Embed Size (px)
Citation preview
APPROACH TO AZOTEMIC PATIENTS
Florencio J. Pine, M.D.

Objective:
Aims to assist the students in learning the following:
Clinical implication of azotemia Gather and analyze the clinical data base for systemtic
and logical assessmemt of azotemic patients Differentiate types and causes of renal failure Differentiate between acute and chronic renal failure Importance of recognizing acute from chronic renal
failure Arrive at the diagnosis using the clinical data base and
judicious utilization of diagnostic tools

Contents
1. Review of the basic renal function, anatomy and physiology
2. Definition and cardinal manifestations of azotemia
3. Diagnostic tools, use and interpretation
4. Types, manifestations and differentiating parameters of renal failure
5. Algorithm
Functions of the Kidney
1. Maintains fluid balance2. Maintains electrolyte balance3. Maintains acid-base balance4. Excretes water/ toxic waste products5. Synthesizes hormones6. Regulates blood pressure7. Contributes in glucose metabolism8. Conserves substrates that can be reused by
the body

The Nephron
The Glomerulus
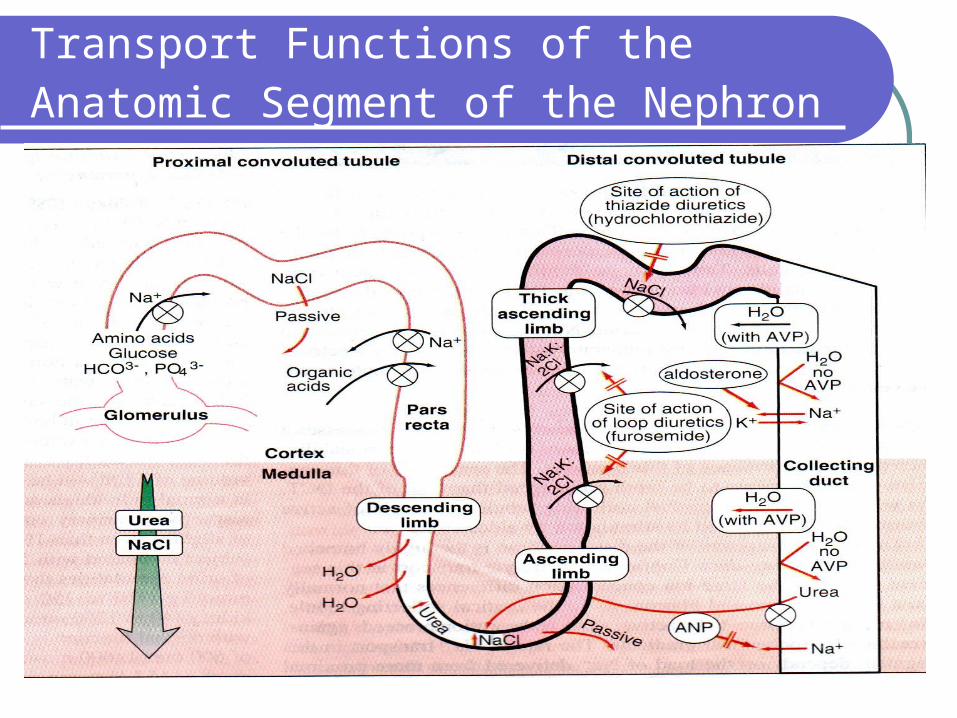
Transport Functions of the Anatomic Segment of the Nephron

Patterns of Adaptation

Azotemia
Definition: Retention of nitrogenous waste products
in the blood
Implication: Renal dysfunction
Phases:Asymptomatic
Uremic state

Cardinal Manifestations: Renal Dysfunction
Oliguria - urine output < 400-500cc/day
Anuria - urine output < 100cc/day
Polyuria - urine output >3L/day with intake of <3L/day
Uremia
Other manifestation- determined by underlying disease

Basic Screening Diagnostic Tools
CBC BUN/Creatinine Urinalysis
Diagnostic Tools: Common Complications
Na, K, Cl ABG Chest Xray ECG
Diagnostic Tools: Causes
1. Uric Acid
2. CPK
3. Urine GS/CS
4. Urine diagnostic indices
5. KUB UTZ
6. Plain KUB Xray
7. CT Stonogram
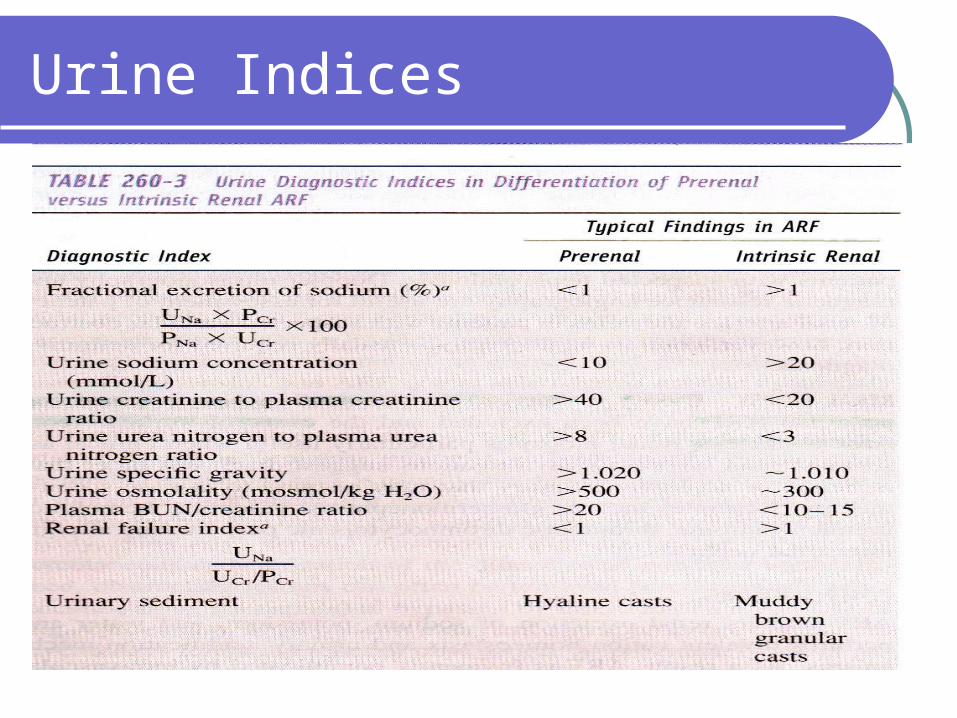
Urine Indices
Estimation of Renal Function
1. BUN
2. Serum Creatinine
3. Creatinine Clearance
4. Estimated Creatinine clearance
Cockroft-Gault Formula:
CrCl (ml/min)=(140-age)(weight) (0.85)if female
(72) (creatinine)
5. Nuclear GFR

Classification
Acute
Functional deterioration within hours to days/ weeks
Potentially reversible damage
Chronic
Functional deterioration w/in weeks to months/years
Irreversible nephron/s injury
Acute renal failure: Classification
Pre- renal: Physiologic disturbance Decreased perfusion Increased waste production
Intrinsic: Definite anatomic damage Glomerulonephritis
Acute tubular necrosis Acute tubulointerstitial nephritis
Acute intratubular obstruction
Post-renal: Obstruction in the drainage Both ureters Urinary bladder outlet
Acute renal failure: Classification
Pre-Renal: Most Common
Intra-Renal: Most Impact Large Vessel Disease Small Vessel/Glomerulus Ischemic/Toxic ATN Acute TIN
Post-renal: Demand Immediate Diagnosis and Treatment
Ischemic/Toxic ATN: >90% of intra-renal
Vulnerability factors: excretes numerous drugs and solutes ability to concentrate solutes hundred fold large surface area high rates of active transport of solutes and
O2 consumption relative hypoperfusion
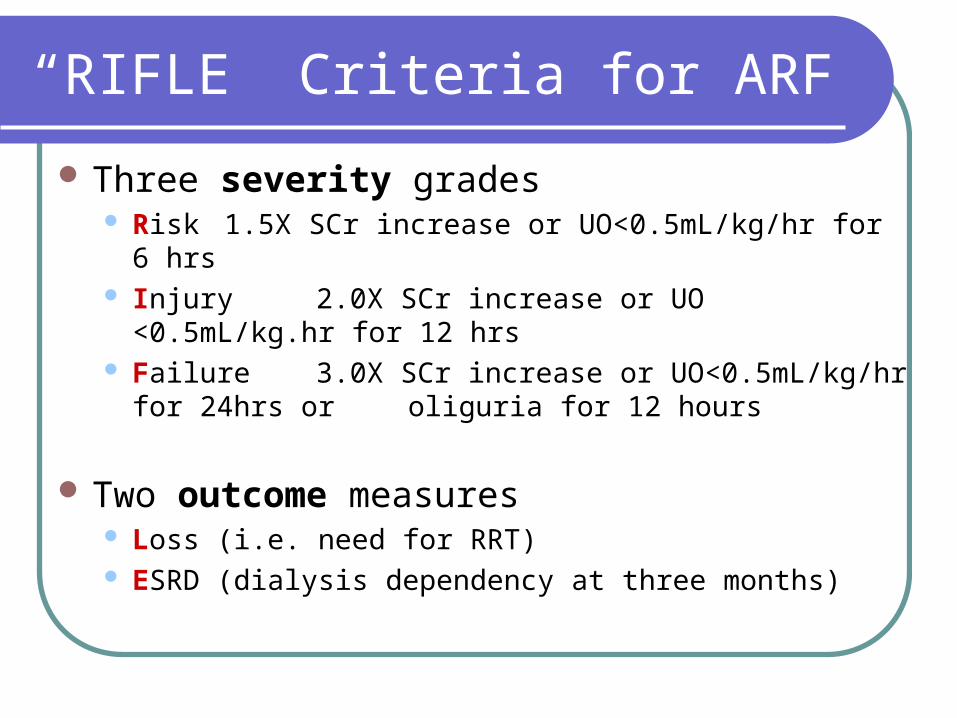
“RIFLE” Criteria for ARF
Three severity grades Risk 1.5X SCr increase or UO<0.5mL/kg/hr for 6 hrs Injury 2.0X SCr increase or UO <0.5mL/kg.hr for 12 hrs Failure 3.0X SCr increase or UO<0.5mL/kg/hr for 24hrs or
oliguria for 12 hours
Two outcome measures Loss (i.e. need for RRT) ESRD (dialysis dependency at three months)

“RIFLE” Criteria for ARF
These gradings were found to have prognostic value
Modified criteria felt to be more useful for patient management
Modified R, I, F categories-changed to stages 1-3 L and E remain as outcomes

Acute Kidney Injury Network (AKIN) Staging
*Stage allocated is highest (worse) of either of the criteria
Stage Creatinine* change over baseline
Oliguria criteria*
1 +27uM or 1.5-2X increase <0.5mL/kg/hr for >6 hrs
2 2-3X increase <0.5mL/kg/hr for >12 hrs
3 >3X increase or <0.3mL/kg/hr for 24 hours or anuria for 12 hours

Laboratory Findings in ARF
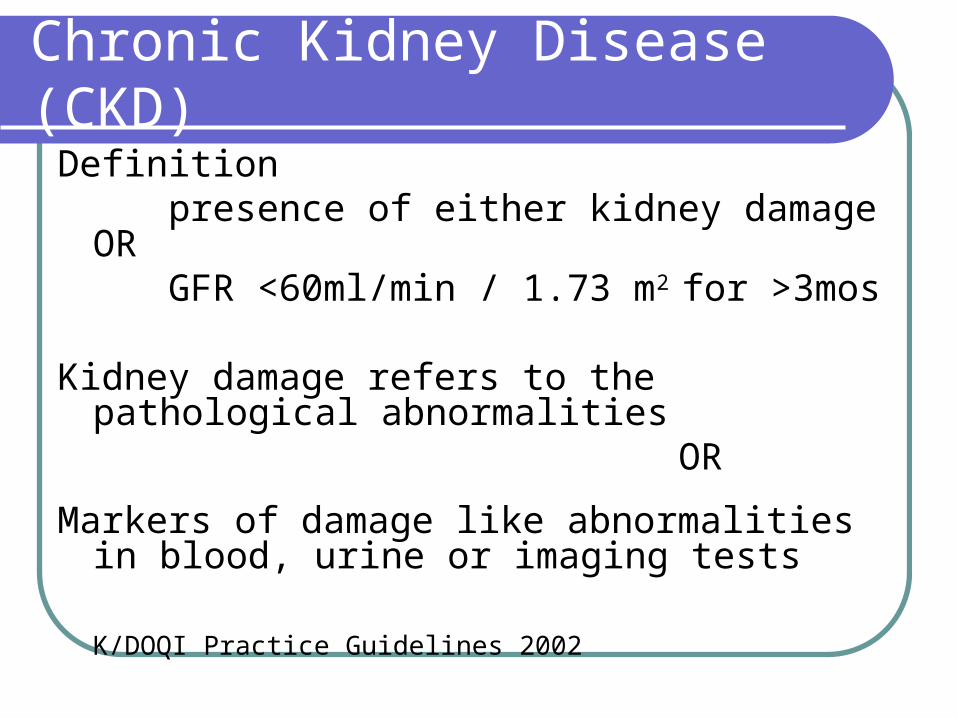
Chronic Kidney Disease (CKD)
Definition presence of either kidney damage OR GFR <60ml/min / 1.73 m2 for >3mos
Kidney damage refers to the pathological abnormalities
OR
Markers of damage like abnormalities in blood, urine or imaging tests
K/DOQI Practice Guidelines 2002
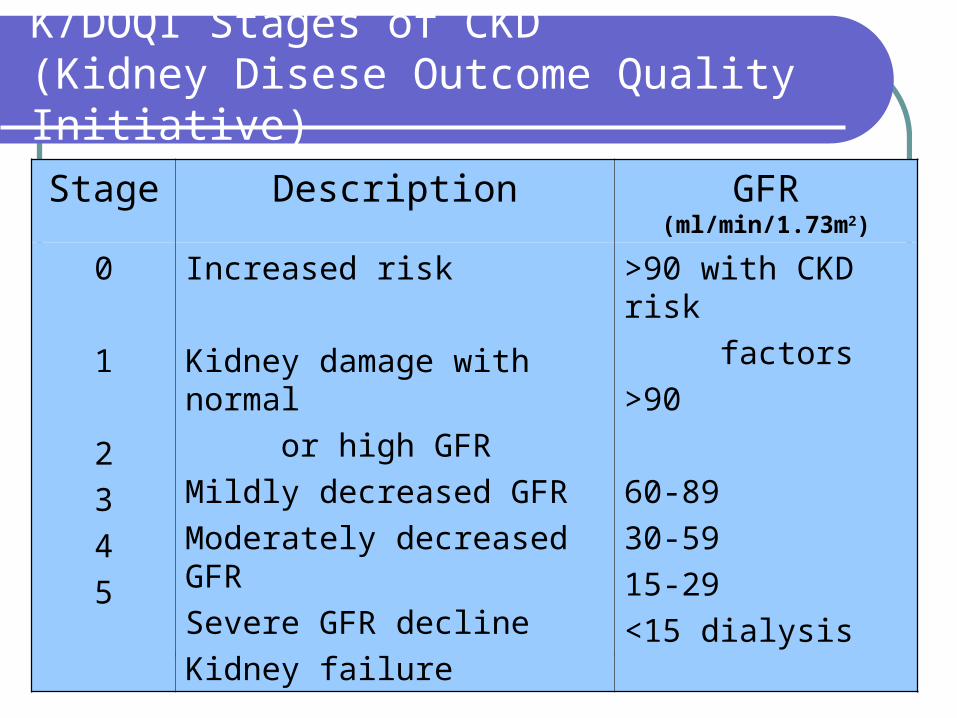
K/DOQI Stages of CKD(Kidney Disese Outcome Quality Initiative)
Stage Description GFR (ml/min/1.73m2)
0
1
2
3
4
5
Increased risk
Kidney damage with normal
or high GFR
Mildly decreased GFR
Moderately decreased GFR
Severe GFR decline
Kidney failure
>90 with CKD risk
factors
>90
60-89
30-59
15-29
<15 dialysis

Causes of CKD- REDCOP Registry
1. Diabetes Mellitus (35%)
2. Chronic Glomerulonephritis (25%)
3. Hypertension (20%)
4. Chronic Pyelonephritis (6%)
5. Autosomal Dominant Polycystic Kidney Disease (2%)
6. Unknown (5%)
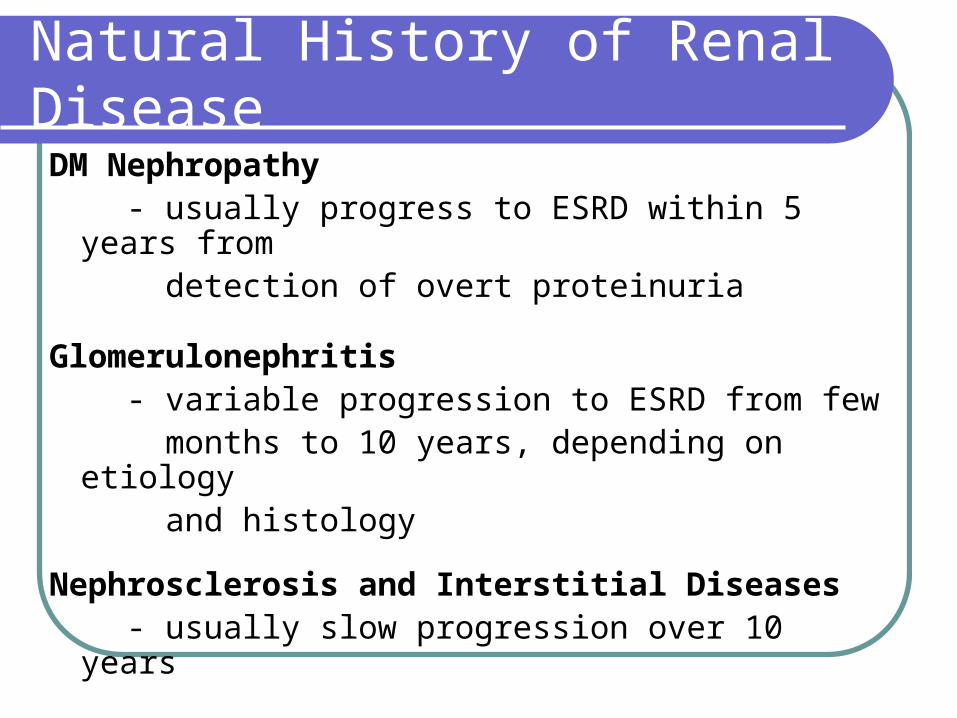
Natural History of Renal Disease
DM Nephropathy - usually progress to ESRD within 5 years from
detection of overt proteinuria
Glomerulonephritis - variable progression to ESRD from few months to 10 years, depending on etiology and histology
Nephrosclerosis and Interstitial Diseases - usually slow progression over 10 years
End Stage Renal Disease (ESRD)
DEFINITION
Residual renal function < 15ml/min Irreversible renal damage

End Stage Renal Disease (ESRD)
CLUES: Permanent Renal Damage
1.History
Uremic features >3mos
Markedly elevated BUN + creatinine without or minimal symptoms
Chronic skin changes of uremia
2. Evidence of renal osteodystrophy
3. Ultrasound changes
-small kidneys
-hyperechoic kidneys with loss of CMJ

End Stage Renal Disease (ESRD)
Philippine Estimate (REDCOP 2004)
- Incidence = 120 million population
- Prevalence= 60 million population
Worldwide Incidence: ↑ by 3.2 -7.6% per year
Clinical Abnormalities in Uremia
Fluid and electrolyte disturbance Endocrine – metabolic disturbances Neuromuscular disturbance Cardiovascular and pulmonary disturbance Dermatologic disturbances Gastrointestinal disturbances Hematologic and immunologic disturbances
Cutaneous Manifestations: Uremia
1. Uremic frost- white dust-like material2. Xerosis3. Changes in skin pigmentation4. Changes in skin appendages Onycodermal bands = crescents
5. Half- and –Half Nails Distal brown + normal or white portion
6. Bullous dermatosis7. Uremic pruritus8. Vascular renocutaneous syndromes - increased capillary fragility

PARAMETER ACUTE CHRONIC
History Previously normal
History of fluid/ blood loss
S/Sx of ineffective
circulating volume
Previously with renal
disease/ chronic
systemic disease
PE
VS
Skin
Appearance
(+) signs of reduced
circulating volume
No change
+ Acutely ill
Hypertension
(+)Pallor
(+)Chronic uremic skin changes
(+)Uremic reath
Chronically ill
Acute vs Chronic Renal Failure

Acute vs Chronic Renal Failure
PARAMETER ACUTE CHRONIC
Laboratory
Hgb/Hct
Ca
Phosphorus
S. Crea
Normal
Usually normal
Often normal
>1mg% per day
Usually low
Usually low
Often elevated
<0.5mg% per day
Ultrasound
Kidney Size
Echogenicity
CMJ
Cortical thickness
Normal to globularly enlarged
Hypoechoic to normal
Normal to blurred
Normal
Normal to small
Hyperechoic, heterogenous
Indisctinct
Thinned out
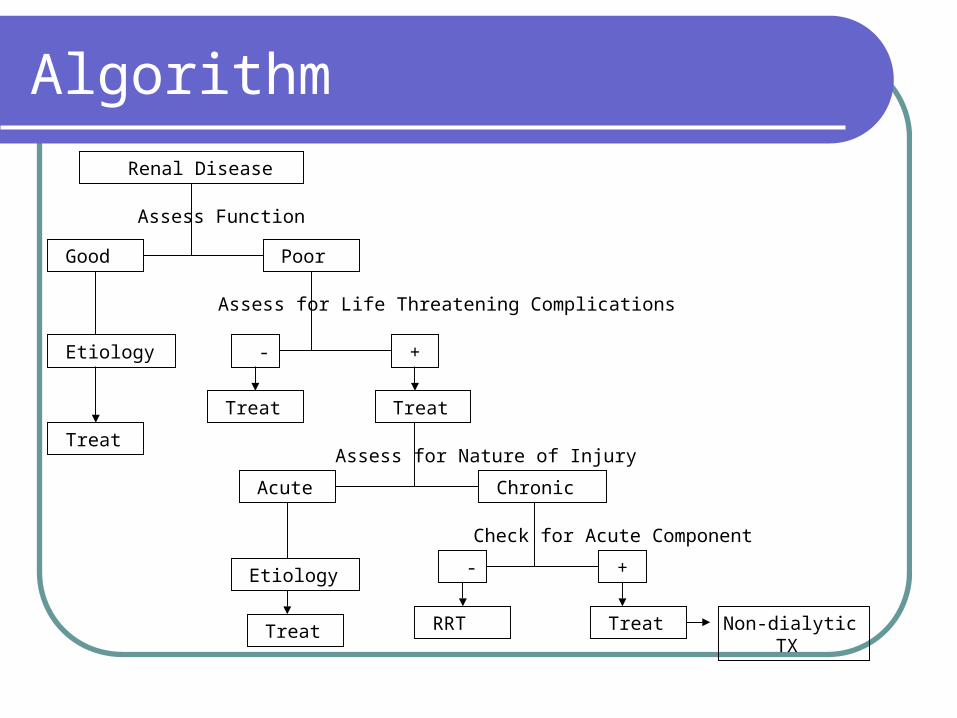
Algorithm
Renal Disease
Good Poor
Non-dialytic TX
Treat
Etiology
-
-
Treat
Treat
Acute Chronic
Treat RRT
+
+Etiology
Assess Function
Assess for Life Threatening Complications
Assess for Nature of Injury
Check for Acute Component
Treat