Embed Size (px)
Citation preview

Endodontic Posts vs Bonded Cores
By John I. Ingle, DDS, MSDSan Diego, CA
I recently read an article in Parkell Todayby Dr. Martin Goldstein suggesting that inthis Adhesive Age we now live in, perform-ing elective RCT on a vital broken-downtooth solely to retain a post and core is oftenunnecessary – perhaps even over-treatment.
That article inspired me to tell you thehistory of my lower left first molar.
I have a long personal history of fractur-ing teeth, molars and premolars. Deep fossaeand steep cusps seem to be the contributingfactor.
My first fracture was when I was in den-
tial, it occurred to me that Parkell hadn’t revis-ited the technique in quite a while. So I thoughtI’d photograph the case and pass it on alongincluding a few of my personal embellish-ments.
By Mike Barr, DDSBoynton Beach, FL
We all know what a pain it can be when youhave to crown a tooth that’s serving as an abut-ment for a perfectly good clasped partial.
Problem #1: Persuading the patient to sur-render the RPD for a week.
Problem #2: If it’s an anterior bridge, ofcourse, you’ll have to make a flipper.
Problem #3: Then you have to very care-fully pick up the partial in an impression.
Problem #4: And whenthe crown comes back fromthe lab – well, you betterschedule an hour for adjust-ments.
The traditional approachnever worked very well inmy hands. I usually had tospend a lot of time adjust-ing the finished crown –and even then the fit wasn’tterrific. I suspect the prob-lem was the transferimpression. With every-thing hidden by a loadedfull-arch tray, it’s very diffi-cult to assure that the partialis both completely seated inthe mouth and passive.
A number of years ago I ran across an arti-cle in Parkell Today by Dr. Allen Weiner ofMedfield, MA describing how to quickly-and-precisely register the relationship between theclasp and the preparation. The technique hadthe obvious advantage of permitting the patientto continue wearing the removable partial den-ture while the crown was being fabricated. (Noneed for anterior flippers!) Less obvious wasthe fact that this new technique producedmuch, much better fitting crowns. At leastthat’s been my experience.
When a patient recently presented requiringa crown on #29, abutment for his free-end par-
300 Executive Drive, Edgewood, NY 11717 • (631) 249-1134 • Fax: (631) 249-12421-800-243-7446 • E-Mail: [email protected] • Visit our Website: www.parkell.com
April 2008
Our 60th Year - Quality System Certified to ISO 9001/ISO 13485VISIT PARKELL AT MAJOR DENTAL MEETINGS:m CDA Anaheim (May 2-4) m San Antonio - ADA (Oct 16-18)m Greater New York (Nov 25-28)
PRIORITY NO.2599
PRSRT. STD.U.S. PostagePAIDIthaca, N.YPermit No. 45
© 2008 Parkell, Inc.
CROWN UNDER CLASP - REDUXHere’s how to create a new crown that fits an old clasp like
a glove, AND THE PATIENT DOESN’T EVEN HAVE TOSURRENDER THE PARTIAL
About the author:A 1988 graduate ofthe University ofTennessee College ofDentistry, Dr. MichaelBarr operates PalmBeach Smiles inBoynton Beach, FL,focusing on cosmeticand reconstructivedentistry. A sought-after speaker who hasserved as a Clinical Instructor in Dr.Larry Rosenthal’s participation courses,Dr. Barr has written numerous articles inboth professional journals and consumermagazines. He can be contacted at [email protected].
Continued on page 22
Because I sent the resin template (below) to the lab, the patientwasn’t forced to surrender the partial dentire. Furthermore, thecrown fit perfectly – so I saved perhaps 45-minutes of crown adjust-ments.
Figure 1: After completing crown propara-tion, express Blu-Mousse over the tooth, seat thepartial and express some more. (You’ll save timeduring trimming if you quickly wipe away someBlu-Mousse to expose the surface of the clasp andocclusal rest.)
Figure 2: When you remove the partial theBlu-Mousse matrix will come with it.
What little remained of mymolar was absolutely flat (seesketch). The bonded amal-gam core and the crown thatrestored it have served menow for 18 years – and are still going strong.
Continued on page 2
Kevin D. Huff, DDS, MAGD Dover, Ohio
Last December Parkell Today printed anarticle by Dr. Bob Obradovich (Apollo, PA)discussing how adhesive C&B-Metabondfrequently helps him find solutions when theideal textbook treatment isn’t an option dueto biological limitations, economicrestraints, or patient preference.
There are, of course, many ways to man-age any given situation1,2. It is the dentist’sethical challenge to find what he considersto be the most appropriate treatment option.In certain situations, a creative “non-text-book” use of material such as those in Dr.Obradovich’s article are not only “ethical”,but actually the preferred treatment option.For example, on numerous occasions, I haveused an adhesive cement to “get the extramile” out of periodontally compromisedmandibular incisors.
Using C&B-Metabond fordirect provisional periodontalsplints is certainly not a newconcept. In fact the techniquewas illustrated by Dr. KenjiIchimura in Parkell Today sev-eral years ago.3 Since then, Ihave used C&B-Metabond forthis purpose at least fifteen
times, and I have been very impressed!
On at least two occasions, I have used itto “ponticize” a hopeless tooth as a provi-sional restoration. Here the tooth wasextracted, the root removed, and the clinicalcrown bonded to the proximal teeth withC&B-Metabond (See Side-Bar page 4).Because the tooth was endodontically treat-ed, a 1mm X 2mm horizontal groove wasprepared mesial distally to serve as a con-nector, and a dentin pin was placed from thelingual for retention of this “support”. (This
Metabond: An Adhesive or a Splint?The patient presents with mobile mandibular anteriors,
including a central judged “hopeless” by the periodontist.Here’s how to stabilize the arch - and preserve the hope-less tooth (at least for now) – in a one-appointment pro-cedure that will allow easy future modification.
About the author: Kevin D. Huff,DDS, MAGD practices general den-tistry in Dover, Ohio. A graduate of theOhio State University College ofDentistry and alumnus of the PankeyInstitute, he is a dedicated CE attendee,frequent speaker on dental matters, anda Clinical Instructor at the Case Schoolof Dental Medicine. He can be contact-ed at [email protected].
Continued on page 4
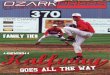
Figure 1: The patient’s mandibular ante-riors showed Class II mobility. Number 24had a guarded prognosis.
Why a resilient composite reduces
leakage and popout inclass V restorations
(page 14)
Take a great impression andsave 50% or more over other
good vinyls(page 23)
Armor-clad your crown prepsto resist sensitivity, pulp damage and a lot more.
(page 12-13)
Noteworthy in this issue ...

was probably unnecessary, but I’m still fair-ly “old school”.) In this situation, I couldnot ethically justify conventional dentistry,such as an FPD or even a cast bonded splintdue to potential financial investment. Sincethe potential abutment teeth had guardedprognoses, conventional dentistry mighthave been considered overtreatment.However, premature edentulation wouldhave caused these patients undue harm.C&B-Metabond allowed me a reasonablealternative treatment to help the patient pre-serve bone for as long as possible. Althoughthe patient and I only hoped for a year or so,those “bridges” are still functioning after 4and 6 years, respectively!
Most recently, a patient presented with aquestionable, but still vital, tooth number 24.A well-respected periodontist had previous-ly attempted connective tissue grafting with-out success, and he had informed the patientthat tooth number 24 would eventuallyrequire extraction. Teeth numbers 22-27showed with class II mobility. For stability,the patient had been wearing a removableHawley orthodontic appliance. (Figures 2and 2a).
Implant therapy to replace tooth number24 was contraindicated due to the lack ofkeratinized gingiva in that site, and he didnot want to sacrifice any more teeth thanwere absolutely necessary. The adjacentteeth were mobile, which posed a relativecontraindication to a conventional fixed par-tial denture, but they had been given a favor-able prognosis by the periodontist.
The patient, the periodontist, and I decid-ed to preserve number 24 as long as possibleand provisionally stabilize the mandibularanteriors using a direct C&B-Metabondadhesive splint. According to Parkell, peri-odontal splinting is the second-most-popularMetabond application in Japan … right nextto crown retention.4 Unlike composite,C&B-Metabond creates proximal connec-tors that are slightly resilient, so they resiststress build-up that can cause fracture anddebonding. Unlike a composite splint withfiber reinforcement, a C&B-Metabond splintis very easy to repair or modify.
When the time comes to ponticize toothnumber 24, there will be several options.Assuming that the adjacent teeth are still sta-ble, a logical choice may be to record thetooth position with a Blu-Mousse matrix,extract the tooth and remove the root, andthen rebond it in place with fresh Metabond.More likely, the tooth could be left in place,the root amputated and removed, and theintaglio surface recontoured in situ.
The procedure to fabricate the C&Bsplint took a total of 40 minutes, and most ofthat was patient preparation time. Step-by-step:
1. A rubber dam was placed from premo-lar to premolar for adequate isolation.
2. The teeth were minimally abradedinterproximally using an ultrafine diamondin a high-speed handpiece. This mechani-cally removed chlorhexidine residue andaccretions (Figure 3). (Some studies alsosuggest than enamel bonds are strongerwhen the surface of the enamel has beenbroken.)
3. Flexible wedges (Flexi-Wedge,Commonsense Dental, Nunica, MI) weregently placed to maintain hygienic gingivalembrasures (Figure 4).
4. Red enamel etchant was appliedaccording to manufacturer’s instructions(Figures 5 and 6). The teeth were rinsedand dried.
5. The “brush bead” technique was usedto mix C&B Metabond (4 drops+1 drop cat-alyst+ clear powder as needed for consisten-cy), and it was applied it to the lingual con-tact areas of the mandibular anterior teeth,filling the lingual embrasures. The gingival,incisal, and facial embrasures were avoidedfor esthetics.
Editor’s Note: The C&B-Metabond kitcomes with two jars of powder. One createsa white, very opaque/radiopaque cement forapplications where dark shades must bemasked or the cement must show up on afilm. The other powder produces aclear/radiolucent cement film. For thisapplication you want the clear powder.
6. Ultrafine diamonds in a conventionalhigh-speed handpiece with copious waterspray were used to shape and polish theextracoronal provisional splint after 5 min-utes setting time (Figure 7).
The final splint was stable, esthetic, andhygienic. (Figure 8).
4
The ponticized toothWhen number 24 required extraction, the
poor periodontal condition of the proximalteeth made the prognosis for a traditionalfixed bridge questionable.
A Blu-Mousse registration index wasmade to accurately record the tooth posi-tion. After extracting the tooth, which hadbeen previously endodontically treated, theroot was smoothed and rounded apically tocreate an anatomic pontic and a conserva-tive lingual channelwas prepared toenable bulk of theresin. A horizontalretentive pin wasplaced to counteractrotational dislodge-ment, but this may nothave been necessary.Then, using the regis-tration to reapproximate the correct positionof the “pontic”, the clinical crown wasbonded to the proximal teeth using C&B-Metabond. The C&B-Metabond was alsoapplied to the interproximal contacts fromteeth numbers 22—27 to stabilize theremaining mobile incisors.
The original intent was for the pontic tofunction for approximately a year. However,this alternative treatment has proved suc-cessful for six years and is still fully func-tional. This photograph and radiographwere taken at the 6-year recall.
EDITOR’S NOTEWhere C&B-Metabond alone
isn’t enough
Notice that Dr. Huff limits his use ofC&B-Metabond stabilization to mobilemandibular teeth. In the maxilla, whereforces are substantially greater, we rec-ommend reinforcing the resin with a wireor fiber strip.
For more than a decade direct splint-ing with C&B-Metabond has been com-mon in Japan in lieu of the traditionalremovable retainer.5,6 However, the forcesinvolved in relapse after orthodontictreatment are substantial, so an additionalreinforcing element is virtually alwaysadded to the adhesive.
In fact, when Dr. Ryan Swain (Chili,NY) tested the use of unreinforced C&B-Metabond after short-term ortho, hefound a high incidence of fracturethrough the interproximal resin.7
Figure 2: The patient had a history ofsevere periodontal disease, and previousattempts at gingival grafting had failed.
Figure 2A: Teeth 22-27 showed classIImobility.
Figure 3: Using a fine diamond the prox-imal enamel was lightly abraded.
Figure 4: Flexible wedges were gentlyplaced, not to separate the teeth, but to cre-ate natural embrasures.
Figure 5: C&B-Metabond’s red etchantwas applied to the proximal surfaces andextended onto the lingual and facial.
Figure 7: After the C&B-Metabond hadset (approximately 8 minutes) the surfacewas mechanically shaped and polished.
Figure 8: The resulting provisional splintwas virtually invisible. (The wide embra-sures should facilitate hygiene.)
1 Sadowsky D. The moral dilemmas of the mul-tiple prescription in dentistry. J Am Coll Dent.1979;46:245.
2 Huff, K., Farah, C., and Huff, M. Ethical deci-sion making for multiple prescription dentistry. GenDent. In press.
3 Ichimura K, et al. A 15-minute adhesive splintfor mobile teeth, Parkell Today. p5 Sept 03
4 Mitsugi H. Durability of splinting. ADHESIONCLINIC. P141-144 1996
5 Mogi M. Making Effective Use of WisdomTeeth. DENTAL OUTLOOK. 94:1, p40-57 1999
6 Mogi M. Making Effective Use of WisdomTeeth. DENTAL OUTLOOK. 94:2, p270-289 1999
7 Swain R – personal communication.
Metabond: An Adhesive or a Splint?(continued from page 1)
Figure 6: After the etchant had remainedon the enamel for 30-secs, the teeth wererinsed and dried, and the C&B-Metabondwas applied using a brush-bead technique.
The phone call came in about 6:15 pmEST.
“I’ve received Parkell Today for years. Ifigured it was just advertising, so I alwaystossed it away without cracking the cover.
For some reason, I really looked at it forthe first time today ... and I wound up read-ing it from cover to cover. There were 3 or4 clinical tips in there I can use.
If I promise to pay better attention in thefuture, can I get some past issues?”
Dr. Paul DodsworthSalida, CO
Unfortunately, we don’t save old issues ofParkell Today. If we did, we’d be up to our eye-balls in paper. Nevertheless, we managed toscrape up a couple to mail to the good doctor.
Sure, it’s advertising. But not “JUST”advertising.
I won’t deny it. Our ultimate objective inpublishing this catalog is to generate orders.It’s pure, blatant capitalism. However we have
an insidious, underhanded way of approachingit.
We figure that if, along with the advertising,we also offer some serious clinical articles -things you can put to work in your practice -maybe we can trick you into reading ParkellToday even when you're not in the market forour products. (And if the articles are really,really good, who knows? You may even save itfor future reference!)
That way, when you do need something -you’ll remember us.
We work a lot harder on the articles thanthe advertising.
Believe it or not, Parkell Today was the firstpublication in the US to discuss the hybrid-layer theory of bonding. (Back in 1989 mostgurus thought the primary bonding mechanismwas resin tags in tubules. At the time, severalgurus told us we were crazy.)
Parkell Today was the first publication topresent the concept of bonded amalgams. (Theeditor of General Dentistry told us we werecrazy.)
It was one of the first to discuss Gary
Schoenrock’s laminar impression technique -as well as Rod Kurthy's recent modification ofit.
Dr. Masaka's technique for adhesive repairof fractured teeth has been described in detail inJapan and France and Germany - but here in theUS? Only in Parkell Today.
We now get so many requests for past arti-cles, we’re starting to post as many as possibleon our website for fast reference(www.parkell.com).
But if you don’t look at this magazine,you’ll ruin our plan.
So even if you’re not in the market for den-tal products at the moment, please thumbthrough this issue. There’s something in hereyou can use.
STOP! Before you throw away this magazine, READ THIS!
CEO-Parkell