Embed Size (px)
Citation preview

Atrial fibrillation (AF) is the most prevalent sustained arrhythmia associated with an increased risk of stroke and global mortality. Warfarin use is limited by its narrow therapeutical range. Therefore, time in therapeutic range (TTR) assessment is a crucial tool to determine if patients have an increased risk of haemorrhagic or thromboembolic complications.
• Increase in therapeutic safety and effectiveness. • Global improvement of 9.83% on TTR • Decrease of 15% of patients with labile INR (<70%) • Globally, there was an improvement in the control of anticoagulated patients.
Improve therapeutic anticoagulation control of patients under treatment with warfarin aiming to increase patients TTR to over 70%
Patient's Safety Anticoagulation monitoring
on atrial fibrillation A. Borges, M. Alves Freire
USF Santa Maria Benedita – ACES Oeste Norte – ARSLVT (Portugal)
Introduction
Sample selection: Adult patients with Atrial Fibrillation (K78, ICPC2) Data extraction: Medical records
Process:
1. Identify patients with atrial fibrillation diagnosis at July 2015
2. Through 01/10/2015 – 31/03/2016 evaluate TTR based on assessment of
INR records (Rosendaal method)
3. Apply an internal protocol on Warfarin Anticoagulation and handouts distribution
4. Reassessment of TTR through 01/05/2016 – 31/10/2016
5. Comparison between first and second assessment
Methods
Goal
Exclusion criteria
- No-anticoagulation - Warfarin start after data collection - Patients under NOACs - Out-patient INR monitoring - Uncertain diagnose - Death - Switch to NOACs during the evaluation - <5 INR records per period - Hospitalization - No records
Conclusions
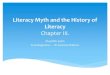
Results
20 17
3
26
13
1
>70 % 30-70% <30%
First Second
105 AF Patients
40 included
65 excluded
Decrease 15% of patients with labile INR
Global raise of 9.83% on mean TTR
60% - 40% 73yo
(median)
Bibliography: Camm AJ, Lip GY, De Caterina R, et al. “2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association”. Europace 2012;14:1385–413; Tideman P et al, “How to manage warfarin therapy”. Aust Prescr. 2015 Apr; 38(2): 44–48; “Anticoagulantes orais: recomendações para a prevenção de tromboembolismo na fibrilação auricular”; Boletim Terapêutico, nº5/2013.