Embed Size (px)
Citation preview

nstlatapbf
Approach to the Patient EvaluationUsing Static and Dynamic Hip PathomechanicsMichael J. Knesek, MD,* Jack G. Skendzel, MD,* Bryan T. Kelly, MD,† and Asheesh Bedi, MD*
The etiology of mechanical hip pain in the absence of osteoarthritic changes requires acareful consideration of static and dynamic factors. Dynamic factors result from abnormalstress and contact between the femoral head and acetabular rim with hip motion, whereasstatic factors result from asymmetric and supraphysiologic loads between the femoral headand acetabular socket when in the standing or axially loaded position. Compensatorymotion resulting from restricted terminal hip motion may adversely affect dynamic muscleforces across the hip joint, leading to several other related extra-articular symptoms andpain. An appreciation of abnormal hip morphology and hip joint mechanics is required tounderstand the important role of both static and dynamic stresses in the development of hippain and early onset osteoarthritis in the young hip. This review describes the static anddynamic factors associated with mechanical hip pain to allow for the development of athoughtful and effective treatment plan.Oper Tech Sports Med 20:260-272 © 2012 Elsevier Inc. All rights reserved.
KEYWORDS hip, mechanical factors, impingement, dysplasia, FAI
afsdcmctpgpcs
The evaluation of hip pain in the active patient populationwithout radiographic evidence of osteoarthritis (OA)
presents a significant challenge to the treating physician. Al-tered hip morphology can affect both the acetabulum andproximal femur.1-3 These alterations in native hip morphol-ogy may predispose the patient to develop early onset OA ofthe hip because of asymmetric loading across the chondralsurfaces with increased contact pressures.4-6 Often these ab-
ormalities of bony structure lead to subsequent damage ofoft tissue structures, such as the acetabular labrum, leadingo hip pain.7 Dolan et al8 recently evaluated 135 patients withabral tears diagnosed by magnetic resonance image (MRI)nd computed tomography (CT) scans and demonstratedhat 90% of these tears were associated with bony structuralbnormalities. The alterations in hip joint mechanics thatredispose to OA are often thought of in terms of a spectrumetween “undercoverage” (dysplasia) and “overcoverage,” oremoroacetabular impingement (FAI).1,2,5,6,9-12 It is now clear
that a comprehensive knowledge and understanding of both
*Department of Orthopaedic Surgery, MedSport, University of MichiganHospitals, Ann Arbor, MI.
†Center for Hip Preservation, Hospital for Special Surgery, New York, NY.Address reprint requests to Asheesh Bedi, MD, Department of Orthopaedic
Surgery, MedSport, University of Michigan Hospitals, Lobby A, Domi-no’s Farms, 24 Frank Lloyd Wright Drive, Ann Arbor, MI 48105. E-mail:
[email protected]260 1060-1872/12/$-see front matter © 2012 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1053/j.otsm.2012.09.004
the dynamic and static mechanical factors is required to for-mulate a comprehensive and effective treatment plan.
A treatment algorithm based on recognizing the dynamicand static mechanical forces contributing to symptomaticprearthritic hip pain has been developed.13 Dynamic factorsre those in which there is abnormal contact between theemoral head and acetabular rim during hip motion that re-ults in abnormal stress and shear forces. Most commonly,uring positions of hip flexion, the abnormal femoral headontacts the anterior acetabular rim and causes impinge-ent. Similarly, abnormal femoral or acetabular anteversion
an result in posterior impingement when the hip is takenhrough full extension and external rotation. Dynamic im-ingement most commonly causes localized anteromedialroin pain, although abnormal mechanical stress and com-ensatory changes secondary to restricted terminal motionan lead to lumbar spine, sacroiliac (SI) joint, pubic symphy-is, and posterior acetabular pain.13 Underlying impinge-
ment can alter the mechanics and motion surrounding thehip joint, which ultimately can alter dynamic muscle forcesacross the pelvis. The surrounding joints and muscles thatmay be subsequently strained and commonly injured includethe adductor longus, proximal hamstrings, abductors, iliop-soas, and hip flexors.
When patients are standing in an upright position with thehip joint axially loaded, static factors can result in abnormal
stresses and asymmetric load to chondral surfaces of the fem-
rtiut
v
sekn
mttl
Static and dynamic hip pathomechanics 261
oral head and acetabulum. Insufficient congruency betweenthe femoral head and acetabular socket causes asymmetricwear of the articular surfaces with or without associated in-stability of the hip.12,14-22 Pain from static factors does notequire hip motion, and although it may also present as an-eromedial groin pain, the surrounding musculature, includ-ng abductors, iliopsoas, and adductors, often becomes oversed, causing fatigue and pain. In this report, we will reviewhe following:
1. Dynamic factorsA. Cam lesions: loss of offset and asphericity of the
femoral head-neck junctionB. Acetabular overcoverage
i. Focal rim impingement lesiona. Cephalad retroversion (focal rim lesion)b. True acetabular retroversion
ii. Global overcoverage of acetabulum—profundaand protrusio
C. Femoral retroversionD. Femoral varus
2. Static factorsA. Anterior or lateral undercoverage of acetabulum
(dysplasia)B. Femoral anteversionC. Femoral valgus
3. Combined patternsA. Impingement with femoral retroversionB. Paradoxical acetabular dysplasia with FAI
4. Additional injury patterns seen with FAIA. Sports hernia and athletic pubalgiaB. Osteitis pubisC. SI jointD. Muscle injuryE. Hip instability
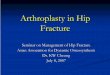
Dynamic FactorsCam Lesions: Asphericityof the Femoral Head-Neck andLoss of OffsetIn the active patient with hip pain, a loss of femoral head-neck offset and asphericity (cam deformity) is a commonmechanical factor associated with hip pathology (Fig. 1). Theabnormal bone in the nonspherical portion of the femoralhead causes shear forces against the acetabulum with termi-nal hip motion, eventually leading to the commonly seenpattern of anterosuperior acetabular cartilage loss and subse-quent degenerative labral changes.1-18,23-42 During dynamichip motion, including flexion and internal rotation for themost typical anterosuperior cam deformity, the transitionzone of the femoral head and adjacent acetabular cartilage aresubjected to resultant shear injury. Because these shear forcesare continually encountered over many cycles, cartilaginouslesions become deeper and involve the weight-bearing domeof the acetabulum (Fig. 2).6,9 The cartilage lesions that de-
elop can be treated surgically with simple debridement and ttabilization, microfracture, or abrasion chondroplasty; how-ver, the long-term effects of this disease process remain un-nown because these treatments are unable to restore theative hyaline articular cartilage.9 Labral tears along with
subsequent cartilage delamination occur at correspondinglocations of the cam deformity along the circumference of thehead-neck junction. In the zone where the abnormal head-neck junction and acetabular rim make pathologic contactwith terminal motion, the labrum is compressed with resul-tant secondary tearing and detachment from the acetabularrim. Healing rates of these tears are favorable compared withintrasubstance tears because of vascular supply from adjacenthip capsule.9 The size of the cam lesion, as assessed by ahigher offset alpha angle, which measures the aspherical por-tion of the femoral head, has been associated with greaterpresence of acetabular chondral defects and delamination ofcartilage (Fig. 3).43 These lesions are commonly addressedwith arthroscopic or open osteochondroplasty. Kelly et al44
recently reported on the arthroscopic outcomes of 56 pa-tients with increased alpha angles associated with combinedcam lesions and labral pathology, with overall improvementin radiographic alpha angle from 68.0 � 10.0 degree preop-eratively to 43.4 � 4.0 degree and corresponding improve-
ent in clinical outcome scores. Anderson et al35 reported onhe retrospective review of 64 hips that had surgical disloca-ion for treatment of FAI. Delamination of acetabular carti-age was found in 44% at the time of open surgical disloca-
Figure 1 Three-dimensional computed tomography (CT) recon-struction of left hip with femoroacetabular impingement (FAI) andprominent cam lesion. There is loss of offset of the typical antero-superior location of the femoral head-neck junction (asterisk). Camimpingement occurs with engagement of the nonspherical bonewith the acetabular rim, and resultant delamination of articularcartilage and labral tears develop overtime.
ion. A higher association of delamination was found with the

262 M.J. Knesek et al
male sex and large cam deformity. Labral tears and delami-nation lesions were found to be directly adjacent within theoperative hip. In this series, the preoperative imaging modal-ity of magnetic resonance arthrography showed low sensitiv-ity for (22%) but high specificity (100%) for delamination.35
For the treating surgeon, cam lesions and loss of head-neckoffset can be addressed surgically by either arthroscopic oropen approaches.35,44 Cadaveric and clinical studies havefound no statistically significant difference in measurements
Figure 2 (A) Axial T1-weighted magnetic resonance arthrographydemonstrating labral tear adjacent to asterisk. Labral pathology ismost commonly seen in the zone where the abnormal head-neckjunction and acetabular rim make pathologic contact in terminalmotion. The labrum is subsequently compressed and, eventually,labral tearing and detachment occur. (B) Coronal T1-weighted mag-netic resonance arthrography demonstrating cartilage delamina-tion. The areas of delamination often occur adjacent to detached ortorn labrum. During dynamic hip motion, the transition zone of theabnormal femoral head and acetabular cartilage is subjected to shearinjury with resultant delamination.
of resection between open and arthroscopic procedures.36 A
recent review of clinical outcomes comparing open surgicaldislocation versus arthroscopy versus combined for treat-ment of FAI found no significant difference; however, ar-throscopic method demonstrated the lowest complicationrate and fastest rehabilitation.45 Preoperative recognition, in-traoperative exposure, and achieving a complete intraopera-tive resection remain the most important technical consider-ations to ensure a favorable long-term outcome, as residualcam deformity remains the most common reason for revisionhip arthroscopy.37,46 A recent radiographic comparison dem-onstrated that arthroscopic osteoplasty can restore head-neck offset and achieve similar depth, arc, and proximal-distal resection for more anterior and anterosuperior cam andfocal rim impingement lesions as open surgical dislocationtechniques and with similar efficacy.47 CT and secondarycomputer modeling may assist in localizing the lesion andpathologic mechanical conflict preoperatively, whether openor arthroscopic resection is performed.48 Whether the proce-dure is arthroscopic or open, the resection is maintained at 2years in the great majority of cases as recorticalizationoccurs.15
Acetabular OvercoverageFocal Rim Impingement LesionFocal acetabular overcoverage or retroversion is commonlyobserved at the cranial aspect of the acetabulum and is an-other dynamic factor that causes hip pain in the young pa-tient. The focal rim lesion can result in degeneration andtearing of the anterosuperior labrum with repetitive cyclical
Figure 3 Axial CT image of patient with FAI and CAM impingementas demonstrated by abnormal alpha angle (72.4°). To measure alphaangle, a concentric circle is drawn around the femoral head. Thesubsequent angle is formed between a line from the center of thefemoral head running perpendicular to a line through the center ofthe femoral neck and a second line from the center of the femoralhead to the point at which the head-neck junction no longer fallsinside the concentric circle. Abnormal alpha is indicated by a value
�55°.
fhPg
srqbelt
rgfrdls
sBrgHsloloni
Tmnpr“
msotaatt
Static and dynamic hip pathomechanics 263
collisions and focal acetabular rim fragments (Fig. 4). In ad-dition, a characteristic posteroinferior cartilage loss is foundwithin the femoral head and corresponding acetabulum(contrecoup pattern).5,6,9 A review of 250 radiographs withocal acetabular rim lesions by Ezoe et al15 demonstrated thatips with OA, developmental dysplasia, or Legg–Calve–erthes disease were significantly more likely to have focal orlobal acetabular retroversion.
Labral injury from the focal rim impingement is commonlyeen as intrasubstance fissuring and can often be difficult toepair directly because of impaired tissue quality. Because theuality of the labrum diminishes overtime, there is moreone apposition between femoral head and acetabulum andventual adjacent callus formation and ossification of theabrum.4,9,33,34 However, the femoral cartilage remains rela-ively uninvolved.
The contrecoup lesion specific to rim lesions is thought toesult because hip flexion and rotation proceeds beyond en-agement of the focal rim lesion, with resultant levering of theemoral head and subsequent shear forces placed on poste-ior hip chondral surfaces (Fig. 5).9 The location of labralegeneration and fissuring is often found with the bony rim
esion, and the resultant contrecoup lesion is directly oppo-ite, usually at the posteroinferior acetabulum.
Arthroscopic resection of pincer-type lesions has demon-trated favorable results at 2-year follow-up, as described byyrd and Jones,49 in isolation or in association with concur-ent cam resection. In their cohort of 100 patients, 79 hadood-to-excellent results and the median improvement inarris Hip Score was 21.5. Recent cadaveric studies demon-
trated that more posterosuperior focal rim lesions may be lessikely to be completely resected arthroscopically via the anteriorr anterolateral portals. Some hip surgeons avoid the postero-ateral portal because of its closer proximity to the medial fem-ral circumflex contribution to the femoral head and sciaticerve;39 therefore, open procedures may be indicated depend-
Figure 4 Axial CT image demonstrating bilateral ossicles on the an-terior acetabular rim. Because of abnormal stress in impinging hips,especially in setting of focal rim impingement, the prominent ace-tabular bone fragment can be seen separated from the adjacent bonemargin.
ng on location of the focal overcoverage.
rue Acetabular Retroversion Although a relatively uncom-on finding, global acetabular retroversion must be recog-ized as a distinct cause of mechanical hip pain in the youngatient without OA. The diagnosis can be based on plainadiographic findings, specifically “crossover sign” with theischial spine sign”50 or “posterior wall sign,” where the pos-
terior wall passes medial to the center of the femoral head ona well-positioned anteroposterior (AP) radiograph (Fig.5).16-18 Although Jamali et al18 reported initially that stan-dardized AP pelvic radiographs can be used as a reliable toolto determine acetabular retroversion, a recent study suggeststhe contrary because of pelvic tilt and inherent limitations ofradiographs.51 Further imaging studies to include CT scans
ay more accurately define the presence of global retrover-ion and/or posterior wall insufficiency (Fig. 6).14 Symptomsf pain during dynamic motion are similar to those of pa-ients with focal rim lesions; however, patients with truecetabular retroversion demonstrate overcoverage anteriorlynd undercoverage posteriorly, which may predispose pa-ients to symptomatic posterior instability and even disloca-ion.52 When open or arthroscopic surgery is performed in
these patients, the surgeon should be cautious about aggres-sive anterior rim trimming to avoid potential for iatrogenicinstability. If these patients have the primary complaint ofinstability, however, an anteverting periacetabular osteotomymay be indicated to improve overall hip mechanics.33,52
Profunda and Protrusio DeformityThe description of an acetabulum that protrudes into the truepelvis was described long ago by Otto53 in 1816 as protrusiodeformity.12 This deepened acetabulum is evidenced by me-dialization of the teardrop, resulting in a global overcoverageof the femoral head, which is a distinct form of dynamicimpingement (Fig. 7). As a result of the protrusio deformity,
Figure 5 Standard anteroposterior (AP) radiograph of patient withFAI, demonstrating bilateral retroverted acetabula as evidenced bythe prominent ischial spines bilaterally (PRIS). On a normal APradiograph, the ischial spine lies lateral to the iliopectineal line,whereas in acetabular retroversion, it can clearly be seen within thepelvic brim. AR, acetabular roof; PW, posterior wall; AW, anterior
wall. Published with permission of Kalberer et al.50
oaiwcdcgw
clpsc
all co
264 M.J. Knesek et al
load transmission is higher through the medial aspect of thehip joint, causing loss of medial joint space and secondaryOA. The craniolateral joint space remains largely unaffectedin this patient population.19 Leunig et al12 recently reportedn morphologic characteristics of patients with protrusio-ssociated arthritis. Their retrospective review revealed thatn comparison with classic joint-space narrowing, patientsith protrusio had decreased medial joint space and in-
reased superior joint space. Furthermore, when viewing ra-iographic differences between protrusio hips and an OAontrol group, they found that all hips in the protrusioroup had an ilioischial line lateral to the acetabular fossa,hereas the opposite was found in the control group. The
Figure 6 (A) AP pelvis radiograph demonstrating “posteriis medial to the center of the femoral head, which indidimensional CT reconstruction of the same right hip shcoverage of the anterior wall and insufficient posterior w
Figure 7 (A) AP pelvis radiograph showing deeper thanilioischial line and subsequent protrusio deformity, a di
results from additional medialization of the femoral head.enter of rotation of the femoral head was also found to beower than the tip of the greater trochanter in 93% ofatients with protrusio, whereas the neck-shaft angle wasubstantially less (121 degrees) in the protrusio groupompared with OA patients (130 degrees).12 On the basis
of findings on protrusio patients who underwent opensurgical dislocation, they proposed that contrecoup de-struction of the posterior joint from chronic impingementis the inciting factor of the osteoarthritic process, insteadof the pathologic medializing forces that are more com-monly discussed.12,20,21,54
Historically, resection arthroplasty and arthrodesis werethe treatment for acetabular protrusio with OA, but total hip
sign” of acetabular retroversion. Note the posterior wallpositive posterior wall sign. (B) Corresponding three-global acetabular retroversion, with subsequent over-
verage.
l acetabulum, with medialization of the teardrop to theorm of dynamic impingement. (B) Protrusio deformity
or wallcates aowing
normastinct f

ollttapaccb
fodlmtmwstdics
cuwmtIn2pla
v
osp
sotp
taontst
Static and dynamic hip pathomechanics 265
arthroplasty is currently the recommended surgical treat-ment. In the young patient without significant arthriticchanges, valgus intertrochanteric osteotomy has also beenrecommended to change the forces across the hip joint.11
These patients typically present with physical examinationfindings similar to those of focal rim lesions; however, it isimportant to understand the extent of the true deformity.Unlike a focal rim lesion, profunda or protrusio results fromcircumferential coverage around the rim, and thus if theproblem is addressed arthroscopically for the typical antero-superior rim resection, only a small component of the me-chanical impingement will be addressed. Furthermore, re-cent finite element models have shown that isolated rimresection, even if thorough, does not correct the medializingforces and chondral overload with profunda and protrusiodeformity.55 As a result, Leunig et al4,9,12 have recommendedpen surgical dislocation for circumferential trimming andabral refixation when appropriate. Some authors discussengthening of the femoral neck via osteochondroplasty ofhe head-neck junction and trochanteric distalization to ob-ain a relative lengthening of the femoral neck. This allows forn overall increase in femoroacetabular clearance.21,22 De-ending on findings of magnetic resonance arthrography andbnormalities of the acetabular cartilage, a valgus intertro-hanteric osteotomy or pelvis-sided osteotomy may be indi-ated to lateralize the femoral head and shift the weight-earing zone.9,21
Femoral RetroversionIn the adult male, the mean femoral anteversion angle mea-sures approximately 15 degrees.56 There is a spectrum ofemoral anteversion, with some patients having relative fem-ral retroversion (�15 degrees) or absolute retroversion (�0egrees). Within this spectrum, those in the relative or abso-
ute range have a distinct dynamic factor that can result inechanical hip pain and impingement with flexion and in-
ernal rotation even in the absence of significant cam defor-ity. In this regard, relative or absolute femoral retroversionith associated cam or rim impingement lesions may amplify
ymptomatology because the cam lesion can be rotated intohe socket before initiation of hip flexion because of the un-erlying hip morphology.13,17,22,57 These patients are also at
ncreased risk for labral pathology, and ultimately may haveompensatory injuries because of necessary adaptationstemming from restricted internal rotation and flexion.
For the majority of patients with femoral retroversion andoncomitant cam lesions, isolated arthroscopic resection issually sufficient. Kelly et al44 demonstrated that patientsith FAI can have an overall improvement in hip range ofotion after arthroscopic surgery, specifically internal rota-
ion, even in the setting of preoperative femoral retroversion.n 56 patients who underwent decompression, average inter-al rotation increased from 9.9 degrees preoperatively to7.6 degrees after arthroscopy. However, there remain someatients with significant posterolateral extension of the cam
esion in which an open dislocation is necessary to achieve
dequate decompression while protecting the retinacular wessels.1,2,4,10,32,57 If this task is attempted with arthroscopicsurgery, it should be performed with the hip in tractionand/or extension to safely access and visualize this area.58
When isolated femoral retroversion is present without ev-idence of cam or rim lesions, a femoral derotational osteot-omy can be considered to treat the mechanical hip pain.However, when both femoral retroversion and cam or rimlesions are simultaneously present, the most inclusive treat-ment involves surgical dislocation with osteoplasty of thehead-neck junction along with concurrent derotational ante-verting osteotomy.1,2,4,10,32,57-59
Femoral VarusFemoral varus, or coxa vara, is the other dynamic factor thatmust be recognized in the evaluation of mechanical hip pain.Although coxa vara can be developmental or acquired(slipped femoral epiphysis, Perthes disease, trauma, infec-tion, rickets, etc), the relative shortening of the femoral neckand prominence of the greater trochanter from the decreasedneck-shaft angle can result in extra-articular lateral impinge-ment of the greater trochanter on the anterior inferior iliacspine and soft tissue.13,60 Furthermore, in patients with camr rim impingement lesions in the setting of coxa vara, theymptomatic intra-articular and lateral impingement is am-lified because of the hip pathomechanics.42,61-64 In mild
coxa vara, isolated cam and rim osteoplasty may offer symp-tomatic relief of symptoms; however, when a significantvarus deformity is present (�125 degrees), a more extensiveurgery may be required in the form of trochanteric osteot-my, relative neck lengthening, valgus intertrochanteric os-eotomy, and/or a distal trochanteric advancement for im-rovement in the articulotrochanteric distance.64
Static FactorsAcetabular DysplasiaHip dysplasia is a developmental condition in which the hipjoint forms incorrectly during early infancy and childhood,with resultant abnormal morphology of the acetabulum, fem-oral head, or both.65 The most common radiographic mea-surement to assess acetabular dysplasia is the center edgeangle of Wiberg,66 formed by a line perpendicular to theransverse axis of the pelvis from the femoral head center andline from the femoral head center to the superolateral pointf the acetabulum. Compared with individuals who haveormal development of the acetabulum, individuals with an-erior or lateral undercoverage have a smaller weight-bearingurface, which results in elevated contact stresses that even-ually contribute to labral and/or articular cartilage damage.67
Studies have demonstrated that contact forces shift towardthe posterosuperior rim of the acetabulum in individualswith dysplasia.68 Additionally, the structural instability thatresults from the undercoverage allows the femoral head to mi-grate into regions where there is acetabular deficiency. The re-current subluxation and instability events ultimately lead to de-generation and damage of the cartilage as well.40,68-70 Compared
ith those with normal hip morphology in the general popula-

mcm
rdtfoli
owtbct
s
266 M.J. Knesek et al
tion, hip OA tends to develop much earlier in patients withdevelopmental dysplasia.68,70-74 This is related to the local eleva-tion in contact forces on articular cartilage, which may lead topremature cartilage degeneration and premature OA (Fig. 8).68
The constellation of elevated contact pressures, recurrent insta-bility, and resultant subluxation leads to anterolateral labral de-generation, anterolateral acetabular chondromalacia, synovialcysts, and acetabular rim lesions, with ultimate development ofhip arthrosis unless the undercoverage is corrected.70,72,73
Acetabular redirection osteotomies are technically chal-lenging procedures used to treat patients with painful hipdysplasia.72 The theoretical goals of periacetabular osteoto-
ies include reorientation of the acetabulum to distributeontact pressures more equally and to better contain the fe-ur and prevent subluxation.40,41,72,74-93 Preoperative assess-
ment of acetabular morphology via CT is important to surgi-cally address and correct the relationship of the abnormalacetabulum and femoral head.91 If performed correctly, peri-acetabular osteotomy can provide multidimensional correc-tion of static undercoverage. This can be concomitantly per-formed with femoral osteotomy if necessary depending onunderlying femoral morphology.40,41,72,74,93 Associated femo-al deformity is not uncommon in the setting of acetabularysplasia, and thus labral pathology, femoral head-neck os-eochondroplasty, trochanteric advancement procedures,emoral neck lengthening, and varus or valgus proximal fem-ral osteotomies performed concomitantly with periacetabu-ar osteotomies will optimize hip joint pathomechan-cs.75,76,78
Since Ganz et al94 described the challenges of the periace-
Figure 8 AP radiograph of patient with acetabular undercoverage(dysplasia) of the right hip. The smaller weight-bearing surface re-sults in static overload and elevated contact stresses, leading toeventual cartilage damage. The local elevation in forces across thearticular cartilage leads to earlier osteoarthritis in these individualscompared with the general population.
tabular osteotomy surgical technique and preliminary re- t
sults, the reported outcomes have improved, as recently re-ported by Millis et al,84 Siebenrock et al,95 and Matheneyet al.96 Steppacher et al97 recently reported 20-year outcomesthat demonstrated preservation of the hip in selected patientsundergoing Bernese periacetabular osteotomy.97 Periace-tabular osteotomy is also performed in conjunction with hiparthroscopy to address concomitant hip pathology, such aslabral tears.98 Although it remains controversial in patientslder than 40 years, periacetabular osteotomy in individualsith early stage OA can achieve satisfactory results, and ar-
hroscopic evaluation of cartilage for staging purposes maye undertaken before any osteotomy procedure to more ac-urately identify patients who will achieve satisfactory long-erm results.84,92,96
Femoral AnteversionFemoral anteversion �15 degrees is considered a morpho-logic abnormality that can be a static cause of mechanical hippain in the active patient population. Recent CT studies havesuggested that femoral anteversion may be more common inpatients with acetabular anteversion and in patients withanterior or global deficiency associated with dysplasia, itcan be found independent of other abnormal hip mor-phology.56,99 When examining these patients, they are foundto have an increase in their functional internal rotation of thehip joint with a correspondingly decreased external rota-tion.44,100-102 As a result of their altered arc of motion, thesepatients may develop both intra-articular and extra-articularsymptomatic impingement. When these patients perform ac-tivities that require hip flexion and simultaneous externalrotation, they may feel the greater trochanter engaging thepelvis, causing extra-articular impingement. During hip ex-tension and external rotation, these patients experience intra-articular impingement of the femoral neck and acetabularrim. It is extremely important to decipher between the causesof intra-articular or extra-articular symptoms in these pa-tients with femoral anteversion to develop an operative planthat will successfully alleviate their symptoms without exac-erbating instability. In patients with severe femoral antever-sion �30 degrees, arthroscopic treatment of the acetabularrim impingement may be unsuccessful if concurrent femoralderotational osteotomy is not performed.100,101
Increased femoral anteversion may also lead to moresymptomatic pain of the anterior hip soft tissue stabilizers,because of the static chondral and subchondral overload ofthe anterosuperior head and dome on the anterior stabilizers,including the capsule and iliopsoas tendon. A recent studydemonstrated that femoral version, specifically femoral ante-version, may lead to inferior outcomes after arthroscopiclengthening of the psoas tendon, likely related to the under-lying overload from the anterosuperior head on the sur-rounding structures and risk of iatrogenic instability.103
Those patients with femoral anteversion �30 degrees, withtatic symptoms, should be considered for derotational os-
eotomy as well.100,101
dv
cohspfttts
cds
wufn�pcicfr
asteasc
1mos
Static and dynamic hip pathomechanics 267
Femoral ValgusCoxa valga is another static factor that must be considered inthe diagnosis and management of hip pain in the youngadult. The finding of an increased neck-to-shaft angle �135
egrees is more common in combination with femoral ante-ersion and acetabular undercoverage.40,41,76,78,82,84,92,96
These patients may complain of symptoms of pain and/orinstability, as the anterosuperior head and dome are sub-jected to static overload, while also experiencing instability inextremes of extension and external rotation. Surgical treat-ment in the form of a varus derotational osteotomy must beconsidered in patients with coxa valga and recurrent me-chanical hip pain combined with other indicated proce-dures.100,104
Commonly EncounteredCombined PatternsImpingement and Femoral RetroversionAs discussed previously in the text, retroversion of the femurfunctionally reduces the internal rotation of the hip.13,17,21 Inthis regard, femoral retroversion may exacerbate symptomsfrom loss of motion due to impingement lesions becausediminished hip flexion and internal rotation is required forengagement of a cam and/or focal rim lesion.13 Kelly et al44
recently reported improvement in overall hip range of mo-tion after arthroscopic decompression of cam lesions, even inthe setting of femoral retroversion, but the impact and mag-nitude of improvement in this setting remain undefined. Fur-ther research is necessary to determine the role for ar-throscopic decompression and/or derotational femoralosteotomy in the management of symptomatic patients.
FAI with Acetabular DysplasiaAlthough uncommon, acetabular dysplasia and FAI can bothbe present and result in mechanical hip pain. Patients under-going periacetabular osteotomy for treatment of dysplasiahave demonstrated concurrent labral pathology and loss offemoral offset, which have been previously addressed withconcurrent anterior arthrotomy at the time of periacetabularosteotomy.70,73 To address concurrent impingement andchondral pathology more accurately, Anderson et al35 re-ently described surgical dislocation before periacetabularsteotomy to manage these patients. In their series, 2 patientsad Legg–Calve–Perthes deformities and 2 others demon-trated evidence of FAI with acetabular deficiency. This ap-lication is likely ideal for patients with profoundly abnormalemoral morphology. At a mean follow-up of 38.8 months,he Harris Hip Score improved from 65 points preoperativelyo 96.8 after staged surgical dislocation followed by periace-abular osteotomy. This is a complex but clinically effectiveolution for the uncommon patient population.
Gunther et al101 presented an alternative algorithm, in-luding simultaneous arthroscopically assisted osteochon-roplasty with periacetabular osteotomy, with short-term re-
ults in 19 patients at an average of 8.9 months. Their short-term radiographic parameters demonstrated an averageimprovement in the alpha angle from 58.3 degrees preoper-atively to 42.5 degrees postoperatively, and improvement incenter-edge angle from 19.0 degrees to a postoperative aver-age of 31 degrees. Harris Hip Scores improved from an aver-age of 67.6 to 89.4, postoperatively.101
Clohisy et al78 reported on a series of 24 hips that under-ent Bernese periacetabular osteotomy, whereas 13 of thosenderwent concurrent femoral valgus-producing osteotomyor the treatment of acetabular dysplasia associated with ab-ormal proximal femoral morphology. At final follow-up of4 years, the mean Harris Hip Score increased from 68.8
reoperatively to 91.3 postoperatively, with 22 of 24 patientslinically improved. There was also significant improvementn multiple radiographic parameters, with the authors con-luding that periacetabular osteotomy along with concurrentemoral procedures allow for comprehensive deformity cor-ection for this complex constellation of pathology.40,75-77
Associated InjuryPatterns with FAIOsteitis PubisOsteitis pubis remains one of the many causes of groin pain inathletes, defined as diffuse pain, inflammation, instability,and eventual bony changes to the symphysis pubis.105,106
This overuse injury is most commonly seen in sports, such assoccer, which involve kicking, rapid changes in accelerationor deceleration, twisting, and abrupt directional changes.The adductor musculature has been implicated, as it insertsat the pubic tubercle (Fig. 9).107-109 Athletes may complain of
constellation of symptoms, although most commonly de-cribe anterior and/or medial groin pain. Scrotal pain, adduc-or tenderness, and lower abdominal pain can also be pres-nt. Treatment is usually self-limiting, which includes rest,nti-inflammatory medications, and rehabilitation, althoughurgical intervention has been rarely reported in persistentases.110-113 Two separate case series, including 25 athletes,
were treated with pubic symphysis curettage, and of thoseathletes, 72% were able to return to full sporting activity at amean of 5.6 months.113,114 Two other case series comprising
3 patients who underwent placement of polypropyleneesh into the preperitoneal retropubic space for refractory
steitis pubis demonstrated a success rate of 92.3% return toport at a mean of 7.2 weeks.115,116
Sports Hernia and Athletic PubalgiaAthletic pubalgia, otherwise known as sports hernia, remainsone of the more difficult diagnoses for the orthopedic sur-geon because of the challenging presentation and broad dif-ferential diagnoses of chronic lower abdomen and groin pain.This syndrome of chronic lower abdominal and groin painoccurs in both male and female competitive and recreationalathletes. It has been defined as a weakness or tearing of therectus abdominus insertion at the superior pubic ramus.117
Athletes typically complain of exercise-related lower abdom-
inal and groin pain that may radiate to the scrotum or inner
na
o
ppasclwt
sspc
tamp
sasa
268 M.J. Knesek et al
thigh.118,119 Sports hernias have been described as occult her-ias because of tearing of the posterior inguinal wall withoutclinically recognizable hernia.120 There has been clinical
correlation between athletic pubalgia and FAI, likely relatedto restriction of hip flexion and internal rotation altering thenormal mechanics of the hemipelvis.13 Larson et al121 re-ported on 37 patients who had both intra-articular hip pa-thology and extra-articular sports pubalgia demonstratingthat when pubalgia was addressed as the index procedure,only 25% (4) of patients returned to sports without limita-tions. However, when both disorders were addressed con-currently, 89% (24 of 27) of patients returned to competitivesporting unrestricted.121 Hammoud et al122 recently reported
Figure 9 (A and B) Coronal T-2 weighted magnetic resonance imageswith injury to the adductor musculature origin and reactive bonemarrow edema of the pubic symphysis. Arrows denote marrowedema at the origin of the adductor musculature at the pubic sym-physis.
n 38 professional athletes who had concomitant athletic
ubalgia and FAI. In this group, 39% (15/38) had athleticubalgia symptoms that resolved with FAI surgery alone, andll 12 patients who underwent combined pubalgia and FAIurgery were able to return to professional competition. Re-ent cadaveric studies have linked the presence of a camesion to increased rotational motion at the pubic symphysis,hich may provide a mechanistic explanation of the connec-
ion between FAI and athletic pubalgia.123 Treatment de-pends on the correct diagnosis, and typically starts with rest,physical therapy for core and hip strengthening, and non-steroidal medications. Laparoscopic or open repair and/orreinforcement of the abdominal wall fascia is indicated inrefractory cases.120,124-128 If other hip pathology is present,urgical management of intra-articular pathology along withurgery to treat athletic pubalgia may provide the most com-rehensive and reliable treatment to achieve favorable clini-al outcomes.121
SI JointLow back pain is a common complaint affecting approxi-mately 70% of individuals at some time in their life, with theSI joint found as the pain generator in up to 30% ofcases.129,130 Pain in the SI joint can result from both degen-erative and inflammatory arthritis, infection, and stress frac-tures, and in the setting of hypermobility, which may occursecondary to the restricted terminal hip motion of FAI. The SIjoint is supported by many muscles, including the gluteusmaximus and minimus, erector spinae, latissimus dorsi, bi-ceps femoris, psoas, piriformis, and transverse and obliqueabdominal muscles, all of which serve to link the lower ex-tremities and the spine, predisposing the bony and soft tissuestructures to injury during athletic activity.131-135 These pa-ients typically complain of pain localized near the buttocknd groin; however, occasional pain radiating into the thighay be present. Palpation over the SI joint can reproduce theain,131-135 and a recent meta-analysis confirmed that provoc-
ative tests, including the thigh thrust and compression test,can reliably reproduce symptoms.136 Treatment is often con-ervative, in the form of physical therapy, core strengthening,nti-inflammatory medication, and corticosteroid injections;urgical arthrodesis may be performed in cases of severe painnd dysfunction.131-136
Muscle InjuryInjury to the adductor complex, specifically adductor longus,is a common cause of groin pain and inability to participate inathletic competition.108,137-140 The muscles about the pelvis,including the adductor complex, are partly responsible forthe stability of the hip joint, and thus are subject to high loadsduring activity.139,141-143 Risk factors for injury to the adduc-tor longus include adductor tightness, previous injury to theadductor muscle, imbalance between the hip adductor-ab-ductor complex,142,143 and decreased hip range of motion.144
Strengthening of the adductor muscle group in a preseasonprogram was found to be a valuable intervention to preventadductor strains in professional ice hockey players.3 Physical
examination may reveal ecchymosis and swelling in the acute
sipmcic
fptt
ct
aatTgNas
Static and dynamic hip pathomechanics 269
period, as well as tenderness at the adductor enthesis.3,141-143
In addition, the patient often has pain with adductor stretch-ing and resisted adduction.137-139,141,143 MRI often demon-trates increased signal within the adductor muscle, confirm-ng the diagnosis if further imaging is required. It has beenreviously hypothesized that patients with symptomatic FAIay demonstrate “cam avoidance gait” and an overall de-
rease in terminal hip range of motion, which may placencreased stress on the adductor complex, resulting inhronic microtrauma and injury.13,108,140 Feeley et al have
recently described the “sports hip triad” involving a labraltear, adductor strain, and rectus strain.13 The underlyingemoral or acetabular deformity involved in FAI may be im-licated in the exacerbation of other muscle injuries aroundhe pelvis in athletes secondary to compensatory motion ofhe hemipelvis.145 Prevention is critical with all muscle in-
juries, including preseason strengthening and stretchingas well as range-of-motion exercises. Mainstay of treat-ment includes rest, ice, physical therapy, stretching, andrange-of-motion exercises.137-139,142,145 Corticosteroid orplatelet-rich plasma injections for muscle injury have beenused with some success.108,140,146 Surgical management in-ludes adductor tenotomy in the cases of chronic tendinopa-hy that has failed all other measures.139,147 Robertson et al147
recently described results from their series of amateur ath-letes who underwent adductor tenotomy for refractory ad-ductor tendinopathy, with 91% (32 of 38) of patients able toreturn to sport at a mean of 15 weeks.
Hip InstabilityHip stability is largely determined by its osseous anatomy andconformity of the femoral head within the acetabular fossa.The spectrum of instability ranges from subluxation to dislo-cation with or without concomitant injuries.148 Just as inother joints, such as the shoulder and knee, hip instabilitycan be a source of great disability leading to devastating con-sequences if left unrecognized in the athlete. The most com-mon mechanism for posterior subluxation and injury re-mains a fall with the hip in flexion and adduction with aposteriorly directed force. Hip dislocation has been reportedin multiple sports, including biking, rugby, football, dancing,track, basketball, and hockey.38,148-153 Both osseous abnor-malities within the hip joint and generalized ligamentous orcapsular laxity have been implicated to predispose patients tohip instability.38,145,148
Patients with traumatic hip instability present with severediscomfort and limited range of motion of the affected ex-tremity. If the patient has a traumatic dislocation, the extrem-ity is usually in flexion, internal rotation, and adduction. Thetreating clinician must have a high awareness for this injurygiven the potentially serious long-term sequelae. Radio-graphs, including AP pelvis and frog-lateral views, can con-firm dislocation, and reduction of the hip should be per-formed within 6 hours to minimize the risk of avascularnecrosis. Subsequent MRI in the event of instability withoutdislocation can demonstrate posterior labral tear, disruption
of the iliofemoral ligament, and hemarthrosis.148,150-153Hip arthroscopy has been described in the treatment afteracute dislocation or recurrent subluxation.38,153 Philippon etl38 described the arthroscopic treatment of 14 professionalthletes who sustained traumatic hip dislocation and werereated with surgery an average of 125 days after the injury.he most common intra-articular pathology identified at sur-ery included labral tears, chondral defects, and loose bodies.ine patients had evidence of FAI on arthroscopy. All 14
thletes were able to return to full competitive professionalports. Berkes et al153 recently described a case series of pos-
terior instability associated with FAI. All patients had evi-dence of posterior acetabular rim fracture associated withlabral injury that was addressed arthroscopically using 3 to 5suture anchors for fixation of bony acetabular fragments.One-year follow-up demonstrated full return to activitieswithout restriction, and the authors suggested that FAI pre-disposed these patients to traumatic posterior subluxationand concomitant acetabular rim fracture secondary to re-stricted internal rotation and secondary levering posteri-orly.153
ConclusionsThe approach to young patients with prearthritic hip painremains a complex and challenging problem for the treatingphysician. A complex constellation of static and dynamicparameters may contribute to mechanical abnormalities thatresult in symptoms in the active athlete. Compensatorychanges within the hip joint and surrounding musculaturemay exacerbate or produce additional extra-articular symp-toms. A comprehensive assessment and careful physical ex-amination in conjunction with appropriate imaging is re-quired for the treating physician to accurately diagnose andtreat this patient population.
References1. Peters CL, Erickson JA: Treatment of femoro-acetabular impingement
with surgical dislocation and debridement in young adults. J BoneJoint Surg Am 88:1735-1741, 2006
2. Peters CL, Erickson J: The etiology and treatment of hip pain in theyoung adult. J Bone Joint Surg Am 88:20-26, 2006
3. Tyler TF, Nicholas SJ, Campbell RJ, et al: The effectiveness of a pre-season exercise program to prevent adductor muscle strains in pro-fessional ice hockey players. Am J Sports Med 30:680-683, 2002
4. Beck M, Leunig M, Parvizi J, et al: Anterior femoroacetabular impinge-ment: Part II. Midterm results of surgical treatment. Clin Orthop RelatRes 418:67-73, 2004
5. Ganz R, Parvizi J, Beck M, et al: Femoroacetabular impingement: Acause for osteoarthritis of the hip. Clin Orthop Relat Res 417:112-120,2003
6. Ito K, Minka-Ii MA, Leunig M, et al: Femoroacetabular impingementand the cam-effect. A MRI-based quantitative anatomical study of thefemoral head-neck offset. J Bone Joint Surg Br 83:171-176, 2001
7. Wenger DE, Kendell KR, Miner MR, et al: Acetabular labral tears rarelyoccur in the absence of bony abnormalities. Clin Orthop Relat Res426:145-150, 2004
8. Dolan MM, Heyworth BE, Bedi A, et al: CT reveals a high incidence ofosseous abnormalities in hips with labral tears. Clin Orthop Relat Res469:831-838, 2011
9. Ganz R, Leunig M, Leunig-Ganz K, et al: The etiology of osteoarthritisof the hip: An integrated mechanical concept. Clin Orthop Relat Res
466:264-272, 2008
270 M.J. Knesek et al
10. Lavigne M, Parvizi J, Beck M, et al: Anterior femoroacetabular im-pingement: Part I. Techniques of joint preserving surgery. Clin Or-thop Relat Res 418:61-66, 2004
11. Leunig M, Ganz R: Femoroacetabular impingement. A common causeof hip complaints leading to arthrosis [in German]. Unfallchirurg108:12-17, 2005
12. Leunig M, Nho SJ, Turchetto L, et al: Protrusio acetabuli: New insightsand experience with joint preservation. Clin Orthop Relat Res 467:2241-2250, 2009
13. Bedi A, Dolan M, Leunig M, et al: Static and dynamic mechanicalcauses of hip pain. Arthroscopy 27:235-251, 2011
14. Werner CM, Copeland CE, Stromberg J, et al: Correlation of thecross-over ratio of the cross-over sign on conventional pelvic radio-graphs with computed tomography retroversion measurements. Skel-etal Radiol 39:655-660, 2010
15. Ezoe M, Naito M, Inoue T: The prevalence of acetabular retroversionamong various disorders of the hip. J Bone Joint Surg Am 88:372-379,2006
16. Frost A, Pavlou G, Richards PJ, et al: Influence of acetabular andfemoral version on fractures of the femoral neck. Clin Orthop RelatRes 468:2224-2229, 2010
17. Dandachli W, Islam SU, Liu M, et al: Three-dimensional CT analysisto determine acetabular retroversion and the implications for themanagement of femoro-acetabular impingement. J Bone Joint Surg Br91:1031-1036, 2009
18. Jamali AA, Mladenov K, Meyer DC, et al: Anteroposterior pelvic ra-diographs to assess acetabular retroversion: High validity of the“cross-over-sign”. J Orthop Res 25:758-765, 2007
19. Crowninshield RD, Brand RA, Pedersen DR: A stress analysis of ace-tabular reconstruction in protrusio acetabuli. J Bone Joint Surg Am65:495-499, 1983
20. Maquet P, Vu Anh T: On the forces exerted on the hip during gait.Arch Orthop Trauma Surg 99:53-58, 1981
21. Turgeon TR, Phillips W, Kantor SR, et al: The role of acetabular andfemoral osteotomies in reconstructive surgery of the hip: 2005 andbeyond. Clin Orthop Relat Res 441:188-199, 2005
22. Yoo WJ, Choi IH, Cho TJ, et al: Out-toeing and in-toeing in patientswith Perthes disease: Role of the femoral hump. J Pediatr Orthop28:717-722, 2008
23. Allen D, Beaulé PE, Ramadan O, et al: Prevalence of associated defor-mities and hip pain in patients with cam-type femoroacetabular im-pingement. J Bone Joint Surg Br 91:589-594, 2009
24. Larson CM: Arthroscopic management of pincer-type impingement.Sports Med Arthrosc 18:100-107, 2010
25. Larson CM, Giveans MR: Arthroscopic management of femoroac-etabular impingement: Early outcomes measures. Arthroscopy 24:540-546, 2008
26. Byrd JW, Jones KS: Arthroscopic femoroplasty in the management ofcam-type femoroacetabular impingement. Clin Orthop Relat Res 467:739-746, 2009
27. Lincoln M, Johnston K, Muldoon M, et al: Combined arthroscopic andmodified open approach for cam femoroacetabular impingement: Apreliminary experience. Arthroscopy 25:392-399, 2009
28. Larson CM, Giveans MR: Arthroscopic debridement versus refixationof the acetabular labrum associated with femoroacetabular impinge-ment. Arthroscopy 25:369-376, 2009
29. Kennedy MJ, Lamontagne M, Beaulé PE: Femoroacetabular impinge-ment alters hip and pelvic biomechanics during gait walking biome-chanics of FAI. Gait Posture 30:41-44, 2009
30. Brunner A, Horisberger M, Herzog RF: Sports and recreation activityof patients with femoroacetabular impingement before and after ar-throscopic osteoplasty. Am J Sports Med 37:917-922, 2009
31. Bardakos NV, Vasconcelos JC, Villar RN: Early outcome of hip ar-throscopy for femoroacetabular impingement: The role of femoralosteoplasty in symptomatic improvement. J Bone Joint Surg Br 90:1570-1575, 2008
32. Peters CL, Erickson JA, Anderson L, et al: Hip-preserving surgery:Understanding complex pathomorphology. J Bone Joint Surg Am 91:
42-58, 200933. Beck M, Kalhor M, Leunig M, et al: Hip morphology influences thepattern of damage to the acetabular cartilage: Femoroacetabular im-pingement as a cause of early osteoarthritis of the hip. J Bone JointSurg Br 87:1012-1018, 2005
34. Tannast M, Goricki D, Beck M, et al: Hip damage occurs at the zone offemoroacetabular impingement. Clin Orthop Relat Res 466:273-280,2008
35. Anderson LA, Peters CL, Park BB, et al: Acetabular cartilage delami-nation in femoroacetabular impingement risk factors and magneticresonance imaging diagnosis. J Bone Joint Surg Am 91:305-313, 2009
36. Mardones RM, Gonzalez C, Chen Q, et al: Surgical treatment of femo-roacetabular impingement: Evaluation of the effect of the size of theresection. J Bone Joint Surg Am 87:273-279, 2005
37. Philippon MJ, Schenker ML, Briggs KK, et al: Revision hip arthros-copy. Am J Sports Med 35:1918-1921, 2007
38. Philippon MJ, Kuppersmith DA, Wolff AB, et al: Arthroscopic findingsfollowing traumatic hip dislocation in 14 professional athletes. Ar-throscopy 25:169-174, 2009
39. Zumstein M, Hahn F, Sukthankar A, et al: How accurately can theacetabular rim be trimmed in hip arthroscopy for pincer-type femoralacetabular impingement: A cadaveric investigation. Arthroscopy 25:164-168, 2009
40. Clohisy JC, Keeney JA, Schoenecker PL: Preliminary assessment andtreatment guidelines for hip disorders in young adults. Clin OrthopRelat Res 441:168-179, 2005
41. Schoenecker PL, Clohisy JC, Millis MB, et al: Surgical management ofthe problematic hip in adolescent and young adult patients. J Am AcadOrthop Surg 19:275-286, 2011
42. Wenger DR, Kishan S, Pring ME: Impingement and childhood hipdisease. J Pediatr Orthop B 15:233-243, 2006
43. Johnston TL, Schenker ML, Briggs KK, et al: Relationship betweenoffset angle alpha and hip chondral injury in femoroacetabular im-pingement. Arthroscopy 24:669-675, 2008
44. Kelly BT, Bedi A, Robertson CM, et al: Alterations in internal rotationand alpha angles are associated with arthroscopic cam decompressionin the hip. Am J Sports Med 40:1107-1112, 2012
45. Botser IB, Smith TW Jr, Nasser R, et al: Open surgical dislocationversus arthroscopy for femoroacetabular impingement: A comparisonof clinical outcomes. Arthroscopy 27:270-278, 2011
46. Heyworth BE, Shindle MK, Voos JE, et al: Radiologic and intraopera-tive findings in revision hip arthroscopy. Arthroscopy 23:1295-1302,2007
47. Bedi A, Zaltz I, De La Torre K, et al: Radiographic comparison ofsurgical hip dislocation and hip arthroscopy for treatment of camdeformity in femoroacetabular impingement. Am J Sports Med 39:20S-28S, 2011
48. Bedi A, Dolan M, Magennis E, et al: Computer-assisted modeling ofosseous impingement and resection in femoroacetabular impinge-ment. Arthroscopy 28:204-210, 2012
49. Byrd JW, Jones KS: Arthroscopic management of femoroacetabularimpingement: Minimum 2-year follow-up. Arthroscopy 27:1379-1388, 2011
50. Kalberer F, Sierra RJ, Madan SS, et al: Ischial spine projection into thepelvis: A new sign for acetabular retroversion. Clin Orthop Relat Res466:677-683, 2008
51. Wassilew GI, Heller MO, Diederichs G, et al: Standardized AP radio-graphs do not provide reliable diagnostic measures for the assessmentof acetabular retroversion. J Orthop Res 30:1369-1376, 2012
52. Kuhn KM, Riccio AI, Saldua NS, et al: Acetabular retroversion inmilitary recruits with femoral neck stress fractures. Clin Orthop RelatRes 468:846-851, 2010
53. Otto AW. Ein Becken, mit kugelformig augedehnten Pfannen. In: HeftE. ed. Seltene Beobachtungen zur Anatomie, Physiologie und Patholo-gie gehorig. Vol IX. Breslau: Verlag Willibald August Holaufer; 19-20,1816
54. McBride MT, Muldoon MP, Santore RF, et al: Protrusio acetabuli:Diagnosis and treatment. J Am Acad Orthop Surg 9:79-88, 2001
55. Chegini S, Beck M, Ferguson SJ: The effects of impingement and

Static and dynamic hip pathomechanics 271
dysplasia on stress distributions in the hip joint during sitting andwalking: A finite element analysis. J Orthop Res 27:195-201, 2009
56. Tayton E: Femoral anteversion: A necessary angle or an evolutionaryvestige? J Bone Joint Surg Br 89:1283-1288, 2007
57. Espinosa N, Rothenfluh DA, Beck M, et al: Treatment of femoro-acetabular impingement: preliminary results of labral refixation. JBJSAm 88:925-935, 2006
58. Philippon MJ, Stubbs AJ, Schenker ML, et al: Arthroscopic manage-ment of femoroacetabular impingement: Osteoplasty technique andliterature review. Am J Sports Med 35:1571-1580, 2007
59. Wagner R, Barcak EA: Simultaneous proximal femoral rotational anddistal femoral varus osteotomies for femoral retroversion and genuvalgum. Am J Orthop 41:175-178, 2012
60. El-Sobky T: Subtrochanteric valgus osteotomy in developmental coxavara. Indian J Orthop 45:320-323, 2011
61. Eijer H, Berg RP, Haverkamp D, et al: Hip deformity in symptomaticadult Perthes’ disease. Acta Orthop Belg 72:683-692, 2006
62. Eijer H, Podeszwa DA, Ganz R, et al: Evaluation and treatment ofyoung adults with femoro-acetabular impingement secondary toPerthes’ disease. Hip Int 16:273-280, 2006
63. Tanzer M, Noiseux N: Osseous abnormalities and early osteoarthritis:The role of hip impingement. Clin Orthop Relat Res 429:170-177,2004
64. Garrido IM, Moltó FJ, Lluch DB: Distal transfer of the greater trochan-ter in acquired coxa vara. Clinical and radiographic results. J PediatrOrthop B 12:38-43, 2003
65. Dezateux C, Rosendahl K: Developmental dysplasia of the hip. Lancet369:1541-1552, 2007
66. Wiberg G: The anatomy and roentgenographic appearance of a nor-mal hip joint. Acta Chir Scand 83:7-38, 1939
67. Mavcic B, Iglic A, Kralj-Iglic V, et al: Cumulative hip contact stresspredicts osteoarthritis in DDH. Clin Orthop Relat Res 466:884-891,2008
68. Russell ME, Shivanna KH, Grosland NM, et al: Cartilage contact pres-sure elevations in dysplastic hips: A chronic overload model. J OrthopSurg Res 1:6, 2006
69. Jäger M, Wild A, Westhoff B, et al: Femoroacetabular impingementcaused by a femoral osseous head-neck bump deformity: Clinical,radiological, and experimental results. J Orthop Sci 9:256-263, 2004
70. Millis MB, Murphy SB: Use of computed tomographic reconstructionin planning osteotomies of the hip. Clin Orthop Relat Res 274:154-159, 1992
71. Jessel RH, Zurakowski D, Zilkens C, et al: Radiographic and patientfactors associated with pre-radiographic osteoarthritis in hip dyspla-sia. J Bone Joint Surg Am 91:1120-1129, 2009
72. Hipp JA, Sugano N, Millis MB, et al: Planning acetabular redirectionosteotomies based on joint contact pressures. Clin Orthop Relat Res364:134-143, 1999
73. Millis MB, Murphy SB, Poss R: Osteotomies about the hip for theprevention and treatment of osteoarthrosis. Instr Course Lect 45:209-226, 1996
74. Murphy SB, Ganz R, Muller ME: The prognosis in untreated dysplasiaof the hip: A study of radiographic factors that predict the outcome.J Bone Joint Surg Am 77:985-989, 1995
75. Clohisy JC, Barrett SE, Gordon JE, et al: Periacetabular osteotomy forthe treatment of severe acetabular dysplasia. J Bone Joint Surg Am87:254-259, 2005
76. Clohisy JC, Nunley RM, Carlisle JC, et al: Incidence and characteris-tics of femoral deformities in the dysplastic hip. Clin Orthop Relat Res467:128-134, 2009
77. Clohisy JC, Schutz AL, St John LS, et al: Periacetabular osteotomy: Asystematic literature review. Clin Orthop Relat Res 467:2041-2052,2009
78. Clohisy JC, St John LC, Nunley RM, et al: Combined periacetabularand femoral osteotomies for severe hip deformities. Clin Orthop RelatRes 467:2221-2227, 2009
79. Cunningham T, Jessel R, Zurakowski D, et al: Delayed gadolinium-
enhanced magnetic resonance imaging of cartilage to predict earlyfailure of Bernese periacetabular osteotomy for hip dysplasia. J BoneJoint Surg Am 88:1540-1548, 2006
80. Garras DN, Crowder TT, Olson SA: Medium-term results of theBernese periacetabular osteotomy in the treatment of symptomaticdevelopmental dysplasia of the hip. J Bone Joint Surg Br 89:721-724,2007
81. Guevara CJ, Pietrobon R, Carothers JT, et al: Comprehensive morpho-logic evaluation of the hip in patients with symptomatic labral tear.Clin Orthop Relat Res 453:277-285, 2006
82. Hsieh PH, Huang KC, Lee PC, et al: Comparison of periacetabularosteotomy and total hip replacement in the same patient: A two- toten-year follow-up study. J Bone Joint Surg Br 91:883-888, 2009
83. Maheshwari R, Madan SS: Pelvic osteotomy techniques and compar-ative effects on biomechanics of the hip: A kinematic study. Orthope-dics 34:941-941, 2011
84. Millis MB, Kain M, Sierra R, et al: Periacetabular osteotomy for ace-tabular dysplasia in patients older than 40 years: A preliminary study.Clin Orthop Relat Res 467:2228-2234, 2009
85. Millis MB, Murphy SB: The Boston experience. Peri-acetabular osteot-omy with simultaneous arthrotomy via direct anterior approach [inGerman]. Orthopade 27:751-758, 1998
86. Murphy S, Deshmukh R: Periacetabular osteotomy: Preoperative ra-diographic predictors of outcome. Clin Orthop Relat Res 405:168-174, 2002
87. Murphy SB, Simon SR, Kijewski PK, et al: Femoral anteversion. J BoneJoint Surg Am 69:1169-1176, 1987
88. Nehme A, Trousdale R, Tannous Z, et al: Developmental dysplasia ofthe hip: Is acetabular retroversion a crucial factor? Orthop TraumatolSurg Res 95:511-519, 2009
89. Peters CL, Erickson JA, Hines JL: Early results of the Bernese periace-tabular osteotomy: The learning curve at an academic medical center.J Bone Joint Surg Am 88:1920-1926, 2006
90. Shindo H, Igarashi H, Taneda H, et al: Rotational acetabular osteot-omy for severe dysplasia of the hip with a false acetabulum. J BoneJoint Surg Br 78:871-877, 1996
91. Suh DH, Lee DH, Jeong WK, et al: Virtual Bernese osteotomy usingthree-dimensional computed tomography in hip dysplasia. Arch Or-thop Trauma Surg 132:447-454, 2012
92. Teratani T, Naito M, Kiyama T, et al: Periacetabular osteotomy inpatients fifty years of age or older. J Bone Joint Surg Am 93:30-39,2011
93. Trumble SJ, Mayo KA, Mast JW: The periacetabular osteotomy. Min-imum 2 year followup in more than 100 hips. Clin Orthop Relat Res363:54-63, 1999
94. Ganz R, Klaue K, Vinh TS, et al: A new periacetabular osteotomy forthe treatment of hip dysplasias. Technique and preliminary results.Clin Orthop Relat Res 232:26-36, 1988
95. Siebenrock KA, Leunig M, Ganz R: Periacetabular osteotomy: TheBernese experience. Instr Course Lect 50:239-245, 2001
96. Matheney T, Kim YJ, Zurakowski D, et al: Intermediate to long-termresults following the Bernese periacetabular osteotomy and predictorsof clinical outcome. J Bone Joint Surg Am 91:2113-2123, 2009
97. Steppacher SD, Tannast M, Ganz R, et al: Mean 20-year followup ofbernese periacetabular osteotomy. Clin Orthop Relat Res 466:1633-1644, 2008
98. Kim KI, Cho YJ, Ramteke AA, et al: Peri-acetabular rotational osteot-omy with concomitant hip arthroscopy for treatment of hip dysplasia.J Bone Joint Surg Br 93:732-737, 2011
99. Akiyama M, Nakashima Y, Fujii M, et al: Femoral anteversion is cor-related with acetabular version and coverage in Asian women withanterior and global deficient subgroups of hip dysplasia: A CT study.Skeletal Radiol, EPub ahead of print, 2012
100. Ateçs Y, Omerõglu H: Varus derotational osteotomy for persistentdysplasia in CDH. J Bone Joint Surg Br 78:853-853, 1996
101. Günther KP, Thielemann F, Hartmann A, et al: Combined hip-dys-plasia and femuroacetabular impingement. Diagnosis and simultane-ous surgical treatment [in German]. Orthopade 37:577-586, 2008
102. Audenaert EA, Peeters I, Vigneron L, et al: Hip morphological char-

272 M.J. Knesek et al
acteristics and range of internal rotation in femoroacetabularimpingement. Am J Sports Med 40:1329-1336, 2012
103. Fabricant PD, Bedi A, De La Torre K, et al: Clinical outcomes afterarthroscopic psoas lengthening: The effect of femoral version. Ar-throscopy 28:965-971, 2012
104. Ganz R, Horowitz K, Leunig M: Algorithm for femoral and periace-tabular osteotomies in complex hip deformities. Clin Orthop Relat Res468:3168-3180, 2010
105. Beatty T: Osteitis pubis in athletes. Curr Sports Med Rep 11:96-98,2012
106. Hiti CJ, Stevens KJ, Jamati MK, et al: Athletic osteitis pubis. SportsMed 41:361-376, 2011
107. Cunningham PM, Brennan D, O’Connell M, et al: Patterns of bone andsoft-tissue injury at the symphysis pubis in soccer players: Observa-tions at MRI. AJR Am J Roentgenol 188:W291-W296, 2007
108. Schilders E, Bismil Q, Robinson P, et al: Adductor-related groin painin competitive athletes. Role of adductor enthesis, magnetic resonanceimaging, and entheseal pubic cleft injections. J Bone Joint Surg Am89:2173-2178, 2007
109. Zajick DC, Zoga AC, Omar IM, et al: Spectrum of MRI findings inclinical athletic pubalgia. Semin Musculoskelet Radiol 12:3-12, 2008
110. Verrall GM, Hamilton IA, Slavotinek JP, et al: Hip joint range ofmotion reduction in sports-related chronic groin injury diagnosed aspubic bone stress injury. J Sci Med Sport 8:77-84, 2005
111. Holt MA, Keene JS, Graf BK, et al: Treatment of osteitis pubis inathletes. Results of corticosteroid injections. Am J Sports Med 23:601-606, 1995
112. Fricker PA, Taunton JE, Ammann W: Osteitis pubis in athletes: Infec-tion, inflammation or injury?. Sports Med 12:266-279, 1991
113. Radic R, Annear P: Use of pubic symphysis curettage for treatment-resistant osteitis pubis in athletes. Am J Sports Med 36:122-128, 2008
114. Mulhall KJ, McKenna J, Walsh A, et al: Osteitis pubis in professionalsoccer players: A report of outcome with symphyseal curettage incases refractory to conservative management. Clin J Sport Med 12:179-181, 2002
115. Paajanen H, Heikkinen J, Hermunen H, et al: Successful treatment ofosteitis pubis by using totally extraperitoneal endoscopic technique.Int J Sports Med 26:303-306, 2005
116. Paajanen H, Hermunen H, Karonen J: Pubic magnetic resonance im-aging findings in surgically and conservatively treated athletes withosteitis pubis compared to asymptomatic athletes during heavy train-ing. Am J Sports Med 36:117-121, 2008
117. Litwin DE, Sneider EB, McEnaney PM, et al: Athletic pubalgia (sportshernia). Clin Sports Med 30:417-434, 2011
118. Nam A, Brody F: Management and therapy for sports hernia. J AmColl Surg 206:154-164, 2008
119. Best R, Niess A, Striegel H: The “sportsman’s hernia” as possible causefor chronic groin pain. Dtsch Z Sportmed 61:33-39, 2010
120. Kachingwe AF, Grech S: Proposed algorithm for the management ofathletes with athletic pubalgia (sports hernia): A case series. J OrthopSports Phys Ther 38:768-781, 2008
121. Larson CM, Pierce BR, Giveans MR: Treatment of athletes with symp-tomatic intra-articular hip pathology and athletic pubalgia/sports her-nia: A case series. Arthroscopy 27:768-775, 2011
122. Hammoud S, Bedi A, Magennis E, et al: High incidence of athleticpubalgia symptoms in professional athletes with symptomatic femo-roacetabular impingement. Arthroscopy, EPub ahead of print, 2012
123. Birmingham PM, Kelly BT, Jacobs R, et al: The effect of dynamicfemoroacetabular impingement on pubic symphysis motion: A cadav-eric study. Am J Sports Med 40:1113-1118, 2012
124. Meyers WC, McKechnie A, Philippon MJ, et al: Experience with“sports hernia” spanning two decades. Ann Surg 248:656-664, 2008
125. Omar IM, Zoga AC, Kavanagh EC, et al: Athletic pubalgia and “sportshernia”: Optimal MR imaging technique and findings. Radiographics28:1415-1438, 2008
126. Farber AJ, Wilckens JH: Sports hernia: Diagnosis and therapeutic
approach. J Am Acad Orthop Surg 15:507-514, 2007127. Ahumada LA, Ashruf S, Espinosa-de-los-Monteros A, et al: Athleticpubalgia: Definition and surgical treatment. Ann Plast Surg 55:393-396, 2005
128. Paajanen H, Syvähuoko I, Airo I: Totally extraperitoneal endoscopic(TEP) treatment of sportsman’s hernia. Surg Laparosc Endosc Percu-tan Tech 14:215-218, 2004
129. Schwarzer AC, Aprill CN, Bogduk N: The sacroiliac joint in chroniclow back pain. Spine 20:31-37, 1995
130. Dietrichs E: Anatomy of the pelvic joints—A review. Scand J Rheu-matol 4-6, 1991
131. Brolinson PG, Kozar AJ, Cibor G: Sacroiliac joint dysfunction in ath-letes. Curr Sports Med Rep 2:47-56, 2003
132. George SZ, Delitto A: Management of the athlete with low back pain.Clin Sports Med 21:105-120, 2002
133. Marymont JV, Lynch MA, Henning CE: Exercise-related stress reac-tion of the sacroiliac joint. An unusual cause of low back pain inathletes. Am J Sports Med 14:320-323, 1986
134. Biedert RM, Warnke K, Meyer S: Symphysis syndrome in athletes:Surgical treatment for chronic lower abdominal, groin, and adductorpain in athletes. Clin J Sport Med 13:278-284, 2003
135. Foley BS, Buschbacher RM: Sacroiliac joint pain: Anatomy, biome-chanics, diagnosis, and treatment. Am J Phys Med Rehabil 85:997-1006, 2006
136. Szadek KM, van der Wurff P, van Tulder MW, et al: Diagnostic valid-ity of criteria for sacroiliac joint pain: A systematic review. J Pain10:354-368, 2009
137. Schick DM, Meeuwisse WH: Injury rates and profiles in female icehockey players. Am J Sports Med 31:47-52, 2003
138. Nicholas SJ, Tyler TF: Adductor muscle strains in sport. Sports Med32:339-344, 2002
139. Akermark C, Johansson C: Tenotomy of the adductor longus tendonin the treatment of chronic groin pain in athletes. Am J Sports Med20:640-643, 1992
140. Schilders E, Talbot JC, Robinson P, et al: Adductor-related groin painin recreational athletes. J Bone Joint Surg Am 91:2455-2460, 2009
141. Lynch SA, Renström PA: Groin injuries in sport: Treatment strategies.Sports Med 28:137-144, 1999
142. Ekstrand J, Gillquist J: The avoidability of soccer injuries. Int J SportsMed 4:124-128, 1983
143. Tyler TF, Nicholas SJ, Campbell RJ, et al: The association of hip strengthand flexibility with the incidence of adductor muscle strains in profes-sional ice hockey players. Am J Sports Med 29:124-128, 2001
144. Ibrahim A, Murrell GA, Knapman P: Adductor strain and hip range ofmovement in male professional soccer players. J Orthop Surg (HongKong) 15:46-49, 2007
145. Feeley BT, Powell JW, Muller MS, et al: Hip injuries and labral tears inthe National Football League. Am J Sports Med 36:2187-2195, 2008
146. Levine WN, Bergfeld JA, Tessendorf W, et al: Intramuscular cortico-steroid injection for hamstring injuries. A 13-year experience in thenational Football League. Am J Sports Med 28:297-300, 2000
147. Robertson IJ, Curran C, McCaffrey N, et al: Adductor tenotomy in themanagement of groin pain in athletes. Int J Sports Med 32:45-48,2011
148. Shindle MK, Ranawat AS, Kelly BT: Diagnosis and management oftraumatic and atraumatic hip instability in the athletic patient. ClinSports Med 25:309-326, ix-x, 2006
149. Moorman CT, Warren RF, Hershman EB, et al: Traumatic posteriorhip subluxation in American football. J Bone Joint Surg Am 85:1190-1196, 2003
150. Pallia CS, Scott RE, Chao DJ: Traumatic hip dislocation in athletes.Curr Sports Med Rep 1:338-345, 2002
151. Anderson K, Strickland SM, Warren R: Hip and groin injuries inathletes. Am J Sports Med 29:521-533, 2001
152. Weber M, Ganz R: Recurrent traumatic dislocation of the hip: Reportof a case and review of the literature. J Orthop Trauma 11:382-385,1997
153. Berkes MB, Cross MB, Shindle MK, et al: Traumatic posterior hipinstability and femoroacetabular impingement in athletes. Am J Or-
thop 41:166-171, 2012














![Hip, Hip, Hooray! - goodsamdayton.org1].pdf · right hip within the month, ... Hip, Hip, Hooray! ... to her new hip. H E A LT H TA L K| O RTHOPEDICS 6. Title: SHTK602-Sum06REVfin](https://img.pdfslide.us/doc/110x75/5ab989bf7f8b9ac1058dfdf4/hip-hip-hooray-1pdfright-hip-within-the-month-hip-hip-hooray-.jpg)