Embed Size (px)
DESCRIPTION
Hipoglucemia del UpToDate
Citation preview

Approach to hypoglycemia in infants and children Authors Agneta Sunehag, MD, PhD Morey W Haymond, MD Section Editor Joseph I Wolfsdorf, MB, BCh Deputy Editor Alison G Hoppin, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Jul 2015. | This topic last updated: Sep 11, 2013.
INTRODUCTION — In healthy individuals, maintenance of a normal plasma glucose concentration
depends upon:
●A normal endocrine system for integrating and modulating substrate mobilization,
interconversion, and utilization
●Functionally intact enzymes for glycogenolysis, glycogen synthesis, glycolysis,
gluconeogenesis, and utilization of other metabolic fuels for oxidation and storage
●An adequate supply of endogenous fat, glycogen, and potential gluconeogenic substrates
(eg, amino acids, glycerol, and lactate)
Adults are capable of maintaining a near-normal blood glucose concentration, even when totally
deprived of calories for weeks or, in the case of obese subjects, months [1]. In contrast, healthy
neonates and young children are unable to maintain normal plasma glucose concentrations after
even a short fast (24 to 36 hours) and exhibit a progressive decline in plasma glucose concentration
to hypoglycemic values [2,3].
Abnormalities in hormone secretion, substrate interconversion, and mobilization of metabolic fuels
contribute to abnormalities in glucose production and utilization that ultimately result in
hypoglycemia in children. The appropriate evaluation and treatment of the child with hypoglycemia
require an understanding of the factors that regulate glucose metabolism and the unique aspects of
glucose metabolism in infants and young children.
Glucose homeostasis and the diagnostic approach to hypoglycemia in infants and children will be
discussed here. The causes of hypoglycemia and hypoglycemia in neonates are discussed
separately. (See "Etiology of hypoglycemia in infants and children" and"Pathogenesis, screening,
and diagnosis of neonatal hypoglycemia".)
GLUCOSE HOMEOSTASIS IN NORMAL INFANTS AND CHILDREN — Throughout gestation,
maternal glucose is transported across the placenta to meet a substantial proportion of the energy
needs of the fetus. In animals, the activity of one or more important rate-limiting enzymes of
gluconeogenesis (pyruvate carboxylase, phosphoenol-pyruvate carboxykinase, glucose-6-
phosphatase, and fructose 1,6 diphosphatase) is absent or very low in the fetus, does not increase
until the perinatal period, and reaches adult levels only after several hours to days of extrauterine
life [4]. In keeping with these findings, there is no evidence of fetal glucose production at birth in
humans [5]. However, hepatic glucose production and gluconeogenesis are well established within
hours of birth, even in very premature infants [6]. The enzymes necessary for glycogen synthesis
and glycogenolysis are present in the fetal liver long before the accumulation of glycogen can be
demonstrated. It is only during the last three to four weeks of gestation in humans that hepatic

glycogen stores increase to reach values at birth seen only in children with glycogen storage
diseases [4].
The interruption of placental blood flow as a result of the clamping of the umbilical cord at birth
requires the infant to utilize his or her own endogenous substrates and challenges the newborn with
his or her first fast. With the clamping of the cord, there is an immediate release of glucagon [7].
However, despite the glucagon surge, plasma glucose decreases over the first two hours of life.
This is accompanied by a decrease in insulin and an increase in free fatty acids (FFAs) and ketone
bodies [8]. By four to six hours of life, in most infants, the plasma glucose concentration is stabilized
or is increasing. It is presumed that much of the initial glucose production is from the mobilization of
hepatic glycogen, since hepatic glycogen content decreases during the first several days of
extrauterine life. This release of hepatic glycogen facilitates a smooth transition from the
continuously fed (intrauterine) to the fasted or relatively fasted condition of the first hours to days of
extrauterine life. However, hepatic glycogen content is limited, and within hours of birth
gluconeogenesis must meet an ever-increasing proportion of endogenous glucose production [6,8].
Fatty acid mobilization and metabolism play a crucial role in the maintenance of glucose
homeostasis in infants and children. Plasma FFAs and ketone bodies can be used by a variety of
body tissues and, thus, decrease the demands of these tissues for glucose as an energy source.
The brain is unique in that it uses glucose at a rate 20 times that of other body tissues (per gram)
and cannot use FFAs directly since they are not transported across the blood-brain barrier.
However, ketone bodies (eg, ß-hydroxybutyric acid and acetoacetic acid) are transported across the
blood-brain barrier, and their metabolism by the brain can partially supplant the need for glucose
[1]. The metabolic response to fasting in children is similar to that in adults. However, children have
a more rapid decline in plasma glucose concentration and a more rapid increase in the plasma
concentration of ketone bodies than do adults. These findings suggest the relative increase in the
glucose requirement in children may result in an acceleration of the normal adaptive mechanism(s)
of fasting observed in adults [3].
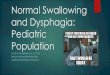
During the first 8 to 10 years of life, the rate of glucose utilization (and production) increases,
followed by a plateau during the next five to seven years, after which the normal adult rate (833 to
944 micromol/min [150 to 170 mg/min]) is achieved (figure 1) [9]. Studies utilizing isotopically-
labeled glucose indicate that, by weight, rates of glucose flux (production and utilization) in adults
are approximately 11 to 13 micromol/kg per min (2 to 2.3 mg/kg per min) in the overnight
postabsorptive state (14-hour fast) and decrease to 9.8micromol/kg per min (1.8 mg/kg per min) by
30 hours of fasting [10]. The rate of glucose flux in infants and children after 4 to 14 hours of fasting
is nearly three times higher (35 micromol/kg per min [6 mg/kg per min]) than that of adults, and
decreases to 23micromol/kg per min (4 mg/kg per min) after a 30- to 40-hour fast [10,11].
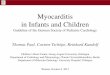
In the premature and term infant, more than 90 percent of the glucose is utilized by the brain. Over
time, this value decreases to approximately 40 percent of glucose turnover in overnight-fasted
adults (figure 2) [9]. The higher rates of glucose turnover per kilogram of body weight in infants and
children when compared with adults are consistent with the relatively higher proportion of brain
mass to body size, which places infants and children at higher risk of hypoglycemia [10,11].
The primary orchestration of substrate mobilization (or storage) and utilization is the result of
classical actions of hormones (eg, insulin, glucagon, catecholamines, cortisol and growth hormone),
although more subtle interactions of other factors (eg, cytokines, neuronal input, ghrelin, leptin,

glucagon-like peptide 1 (GLP1) post-receptor activation mechanism) are now being recognized.
Insulin secretion plays a central role in glucose homeostasis and is affected by a number of factors,
the most important of which is the plasma glucose concentration. A more detailed description of the
secretion and actions of insulin is presented separately. However, we provide a brief description
here. (See "Insulin secretion and pancreatic beta cell function" and "Insulin action".)
When the plasma glucose concentration increases after a meal in normal individuals, glucose is
transported into the pancreatic beta-cell via the GLUT2 transporter, is phosphorylated by
glucokinase, and metabolized via the glycolytic pathway. This results in an increase in
the ATP/ADP ratio, which closes the KATP channels, depolarizes the cell membrane, opening the
Ca++ channels, resulting in fusion of the insulin granule with the plasma membrane causing insulin
secretion. Conversely, a decrease in blood glucose concentration results in decreased glucose
metabolism in the beta-cell, which leads to a reduced ATP/ADP ratio, opening of the KATP channels,
hyperpolarization of the cell membrane, and closure of Ca++ channels, thus blocking Ca++ influx and
reducing insulin secretion. Fundamental problems in these processes can lead to profound
hypoglycemia in children [12]. (See "Pathogenesis, clinical features, and diagnosis of persistent
hyperinsulinemic hypoglycemia of infancy".)
During controlled insulin-induced hypoglycemia, children typically mount a greater counterregulatory
hormone response (eg, with cortisol, epinephrine, and glucagon) than do adults [13,14]. However,
with repeated episodes of hypoglycemia, secretion of counterregulatory hormones wanes, leading
to what is called "hypoglycemic unawareness" in an individual with diabetes. In the absence of
classical symptoms of hypoglycemia, perhaps as a result of this process, the diagnosis of
hypoglycemia can be missed in some children for months.
DEFINITION OF HYPOGLYCEMIA — The overall goal of identifying children with hypoglycemia is
to protect their central nervous systems from irreparable damage as a result of severe,
prolonged and/or repeated episodes of hypoglycemia.
The precise definition of hypoglycemia in infants and children continues to be controversial.
Knowing the conditions preceding the collection of blood for a quantitative glucose determination is
critical to its interpretation. As an example, the normal distribution of glucose values following a
meal, an overnight fast, or a 30- to 40-hour fast, will be strikingly different. Creating different
definitions of hypoglycemia based upon the child's age, gestation and/or weight (small, average, or
large for gestational age), feeding or fasting will not resolve this controversy. There is no a priori
reason that a premature or low-birth-weight infant should tolerate a low glucose concentration better
than an older child; in fact, quite the opposite might be argued.
For diagnostic purposes, we define hypoglycemia as a plasma glucose value of ≤40 mg/dL (2.22
mM) regardless of age. As discussed above, the physiologic nadir of the plasma glucose occurs in
the first two to four hours of life, but normally increases to values >60mg/dL by six hours of life.
Other than this unique circumstance, a documented plasma glucose concentration of
≤40 mg/dL (2.22 mM) should trigger a formal evaluation. However, this concentration should not be
construed as ideal or necessarily safe over time, and should only be used in identifying an
individual at risk for and/or diagnosing hypoglycemia. An elective fast should be considered as a
diagnostic maneuver, under carefully controlled conditions. (See 'Elective fast' below.)

ETIOLOGY OF HYPOGLYCEMIA — The body maintains a delicate balance between the rate at
which glucose is produced or enters the circulation (appearance rate) and the rate at which it is
utilized (disappearance rate). When the rate of appearance of glucose into the plasma exceeds the
rate of disappearance, the plasma glucose concentration increases. Conversely, when the rate of
disappearance is greater than the rate of appearance, the plasma glucose concentration
decreases. In many hypoglycemic conditions, the understanding of glucose kinetics is insufficient to
assign a clear cause (eg, increased utilization or decreased production). In other conditions, a
combination of decreased production and increased utilization is thought to contribute to the
development of hypoglycemia. Specific causes of hypoglycemia in infants and children are
discussed elsewhere. (See "Etiology of hypoglycemia in infants and children".)
CLINICAL FEATURES — In infants, the signs of hypoglycemia are frequently nonspecific, but may
include the signs of severe neuroglycopenia discussed below. The signs of hypoglycemia include
jitteriness, irritability, feeding problems, lethargy, cyanosis, tachypnea, and hypothermia. These
signs are not specific for hypoglycemia and may be early manifestations of a number of other
disorders, including septicemia, congenital heart disease, ventricular hemorrhage, and respiratory
distress syndrome. Infants are at greatest risk for hypoglycemia during the first few days of life.
Neonatal hypoglycemia is discussed separately. (See "Pathogenesis, screening, and diagnosis of
neonatal hypoglycemia".)
In children and adults, the symptoms of hypoglycemia can be divided into two categories: those
caused by the autonomic response to hypoglycemia and those caused by neuroglycopenia [14].
Autonomic response — The early manifestations of hypoglycemia are caused by the autonomic
response to hypoglycemia and include sweating, weakness, tachycardia, tremor, and feelings of
nervousness and/or hunger. These symptoms and signs usually occur at higher blood glucose
concentrations (between 40 and 70 mg/dL [2.2 and 3.9 mM]) than the neuroglycopenic signs and
symptoms, and may function as a "warning system." However, with repeated or prolonged episodes
of hypoglycemia, the threshold for autonomic symptoms decreases to that for neuroglycopenic
symptoms. This can result in the appearance of severe symptoms of hypoglycemia with little or no
warning: "hypoglycemic unawareness." (see 'Glucose homeostasis in normal infants and
children' above).
Neuroglycopenia — Symptoms and signs of neuroglycopenia occur with prolonged hypoglycemia
and at lower plasma concentrations of glucose (approximately 10 to 50 mg/dL [0.5 to 2.8 mM]).
These include lethargy, irritability, confusion, uncharacteristic behavior, hypothermia, and, in
extreme hypoglycemia, seizure and coma. Severe and repeated episodes of hypoglycemia can
result in permanent central nervous system damage, and occasionally, death.
IMMEDIATE MANAGEMENT — The immediate management of the infant or child with
hypoglycemia involves obtaining critical samples and administering parenteral glucose. These steps
are summarized in a rapid overview (table 1).
Critical samples — When the diagnosis of hypoglycemia is suspected and supported by a rapid
indicator of the blood glucose concentration (and β-hydroxybutyrate, if available as a point-of-care
measurement), a 5 to 10 mL sample of blood should be obtained beforetherapeutic intervention.
This sample is used to confirm the diagnosis by an established quantitative laboratory method and
to permit additional biochemical tests, as described below.

Blood — Blood should be drawn in the appropriate tubes according to the requirements of
individual clinical laboratories. However, most of the studies can be performed on blood treated with
heparin or EDTA. Blood samples should be transported on ice to the laboratory. Excess plasma
should be stored at -70ºC until all the ordered results are available.
Blood tests that should be performed immediately include:
●Measurement of key substrates: plasma glucose, free fatty acids (FFAs), ß-hydroxybutyrate,
lactate, total and free carnitine, and acylcarnitines
●Measurement of glucoregulatory hormones: plasma insulin, C-peptide, cortisol, and growth
hormone
Other tests that are helpful include:
●Serum electrolytes (for calculation of the anion gap)
●Liver function tests
●Ammonia
●Toxicology studies (salicylate, ethanol, sulfonylurea)
●Metabolic screening for some disorders.
Urine — In addition to the critical blood sample, the first voided urine should be collected. A sample
should be tested for ketones (if plasma ketones are not available) and reducing substances. The
presence of non-glucose reducing substances in the urine suggests galactosemia or hereditary
fructose intolerance if other reducing substances (eg, streptomycin) are excluded.
(See "Galactosemia: Clinical features and diagnosis" and "Etiology of hypoglycemia in infants and
children".)
The remaining urine should be frozen and saved for toxicology studies, organic acids, dicarboxylic
acids, and/or acylglycines if indicated by subsequent evaluation. (See "Approach to the child with
occult toxic exposure".)
Clinical management
Glucose therapy
Oral therapy — If the patient is conscious and able to drink and swallow safely, a rapidly-absorbed
carbohydrate (eg, glucose tablets, glucose gel, table sugar, fruit juice, or honey) should be given by
mouth. Administer 0.3 grams/kg (10 to 20 grams) of a rapidly absorbed carbohydrate. This can be
supplied by 2 to 3 glucose tablets, a tube of gel with 15 grams, 4 oz (120 mL) sweetened fruit juice,
non-diet soda, or a teaspoon (5 mL) of honey or table sugar. This process may be repeated in 10 to
15 minutes. However, if the hypoglycemia does not improve within 15 to 30 minutes, parenteral
glucose must be seriously considered and is recommended.
Intravenous therapy — Infants and children with altered consciousness and/or who are unable to
safely swallow rapidly absorbed carbohydrate should be treated with intravenous (IV) dextrose.
While placing the intravenous lines, subcutaneous or intramuscularglucagon should be
considered.(See 'Glucagon' below.)
●Initial bolus of dextrose, 0.25 grams/kg of body weight (maximum single dose, 25 grams).
This is usually achieved with 2.5 mL/kg of 10 percent dextrose solution, since extravasation of

higher concentrations of glucose will lead to severe tissue damage. The bolus should be
administered slowly (2 to 3 mL/min), regardless of age. Somewhat lower concentration of
dextrose solution is often used for management of hypoglycemia in neonates.
(See "Pathogenesis, screening, and diagnosis of neonatal hypoglycemia".) The infusion is
given slowly to avoid acute hyperglycemia, which can cause rebound hypoglycemia.
●After the bolus, plasma glucose should be maintained by an infusion of dextrose at 6 to
9 mg/kg per minute. The rate of glucose infusion (mg/kg per minute) can be calculated as
follows:
Rate of infusion (mg/kg per min) = (Percent dextrose in solution x 10 x rate of infusion [mL per
hr]) ÷ (60 x weight [kg])
Higher doses of dextrose (eg, 0.5 to 1.0 g/kg) have been recommended for the initial bolus.
However, our clinical experience in children and infants, and studies in adults, suggest that such
doses are excessive and are likely to cause hyperosmolarity and hyperglycemia which can result in
rebound hyperinsulinemia, and recurrence of hypoglycemia [15,16].
Symptomatic hypoglycemia caused by sulfonylurea overdose is managed with boluses of dextrose
as described above, with close monitoring for recurrent hypoglycemia. If hypoglycemia recurs or
becomes more severe, octreotide should be considered. (See"Sulfonylurea agent poisoning".)
Glucagon — If IV access is not readily available and the patient is unable to safely swallow a
rapidly absorbed carbohydrate, hypoglycemia may be treated with glucagon, given intramuscularly
or subcutaneously (0.03 mg/kg up to a maximum of 1 mg). Glucagon is generally effective for initial
treatment of hypoglycemia caused by hyperinsulinemia (eg, in a patient with diabetes treated with
exogenous insulin). The response is frequently transient. Thus, if the hyperinsulinemia persists,
repeated administration of glucose and/orglucagon may be required. The response to glucagon
also may provide diagnostic information for patients in whom the etiology of hypoglycemia is
unknown. (See 'Glucagon challenge' below.)
Monitoring — During the initial treatment phase, the plasma glucose should be monitored every 30
to 60 minutes and the dextrose infusion adjusted accordingly, until a stable plasma glucose
concentration between 70 and 120 mg/dL (3.9 to 6.7 mmol/L) is attained. Thereafter, plasma
glucose should be monitored every two to four hours. Hyperinsulinemia is highly likely when rates of
glucose infusion greater than 6 to 10 mg/kg per minute are necessary to maintain normal plasma
glucose concentrations. (See "Pathogenesis, clinical features, and diagnosis of persistent
hyperinsulinemic hypoglycemia of infancy".)
DIAGNOSTIC EVALUATION
Overview — Numerous diagnostic procedures are available to clarify the pathogenesis of the
various hypoglycemic disorders, but a systematic approach will yield the most interpretable results.
The results obtained from the history, physical examination, and initial plasma samples should
guide further testing.
History — The history in a hypoglycemic child should include a thorough exploration of the past
medical history (including perinatal history), details of the acute event as well as previous episodes,
and family history [17].

Past medical history — The perinatal history should include the birth weight, gestational age, and
whether the child had hypoglycemic symptoms at birth or in the neonatal period. It is important to
explore the child's past medical history, and to review available medical records, to determine
whether the child had other episodes suggestive of hypoglycemia that may have been missed or
diagnosed as other conditions (eg, seizure disorder, etc).
Age at onset — What was the age at the onset of symptoms? Although there is considerable
overlap, the age of onset suggests diagnostic categories:
●Neonatal period or the first two years of life – Most inborn errors of metabolism (including
causes of hyperinsulinemia) and congenital hormone deficiencies. (See "Pathogenesis,
clinical features, and diagnosis of persistent hyperinsulinemic hypoglycemia of
infancy" and "Overview of inherited disorders of glucose and glycogen metabolism".)
●One year to early childhood – Ketotic hypoglycemia, isolated growth hormone deficiency,
and cortisol deficiency. (See "Etiology of hypoglycemia in infants and children", section on
'Ketotic hypoglycemia' and "Etiology of hypoglycemia in infants and children", section on
'Hormone deficiencies'.)
●Toddlers and young children – Ingestion should always be considered in this age group.
(See "Approach to the child with occult toxic exposure" and "Etiology of hypoglycemia in
infants and children", section on 'Ingestions'.)
Dietary factors — The details of the acute event should include information about the child's
dietary intake before the event. Did acute illness prevent the child from achieving adequate
carbohydrate intake? Was the child in the fed or fasting condition at the time of hypoglycemia? All
of this information can help to narrow the differential diagnosis [18]. (See "Etiology of hypoglycemia
in infants and children".)
●Symptoms after ingestion of milk products or fructose may indicate galactosemia or
hereditary fructose intolerance, respectively.
●Children who have hereditary defects of amino acid or organic acid metabolism may develop
hypoglycemia shortly after the ingestion of protein. (See "Organic acidemias".)
●Was there a history of ingestion, or opportunity for ingestion of alcohol, oral hypoglycemic
agents, aspirin, beta blockers, or quinine (all of which can cause hypoglycemia in children)?
Was there ingestion of foods containing toxins (eg, unripened ackee fruit, a staple in Jamaican
diets)? (see "Approach to the child with occult toxic exposure").
Family history — A family history of Reye syndrome, unexplained infant deaths, or other affected
family members suggests an inborn error of metabolism, particularly a fatty acid oxidation defect
[4,12,13]. Hormonal deficiencies and hyperinsulinism also may run in families [19]. (See "Etiology of
hypoglycemia in infants and children", section on 'Disorders of fatty acid metabolism'.)
Physical examination — The examination may provide important clues to the diagnosis.
●The child's weight and length or height should be measured and plotted on an appropriate
growth chart, and the child's growth trajectory should be evaluated. Short stature may indicate
hypopituitarism or growth hormone deficiency. (See "Causes of short stature".) Disorders of
amino acid, organic acid, and carbohydrate metabolism are usually associated with failure to
thrive, whereas children with fatty acid oxidation disorders typically have normal growth.

Children who are underweight for age may be at risk for ketotic hypoglycemia; poor weight
gain also may be caused by hypopituitarism and ACTH unresponsiveness [20,21].
●Midline facial defects (eg, a single central incisor, optic nerve hypoplasia, cleft lip or palate)
and microphallus or undescended testicles in boys may indicate hypopituitarism and/or growth
hormone deficiency. (See "Diagnosis of growth hormone deficiency in children".)
●Macrosomia, hepatosplenomegaly, and umbilical hernia may indicate Beckwith-Wiedemann
syndrome, whereas hepatomegaly and hypotonia may indicate a glycogen storage disease,
defects in gluconeogenesis, galactosemia, or hereditary fructose intolerance [20].
(See "Overview of inherited disorders of glucose and glycogen metabolism".)
●Hyperventilation may be a clue to metabolic acidosis from an inborn error of metabolism.
(See "Inborn errors of metabolism: Epidemiology, pathogenesis, and clinical
features" and "Inborn errors of metabolism: Metabolic emergencies".)
●Hyperpigmentation may be a clue to adrenal insufficiency. (See "Causes and clinical
manifestations of primary adrenal insufficiency in children".)
Elective fast — For most children with a history of hypoglycemia, a diagnostic fast under carefully
controlled conditions should be considered. Because of the potential risk of provoking an episode of
severe encephalopathy in a child with a defect in fatty acid orcarnitine metabolism, the plasma
carnitine concentration (and plasma concentrations of the acylcarnitines) should be proven to be
normal before initiating an elective fast. (See "Etiology of hypoglycemia in infants and children",
section on 'Disorders of fatty acid metabolism' and "Metabolic myopathies caused by disorders of
lipid and purine metabolism".)
The duration of the fast depends upon the child's age and normal feeding pattern. For infants and
very young children who are normally fed every three to six hours, the fast may consist of omitting
one or more feedings. For an older child, who by history, typically fasts overnight, a 24- to 30-hour
fast should be initiated after the evening meal. Children fasted according to such a protocol are at
risk to develop hypoglycemia between 10:00 AM and 6:00 PM, a time during which they should be
awake and alert, and the availability of the physician and laboratory staff is optimal.
During the fast, plasma concentrations of glucose, ketone bodies, lactate, alanine, and insulin
should be serially monitored and compared with normal standards. Plasma concentrations of
growth hormone and cortisol should be obtained at the time of hypoglycemia (although their
interpretation is not always clear).
Hypoglycemia without (or with only minimal) hepatomegaly and the absence of substantial
ketonuria or ketonemia should focus attention on abnormalities of insulin secretion, or disorders of
ketogenesis or fatty acid oxidation. Hyperinsulinism is best documented by obtaining a number of
plasma samples for simultaneous determination of the glucose and insulin levels at times of
hypoglycemia. The plasma insulin concentration after 24 hours of fasting in normal children,
depending upon the laboratory assay used, is usually <15pmol/L (2 mcU/mL) and rarely greater
than 35 pmol/L (5 mcU/mL), except in markedly obese children. Plasma insulin concentrations
greater than 35 pmol/L (5 mcU/mL) with concomitant blood glucose value less than 2.8 mM
(50 mg/dL), regardless of the period of fasting, are distinctly abnormal and are indications for further
studies to document potential hyperinsulinemia.
If the patient becomes hypoglycemic (plasma glucose <40 mg/dL [2.2 mM]), a glucagon challenge
test should be performed.

Glucagon challenge — In the case of a child with hypoglycemia of unknown cause,
a glucagon challenge test (or glucagon stimulation test) at the time of hypoglycemia can provide
very useful diagnostic information about glycogen stores. Following infusion (or IM injection) of
glucagon (0.03 mg per kg), the glycemic response should be measured at 10, 20, and 30 minutes.
A clear glycemic response (>20 to 30 mg/dL [1 to 2 mmol/L] during the first 10 to 20 minutes) in a
hypoglycemic child suggests inappropriate sequestration of hepatic glycogen caused by
hyperinsulinemia, which may be of endogenous or exogenous origin. Since the beta cell co-
secretes C-peptide in equimolar amounts with insulin, the plasma C-peptide concentrations reflect
endogenous insulin secretion. Therefore, a low C-peptide concentration in a patient with a positive
glycemic response to a glucagon challenge indicates that the source of the insulin is exogenous.
Plasma insulin levels may be either high or low in patients whose hypoglycemia is caused by covert
exogenous administration of insulin [22]. This is because recombinant modified human insulins may
not be detected in the new monoclonal sandwich assays used by many commercial laboratories to
measure specifically unmodified human insulin. Thus, if measured plasma insulin concentrations
are low (and the C-peptide level is also low), polyclonal insulin assays must be sought to detect
exogenous insulin. (See "Etiology of hypoglycemia in infants and children", section on
'Hyperinsulinism'.)
Additional testing — Today a variety of disorders are diagnosed with DNA analyses (eg, defects in
glycogen and free fatty acid [FFA] metabolism, hyperinsulinemia, defects in gluconeogenesis or
glycogenolysis). The clinical presentation and the critical blood samples serve to narrow the
diagnostic possibilities and guide further testing. If such targeted testing does not establish the
diagnosis, then other provocative tests may be considered. As examples, galactose, fructose, and
alanine tolerance tests may be performed in children with suspected defects in gluconeogenesis
(see "Etiology of hypoglycemia in infants and children"), or leucine tolerance tests for suspected
hyperinsulinism-hyperammonemia (HIHA) syndrome (see "Pathogenesis, clinical features, and
diagnosis of persistent hyperinsulinemic hypoglycemia of infancy", section on 'Glutamate
dehydrogenase defects'). However, as a general rule, these tests should be performed only in
selected circumstances and by individuals who are experienced in their performance and
interpretation.
If the diagnosis and appropriate therapy cannot be reasonably determined, the child should be
transferred to a center prepared and experienced to make an even more thorough evaluation of the
child’s or families’ DNA. On occasion, a liver biopsy may be necessary to measure deficiencies of
hepatic enzymes when all else has been exhausted. (See "Inborn errors of metabolism: Identifying
the specific disorder".)
INTERPRETATION OF RESULTS — Whether the critical sample is obtained at the time of initial
presentation or after an elective fast, the results can help in determining the etiology of
hypoglycemia. Assuming that true hypoglycemia occurred, the first step in interpretation is to
determine whether the degree of ketosis is appropriate or inappropriate for the degree of
hypoglycemia. The degree of ketosis can only be determined by measurement of beta-
hydroxybutyrate in the serum.
Inappropriate ketosis — The presence of only mild or moderate ketosis (beta-hydroxybutyrate of
<2.5 mmol/L) at the time of hypoglycemia in a child indicates that FFAs are not being mobilized

appropriately or cannot be used for ketone body formation. These findings suggest hyperinsulinism
or fatty acid oxidation defects, respectively.
Hyperinsulinemia is the primary diagnostic consideration. A robust glycemic response (>20 to
30 mg/dL) to glucagon at the time of hypoglycemia would further strengthen this possibility.
Elevated plasma insulin concentration confirms hyperinsulinemia, but clear and unequivocal
elevation of the plasma insulin concentration is frequently not observed. (See 'Glucagon
challenge' above.)
In fatty acid oxidation defects, the plasma FFA concentrations may be very high (>1800 mM) in the
face of relatively modest ketonemia, and very low or undetectable plasma insulin concentrations.
However, some disorders of FFA oxidation (eg, hydroxyacyl-coenzyme A dehydrogenase, HADH,
previously known as short-chain L-3-hydroxyacly CoA dehydrogenase deficiency, SCHAD) can
cause disturbance of ADP/ATP ratios in the beta cell and have been associated with
hyperinsulinemia [23]. (See "Pathogenesis, clinical features, and diagnosis of persistent
hyperinsulinemic hypoglycemia of infancy".)
Children with glycogen storage disease type I (GSD I, glucose-6-phosphatase deficiency, von
Gierke disease) also have relative hypoketonemia. However, additional clinical features permit
differentiation of these patients from those with hyperinsulinemia or defects of fatty acid oxidation.
Clinical features of glucose-6-phosphatase deficiency include profound hepatomegaly (except in the
newborn), hypertriglyceridemia, and failure to generate a clear glycemic response, but dramatic
lactate response, following glucagon stimulation test. (See "Glucose-6-phosphatase deficiency
(glycogen storage disease I, von Gierke disease)".)
Appropriate ketosis — The presence of ketonemia (beta-hydroxybutyrate >2.5 mmol/L) indicates
that the child is able to mobilize FFAs and use them for ketone body formation. Diagnostic
considerations in these children include a normal fasting response, ketotic hypoglycemia, growth
hormone and/or cortisol deficiency [24], some disorders of fatty acid oxidation, and disorders of
amino and organic acids. The measurement of qualitative urine organic acids and the presence or
absence of hepatomegaly can help to distinguish among these possibilities. (See "Organic
acidemias".)
SUMMARY AND RECOMMENDATIONS — Hypoglycemia in infants and children requires prompt
recognition and treatment to prevent permanent neurologic sequelae.
Symptoms
●Symptoms of hypoglycemia include autonomic (adrenergic) symptoms, and neuroglycopenic
symptoms. The severity of symptoms may or may not predict the severity of the
hypoglycemia. Neuroglycopenic symptoms typically occur at lower blood glucose levels than
autonomic symptoms. However, with repeated episodes of hypoglycemia, the threshold
glucose concentration for adrenergic symptoms decreases, such that they may not appear
before the onset of neuroglycopenic symptoms. (See 'Clinical features'above.)
●Autonomic symptoms of hypoglycemia in infants are nonspecific and include jitteriness,
irritability, feeding problems, lethargy, cyanosis, and tachypnea. Older children may have the
characteristic symptoms due to increased adrenergic activity (sweating, weakness,
tachycardia, tremor, and feelings of nervousness and/or hunger). (See 'Autonomic
response' above.)

●Symptoms of neuroglycopenia include lethargy, irritability, confusion, behavior that is out of
character, hypothermia, and, in extreme hypoglycemia, seizure and coma.
(See 'Neuroglycopenia' above.)
●When hypoglycemia is suspected, a rapid (bedside) blood glucose determination should be
performed. If it is low (≤40 mg/dL [2.2 mmol/L]), critical samples should be obtained and
subsequently treatment should be initiated. Obtaining critical samples before the initiation of
therapy, and collecting the first voided urine sample can dramatically improve the ability to
diagnose the etiology of the hypoglycemia and greatly simplify the subsequent diagnostic
evaluation. (See 'Critical samples' above.)
Treatment — Treatment of hypoglycemia varies with the degree of hypoglycemia and associated
symptoms. The key steps for diagnosis and treatment are summarized in a rapid overview (table 1).
(See 'Immediate management' above.)
●If the patient is fully conscious and able to drink and swallow safely, a rapidly-absorbed
carbohydrate (eg, glucose tablets, glucose gel, table sugar, or fruit juice) should be given by
mouth. If the hypoglycemia does not improve within 10 to 15 minutes, parenteral glucose must
be administered. (See 'Glucose therapy' above.)
●Individuals with altered consciousness and/or who are unable to safely swallow a rapidly-
absorbed carbohydrate should be treated with intravenous (IV) dextrose, at a dose of
0.25 g/kg of body weight. This is usually achieved with 2.5 mL/kg of 10 percent dextrose
solution, given slowly (2 to 3 mL/min). (See 'Glucose therapy' above.)
●Subsequent management – The intravenous bolus described above should be followed by
an infusion of dextrose. Plasma glucose should be monitored every 30 to 60 minutes and the
dextrose infusion adjusted accordingly, until stable plasma glucose concentration between 70
and 120 mg/dL (3.9 to 6.7 mmol/L) is attained. Thereafter, frequency of glucose monitoring
should be decreased according to the patient's clinical and biochemical responses.
(See 'Glucose therapy' above.)
●Sulfonylurea overdose – Symptomatic hypoglycemia caused by sulfonylurea overdose is
managed with boluses of dextrose and sometimes also with octreotide. (See "Sulfonylurea
agent poisoning".)
●Mild symptoms – If the hypoglycemia is mild and the patient is able to tolerate an oral
carbohydrate, oral glucose administration can be attempted. However, if the hypoglycemia
does not improve within 10 to 15 minutes, parenteral glucose must be administered.
Diagnosis
●The diagnostic evaluation depends upon the findings of the history, examination, and
preliminary laboratory results. A controlled elective fast may be necessary, but should be
performed only after disorders of fatty acid oxidation have been excluded. (See'Diagnostic
evaluation' above.)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Cahill GF Jr, Herrera MG, Morgan AP, et al. Hormone-fuel interrelationships during fasting. J Clin Invest 1966; 45:1751.

2. Chaussain JL, Georges P, Calzada L, Job JC. Glycemic response to 24-hour fast in normal children: III. Influence of age. J Pediatr 1977; 91:711.
3. Haymond MW, Karl IE, Clarke WL, et al. Differences in circulating gluconeogenic substrates during short-term fasting in men, women, and children. Metabolism 1982; 31:33.
4. Darmaun D, Haymond MW, Bier DM. Metabolic aspects of fuel homeostasis in the fetus and neonate. In: Endocrinology, 3rd ed, DeGroot LJ, Besser M, Burger HG, et al (Eds), WB Saunders, Philadelphia 1995. p.2258.
5. Kalhan SC, D'Angelo LJ, Savin SM, Adam PA. Glucose production in pregnant women at term gestation. Sources of glucose for human fetus. J Clin Invest 1979; 63:388.
6. Sunehag A, Ewald U, Gustafsson J. Extremely preterm infants (< 28 weeks) are capable of gluconeogenesis from glycerol on their first day of life. Pediatr Res 1996; 40:553.
7. Grajwer LA, Sperling MA, Sack J, Fisher DA. Possible mechanisms and significance of the neonatal surge in glucagon secretion: studies in newborn lambs. Pediatr Res 1977; 11:833.
8. Cornblath M, Schwartz R. Disorders of Carbohydrate Metabolism in Infancy, Blackwell Publications, Cambridge, MA 1991.
9. Haymond MW, Sunehag A. Controlling the sugar bowl. Regulation of glucose homeostasis in children. Endocrinol Metab Clin North Am 1999; 28:663.
10. Haymond MW, Howard C, Ben-Galim E, DeVivo DC. Effects of ketosis on glucose flux in children and adults. Am J Physiol 1983; 245:E373.
11. Bier DM, Leake RD, Haymond MW, et al. Measurement of "true" glucose production rates in infancy and childhood with 6,6-dideuteroglucose. Diabetes 1977; 26:1016.
12. Huopio H, Shyng SL, Otonkoski T, Nichols CG. K(ATP) channels and insulin secretion disorders. Am J Physiol Endocrinol Metab 2002; 283:E207.
13. Amiel SA, Simonson DC, Sherwin RS, et al. Exaggerated epinephrine responses to hypoglycemia in normal and insulin-dependent diabetic children. J Pediatr 1987; 110:832.
14. Cryer PE. Banting Lecture. Hypoglycemia: the limiting factor in the management of IDDM. Diabetes 1994; 43:1378.
15. Collier A, Steedman DJ, Patrick AW, et al. Comparison of intravenous glucagon and dextrose in treatment of severe hypoglycemia in an accident and emergency department. Diabetes Care 1987; 10:712.
16. Wiethop BV, Cryer PE. Alanine and terbutaline in treatment of hypoglycemia in IDDM. Diabetes Care 1993; 16:1131.
17. Haymond MW. Hypoglycemia in infants and children. Endocrinol Metab Clin North Am 1989; 18:211.
18. Verrotti A, Fusilli P, Pallotta R, et al. Hypoglycemia in childhood: a clinical approach. J Pediatr Endocrinol Metab 1998; 11 Suppl 1:147.
19. Stanley CA, Lieu YK, Hsu BY, et al. Hyperinsulinism and hyperammonemia in infants with regulatory mutations of the glutamate dehydrogenase gene. N Engl J Med 1998; 338:1352.
20. Roe TF, Kogut MD. Hypopituitarism and ketotic hypoglycemia. Am J Dis Child 1971; 121:296. 21. Kershnar AK, Roe TF, Kogut MD. Adrenocorticotropic hormone unresponsiveness: report of a girl
with excessive growth and review of 16 reported cases. J Pediatr 1972; 80:610. 22. Green RP, Hollander AS, Thevis M, et al. Detection of surreptitious administration of analog insulin
to an 8-week-old infant. Pediatrics 2010; 125:e1236. 23. Clayton PT, Eaton S, Aynsley-Green A, et al. Hyperinsulinism in short-chain L-3-hydroxyacyl-CoA
dehydrogenase deficiency reveals the importance of beta-oxidation in insulin secretion. J Clin Invest 2001; 108:457.
24. Cornblath M, Pildes RS, Schwartz R. Hypoglycemia in infancy and childhood. J Pediatr 1973; 83:692.
Topic 5805 Version 13.0