Embed Size (px)
Citation preview
1112 Journal of Pain and Symptom Management Vol. 45 No. 6 June 2013
Brief Methodological Report
Appropriateness and Reliability Testing of theModified Richmond Agitation-Sedation Scalein Spanish Patients With Advanced CancerMiguel Angel Benıtez-Rosario, MD, PhD, Manuel Castillo-Padr�os, MD,Belen Garrido-Bernet, MD, Toribio Gonz�alez-Guillermo, MD,Luis Pedro Martınez-Castillo, MD, and Aceysele Gonz�alez, MD, and Members ofthe Asocaci�on Canaria de Cuidados Paliativos (CANPAL) Research NetworkThe Palliative Care Unit (M.A.B.-R., M.C.-P., T.G.-G., L.P.M.-C., A.G.) and Internal Medicine Unit
(B.G.-B.), NS Candelaria University Hospital, Tenerife, Spain
Abstract
Context. A tool to quantify agitation severity and sedation level in patients withadvanced cancer is needed.Objectives. To test the appropriateness and reliability of the Richmond
Agitation-Sedation Scale (RASS) in Spanish patients with advanced cancer.Methods. The original RASS was translated into Spanish according to the
standard guidelines. Face validity was assessed by members of the palliative careteam, and interrater reliability was assessed, using a weighted kappa, fromobservations of patients admitted to the palliative care unit. The associationbetween scores of the RASS, Ramsay Sedation Scale, and Glasgow Coma Scale wasevaluated using Spearman’s r.
Results. Three hundred twenty-two observations were performed in 156 patients:116 observations were performed for delirious patients, 76 observations for sedatedpatients, and 130 observations for patients admitted for other symptom control. Theweighted kappa values were practically equal to or greater than 0.90 between nursesandnurses andphysicians.Theagreement levelbetweenobservers foreachRASSscorewas roughly 90%. The correlation between the RASS and the Ramsay and GlasgowScale values was analyzed for 196 observations recorded in 80 patients. The sedationscale of theRASShad a strong correlationwith both theRamsay (Spearman’s r,�0.89;P < 0.001) and the Glasgow Coma Scales (Spearman’s r, 0.85; P < 0.001).
Conclusion. These data support the use of the RASS in Spanish patients withadvanced cancer. J Pain Symptom Manage 2013;45:1112e1119. � 2013 U.S.Cancer Pain Relief Committee. Published by Elsevier Inc. All rights reserved.
Key Words
RASS, agitation scale, sedation scale, palliative care, advanced cancer patientsAddress correspondence to: Miguel Angel Benıtez-Rosario, MD, PhD, P.O. Box 10521, SC Tenerife,Spain. E-mail: [email protected]
Accepted for publication: June 3, 2012.
� 2013 U.S. Cancer Pain Relief Committee.Published by Elsevier Inc. All rights reserved.
IntroductionThe availability of a tool to quantify agitationseverity and sedation level facilitates the de-scription of the clinical characteristics and
0885-3924/$ - see front matterhttp://dx.doi.org/10.1016/j.jpainsymman.2012.05.015

Vol. 45 No. 6 June 2013 1113Validation of the RASS in Spanish Cancer Patients
treatment monitoring of patients with ad-vanced cancer, such as those with deliriumand those undergoing palliative sedation ther-apy. Delirious patients can suffer a wide rangeof clinical situations, from severe agitation tointense somnolence, resulting from both theclinical expression of hyper- or hypoactive de-lirium and the treatment.1,2 Palliative sedationtherapy is the monitored use of medicationsintended to induce a state of decreased or ab-sent awareness (unconsciousness) to relievethe burden of otherwise intractable suffer-ing.3,4 In these clinical situations, the Rich-mond Agitation-Sedation Scale (RASS) couldbe useful for evaluating patients’ agitation orreduced awareness.
The RASS was developed by Sessler et al.5 toassess the level of consciousness and agitatedbehavior of patients admitted to an intensivecare unit. The validity and reliability of thescale have been established in intensive careunit patients,5e9 but, to the best of our knowl-edge, the tool has not been validated in otherpatient care settings. Therefore, we designedthe present study to test the appropriatenessand reliability of the RASS for use with Spanishpatients with advanced cancer.
MethodsTo evaluate the appropriateness and useful-
ness of the scale, we tested the 1) face validity,2) correlation of the RASS scores with those ofboth the Spanish versions of the Ramsay Seda-tion and the Glasgow Coma Scales, and 3) in-terrater reliability. Permission to use the toolwas obtained from the developers of the origi-nal scale via e-mail.
Translation and Face ValidityThe original RASS was translated into Span-
ish according to the standard guidelines, in-volving forward and backward translation.10
The RASS has a single-item numerical structurethat involves the description of four levels ofagitation (from þ1, restless, to þ4, combative)and five levels of sedation (from �1, somno-lence, to �5, to unarousable) (Appendix).5,6
Each level of agitation and sedation is estab-lished according to precise definitions, whichinvolve the patient’s behavior or response tocommon stimuli. The levels are designated
with both numbers and words (e.g., restless,somnolence, and so on), closely related tothe clinical situation.
The face validity of the tool was initiallytested by nurses and physicians of the palliativecare (PC) team in five patients with differentclinical conditions. After this evaluation, ameeting was held to discuss whether theRASS was a feasible and clinically useful mea-surement of agitation and reduced conscious-ness in patients with advanced cancer.
Evaluation of Both Interrater Reliability andCorrelation of the RASS With Other SedationScales
The study was performed between January2008 and January 2010 in patients who wereadmitted to the PC unit on the day of the as-sessment; no exclusion criteria were applied.The study was carried out independentlyfrom the inpatient care physicians, so the treat-ment of the patients was not influenced by theresearch. All patients or, in the case of patientswith delirium or reduced consciousness, theirrelatives received a full explanation of thestudy and provided verbal consent.
PC physicians and PC nurses andmedical res-idents were considered, for methodologicalpurposes, observers. The observers, who wereunaware of each other’s assessment, recordeda RASS score for every patient during a three-minute encounter with them. Several observerscould simultaneously evaluate a patient duringan encounter, but the observation teams werealtered in the different encounters. The pa-tients could contribute to more than one mea-surement; however, measurements were doneon different days, which were established ac-cording to the availability of each health profes-sional to process the assessment. The scores ofthe Ramsay Sedation and Glasgow Coma Scalesalso were recorded during the observation ofnonagitated patients. Testing with the RASS ag-itation scale was performed, following bedsidenurse detection, in the first minutes of the pa-tient’s agitation crisis until the tranquilizertreatment became effective.
Data CollectionPatient data collected from the medical
chart included age, gender, type of cancer,presence of delirium, and palliative sedationor reduced consciousness by the illness.

Table 1Patient Characteristics
Characteristic n (%)
Sample size, N 156Age, years, mean (range) 69 (31e98)Gender (male/female) 83(53)/73(47)Primary cancerGenitourinary 42 (27)Gastrointestinal 51 (33)Lung 23 (15)
1114 Vol. 45 No. 6 June 2013Benıtez-Rosario et al.
According to the protocols of the PC unit, thediagnosis of delirium was made using criteriafrom the Diagnostic and Statistical Manual ofMental Disorders, Fourth Edition, supported bythe Mini-Mental State Examination.11 For thepurposes of this study, we used the expressionpalliative sedation therapy as an equivalent totransitory or continuous slight or deep pallia-tive sedation.12
Statistical AnalysisFor the analysis, the following observer pairs
were established: PC physician-PC physician,PC physician-PC nurse, PC nurse-PC nurse, PCphysician-medical resident, PC nurse-medicalresident, andmedical resident-medical resident.The PC physician researcher involved in the en-counter with the patient was considered as themain observer; therefore, PC physician ratingswere used as the reference of clinical status inthe RASS. The RASS scores established at everyencounter were considered independent mea-surements, without connection to the assess-ments carried out on other days by differentobservers. Patients with reduced consciousnesssecondary to advanced cancer or pharmacologictreatment, including palliative sedation therapy,were considered as a single group named ‘‘re-duced awareness.’’
A weighted kappa was used to measure theagreement for data between observers. Kappavalues of more than 0.8 and more than 0.6were considered to have ‘‘very good’’ or ‘‘sub-stantial’’ agreement, respectively.13 The meanof the percentage of agreement between theobservers was used to describe the interraterreliability of each item of the RASS. The asso-ciation between scores of the RASS, Ramsay Se-dation Scale, and Glasgow Coma Scale wasevaluated using Spearman’s r. R version2.11.1 (The R Foundation for Statistical Com-puting, www.r-project.org) was used for statisti-cal analysis.
Brain 10 (6)Breast 5 (3)Others 25 (16)
Clinical situationDelirium 57 (37)Palliative sedation 38 (24)Othera 61 (39)
Analgesic and sedative drugsStrong opioids 142 (91)Neuroleptics 50 (32)Midazolam 45 (29)
aPalliative care unit admission for pain, dyspnea, vomiting, orother symptom control.
ResultsPhase 1
The face validity of the RASS was examinedby the PC team, which comprised seven physi-cians and 10 nurses with more than five yearsof PC experience. The team considered theRASS to be a very useful tool for assessing
agitation and sedation levels in patients withadvanced cancer, with a good sensitivity fordescribing clinical change. The fact that bothagitation and sedation scales were representedin a single tool could facilitate fluid communi-cation among the PC team about patients’level of sedation or agitation and treatmenttitration. However, the team considered thefollowing modifications to be necessary tocomprehend the whole clinical picture ofpatients receiving PC: 1) removal of the refer-ence to assisted ventilation from the definitionof agitation level and 2) an addition that ad-dressed the fact that the RASS score þ1, orrestless, can be present in patients who arenot fully alert (the aforementioned modifica-tions are included in the RASS described inthe Appendix).
Phase 2The study was undertaken in 156 patients
with advanced cancer who were admitted forsymptom control or end of life care to the Pal-liative Care Unit of the University Hospital ofLa Candelaria, Tenerife, Spain. Table 1 sum-marizes the most relevant patient characteris-tics. Ten PC nurses, three PC physicians, and23 residents from several medical specialties(four oncologists, three internal medicine phy-sicians, and 18 family medicine physicians) re-corded the RASS scores.

Vol. 45 No. 6 June 2013 1115Validation of the RASS in Spanish Cancer Patients
Three hundred twenty-two observationswere performed in 156 patients, with a medianof 2 (range 1e3) observations per patient, fortesting the RASS interrater reliability. At leastone PC physician from the research team wasinvolved in every observation; the PC nurseswere involved in 96 observations and the resi-dents in 196 observations. A total of 116 obser-vations were performed for delirious patients,76 observations for reduced awareness pa-tients, and 130 observations for patients ad-mitted for other symptom control. Table 2summarizes the RASS score distribution ac-cording to the records of the main PC physi-cian. The 322 RASS scores ranged from �5to þ3; scores of þ4 were not present. Roughly50% of RASS scores were in the sedation-somnolence range and 8% in the agitationrange. Most of the RASS scores recorded fordelirious and reduced awareness patientswere in the sedation range, but in nondeliri-ous and nonsedated patients, the RASS scoreswere 0.
Table 3 describes the agreement betweenobservers. The weighted kappa values werepractically equal to or higher than 0.85
Table 2RASS Scores Distribution According to
Evaluation of the Main Palliative Care Physicianand Clinical Characteristics of the Patients
RASS Scores n (%)
RASS scores (complete sample) 322Sedation range (�5 to �3) 80 (25)Somnolence range (�2 to �1) 63 (20)Alert and calm (0) 151 (47)Restless/agitated (þ1 to þ2) 14 (4)Very agitated (þ3) 14 (4)
RASS scores inDelirium 116Sedation range (�5 to �3) 8 (7)Somnolence range (�2 to �1) 48 (41)Alert and calm (0) 32 (28)Restless/agitated (þ1 to þ2) 14 (12)Very agitated (þ3) 14 (12)Combative (þ4) 0
Palliative sedation 76Sedation range (�5 to �3) 72 (95)Somnolence range (�2 to �1) 4 (5)Alert and calm (0) 0Restless/agitated (þ1 to þ2) dVery agitated (þ3) d
Nondelirium-nonsedation 130Sedation range (�5 to �3) dSomnolence range (�2 to �1) 11 (8)Alert and calm (0) 119 (92)Restless/agitated (þ1 to þ2) dVery agitated (þ3) d
RASS ¼ Richmond Agitation-Sedation Scale.
between observers with experience in PC;therefore, the RASS interrater reliability wasvery good. The agreement level betweennurses and residents for patients with deliriumand with reduced consciousness was slightlylower than the overall sample. The analysis ofthe agreement between observers in both ageand sex groups did not offer wide differences:the weighted kappa values were in the range ofvery good agreement, and the observers withPC experience achieved the highest level ofagreement, among themselves.
The agreement level for each RASS score be-tween the observers and the main observer,a PC physician, is displayed in Table 4. Theagreement was higher than 90% for all theRASS scores, except for þ1 and þ2 scores,which had about 85% of agreement.
The correlations between the RASS and theRamsay Sedation and Glasgow Coma Scaleswere analyzed using 196 observations recordedin 80 patients. Only the PC physician and med-ical resident observations were used for thisanalysis. Table 5 summarizes the agreementwith the Ramsay Sedation and Glasgow ComaScales between the observers. The sedationscale of the RASS had a strong correlationwith both the Ramsay Sedation Scale (Spear-man’s r, 0.89 and 0.82, P < 0.001, for PC phy-sician and medical resident observations,respectively) and the Glasgow Coma Scale(Spearman’s r, 0.85 and 0.81, P < 0.001, forPC physician and medical resident observa-tions, respectively).
DiscussionIn the present study, we tested the appropri-
ateness and reliability of a Spanish version ofthe RASS in patients with advanced cancer.The face validity of the RASS was very goodas tested by the PC team. In fact, the RASS isa tool that uses precise definitions for sedationand agitation levels, and each level is estab-lished in a logical progression, from an un-conscious state to combative behavior. Thispsychometric structure facilitates its utilizationin different clinical settings.14 Nevertheless, itwas necessary to introduce a modification tothe þ1 score definition that addressed the pos-sibility that a patient could have disturbed be-havior while not being fully alert, and to

Table 3Agreement in RASS Scores Between Observers
Clinical Characteristics of the Patients Weighted Kappa (95% CI)
Overall samplePC physician-PC physician 0.94 (0.91e0.96)PC physician-nurse 0.95 (0.91e0.98)Nurse-nurse 0.94 (0.86e0.98)PC physician-medical residenta 0.89 (0.84e0.92)Medical resident-medical resident 0.85 (0.85e0.92)
Patients with deliriumPC physician-PC physician 0.89 (0.75e0.91)PC physician-nurse 0.88 (0.75e0.96)Nurse-nurse 0.91 (0.66e0.98)PC physician-medical resident 0.82 (0.69e0.90)Medical resident-medical resident 0.82 (0.66e0.90)
Patients with reduced awarenessb
PC physician-PC physician 0.85 (0.74e0.95)PC physician-nurse 0.84 (0.64e0.98)Nurse-nurse 0.88 (0.60e1.00)PC physician-medical resident 0.72 (0.57e0.84)Medical resident-medical resident 0.66 (0.43e0.83)
Patients aged <75/$75 yearsPC physician-PC physician 0.90 (0.80e0.95)/0.95 (0.85e1.00)PC physician-nurse 0.97 (0.88e1.00)/0.94 (0.85e0.98)Nurse-nurse 0.90 (0.75e1.00)/0.95 (0.85e1.00)PC physician-medical resident 0.79 (0.66e0.88)/0.92 (0.89e0.95)Medical resident-medical resident 0.90 (0.80e0.95)/0.95 (0.85e0.98)
Male/femalePC physician-PC physician 0.86 (0.80e0.92)/0.89 (0.82e0.94)PC physician-nurse 0.90 (0.86e0.99)/0.91 (0.72e0.99)Nurse-nurse 0.88 (0.82e0.99)/0.89 (0.68e0.99)PC physician-medical resident 0.89 (0.62e0.95)/0.89 (0.84e0.93)Medical resident-medical resident 0.83 (0.80e0.86)/0.86 (0.71e0.92)
RASS ¼ Richmond Agitation-Sedation Scale; PC ¼ palliative care.aMedical residents who were in temporary palliative care training.bThis category grouped patients with reduced awareness secondary to either advanced cancer or palliative sedation.
1116 Vol. 45 No. 6 June 2013Benıtez-Rosario et al.
remove the reference to assisted ventilationfrom the definition of agitation level.
In our judgment, the RASS, with our scoredefinition corrections, is a useful scale to de-scribe the clinical situation of cancer patientswith delirium and for monitoring the responseof behavior disturbances to treatment. Another
Table 4Agreement Level for Each RASS Score Between
the Main Observer and the Co-Observers
RASS ScorePC
Physician NursesMedical
Residentsa
�5 100 99 95�4 99 94 91�3 97 96 93�2 95 92 89�1 96 94 890 100 99 981 86 84 802 86 85 833 100 100 984 d d d
RASS ¼ Richmond Agitation-Sedation Scale.Numbers indicate the mean of the percentages of agreement.aMedical residents who were in temporary palliative care training.
application, as a result of its daily routine clini-cal use, could be the diagnosis of hyper-/hypo-deliriumddetecting both the inappropriatebehavior and the inappropriate communica-tion of patients. These clinical characteristicsare included in the Confusion Rating Scaleand Nursing Delirium Screening Scale,15,16
which are used for screening and diagnosing
Table 5Interrater Reliability of the Ramsay SedationScale and the Glasgow Coma Scale Between
Observers
Scale of SedationWeighted Kappa
(95% CI)
Ramsay Sedation ScalePC physician-PC physician 0.92 (0.88e0.96)PC physician-medical resident 0.90 (0.86e0.93)Medical resident-medical residenta 0.90 (0.83e0.93)
Glasgow Coma ScalePC physician-PC physician 0.91 (0.86e0.97)PC physician-medical resident 0.92 (0.87e0.95)Medical resident-medical resident 0.90 (0.85e0.92)
PC ¼ palliative care.aMedical residents who were in temporary palliative care training.

Vol. 45 No. 6 June 2013 1117Validation of the RASS in Spanish Cancer Patients
delirium. However, the RASS should not substi-tute for the clinical evaluation or informationobtained with other tools, such as theMemorialDelirium Assessment Scale, for establishing theimprovement of delirium.17e19 In fact, theRASS was not developed for measuring delir-ium severity, so the evaluation of severity of psy-chotic symptoms and cognitive failure is notincluded in the scale. Future studies investigat-ing delirium diagnosis and its response to drugsshould confirm our hypothesis about the RASSusefulness in these fields.
The RASS detected patient sedation stateswith a good correlation with the Ramsay Seda-tion and Glasgow Coma Scales. These scalesare habitually used to establish the sedationand coma levels secondary to treatment andbrain injury, respectively.14,20 Indeed, the Ram-say Sedation Scale also has been used as the‘‘gold standard’’ to compare the accuracy ofthe Bispectral index as ameasurement of the se-dation level of patients in different medical set-tings.14,21,22 Our data of face validity of theRASS, together with the aforementioned data,should be taken into account to promote theRASS as another validated tool for monitoringsedation depth in patients with advanced can-cer requiring palliative sedation. In fact, thePalliative Care Sedation Framework of theEuropean Association for Palliative Care3 rec-ommended its use despite the scale not havingbeen validated at the timeof publication.Webe-lieve our findings contribute to a reduction inthe lack of international validated tools to mon-itor sedation level, recently shownby the system-atic review by Brinkkemper et al.23
Our proposal about the usefulness of theRASS inPCsettings also is supportedbyourfind-ings of interrater reliability. Theweighted kappavalues obtained show an excellent interrater re-liability for every member of the PC team. Theinterrater reliability for the RASS is also highlyacceptable across a broad spectrum of patientswith advanced cancer, independent of patientcharacteristics such as age, gender, and clinicalstatus. Moreover, the interrater reliability alsowas observed for every score of the scale, witha between-observer agreement higher than80%.Our data from a PC unit confirm those ob-tained by other researchers who conducted val-idity testing of both the original scale and thenon-English versions of the RASS.5e9 Neverthe-less, our results show that the members of the
PC team were those who arrived at the bestagreement. Therefore, using the RASS requirestraining in recognition of the clinical state of thepatient and how to describe it in a single item ofthe RASS.
The main value of the RASS in caring for pa-tients with advanced cancer, in contrast withother scales, is that it combines into a singletool, with good face validity and interrater reli-ability, the description of different levels ofrestlessness and reduced consciousness. Thatnotwithstanding, we cannot establish that theRASS is the best tool for evaluating the afore-mentioned clinical situations because of thelack of both reference standard tools and stan-dard criteria for performing a comprehensivecomparison between the available scales. Addi-tionally, our results should be considered withcaution because of the inherent limitations ofresearch performed at a single site.
ConclusionOur data support the use of the RASS in
patients with advanced cancer. Future studiescarried out in PC units of different countriesought to confirm our findings and also shouldpromote the scale’s standardized use for im-proving our knowledge about agitation and se-dation monitoring.
Disclosures and AcknowledgmentsNo funding was received for this study, and
the authors declare no conflicts of interest.The authors thank Mr. Greg Haughton for
his contribution to the translation process ofthe tool and help in the English editing ofthe article.
The members of the CANPAL Research Net-work include Rosa Garcıa Garcıa, RN, Montser-rat Otero Tejera, RN, Lidia Cruz Gil, RN, Jos�eMarıa Reyes P�erez, RN, Ana Mercader Tor-reiro, RN, Raquel Miranda C�aceres, RN, Can-delaria Afonso Flores, RN, M�onica AfonsoHerrera, RN, and Jos�e Marıa Pellicer, RN.
References1. Caraceni A, Simonetti F. Palliating delirium inpatients with cancer. Lancet Oncol 2009;10:164e172.
1118 Vol. 45 No. 6 June 2013Benıtez-Rosario et al.
2. Bruera E, Bush SH, Willey J, et al. Impact of de-lirium and recall on the level of distress in patientswith advanced cancer and their family caregivers.Cancer 2009;115:2004e2012.
3. Cherny NI, Radbruch L, Board of the EuropeanAssociation for Palliative Care. European Associa-tion for Palliative Care (EAPC) recommendedframework for the use of sedation in palliativecare. Palliat Med 2009;23:581e593.
4. Kirk TW, Mahon MM, Palliative Sedation TaskForce of the National Hospice and Palliative CareOrganization Ethics Committee. National Hospiceand Palliative Care Organization (NHPCO) positionstatement and commentary on the use of palliativesedation in imminently dying terminally ill patients.J Pain Symptom Manage 2010;39:914e923.
5. Sessler CN, Gosnell MS, Grap MJ, et al. TheRichmond Agitation-Sedation Scale: validity and re-liability in adult intensive care unit patients. Am JRespir Crit Care Med 2002;166:1338e1344.
6. Ely EW, Truman B, Shintani A, et al. Monitoringsedation status over time in ICU patients: reliabilityand validity of the Richmond Agitation-SedationScale (RASS). JAMA 2003;289:2983e2991.
7. Nassar AP Jr, Pires Neto RC, de Figueiredo WB,Park M. Validity, reliability and applicability of Por-tuguese versions of sedation-agitation scales amongcritically ill patients. Sao Paulo Med J 2008;126:215e219.
8. Almgren M, Lundmark M, Samuelson K. TheRichmond Agitation-Sedation Scale: translationand reliability testing in a Swedish intensive careunit. Acta Anaesthesiol Scand 2010;54:729e735.
9. Vasilevskis EE, Morandi A, Boehm L, et al. Delir-ium and sedation recognition using validated instru-ments: reliability of bedside intensive care unitnursing assessments from 2007 to 2010. J Am Ger-iatr Soc 2011;59:S249eS455.
10. Beaton DE, Bombardier C, Guillemin F,Marcos B. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine J2000;25:3186e3191.
11. Wong CL, Holroyd-Leduc J, Simel DL,Straus SE. Does this patient have delirium? Valueof bedside instruments. JAMA 2010;304:779e786.
12. Graeff AD, Dean M. Palliative sedation therapyin the last weeks of life: a literature review and rec-ommendations for standards. J Palliat Med 2007;10:67e85.
13. Tooth LR, Ottenbacher KJ. The kappa statisticin rehabilitation research: an examination. ArchPhys Med Rehabil 2004;85:1371e1376.
14. Olson DM, Thoyre SM, Auyong DB. Perspec-tives on sedation assessment in critical care. AACNAdv Crit Care 2007;18:380e395.
15. Gagnon P, Allard P, Masse B, DeSerres M. Delir-ium in terminal cancer: a prospective study usingdaily screening, early diagnosis, and continuousmonitoring. J Pain Symptom Manage 2000;19:412e426.
16. Gaudreau JD, Gagnon P, Harel F, Tremblay A,Roy MA. Fast, systematic, and continuous deliriumassessment in hospitalized patients: the nursing de-lirium screening scale. J Pain Symptom Manage2005;29:368e375.
17. Bosisio M, Caraceni A, Grassi L, Italian DeliriumStudy Group. Phenomenology of delirium in cancerpatients, as described by the Memorial Delirium As-sessment Scale (MDAS) and the Delirium RatingScale (DRS). Psychosomatics 2006;47:471e478.
18. Yang FM, Marcantonio ER, Inouye SK, et al.Phenomenological subtypes of delirium in olderpersons: patterns, prevalence, and prognosis. Psy-chosomatics 2009;50:248e254.
19. Kazmierski J, Kowman M, Banach M, et al. Theuse of DSM-IV and ICD-10 criteria and diagnosticscales for delirium among cardiac surgery patients:results from the IPDACS study. J NeuropsychiatryClin Neurosci 2010;22:426e432.
20. Rost NS, Smith EE, Chang Y, et al. Prediction offunctional outcome in patients with primary intrace-rebral hemorrhage: the FUNC score. Stroke 2008;39:2304e2309.
21. Haenggi M, Ypparila-Wolters H, Bieri C, et al.Entropy and bispectral index for assessment of seda-tion, analgesia and the effects of unpleasant stimuliin critically ill patients: an observational study. CritCare 2008;12:R119.
22. Hern�andez-Gancedo C, Pesta~na D, P�erez-Chrzanowska H, Martinez-Casanova E, Criado A.Comparing entropy and the bispectral index withthe Ramsay score in sedated ICU patients. J ClinMonit Comput 2007;21:295e302.
23. Brinkkemper T, van Norel AM, Szadek KM,et al. The use of observational scales to monitorsymptom control and depth of sedation in patientsrequiring palliative sedation: a systematic review.Palliat Med 2013;27:54e67.
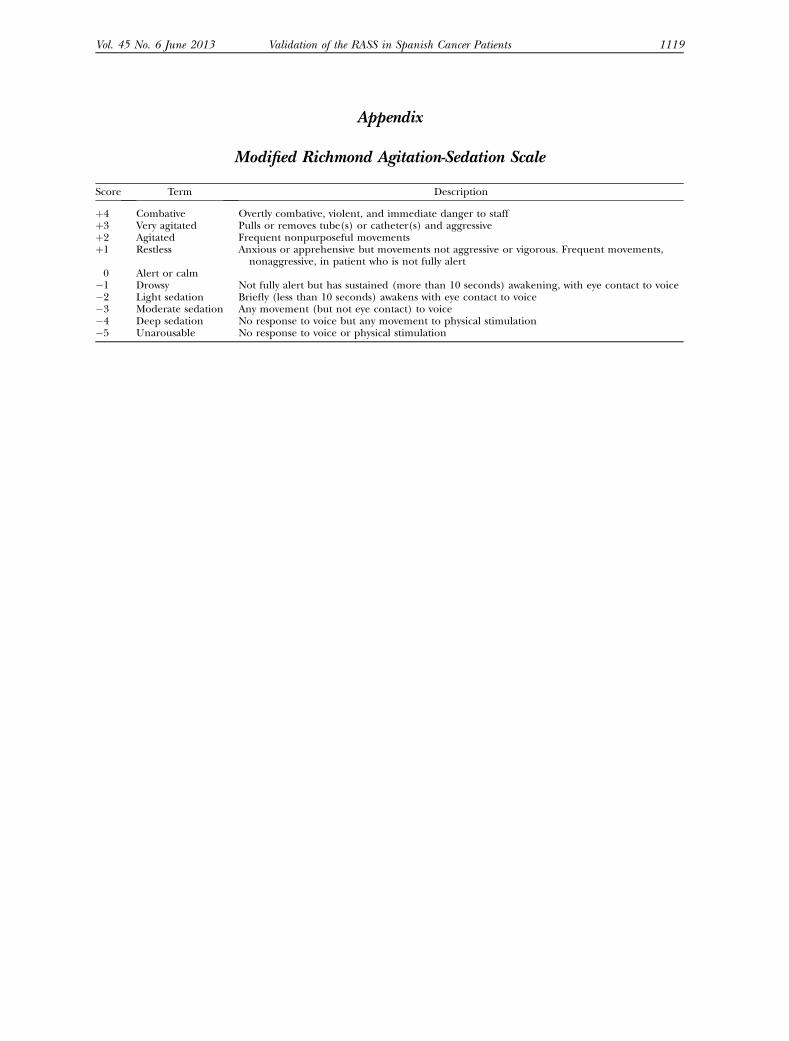
Appendix
Modified Richmond Agitation-Sedation Scale
Score Term Description
þ4 Combative Overtly combative, violent, and immediate danger to staffþ3 Very agitated Pulls or removes tube(s) or catheter(s) and aggressiveþ2 Agitated Frequent nonpurposeful movementsþ1 Restless Anxious or apprehensive but movements not aggressive or vigorous. Frequent movements,
nonaggressive, in patient who is not fully alert0 Alert or calm
�1 Drowsy Not fully alert but has sustained (more than 10 seconds) awakening, with eye contact to voice�2 Light sedation Briefly (less than 10 seconds) awakens with eye contact to voice�3 Moderate sedation Any movement (but not eye contact) to voice�4 Deep sedation No response to voice but any movement to physical stimulation�5 Unarousable No response to voice or physical stimulation
Vol. 45 No. 6 June 2013 1119Validation of the RASS in Spanish Cancer Patients





























