Embed Size (px)
Citation preview

April 23, 2015
Mini-Lecture
Nathan King M.D.
Anticoagulation Reversal Part 2: UFH & LMWH

Objectives
Regarding UFH and LMWH:
• Explore mechanisms of action of anticoagulant drug and reversal agents
• Discuss indications for anticoagulation reversal
• Review methods of anticoagulant reversal

A 52 year old woman with is in the CCU for an NSTEMI. Cardiac catheterization did not reveal significant stenosis. While on a heparin drip she had an acute alteration in mental status and CT head revealed an intracranial hemorrhage with midline shift. Neurosurgery is preparing decompressive craniotomy.
What is the next most appropriate next step?
A. Treat with FFPB. Treat with Recombinant Factor VIIaC. Treat with Protamine SulfateD. Treat with Vitamin K1
Case Vignette #1

Case Vignette #2
A 67 year old woman with history of a right lower extremity DVT on 40mg BID Lovenox, presents with acute altered mental status after 3 days of watery diarrhea and one day of decreased urine output. She last received medications more than 12 hours ago. On exam, she is confused, mucous membranes are dry, and her left thigh is much larger than her right.
Labs 7 days ago: Hgb 9.3, BUN/Cr 12/1.1 Labs show now: Hgb 7.4, BUN/Cr 55/2.3CT now: new enlargement muscles in the medial left thigh compared
to prior CT
What is the most appropriate next step?A. Call Interventional Radiology, treat with IV NovoSevenB. Call Nephrology consult, place HD catheter for emergent dialysisC. Call ACS surgery consult, treat with IV Vitamin K1D. Call ACS surgery, treat with IV protamine

Mechanism of UFH and LMWH and Reversal
LMWH• Primarily acts on Xa• Longer Half-life (3-6 hrs)
Protamine• Reversal agent for Heparinoids
Heparinoids:• Potentiate Antitithrombin III (AT)
UFH (Unfractionated Heparin)• Half-life shorter (30-60 minutes)• Elevates PTT

Indications for anticoagulation reversal
Indication for emergent reversal: o Intracranial Hemorrhage o Need for emergent surgeryo Major bleeding
Minor Bleeding:o Supportive Measures / Monitoro Clinical Assessment
Reversal Appropriate for offending agent
o Consider activated charcoal or gastric lavage
Coagulopathy no active bleeding: o Supportive Measures / Monitor o Clinical Assessment
Suspected anticoagulant exposure in patient with bleeding or bleeding risk
Supportive Measures / Monitoring: • Support renal function with IVF and avoid nephrotoxins• Monitor CBC and coags at lease Q12 hours
Clinical Assessment:• anticoagulation exposure• possible medication interactions• laboratory assessment: CBC, renal function, LFTs, and
DIC screen
If not already done:o Supportive Measures / Monitoro Clinical Assessment
Reversal Indicated by: o Indication specific to clinical scenarioo Clinical JudgmentYes
No: o Continue Support
and Monitoring

UFH and LMWH Reversal
Protamine
Dosing• 25mg to 50mg boluses usually sufficient • Based on timing, dose, and route of heparinoid
to reverse
Reactions• Anaphylaxis can occur after previous exposure
Special considerations• Incompletely arrests anti-Xa activity of LMWH

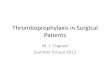
UFH ReversalKnown UFH exposure with clinically determined need for reversal:
Emergent reversal (ICH, emergent surgery, major bleeding)Other bleeding or risk of bleeding determined by clinical judgment to
be an indication
IF Intravenous UFH exposureSum TOTAL (T) UFH given in last 2.5 – 2 hoursDetermine time since UFH stopped Dose (D) Protamine using Table 1 and the
following equations: (T/100) x D = protamine dose
IF Subcutaneous UFH exposureCalculate dose: 1-1.5 mg protamine per 100 units
heparinInfuse slowly a portion of calculated dose (eg, 25-
50 mg) Remaining portion as continuous infusion over 8-
16 hours
Administer Protamine SulfateDose to neutralize estimated amount of active UFH
Time since UFH stopped (D) Protamine Dose to Neutralize 100 units of UFH
Immediate 1 – 1.5
30-60 minutes 0.5 – 0.75
>2 hours 0.25 – 0.375
Copyright 1978-2015 Lexicomp, Inc. All rights reserved.

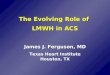
LMWH ReversalKnown LMWH exposure with clinically determined need for reversal:
Emergent reversal (ICH, emergent surgery, major bleeding)Other bleeding or risk of bleeding determined by clinical judgment to
be an indication
Last dose LMWH given ≤ 8 hours ago
Administer Protamine SulfateDose to neutralize estimated amount of active LMWH
Administer 1mg of protamine per 1mg enoxaperin
Elevation of PTT or continued bleeding at 2-4 hours post dosing
Last dose LMWH given > 8 hours ago
Administer 0.5mg of protamine per 1mg enoxaperin
Repeat Dosing
Copyright 1978-2015 Lexicomp, Inc. All rights reserved.

A 52 year old woman with is in the CCU for an NSTEMI. Cardiac catheterization did not reveal significant stenosis. While on a heparin drip she had an acute alteration in mental status and CT head revealed an intracranial hemorrhage with midline shift. Neurosurgery is preparing decompressive craniotomy.
What is the next most appropriate next step?
A. Treat with FFPB. Treat with Recombinant Factor VIIaC. Treat with Protamine SulfateD. Treat with Vitamin K1
Case Vignette #1

A 52 year old woman with is in the CCU for an NSTEMI. Cardiac catheterization did not reveal significant stenosis. While on a heparin drip she had an acute alteration in mental status and CT head revealed an intracranial hemorrhage with midline shift. Neurosurgery is preparing decompressive craniotomy.
What is the next most appropriate next step?
A. Treat with FFPB. Treat with Recombinant Factor VIIaC. Treat with Protamine SulfateD. Treat with Vitamin K1
Case Vignette #1

Case Vignette #2
A 67 year old woman with history of a right lower extremity DVT on 40mg BID Lovenox, presents with acute altered mental status after 3 days of watery diarrhea and one day of decreased urine output. She last received medications more than 12 hours ago. On exam, she is confused, mucous membranes are dry, and her left thigh is much larger than her right.
Labs 7 days ago: Hgb 9.3, BUN/Cr 12/1.1 Labs show now: Hgb 7.4, BUN/Cr 55/2.3CT now: new enlargement muscles in the medial left thigh compared
to prior CT
What is the most appropriate next step?A. Call Interventional Radiology, treat with IV NovoSevenB. Call Nephrology consult, place HD catheter for emergent dialysisC. Call ACS surgery consult, treat with IV Vitamin K1D. Call ACS surgery, treat with IV protamine

Case Vignette #2
A 67 year old woman with history of a right lower extremity DVT on 40mg BID Lovenox, presents with acute altered mental status after 3 days of watery diarrhea and one day of decreased urine output. She last received medications more than 12 hours ago. On exam, she is confused, mucous membranes are dry, and her left thigh is much larger than her right.
Labs 7 days ago: Hgb 9.3, BUN/Cr 12/1.1 Labs show now: Hgb 7.4, BUN/Cr 55/2.3CT now: new enlargement muscles in the medial left thigh compared
to prior CT
What is the most appropriate next step?A. Call Interventional Radiology, treat with IV NovoSevenB. Call Nephrology consult, place HD catheter for emergent dialysisC. Call ACS surgery consult, treat with IV Vitamin K1D. Call ACS surgery, treat with IV protamine

IF Suspected of bleeding or bleeding risk on UFH or LMWH:
Determine if emergent reversal needed: • ICH, emergent surgery, and major bleeding Initiate Supportive Measures and Clinical Assessment
Reverse with Protamine:• Incomplete arrest of LMWH• Protamine treatment guided by route, timing, and dosage
Summary