Embed Size (px)
DESCRIPTION
The Journal MSMA has a circulation of 5,000, which includes the membership of the Association and paid subscribers. The year 2012 represents the Journal’s 53rd year of continuous publication. The monthly scientific journal is the official publication of the Mississippi State Medical Association (MSMA), a physician organization serving as an advocate for its members, their patients and the public health. The association promotes ethical, educational and clinical standards for the medical profession and the enactment of just medical laws. Founded in 1856, the Mississippi State Medical Association provides a way for members of the medical profession to unite and act on matters affecting public health and the practice of medicine.
Citation preview
April 2012
VOL. LIII No. 4

April 2012 JOURNAL MSMA 101
“Pretty in Pink!”— Mimosas, also called silk trees, grace the landscape with fine green leaves and clusters of dainty pink flowers throughout the summer. Their fragrant flowers attract hummingbirds, bees, and butterflies. They also produce attractive brown pods. Because of its multi-part fern-like leaves and large pom-pom flowers it was introduced into the U.S. as an ornamental tree. However, the mimosa tree reproduces quickly and began to out-compete native species. As a result the mimosa tree has been declared as an invasive species in some states. Photo by Catherine H. (Cathy) Stroud, MD, a retired internist, avid photographer, and community volunteer, who resides in Madison County raising two teenagers with her husband, Larry. r
APRIL 2012 VOLUME 53 NUMBER 4
Journal of the Mississippi state Medical association (issn 0026-6396) is owned and published monthly by the Mississippi State Medical Association, founded 1856, located at 408 West Parkway Place, Ridgeland, Mississippi 39158-2548. (ISSN# 0026-6396 as mandated by section E211.10, Domestic Mail Manual). Periodicals postage paid at Jackson, MS and at additional mailing offices. correspondence: Journal MSMA, Managing editor, Karen a. evers, p.o. Box 2548, ridgeland, Ms 39158-2548, ph.: (601) 853-6733, fax: (601)853-6746, www.MsMaonline.com. suBscription rate: $83.00 per annum; $96.00 per annum for foreign subscriptions; $7.00 per copy, $10.00 per foreign copy, as available. advertising rates: furnished on request. cristen hemmins, hemmins hall, inc. advertising, p.o. Box 1112, oxford, Mississippi 38655, ph: (662) 236-1700, fax: (662) 236-7011, email: [email protected] postMaster: send address changes to Journal of the Mississippi State Medical Association, P.O. Box 2548, Ridgeland, MS 39158-2548. The views expressed in this publication reflect the opinions of the authors and do not necessarily state the opinions or policies of the Mississippi State Medical Association.
copyright© 2012 Mississippi state Medical association.
ME
DIC
AL ASS OCIAT
ION
MIS
SISSIPPI STAT
E
official publication of the MsMa since 1959
Lucius M. Lampton, MDEditor
D. Stanley Hartness, MDRichard D. deShazo, MD
AssociAtE Editors
Karen A. EversMAnAging Editor
PublicAtions coMMittEE
Dwalia S. South, MD chair
Philip T. Merideth, MD, JDMartin M. Pomphrey, MD
Leslie E. England, MD, Ex-OfficioMyron W. Lockey, MD, Ex-Officio
and the editors
thE AssociAtion
Thomas E. Joiner, MDpresident
Steven L. Demetropoulos, MDpresident-elect
J. Clay Hays, Jr., MDsecretary-treasurer
Lee Giffin, MD speaker
Geri Lee Weiland, MD vice speaker
Charmain Kanosky executive director
Scientific ArticleS
EXIT Procedure: A Report of the First Three Mississippi Cases 104Justin Brewer, MD; Kenneth W. Liechty, MD and James A. Bofill, MD
Just Off the Press- Info You Want to Know: Control in Patients 109with Type 2 Diabetes MellitusLucy Cadwallader, PharmD; Richard L. Ogletree, Jr, PharmD
Clinical Problem-Solving Case: Just A Simple Cerebral Vascular Accident? 111Thaibinh T. Phan, MD
PreSident’S PAge And Down the Stretch They Come 113Thomas E. Joiner, MD; MSMA President
relAted OrgAnizAtiOnS
Mississippi State Department of Health 110
editOriAlS
Mirror, Mirror 115D. Stanley Hartness, MD; Associate Editor
Bold Changes to the Norm 118Philip Merideth, MD, JD
A Look into Preconceived Ideas 123Elliott Browning
SPeciAlArticle
G. H. Tichenor, MD, and His Antiseptic Solution: 127The Tichenor in Dr. Tichenor’s - Part 2 of 2Michael C. Trotter, MD, FACS
dePArtmentS
MSMA Annual Session Registration 116MSMA Amendments to the MSMA Constitution and Bylaws 119Placement / Classified 125Letters 126Physician’s Bookshelf - Una Voce 132
ASclePiAd Ralph Lucius Brock, MD 136
AbOut the cOver:

102 JOURNAL MSMA April 2012
The practice of medicine is a difficult art, and our families provide us with essential healing, sustenance, and support. This month, our physician
portrait at the Journal’s end is of Dr. Ralph Brock, a brilliant physician who has been a leading proponent of organized medicine in the state. I can’t think of Ralph without thinking of his dear, late wife, Billie, whose ebullient and generous personality so warmed the lives of her family and friends. Billie’s father, a Magnolia pharmacist (who operated the legendary “Corner Drugstore” there), must have wanted a boy, says Ralph, because he nicknamed his daughter (whose full name was Wilma Louise Andrews) “Billie.” Ralph and Billie married at the end of his junior year of Tulane Medical School, and like so many physician’s wives, Billie was Ralph’s greatest supporter and the glue of his family and professional life. “I never heard her complain,” Ralph says of Billie, “not one time. We had a good time!”
The funniest story Billie told me was a memory of an MSMA annual session on the Coast long ago. Billie had gone shopping with some of her lady friends and left Ralph a note at the front desk of the Edgewater Gulf Hotel: “Ralph, find an appendectomy quick! I’ve gone shopping!” Billie remembered
that Ralph got $100 for performing an appendectomy, a princely sum for a physician in that day. Physicians must treasure our spouses and our families. We can’t fight our stressful battles without them.
The April Journal is filled with good stuff: three relevant scientific articles, part two of Dr. Trotter’s excellent article on Dr. Tichenor, three insightful editorials, Dr. Joiner’s President’s Page, and articles on the upcoming annual session (which should be one of the best yet!). As well, there’s a review of Dr. Dwalia South’s new book, “Una Voce,” one of the best books published in Mississippi this year. Dwalia has meant so much to our profession, and her wise reflections on the often delicate complexities of a small town medical practice are both inspiring and humorous.
The editors of the Journal encourage your letters to the editor, contributed editorials, poetry, and historical, scientific, and feature articles. This is your journal, and it is only as good as our members make it. My email is [email protected]. —Lucius “Luke” Lampton, MD, Editor
R. Scott Anderson, MD, FACR
Chair, Journal Editorial Advisory BoardJournal Editorial Advisory BoardJournal
Radiation Oncologist and Medical Director,
Anderson Regional Cancer Center, Meridian
Diane K. Beebe, MD
Professor and Chair,
Department of Family Medicine,
University of MS Medical Center, Jackson
Claude D. Brunson, MD
Senior Advisor to the Vice Chancellor
for External Affairs,
University of Mississippi Medical Center, Jackson
Jeffrey D. Carron, MD, FAAP, FACS
Associate Professor,
Department of Otolaryngology
& Communicative Sciences,
University of Mississippi Medical Center, Jackson
Gordon (Mike) Castleberry, MD
Urologist, Starkville Urology Clinic
Mary Currier, MD, MPH
State Health Officer
Mississippi State Department of Health, Jackson
Thomas E. Dobbs, MD, MPH
Health Officer, District VII/VIII
Mississippi State Department of Health, Hattiesburg
Sharon Douglas, MD
Chair, AMA Council on Ethical & Judicial Affairs
Professor of Medicine and Associate Dean for V A
Education, University of Mississippi School of Medicine,
Associate Chief of Staff for Education and Ethics,
G.V. Montgomery VA Medical Center, Jackson
Daniel P. Edney, MD
Executive Committee Member,
National Disaster Life Support Education Consortium,
Internist
The Street Clinic, Vicksburg
Owen B. Evans, MD
Professor of Pediatrics and Neurology
University of Mississippi Medical Center, Jackson
Maxie L. Gordon, MD
Assistant Professor, Department of Psychiatry and
Human Behavior, Director of the Adult Inpatient
Psychiatry Unit and Medical Student Education,
University of Mississippi Medical Center, Jackson
Scott Hambleton, MD
Medical Director
Mississippi Professionals Health Program, Ridgeland
John Edward Hill, MD, FAAFP
Residency Program Director
North Mississippi Medical Center, Tupelo
John D. Isaacs, Jr., MD
Infertility Specialist,
Mississippi Fertility Institute
at Women’s Specialty Center, Jackson
Kent A Kirchner, MD
Chief of Staff
G.V. Montgomery VA Medical Center, Jackson
Brett C. Lampton, MD
Internist/Hospitalist
Baptist Memorial Hospital, Oxford
Philip L. Levin, MD
President, Gulf Coast Writers Association
Emergency Medicine Physician, Gulfport
William Lineaweaver, MD, FACS
Editor, Annals of Plastic Surgery
Medical Director
JMS Burn and Reconstruction Center, Brandon
John F. Lucas,III, MD
Surgeon
Greenwood Leflore Hospital
Gailen D. Marshall, Jr., MD, PhD, FACP
Professor of Medicine and Pediatrics,
Vice Chair for Research,
Director, Division of Clinical Immunology and Allergy,
Chief, Laboratory of Behavioral Immunology Research
The University of Mississippi Medical Center, Jackson
Alan R. Moore, MD
Clinical Neurophysiologist
Muscle and Nerve, Jackson
Paul “Hal” Moore Jr., MD, FACR
Radiologist
Singing River Radiology Group, Pascagoula
Jason G. Murphy, MD
Surgeon
Surgical Clinic Associates, Jackson
Ann Myers, MD
Rheumatologist
Mississippi Arthritis Clinic, Jackson
Jimmy L. Stewart, Jr., MD
Program Director, Combined Internal Medicine/
Pediatrics Residency Program,
Associate Professor of Medicine and Pediatrics
University of Mississippi Medical Center, Jackson
Samuel Calvin Thigpen, MD
Hematology-Oncology Fellow, Department of Medicine
University of Mississippi Medical Center, Jackson
Thad F. Waites, MD, FACC
Clinical Cardiologist, Hattiesburg Clinic
Chris E. Wiggins, MD
Orthopaedic Surgeon
Bienville Orthopaedic Specialists, Pascagoula
John E. Wilkaitis, MD, MBA, CPE, MS
Chief Medical Officer Chief Medical Officer Chief Medical Officer
Brentwood Behavioral Healthcare, Flowood
Journal editorial advisory Board
Lucius M. Lampton, MD
Editor
From the Editor
April 2012 JOURNAL MSMA 103
Medical Assurance Company of Mississippi
For the physicians of Biloxi Internal Medicine, Medical Assurance Company of Mississippi is not just their insurance company, but also a member of the team. MACM’s Risk Management Department is invited into the clinic for risk assessments and staff presentations on a regular basis. The physicians want to keep their focus on providing professional care and seek out MACM’s assistance to do just that.
Having MACM available to them and to their office staff is just one of the benefits they realize as insureds. With MACM’s help and advice, they can improve on what they already love to do.
For over 30 years, Mississippi physicians have looked to Medical Assurance Company of Mississippi for their professional liability needs. Today, MACM is an integral part of the health care community through its dedication to risk management services for our insureds.
A dedicated staff and physician involvement at every level guarantees that the interests of our policyholders remain the top priority. This, combined with the many years of loyalty and support from our insureds, is what allows us to be the carrier of choice in Mississippi.
Please call on us to assist with your professional liability needs.
1.800.325.4172 • www.macm.net
Partnership keeps physicians focused on medicine
Left to Right: Regina C. Mills, MDReza Motakhaveri, MDYashashree Bethala, MDBen W. Cheney, MDMarion J. Wainwright, MD
104 JOURNAL MSMA April 2012
• Scientific ArticleS •
EXIT Procedure: A Report of the First Three Mississippi Cases
The University of Mississippi Medical Center has initi-ated a state-of-the-art Fetal Center. This project involves col-laboration between multiple disciplines including anesthesi-ology, pediatric surgery, maternal-fetal medicine, radiology, neonatology, genetics, pediatric cardiology and other pediatric subspecialties, nursing, and social work. Complicated fetal pa-tients from throughout the southeastern USA may be referred to this center and benefit from new and innovative interven-tions that have not been available to this region in the past. The first three EXIT (Ex-Utero Intrapartum Treatment) proce-dures were recently performed at Batson Children’s Hospital at the University of Mississippi Medical Center. Our objec-tive is to share our recent experiences with this novel proce-dure and to detail some of the basics of an EXIT delivery.
Keywords: EXIT procEdurE, AIrwAy obsTrucTIon, EcMo
Case 1The patient was a primigravid 39-year-old who was re-
ferred to the Fetal Center at 31 weeks and 4 days of gestation after a large fetal neck mass was detected by routine ultrasound. The patient’s pregnancy had been uncomplicated until presentation
and previous ultrasound exams had revealed no abnormalities. Targeted ultrasonography in the Fetal Center revealed a male fetus with a large neck mass which extended medially from the right mandibular angle and measured 6.2 x 5.0 x 4.8 cm. The mass exhibited both cystic and solid areas and had the typical ap-pearance of a teratoma. There was no evidence of fetal hydrops or evidence of occlusion of the fetal esophagus, trachea or neck vessels. Appropriate fetal swallowing was suggested by the vi-sualization of a normal fetal stomach and the lack of hydram-nios. A thorough examination revealed no other fetal structural malformations. Cervical teratoma was placed at the top of the differential diagnosis, and the plan was made to perform twice weekly fetal testing using the biophysical profile and Doppler studies. Ultrasonography would also be used to monitor for any signs of obstruction of the fetal esophagus and airway by this growing lesion. A fetal magnetic resonance imaging study was ordered which confirmed the ultrasound findings. Fetal echocar-diography, including combined ventricular output, was normal.
Ultrasound surveillance and fetal testing continued over the next six weeks. The presumed fetal cervical tera-toma continued to enlarge until it reached the size of 8 x 6 x 6 cm. The patient gradually developed hydramnios with a four-quadrant amniotic fluid index that reached 35 cm. The hydramnios was attributed to decreased fetal swallowing of amniotic fluid even though the fetal stomach still contained some fluid. Tracheal obstruction was implied by mild flat-tening of the domes of the fetal diaphragm and the inabil-ity to clearly visualize the tracheal lumen by ultrasound. At this point it was considered that this fetal neck mass would clearly pose difficulty in establishing a safe airway at deliv-ery. Plans were then made to perform the EXIT procedure.
Because the patient was considered to be at high risk for labor secondary to hydramnios, the decision was made to
Abstract
Author AffiliAtionS: Department of Obstetrics and Gynecology, Division of Maternal-Fetal Medicine, University Center for Fetal Medicine (Dr. Brewer and Dr. Bofill); Divisions of Maternal-Fetal Medicine and Pediatric Surgery (Dr. Liechty); University of Mississippi Medical Center, Jackson.
correSponding Author: Justin Brewer, MD, University Center for Fetal Medicine, University of Mississippi Medical Center, 2500 North State Street, Jackson, MS 39216-4505, ([email protected]), (601)668-9431.
Justin Brewer, MD; Kenneth W. Liechty, MD and James A. Bofill, MD

April 2012 JOURNAL MSMA 105
proceed with delivery at 37 weeks gestation. The patient was hospitalized at 37 weeks and met with the delivery team for a final round of counseling. The delivery team consisted of physicians from Anesthesia, Maternal-Fetal Medicine, and Pediatric Surgery. The following day the patient was taken to the Batson Children’s Hospital where she underwent her EXIT procedure. This began with ultrasonography to again map the placenta and plan the uterine incision. A pre-operative amnio-reduction of 900ml of amniotic fluid was performed to allow better visualization of the placental edge, to simplify deliv-ery, and to decrease the chances of a placental abruption. The maternal abdomen and uterus were then opened in the typi-cal fashion for an EXIT procedure. The fetal head, arms, and shoulders were delivered through the uterine incision with the fetal trunk, abdomen, and lower extremities remaining within the uterus to preserve uterine volume. The fetus continued gas exchange through the placenta while the cervical mass was di-rectly examined. Direct laryngoscopy demonstrated that this mass was impinging and occluding the trachea making direct intubation impossible. Using fiberoptic laryngoscopy and bron-choscopy, the pediatric ENT specialist was able to pass and se-cure a guarded endotracheal tube. Ventilation of the fetus was then directly observed and confirmed using pulse oximetry.
The figure shows an intraoperative photograph during the EXIT procedure. The giant neck mass is seen, and an endotracheal tube has been placed. The fetus is undergoing echocardiography.
With the airway established, the remainder of the fetus was delivered, the umbilical cord clamped, and the infant taken to an adjacent operating room for resection of the cervical mass. The fetus was on “placental bypass” for 39 minutes. The neonate had umbilical artery/venous catheters placed, and the neck mass was completely excised. The resection was uncomplicated, and the newborn was transferred to the PICU in stable condition. The mother’s uterus and abdomen were closed in standard fash-
ion, and her post-operative course was uncomplicated. She was discharged home on post-operative day #3. The neonate also did very well and was able to be extubated in the immediate post-op-erative period. He was initiated on oral feedings and was able to be discharged home on post-operative day #11. Final pathology on the fetal neck mass returned as a mature cervical teratoma.
case 2The patient was a primigravid 20-year-old who was re-
ferred to the Fetal Center at a gestational age of 37 weeks and 1 day. While two ultrasound studies earlier in pregnancy had dem-onstrated no fetal anomalies, a late study ordered to estimate the rate of fetal growth noted a significant fetal oral mass. The patient’s past medical history was benign, and her pregnancy had been entirely uncomplicated to this point. Targeted ultra-sonography in the Fetal Center noted a female fetus with a 3 x 2.5 x 2.8 cm mass that appeared to extend from the lips inward and fill the oral cavity. The mass appeared to demonstrate both solid and cystic components and did not appear to be attached to the fetal tongue. The amniotic fluid index was within normal limits, and the fetal stomach was noted to be normally filled suggesting that the mass had not yet fully impaired fetal swal-lowing. No other fetal structural malformations were noted, and the fetus was appropriately developed for gestational age. A magnetic resonance study considered that this mass probably represented macroglossia or an oropharyngeal teratoma. By ultrasound criteria the differential diagnosis for this oral mass included a teratoma (epignathus), an epulis, or a lingual thyroid. There was concern that this mass could produce significant air-way compromise at the time of delivery. After lengthy counsel-ing and discussion with the patient and family the decision was made to deliver via an EXIT procedure. As with the first pa-tient, fetal surveillance included twice weekly biophysical pro-files with close attention paid to signs of developing obstruc-tion by the oral mass. For the last two weeks of the pregnancy the patient relocated to Jackson to be nearby in case of labor.
The patient was admitted at 39 weeks gestation and subsequently underwent an uncomplicated EXIT procedure in the Batson Children’s Hospital. Following delivery of the fetal head and chest, the oral mass was noted to be arising from the maxillary alveolar ridge and obstructing the oral cav-ity. Direct laryngoscopy was not possible due to obstruction of the view of the airway by the mass. Fiber optic rigid la-ryngoscopy and bronchoscopy were then used to secure the airway. After the establishment of a safe airway, the umbili-cal cord was then doubly clamped and cut and the infant fully delivered. The “placental bypass” time was approximately 30 minutes. The anesthetized infant was transferred to an adjoin-ing operating room where the oral mass was excised without any complications. The mother’s uterus and abdomen were closed in the typical manner, and the procedure was complet-ed. The post-operative course was uneventful and the patient
Figure. EXIT procedure showing giant neck mass with
endotracheal tube placed while the fetus is undergoing
echocardiography
• Scientific Article •
106 JOURNAL MSMA April 2012
A Summit on Prescription Drug Abuse in Mississippi
Wednesday, July 18, 20128:00 a.m. - 5:00 p.m.
Mississippi Trade Mart Building, West Wing, Jackson
SPONSORED BY:U.S. Attorney’s Office, Southern & Northern Districts of Mississippi
NOTIFICATION WILL BE SENT WHEN REGISTRATION OPENS
CO-SPONSORED BY:DREAM of JacksonDrug Enforcement AdministrationGulf Coast HIDTAOffice of National Drug Control PolicyMississippi Academy of Physician AssistantsMississippi Bureau of NarcoticsMississippi Department of Mental Health
Mark Your Calendar
Mississippi Department of Public SafetyMississippi State Medical AssociationMississippi Nurses AssociationMississippi Pharmacists AssociationMississippi Independent Pharmacies AssociationMississippi Dental AssociationPine Grove Behavioral Health and Addiction ServicesSt. Dominic Hospital
22years1989-2011
MEDLEY & BROWN, LLCF I N A N C I A L A D V I S O R S
www.medleybrown.com
PERFORMANCE It is one of the most important things to consider when selecting an investment advisor. Our past performance can be seen on our website...right now.
601-982-4123
M&B Perf MSMA Feb'12.indd 1 1/31/12 12:06 PM
was discharged home on post-operative day #4. The infant was monitored in the NICU where she likewise had an un-eventful post-operative course and was able to be discharged home the same day as her mother. Final pathology on the oral mass returned as a congenital gingival granular cell tu-mor. This is a rare tumor, typically seen only in newborns and interestingly has a marked female preponderance of 8:1.
case 3The patient was a 29-year-old gravid 3 para 0 who was
referred to the Fetal Center at a gestational age of 33 weeks for concerns of mandibular hypoplasia. The patient’s past medi-cal history was remarkable for mitral valve prolapse, MTHFR mutation, and 2 prior miscarriages. Her pregnancy had been entirely uncomplicated to this point. Targeted ultrasonography in the Fetal Center noted a male fetus with severe mandibular hypoplasia. In addition, there were abnormal thumbs. The am-niotic fluid index was elevated at 33 cm. No other fetal structur-al malformations were noted, and the fetus was appropriately developed for gestational age. A magnetic resonance study con-firmed severe micrognathia. The fetal karyotype was normal. There was concern that there could be significant airway com-promise at the time of delivery. After lengthy counseling and discussion with the patient and family, the decision was made to deliver via an EXIT procedure. As with the first two patients, fetal surveillance included twice weekly biophysical profiles.

April 2012 JOURNAL MSMA 107
The patient was admitted at 37 weeks gestation and sub-sequently underwent an EXIT procedure in the Batson Chil-dren’s Hospital. At the time of the EXIT procedure, the airway was unable to be visualized due to the severe micrognathia ne-cessitating the creation of a surgical airway, or tracheostomy. After the establishment of a safe airway the umbilical cord was then doubly clamped and cut and the infant fully delivered. The “placental bypass” time was approximately 29 minutes. The anesthetized infant was transferred to an adjoining operating room, stabilized, and then transferred to the NICU. The moth-er’s uterus and abdomen were closed in the typical manner, and the procedure was completed. The mother’s post-operative course was uneventful, and the mom was discharged home on post-operative day #4. The infant was monitored in the NICU, and consultation was obtained with genetics, orthopedic sur-gery, pediatric plastic surgery, and the oromaxillofacial service for planning of subsequent reconstructive procedures. During the genetics evaluation the infant was diagnosed with Nager syndrome given the constellation of mandibular hypoplasia and radial anomalies. The infant was weaned off ventilator sup-port to humidified trach collar. The tracheostomy was changed on hospital day #7. On hospital day #18 a surgical gastros-tomy was performed to obtain long-term enteral access. Once weight gain was established and tracheostomy teaching per-formed, the infant was discharged home on hospital day #42.
discussion
The Ex-Utero Intrapartum Treatment or EXIT proce-dure was first described as a means to reverse tracheal oc-clusion in fetuses that had been treated for severe congenital diaphragmatic hernia. As experience with this procedure has increased, the indications for its use have been expanded to in-clude other cases where the airway is a concern or resuscita-tion may be compromised. The guiding principles of the pro-cedure are to maintain a controlled state of uterine hypotonia and uterine volume to maintain uteroplacental circulation and gas exchange while various fetal interventions are performed. Currently the indications for an EXIT procedure include any anatomic process which would endanger the establishment of a proper neonatal airway at the time of delivery. The typical anatomic issues are large fetal neck masses, mediastinal mass-es, and congenital high airway obstruction syndrome (CHA-OS) including severe micrognathia. The EXIT procedure has also seen utility in cases when resuscitation of the fetus may be compromised. This includes large thoracic or mediasti-nal masses or when the fetus may require immediate ECMO (Extra Corporeal Membrane Oxygenation). In these cases the “placental bypass” time is used to resect the mass or to place the ECMO cannulas so that the fetus/infant is not exposed to prolonged episodes of hypoxia and extended resuscitation.
The EXIT procedure involves the simultaneous treatment of two patients, mother and fetus/infant, and a comprehensive team approach is necessary to maximize outcome and safety.
The team will usually include pediatric surgery, maternal-fetal medicine, two anesthesiologists (one for mother; one for fetus/infant), pediatric otolaryngology, and a host of nursing and op-erative support staff. An EXIT procedure is much more than an elaborate Cesarean delivery. The procedure typically begins by obtaining a deep level of maternal general anesthesia us-ing halogenated inhalational agents. This profound anesthesia is required for the maintenance of uterine relaxation during the procedure. A uterus that contracts will interrupt uteroplacental blood flow impairing gas exchange and will likely shear the placenta from its implantation site. Ultrasound is performed to carefully locate the placenta and to plan the uterine incision. The choice of skin incision is based largely on the proposed site of the hysterotomy incision. The maternal abdominal inci-sion is usually significantly larger than the usual Pfannenstiel, and the maternal abdominal rectus muscles are also divided so as to allow room for the surgeons to operate on the fetus after partial delivery. A vertical midline skin incision is sometimes required in those cases where the placenta implants over near-ly the entire anterior aspect of the uterus and a posterior hys-terotomy is required. Intraoperative ultrasound may be used prior to the entering the uterus to be certain that the incision will not compromise the placenta. The uterus is entered in a nearly bloodless manner using electrocautery, and the uterine incision is extended using specialized stapling devices which fire a double-row of staples and divide the uterus controlling the membranes while providing hemostasis at the edges of the hysterotomy. It is important to maintain intrauterine volume to decrease the risk of both placental abruption and umbili-cal cord compression so a warmed lactated Ringer’s solution is continuously infused to maintain uterine volume. The fetus is then partially delivered to the level of mid-chest so that the head and both of the fetal arms are beyond the hysterotomy. A pulse oximetry probe is attached to one hand while intra-venous access is secured in the other hand. The fetus is com-pletely anesthetized and, at this point, is still being oxygen-ated through the placental circulation. Continuous monitoring of fetal cardiac status is important and is performed using an intraoperative sterile ultrasound probe which allows real-time echocardiography with particular attention being given to ven-tricular filling. The surgeons then perform whatever maneuvers or procedures are required. When all planned interventions are complete and an airway has been secured, the infant is de-livered and the umbilical cord is clamped and divided. The time from the partial delivery of the fetus/infant through the hysterotomy incision until the umbilical cord is clamped and divided and the delivery completed is considered the “placental bypass” time. The infant is then passed off the operative field. Intravenous oxytocin is then administered, and the inhalational anesthetic agents are decreased to allow the uterus to begin to contract and lessen maternal blood loss. There is a significant risk for maternal uterine hemorrhage if the uterus has not re-gained appropriate tone prior to the delivery of the placenta,
108 JOURNAL MSMA April 2012
requiring extensive communication between surgeons and anesthesiology. The hysterotomy incision is then closed in a running fashion while the maternal abdomen is then closed in layers and the mother is extubated at the appropriate time.
The successful completion of the first three EXIT procedures in the State of Mississippi ushers in an excit-ing time. Our hope is that the Fetal Center will allow pa-tients from our State and the surrounding region to have ready access to new and innovative interventions which have not typically been available without long-distance travel.
acKnowledgements
Physicians and Staff (listed by Department) who contribute to the University Center for Fetal Medicine include the following:Fetal Center Coordinator: Billie J. Mize, RN; Anesthesia: Arthur Calimaran, MD, Michelle Sheth, MD, Stanley Musick, MD; Neonatology: Mary Anne Kosek, MD., Umotola Famuyide, M.D; Palliative Care: Rick Boyte, MD, Jackie Carillo, RNP; Genetics: Omar Abdulrahman, MD, Christhopher Friedrich, MD, Holly Zimmerman, CGC; Maternal-Fetal Medicine: James Bofill, MD, Michelle Owens, MD; Pediatric/
Fetal Surgery: Kenneth Liechty, MD, Christopher Blewett, MD, David Sawaya, MD, Barry Berch, MD; Pediatric Cardiology: Jennifer Shores, MD, Makrum Ebeid, MD, Charlie Gaymes, MD; Pediatric Cardiothoracic Surgery: Jorge Salazar, MD; Pediatric Urology: Ed Harmon, MD; Radiology (MRI): Majid Khan, MD, Manohar Roda, MD.
references:
1. Jones, KL. Smith’s Recognizable Patterns of Human Malformation. Sixth Edition. Elsevier Saunders. Philadelphia, PA. 2006:288-289.
2. Mychaliska GB, Bealer JF, Graf JL, et al. Operating on placental support: The ex-utero intrapartum treatment procedure. J Pediatr Surg. 1997; 32:227-30.
3. Liechty KL, Crombleholme TM, Flake AW, et al. Intrapartum airway management for giant fetal neck masses: the EXIT (ex-utero intrapartum treatment) procedure. Am J Obstet Gynecol. 1997; 177:870.
4. Hirose S, Sydorak RM, Tsao K, et al. Spectrum of intrapartum management strategies for giant fetal cervical teratoma. J Pediatr Surg. 2003; 38:446.
5. Bouchard S, Johnson MP, Flake AW, et al. The EXIT procedure: Experience and outcome in 31 cases. J Pediatr Surg 2002; 37:418.
6. Kunisaki SM, Fauza DO, Barnewolt CE, et al. Ex-utero intrapartum treatment with placement on extracorporeal membrane oxygenation for fetal thoracic masses. J Pediatr Surg. 2007; 42:420.
TAX FREE Retirement For Physicians
For More Information on How to Generate a Tax Free Income
Contact Sean Patin Vice President of
L.D. O’Mire Financial Services 406 Orchard Park #2 Ridgeland, MS 39157
1.800.844.3254
BRANDON BYRAM CANTON CLINTON JACKSON LAURELMADISON PEARL RICHLAND RIDGELAND SPILLWAY VICKSBURG
April 2012 JOURNAL MSMA 109
Article: Buehler AM, Cavalcanti AB, Berwanger O, et al. Effect of tight blood glucose control versus conventional control in patients with type 2 diabetes
mellitus: a systematic review with meta-analysis of randomized controlled trials. Cardiovascular Therapeutics; 2011: doi: 10.1111/j.1755-5922.2011.00308.x. [Epub ahead of print]Background: Diabetes complications, both microvascular and macrovascular, are important causes of morbidity and mortality worldwide. Tight blood glucose control (HbA1C <6.5%) has been associated with decreased microvascular complications; however, evidence regarding cardiovascular events is conflicting.
Objective: To examine the effects of tight versus conventional glucose control on total mortality, cardiovascular and microvas-cular events, and hypoglycemia in patients with type 2 diabetes.
Design: Systematic review with meta-analysis of randomized controlled trials.
Methods: MEDLINE, Cochrane library, EMBASE and ISI Web of Knowledge were searched from 1966 to 2011. Inclusion crite-ria consisted of randomized controlled trials that enrolled patients > 18 years of age with diabetes. In addition, the trial should have randomized patients to at least two treatment arms with different blood glucose targets. The minimal follow-up was 12 months. Two independent reviewers extracted data from eligible studies.
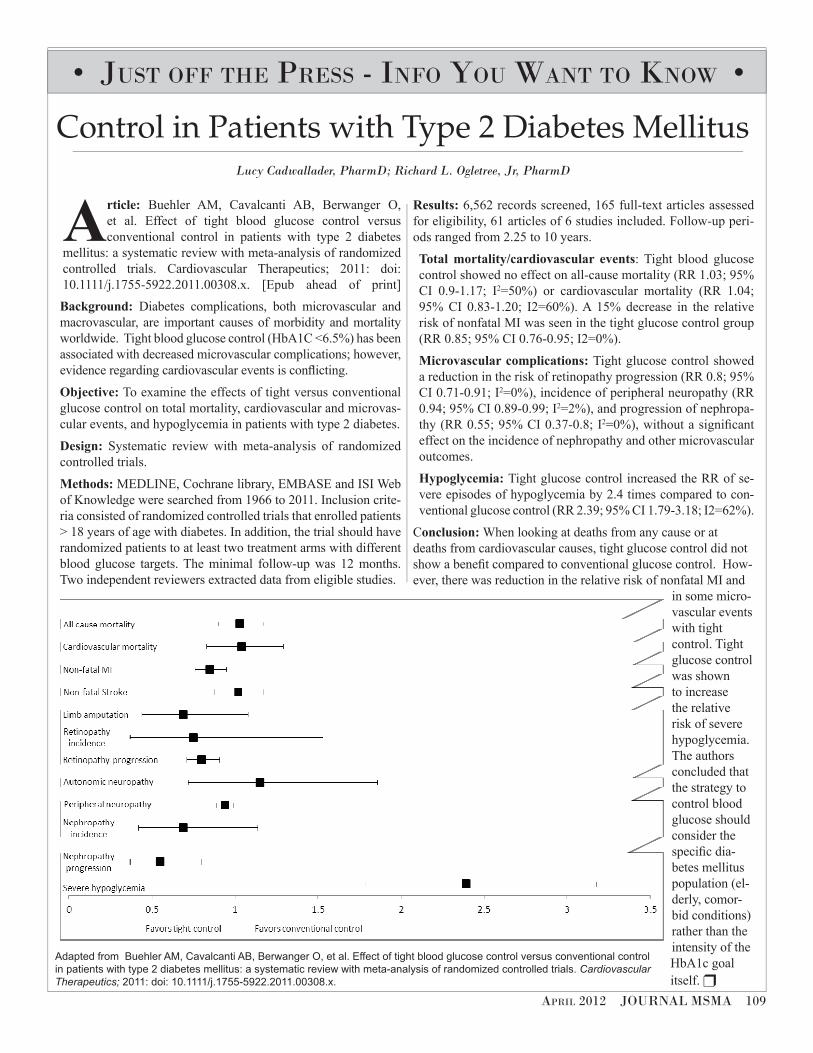
Results: 6,562 records screened, 165 full-text articles assessed for eligibility, 61 articles of 6 studies included. Follow-up peri-ods ranged from 2.25 to 10 years.
Total mortality/cardiovascular events: Tight blood glucose control showed no effect on all-cause mortality (RR 1.03; 95% CI 0.9-1.17; I2=50%) or cardiovascular mortality (RR 1.04; 95% CI 0.83-1.20; I2=60%). A 15% decrease in the relative risk of nonfatal MI was seen in the tight glucose control group (RR 0.85; 95% CI 0.76-0.95; I2=0%).
Microvascular complications: Tight glucose control showed a reduction in the risk of retinopathy progression (RR 0.8; 95% CI 0.71-0.91; I2=0%), incidence of peripheral neuropathy (RR 0.94; 95% CI 0.89-0.99; I2=2%), and progression of nephropa-thy (RR 0.55; 95% CI 0.37-0.8; I2=0%), without a significant effect on the incidence of nephropathy and other microvascular outcomes.
Hypoglycemia: Tight glucose control increased the RR of se-vere episodes of hypoglycemia by 2.4 times compared to con-ventional glucose control (RR 2.39; 95% CI 1.79-3.18; I2=62%).
Conclusion: When looking at deaths from any cause or at deaths from cardiovascular causes, tight glucose control did not show a benefit compared to conventional glucose control. How-ever, there was reduction in the relative risk of nonfatal MI and
in some micro-vascular events with tight control. Tight glucose control was shown to increase the relative risk of severe hypoglycemia. The authors concluded that the strategy to control blood glucose should consider the specific dia-betes mellitus population (el-derly, comor-bid conditions) rather than the intensity of the HbA1c goal itself. r
Control in Patients with Type 2 Diabetes Mellitus Lucy Cadwallader, PharmD; Richard L. Ogletree, Jr, PharmD
• JuSt off the preSS - info You WAnt to KnoW •
Adapted from Buehler AM, Cavalcanti AB, Berwanger O, et al. Effect of tight blood glucose control versus conventional control
in patients with type 2 diabetes mellitus: a systematic review with meta-analysis of randomized controlled trials. Cardiovascular
Therapeutics; 2011: doi: 10.1111/j.1755-5922.2011.00308.x.
110 JOURNAL MSMA April 2012
• MSdh •
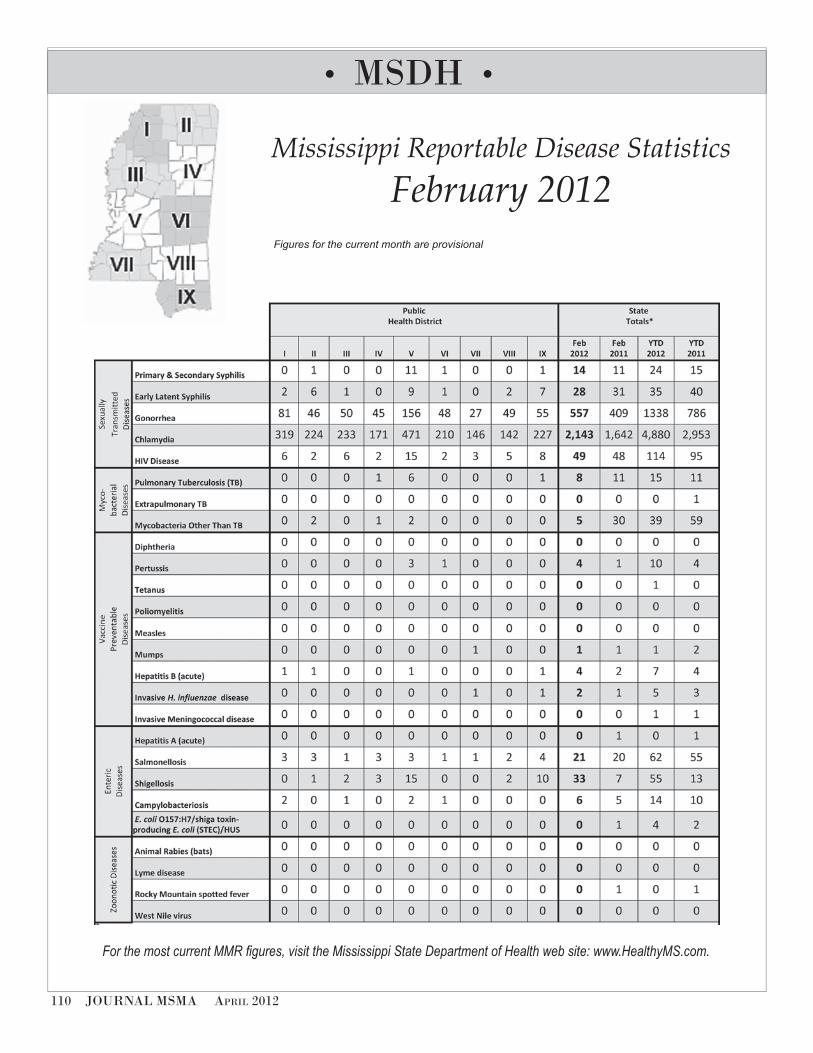
Mississippi Reportable Disease Statistics
February 2012Figures for the current month are provisional
For the most current MMR figures, visit the Mississippi State Department of Health web site: www.HealthyMS.com.
April 2012 JOURNAL MSMA 111
A 52-year-old African American female presented to clinic with a 1-day history of left-sided weakness, mild dysphasia and two
episodes of left-sided mouth twitching. The patient also complained of a worsening pressure headache for 3 months with some relief provided by acetaminophen (Tylenol) and ibuprofen (Motrin). The headache persisted throughout the day with associated nausea but not vomiting. She also complained of weakness, poor appetite, and weight loss of 5 to 10 pounds during the previous 4 months. She reported dull, chronic intermittent abdominal pain lasting more than 3 months without significant change in bowel movements.
With her presentation of left-sided weakness and dys-phasia, my first thought is a cerebral vascular accident (CVA). Her complaint of resolved mouth twitching suggests possible underlying abnormal neurological activity. Post-stroke seizure is one of the most common medical complications of CVA.¹ Her chronic headache, weakness, weight loss, and abdominal pain can be related to her clinical presentation. A more thor-ough medical history will help us investigate the cause of her symptoms.
The patient’s past medical history included type II diabetes mellitus, hypertension, anemia, arthritis, and hy-percholesterolemia. She denied any seizure history. The pa-tient reported smoking less than one-half pack per day for 30 years. Her medications included glipizide (Glucotrol), metformin (Glucophage), hydrochlorothiazide (Microzide), amlodipine (Norvasc), quinapril (Accupril), and atorvas-tatin (Lipitor).
Diabetes, hypertension, hypercholesterolemia, and smok-ing are risk factors for developing arteriosclerosis, which is a major cause of CVA. She also has symptoms that are not associ-ated with CVA including chronic fatigue, anemia, and abdomi-nal pain. We will focus our investigation on a possible CVA.
The patient had presented to an emergency room (ER) 2 days prior to this visit with a complaint of feeling weak and tired. A urinalysis (UA) showed proteinuria of 70 mg/dL, hematuria with RBC of 31/HPF (high-power field) and urine WBC of 7/HPF. There were no urine bacteria, and leukocytes, nitrites, and serum electrolytes were nor-mal. Complete blood count showed hemoglobin of 10.0 gm/dL and hematocrit of 30.6%. (One year ago her hemoglobin and hematocrit were 11.6 gm/dL and 35.5%, respectively.) The patient was diagnosed with anemia and urinary tract infection. She was discharged from the ER with prescrip-tions for an iron supplement and an antibiotic and was scheduled to follow up in clinic. However, she did not im-prove and developed left-sided weakness, mild dysphasia, and mouth twitching.
The patient has an abnormal urinalysis and anemia. Her urinalysis does not support a diagnosis of urinary tract infec-tion because of the negative leukocyte and nitrite with mildly elevated white blood cell count. Further, the proteinuria and he-maturia in the absence of infection raise concern of a structural/functional abnormality of the urinary system. Her urinalysis and anemia may not relate to her complaint of left-sided weak-ness, but they need to be investigated further.
The patient was not distressed but appeared exhaust-ed. On physical exam her vital signs were within normal limits. Cardiopulmonary and abdominal exams were nor-mal. Neurological exam was significant for left-sided weak-ness of the upper and lower extremities with motor strength of 4/5. There was no obvious facial weakness, and cranial nerves II to XII were grossly intact.
The left-sided weakness supports the primary working diagnosis of CVA. However, there are other possible causes, including increased intracranial pressure, focal mass effect, and infection. With her chronic symptoms of fatigue, weight loss, headache and anemia in addition to the new symptoms, includ-ing left-sided weakness, worsening headache, anemia, and the history of smoking, there is a high suspicion of malignancy.
The patient was directly admitted to the hospital with the working diagnosis of CVA, questionable new onset sei-zure activity and acute, worsening fatigue and weakness. The initial investigation showed low hemoglobin and hema-
• CliniCal Problem-Solving •Presented and edited by the Department of Family Medicine, University of Mississippi Medical Center, Diane K. Beebe, MD, Chair
AuthOr infOrmAtiOn: Dr. Phan was a third-year resident in the Department of Family Medicine, University of Mississippi Medical Center in Jackson.
cOrreSPOnding AuthOr: Thaibinh T. Phan, MD, 306 East 2nd Street, Alturas, CA 96101. Practice location: Modoc Medical Center Alturas, CA.
• clinicAl probleM-Solving •
Just a simple cerebral vascular accident?
Thaibinh T. Phan, MD
Presented and edited by the Department of Family Medicine, University of Mississippi Medical Center, Diane K. Beebe, MD, Chair

112 JOURNAL MSMA April 2012
tocrit. Thyroid-stimulating hormone, electrolytes, and liver panel were normal. Electroencephalography showed mildly slow activity that was normal for her age. Head computed tomography (CT) showed multiple bilateral hyperdense mass lesions within the brain with significant surrounding vasogenic edema. The patient felt better after hydration and rest, and there was no change in her neurological exam on admission day one.
With no history or clinical presentation of infection along with no new-onset severe headache or altered mental status, the head CT result strongly increases suspicion of metastatic brain cancer. This finding helps to explain her chronic anemia, fatigue, weakness, weight loss, headache and finally her left-sided weakness. However, we need to locate her primary tumor.
In adults, common primary cancers that metastasize to the brain include melanoma and cancer of the lung, breast, and kidney. Uncommon primary cancers that metastasize to the brain include colon and ovarian cancers.² The patient is a chron-ic smoker which puts her at higher risk for lung cancer. She has a first-degree relative with breast cancer, but her mammogram performed one year ago was negative. She has had no previous screening colonoscopy but denies bloody and tarry stool, and there is no colon cancer in her family. She complains of chronic intermittent abdominal pain without clear associating factors. The ER urinalysis shows heavy proteinuria and hematuria with-out other evidence of UTI. Based on the patient’s medical his-tory, the most probable primary cancers are lung, renal, colon, and ovarian.
A chest radiograph showed abnormal nodular den-sity in the left lower lung field. A chest CT showed multiple soft-tissue pulmonary nodules consistent with pulmonary metastases. Markers for breast, ovarian, and colorectal cancers CA 27.29, CA 125 II and CEA, respectively, were within normal limits.
The patient’s chest CT result indicates that the cancer has already metastasized to her lung. Metastatic breast cancer is not likely since she had a normal mammogram the previous year. Melanoma is not likely as she does not have a skin lesion. The normal tumor markers put colon and ovarian cancers low on the differential. The chronic abdominal pain and the abnormal urine still need to be investigated.
Results of an abdominal and pelvic CT showed large renal cell carcinoma (RCC) of the right kidney with tumor thrombus extending from the right renal vein into the infe-rior vena cava and to the intrahepatic inferior vena cava. Guided needle biopsy of right renal mass indicated that the patient has stage IV clear cell RCC. On further questioning, the patient reported intermittent gross hematuria at home. A repeated urinalysis one day after the admission was unre-markable with minimal hematuria and proteinuria.
The patient has metastatic, stage IV clear cell RCC.³ This explains her abdominal pain, sporadic proteinuria and hema-turia and other chronic symptoms. Many RCCs are clinically silent; thus, the diagnosis is not made until the disease is either locally advanced and unresectable or metastatic. The five-year survival rate of stage IV RCC is less than 10 percent.
This patient presented with worrisome symptoms in-cluding chronic anemia, fatigue and headache. In review, ER urinalysis two days prior to the admission was unremarkable except for hematuria and proteinuria. Creatine was 0.8 mg/dL two years ago and increased to 1.2 mg/dL one year ago. Hemo-globin was 13 g/dL and hematocrit was 40% five years ago but decreased to 9.5 g/dL and 29.8%, respectively, one year ago. These lab results are not specific enough to raise concern for RCC. In addition, her comorbidities can mislead the investiga-tion and make it more difficult to diagnose the disease sooner.
The patient was given phenytoin (Dilantin) to control her focal seizure symptoms. Palliative radical nephrectomy was not a treatment option as the cancer had already metas-tasized.4 The patient was given palliative whole-brain radio-therapy for symptomatic relief of her left-sided weakness and headache. She continued outpatient radiation treat-ment, but her condition worsened. She was admitted to a hospice facility and died a few months later.
RCC represents about 2% of the total cancer incidence in the United States. Clear cell RCC occurs in 75%–85% of all RCC.5 Most RCCs are sporadic. Patients with RCCs can pres-ent with a range of symptoms; unfortunately, many patients are asymptomatic until the disease is advanced. The most common presenting symptoms are hematuria, abdominal mass, abdom-inal pain, and weight loss. The anatomic extent of disease is the most consistent factor that determines prognosis. CT is the diagnostic test of choice, and surgical excision is the primary treatment for RCC.6
Key words: rEnAl cEll cArcInoMAs
references
1. Langhorne P, Stott DJ, Robertson L, et al. Medical complications after stroke. Stroke. 2000;31(6):1223–1229.
2. Schouten LJ, Rutten J, Huveneers HA, Twijnstra A. Incidence of brain metastases in a cohort of patients with carcinoma of the breast, colon, kidney, and lung and melanoma. Cancer. 2002;94(10):2698–2705.
3. Frank I, Blute ML, Leibovich BC, Cheville JC, Lohse CM, Zincke H. Independent validation of the 2002 American Joint Committee on cancer primary tumor classification for renal cell carcinoma using a large, single institution cohort. J Urol. 2005;173:1889–1992.
4. Shuch B, La Rochelle JC, Klatte T, et al. Brain metastasis from renal cell carcinoma: presentation, recurrence, and survival. Cancer. 2008;113(7):1641–1648.
5. Emal A, Siegel R, Xu J, Ward E. Cancer statistics. CA: A Cancer Journal for Clinicians. 2010;60:277–300.
6. Cohen HT, McGovern FJ. Renal-cell carcinomas. New Engl J Med. 2005;353:2477–2490.
• Scientific •
April 2012 JOURNAL MSMA 113
• preSident’S pAge •
thoMAS e. Joiner, Md2011-12 MSMA preSident
And Down the Stretch
They Come!
one being the best. Grade ones include the Arkansas Derby, Florida Derby, Wood Memorial, and the Santa Anita Derby, as well as the Bluegrass Stakes from Keeneland. Grade twos, such as the Louisiana Derby, Tampa Bay Derby, and grade threes count in the earnings race.
The Arkansas Derby, being a grade one and having a purse of $1 million, attracts some of the greatest horses out there, such as Curlin, Smarty Jones, and Afleet Alex. Any horse that seizes the winner’s share of that race will have enough graded stakes money to get in the Derby field; therefore, a “slew” of great horses have come through Hot Springs. It is great to have such first class racing so close to home.
So, who will take the Garland of Roses home this year? Will it be Hansen, winner of the Breeders Cup Juvenile last year, owned by an eccentric pain specialist from Kentucky; Union Rags who ran second to Hansen in that race; Take Charge Indy, winner of the Florida Derby; Gemologist, winner of the Wood; Dullahan, winner of the Bluegrass Stakes; or any of the other twenty starters? Well, if you ask me, Bodemeister, runaway winner of the Arkansas Derby gets the nod. This horse is named after Hall of Fame trainer Bob Baffert’s son, and Baffert flew in Hall of Fame Jockey Mike Smith to ride him in one of the richest preps races. I do not think that he meant to lose! The horse responded by running the last eighth in 11 and 4/5th seconds, blazing at the end of a mile and an eighth. If you want an exacta, fill it out with Take Charge Indy. However, it is a horse race, and anything can happen! (Big Brown)
Off to the races,
Well, here it is, the time of the year I find so exciting: the culmination of the run up to the Run for the Roses. All the major preps have been run, and the field is taking shape.
In case you are wondering how the derby field is set, a short lesson in Derby 101 is in order. Every trainer or owner who thinks they have a horse capable of the Triple Crown will have nominated that horse to the races at least by January, some much earlier. The fee at this time is $600, with a late fee in March of $6,000. Although this allows you to enter the races (Kentucky Derby, Preakness, Belmont Stakes), you still have to enter each race itself. The fee to enter the Kentucky Derby is $25,000, with a supplemental fee of $200,000 if you are late or your horse is a “late bloomer.” The field is made up of the top 20 horses in terms of “graded stakes earnings” or those stake races that have received a grade of one, two, or three by the Jockey Club,
2012 Triple Crown LengthMay 5 Kentucky Derby - Churchill Downs, Louisville, KY 1 ¼ mile
May 19 Preakness Stakes - Pimlico Raceway, Baltimore, MD 1 ³⁄16
mile
June 9 Belmont Stakes - Belmont Park, Elmont, NY 1 ½ mile
114 JOURNAL MSMA April 2012
Medicine is feeling the effects of regulatory and legislative changes, increasing risk, and profitability demands—all contributing to an atmosphere of uncertainty and lack of control.
What we do control as physicians: our choice of a liability partner.
I selected ProAssurance because they stand behind my good medicine and understand my business decisions. In spite of the maelstrom of change, I am protected, respected, and heard.
I believe in fair treatment—and I get it.
One thing I am certain about is my malpractice protection.”
“As physicians, we have so many unknowns coming our way...
Professional Liability Insurance & Risk Management Services
ProAssurance Group is rated A (Excellent) by A.M. Best. www.ProAssurance.com • 800.492.7212
2007-20115 Years Running
®

April 2012 JOURNAL MSMA 115
Mirror, Mirror D. Stanley Hartness, MD; Associate Editor
• editoriAl •
An awkward “thank you?” An apologetic “maybe he was having a bad day?” An astounded “surely we’re not talk-ing about the same doctor?”
How DO you respond to a back-handed compliment?
One of the perks my “semi-retired/part-time employment” status affords is the opportunity to treat pediatric patients once again. Whereas in Kosciusko my patient base had grown “older” with me, I’d almost forgotten the joys of interacting with chil-dren whose illnesses usually come on quickly and whose recoveries, as a rule, occur just as quickly.
On a recent Saturday when, in a weak moment, I had agreed to work, a 5-year-old boy was brought in by his mom with a two day history of fever to 102, severe cough, earache, and malaise. After what I considered a typical examination, I ordered a flu swab and CBC. With lab results in hand (or rather, available on the computer), I re-entered the exam room. Before I could say anything, the mom began, “Can I ask you a question? Can I bring my son back here to see you when he’s sick again?” The quiz-zical look on my face must have belied my “certainly” answer as she continued, “He’s always seen a pediatrician, but he’s never been examined like you just did.” Now I’d call that one of those back-handed compliments.
A recent Clarion Ledger newspaper article highlighted teen job-seekers. One of the teens featured was a 17-year-old who had been raised by her nurse grandmother who had inspired her to want to go into medicine. Any doubts about her decision were erased after she broke her back a year ago. After the accident, her encounter with doctors was said to have injected a bit of ur-gency into her plan. She related that, while her experience with one of them was good, “it was not good with the other. I want to be like the good doctor. There aren’t many doctors like him who will sit down and listen to you and explain to you what you want to know, who will help you feel better about your situation.”
There you have it: out of the mouth of babes, an indictment of our profession. And since perception is indeed reality, we need to step up our game. You remember the statistics: a patient who has a bad experience in our office will tell twenty others while perhaps five others will hear about a positive encounter. Unfortunately we all know patients who would blame a bad expe-rience on nothing more than out-of-date magazines or poor television reception in the waiting room.
Our knowledge and ability are givens; after all, we do have “that degree” after our names. Modern technology makes child’s play out of the most complex procedure. The jury is still out on the judgment issue. But as physicians we can and must take stock of our “bedside manner” and make a conscientious effort to ensure that each patient is shown the common courtesy (maybe even the “uncommon” courtesy) that we expect when we or our family members are on the receiving end.
It’s not too late to turn this thing around. I don’t know about you, but I don’t care if I never receive a back-handed compli-ment again. r
116 JOURNAL MSMA April 2012
A BIG FAT
GREEK GALA
Join us for the Inaugural Gala honoringMSMA’s 145th President Steve Demetropoulos, MD
President’s Inaugural Reception and Dinner-DanceSaturday, June 9 | 6:30 PM | $120 per ticket
Live Authentic Greek Music by Nick Demos and the Greek Islanders
Register now at MSMAonline.com for the 145th MSMA Annual Session!June 7 – 10, 2012 · Point Clear, Alabama
Questions? [email protected] or 601-853-6733, Ext. 340
April 2012 JOURNAL MSMA 117
MSMA Annual Session Schedule Thursday, June 7 (Registration 1pm – 5pm) 8:30 10:30 CME Presented by MACM (2hrs CME) 11:00 until MACM Golf Tournament
Grand Marriott Golf Club 3:00 5:00 Medical Affairs Forum (2hrs CME) 5:30 7:00 MSMA / UMC Welcome Reception 7:30 until Committee on Publications
Meeting/Dinner
Friday, June 8 (Registration 7am – 5pm) 7:00 8:00 MSMA Board of Trustees 7:30 9:30 Breakfast with Exhibitors 7:30 8:30 Reference Committee
Orientation/Breakfast 9:00 11:30 House of Delegates 11:30 1:00 Lunch with Exhibitors 11:30 12:30 MPCN Executive Committee Meeting 12:30 1:30 MPCN Board of Directors Luncheon 1:00 1:30 MSMA Board of Trustees Meeting 1:30 3:30 Reference Committee Hearings 3:30 4:30 Journal Editorial Advisory Board Meeting 3:30 4:30 MMPAC Board of Directors Meeting 3:30 4:30 YPS Business Meeting 3:30 4:30 Women in Medicine Business Meeting 3:30 5:00 MSMA Surveyor Training Workshop/
Council on Medical Education 6:30 8:00 President’s Reception – Crawfish Boil 8:00 9:00 Southern Medical Ice Cream Social
Saturday, June 9 (Registration 6:30am – 5pm) 6:30 8:00 Breakfast 7:00 12:30 Medical Affairs Forum (5hrs CME) 12:30 1:30 Candidate Speeches to Caucuses/
Boxed Lunch 1:30 2:30 Specialty Society Meetings 2:30 4:30 Guest Speakers with Book Signing
Topic: World War II 3:30 5:30 MSMA Board of Trustees 6:30 7:30 MSMA Reception and Alliance Raffle 7:30 11:00 President’s Inaugural Dinner Dance
Tickets: $120 per person
Sunday, June 10 (Registration 7am – 11am) 7:15 7:45 Worship Service 7:30 9:00 Voting 7:30 9:00 Continental Breakfast 8:00 9:00 VIP Breakfasts: 50-Year Club and
Past-Presidents’ 8:00 9:00 MSMA Board of Trustees 9:00 11:00 House of Delegates 11:00 11:15 MSMA Board of Trustees
MSMA ALLIANCE SCHEDULE Friday, June 8 10:00 am Pre-Convention Board Meeting 12:00 pm Luncheon (Dutch Treat)
Saturday, June 9 8:30 am House of Delegates 12:00 pm Installation Luncheon
Sunday, June 10 8:00 am Past Presidents’ Breakfast
REGISTER NOW AT MSMAonline.com OR RETURN THIS FORM BY MAIL
Name: Email: Specialty / Title: Address: City, State Zip: Phone: Fax: Cell: Spouse / Guest: Payment Information Credit Card Type: Visa MC AmEx Exp. Date: Credit Card #: Name on Card:
Please check the boxes and indicate number of attendees for each event below.
Physician Registration (Asterisks indicate family events.)
THURSDAY, JUNE 7 SATURDAY, JUNE 9 CME Presented by MACM ____ Medical Affairs Forum ____ Medical Affairs Forum ____ Pres.-Elect Reception ____ Welcome Reception ____ Pres.’s Dinner/Dance ____
($120 per person)
FRIDAY, JUNE 8 SUNDAY, JUNE 10 Breakfast with Exhibitors ____ Breakfast ____ House of Delegates ____ House of Delegates ____ Medical Affairs Forum ____ Lunch with Exhibitors ____ President’s Reception* ____ Ice Cream Social* ____
Alliance Registration FRIDAY, JUNE 8
Alliance Board Luncheon (Dutch) ____
SATURDAY, JUNE 9 Alliance House of Delegates ____ Alliance Installation Luncheon ____ ($45 tickets will be sold only on site.)
SUNDAY, JUNE 10 Past Presidents’ Breakfast ____
Mail completed form to MSMA c/o Becky Wells
PO Box 2548, Ridgeland, MS 39158-2548
Questions? [email protected] or 601-853-6733
118 JOURNAL MSMA April 2012
• editoriAl •
Bold Changes to the Norm
According to the MSMA Bylaws, “The Council on Constitution and Bylaws shall be responsible for the continuing study of the organization of the Association.” Pursuant to that charge, the Council on Constitution and Bylaws (CCB) will present a report to the House of Delegates that contains several important recommendations
about the organization of our association at the annual session meeting in Point Clear, Alabama, on June 7-10, 2012. These recommendations come after the CCB’s study of issues involving the future leadership and direction of MSMA and they call for “bold changes to the norm” (quoting from the report) in the way MSMA is organized and conducts its business. Briefly stated, the CCB’s report as of press time for this issue includes recommendations for the establishment of immunity and indemnity of MSMA officers, allowance for HOD meetings by way of the internet, and revisions to the method of nomination of MSMA officers and amendment of our bylaws.
The CCB is aware of the opinion of some members who believe that MSMA needs to do more to identify new physician leaders and to encourage all members to participate in the work of the association. The CCB is also aware of the sentiment of some members that only members with years of seniority who are willing to physically attend meetings are knowledgeable enough to hold leadership positions and thereby “control” the work of the association. Such hubris in our association is unfortunate, since we purport to function as an open, inclusive, and democratic organization.
The CCB believes that increased efforts to recruit physician leaders within the current membership of the association and to stimulate participation in MSMA by all members will have the potential to invigorate the association. Furthermore, this will likely improve attendance at MSMA events and further the goals of the association by giving all members the opportunity to have access to information about MSMA activities and to have meaningful input into the work of the association. Business as usual is not enough for the MSMA to move forward as a strong, united voice for health care in Mississippi. Therefore, fundamental changes in the way that the MSMA conducts its business and interacts with its members are in order to insure confidence in all members and the public that we are moving in the right direction – together.
With these issues in mind, the CCB’s pending report to the House of Delegates will recommend that MSMA consider increasing member participation by allowing attendance at annual sessions and voting for officers by electronic means. The CCB will also recommend expanding the grassroots focus of the Nominating Committee by changing the composition of the committee to include one member from each of MSMA’s 13 component societies with a Chair elected by the House of Delegates. Another CCB recommendation is that a limit be placed on the number of elected and appointed MSMA positions that a member may hold at one time, in order to allow more members the opportunity to participate in leadership activities. Providing immunity and indemnity to MSMA officers will also encourage more members to get involved in the leadership of our association. Lastly, the CCB report recommends that our bylaws be amended to allow for the amendment of the bylaws by a simple majority vote (instead of the current 2/3’s supermajority vote requirement), if the amendment is recommended by the CCB, and notice is available to all members at least 30 days in advance of the meeting of the House of Delegates. The last CCB meeting before this year’s annual session will be in May, so there may be more recommendations forthcoming from the CCB for the House of Delegates to consider this year.
These recommendations by the Council on Constitution and Bylaws, as well as resolutions, officer elections, and other business will likely generate much debate at the 2012 annual session of the House of Delegates. The Journal urges all MSMA members to participate in that debate and the “continuing study of the organization of the Association.” Attend the annual session as a delegate from your component society to voice your opinion in the reference committee meetings on June 8, 2012, as well as the House of Delegates business meeting and officer elections on June 10, 2012. If you cannot attend in person, consider expressing your views on these issues to a colleague who is attending the annual session as a delegate. Please see the current draft of the CCB’s report to the HOD that follows this editorial on the next page.
In the words of the French philosopher Joseph Joubert, “The aim of argument, or of discussion, should not be victory, but progress.” All members of MSMA owe it to the association to participate, either in person or by proxy, in the discussion of the issues raised at this year’s annual session. Regardless of the outcome of the discussions our MSMA, and we as its members, will be the better for it.
—Philip Merideth, MD, JD Member of the Committee on Publications and the Council on Constitution and Bylaws
April 2012 JOURNAL MSMA 119
Background: According to the MSMA Bylaws Chapter XIII, Section (4) the Council on Constitution and Bylaws is described as follows:
The Council on Constitution and Bylaws shall be responsible for the continuing study of the organization of the Association. It shall receive all referred suggested amendments and changes and shall recommend to the House of Delegates and the Board of Trustees any amendments or revisions which seem necessary or advisable. The Council shall meet at least once a year and shall make a report to the House of Delegates on the state of the Constitution and Bylaws every two years. The Council shall consist of three (3) members elected by the House of Delegates for terms of three (3) years each and shall meet at least on an annual basis and more often as necessary.
The Council on Constitution and Bylaws met on December 2, 2011 and on January 20, 2012 and recommends the MSMA House of Delegates approve the following changes to the Articles of Incorporation at the 144th MSMA Annual Session June 7-10, 2012.
Discussion: All corporations including non-profits and trade associations like MSMA are subject to state laws regarding corporations such as the Mississippi Model Nonprofit Corporation Act. During the 2011 Regular Legislative Session, Senate Bill 2444 was adopted which represented a revision to Mississippi’s Model Nonprofit Corporation Act. This legislative action coincides with the Council on Constitution and Bylaws two-year review of MSMA’s Constitution and Bylaws. Thus, the MSMA Council on Constitution and Bylaws recommends changes in the MSMA Constitution which will modernize the Association’s Constitution in a manner consistent with the new non-profit corporation laws.
There are two proposed changes to the Articles of Incorporation: (1) a constitutional amendment clarifying the intent of the Association to limit the personal liability of its voluntary directors (trustees) and officers to MSMA or its members as set forth in Miss. Code Ann. Section 79-11-267, and (2) though the adoption of an immunity constitutional amendment is significant to minimize exposure of trustees and officers, the Association should consider additional provisions in the constitution and bylaws which grant discretion to the Association to indemnify its trustees and officers.
Recommendation 1: The MSMA Council on Constitution and Bylaws recommends that the MSMA Constitution be amended as follows:
MSMA CONSTITUTION
Article IX Board of Trustees:
Section 1. Duties: The Board of Trustees shall be the executive and governing body of the Association during vacation of the House of Delegates and shall perform such duties as are prescribed by law governing directors of corporations and in the bylaws of the Association.
Section 2. Composition: The Board shall consist of the district trustees, the president, president-elect, immediate past president, secretary-treasurer, Speaker of the House of Delegates, one medical student trustee and one resident/fellow trustee.
Section 3. Finance: The Board of Trustees shall constitute the Finance Committee of the House of Delegates.
Section 4. Liability of Board of Trustees: The members of the Board of Trustees shall not be liable to the Association or its members for money damages for any action taken or any failure to take any action as a director, except liability for:
(a) The amount of a financial benefit received by the trustee to which the trustee is not entitled;
(b) An intentional infliction of harm;
(c) A violation of Miss. Code Ann. Section 79-11-270; or
(d) An intentional violation of criminal law.
• MSMA •2012
Mississippi State Medical Association 144th Annual Session June 7-10, 2012Point Clear, Alabama
Report of the Council On Constitution & Bylaws*
Subject: Amendments to the MSMA Constitution and BylawsFrom: Eric Lindstrom, Chair, MSMA Council on Constitution and BylawsReferred to: Reference Committee on Constitution and Bylaws
120 JOURNAL MSMA April 2012
Recommendation 2: Though the adoption of the immunity constitutional amendment is significant to minimize exposure of trustees and officers, the Association should consider adopting an additional constitutional and complementary bylaw provision which grants discretion to the Association to indemnify its trustees and officers, to wit:
MSMA CONSTITUTION
Article XI Indemnification
Each person who was or is made a party or is threatened to be made a party to or is involved in any action, suit or proceeding, whether civil, criminal, administrative or investigative by reason of the fact that he or she, or a person of whom he or she is the legal representative, is or was a trustee or officer of the corporation or while a trustee or officer of the Association is or was serving at the request of the Association as a trustee or officer of another corporation or of a partnership, joint venture, trust or other incorporated or unincorporated enterprise, including service with respect to employee benefit plans or trusts, whether the basis of such proceeding is alleged action or inaction in an official capacity as a trustee or officer or in any other capacity while serving as a trustee or officer may be indemnified and held harmless by the Association to the fullest extent authorized by the Mississippi Non-profit Corporation Act as the same exists or may hereafter be amended and pursuant to the Association’s bylaws as such bylaws may be amended.
Bylaws Chapter XVIII Indemnification of Trustees and Officers
Section 1. Power to Indemnify in Actions, Suits or Proceedings. The Association may indemnify a person who was or is a party or is threatened, pending or completed action, suit or proceeding, whether civil, criminal, administrative or investigative, other than an action by or in the right of the Association, by reason of the fact that such person is or was a trustee or officer of the Association, against expenses, including reasonable attorneys’ fees, judgments, fines and amounts paid in settlement actually and reasonably incurred by such person in connection with such action, suit or proceeding to the extent provided by the provisions of the Mississippi Non-Profit Corporation Act, as such act shall be amended from time to time, and to the extent insurance coverage is available to fund the indemnification.
Section 2. Insurance. The Corporation may purchase and maintain insurance on behalf of any person who is or was an employee, trustee or officer of the Corporation or who serves in the capacity of Medical Director for the Association, against any liability asserted against such person and incurred by such person in any such capacity, or arising out of such person’s status as such, whether or not the Association would have the power or the obligation to indemnify him or her against such liability under the provisions of this Article.
The MSMA Constitution and Bylaws will be renumbered accordingly.
Recommendation 3: MSMA Constitution Article V1 requires that the Association meet annually in a place determined by the House of Delegates and in compliance with corporate laws. New non-profit corporation laws anticipate technology and clarify that the “place” for an annual or special meeting can be cyberspace.
MSMA Bylaws
Chapter II. Annual and Special Sessions
Section 1. Time and Place: An annual session shall be held prior to the annual session of the American Medical Association at a time and place to be determined by the House of Delegates. The Board of Trustees shall recommend to the House the location and dates of annual meetings. The dates and site of the annual session selected may be changed by majority vote of the Board of Trustees if necessary.
Section 2. Special Session: A special session of the Association or of the House of Delegates may be called by the President, with the approval of the Board of Trustees. The Board of Trustees is empowered to call a special session by majority vote.
Section 3. An annual or special meeting of the House of Delegates does not need to be held at a geographic location if the meeting is held by means of the Internet or other electronic communication technology in a fashion which affords the delegates and alternate delegates the opportunity to read or hear the proceedings substantially concurrently with their occurrence, vote on matters submitted to the delegates and alternate delegates, pose questions, and make comments.
The remaining section of Chapter II will be renumbered accordingly.
Recommendation 4: The MSMA Council on Constitution and Bylaws determined that the MSMA House of Delegates should consider bold changes to the norm including changing the way in which MSMA conducts its voting for elected officers and recommends that MSMA conduct a survey of members to gauge interest in forms of electronic voting for officers of the Association and report back to the MSMA House of Delegates during its next Annual Session.
1 ARTICLE V Sessions and Meetings: The Association shall hold a meeting of the House of Delegates at least annually and at other times as deemed necessary or as provided in the bylaws. The time and place for holding the annual session shall be determined by the House of Delegates, but the Board of Trustees shall have the power to determine or change the time or place or both of the annual session if necessary.
April 2012 JOURNAL MSMA 121
Recommendation 5: The MSMA Council on Constitution and Bylaws determined that the MSMA House of Delegates should consider additional methods for adoption of amendments to the bylaws.
The current method of amending the bylaws is found in Chapter XVIII and it requires a 2/3rds vote for adoption but does not require notice of the proposed changes prior to the annual session. Following the adoption of a new provision during the 143rd Annual Session, the bylaws require a 30-day notice of a special session (whether to change the bylaws or otherwise) and establish the method to use proxy votes. (See Chapter VIII, Section 3.) The following recommendation creates an alternative method for amending the bylaws which is consistent with the current bylaws and blends concepts of notice and fairness:
Chapter XVIII Amendments: These Bylaws may be amended at any annual session or at any special session by a vote of two-thirds of the delegates present or voting by duly authorized proxy at that session, after the amendment has lain upon the table for one (1) day. Alternatively, upon the report and recommendation of the Council on Constitution and Bylaws and upon 30-days notice to the members, these Bylaws may be amended at any annual session or at any special session by a majority vote of the legal delegate votes cast or voting by duly authorized proxy at that session, after the amendment has lain upon the table for one (1) day.
Recommendation 6: The Council on Constitution and Bylaws recommends several changes to the structure of the Nominating Committee and other changes designed to limit the qualifications for elected MSMA office for the following reasons:
· MSMA needs to identify new physician leaders.
· Changing the nominations process and expanding the role of component societies are two ways to accomplish this goal.
· Limiting terms and qualifications for elected MSMA offices is another way to encourage new physicians.
· Growing participation within MSMA would invigorate the Association and improve attendance at the MSMA Annual Session and other events.
Therefore, the Council on Constitution and Bylaws recommends the following changes to MSMA Bylaws:
Chapter X. Election of OfficersSection 1. Ballot: All elections shall be by secret ballot, and a majority of the votes cast shall be necessary to elect, unless otherwise provided for in the bylaws.
Section 2. Nominations Composition of Committee on Nominations. The Committee on Nominations each year shall be composed of a representative from each component society selected -in a manner as determined by the component society the nine (9) most recent Past Presidents of the Association, with the Immediate Past President serving as an ex officio non-voting member. No person can serve more than three (3) years on the Committee on Nominations.
Section 3. Chair of the Committee on Nominations: The chair of the Committee on Nominations shall be annually elected by the MSMA House of Delegates. No member shall be eligible for re-election as Chair after he or she has served three (3) terms. It shall be the duty of this Committee to consult with the members of the Association and to hold one or more meetings, at least 90 days prior to the Annual Session, at which the best interest of the Association and of the profession of the state for the ensuing year will be carefully considered.
Section 4. Nominations. It shall be the duty of this Committee to consult with the members of the Association and to hold one or more meetings, at least 90 days prior to the Annual Session, at which the best interest of the Association and of the profession of the state for the ensuing year will be carefully considered. The Committee shall nominate at least one (1) but no more than three (3) persons for each office. No person shall be nominated by the Committee unless a member of the Committee has discussed the office with such person and the person to be nominated has expressed a desire to be nominated and has agreed to serve if elected. Except for election as a MSMA Delegate or Alternate Delegate to the AMA, no member may be nominated to more than one elected office. The list of nominees developed by the Committee shall be published to the entire membership at least 60 days prior to the Annual Session. Nominations for appointment to membership on the State Board of Medical Licensure shall be made by the Board of Trustees, who shall submit the names of at least three (3) physicians to the Nominating Committee for each vacancy to be voted on by the House of Delegates. The House of Delegates and /or the Nominating Committee may add additional names to the list of those to be voted on, provided that no more than three (3) physicians are elected for each vacancy and submitted to the Governor for his consideration in accordance with Section 73-43-3, Mississippi Code of 1972, annotated as amended; provided further, no physician shall be nominated who has served two (2) consecutive terms.
Section _5. Nominations to the State Board of Medical Licensure: The Board of Trustees shall nominate at least three (3) physicians for each vacancy on the State Board of Medical Licensure and present these nominees to be voted on by the House of Delegates. The House of Delegates and /or the Nominating Committee may add additional names to the list of those to be voted on, provided that no more than three (3) physicians are elected for each vacancy and submitted to the Governor for his or her consideration in accordance with Section 73-43-3, Mississippi Code of 1972, annotated as amended. No physician shall be nominated who has served two (2) consecutive terms.
Section 46. Report of Nominations: The House of Delegates shall receive the report of the Committee on Nominations of Officers, Trustees, and Council Members and others on the first day of the Annual Session and shall elect Officers, Trustees, and Council
122 JOURNAL MSMA April 2012
members and others on the last day of the Annual Session. All nominees must be active members of the Association.
Section 57. Nominations from the Floor: Nothing in this chapter shall be construed to prevent additional nominations being made from the floor by members of the House of Delegates.
Section 8. Except for election as a MSMA Delegate or Alternate Delegate to the AMA, no member may be nominated by the Nominations Committee or from the floor if that person holds an elected office or has been appointed to an office within a corporate subsidiary of MSMA or with an agency of the state of Mississippi. Members who are elected as an AMA Delegate or Alternate Delegate are eligible to be elected to only one (1) other MSMA position.
Section 9. Nothing in this section shall preclude a member from serving as an officer in MSMA or as a representative from MSMA to one of its corporate subsidiaries or a government agency while also serving as a member of the House of Delegates or as an officer of an MSMA component society. Nothing in this section shall preclude a member who is a physician employed by the State of Mississippi from being eligible for election or appointment based solely on their employment status.
Section 10. Nothing in this Chapter shall act to void the valid election of a member. All controversies regarding the interpretation and enforcement of this section shall be resolved by the MSMA Council on Ethical and Judicial Affairs.
Chapter XI. Duties of Offices Section 1. President: The president shall have general supervision over all meetings of the various bodies of the Association and shall appoint chairs of all committees and councils not otherwise provided for. He or she shall deliver an annual address at such time and place as may be arranged, and shall perform such other duties as custom and parliamentary usage may require. He or she shall fill by appointment of a member who would otherwise be qualified to be elected all vacancies occurring during his or her tenure of office among the general officers, the Board of Trustees, Councils, committees, and AMA Delegation. He or she shall be empowered to appoint such committees on an ad hoc basis as may be desired or required to conduct the affairs of the Association. He or she shall be an ex officio member of all Councils and committees. He or she shall be the real and acknowledged head, as well as the personal representative, of the medical profession of the State of Mississippi during his or her term of office, and insofar as practicable, shall visit by appointment the various sections of the state and the component societies of the Mississippi State Medical Association and assist the Trustees in their tasks of aiding and strengthening the component societies and in making their work more useful.
(These changes shall take effect January 1, 2013.)
Council Membership: Members of the Council for the 2011-2012 year are Eric E. Lindstrom, MD, of Laurel; Philip T. Merideth, MD, JD of Jackson; and Edwin D. Meeks, II, MD of Columbus.
*The Council on Constitution and Bylaws reserves the right to make changes to the Report prior to final submission to the MSMA House of Delegates. r
DiD your last meeting leave you feeling a taD
“ECTOPIC”If so, you should consider having
your next meeting in Tupelo!
We’re right in the middle of the mid-south and tupelo is the headquarters of the north mississippi medical Center, the largest non-metropolitan hospital in the
united states, and is a winner of the prestigious malcolm Baldrige national
Quality award!And we promise you won’t feel out of place here!
For information about setting up your next meeting, give Linda Elliff a call at 800-533-0611.
T he comments expressed in this Journal are those of the indicated author. Comments and opinions are not expressions
of the views or official policies of the Mississippi State Medical Association. We encourage our membership to submit comments for publication regarding any opinion expressed or information contained in the Journal.
E mail to Managing Editor, Karen Evers: [email protected] or mail to: Editor Lucius Lampton, MD, 111 Magnolia St., Magnolia, MS 39652-2825.
We encourage your comments.

April 2012 JOURNAL MSMA 123
• editoriAl •
A Look into Preconceived IdeasElliott Browning, Auburn University
Preconceived ideas have been present throughout human history, but there have been courageous, and some say crazy, individuals who have tested those beliefs making discoveries that have changed the world. At one time, the popular belief was that the earth was flat. People assumed the horizon line was the edge of the earth. As time went on, men
began to gain more knowledge in astronomy and navigation. A few intelligent men started to notice certain circumstances that contradicted the preconceived notion of a flat earth. Specifically, a man named Eratosthenes found that a stick casts a shadow at noon in Alexandria, Egypt, while the pillars in Syrene, Egypt, cast a shadow of a different length at noon at the same time of year.1 How could this be if the earth were flat? It was very uncomfortable during that time and even today for people to question a prevailing belief and many were apprehensive in showing evidence contradicting a preconceived idea. Some, however, did not want to accept society’s assumption and explored with great persistence what they believed to be true, that the earth was indeed round.
Around the 1940s and early 50s, doctors and scientists claimed that the human being was physically incapable of running a four minute mile. Many athletes during that time attempted the four minute mile, but all of them failed. People began to believe the doctors and accepted the idea as fact that a human being is physically unable to accomplish such a feat. On May 6, 1954, Roger Bannister ran a mile in 3:59.4 seconds and achieved the “impossible.”2 After the run, Bannister was quoted saying, “Doc-tors and scientists said that breaking the four-minute mile was impossible, that one would die in the attempt. Thus, when I got up from the track after collapsing at the finish line, I figured I was dead.”3 Remarkably, a very short time after Bannister made his mark in history, many runners, including John Landy, also ran the mile in under four minutes. Because of Bannister’s milestone, his run paved the way for other athletes to believe that running a mile in less than four minutes was, in fact, possible.4 For people, including the medical doctors of that time, to claim that an idea is humanly impossible, they did not take into account human will. Keeping an open mind to possibilities and not focusing on perceived limitations have allowed human beings to progress. Think of all the challenges in your own life that you thought were impossible until you simply tried.
In the late 1800s, some doctors wanted to attempt surgery on the human heart. Prominent leading doctors of the day be-lieved heart surgery to be ridiculous, and patients would never survive. Due to the stature of the leading doctors, people blindly accepted the idea that the heart was inoperable. In 1883, a surgeon named Theodor Billroth claimed, “that the surgeon who should attempt to suture a wound of the heart would lose the respect of his colleagues.”5 In 1893, a man suffers a stab wound to his heart. Dr. Daniel Hale Williams is credited with one of the first successful surgeries that involved a heart wound, but Dr. Wil-liams was only able to suture the pericardium. A short time after Dr. Williams’ operation, many surgeons attempted to stitch the heart itself, but the patients died.6 After the many failed attempts, a surgeon named Dr. Stephen Paget described the progress of heart surgery saying, “Surgery of the heart has probably reached the limits set by nature to all surgery; no new method and no new discovery can overcome the natural difficulties that attend a wound of the heart.”5 For some, the heart was considered to be un-touchable, but one surgeon, Dr. Ludwig Rehn, performed the first successful heart surgery in which he actually sutured the heart, itself.6 Dr. Rehn’s operation was groundbreaking, thus proving that cardiac surgery on a living heart is certainly possible.
After many years of experimentation and trial and error, doctors and surgeons expanded their knowledge of cardiac surgery. Not enough can be said of the bravery shown by the doctors who attempted every means possible to save their patients and pass on the experience. After many of the early operations in history were performed, the surgeons found a major problem. They needed to figure out a way for the blood flow to bypass the heart while they were operating. Dr. Walt Lillehei, who is considered to be the father of open heart surgery, initiated the idea of cross-circulation in which the patient was connected to another person, usually one of the parents. The person basically functioned as an oxygenator for the patient while the surgeon was operating.7 Because of the increased risk involved with cross-circulation, many doctors, including John Gibbon, worked for years to build a
“For the greatest enemy of truth is very often not the lie — deliberate, contrived and dishonest — but the myth — persistent, persuasive, and unrealistic. Too often we hold fast to the clichés of our forebears. We subject all facts to a prefabricated set of interpretations. We enjoy the comfort of opinion without the discomfort of thought.”
— John F. Kennedy, Yale University commencement address (June 11, 1962)

124 JOURNAL MSMA April 2012
machine that would bypass the heart and lungs and deliver oxygen to the tissues of the body. With the help of some IBM engi-neers as well as inventions created by Dr. Michael DeBakey and others, Gibbon created a heart-lung bypass machine.6 The bypass machine revolutionized cardiac surgery, and surgeons were able to perform very complex operations to fix major heart defects. After a few years, many doctors were contemplating the idea of heart transplants. Building off the research of Dr. Norman Shum-way and others, Dr. Christiaan Barnard performed the first human to human heart transplant in history on December 3, 1967.8 Although many of the patients of these pioneer surgeons did not survive, the doctors have learned from their failures even more so than their successes and have made innovative discoveries that have allowed the progression of cardiac surgery over time. For the pioneer surgeons to perform high risk operations on such a vital organ is extremely admirable, and without their bravery to take a leap of faith, cardiac surgery would not be as advanced as it is today.
As surgeons gained more experience with cardiac surgery, many began to operate on progressively younger patients. Pedi-atric cardiac surgery has improved over the years in that the mortality rate of patients has drastically decreased. Pediatric cardiac programs have been created in many hospitals all over the nation. Many of these programs have failed, while some have been very successful. The majority of the programs have been effective in major cities in the United States such as: Boston Children’s, Children’s Hospital of Philadelphia, Texas Children’s in San Antonio, and Children’s Hospital of Michigan in Detroit. Some pro-grams, however, have been able to succeed in smaller cities across the country. Specifically, at the Blair Batson Children’s Hos-pital in Jackson, MS, Dr. Jorge Salazar and others began a pediatric cardiac unit about eighteen months ago, and it has produced results that emulate some of the best programs in the country. I was honored to be given the opportunity to shadow Dr. Salazar and his team for several weeks. Dr. Salazar and his team have given children a chance at life that a couple of years ago was not possible in Mississippi. Because of the perseverance and skill of the surgeons, doctors, and nurses, the program has surpassed the preconceived limitation of being in a small city.
Even if the heart surgeon has much experience, the surgeon has to be prepared for the extraordinary. When the tiny chest of a child is open and the child’s life is on the line, persistence, faith, and courage play a major role in overcoming the unexpected in the operating room. Recently, a four-year old child at Blair Batson was suffering from congestive heart failure, and initially he was going to be placed on the transplant list. After a series of tests, a diagnosis of an anomalous left coronary was determined, and the child was scheduled for surgery. During the surgery, the right main coronary was partially obstructed, and the left main coronary was nowhere to be found. After hours of searching, the surgeon discovered that the left main coronary, which was two and half millimeters in diameter, was disconnected from the aorta. The duration of the entire surgery was about ten hours, and the patient spent four of them on bypass. After only a week of recovery, the child was able to return home. All of the tests performed on the child’s heart before the operation give the surgeon a preconceived idea of the condition of the heart. However, the surgeon’s relying on a preconceived idea is very dangerous because nothing is known for sure until the surgeon is able to look directly into the child’s chest during the operation. Pediatric cardiac surgery has saved the lives of countless children who would have otherwise died, and the dedication shown by the surgical team should not be overlooked. After all of the progress of the last century, pediatric heart surgeons take a leap of faith even today because there are still extraordinary circumstances that go unex-plained. Conditions that are believed by many to be impossible to survive have been overcome due to the persistence, skill, and courage of the surgeon. Faith in the strength of the human will to survive undermines the preconceived idea that all is explainable. Preconceived ideas have throughout history defined our beliefs, especially with situations that are believed to be humanly impos-sible, and many of them have been found to be false. Dr. Salazar, in the short time we had together, taught me that children have a will to survive, and the skill of the surgeon makes it possible for that life to be comfortable, normal, and fulfilling. Keeping an open-mind and having faith make innovative discoveries possible and save lives.
author information
Browning is a pre-med student majoring in biomedical sciences at Auburn University. He recently shadowed Dr. Jorge Salazar at the Blair Batson Children’s Hospital at the University of Mississippi Medical Center in Jackson.
references1. Glass D. Who knew the earth was round. Moment of Science. 2008. http://indianapublicmedia.org/amomentofscience/sizing-up-the-earth/. Accessed Decem-ber 29, 2011.
2. First four-minute mile. The History Channel Web site. http://www.history.com/this-day-in-history/first-four-minute-mile. Accessed January 2, 2012.
3. The sports quote…the best of the best. Famous Quotes and Quotations Web site. http://www.famous-quotes-and-quotations.com/sports-quote.html. Accessed January 2, 2012.
4. Dunaway J. Track and field; from impossible to commonplace. The New York Times. 2003; http://www.nytimes.com/2003/05/04/sports/track-and-field-from-impossible-to-commonplace.html. Accessed January 2, 2012.
5. Elkin DC. Suturing wounds of the heart. Annals of Surgery. 1932;95(4): 573-577. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1391585/pdf/ann-surg00641-0094.pdf. Accessed December 29, 2011. PMCID: PMC1391585.
6. Stephenson LW. History of cardiac surgery. In: Cohn LH, Edmunds LH Jr, eds. Cardiac Surgery in the Adult. 3rd ed. New York, NY: McGraw-Hill Co; 2003:3-29.
7. Miller GW. King of hearts: the true story of the maverick who pioneered open heart surgery. Texas Heart Institute Journal. 2000;27(2):224-225. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC101066/. Accessed January 21, 2012. PMCID: PMC101066.
8. Silbergleit A. Norman E. Shumway and the early heart transplants. Texas Heart Institute Journal. 2006;33(2):274-275. http://www.ncbi.nlm.nih.gov/pmc/ar-ticles/PMC1524691/. Accessed January 21, 2012. PMCID: PMC1524691.

April 2012 JOURNAL MSMA 125
PHYSICIANS NEEDED
We are a Medical Group looking for a physician to join our group and perform Consultative Exams
for Social Security in Mississippi. Part-time or full-time. No call or weekends.
Travel within state will be necessary. Pay for day’s work is guaranteed
regardless of turnout and is paid promptly regardless
of time of collection. All administrative needs including scheduling, transcription, assisting,
and billing are provided. Contact: Susan Gladys
866-929-8766 or email [email protected]
Space for Lease. Medical Office/Clinic. Richland Medical Plaza, Richland, MS area. One of the highest traffic areas in the Jackson Metro area. Next door to four medical clinics, tremendous referral potential for pediatrics, orthopedics, ophthalmology, OBGYN, home health, etc.
Call 601-214-9019 or email [email protected]
PHYSICIANS NEEDED
Internists, Cardiologists, Ophthalmologists, Pediatricians, Orthopedists, Neurologists, Psychiatrists, etc. interested in performing consultative evaluations according to Social Security guidelines.
OR
Physicians to review Social Security disability claims at the Mississippi Department of Rehabilitation Services (MDRS) in Madison MS.
Contact us at:
Leola Meyer 601-853-5487
Toll Free 1-800-962-2230 (Ext. 5487) or
Jo Ann Summers 601- 853-5599
DISABILITY DETERMINATION SERVICES 1-800-962-2230
• plAceMent / clASSified •
126 JOURNAL MSMA April 2012
Dear JMSMA Editor,In response to the guest editorial by Carl Feind (Elec-tronic Medical Records and the End of Value: Physi-
cians, Nurses, and Scribes, March 2012), I was one of those who fought tooth and nail against electronic medical records when it was implemented in our office seven years ago. And like Dr. Feind, I saw it as the end of good medicine—I was being swept into the abyss of paperless, impersonal, time con-suming, digitally induced poor quality of care. But how wrong I was! Yes, the first year was a nightmare as we, a group of not-so-computer-savvy doctors, had to learn a whole new way of recording and processing information, with each patient essentially being a new patient, with records being digitalized, and data being entered by hand. It was time consuming and frustrating, and there were times when, if I had been a few years older and a little more financially secure, I would have hung it up and gone home. But like so many things we do, including surgery and sound medical thinking, repetition and practice are the keys to learning, and now I don’t know how I functioned for all those years without electronic records.
No longer are there charts as thick as a New York phone book, no longer do I have to wade through those thick records to find information, no longer are there lost charts—everything is just a click away. Data retrieval is instantaneous. And efficiency has improved. With standardized template-driven notes, I spend much less time “writing” notes than I ever did longhand or dictating—and the notes are much more complete. If a healthcare provider is spending 15 to 20 minutes in the chart before seeing the patient and another 20 minutes completing the record, either he is new at the process, he has not “tweaked” the templates to fit his practice, or he has a medical record system that is not user friendly—and there are plenty of those out there.
It continues to baffle my non medical friends at how in the Dark Ages medicine is, as far as recording data is concerned. What would you think if your banker was still pulling out a hand written ledger to look at and calculate your balance? Please know there is light at the end of the tunnel when it comes to electronic medical records. Practice may not make perfect, but medicine has never been a perfect science anyway—it is a practice—and like medical problem solving, electronic notes can become second nature to you if you let it. And as far as a scribe, the last thing I need is another employee. —Thomas L. Wiley, MD, Jackson
• letterS •Light at the Tunnel’s End: Response to EMR End of Value Editorial
• ComprehensiveManagement• ComprehensiveConsulting• Billing&AccountsReceivableManagement• Coding&Documentation• PracticeAssessments&RevenueEnhancement• ProfitabilityImprovement• PracticeStart-ups• PersonnelManagement
We specialize in the business of healthcare
1600NorthStateStreetSuite400Jackson,MS39202
Telephone:601.944.1717WATS:1.800.355.4231www.mpsbilling.com
The Pen is MighterThan the Sword
Express your opinion in the JMSMA through a letter to the editor or guest editorial. The
Journal MSMA welcomes letters to the editor. Letters for publication should be less than 300 words. Guest editorials or comments may be longer, with an average of 600 words All letters are subject to editing for length and clarity. If you are writing in response to a particular article, please mention the headline and issue date in your letter. Also include your contact information. While we do not publish street addresses, e-mail addresses or telephone numbers, we do verify authorship, as well as try to clear up ambiguities, to protect our letter-writers. You can submit your letter via email to KEvers@MSMA online.com or mail to the Journal office at MSMA headquarters: P.O. Box 2548, Ridgeland, MS 39158-2548.
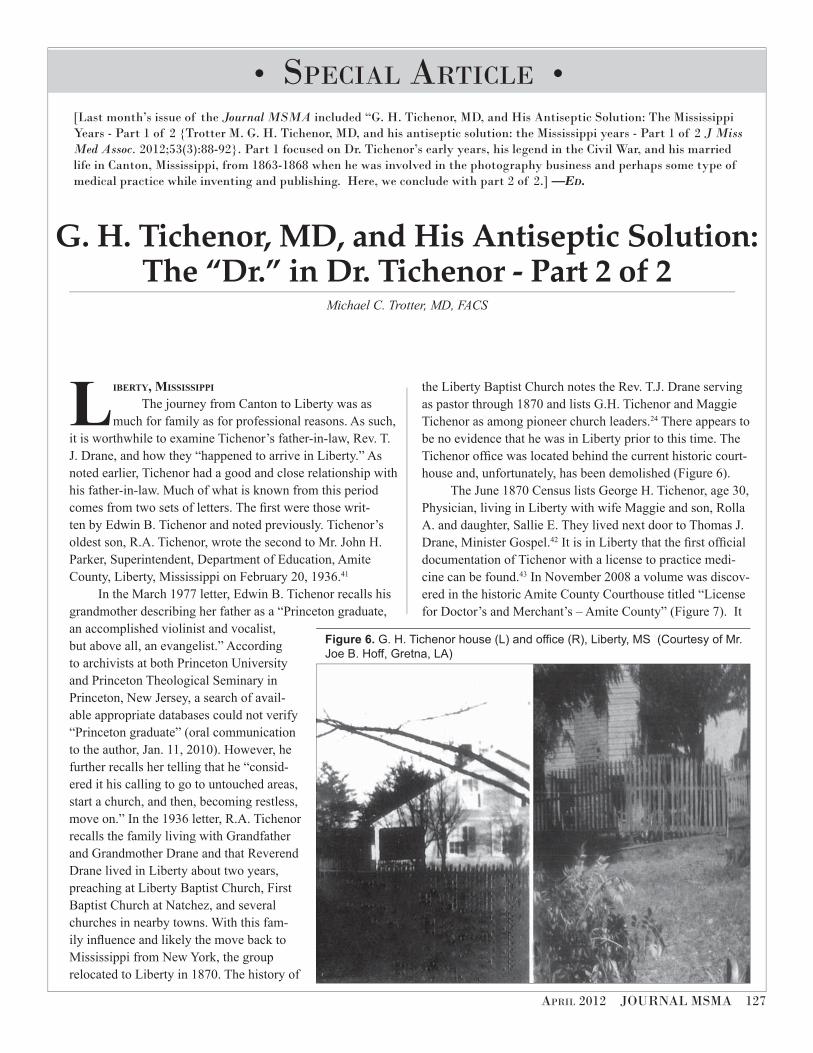
April 2012 JOURNAL MSMA 127
liberty, mississippi
The journey from Canton to Liberty was as much for family as for professional reasons. As such,
it is worthwhile to examine Tichenor’s father-in-law, Rev. T. J. Drane, and how they “happened to arrive in Liberty.” As noted earlier, Tichenor had a good and close relationship with his father-in-law. Much of what is known from this period comes from two sets of letters. The first were those writ-ten by Edwin B. Tichenor and noted previously. Tichenor’s oldest son, R.A. Tichenor, wrote the second to Mr. John H. Parker, Superintendent, Department of Education, Amite County, Liberty, Mississippi on February 20, 1936.41
In the March 1977 letter, Edwin B. Tichenor recalls his grandmother describing her father as a “Princeton graduate, an accomplished violinist and vocalist, but above all, an evangelist.” According to archivists at both Princeton University and Princeton Theological Seminary in Princeton, New Jersey, a search of avail-able appropriate databases could not verify “Princeton graduate” (oral communication to the author, Jan. 11, 2010). However, he further recalls her telling that he “consid-ered it his calling to go to untouched areas, start a church, and then, becoming restless, move on.” In the 1936 letter, R.A. Tichenor recalls the family living with Grandfather and Grandmother Drane and that Reverend Drane lived in Liberty about two years, preaching at Liberty Baptist Church, First Baptist Church at Natchez, and several churches in nearby towns. With this fam-ily influence and likely the move back to Mississippi from New York, the group relocated to Liberty in 1870. The history of
the Liberty Baptist Church notes the Rev. T.J. Drane serving as pastor through 1870 and lists G.H. Tichenor and Maggie Tichenor as among pioneer church leaders.24 There appears to be no evidence that he was in Liberty prior to this time. The Tichenor office was located behind the current historic court-house and, unfortunately, has been demolished (Figure 6).
The June 1870 Census lists George H. Tichenor, age 30, Physician, living in Liberty with wife Maggie and son, Rolla A. and daughter, Sallie E. They lived next door to Thomas J. Drane, Minister Gospel.42 It is in Liberty that the first official documentation of Tichenor with a license to practice medi-cine can be found.43 In November 2008 a volume was discov-ered in the historic Amite County Courthouse titled “License for Doctor’s and Merchant’s – Amite County” (Figure 7). It
Figure 6. G. H. Tichenor house (L) and office (R), Liberty, MS (Courtesy of Mr.
Joe B. Hoff, Gretna, LA)
• SpeciAl Article •
G. H. Tichenor, MD, and His Antiseptic Solution: The “Dr.” in Dr. Tichenor - Part 2 of 2
Michael C. Trotter, MD, FACS
[Last month’s issue of the Journal MSMA included “G. H. Tichenor, MD, and His Antiseptic Solution: The Mississippi Years - Part 1 of 2 {Trotter M. G. H. Tichenor, MD, and his antiseptic solution: the Mississippi years - Part 1 of 2 J Miss Med Assoc. 2012;53(3):88-92}. Part 1 focused on Dr. Tichenor’s early years, his legend in the Civil War, and his married life in Canton, Mississippi, from 1863-1868 when he was involved in the photography business and perhaps some type of medical practice while inventing and publishing. Here, we conclude with part 2 of 2.] —Ed.
128 JOURNAL MSMA April 2012
was a License Roll Book, and it begins April 11, 1861 and ends August 16, 1870. On July 25, 1870, G.H. Tichenor paid $10.00 for a 12-month license to practice medicine (Figure 8). The remarkable aspect about this book is its uniqueness – there were no others like it. It documents, in an official sense, the “Doctor” in Dr. Tichenor. This is likely the only documentation of G.H. Tichenor as a licensed M.D. in Mis-sissippi. To this day, medical licenses in Mississippi are valid for 12 months.
Of note, between July 23 and August 16, 1870, there were 41 total licenses recorded. These included:
• 17 M.D.’s with a license fee of $10.00 each10 lawyers with a license fee of $10.00 each4 druggists with a license fee of $25.00 each3 dentists with a license fee of $10.00 each3 retail dealers with a license fee of $200.00 each2 insurance agents with a license fee of $100.00
each1 wholesale dealer with a license fee of $50.001 broker with a license fee of $50.00
It appears Liberty was well supplied with doctors in 1870. Interestingly, one of the insurance agents listed was T.J. Drane. It is unclear what type of medical practice Tichenor had in Liberty. Business competition was keen. In his 1936 letter, R.A. Tichenor states that his father was using the antiseptic solution during this time.41
waKefield landing, mississippi
The final chapter in Mississippi began with a long distance commute to Wilkinson County, Mississippi, in December 1869. In the 1936 letter, R. A. Tichenor noted that his father moved to the area 45 miles south of Natchez on the Mississippi River.41 This area would later become known as Wakefield Landing and no longer exists as a town or commu-nity. While there, he prepared a home for his family whom he had left with his in-laws in Liberty. It is unclear if he was involved in the antiseptic solution business, the practice of medicine, or both. Perhaps he felt his opportunities were better closer to the Mississippi River. He planned to move his family there when he felt the time was appropriate. He visited his family monthly, sometimes taking three days to travel the 70 miles due to the rough terrain.41 Rev. T.J. Drane and family moved to Shreveport about a year later, in late 1870 or early 1871. It is possible that the antiseptic solu-tion was used clinically by Tichenor in Canton and perhaps earlier. It is probable that it was used in Liberty. In his 1936 letter, R.A. Tichenor notes that his father began bottling and selling the antiseptic solution while in the Wilkinson County home as well as practicing medicine.41 In the March 1977 let-ter, Edwin B. Tichenor notes that his grandmother remarked to him,“Grandfather made up his antiseptic on the battlefield at first.”37 This is the closest direct link to the ‘Legend’ and introduces the concept of accidental discovery. Edwin B. Tichenor recalls his grandmother telling him that his grand-father “had a place which served as a dispensatory and that he was constantly trying all sorts of proportions and methods, etc. She, as a sort of prank, poured something into one of his experimental batches and it led him to the ultimate answer.”37 Two more children, Waller Larue and George Humphrey, Jr., were born in 1871 and 1876, respectively.13
Figure 7. License Roll Book, Liberty, MS (Courtesy of the
author)
Figure 8. First medical license (Courtesy of Mr. Ronny
Taylor, Chancery Court Clerk, Amite County, Liberty, MS)
April 2012 JOURNAL MSMA 129
beyond mississippi The rest of the story is beyond the scope of this article but
will be chronicled in the future.44 It is worthwhile to look at a brief summary.
Tichenor moved across the river to Red River Landing, Louisiana, in 1877. He continued practicing medicine and developing his antiseptic solution, offering it for sale (Figure 9). He published a successful treatment for poisonous snake-bite (Figure 10) and developed a treatment for yellow fever. He also endured personal hardship and the impacts of epidemic disease and Mississippi River flooding. In 1884, he moved to Baton Rouge, and in 1885, he formed the partnership of
Tichenor & Sherrouse to further sales. Also in 1885, he was fully credentialed as a physician in Louisiana under Sections 3, 4, 5, and 8 of the 1882 Act 34 of the state legislature.
In 1888, he moved to New Orleans and continued to prosper. The Sherrouse Medicine Company, Ltd. was formed in 1893 with Tichenor as “Manufacturing Chemist” (Figure 11). The Louisiana State Board of Medical Examiners was created in 1884, and in 1899 Tichenor was issued License No. MD.B01846. The formula was sold and the Dr. G. H. Tichenor Antiseptic Company was formed by Arthur Parker and William Irby in 1905 (Figure 12). Tichenor remained as “Manufacturing Chemist.” He became active in the United Confederate Veterans
Figure 9. Early advertisement, Pointe Coupee Parish, Louisiana
Figure 10. Snakebite treatment
Figure 11. Sherrouse Medicine Co., Ltd. (Courtesy
of the Dr. G. H. Tichenor Antiseptic Company, New
Orleans, LA).
Figure 12. Dr. G. H. Tichenor Antiseptic Co.
(Courtesy of the Dr. G. H. Tichenor Antiseptic
Company, New Orleans, LA)
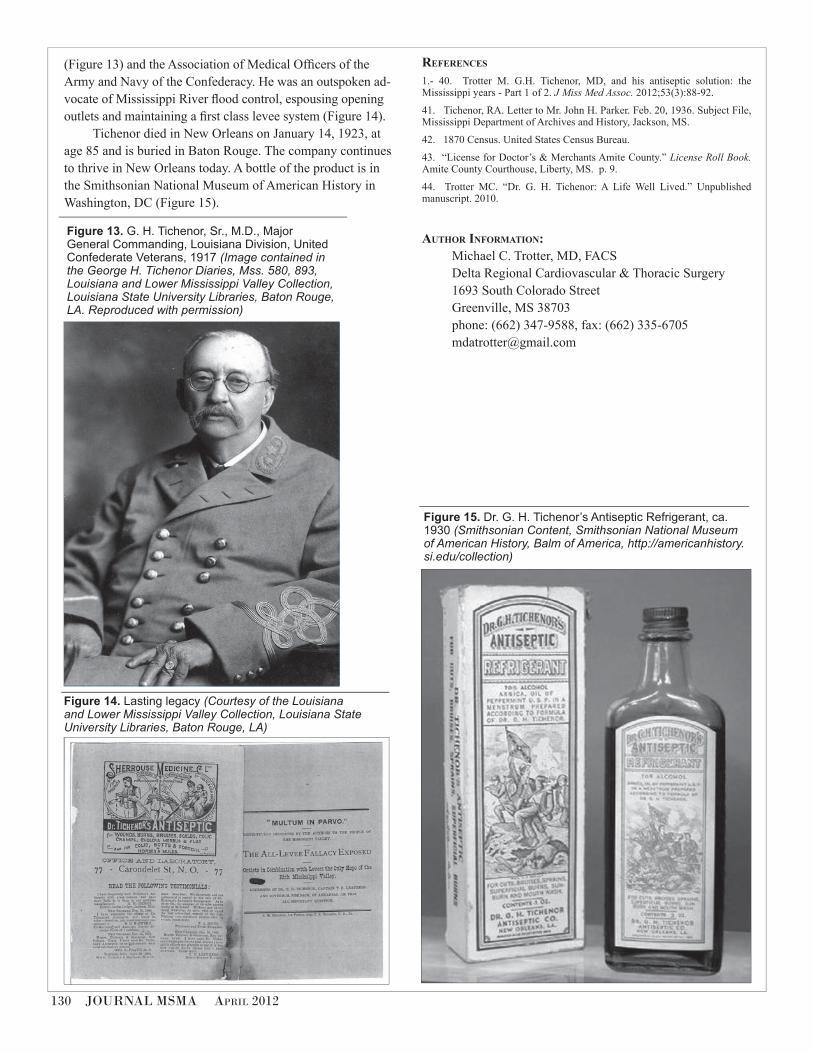
130 JOURNAL MSMA April 2012
Figure 15. Dr. G. H. Tichenor’s Antiseptic Refrigerant, ca.
1930 (Smithsonian Content, Smithsonian National Museum
of American History, Balm of America, http://americanhistory.
si.edu/collection)
Figure 13. G. H. Tichenor, Sr., M.D., Major
General Commanding, Louisiana Division, United
Confederate Veterans, 1917 (Image contained in
the George H. Tichenor Diaries, Mss. 580, 893,
Louisiana and Lower Mississippi Valley Collection,
Louisiana State University Libraries, Baton Rouge,
LA. Reproduced with permission)
Figure 14. Lasting legacy (Courtesy of the Louisiana
and Lower Mississippi Valley Collection, Louisiana State
University Libraries, Baton Rouge, LA)
(Figure 13) and the Association of Medical Officers of the Army and Navy of the Confederacy. He was an outspoken ad-vocate of Mississippi River flood control, espousing opening outlets and maintaining a first class levee system (Figure 14).
Tichenor died in New Orleans on January 14, 1923, at age 85 and is buried in Baton Rouge. The company continues to thrive in New Orleans today. A bottle of the product is in the Smithsonian National Museum of American History in Washington, DC (Figure 15).
references
1.- 40. Trotter M. G.H. Tichenor, MD, and his antiseptic solution: the Mississippi years - Part 1 of 2. J Miss Med Assoc. 2012;53(3):88-92.
41. Tichenor, RA. Letter to Mr. John H. Parker. Feb. 20, 1936. Subject File, Mississippi Department of Archives and History, Jackson, MS.
42. 1870 Census. United States Census Bureau.
43. “License for Doctor’s & Merchants Amite County.” License Roll Book. Amite County Courthouse, Liberty, MS. p. 9.
44. Trotter MC. “Dr. G. H. Tichenor: A Life Well Lived.” Unpublished manuscript. 2010.
author information:Michael C. Trotter, MD, FACS Delta Regional Cardiovascular & Thoracic Surgery1693 South Colorado StreetGreenville, MS 38703phone: (662) 347-9588, fax: (662) [email protected]
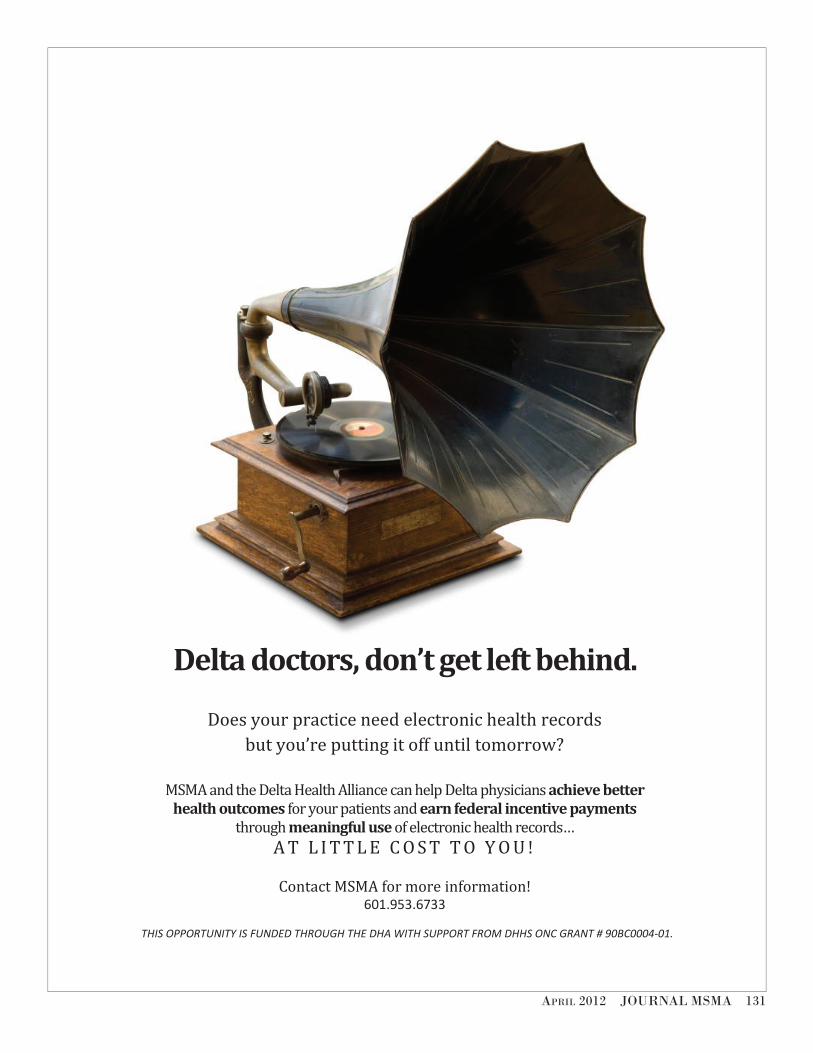
April 2012 JOURNAL MSMA 131
THIS OPPORTUNITY IS FUNDED THROUGH THE DHA WITH SUPPORT FROM DHHS ONC GRANT # 90BC0004-01.
Delta doctors, don’t get left behind.
Does your practice need electronic health records but you’re putting it off until tomorrow?
MSMA and the Delta Health Alliance can help Delta physicians achieve better
health outcomes for your patients and earn federal incentive payments through meaningful use of electronic health records…
A T L I T T L E C O S T T O Y O U !
Contact MSMA for more information! 601.953.6733
132 JOURNAL MSMA April 2012
Dr. Dwalia South and the Literary Terrains of Medicine
Dwalia S. South, MD
• phYSiciAn’S booKShelf •
Medical training is a great gift for a writer. The late physician-writer Walker
Percy once told me that smelly hospitals wards, besot with blood, feces, and urine, were more instructive training grounds for writers than ivy-coated centers of academia. The terrain of the physician is what a good writer needs: humanity’s sufferings, ills, and pathologies. The everyday practice of medicine offers a physician entrance into the intimate lives of our patients, allowing him or her to explore humanity from the inside out. Who in today’s society is privileged with such intimacy but a doctor? Pasternak’s Doctor Zhivago, fiction’s best drawn physician-writer, combined the two arts into one; Zhivago’s poetry was simply an extension of his medical healing. In a perceptive physician-writer, something rare exists: literary talent combined with intimate knowledge.
I was present at the birth of the Una Voce. Neither father nor mother, rather I was a frightened midwife, doing little more than allowing a natural process to occur, trying my best just to stay out of the way and not screw things up. As an Editor of the Journal of the Mississippi State Medical Association, one of this nation’s few remaining state scientific medical journals still published monthly, I asked the state’s best physician-writer to offer up a small page of reflection as a regular column to close out the journal each month. Dwalia South is that brilliant physician-writer, and for more than a decade, she had published numerous essays and poetry in diverse journals and magazines. She also was a past Associate
Editor of the Journal and had recently written an essay entitled “Putting the Car in the Garage,” which had struck a chord with our readership. Its printing had resulted in an almost continuous barrage of praise and interest by many of the Journal’s more than 4,000 readers. My job as Editor is to give the physicians something good to read, and it was more than evident that
our readers craved more offerings from Dwalia’s pen. Dwalia is a born writer, and while her writing is far from
effortless, she can write on a regular schedule and meet a deadline, something important for a monthly publication. So, she accepted my challenge, and the column was born. I still have a sheet of notebook paper Dwalia and I passed back and forth to each other while pretending to listen to a physician lecture. Among the column names we considered were: Southernisms, Parting Shots, Afterthoughts, The Last Word, The Last Appointment, and Last Call. We left the meeting settled on “Away with Words,” but in time, Dwalia found a better name for her column, “Una Voce,” a Latin phrase meaning “with one voice.”
As I said, Dwalia is the best physician-writer in Mississippi; she’s also one of the most versatile and insightful physician-writers alive. Like Anton Chekhov, John Keats, John Stone, and Walker Percy, hers is a medical tradition. However, medicine has not been her only influence. Many have compared her often humorous writings to Mark Twain, and there are similarities. However, her literary tradition is
Una Voce: A Collection,
by Dwalia South,
China Grove Press:
Magnolia (MS),
2011; 217 pages,
hardback, $27.95.

April 2012 JOURNAL MSMA 133
also that of the great Mississippi writer William Faulkner and his great-grandfather, the famous Col. William Falkner, a feisty railroad builder and war hero who was shot dead on the streets of her hometown of Ripley. Her great-grandfather South had served as an overseer for the Colonel before “the War,” as it is called in Ripley, and the Falkner, Murry, and South families have been marrying and intermingling for the last 150 years. Like Faulkner, Dwalia inherited her own little “postage stamp of native soil,” and it is the red clay hills of north Mississippi. Her sense of place is Tippah County; her voice is covered by the bark of the trees; it drips the undulations of the rolling hills. Since she was a little girl, when writer John Grisham sat behind her in the second grade classroom and pulled on her pigtails, she has absorbed the voices and traditions of this rural Southern community. In future years, I expect the prolific Grisham to remind interviewers that he once shared a classroom with the great Dwalia South, even once daring to pull her pigtails!
Dwalia is, in the words of Percy, a “literary clinician.” Percy, who was reared in Mississippi, wrote in an essay entitled “Diagnosing the Modern Malaise” that physician-writers possess a “certain set of mind…the diagnostic stance which comes so naturally to the physician-diagnostic at the outset, and in the end, one hopes therapeutic.” As observers, physicians study and record pathology and faults without judgment. Our perceptions should follow the scientific method, as is ingrained in medical training, based on reality and experience. Fact is not bent to fiction, and conclusions are based on evidence and not anecdote. For Percy and his literary mentor Chekhov, as writers, this perspective proved indispensible.
A physician’s eye not only seeks what is “real” but also perceives the world differently than others. A monster Laurel Oak leafless in stark silhouette against a gray winter sky and a yellow Mississippi field at sunset is seen by a physician-anatomist not as a lovely tree but as a perfect vascular system duplicating the body’s own vascular systems in close detail. The art of medicine requires all human senses: looking, touching, hearing, smelling, and, yes, even tasting, the human body and experience in all of its forms. (With taste, I don’t talk of cannibalism, but rather I offer the taste of an abscess which exploded rather than drained with incision or palpation!) Doctors experience vicariously dozens of patient lives daily.
The medical life affects each physician differently. Some protect themselves from the emotional stress with detachment and humor; some become cold and heartless and view the patient as an adversary. Others give their all, then blow their brains out, or turn to alcohol, drugs, or sex. All docs would prove fertile ground for a psychiatrist. However, when the heart and mind come together in a physician, a compassionate healer and a patient advocate
emerge. Medical schools and training need to explore ways to encourage the art of medicine and healing in our future physicians.
One important theme in this work is the perspective of the patient, provided especially by Dwalia’s experience with illness which in many ways spawned this project. A physician as patient is given a special insight into medicine, illness, and mortality. Chekhov and Percy both suffered from pulmonary tuberculosis. Hemoptysis and a hacking cough have special meaning in their work. The physician who experiences illness takes one step closer in intimacy with his patients, the final step beyond vicarious experience to actual experience. The physician as patient not only can see and treat the illness but also can truly know what it is like to look death in the eye and begin to fight. There is also an awakening in the physician-patient to the weakness in the art of medicine and the obstacles many other physicians never see in the provision of what is necessary for their patient’s healing. Patients takes their illnesses home with them after the clinic visit and sleep with them at night, awaking often overwhelmed with fear and many times alone. Physicians must do a better job of getting in the ditch with our patients and fighting with them along their sides.
As this volume is published, medicine is at a crossroads. Technology has become king, and the doctor-patient relationship, the center of medicine since Hippocrates, is being displaced by computers, insurance companies, physician extenders, telemedicine, and piles of paperwork. The art of medicine is disappearing as physicians are encouraged to spend their time typing into a handheld computer rather than touching their patients. These essays make clear that medicine’s last stand must be won by the only two who really care about the patient’s health: the doctor and the patient. Also, these essays reveal the indispensability of the physician’s voice in modern society. Physicians must remember Dr. Osler’s encouragement to his peers one hundred years ago, “Write down your thoughts and publish them.”
Physician writers often have had no formal training as writers and embrace the label “amateur.” These brilliant essays by this practicing physician reveal that there is no better training environment for writers in the twenty-first century than medicine. The physician-poet William Carlos Williams was known often to deliver a baby and afterwards pull out his prescription pad and scratch down a phrase or line of poetry which had come to him during the delivery. Medicine was the source of some of Doc Williams’s best poetry. After reading these essays, it is clear that more prose and poetry need to be published which has been first written on prescription pads.
—Lucius “Luke” Lampton, MD Editor
134 JOURNAL MSMA April 2012
more about una Voce (the booK)
Una Voce was already the most popular aspect of the Journal when I wandered in off of the street and took on the task of keeping it going
for Dr. Dwalia South when she was elected president of the Mississippi State Medical Association. I was happy to have the opportunity to fill in as its author for the next two years. I was not happy about why my tenure was extended. Dwalia at the end of her term in office was diagnosed with cancer of her parotid gland.
As an oncologist, cancer is something I deal with on a daily basis. For the past twenty-plus years I’ve been the confidant of patients as they stood in the shadow of death. During that time I’ve been privileged to share both the hopes and regrets of many of them. Some emerged from that shadow and some didn’t, but virtually no one got by unaffected by what they’d gone through.
My friend, Dwalia, was facing such a time in her life. She didn’t need me to care for her as a physician; her illness was already being managed by a group of caring and competent colleagues. It wasn’t until she got through her treatment that I felt that there was something I needed to do. The end of treatment is, in many cases, just the beginning of the road to recovery.
Cancer is much worse than a simple killer. A killer foiled is vanquished. Cancer on the other hand is a terrorist. It imparts a fear and a sense of limitations that doesn’t go away. It invokes a sense of loss and betrayal that is of such a personal nature that it’s difficult for anyone who has not experienced it to understand its depths. It is a loss of self. It is a betrayal of self. It is one’s own body that has betrayed and tried to kill.
That’s a difficult thing to get past. How can one escape an assailant that is oneself? It leads to obsession, depression, and a loss of hope for the future. I heard many of these things in my friend’s voice and asked myself, “What tool do I need? What tool must I be to help her now?”
Authoring a book represented the fulfillment of one of Dwalia’s life dreams and that was what I came up with. It has been delayed by the illness and loss of Robert Bitter, Dwalia’s beloved husband, a story she’s told more eloquently than I could ever hope to. But here, finally, is the story of a life, told in snatches of bright vision, like looking through a family photo album. Told by a wonderful author who has framed her own life in the stories she’s shared over the years.
—R. Scott Anderson, MD Chair, Journal MSMA Editorial Advisory Board
April 2012 JOURNAL MSMA 135
Small gene pool?Are medical journals headed for the endangered species list? Not on your
life. Scientific medical publications continue to be a primary source for up-
to-date data. Your Journal of the Mississippi State Medical Association is alive
and kicking. Immerse yourself. Read the Journal.

136 JOURNAL MSMA April 2012
rAlph lucIus brock, Md, of MccoMb— This month’s physician portrait is of Ralph Lucius Brock, MD, past MSMA President (1985-6), past MAFP President (1977-8), and for more than six decades a member of our MSMA. This third generation physician was born in Mt. Herman, Louisiana, but at seven months of age moved to McComb, and he has been
there ever since. He remembers his father, Dr. Lucius W. Brock, enjoying him recite at 3 years of age a speech which began, “I am going to be a doctor like my daddy…” He adds, “It never occurred to me to do anything else.” .
Ralph went to college at Ole Miss, then graduated from the two year medical school there, before finishing his medical training at Tulane. He then did a one year rotating internship at Charity Hospital in New Orleans. He remembers getting paid $10/month during this internship, and he notes that an additional $1.50 in taxes was taken out of that pittance. After his year at Charity, he returned home to join his father and brother Jim in their medical practice, which was the great era of family practice: full clinics without appointments (first come, first serve), hospital rounds, house calls, surgery, and delivering babies. He began his practice of medicine in July 1949 and retired in August 1995.
In McComb, “Dr.Ralph,” as he became known (to distinguish him from his doctor father and doctor brother), became a beloved icon and a respected physician leader. He would practice with his father for 15 years, and from him, he learned many things: a strong work ethic, the importance of the patient/physician relationship, and the pride of our profession. He explained, “My father impressed upon me the pride of being a doctor, that being a part of this profession means something! If I go out in the public now, I want to look like a doctor.” When asked about the future of medicine, he laments, “There are now too many people between the doctor and the patient in the doctor/patient relationship!”
In the photograph, Ralph is wearing what he calls his “New Orleans uniform,” a blue cotton seersucker suit. He’s standing in front of his church, J. J. White Presbyterian Church, McComb’s historic church named after one of the town’s earliest lumber barons (who also was father to a Mississippi Governor). He grew up and was baptized as a Baptist, but his beloved wife Billie was a “dyed in the wool” Presbyterian who slowly pulled him away from the Baptist fold. He’s been a member of J. J. White for 50 years, and it remains one of the most meaningful aspects of his life. Photo by Donna DeLee.
— Lucius M. Lampton, MD JMSMA Editor
• ASclepiAd •
What’s Your Specialty?
Our specialty
is NETWORKING...
Sponsored by the Mississippi State Medical Association
Physicians CareN E T W O R K
M I S S I S S I P P I
PhysiciansHospitals
Employer
Groups
TPAs
Insurance
Companies
Ancillary
Providers
MPCN - THE OBVIOUS CHOICEChange Networks. Not Doctors.
601-605-4756 • www.mpcn-ms.com
In a life settlement agreement, the current life insurance policy owner transfers the ownership and beneficiary designations to a third party, who receives the death proceeds at the passing of the insured. As a result, this buyer has a financial interest in the seller’s death. When an individual decides to sell their policy, he or she must provide complete access to his or her medical history, and other personal information, that may affect his or her life expectancy. This information is requested during the initial application for a life settlement. After the completion of the sale, there may be an ongoing obligation to disclose similar and additional information at a later date. A life settlement may affect the seller’s eligibility for certain public assistance programs, such as Medicaid, and there may be tax consequences. Individuals should discuss the taxation of the proceeds received with their tax advisor. ValMark Securities considers a life settlement a security transaction. ValMark and its registered representatives act as brokers on the transaction and may receive a fee from the purchaser. A life settlement transaction may require an extended period of time to complete. Due to complexity of the transaction, fees and costs incurred with the life settlement transaction may be substantially higher than other securities.
Securities Offered Through ValMark Securities, Inc. Member FINRA, SIPCInvestment Advisory Services Offered Through
ValMark Advisers, Inc. a SEC Registered Investment Advisor130 Springside Drive, Suite 300 Akron, Ohio 44333-2431* 1-800-765-5201
Executive Planning Group is a separate entity from ValMark Securities, Inc. andValMark Advisers, Inc.
Have You Considered a Life Settlement For Your Old Life Insurance Policy?
What is a Life Settlement?A life settlement is the sale of an existing life insurance policy on the secondary market to a third party investor.
Who or What May Qualify?
Why Use a Life Settlement? Term life insurance policy will expire
Old policy that is no longer needed or premiums cannot be paid
A policy that was purchased for a business buy/sell and is no longer needed
A policy was purchased for a business that has been sold or is not needed
There may be a better policy available at a lower cost
Estate value has changed and the policy is no longer needed
If the person insured by the policy is age 70 or older
If the person insured has any major medical conditions
If the policy has a death benefit of $250,000 or more
Policies including, but not limited to, universal life, term insurance, variable life insurance or whole life insurance
If any cash value exists in the policy, the amount is relatively small
For More Information on Life Settlements, contact:
H. Larry Fortenberry, CPA, CLU, ChFCExecutive Planning Group, PA
1640 Lelia Drive, Suite 220PO Box 16566
Jackson, MS 39216(601) 982-3000


























