Embed Size (px)
Citation preview

Page 1 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
.A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
Approaches and landmarks for nucleus accumbens area:a review of the literature and review-based suggestions for
nucleus accumbens surgery
IN Mavridis1*
AbstractIntroductionThe paper reviews the literature regarding the existing neurosurgical techniques for approaching nucleus accumbens (NA) area and suggests new (non-stereotactic and alternative stereotactic) approaches to this nucleus as well as relative anatomical landmarks.
DiscussionThe well established approach to the NA through the internal capsule co-uld be used for strereotactic biopsy or aspiration. A transorbital, trans-nasal or an endoscopic approach through the lateral ventricle could be applied to the NA. More invasi-vely, an inferior frontal or an appr-oach through the frontal horn of the lateral ventricle could be appl-ied. Stereotactic radiosurgery and inferior frontal approach could be useful for stereotactic ablation of the NA. Based on its anatomical loca-tion and relations, new potential landmarks useful in non-stereo-tactic surgery of this nucleus are also presented.ConclusionApart from the approaches and land-marks that are used nowadays for approaching the NA area, there are some other potential approaches and landmarks for reaching this crucial area of the human brain.
IntroductionSurgery of the human nucleus accum-bens (NA) is a neurosurgical achieve-ment of the 21st century. Deep brain stimulation (DBS) of the NA was first reported in 2003 by Sturm et al. for the treatment of obsessive–compulsive and anxiety disorders1. Also, in 2003, stereotactic ablation of the NA was first reported by Gao et al. for alleviating opiate drug psychological depend-ence2. During the last few years, the number of reports of NA DBS has been geometrically increasing, and the number of countries reporting this procedure has also been increasing (mainly in Europe). DBS is the main surgical procedure that is nowadays applied to the NA in some carefully selected patients suffering from refractory major depression, obsessive– compulsive disorder and Tourette’s syndrome3–5. There are also other reports for NA ablation in opiate addicts6 and alcoholics7. Moreover, the NA has been discussed in the literature as a potential target for neurosurgical intervention in treating obesity8 and schizophrenia9.
The expanding dynamics of the NA DBS is promising. The well established benefits of DBS have set this minimally invasive procedure as the surgical intervention of choice in NA surgery, with only one reported alternative intervention, namely the ablation. They are both based on similar standard surgical procedures, following specific reported approaches to reach the NA through the anterior limb of the inter-nal capsule (ALIC). There are several
stereotactic or even non-stereotact-ic (endoscopic or non-endoscopic) NA surgery. Further, we believe that there are also some other anatomical landmarks potentially useful in NA surgery. Our purpose was to explore the existing neurosurgical techniques from an anatomical point of view and suggest new approaches and relative landmarks.We reviewed the literature regarding neurosurgical approaches (more or less invasive) to the posterior-medial part of the anterior cranial fossa (where NA is located) and anatomical landmarks that have been reported for NA surgery (always stereotactic). We also reviewed the literature about the existing use (other than NA surgery) of other approaches potentially applicable to the NA.
Approaches Through the ALIC DBS certainly is the most promising new technique in psychosurgery. It constitutes a significant step forward because it allows an even more focused inter-vention into neural circuits.
* Corresponding authorEmail: [email protected] Department of Anatomy, University of Athens
School of Medicine, Athens, Greece
reported anatomical landmarks used for these procedures. We strongly believe that there are also other ap-proaches that can be used either for
Clin
ical Anato
my
The literature regarding neurosurg-ical approaches applicable to the NA area as well as relative anatomical landmarks was reviewed.
DiscussionThe author has referenced some of its own studies in this review. The protocols of these studies have been approved by the relevant ethics committees related to the institution in which they were performed.
We included potential approaches to reach the NA for non-stereotactic surgery purposes (endoscopic or not), as well as anatomical structures useful as landmarks for such interventions.

Page 2 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
Using thin electrodes, the smallest areas of the brain and fibre tracts can be targeted with high accuracy; this considerably lowers the subsequent rate of side effects10. Therefore, nowa-days, the term ‘NA surgery’ is almost synonymous to the term ‘NA DBS’. A trajectory through the ALIC for NA DBS is strongly supported as per the literature4,11,12. Specifically, it follows the angle of the white matter fibre
tract in coronal plane so that the elec-trodes traverse the ALIC and termi-nate in the vicinity of the NA4,12. Entry point and final trajectory are planned to avoid ventricles, sulci and vessels present along the electrode path13.
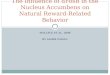
Reaching the NA through the ALIC (Figure 1a–d) is the only surgical approach that is used nowadays for DBS or stereotactic ablation. The burr hole is usually placed at the frontal
bone, a few millimetres anterior to the coronal suture, and after opening the meninges, the brain is usually entered at the middle frontal gyrus (where the electrode’s trajectory is planned to pass through). Approxi-mately, the first half of the electrode’s course within the brain (after pene-trating the frontal cortex) is through the white matter of the frontal lobe, whereas the second half of the course follows the ALIC till the NA.
Based on this method, stereotactic or computed tomography (CT)-guided biopsy of the NA could be performed. The involvement of this major ‘pleasure centre’ in several neurological and psychiatric disorders may potentially lead to the application of such a proce-dure in future. Moreover, stereotactic or CT-guided aspiration of a cystic lesion in this area could be another option. CT-guided aspiration could be the first-choice approach for treating spon-taneous putaminal haemorrhage considering bleeds of ≤50 ml, while the key-hole approach may be more suitable for those with larger haema-tomas14. Since the NA is the area of continuity between the caudate nucleus and putamen, such a treatment is appli-cable to NA haemorrhage as well.
TransorbitalThe transorbital key-hole approach to anterior communicating artery aneu-rysms was developed as a minimally invasive method for safe control of the anterior communicating artery com-plex. This approach does not necessi-tate resection of the gyrus rectus. The orbitocranial key-hole approach seems to be substantially better than crani-otomy, although it requires additional effort and time. Technically, the orbital cortex should be gently elevated and the posterior aspect of the gyrus rectus should be separated from the optic chiasm15.
The supraorbital craniotomy allows wide intracranial exposure of the deep-seated supra- and parasellar region (where the NA lies, Figures 2a, 3a and 4a), according to the concept of
Figure 1: Approach to the NA through the ALIC. (a) Human brain, right cerebral hemisphere, coronal section 2 mm anterior to the AC and visceral skull. (b) Human brain, right cerebral hemisphere, coronal section 2 mm anterior to the AC, sagittal section 7 mm lateral to the midline, axial section at the intercommissural plane. (c) Human brain, right cerebral hemisphere, coronal section 2 mm anterior to the AC and right hemi-skull, internal surface. (d) Human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC, axial section at the intercommissural plane, sagittal section 7 mm lateral to the midline.

Page 3 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
key-hole approaches16. The supraor-bital approach, through an eyebrow incision, involves a small craniotomy flap flush to the orbital roof17. As used for meningiomas surgery17, it could be performed for NA surgery by introducing the endoscope through the key-hole and advancing between the frontal lobe and the floor of the anterior skull base, all the way to the NA. To get better basal view, the pos-terior frontal bone, sphenoid ridge or superior orbital roof could be drilled away. This allows an overview of the ipsilateral and parts of the contralat-eral anterior fossa17.
The transorbital roof craniotomy is a frontal craniotomy that incorporates the orbital roof and is performed via a suprabrow incision. This technique, primarily used for resection of mass lesions, provides excellent exposure to the orbit, anterior fossa and para-sellar region, with little significant morbidity18. Together with supraorbi-tal craniotomy, there are more invasive procedures and should be considered in cases of NA area tumours only.
Following the principles of tran-sorbital key-hole endoscopic surgery, the anterior cranial fossa can be
accessed through a hole at the supe-rior orbital wall located very close to the midpoint of the superior orbital ring. After a diagonal course at the floor of the anterior fossa, the NA can be reached by penetrating the inferior hemispheric surface (Figure 2a–b), just posterior to the formation of the olfactory tract (at approximately 10 mm laterally to the midline) or medially to the initial part of this tract. Endoscopic surgery of this nucleus could be performed with this method. Attention should be paid not to trauma-tize the olfactory tract, optic nerve (as it emerges from the optic chiasm) and arterial branches (mainly of the recur-rent artery of Heubner), which enter the anterior perforated substance. Reaching the NA through a supraorbital or transorbital roof craniotomies are more invasive techniques and perhaps preferable for mass resections.
TransnasalAlthough endonasal anatomical variations occur frequently, they rarely cause trouble in gaining access to the sellar region and therefore require experienced pituitary surgeon in practically all cases19. Endoscopic
transsphenoidal surgery has a clear place in the extended approach to suprasellar tumours, such as crani-opharyngiomas, and is far better in managing some complications, such as cerebrospinal fluid leaks20. More-over, the free-head navigation endo-nasal transsphenoidal technique, which combines microscopy and endoscopy, is a safe, quick and effective approach to lesions of the sellar region. This combined approach saves time, avoids mucosal disruption, maximises the resection and shortens the patient’s hospital stay21.
Endonasal approaches achieve a direct and wide exposure of the mid-line cranial base anatomy. The main lateral limitations of these approaches are the optic nerves, lateral cavern-ous sinus, vidian nerve, internal carotid artery, abducens nerve in Dorello’s canal, jugular tubercle and hypo-glossal canals22. Given the location of the NA, these limitations would not really be an issue in NA surgery. Under-standing the anatomical limits of each approach aids a surgeon in providing a full surgical armamentarium to address cranial base pathology. Three-dimensional visualisations aid in understanding the deep relationships of the densely packed, highly sensitive neural and vascular elements of the paramedian cranial base22, where the NA is located (Figures 2a and 3a).
Following the principles of transs-phenoidal endoscopic surgery, the anterior cranial fossa can be accessed at its posterior part, considerably close to the midline. Subsequently, the NA can be reached either through the inferior hemispheric surface (Figure 3a–c), just posterior to the for-mation of the olfactory tract (or lateral to the latter’s initial part), or through the internal hemispheric surface (Figure 3b–d), just anterior to the ante-rior commissure (AC). In both varia-tions of this technique, the intracerebral course to the NA is only a few milli-metres. While applying the first varia-tion, attention should be paid not to traumatize the olfactory tract, optic
Figure 2: Transorbital approach to the NA. (a) Human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC and skull base. (b) Visceral skull.

Page 4 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
nerve and arterial branches, which enter the anterior perforated sub-stance. Regarding the second varia-tion of the transnasal approach to the NA, special care should be taken to avoid injury to the anterior cerebral artery (anterior to the anterior communicating artery) at the internal hemispheric surface.
Inferior frontalThis approach, if used for NA stereo-tactic surgery, has the advantage
that the trajectory passes through a safer path when compared with the ALIC (where so many important fibres are closely located). Other approaches used for frontal cranial base surgery include the unilateral and bilateral subfrontal (bifrontal) approaches17. The frontolateral approach for olfac-tory groove meningiomas has been reported to be preferable because it provides quick access to the tumour with less brain exposure, while still enabling total tumour removal with a
low morbidity rate and no mortality23. A reported approach to symptomatic cavernous malformations deep in the anteroinferior basal ganglia (where the NA lies) is through the supraca-rotid triangle, between ascending per-forators and through the basomedial frontal lobe. The supracarotid– infrafrontal approach incorporates an orbitozygomatic craniotomy, wide microsurgical exposure of the supra-carotid triangle, dissection of perfo-rating arteries and image-guided resection through the posterior part of the medial orbital gyrus and anterior perforated substance24. All these approaches seem to be too invasive to have a place in NA surgery, except for cases involving extended tumour resection.
To apply a transcortical key-hole approach, the anterior cranial fossa can be entered through a hole at the frontal bone at approximately 20 mm lateral to the midline and 15 mm superior to the eyebrow. Subsequently, the NA can be reached via a straight course within the inferior-medial part of the (ipsilateral) frontal lobe (Figure 5a–b). Stereotactic surgery (ablation) of the NA could also be applied with this method.
Through the lateral ventricleThe transsylvian approach (performed via a pterional craniotomy of 5 cm in diameter) or the less invasive trans-cortical key-hole approach can be used to enter the temporal horn of the lateral ventricle25. In the latter, a 3 cm craniotomy is centred on the projec-tion of the middle temporal gyrus. Neuronavigation is used to determine the optimal placement of a 2 cm corti-cotomy in the middle temporal gyrus and to direct the white matter cleavage to the temporal horn of the lateral ventricle25. Respectively, a frontal craniotomy centred on the projection of the middle frontal gyrus can be performed for a transcortical key-hole approach to the NA through the frontal horn of the lateral ventricle.
Figure 3: Transnasal approaches to the NA. (a) Human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC and visceral skull–skull base. The NA is reached from the inferior hemispheric surface. (b) Visceral skull. (c) Visceral skull, lateral surface, zygomatic arc removed. (d) Human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC and visceral skull–skull base. The NA is reached from the internal hemispheric surface.

Page 5 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
We consider that flexible endoscopes would be more adequate and safer for approaching the NA and also other paraventricular nuclei through the lateral ventricle.
Following the principles of interven-tricular endoscopic surgery (transcorti-cal key-hole approach, temporal craniotomy), the endoscope is guid-ed to the frontal horn of the lateral ventricle, after an interventricular course through its body. The NA can be reached by penetrating the floor of the horn anterior to the AC (Figure 4b). Alternatively, the ventricular sys-tem can be entered through the fron-tal lobe, following a straight diagonal intracerebral course within this lobe, from the middle frontal gyrus (also transcortical key-hole approach, frontal craniotomy) to the lateral aspect of the roof of the frontal horn of the lateral ventricle (Figure 4a).
IntravascularA multidisciplinary approach that considers observation, microsurgery, embolization and radiosurgery, alone or in combination, is imperative to the effective management of arterio-venous malformations (AVMs) of the basal ganglia (where the NA lies) and thalamus. Malformations, lateral to the carotid bifurcation, usually receive arterial supply from the M1 segment of the middle cerebral artery or the recurrent artery of Heubner and their venous drainage to the basal vein26. Such an AVM pattern is highly proba-ble for NA area, given that the NA is usually supplied by this artery and is also placed lateral to the carotid bifurcation. A theoretical NA necrosis with interventional radiology tech-niques would probably necessitate a hyperselective vascular embolization.
In selected cases, intravascular approach to the NA could be consid-ered. After careful identification of the vessels supplying blood to the NA with angiography of the internal carotid system (digital subtraction angiography or magnetic resonance
Figure 4: Approach to the NA through the lateral ventricle. (a) Human brain, right cerebral hemisphere, coronal section 2 mm anterior to the AC and visceral skull–posterior cranial fossa. (b) Human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC (axial section at the intercommissural level).
Figure 5: Inferior frontal approach to the NA. (a) Human brain, right cerebral hemisphere, coronal section 2 mm anterior to the AC and right hemi-skull, internal surface (coloured bones of the visceral skull). (b) Human brain, right cerebral hemisphere (removed frontal and parietal opercula), coronal section 2 mm anterior to the AC and skull (removed parts of the frontal and parietal bones, coloured bones of the skull).

Page 6 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
angiography), they can be reached by using interventional radiology tech-niques. Infusion of drugs to affect the NA function, chemotherapeutics for tumours in the NA area as well as materials to selectively occlude these vessels could be achieved via this method. Selective occlusion of the NA vessels could be used instead of stereotactic ablation, for embolization of regional AVMs or aneurysms and for oncological purposes.
RadiosurgeryIn our opinion, it is only a matter of time for stereotactic radiosurgery of the NA to be applied. Ablation of this structure would probably be the easi-est and most effective application of this method. By using carefully iden-tified stereotactic coordinates, precise targeting can be achieved. Of course, conventional radiosurgery owns its rightful place in treating tumours of the NA area.
Landmarks Brain structuresThere are four alternative reference landmarks which have been reported to date for measuring Y stereotactic coordinate of the NA target area for NA DBS: the anterior border of the AC1,4,5, the posterior border of the AC27, the mid-commissural point2 and the posterior commissure (PC)28. Of these, the most adequate for measur-ing this coordinate is the anterior bor-der of the AC, as we have previously anatomically explained29. On the other hand, there is an agreement among authors regarding the reference land-marks for measuring the X and Z stereotactic coordinates, which rep-resent the midline and AC–PC plane, respectively1,2,4,5. Some authors use the term ‘AC–PC line’, meaning the common linear part of the AC–PC plane and the midline2,28. This landmark allows measurements of both X and Z stereotactic coordinates.
The role of the ALIC as an ana-tomical landmark in NA DBS has
been mentioned above. The olfactory tract and optic nerve (near the optic chiasm) are identified mainly for their specific anatomical location. The frontal horn of the lateral ventricle is easily identifiable intraoperatively as well as on CTs and magnetic reso-nance images. Finally, the recurrent artery of Heubner (occasionally duplicated) usually originates from the A2 segment of the anterior cere-bral artery, from the anterior cerebral artery–anterior communicating artery junction, or rarely from the A1 seg-ment. Its branches include olfactory, frontal, branches for the Sylvian fissure and branches penetrating the anterior perforated substance30.
The midline and middle frontal gyrus have also been used as landmarks for stereotactic surgery of the NA. As mentioned above, the AC and middle frontal gyrus can be used as anatomical landmarks for non-stereotactic NA surgery as well. Further, the olfactory tract, optic nerve (near the optic chiasm), ground and superior-lateral aspect of the lateral ventricle’s frontal horn as well as the recurrent artery of Heubner could also be used as such landmarks.
Bony and skin structuresThe inferior orbital ring and external auditory meatus have been reported as external landmarks for a parallel to the AC–PC line placement of the DBS stereotactic frame13. In ALIC DBS in the vicinity of the NA for treating Tourette’s syndrome, burr holes were reported to be placed 3.5 cm lateral to the midline12. In a similar procedure for refractory obsessive–compulsive disorder, the trajectory has been reported to lead (in sagittal plane) to a burr hole just anterior to the coronal suture11. In addition, intraoperative5 and postoperative X-ray as well as cranial CT have been used to verify the correct positioning of the DBS electrodes4. Finally, according to a few reports of stereotactic ablation of the human NA, the incision on the scalp
skin is placed 9–11 cm above the eyebrows and 2.5 cm lateral to the midline2,6,7. As mentioned above, the midline, superior orbital ring and eyebrow can be used as anatomical landmarks for non-stereotactic NA surgery.
ConclusionThe well-established approach to the NA through the ALIC could be used for stereotactic biopsy or aspiration. Considering the possibility of endo-scopic surgery of this area, we sug-gest that a transorbital, transnasal or an endoscopic approach through the lateral ventricle could be used (Figure 6). Considering the possibility of more invasive surgery in this area, we suggest that an inferior frontal or an approach through the frontal horn of the lateral ventricle could be applied. In selected cases, intravascu-lar intervention and radiosurgery could also have a role. Further, we believe that stereotactic radiosurgery as well as an inferior frontal approach could be useful in NA stereotactic ablation.
Except for the nowadays used cerebral, bony and skin anatomical landmarks for NA stereotactic sur-gery, there are also other potential landmarks useful in non-stereotactic (endoscopic or non-endoscopic) sur-gery, which are based on its anatomical location and relations.
Abbreviations listAC, anterior commissure; ALIC, anterior limb of the internal capsule; AVM, arteriovenous malformation; CT, computed tomography; DBS, deep brain stimulation; NA, nucleus accum-bens; PC, posterior commissure.
AcknowledgementsThe author thanks Prof. Sophia Anagnostopoulou (Department of Anatomy, University of Athens School of Medicine) for providing the anatomical materials used for the artworks of this article.

Page 7 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
References1. Sturm V, Lenartz D, Koulousakis A, Treuer H, Herholz K, Klein JC, et al. The nucleus accumbens: a target for deep brain stimulation in obsessive-compulsive and anxiety disorders. J Chem Neuroanat. 2003 Dec;26(4):293–9.2. Gao G, Wang X, He S, Li W, Wang Q, Liang Q, et al. Clinical study for alleviat-ing opiate drug psychological dependence by a method of ablating the nucleus accumbens with stereotactic surgery. Stereotact Funct Neurosurg. 2003;81(1-4): 96–104.3. Huff W, Lenartz D, Schormann M, Lee SH, Kuhn J, Koulousakis A, et al. Unilateral deep brain stimulation of the nucleus accumbens in patients with treatment-resistant obsessive–compulsive disorder: outcomes after one year. Clin Neurol Neurosurg. 2010 Feb;112(2):137–43.4. Kuhn J, Lenartz D, Huff W, Mai JK, Koulousakis A, Maarouf M, et al. Transient manic-like episode following bilateral deep brain stimulation of the nucleus accumbens and the internal capsule in a patient with Tourette syndrome. Neuro-modulation. 2008 Apr;11(2):128–31.5. Schlaepfer TE, Cohen MX, Frick C, Kosel M, Brodesser D, Axmacher N, et al. Deep brain stimulation to reward circuitry alleviates anhedonia in refractory major depression. Neuropsychopharmacology. 2008 Jan;33(2):368–77.6. He F, Guan H, Zhao Z, Miao X, Zhou Q, Li L, et al. Evaluation of short-term psychological functions in opiate addicts after ablating the nucleus accumbens via stereotactic surgery. Stereotact Funct Neurosurg. 2008;86(5):320–9.7. Wu HM, Wang XL, Chang CW, Li N, Gao L, Geng N, et al. Preliminary findings in ablating the nucleus accumbens using stereotactic surgery for alleviating psy-chological dependence on alcohol. Neurosci Lett. 2010 Apr;473(2):77–81.8. Halpern CH, Wolf JA, Bale TL, Stunkard AJ, Danish SF, Grossman M, et al. Deep brain stimulation in the treatment of obe-sity. J Neurosurg. 2008 Oct;109(4):625–34.9. Mikell CB, McKhann GM, Segal S, McGovern RA, Wallenstein MB, Moore H. The hippocampus and nucleus accum-bens as potential therapeutic targets for neurosurgical intervention in schizophre-nia. Stereotact Funct Neurosurg. 2009; 87(4):256–65.
Figure 6: Schematic drawing of the approaches to the NA (human brain, left cerebral hemisphere, coronal section 2 mm anterior to the AC and visceral skull–skull base). 1. Through the ALIC; 2. Transorbital approach; 3. Transnasal approaches; 4. Inferior frontal approach; 5. Through the lateral ventricle (entered for example from the temporal horn); 6. Head of the caudate nucleus; 7. ALIC; 8. Putamen; 9. Insula; 10. Middle frontal gyrus; 11. Internal hemispheric surface; 12. Olfactory groove; 13. Superior orbital rim. Trajectories are lightened when passing through structures where they are superimposed on.

Page 8 of 8
Critical review
Licensee OA Publishing London 2013. Creative Commons Attribution License (CC-BY)
Com
petin
g in
tere
sts:
non
e de
clar
ed. C
onfli
ct o
f int
eres
ts: n
one
decl
ared
. A
ll au
thor
s co
ntrib
uted
to th
e co
ncep
tion,
des
ign,
and
pre
para
tion
of th
e m
anus
crip
t, a
s w
ell a
s re
ad a
nd a
ppro
ved
the
final
man
uscr
ipt.
All
auth
ors
abid
e by
the
Ass
ocia
tion
for M
edic
al E
thic
s (A
ME)
eth
ical
rule
s of
dis
clos
ure.
For citation purposes: Mavridis IN. Approaches and landmarks for nucleus accumbens area: a review of the literature and review-based suggestions for nucleus accumbens surgery. OA Anatomy 2013 Feb 01;1(1):1.
10. Juckel G, Uhl I, Padberg F, Brüne M, Winter C. Psychosurgery and deep brain stimulation as ultima ratio treatment for refractory depression. Eur Arch Psychiatry Clin Neurosci. 2009 Feb;259(1):1–7.11. Abelson JL, Curtis GC, Sagher O, Albucher RC, Harrigan M, Taylor SF, et al. Deep brain stimulation for refractory obsessive–compulsive disorder. Biol Psychiatry. 2005 Mar;57(5):510–16.12. Flaherty AW, Williams ZM, Amirnovin R, Kasper E, Rauch SL, Cosgrove GR, et al. Deep brain stimulation of the anterior internal capsule for the treatment of Tourette syndrome: technical case report. Neurosurgery. 2005 Oct;57(4 Suppl):E403.13. Pinsker MO, Volkmann J, Falk D, Herzog J, Steigerwald F, Deuschl G, et al. Deep brain stimulation of the internal globus pallidus in dystonia: target localisation under general anaesthesia. Acta Neurochir (Wien). 2009 Jul;151(7): 751–8.14. Zhao JZ, Zhou LF, Zhou DB, Wang RZ, Wang M, Wang DJ, et al. Computed tomography-guided aspiration versus key-hole craniotomy for spontaneous putaminal haemorrhage: a prospective comparison of minimally invasive procedures. Hong Kong Med J. 2009 Aug;15(4):274–9.15. Steiger HJ, Schmid-Elsaesser R, Stummer W, Uhl E. Transorbital key-hole approach to anterior communicating artery aneurysms. Neurosurgery. 2001 Feb; 48(2):347–51.16. Reisch R, Perneczky A, Filippi R. Surgical technique of the supraorbital key-hole craniotomy. Surg Neurol. 2003 Mar;59(3):223–7.17. Rachinger W, Grau S, Tonn JC. Different microsurgical approaches to
meningiomas of the anterior cranial base. Acta Neurochir (Wien). 2010 Jun;152(6): 931–9.18. Shanno G, Maus M, Bilyk J, Schwartz S, Savino P, Simeone F, et al. Image-guided transorbital roof craniotomy via a suprabrow approach: a surgical series of 72 patients. Neurosurgery. 2001 Mar; 48(3):559–67.19. van Lindert EJ, Ingels K, Mylanus E, Grotenhuis JA. Variations of endonasal anatomy: relevance for the endoscopic endonasal transsphenoidal approach. Acta Neurochir (Wien). 2010 Jun;152(6): 1015–20.20. Powell M. Microscope and endoscopic pituitary surgery. Acta Neurochir (Wien). 2009 Jul;151(7):723–8.21. Al-Mefty O, Pravdenkova S, Gragnaniello C. A technical note on endonasal combined microscopic endoscopic with free head navigation technique of removal of pituitary adenomas. Neurosurg Rev. 2010 Apr; 33(2):243–8.22. Roth J, Singh A, Nyquist G, Fraser JF, Bernardo A, Anand VK, et al. Three- dimensional and 2-dimensional endoscopic exposure of midline cranial base targets using expanded endonasal and transcra-nial approaches. Neuro surgery. 2009 Dec; 65(6):1116–28.23. Nakamura M, Struck M, Roser F, Vorkapic P, Samii M. Olfactory groove meningiomas: clinical outcome and recur-rence rates after tumor removal through the frontolateral and bifrontal approach. Neurosurgery. 2007 May;60(5):844–51.24. Waldron JS, Lawton MT. The supracarotid-infrafrontal approach: surgical technique and clinical application to cav-ernous malformations in the anteroinferior
basal ganglia. Neurosurgery. 2009 Mar; 64(3 Suppl):86–95.25. Lutz MT, Clusmann H, Elger CE, Schramm J, Helmstaedter C. Neuropsy-chological outcome after selective amyg-dalohippocampectomy with transsylvian versus transcortical approach: a rand-omized prospective clinical trial of surgery for temporal lobe epilepsy. Epilepsia. 2004 Jul;45(7):809–16.26. Gross BA, Duckworth EA, Getch CC, Bendok BR, Batjer HH. Challenging tradi-tional beliefs: microsurgery for arterio-venous malformations of the basal ganglia and thalamus. Neurosurgery. 2008 Sep; 63(3):393–410.27. Malone DA Jr, Dougherty DD, Rezai AR, Carpenter LL, Friehs GM, Eskandar EN, et al. Deep brain stimulation of the ventral capsule/ventral striatum for treat-ment-resistant depression. Biol Psychiatry. 2009 Feb;65(4):267–75.28. Aouizerate B, Cuny E, Bardinet E, Yelnik J, Martin-Guehl C, Rotge JY, et al. Distinct striatal targets in treating obsessive–compulsive disorder and major depression. J Neurosurg. 2009 Oct; 111(4):775–9.29. Mavridis I, Boviatsis E, Anagnosto-poulou S. Microsurgical anatomy of the nucleus accumbens: the role of the two commissures in measuring stereotactic coordinates of the target and the ablation- vs. stimulation-target area. Stereotact Funct Neurosurg. 2010;88(4):264–5.30. Avci E, Fossett D, Aslan M, Attar A, Egemen N. Branches of the anterior cere-bral artery near the anterior communicat-ing artery complex: an anatomic study and surgical perspective. Neurologia Med Chir. 2003 Jul;43(7):329–33.