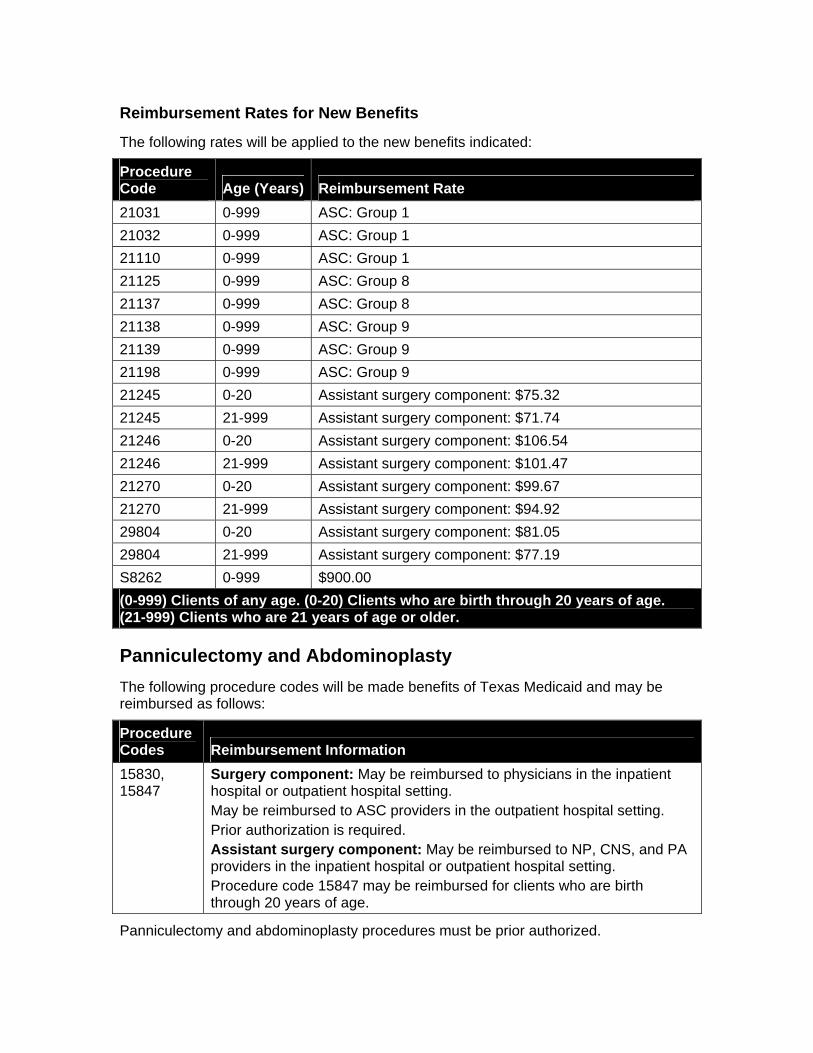
Reimbursement Rates for New Benefits
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 21031 0-999 ASC: Group 1 21032 0-999 ASC: Group 1 21110 0-999 ASC: Group 1 21125 0-999 ASC: Group 8 21137 0-999 ASC: Group 8 21138 0-999 ASC: Group 9 21139 0-999 ASC: Group 9 21198 0-999 ASC: Group 9 21245 0-20 Assistant surgery component: $75.32 21245 21-999 Assistant surgery component: $71.74 21246 0-20 Assistant surgery component: $106.54 21246 21-999 Assistant surgery component: $101.47 21270 0-20 Assistant surgery component: $99.67 21270 21-999 Assistant surgery component: $94.92 29804 0-20 Assistant surgery component: $81.05 29804 21-999 Assistant surgery component: $77.19 S8262 0-999 $900.00 (0-999) Clients of any age. (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older.
Panniculectomy and Abdominoplasty The following procedure codes will be made benefits of Texas Medicaid and may be reimbursed as follows:
Procedure Codes Reimbursement Information 15830, 15847
Surgery component: May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting. May be reimbursed to ASC providers in the outpatient hospital setting. Prior authorization is required. Assistant surgery component: May be reimbursed to NP, CNS, and PA providers in the inpatient hospital or outpatient hospital setting. Procedure code 15847 may be reimbursed for clients who are birth through 20 years of age.
Panniculectomy and abdominoplasty procedures must be prior authorized.
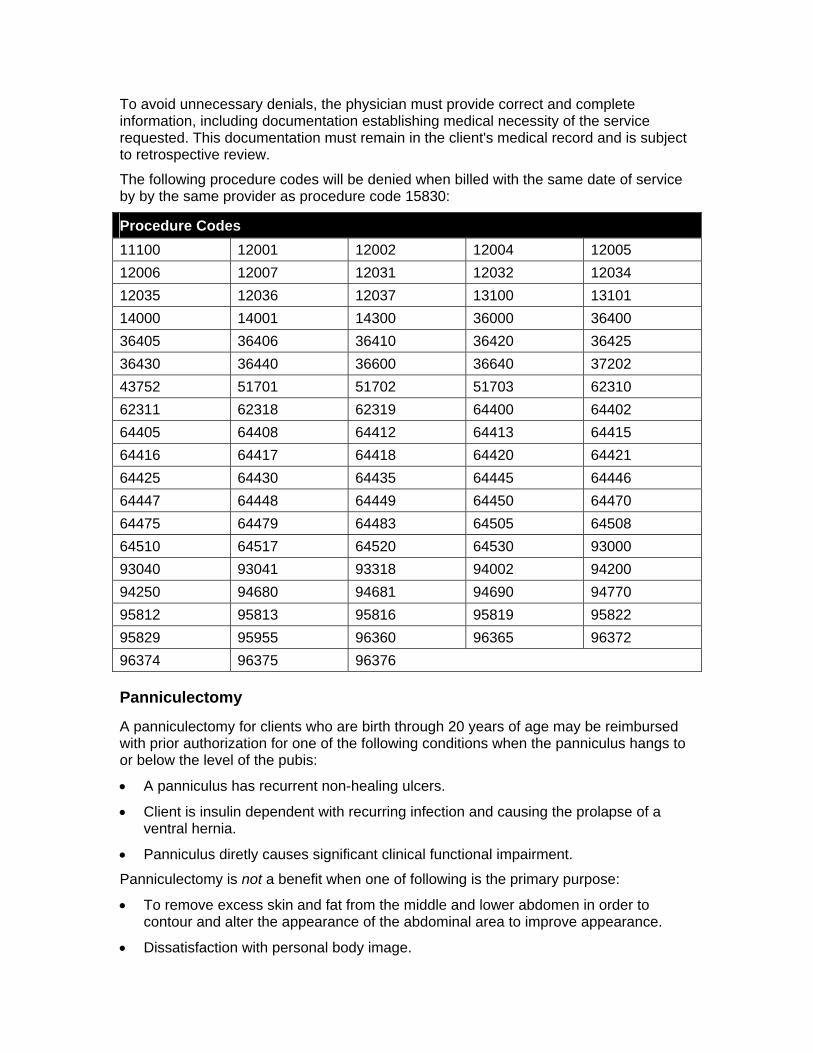
To avoid unnecessary denials, the physician must provide correct and complete information, including documentation establishing medical necessity of the service requested. This documentation must remain in the client's medical record and is subject to retrospective review.
The following procedure codes will be denied when billed with the same date of service by by the same provider as procedure code 15830:
Procedure Codes 11100 12001 12002 12004 12005 12006 12007 12031 12032 12034 12035 12036 12037 13100 13101 14000 14001 14300 36000 36400 36405 36406 36410 36420 36425 36430 36440 36600 36640 37202 43752 51701 51702 51703 62310 62311 62318 62319 64400 64402 64405 64408 64412 64413 64415 64416 64417 64418 64420 64421 64425 64430 64435 64445 64446 64447 64448 64449 64450 64470 64475 64479 64483 64505 64508 64510 64517 64520 64530 93000 93040 93041 93318 94002 94200 94250 94680 94681 94690 94770 95812 95813 95816 95819 95822 95829 95955 96360 96365 96372 96374 96375 96376
Panniculectomy
A panniculectomy for clients who are birth through 20 years of age may be reimbursed with prior authorization for one of the following conditions when the panniculus hangs to or below the level of the pubis:
• A panniculus has recurrent non-healing ulcers.
• Client is insulin dependent with recurring infection and causing the prolapse of a ventral hernia.
• Panniculus diretly causes significant clinical functional impairment.
Panniculectomy is not a benefit when one of following is the primary purpose:
• To remove excess skin and fat from the middle and lower abdomen in order to contour and alter the appearance of the abdominal area to improve appearance.
• Dissatisfaction with personal body image.
• To minimize the risk of ventral hernia formation of recurrence.
• For the sole purpose of treating neck or back pain.
Panniculectomy may be prior authorized when the client meets one of the following:
• Panniculectomy is planned and there is no history of significant weight loss or gastric bypass surgery.
• Panniculectomy is planned without history of gastric bypass surgery but with significant weight loss and the paniculus hangs to or below the level of the pubis.
• Panniculectomy is planned with history of gastric bypass surgery or abdominoplasty and the client is 12 months post-surgery.
If a panniculectomy is planned and there is no history of significant weight loss or gastric bypass surgery, or a panniculectomy is planned without history of gastric bypass surgery but with significant weight loss and the paniculus hangs to or below the level of the pubis, one of the following must be met:
• Documentation of recurrent episodes of infection or recurrent non-healing ulcers over 3 months that are non-responsive to treatment or appropriate medical therapy, such as oral or topical prescription.
• The client is insulin-dependent and has a serious infection control problem and the panniculus is causing the prolapse of a ventral hernia.
• Documentation by the treating physician that the panniculus directly causes significant clinical functional impairment. Clinical functional impairment may be indicated by associated musculoskeletal dysfunction or interference with activities of daily living and there is reasonable evidence to support that this surgical intervention will correct the condition.
If a panniculectomy is planned with a history of gastric bypass surgery or abdominoplasty and the client is 12 months post-surgery, the following must be met:
• Documentation that the panniculus hangs to or below the level of the pubis and the individual has maintained a significant (100 pounds or more), stable weight loss for at least 6 months. Documentation must include the weight loss history, prior and current height, and prior and current weight, and the history and physical including all previous surgeries.
• Documentation of recurrent episodes of infection or recurrent non-healing ulcers over 3 months that are non-responsive to treatment or appropriate medical therapy, such as oral or topical prescription. The 12-month post-gastric bypass requirement may be waived.
• The client is insulin-dependent and has a serious infection control problem and the panniculus is causing the prolapse of a ventral hernia. The 12-month post-gastric bypass requirement may be waived.
• Documentation by the treating physician that the panniculus directly causes significant clinical functional impairment. The 12-month post-gastric bypass requirement may be waived. Clinical functional impairment may be indicated by associated musculoskeletal dysfunction or interference with activities of daily living and there is reasonable evidence to support that this surgical intervention will correct the condition.
All medical record documentation pertinent to the individual's evaluation and treatment must support medical necessity of the panniculectomy. Documentation may include the following:
• Office records
• Consultation reports
• Operative reports
• Other hospital records (examples: pathology report, history and physical)
Documentation to support the panniculectomy must be submitted with the request for prior authorization. In addition to medical record documentation, the provider may also submit a letter of support or an explanation to substantiate medical necessity.
This service is typically expected to be limited to once per lifetime; however, repeat panniculectomies may be considered for prior authorization upon submission of supporting documentation as outlined above.
A panniculectomy provided as a secondary surgery may be considered for prior authorization when the panniculus interferes with a medically necessary intra-abdominal surgery (e.g., abdominal hernia repair or hysterectomy) or to facilitate an improved anatomical field in order to provide radiation treatment to abdomen. Documentation of medical necessity must include:
• The comorbidity for the diagnosis of the primary surgery or for the nature of the condition undergoing radiation treatment.
• Documentation supporting the need for the panniculectomy as the panniculus hangs below the level of the pubis and will significantly interfere with planned surgical procedure, or the abdominal structures identified as requiring radiation therapy will not be adequately treated due to the size of the panniculus.
A panniculectomy provided as a secondary surgery may be considered when the primary surgery was performed for an urgent condition defined as a symptom or condition that is not an emergency, but requires further diagnostic work-up or treatment within 24 hours to avoid a subsequent emergent situation.
The need for the panniculectomy as a secondary surgery in conjunction with a primary urgent surgery must be supported by retrospective review of submission of all of the following documentation:
• History and physical and the operative report.
• The panniculus hangs below the level of the pubis and would have significantly interfered with the urgent primary surgical procedure.
Abdominoplasty
An abdominoplasty for a client who is birth through 20 years of age may be reimbursed with prior authorization for one of the following conditions:
• Prune belly.
• Diastasis recti in the presence of a true midline hernia (ventral or umbilical).
Abdominoplasty is not a benefit when one of the following is the primary purpose:
• To remove excess skin and fat and tighten abdominal wall from the middle and lower abdomen in order to contour and alter the appearance of the abdominal area to improve appearance.
• Dissatisfaction with personal body image.
• To repair diastases recti (unless prior authorization as outlined below has been met).
Abdominoplasty may be prior authorized when the client meets all of the following criteria:
• Documented diagnosis of prune belly (i.e., Eagle Barret syndrome) or repair of diastasis recti in the presence of a true midline hernia (ventral or umbilical).
• Documentation for reconstructive surgery that must include, appropriate historical medical record documentation and may include any of the following:
o Consultation reports.
o Operative reports and/or other applicable hospital records (examples: pathology report, history and physical).
o Office records.
o Letters with pertinent information from provider. (When medical records are requested, a letter of support and/or explanation may be helpful, but alone will not be considered sufficient documentation to make a medical necessity determination.)
• For repair of diastasis recti with a true midline hernia, documentation must also include all of the following:
o The size of the hernia.
o Whether it is reducible, painful, or other symptoms.
o Whether there is a defect rather than just thinning of the abdominal fascia.
• Consideration of other abdominal diagnosis may be considered for prior authorization with the submission of additional supporting documentation that may include the following:
o Consultation reports.
o Operative reports and/or other applicable hospital records (examples: pathology report, history and physical).
o Office records.
o Letters with pertinent information from provider (When medical records are requested, a letter of support and/or explanation may be helpful, but alone will not be considered sufficient documentation to make a medical necessity determination.)
Reimbursement Rates for New Panniculectomy and Abdominoplasty Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 15830 0-20 Surgery component: $858.05 15830 21-999 Surgery component: $817.19 15830 0-20 Assistant surgery component: $137.19 15830 21-999 Assistant surgery component: $130.65 15830 0 - 999 ASC: Group 6 15847 0-20 Surgery component: $831.99 15847 0-20 Assistant surgery component: $133.18 15847 0 - 999 ASC: Group 6 (0-999) Clients of any age. (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older.
Penile and Testicular Prosthesis The following services may be reimbursed by Texas Medicaid with prior authorization:
• Removal of a penile prosthesis without replacement.
• Insertion of testicular prosthesis for the replacement of congenitally absent testes or testes lost due to disease, injury, or surgery.
The following procedure codes will be made benefits of Texas Medicaid and may be reimbursed as follows:
Procedure Codes Reimbursement Information 54406, 54415
May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting for male clients who are 21 years of age or older. Prior authorization is required.
54660 May be reimbursed to physicians in the inpatient hospital or outpatient hospital setting for male clients who are birth through 20 years of age. Prior authorization is required.
Prior authorization is required for testicular prosthesis (procedure code 54660) with the following criteria:
• The male client is birth through 20 years of age.
• The client has lost a testicle as a result of cancer or trauma or has congenital absence of a testicle.
• The loss of the testicle has resulted in detrimental psycho-social sequelae, as evidenced by a psychiatric evaluation.
Removal of a penile prosthesis may be considered for prior authorization with documentation submitted indicating the prosthetic has resulted in infection, erosion, or pain.
Prior authorization requests for PCCM clients must be submitted by the physician to the PCCM Outpatient Prior Authorization Department. Authorizations may be submitted online at www.tmhp.com, by phone at 1-888-302-6167, or by fax to 1-512-302-5039. Providers must use the PCCM Inpatient/Outpatient Authorization Form. The request must be submitted with documentation that supports medical necessity.
All other requests for prior authorization must be submitted by the physician to the SMPA department using the Special Medical Prior Authorization (SMPA) Request Form. Authorizations may be submitted online at www.tmhp.com, by fax to 1-512-514-4213, or by mail at:
Texas Medicaid & Healthcare Partnership Special Medical Prior Authorization Department
12357-B Riata Trace Parkway, Suite 150 Austin TX 78727
The request must be submitted with documentation that supports medical necessity.
The following procedure codes will be denied when submitted with the same date of service as procedure code 54406 or 54415:
Procedure Codes 36000 36400 36405 36406 36410 36420 36425 36430 36440 36600 36640 37202 43752 51703 54470 62318 62319 64415 64416 64417 64450 64475 64479 64483 64505 64508 64510 64517 64520 64530 93000 93040 93041 93318 94002 94200 94250 94680 94681 94690 94770 95812 95813 95816 95819 95822 95829 95955 96365 96372 96374 96375 96376
Reimbursement Rates for New Penile and Testicular Prosthesis Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 54406 0-20 Surgery component: $600.29 54406 21-999 Surgery component: $571.70 54406 0-20 Assistant surgery component: $96.23
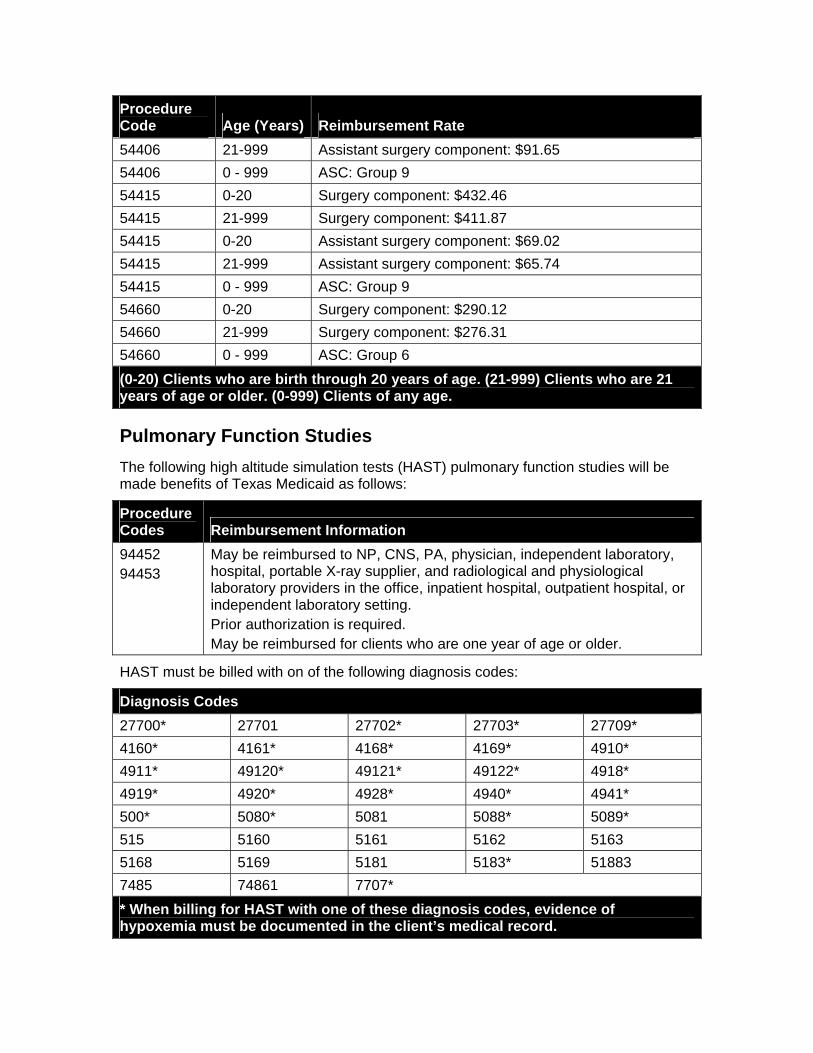
Procedure Code Age (Years) Reimbursement Rate 54406 21-999 Assistant surgery component: $91.65 54406 0 - 999 ASC: Group 9 54415 0-20 Surgery component: $432.46 54415 21-999 Surgery component: $411.87 54415 0-20 Assistant surgery component: $69.02 54415 21-999 Assistant surgery component: $65.74 54415 0 - 999 ASC: Group 9 54660 0-20 Surgery component: $290.12 54660 21-999 Surgery component: $276.31 54660 0 - 999 ASC: Group 6 (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older. (0-999) Clients of any age.
Pulmonary Function Studies The following high altitude simulation tests (HAST) pulmonary function studies will be made benefits of Texas Medicaid as follows:
Procedure Codes Reimbursement Information 94452 94453
May be reimbursed to NP, CNS, PA, physician, independent laboratory, hospital, portable X-ray supplier, and radiological and physiological laboratory providers in the office, inpatient hospital, outpatient hospital, or independent laboratory setting. Prior authorization is required. May be reimbursed for clients who are one year of age or older.
HAST must be billed with on of the following diagnosis codes:
Diagnosis Codes 27700* 27701 27702* 27703* 27709* 4160* 4161* 4168* 4169* 4910* 4911* 49120* 49121* 49122* 4918* 4919* 4920* 4928* 4940* 4941* 500* 5080* 5081 5088* 5089* 515 5160 5161 5162 5163 5168 5169 5181 5183* 51883 7485 74861 7707* * When billing for HAST with one of these diagnosis codes, evidence of hypoxemia must be documented in the client’s medical record.
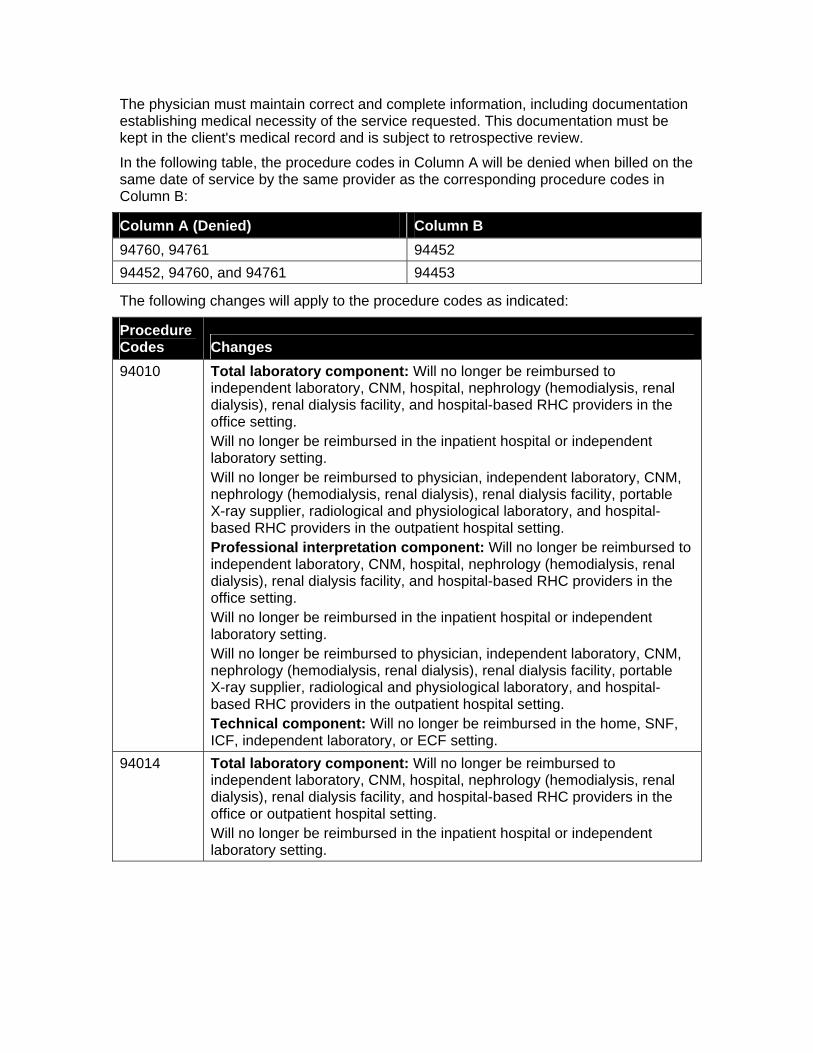
The physician must maintain correct and complete information, including documentation establishing medical necessity of the service requested. This documentation must be kept in the client's medical record and is subject to retrospective review.
In the following table, the procedure codes in Column A will be denied when billed on the same date of service by the same provider as the corresponding procedure codes in Column B:
Column A (Denied) Column B 94760, 94761 94452 94452, 94760, and 94761 94453
The following changes will apply to the procedure codes as indicated:
Procedure Codes Changes 94010 Total laboratory component: Will no longer be reimbursed to
independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Technical component: Will no longer be reimbursed in the home, SNF, ICF, independent laboratory, or ECF setting.
94014 Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office or outpatient hospital setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting.
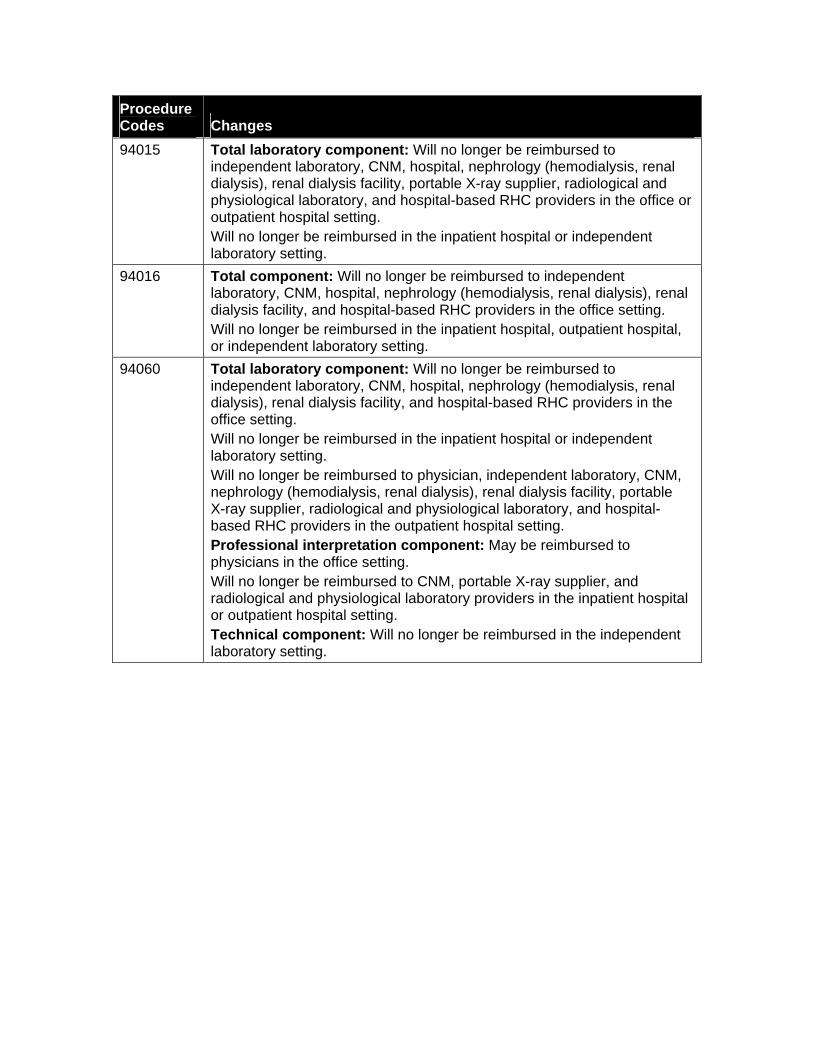
Procedure Codes Changes 94015 Total laboratory component: Will no longer be reimbursed to
independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the office or outpatient hospital setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting.
94016 Total component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital, outpatient hospital, or independent laboratory setting.
94060 Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed in the independent laboratory setting.
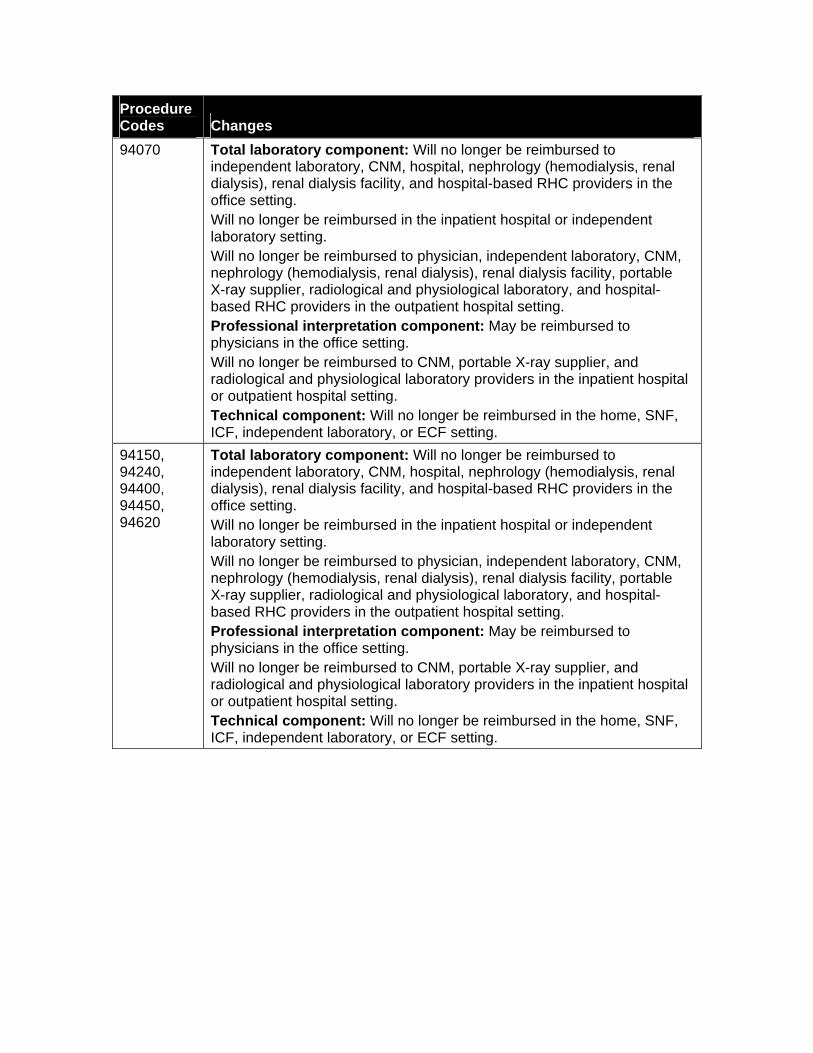
Procedure Codes Changes 94070 Total laboratory component: Will no longer be reimbursed to
independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed in the home, SNF, ICF, independent laboratory, or ECF setting.
94150, 94240, 94400, 94450, 94620
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed in the home, SNF, ICF, independent laboratory, or ECF setting.
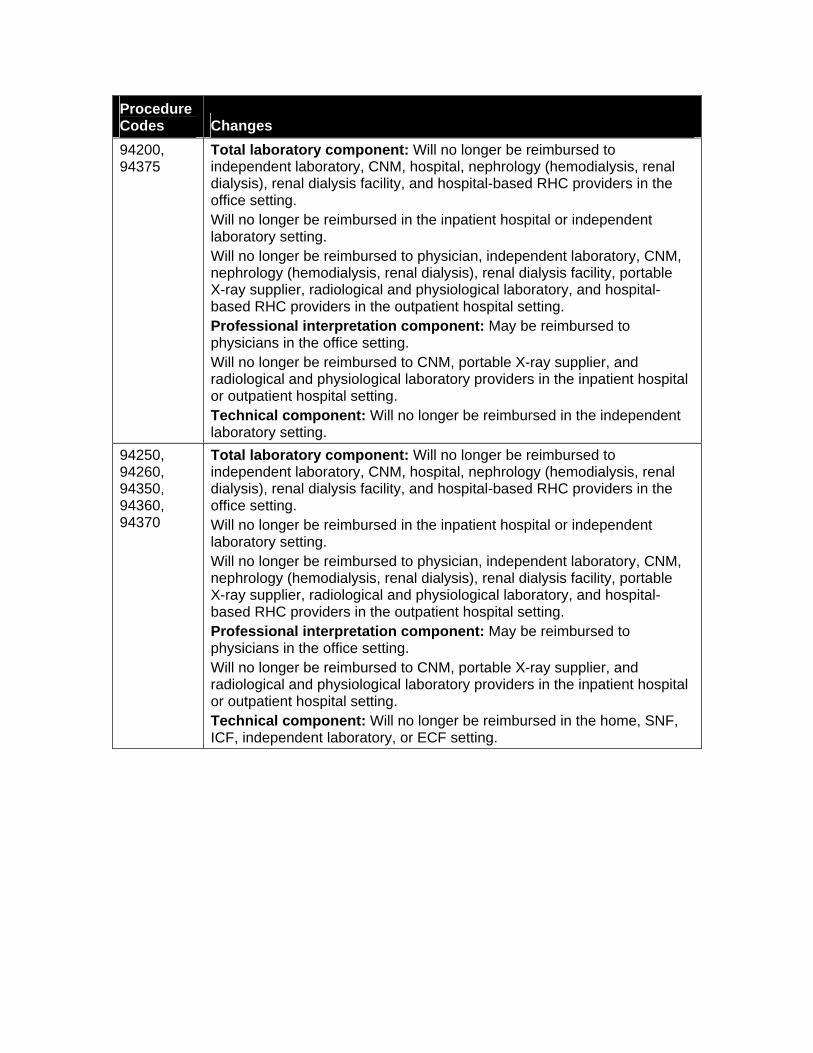
Procedure Codes Changes 94200, 94375
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed in the independent laboratory setting.
94250, 94260, 94350, 94360, 94370
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed in the home, SNF, ICF, independent laboratory, or ECF setting.
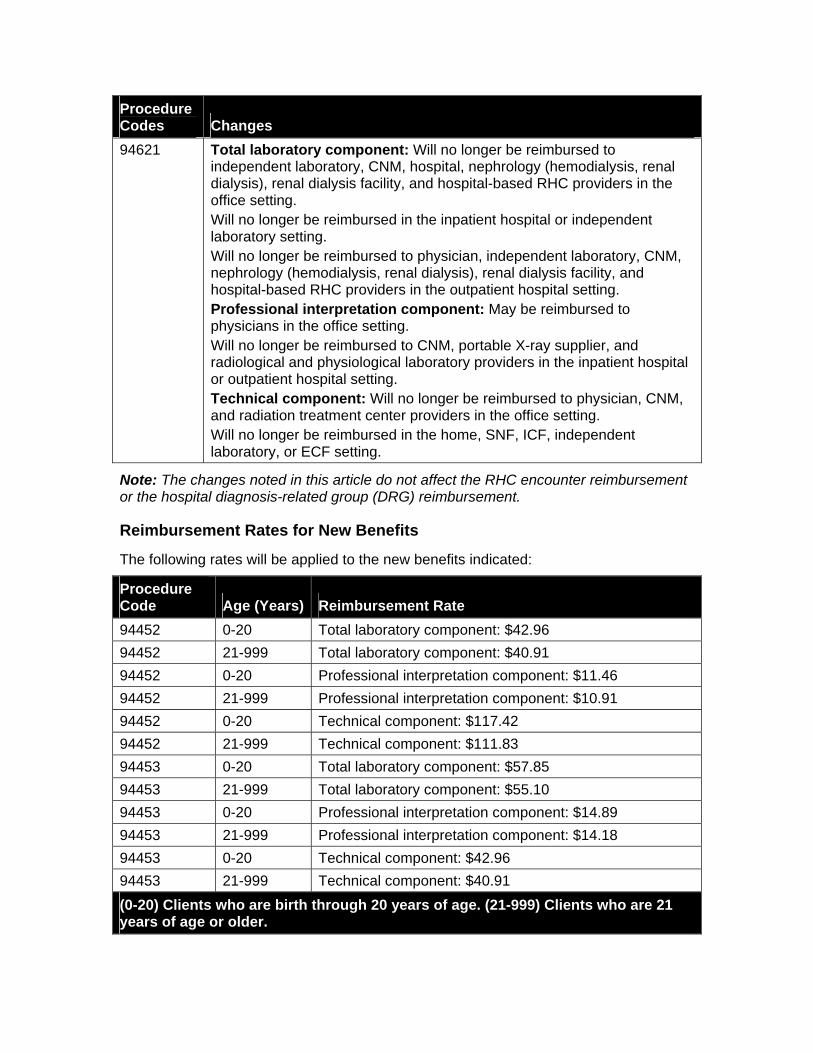
Procedure Codes Changes 94621 Total laboratory component: Will no longer be reimbursed to
independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: May be reimbursed to physicians in the office setting. Will no longer be reimbursed to CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. Technical component: Will no longer be reimbursed to physician, CNM, and radiation treatment center providers in the office setting. Will no longer be reimbursed in the home, SNF, ICF, independent laboratory, or ECF setting.
Note: The changes noted in this article do not affect the RHC encounter reimbursement or the hospital diagnosis-related group (DRG) reimbursement.
Reimbursement Rates for New Benefits
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 94452 0-20 Total laboratory component: $42.96 94452 21-999 Total laboratory component: $40.91 94452 0-20 Professional interpretation component: $11.46 94452 21-999 Professional interpretation component: $10.91 94452 0-20 Technical component: $117.42 94452 21-999 Technical component: $111.83 94453 0-20 Total laboratory component: $57.85 94453 21-999 Total laboratory component: $55.10 94453 0-20 Professional interpretation component: $14.89 94453 21-999 Professional interpretation component: $14.18 94453 0-20 Technical component: $42.96 94453 21-999 Technical component: $40.91 (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older.
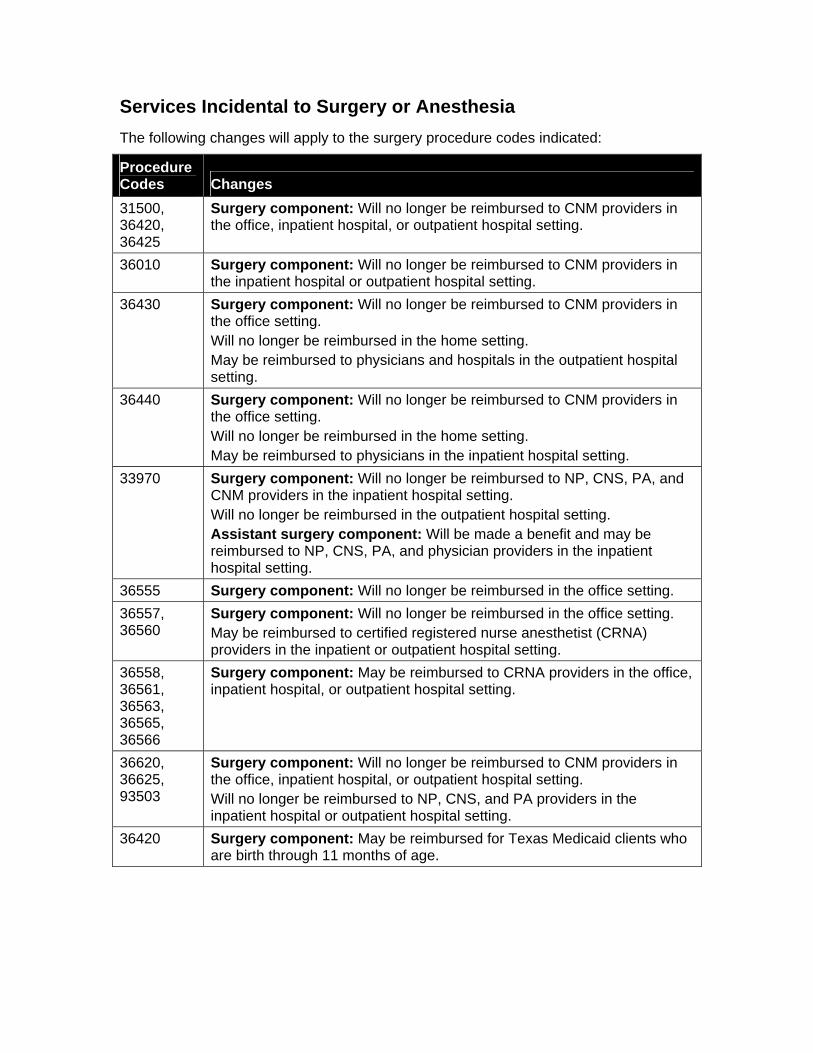
Services Incidental to Surgery or Anesthesia The following changes will apply to the surgery procedure codes indicated:
Procedure Codes Changes 31500, 36420, 36425
Surgery component: Will no longer be reimbursed to CNM providers in the office, inpatient hospital, or outpatient hospital setting.
36010 Surgery component: Will no longer be reimbursed to CNM providers in the inpatient hospital or outpatient hospital setting.
36430 Surgery component: Will no longer be reimbursed to CNM providers in the office setting. Will no longer be reimbursed in the home setting. May be reimbursed to physicians and hospitals in the outpatient hospital setting.
36440 Surgery component: Will no longer be reimbursed to CNM providers in the office setting. Will no longer be reimbursed in the home setting. May be reimbursed to physicians in the inpatient hospital setting.
33970 Surgery component: Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital setting. Will no longer be reimbursed in the outpatient hospital setting. Assistant surgery component: Will be made a benefit and may be reimbursed to NP, CNS, PA, and physician providers in the inpatient hospital setting.
36555 Surgery component: Will no longer be reimbursed in the office setting. 36557, 36560
Surgery component: Will no longer be reimbursed in the office setting. May be reimbursed to certified registered nurse anesthetist (CRNA) providers in the inpatient or outpatient hospital setting.
36558, 36561, 36563, 36565, 36566
Surgery component: May be reimbursed to CRNA providers in the office, inpatient hospital, or outpatient hospital setting.
36620, 36625, 93503
Surgery component: Will no longer be reimbursed to CNM providers in the office, inpatient hospital, or outpatient hospital setting. Will no longer be reimbursed to NP, CNS, and PA providers in the inpatient hospital or outpatient hospital setting.
36420 Surgery component: May be reimbursed for Texas Medicaid clients who are birth through 11 months of age.
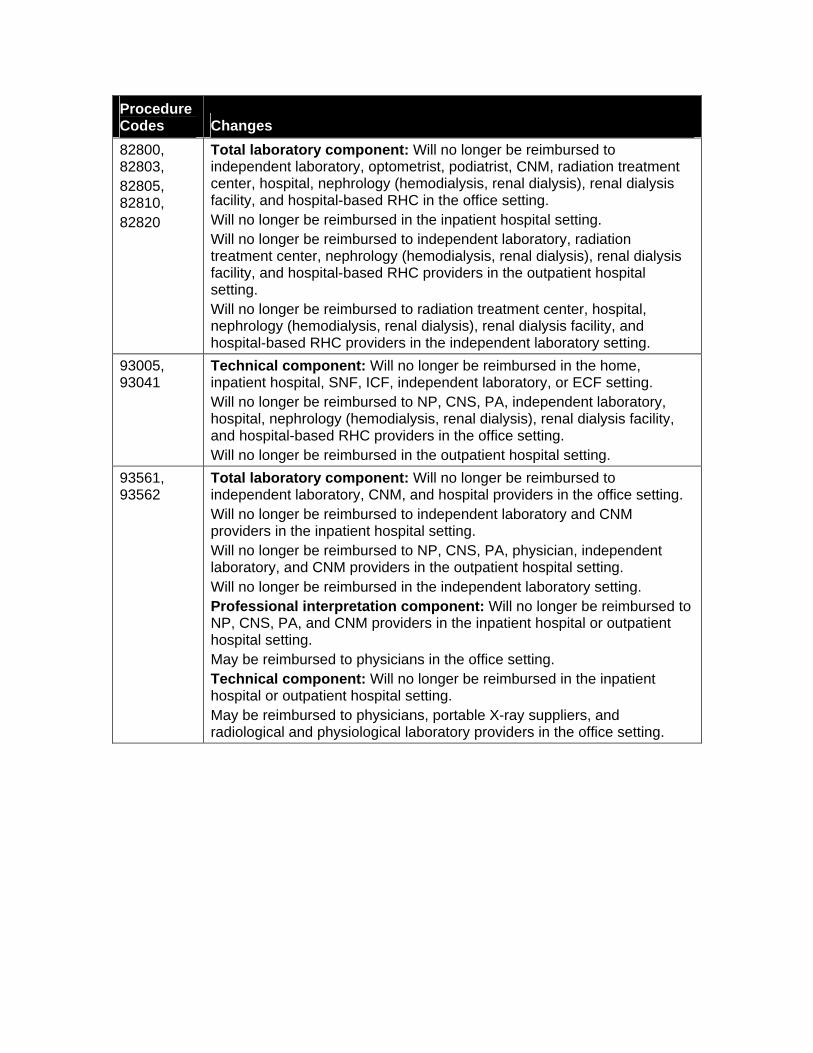
Procedure Codes Changes 82800, 82803, 82805, 82810, 82820
Total laboratory component: Will no longer be reimbursed to independent laboratory, optometrist, podiatrist, CNM, radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC in the office setting. Will no longer be reimbursed in the inpatient hospital setting. Will no longer be reimbursed to independent laboratory, radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the outpatient hospital setting. Will no longer be reimbursed to radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the independent laboratory setting.
93005, 93041
Technical component: Will no longer be reimbursed in the home, inpatient hospital, SNF, ICF, independent laboratory, or ECF setting. Will no longer be reimbursed to NP, CNS, PA, independent laboratory, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the outpatient hospital setting.
93561, 93562
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, and hospital providers in the office setting. Will no longer be reimbursed to independent laboratory and CNM providers in the inpatient hospital setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, and CNM providers in the outpatient hospital setting. Will no longer be reimbursed in the independent laboratory setting. Professional interpretation component: Will no longer be reimbursed to NP, CNS, PA, and CNM providers in the inpatient hospital or outpatient hospital setting. May be reimbursed to physicians in the office setting. Technical component: Will no longer be reimbursed in the inpatient hospital or outpatient hospital setting. May be reimbursed to physicians, portable X-ray suppliers, and radiological and physiological laboratory providers in the office setting.
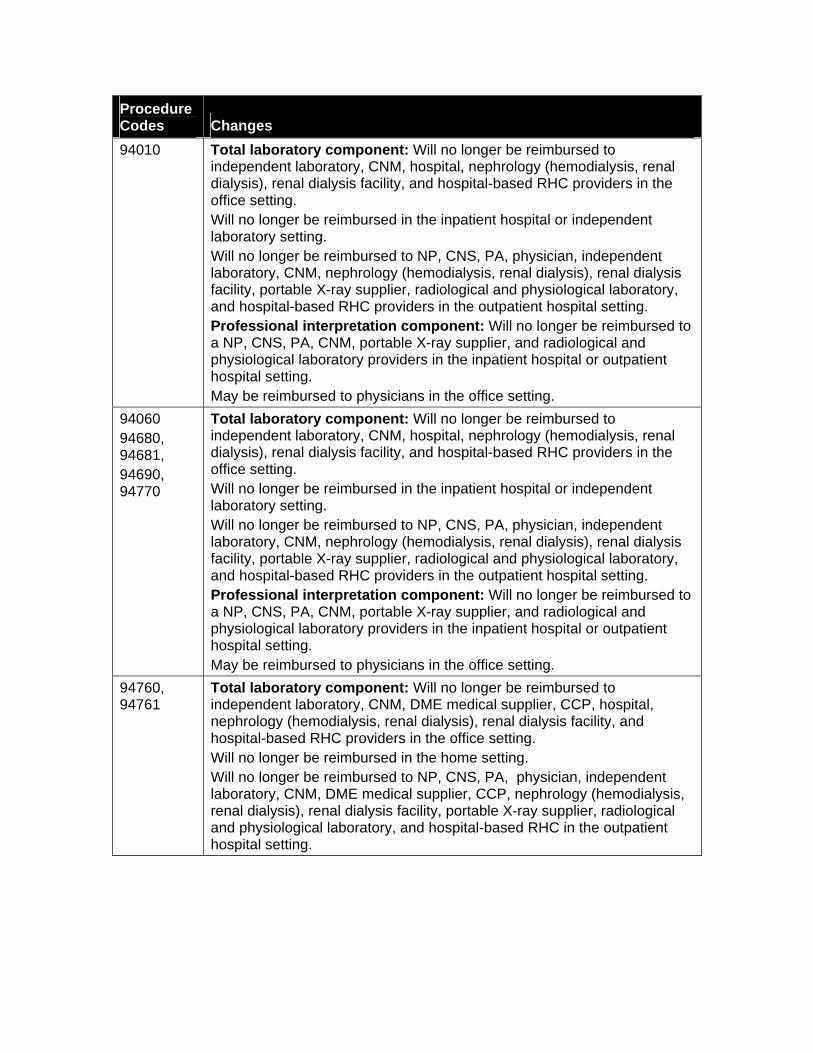
Procedure Codes Changes 94010 Total laboratory component: Will no longer be reimbursed to
independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: Will no longer be reimbursed to a NP, CNS, PA, CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. May be reimbursed to physicians in the office setting.
94060 94680, 94681, 94690, 94770
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the inpatient hospital or independent laboratory setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting. Professional interpretation component: Will no longer be reimbursed to a NP, CNS, PA, CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital or outpatient hospital setting. May be reimbursed to physicians in the office setting.
94760, 94761
Total laboratory component: Will no longer be reimbursed to independent laboratory, CNM, DME medical supplier, CCP, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, and hospital-based RHC providers in the office setting. Will no longer be reimbursed in the home setting. Will no longer be reimbursed to NP, CNS, PA, physician, independent laboratory, CNM, DME medical supplier, CCP, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC in the outpatient hospital setting.
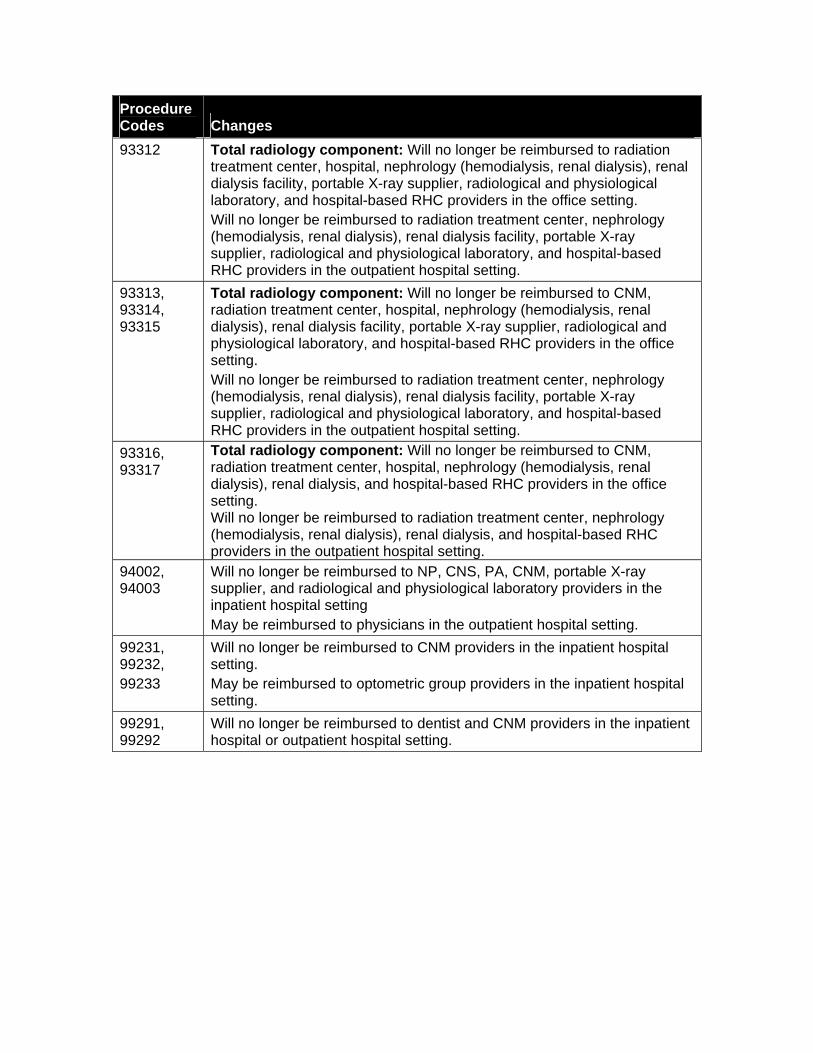
Procedure Codes Changes 93312 Total radiology component: Will no longer be reimbursed to radiation
treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting.
93313, 93314, 93315
Total radiology component: Will no longer be reimbursed to CNM, radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis facility, portable X-ray supplier, radiological and physiological laboratory, and hospital-based RHC providers in the outpatient hospital setting.
93316, 93317
Total radiology component: Will no longer be reimbursed to CNM, radiation treatment center, hospital, nephrology (hemodialysis, renal dialysis), renal dialysis, and hospital-based RHC providers in the office setting. Will no longer be reimbursed to radiation treatment center, nephrology (hemodialysis, renal dialysis), renal dialysis, and hospital-based RHC providers in the outpatient hospital setting.
94002, 94003
Will no longer be reimbursed to NP, CNS, PA, CNM, portable X-ray supplier, and radiological and physiological laboratory providers in the inpatient hospital setting May be reimbursed to physicians in the outpatient hospital setting.
99231, 99232, 99233
Will no longer be reimbursed to CNM providers in the inpatient hospital setting. May be reimbursed to optometric group providers in the inpatient hospital setting.
99291, 99292
Will no longer be reimbursed to dentist and CNM providers in the inpatient hospital or outpatient hospital setting.
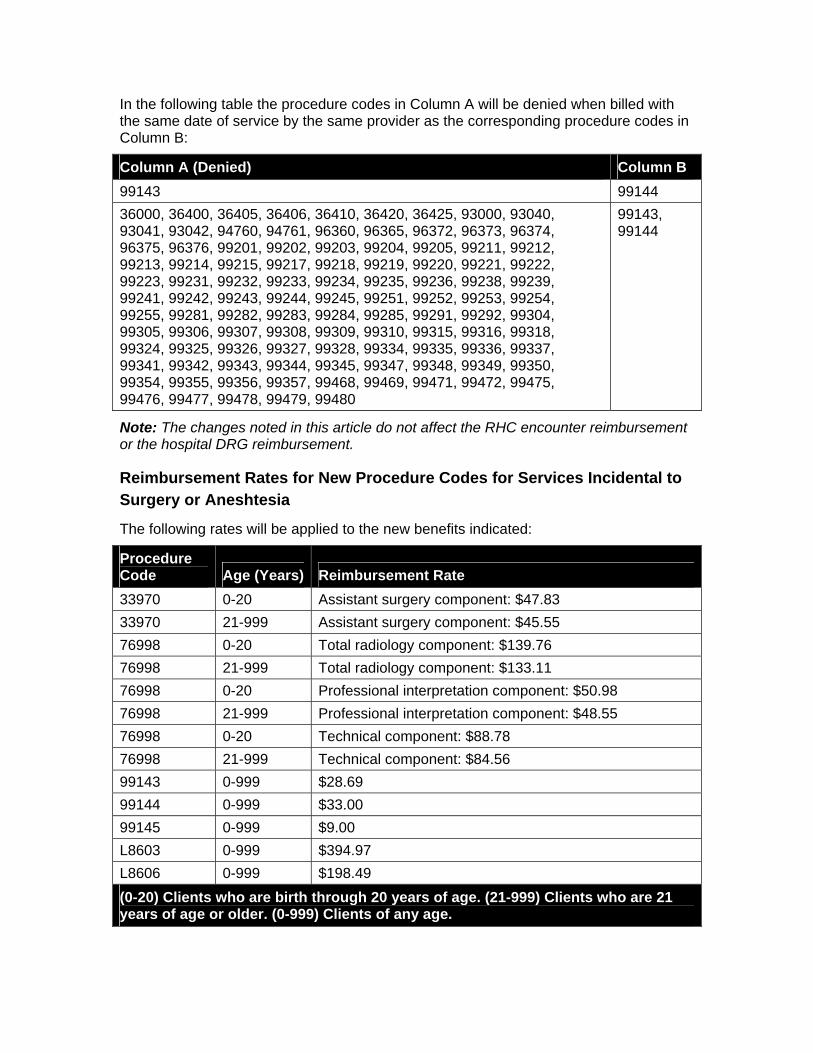
In the following table the procedure codes in Column A will be denied when billed with the same date of service by the same provider as the corresponding procedure codes in Column B:
Column A (Denied) Column B 99143 99144 36000, 36400, 36405, 36406, 36410, 36420, 36425, 93000, 93040, 93041, 93042, 94760, 94761, 96360, 96365, 96372, 96373, 96374, 96375, 96376, 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99217, 99218, 99219, 99220, 99221, 99222, 99223, 99231, 99232, 99233, 99234, 99235, 99236, 99238, 99239, 99241, 99242, 99243, 99244, 99245, 99251, 99252, 99253, 99254, 99255, 99281, 99282, 99283, 99284, 99285, 99291, 99292, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99318, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, 99354, 99355, 99356, 99357, 99468, 99469, 99471, 99472, 99475, 99476, 99477, 99478, 99479, 99480
99143, 99144
Note: The changes noted in this article do not affect the RHC encounter reimbursement or the hospital DRG reimbursement.
Reimbursement Rates for New Procedure Codes for Services Incidental to Surgery or Aneshtesia
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 33970 0-20 Assistant surgery component: $47.83 33970 21-999 Assistant surgery component: $45.55 76998 0-20 Total radiology component: $139.76 76998 21-999 Total radiology component: $133.11 76998 0-20 Professional interpretation component: $50.98 76998 21-999 Professional interpretation component: $48.55 76998 0-20 Technical component: $88.78 76998 21-999 Technical component: $84.56 99143 0-999 $28.69 99144 0-999 $33.00 99145 0-999 $9.00 L8603 0-999 $394.97 L8606 0-999 $198.49 (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older. (0-999) Clients of any age.
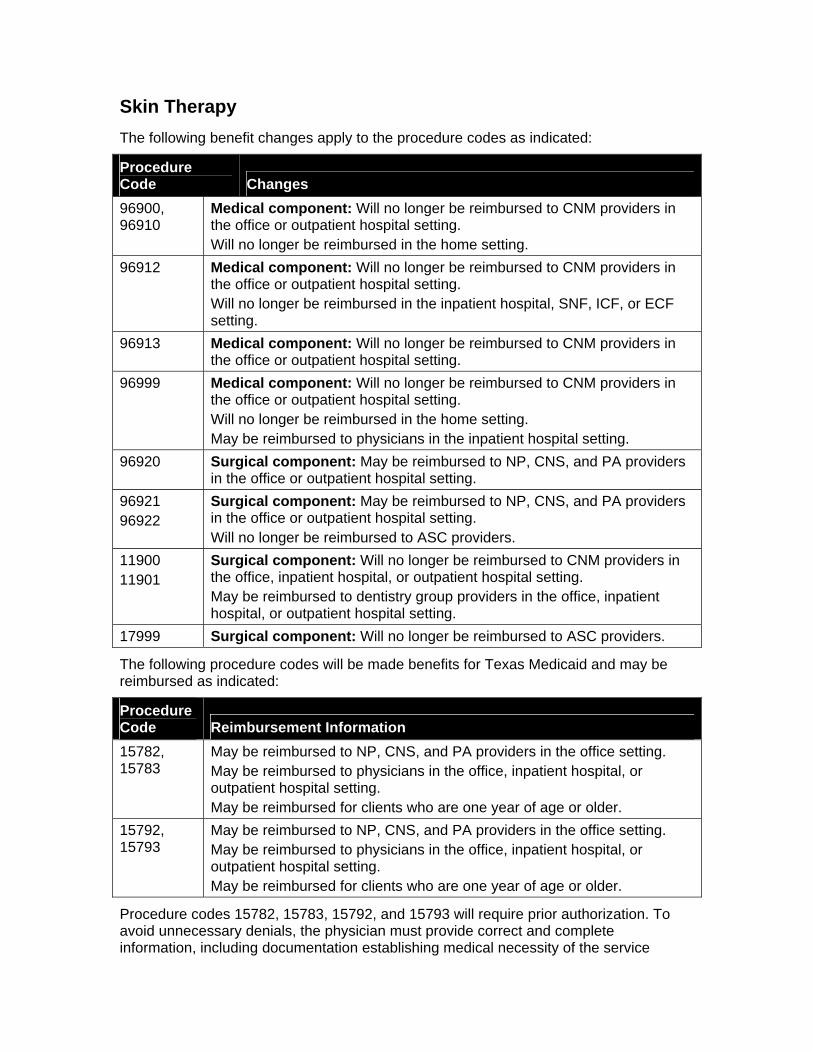
Skin Therapy The following benefit changes apply to the procedure codes as indicated:
Procedure Code Changes 96900, 96910
Medical component: Will no longer be reimbursed to CNM providers in the office or outpatient hospital setting. Will no longer be reimbursed in the home setting.
96912 Medical component: Will no longer be reimbursed to CNM providers in the office or outpatient hospital setting. Will no longer be reimbursed in the inpatient hospital, SNF, ICF, or ECF setting.
96913 Medical component: Will no longer be reimbursed to CNM providers in the office or outpatient hospital setting.
96999 Medical component: Will no longer be reimbursed to CNM providers in the office or outpatient hospital setting. Will no longer be reimbursed in the home setting. May be reimbursed to physicians in the inpatient hospital setting.
96920 Surgical component: May be reimbursed to NP, CNS, and PA providers in the office or outpatient hospital setting.
96921 96922
Surgical component: May be reimbursed to NP, CNS, and PA providers in the office or outpatient hospital setting. Will no longer be reimbursed to ASC providers.
11900 11901
Surgical component: Will no longer be reimbursed to CNM providers in the office, inpatient hospital, or outpatient hospital setting. May be reimbursed to dentistry group providers in the office, inpatient hospital, or outpatient hospital setting.
17999 Surgical component: Will no longer be reimbursed to ASC providers.
The following procedure codes will be made benefits for Texas Medicaid and may be reimbursed as indicated:
Procedure Code Reimbursement Information 15782, 15783
May be reimbursed to NP, CNS, and PA providers in the office setting. May be reimbursed to physicians in the office, inpatient hospital, or outpatient hospital setting. May be reimbursed for clients who are one year of age or older.
15792, 15793
May be reimbursed to NP, CNS, and PA providers in the office setting. May be reimbursed to physicians in the office, inpatient hospital, or outpatient hospital setting. May be reimbursed for clients who are one year of age or older.
Procedure codes 15782, 15783, 15792, and 15793 will require prior authorization. To avoid unnecessary denials, the physician must provide correct and complete information, including documentation establishing medical necessity of the service
requested. This documentation must remain in the client's medical record and is subject to retrospective review.
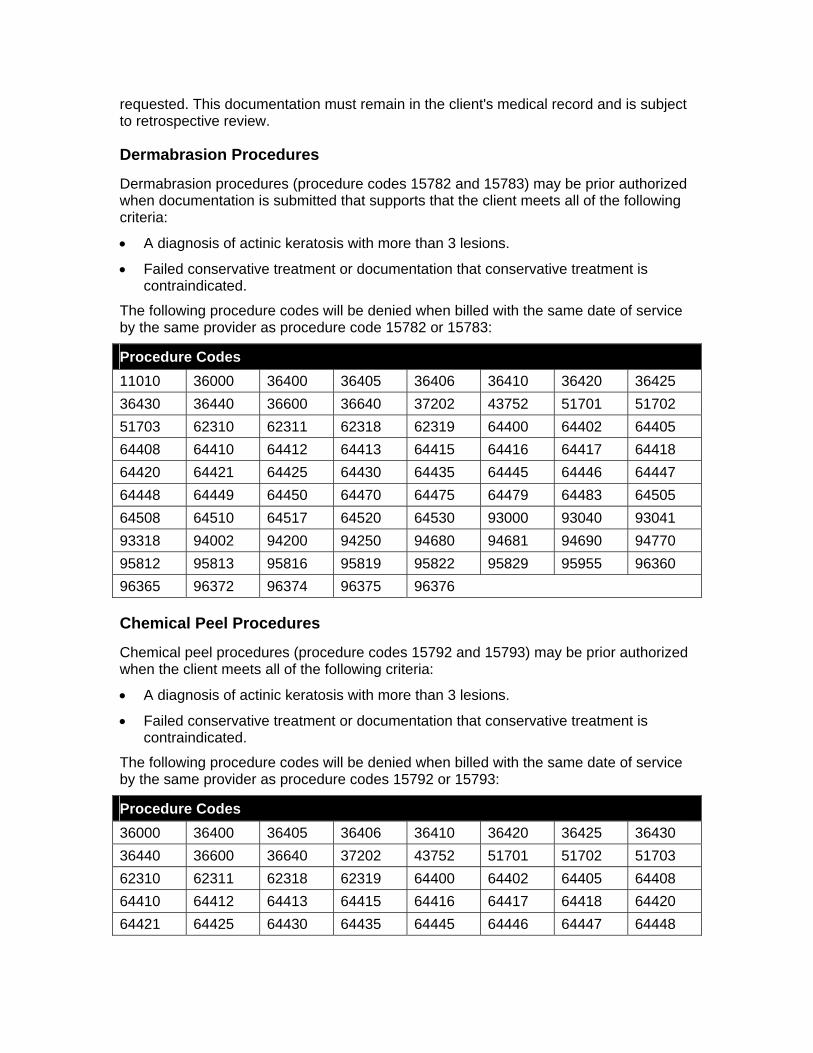
Dermabrasion Procedures
Dermabrasion procedures (procedure codes 15782 and 15783) may be prior authorized when documentation is submitted that supports that the client meets all of the following criteria:
• A diagnosis of actinic keratosis with more than 3 lesions.
• Failed conservative treatment or documentation that conservative treatment is contraindicated.
The following procedure codes will be denied when billed with the same date of service by the same provider as procedure code 15782 or 15783:
Procedure Codes 11010 36000 36400 36405 36406 36410 36420 36425 36430 36440 36600 36640 37202 43752 51701 51702 51703 62310 62311 62318 62319 64400 64402 64405 64408 64410 64412 64413 64415 64416 64417 64418 64420 64421 64425 64430 64435 64445 64446 64447 64448 64449 64450 64470 64475 64479 64483 64505 64508 64510 64517 64520 64530 93000 93040 93041 93318 94002 94200 94250 94680 94681 94690 94770 95812 95813 95816 95819 95822 95829 95955 96360 96365 96372 96374 96375 96376
Chemical Peel Procedures
Chemical peel procedures (procedure codes 15792 and 15793) may be prior authorized when the client meets all of the following criteria:
• A diagnosis of actinic keratosis with more than 3 lesions.
• Failed conservative treatment or documentation that conservative treatment is contraindicated.
The following procedure codes will be denied when billed with the same date of service by the same provider as procedure codes 15792 or 15793:
Procedure Codes 36000 36400 36405 36406 36410 36420 36425 36430 36440 36600 36640 37202 43752 51701 51702 51703 62310 62311 62318 62319 64400 64402 64405 64408 64410 64412 64413 64415 64416 64417 64418 64420 64421 64425 64430 64435 64445 64446 64447 64448
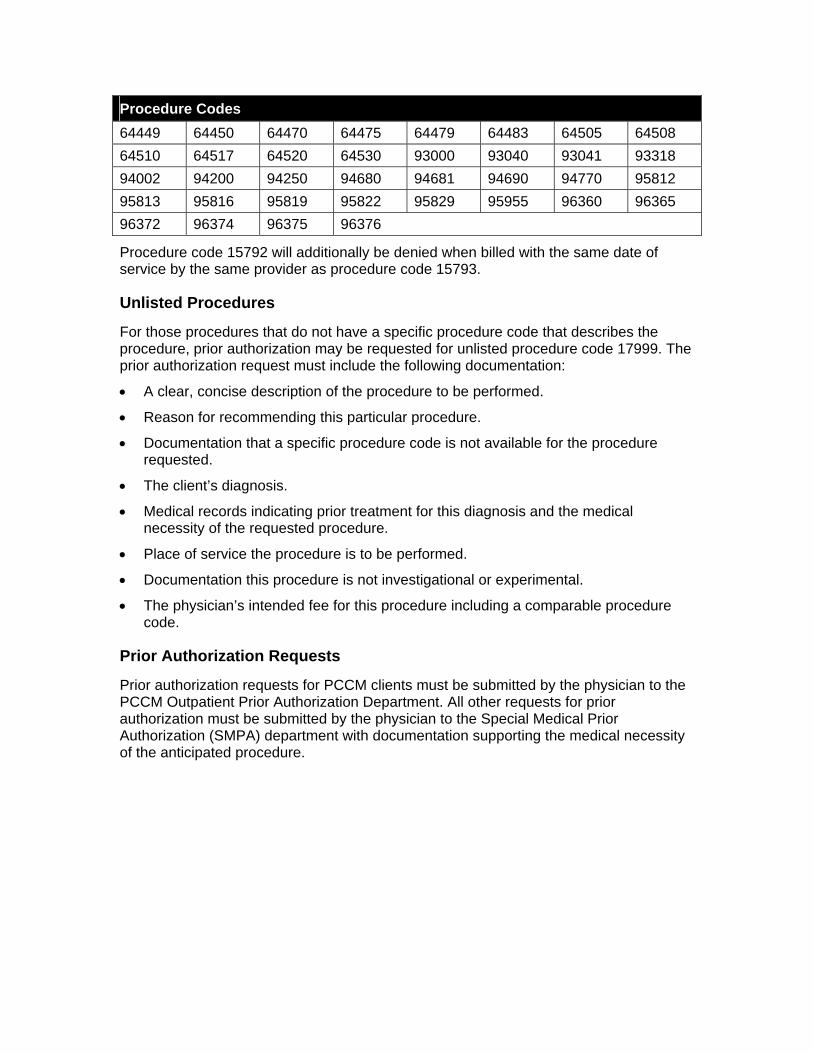
Procedure Codes 64449 64450 64470 64475 64479 64483 64505 64508 64510 64517 64520 64530 93000 93040 93041 93318 94002 94200 94250 94680 94681 94690 94770 95812 95813 95816 95819 95822 95829 95955 96360 96365 96372 96374 96375 96376
Procedure code 15792 will additionally be denied when billed with the same date of service by the same provider as procedure code 15793.
Unlisted Procedures
For those procedures that do not have a specific procedure code that describes the procedure, prior authorization may be requested for unlisted procedure code 17999. The prior authorization request must include the following documentation:
• A clear, concise description of the procedure to be performed.
• Reason for recommending this particular procedure.
• Documentation that a specific procedure code is not available for the procedure requested.
• The client’s diagnosis.
• Medical records indicating prior treatment for this diagnosis and the medical necessity of the requested procedure.
• Place of service the procedure is to be performed.
• Documentation this procedure is not investigational or experimental.
• The physician’s intended fee for this procedure including a comparable procedure code.
Prior Authorization Requests
Prior authorization requests for PCCM clients must be submitted by the physician to the PCCM Outpatient Prior Authorization Department. All other requests for prior authorization must be submitted by the physician to the Special Medical Prior Authorization (SMPA) department with documentation supporting the medical necessity of the anticipated procedure.
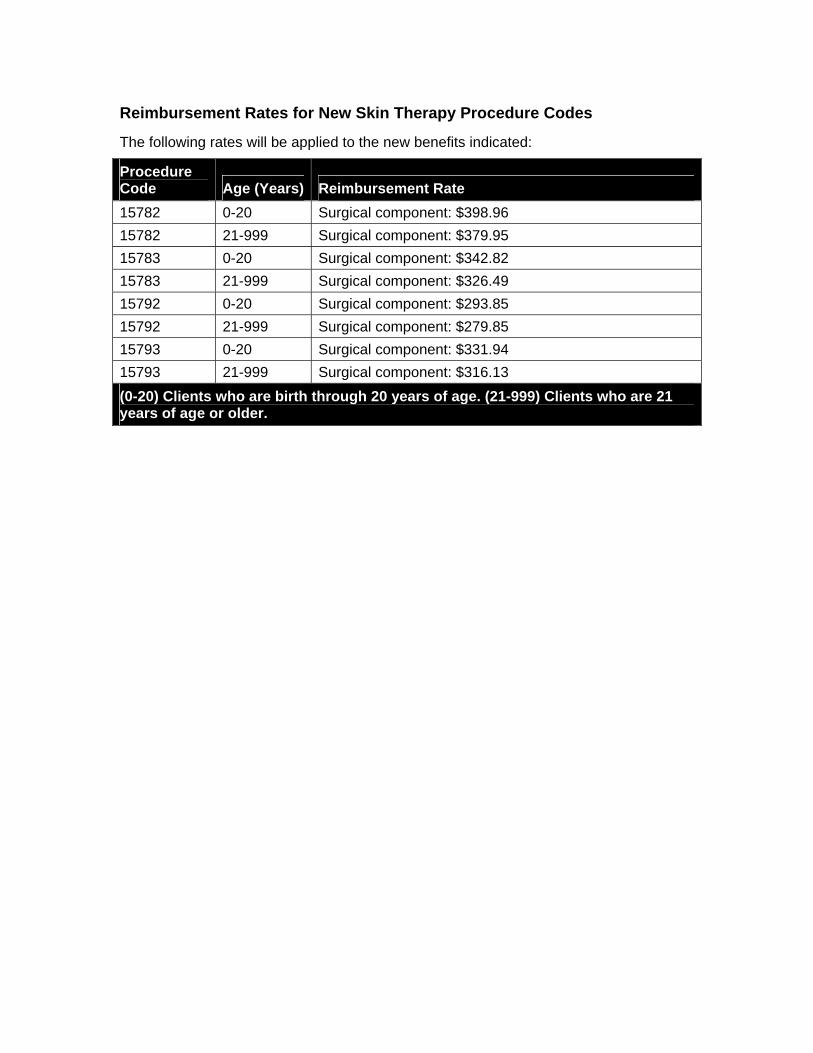
Reimbursement Rates for New Skin Therapy Procedure Codes
The following rates will be applied to the new benefits indicated:
Procedure Code Age (Years) Reimbursement Rate 15782 0-20 Surgical component: $398.96 15782 21-999 Surgical component: $379.95 15783 0-20 Surgical component: $342.82 15783 21-999 Surgical component: $326.49 15792 0-20 Surgical component: $293.85 15792 21-999 Surgical component: $279.85 15793 0-20 Surgical component: $331.94 15793 21-999 Surgical component: $316.13 (0-20) Clients who are birth through 20 years of age. (21-999) Clients who are 21 years of age or older.