Embed Size (px)
Citation preview
1
Approach to the Achy Patient
Andrew J. Gross, MD
Rheumatology Clinic Chief
Associate Clinical Professor
University of California, San Francisco
Clinical Case #1
• 52 year old woman with 5 months of joint pain. Initially she had pain in her hands. Over time, she developed pain in her shoulders, knees and feet. Ibuprofen has been helpful for the pain.
• Review of systems is notable for moderately severe fatigue, and occasional sharp chest pains. She also reports symptoms of Raynaud’s phenomenon.
• Past medical, family and social history are unremarkable.
Clinical Case #1
• General physical examination is unremarkable.
• On musculoskeletal exam, you are uncertain if there are any swollen joints. Many joints are tender, particularly her PIP and MCP joints, her wrists and knees.
What is the diagnosis?
Differential Diagnosis
Inflammatory • Autoimmune
– Lupus/Scleroderma
– Rheumatoid Arthritis
– Spondyloarthritis
• Crystal Disease
• Infectious– Viral
– Chronic bacterial
• Neoplastic
Non-Inflammatory• Osteoarthritis
• Endocrine– Thyroid Disease
– Diabetes
– Calcium metabolism
• Overuse
• Somatic/Fibromyalgia– Hypermobility
2
Approach to Arthritis(clinical clues)
• age
• gender
• family history
• onset of disease (acute/chronic)
• pattern of joint involvement
(& presence of enthesitis)
Pattern of Joint Involvement
All of the following conditions commonly involve PIP & MCP joints, wrists and knees EXCEPT:
A. Osteoarthritis
B. Rheumatoid Arthritis
C. SLE
D. CPPD disease (“pseudogout”)
E. Parvovirus B19 induced arthritis
Approach to Arthritis(clinical clues)
• age
• gender
• family history
• onset of disease (acute/chronic)
Lupus/MCTD/scleroderma
Rheumatoid Arthritis
Peri-menopausal osteoarthritis
Psoriatic Arthritis
• pattern of joint involvement
(& presence of enthesitis)• extra-articular manifestations
• diagnostic testing
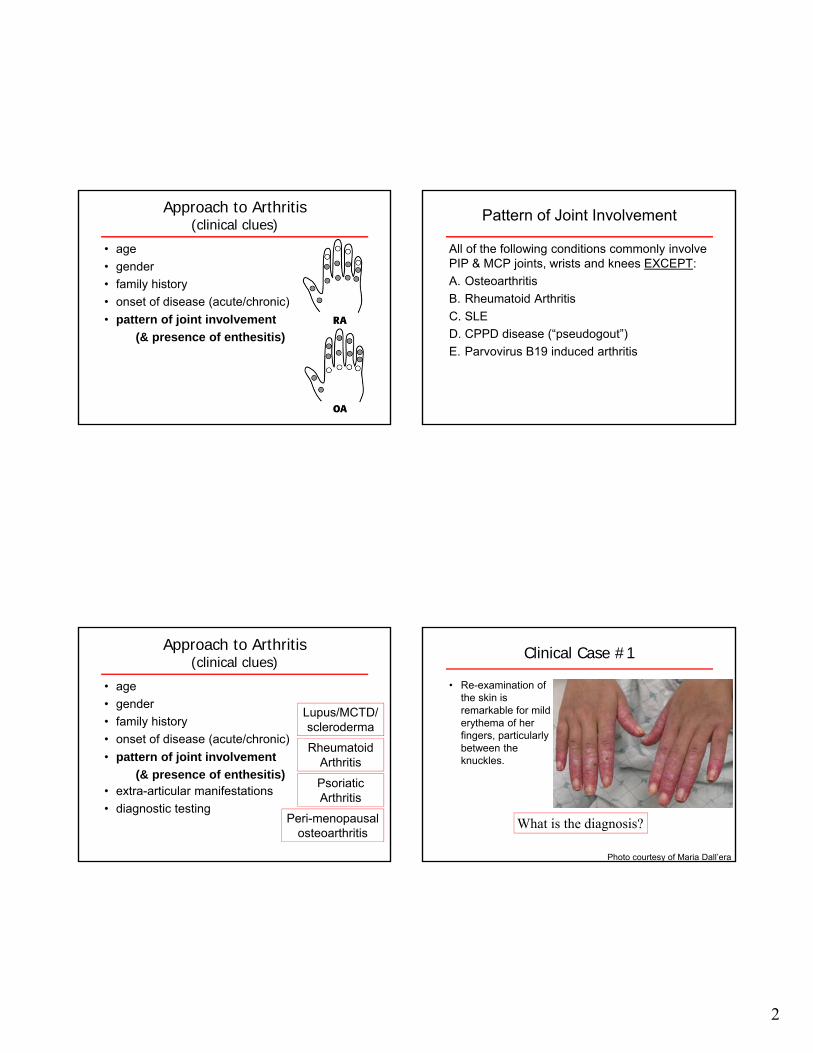
Clinical Case #1
• Re-examination of the skin is remarkable for mild erythema of her fingers, particularly between the knuckles.
What is the diagnosis?
Photo courtesy of Maria Dall’era
3
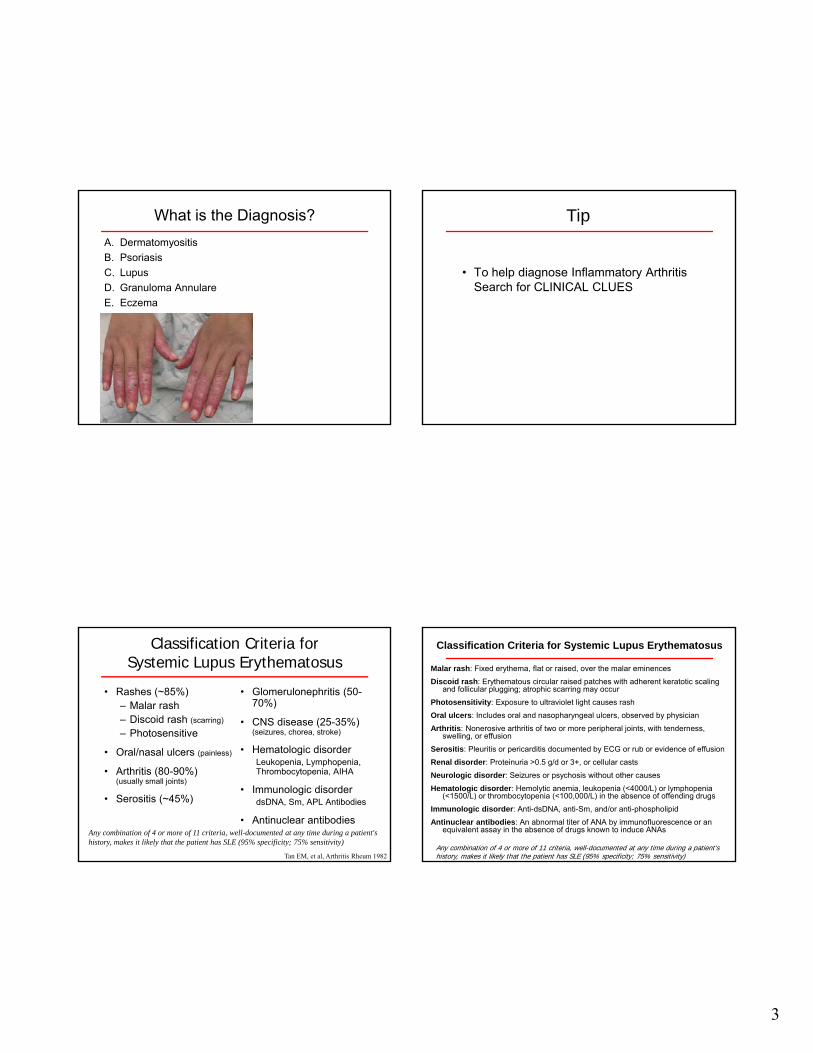
What is the Diagnosis?
A. Dermatomyositis
B. Psoriasis
C. Lupus
D. Granuloma Annulare
E. Eczema
Tip
• To help diagnose Inflammatory Arthritis Search for CLINICAL CLUES
Classification Criteria for Systemic Lupus Erythematosus
• Rashes (~85%)– Malar rash– Discoid rash (scarring)
– Photosensitive
• Oral/nasal ulcers (painless)
• Arthritis (80-90%)(usually small joints)
• Serositis (~45%)
• Glomerulonephritis (50-70%)
• CNS disease (25-35%) (seizures, chorea, stroke)
• Hematologic disorderLeukopenia, Lymphopenia, Thrombocytopenia, AIHA
• Immunologic disorderdsDNA, Sm, APL Antibodies
• Antinuclear antibodiesAny combination of 4 or more of 11 criteria, well-documented at any time during a patient's history, makes it likely that the patient has SLE (95% specificity; 75% sensitivity)
Tan EM, et al, Arthritis Rheum 1982
Classification Criteria for Systemic Lupus Erythematosus
Malar rash: Fixed erythema, flat or raised, over the malar eminences
Discoid rash: Erythematous circular raised patches with adherent keratotic scaling and follicular plugging; atrophic scarring may occur
Photosensitivity: Exposure to ultraviolet light causes rash
Oral ulcers: Includes oral and nasopharyngeal ulcers, observed by physician
Arthritis: Nonerosive arthritis of two or more peripheral joints, with tenderness, swelling, or effusion
Serositis: Pleuritis or pericarditis documented by ECG or rub or evidence of effusion
Renal disorder: Proteinuria >0.5 g/d or 3+, or cellular casts
Neurologic disorder: Seizures or psychosis without other causes
Hematologic disorder: Hemolytic anemia, leukopenia (<4000/L) or lymphopenia (<1500/L) or thrombocytopenia (<100,000/L) in the absence of offending drugs
Immunologic disorder: Anti-dsDNA, anti-Sm, and/or anti-phospholipid
Antinuclear antibodies: An abnormal titer of ANA by immunofluorescence or an equivalent assay in the absence of drugs known to induce ANAs
Any combination of 4 or more of 11 criteria, well-documented at any time during a patient's history, makes it likely that the patient has SLE (95% specificity; 75% sensitivity)
4
Clinical Case #1 – Alternative Scenario
• General physical examination is unremarkable.
• On musculoskeletal exam, you are unsure if there are any swollen joints. Many joints are tender, particularly her PIP and MCP joints, her wrists and knees.
• Skin exam is unremarkable
In the absence of clinical cluesAre there diagnostic tests that will
help identify the diagnosis?
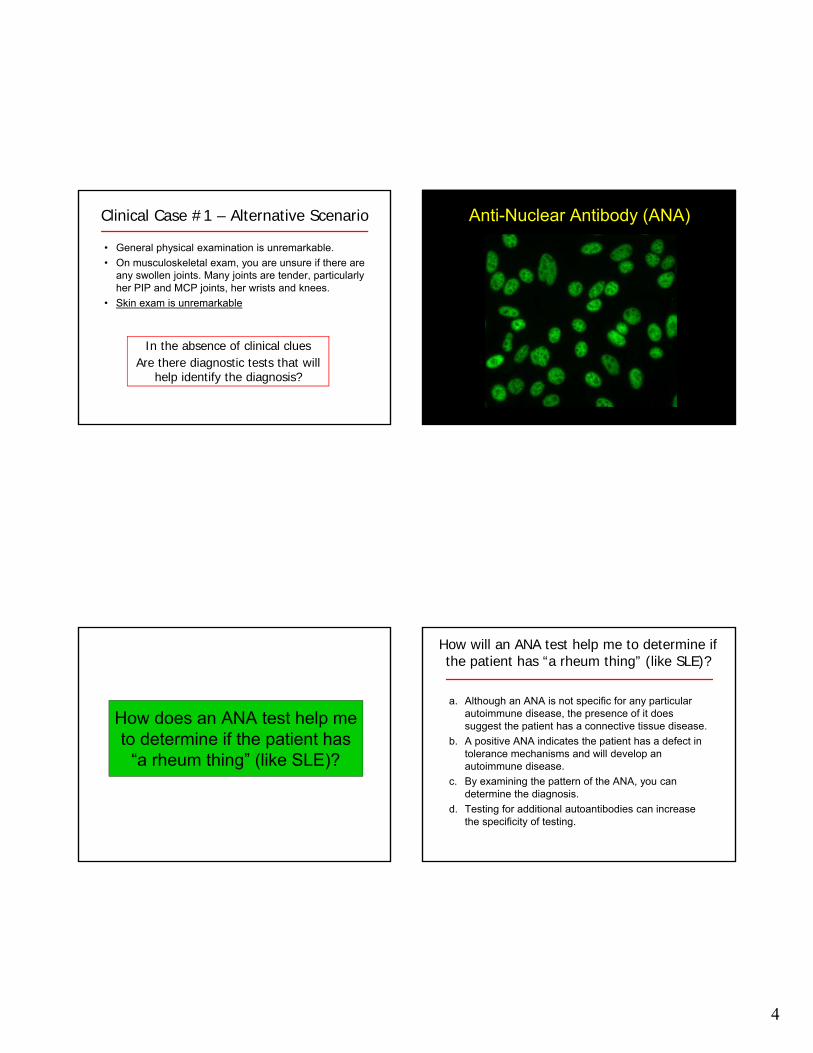
Anti-Nuclear Antibody (ANA)
How does an ANA test help me to determine if the patient has
“a rheum thing” (like SLE)?
How will an ANA test help me to determine if the patient has “a rheum thing” (like SLE)?
a. Although an ANA is not specific for any particular autoimmune disease, the presence of it does suggest the patient has a connective tissue disease.
b. A positive ANA indicates the patient has a defect in tolerance mechanisms and will develop an autoimmune disease.
c. By examining the pattern of the ANA, you can determine the diagnosis.
d. Testing for additional autoantibodies can increase the specificity of testing.
5
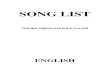
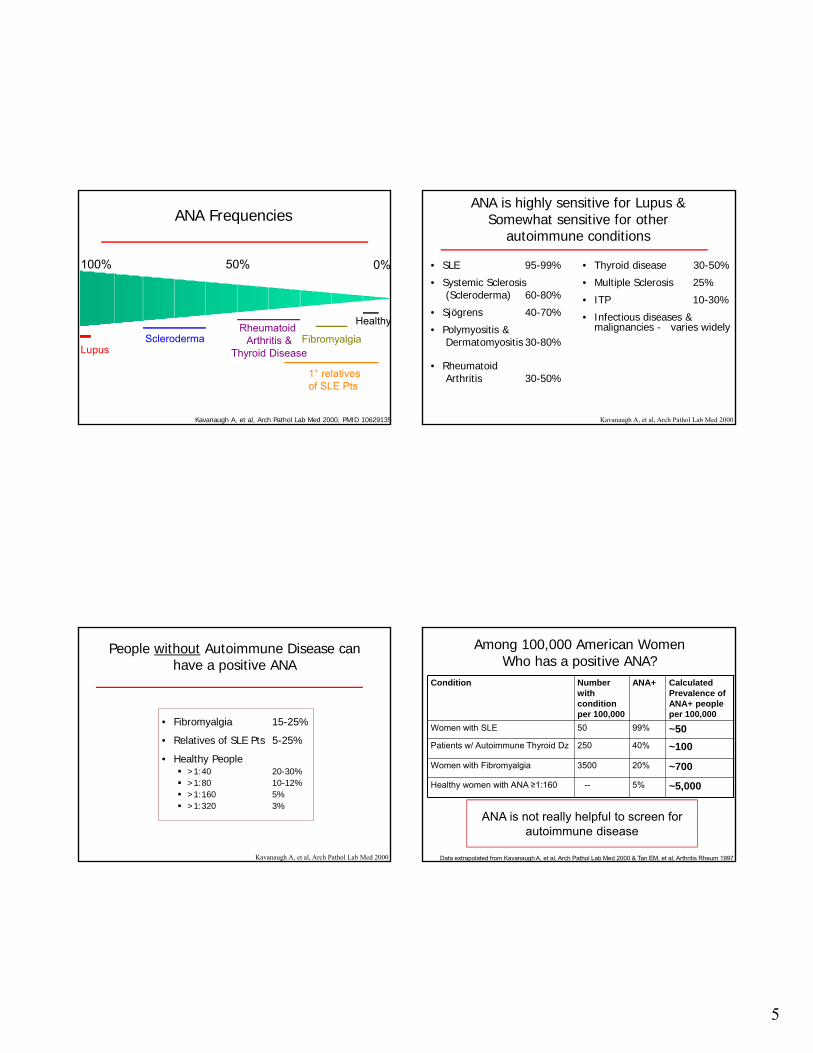
ANA Frequencies
100% 0%
Lupus
Healthy
Scleroderma
1° relativesof SLE Pts
Rheumatoid Arthritis &
Thyroid Disease
50%
Fibromyalgia
Kavanaugh A, et al, Arch Pathol Lab Med 2000, PMID 10629135
ANA is highly sensitive for Lupus &Somewhat sensitive for other
autoimmune conditions
• SLE 95-99%
• Systemic Sclerosis (Scleroderma) 60-80%
• Sjögrens 40-70%
• Polymyositis & Dermatomyositis 30-80%
• RheumatoidArthritis 30-50%
• Thyroid disease 30-50%
• Multiple Sclerosis 25%
• ITP 10-30%
• Infectious diseases & malignancies - varies widely
Kavanaugh A, et al, Arch Pathol Lab Med 2000
People without Autoimmune Disease can have a positive ANA
• Fibromyalgia 15-25%
• Relatives of SLE Pts 5-25%
• Healthy People >1:40 20-30% >1:80 10-12% >1:160 5% >1:320 3%
Kavanaugh A, et al, Arch Pathol Lab Med 2000
Among 100,000 American WomenWho has a positive ANA?
Data extrapolated from Kavanaugh A, et al, Arch Pathol Lab Med 2000 & Tan EM, et al, Arthritis Rheum 1997
Condition Number with condition per 100,000
ANA+ Calculated Prevalence of ANA+ people per 100,000
Women with SLE 50 99% ~50
Patients w/ Autoimmune Thyroid Dz 250 40% ~100
Women with Fibromyalgia 3500 20% ~700
Healthy women with ANA ≥1:160 -- 5% ~5,000
ANA is not really helpful to screen for autoimmune disease
6
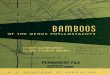
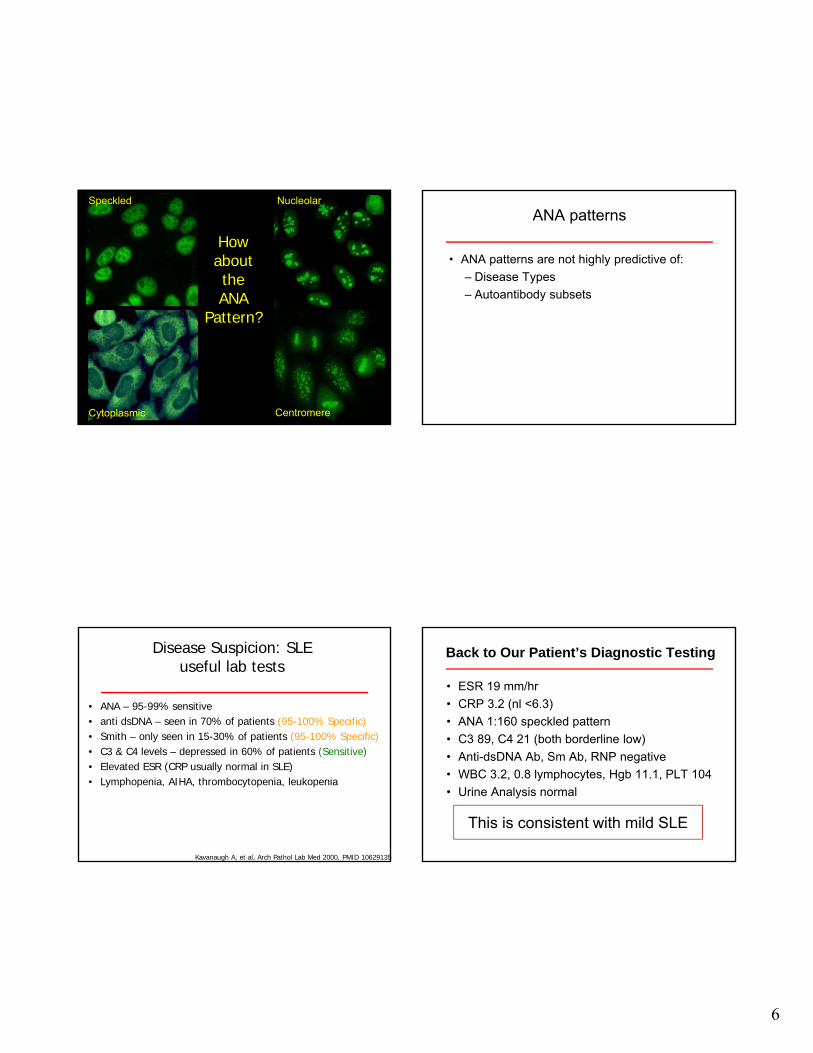
HowabouttheANA
Pattern?
Speckled
Cytoplasmic
Nucleolar
Centromere
ANA patterns
• ANA patterns are not highly predictive of:
– Disease Types
– Autoantibody subsets
Disease Suspicion: SLEuseful lab tests
• ANA – 95-99% sensitive• anti dsDNA – seen in 70% of patients (95-100% Specific)• Smith – only seen in 15-30% of patients (95-100% Specific)• C3 & C4 levels – depressed in 60% of patients (Sensitive)• Elevated ESR (CRP usually normal in SLE)• Lymphopenia, AIHA, thrombocytopenia, leukopenia
Kavanaugh A, et al, Arch Pathol Lab Med 2000, PMID 10629135
Back to Our Patient’s Diagnostic Testing
• ESR 19 mm/hr
• CRP 3.2 (nl <6.3)
• ANA 1:160 speckled pattern
• C3 89, C4 21 (both borderline low)
• Anti-dsDNA Ab, Sm Ab, RNP negative
• WBC 3.2, 0.8 lymphocytes, Hgb 11.1, PLT 104
• Urine Analysis normal
This is consistent with mild SLE
7
Tips to help diagnose SLE
• Search for CLINICAL CLUES!
• Biopsy persistent skin rashes
• Check complement levels
• Check urine for hemoglobin & protein, especially if the patient has dsDNA Ab
• Look for lymphopenia and thrombocytopenia
Clinical Case #2
• 52 year old woman with 5 months of joint pain. Initially she had pain in her hands. Over time, she developed pain in her shoulders, knees and feet. It takes a couple of hours for her joint stiffness to improve in the mornings.
• General physical examination is unremarkable.
• On musculoskeletal exam, you think a few fingers and her right wrist might be swollen. Many joints are tender, particularly her PIP and MCP joints, her wrists and shoulders.
Approach to Arthritis(clinical clues)
• age
• gender
• family history
• onset of disease (acute/chronic)
• pattern of joint involvement
(& presence of enthesitis)
• extra-articular manifestations
• diagnostic testing
Lupus/MCTD/scleroderma
Rheumatoid Arthritis
Peri-menopausal osteoarthritis
Psoriatic Arthritis
Part 2 – Patient’s Diagnostic Testing
• WBC 7.1, Hgb 11.8, PLT 291
• ESR 19 mm/hr
• CRP 7.8 (nl <6.3)
• ANA 1:40 speckled pattern
• C3 128 (normal), C4 36 (slightly elevated)
• Anti-dsDNA Ab, Sm Ab, RNP negative
• Urine Analysis normal
Does not seem like Lupus or Scleroderma.Could this be Rheumatoid Arthritis?
8
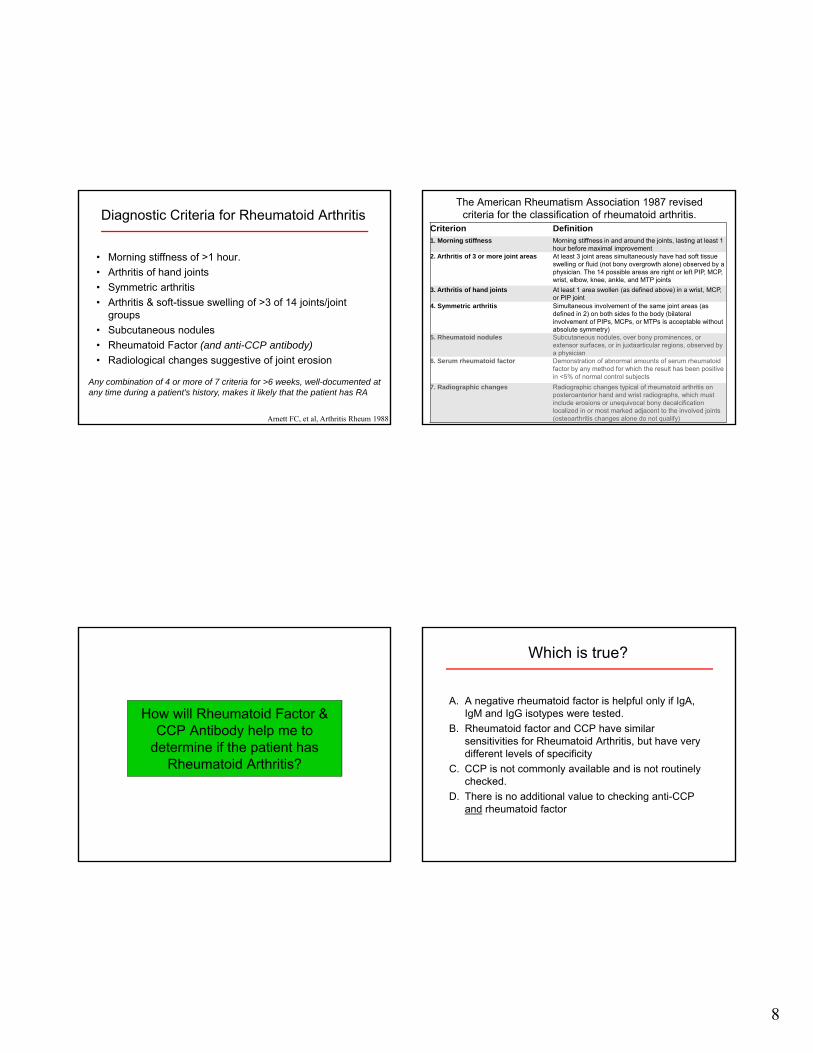
Diagnostic Criteria for Rheumatoid Arthritis
• Morning stiffness of >1 hour.
• Arthritis of hand joints
• Symmetric arthritis
• Arthritis & soft-tissue swelling of >3 of 14 joints/joint groups
• Subcutaneous nodules
• Rheumatoid Factor (and anti-CCP antibody)
• Radiological changes suggestive of joint erosion
Any combination of 4 or more of 7 criteria for >6 weeks, well-documented at any time during a patient's history, makes it likely that the patient has RA
Arnett FC, et al, Arthritis Rheum 1988
The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis.
Criterion Definition1. Morning stiffness Morning stiffness in and around the joints, lasting at least 1
hour before maximal improvement2. Arthritis of 3 or more joint areas At least 3 joint areas simultaneously have had soft tissue
swelling or fluid (not bony overgrowth alone) observed by a physician. The 14 possible areas are right or left PIP, MCP, wrist, elbow, knee, ankle, and MTP joints
3. Arthritis of hand joints At least 1 area swollen (as defined above) in a wrist, MCP, or PIP joint
4. Symmetric arthritis Simultaneous involvement of the same joint areas (as defined in 2) on both sides fo the body (bilateral involvement of PIPs, MCPs, or MTPs is acceptable without absolute symmetry)
5. Rheumatoid nodules Subcutaneous nodules, over bony prominences, or extensor surfaces, or in juxtaarticular regions, observed by a physician
6. Serum rheumatoid factor Demonstration of abnormal amounts of serum rheumatoid factor by any method for which the result has been positive in <5% of normal control subjects
7. Radiographic changes Radiographic changes typical of rheumatoid arthritis on posteroanterior hand and wrist radiographs, which must include erosions or unequivocal bony decalcification localized in or most marked adjacent to the involved joints (osteoarthritis changes alone do not qualify)
How will Rheumatoid Factor & CCP Antibody help me to
determine if the patient has Rheumatoid Arthritis?
Which is true?
A. A negative rheumatoid factor is helpful only if IgA, IgM and IgG isotypes were tested.
B. Rheumatoid factor and CCP have similar sensitivities for Rheumatoid Arthritis, but have very different levels of specificity
C. CCP is not commonly available and is not routinely checked.
D. There is no additional value to checking anti-CCP and rheumatoid factor
9
Rheumatoid Factor
• False Positives– 15% of normal persons over the age of 65
– Infections: Hepatitis C, Parvovirus, HIV, SBE
– Neoplastic disease (especially hematogenous)
– Autoimmune Disease: Sjogren’s, cryoglobulinemia,…
– Chronic Inflammation
• IgM directed against the Fc portion of IgG
• Present in ~70% of patients with RA
• Higher titers associated with more erosive disease
anti-CCP antibodies(anti-Cyclic Citrullinated Peptide antibodies)
• Sensitive (~70%)
• Specific (92%-99%) for diagnosis of RA
• Early marker for RA
Nishimura K, et al Ann Intern Med. 2007;146:797-808
Lab tests can help evaluate for RA
• RF & CCP combined:
• Sensitivity ~80%
• Specificity (depends on which one is positive)
Lee DM, Schur P, Ann Rheum Dis. 2003
RF and CCP are helpful to evaluate patients with joint pain for RA
Tests are limited by their sensitivityRF is limited by its non-specificity
TIP:
Recognize the value of the plain x-ray
• Erosions indicate inflammatory arthritis– Rheumatoid Arthritis
– Spondyloarthritis
– Crystal Arthritis
– Septic Arthritis (Tb)
10
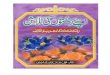
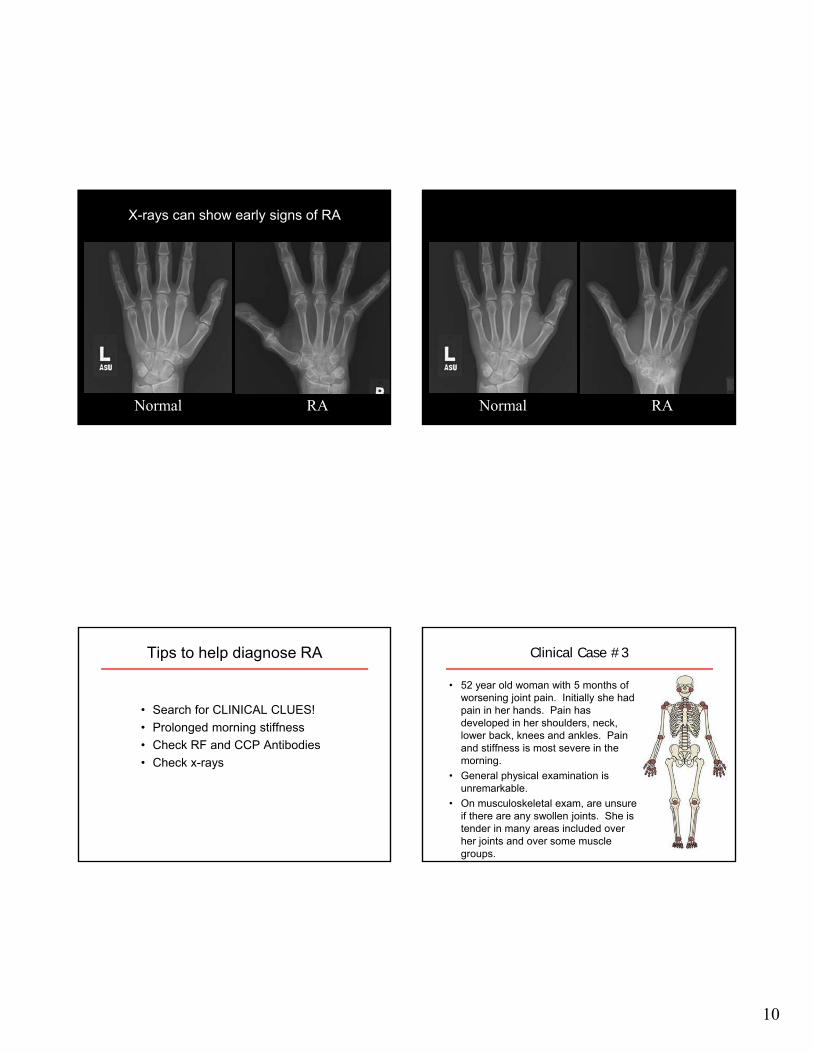
RANormal
X-rays can show early signs of RA
RANormal
Tips to help diagnose RA
• Search for CLINICAL CLUES!
• Prolonged morning stiffness
• Check RF and CCP Antibodies
• Check x-rays
Clinical Case #3
• 52 year old woman with 5 months of worsening joint pain. Initially she had pain in her hands. Pain has developed in her shoulders, neck, lower back, knees and ankles. Pain and stiffness is most severe in the morning.
• General physical examination is unremarkable.
• On musculoskeletal exam, are unsure if there are any swollen joints. She is tender in many areas included over her joints and over some muscle groups.
11
Approach to Arthritis(clinical clues)
• age
• gender
• family history
• onset of disease (acute/chronic)
• pattern of joint involvement
(& presence of enthesitis)
• extra-articular manifestations
• diagnostic testing
Ankylosing Spondylitis
Regional Pain syndromes
Osteoarthritis
Fibromyalgia
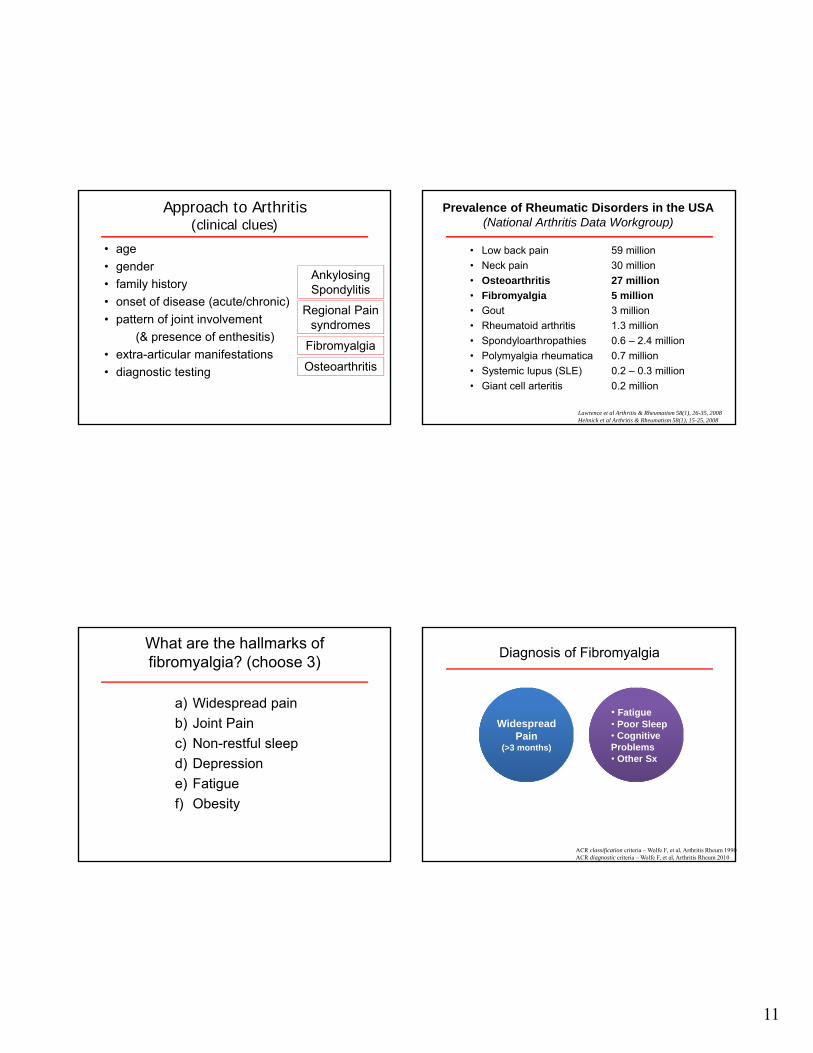
Prevalence of Rheumatic Disorders in the USA(National Arthritis Data Workgroup)
• Gout 3 million
• Rheumatoid arthritis 1.3 million
• Spondyloarthropathies 0.6 – 2.4 million
• Polymyalgia rheumatica 0.7 million
• Systemic lupus (SLE) 0.2 – 0.3 million
• Giant cell arteritis 0.2 million
Lawrence et al Arthritis & Rheumatism 58(1), 26-35, 2008Helmick et al Arthritis & Rheumatism 58(1), 15-25, 2008
• Low back pain 59 million
• Neck pain 30 million
• Osteoarthritis 27 million
• Fibromyalgia 5 million
What are the hallmarks of fibromyalgia? (choose 3)
a) Widespread pain
b) Joint Pain
c) Non-restful sleep
d) Depression
e) Fatigue
f) Obesity
Diagnosis of Fibromyalgia
ACR classification criteria – Wolfe F, et al, Arthritis Rheum 1990ACR diagnostic criteria – Wolfe F, et al, Arthritis Rheum 2010
Widespread Pain
(>3 months)
• Fatigue• Poor Sleep• Cognitive Problems• Other Sx
12
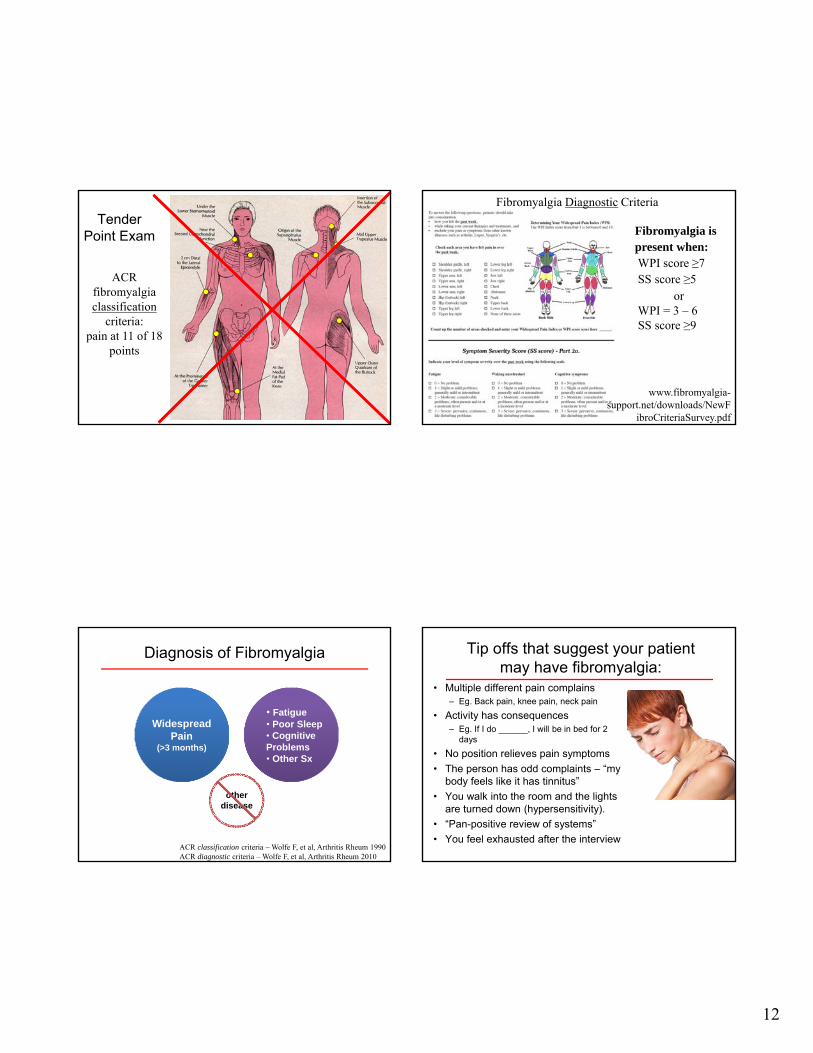
Tender Point Exam
ACR fibromyalgia classification
criteria:pain at 11 of 18
points
www.fibromyalgia-support.net/downloads/NewF
ibroCriteriaSurvey.pdf
Fibromyalgia is present when:WPI score ≥7SS score ≥5
Fibromyalgia Diagnostic Criteria
orWPI = 3 – 6SS score ≥9
Diagnosis of Fibromyalgia
ACR classification criteria – Wolfe F, et al, Arthritis Rheum 1990ACR diagnostic criteria – Wolfe F, et al, Arthritis Rheum 2010
Widespread Pain
(>3 months)
• Fatigue• Poor Sleep• Cognitive Problems• Other Sx
other disease
Tip offs that suggest your patient may have fibromyalgia:
• Multiple different pain complains– Eg. Back pain, knee pain, neck pain
• Activity has consequences– Eg. If I do ______, I will be in bed for 2
days
• No position relieves pain symptoms
• The person has odd complaints – “my body feels like it has tinnitus”
• You walk into the room and the lights are turned down (hypersensitivity).
• “Pan-positive review of systems”
• You feel exhausted after the interview
13
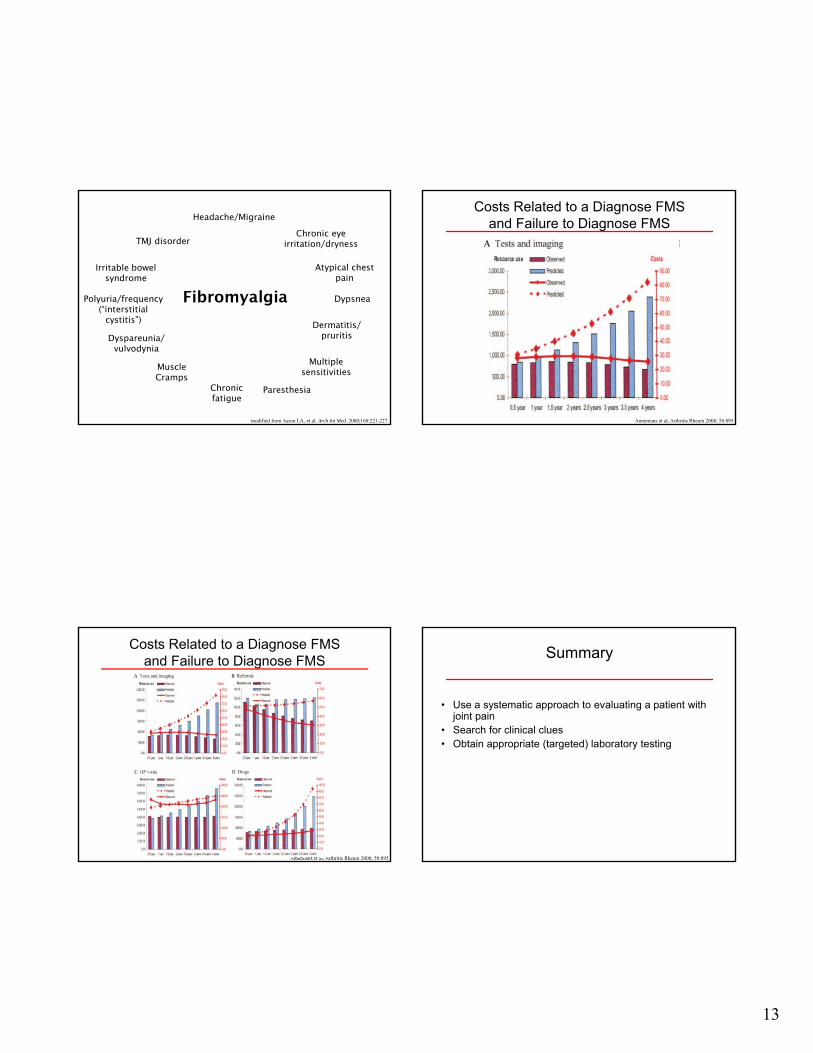
Fibromyalgia
Headache/Migraine
TMJ disorder
Dermatitis/ pruritis
Chronic eye irritation/dryness
Atypical chest pain
Irritable bowel syndrome
Polyuria/frequency(“interstitial
cystitis”)
Dyspareunia/ vulvodynia
ParesthesiaChronic fatigue
Muscle Cramps
Dypsnea
Multiple sensitivities
modified from Aaron LA, et al. Arch Int Med. 2000;160:221-227.
Costs Related to a Diagnose FMS and Failure to Diagnose FMS
Annemans et al, Arthritis Rheum 2008; 58:895
Annemans et al, Arthritis Rheum 2008; 58:895
Costs Related to a Diagnose FMS and Failure to Diagnose FMS Summary
• Use a systematic approach to evaluating a patient with joint pain
• Search for clinical clues• Obtain appropriate (targeted) laboratory testing