Embed Size (px)
Citation preview
PEDIATRIC ANNALS 43:4 | APRIL 2014 Healio.com/Pediatrics | 153
FEATURE
Approach to Acute Ataxia in Childhood: Diagnosis and EvaluationLalitha Sivaswamy, MD
Lalitha Sivaswamy, MD, is Associate Profes-
sor of Pediatrics and Neurology, Department
of Neurology, Wayne State University School of
Medicine; and Medical Director, Headache Clinic,
Children’s Hospital of Michigan.
Address correspondence to: Lalitha Sivas-
wamy, MD, Department of Neurology, Wayne
State University School of Medicine, Children’s
Hospital of Michigan, 3901 Beaubien, Detroit, MI
48201; email: [email protected].
Disclosure: The author has no relevant finan-
cial relationships to disclose.
doi: 10.3928/00904481-20140325-13
Abstract
Ataxia refers to motor incoordination that is
usually most prominent during movement
or when a child is attempting to maintain a
sitting posture. The first part of the review
focuses on the anatomic localization of
ataxia — both within the nervous system
and without — using a combination of his-
torical features and physical findings. The
remainder of the review discusses etio-
logical considerations that vary depending
on the age group under consideration. In
infancy, certain specific diseases, such as
opsoclonus myoclonus ataxia syndrome,
must receive special mention because the
underlying disease process may be ame-
nable to surgical intervention. In the tod-
dler- and school-age groups, certain condi-
tions (such as stroke and acute cerebellitis)
require immediate recognition and imag-
ing, whereas others (such as post-infec-
tious ataxia and concussion) require close
follow-up. Finally, mention must be made
of diseases outside of the central nervous
system that can present with ataxia, such
as Guillain-Barré syndrome.
The word ataxia is derived from the Greek word ataktos, which means “lack of order.” Ataxia
is characterized by disturbances in the voluntary coordination of posture and movement. In children, it is most prominent during walking (the sine qua non being a staggering gait with impaired tandem), but it can also be present during sitting or standing, or when the child is performing move-ments of the arms, legs, or eyes.
This review focuses on the etiol-ogy and diagnostic considerations for acute ataxia, which for the purposes of this discussion refers to ataxia with a symptom evolution time of less than 72 hours.1
Motor coordination requires sensory input from muscles and joints. This sen-sory information is transmitted through myelinated axons, via the posterior columns of the spinal cord, to higher centers in the cortex and basal ganglia.
© S
hutte
rsto
ck
154 | Healio.com/Pediatrics PEDIATRIC ANNALS 43:4 | APRIL 2014
FEATURE
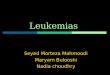
These central structures generate their modulating output, which is conveyed through motor tracts that lay in the brain stem and spinal cord and then conveyed through peripheral nerves to the rel-evant muscle groups, thereby closing the action loop. The cerebellum exerts a modulating control at various lev-els of this loop. Furthermore, the ves-tibular system in the inner ear monitors angular and linear accelerations of the head. This information is also conveyed to the cerebellum, which utilizes this feedback to maintain posture.2 Ataxia can, therefore, arise from disturbances in various parts of the nervous system (eg, the cerebellum, brain stem, spinal cord, and peripheral nerves), as well as the inner ear (Figure 1). To equate ataxia with disease of the cerebellum alone is, therefore, inaccurate. Finally, certain non-neurological conditions,
such as musculoskeletal pathology, can lead to clumsy gait. There are no clear data regarding incidence or gender pre-diction of acute ataxia in the pediatric age group.
CLINICAL EVALUATION History
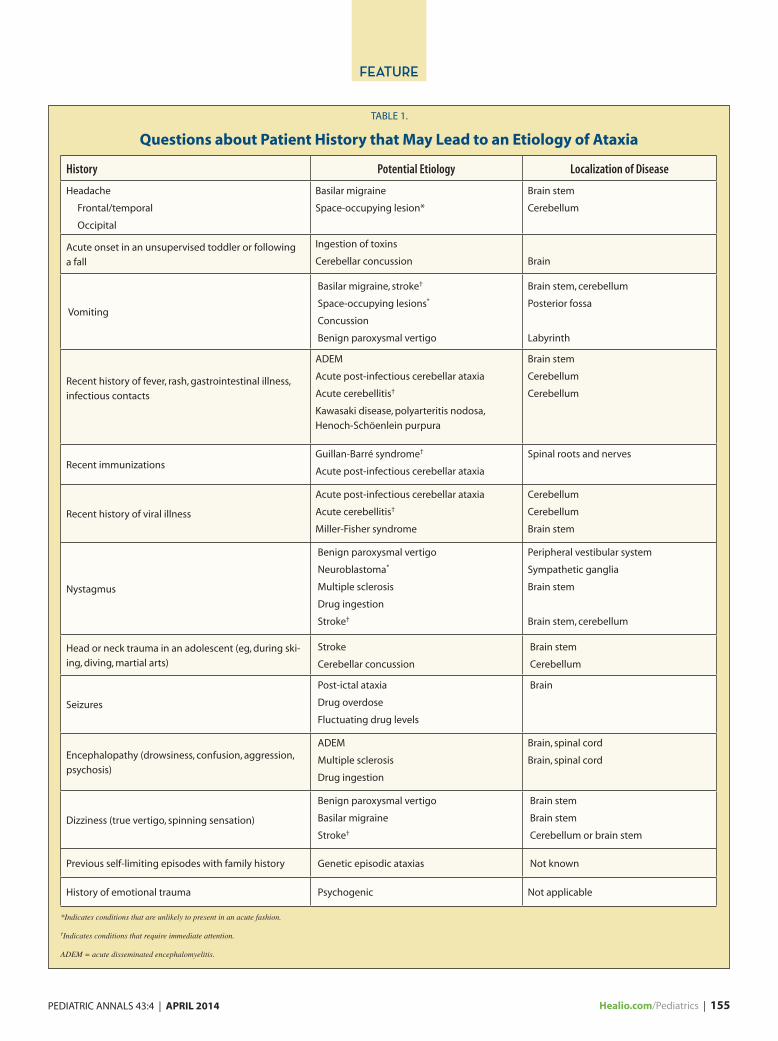
Important questions about patient history that may lead to an etiology are summarized in Table 1. As can be seen, there is significant overlap in symptomatology between different disease states, so it may be difficult to distinguish “central” from “peripheral” causes by history alone. Symptom on-set may occur in just a few minutes or over the course of hours or days.
Physical ExaminationPhysical examination should focus
on identifying life-threatening condi-
tions that may require immediate in-tervention. Presence of confusion, hallucinations, mood disturbances, or somnolence must be noted. Such symp-toms may indicate toxic ingestion, de-myelinating diseases such as acute dis-seminated encephalomyelitis (ADEM), stroke, or meningo-encephalitis. The presence of papilledema, pupillary dila-tion, and lateral rectus palsy indicates elevated intracranial pressure. Motor examination should focus on eliciting weakness in an anatomically significant pattern, such as one-half of the body or both lower extremities. Often, a younger child with hemiparesis or paraparesis will present with ataxia as opposed to focal weakness of the affected body part (ie, “paretic ataxia”).
A detailed cerebellar exam should follow. Dysfunction of midline cerebel-lar structures causes truncal ataxia and head tremor. Disorders of the lateral aspects of the cerebellum cause limb ataxia, which can be evaluated by the finger-nose or finger-finger test, inten-tion tremor, and dysdiadochokinesia. In the lower extremity, one can perform the heel-shin test to look for incoordina-tion. Cerebellar incoordination tends to be most prominent when movements are performed slowly. Ataxia caused by pathology of the cerebellum is not ex-acerbated by eye closure; therefore, a Romberg test will be negative.
Presence of nystagmus should be not-ed with relevant details. Nystagmus may arise from pathology in the vestibular system (“peripheral” type) or the central nervous system (“central”). Certain spe-cific types of nystagmus, such as opsoc-lonus, may rarely be noted.
Finally, a comprehensive sensory exam and an examination of deep ten-don reflexes should be performed to rule out diseases of peripheral nerves or roots (ie, “sensory” ataxia). Plantar responses are not affected by diseases of the cer-ebellum; hence, a positive Babinski test is indicative of disease processes in the
Figure 1. Fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging (MRI) demonstrating left cerebellar demyelinating lesion in a teenager with acute-onset ataxia. Similar lesions are noted in the cortex, as well. A final diagnosis of multiple sclerosis was made on the basis of imaging and investigations.
Imag
e co
urt
esy
of L
alit
ha
Siva
swam
y, M
D.
PEDIATRIC ANNALS 43:4 | APRIL 2014 Healio.com/Pediatrics | 155
FEATURE
TABLE 1.
Questions about Patient History that May Lead to an Etiology of Ataxia
History Potential Etiology Localization of Disease
Headache
Frontal/temporal
Occipital
Basilar migraine
Space-occupying lesion*
Brain stem
Cerebellum
Acute onset in an unsupervised toddler or following
a fall
Ingestion of toxins
Cerebellar concussion
Brain
Vomiting
Basilar migraine, stroke†
Space-occupying lesions*
Concussion
Benign paroxysmal vertigo
Brain stem, cerebellum
Posterior fossa
Labyrinth
Recent history of fever, rash, gastrointestinal illness,
infectious contacts
ADEM
Acute post-infectious cerebellar ataxia
Acute cerebellitis†
Kawasaki disease, polyarteritis nodosa,
Henoch-Schöenlein purpura
Brain stem
Cerebellum
Cerebellum
Recent immunizationsGuillan-Barré syndrome†
Acute post-infectious cerebellar ataxia
Spinal roots and nerves
Recent history of viral illness
Acute post-infectious cerebellar ataxia
Acute cerebellitis†
Miller-Fisher syndrome
Cerebellum
Cerebellum
Brain stem
Nystagmus
Benign paroxysmal vertigo
Neuroblastoma*
Multiple sclerosis
Drug ingestion
Stroke†
Peripheral vestibular system
Sympathetic ganglia
Brain stem
Brain stem, cerebellum
Head or neck trauma in an adolescent (eg, during ski-
ing, diving, martial arts)
Stroke
Cerebellar concussion
Brain stem
Cerebellum
Seizures
Post-ictal ataxia
Drug overdose
Fluctuating drug levels
Brain
Encephalopathy (drowsiness, confusion, aggression,
psychosis)
ADEM
Multiple sclerosis
Drug ingestion
Brain, spinal cord
Brain, spinal cord
Dizziness (true vertigo, spinning sensation)
Benign paroxysmal vertigo
Basilar migraine
Stroke†
Brain stem
Brain stem
Cerebellum or brain stem
Previous self-limiting episodes with family history Genetic episodic ataxias Not known
History of emotional trauma Psychogenic Not applicable
*Indicates conditions that are unlikely to present in an acute fashion.
†Indicates conditions that require immediate attention.
ADEM = acute disseminated encephalomyelitis.

156 | Healio.com/Pediatrics PEDIATRIC ANNALS 43:4 | APRIL 2014
FEATURE
upper motor neuron pathway, outside of the cerebellum.
ETIOLOGY ON THE BASIS OF AGE Infancy Opsoclonus Myoclonus Ataxia Syndrome
Opsoclonus myoclonus ataxia (OMA) syndrome can present as early as age 6 months. OMA syndrome is a paraneoplastic autoimmune phenom-enon characterized by chaotic conjugate high-amplitude eye movements, body jerks, and truncal/limb ataxia, along with developmental regression and irritability. An underlying neuroblastoma or gan-glioneuroblastoma is often recognized, although not universally present. Rec-ognition is facilitated when the triad of symptoms manifest in close proximity to each other. However, ataxia alone may precede the eye findings, leading to di-agnostic confusion and delays of months to years in initiating investigations.3 Nuclear scanning with metaiodobenzyl-guanidine scintigraphy (MIBG scan) has moderately high sensitivity, but children whose scans are negative should receive high-resolution computerized tomogra-phy (CT) or magnetic resonance imaging (MRI) of the chest and abdomen.4
Children Age 1 to 4 Years (Preschool)Acute Post-Infectious Cerebellar Ataxia
Acute post-infectious cerebellar ataxia (APCA), which accounts for up to 40% of cases of acute cerebellar ataxia in certain case series, typically occurs af-ter a febrile illness or immunizations.5 A prior history of varicella was reported in up to 26% of patients by some authors.1 A large number of other viruses have been implicated, including coxsackie B, echoviruses, mumps, Epstein-Barr, and influenza A and B. The pathology is be-lieved to be acute demyelination caused by cross-reacting antibodies to epitopes in the cerebellum.6 The disease onset can be up to 3 weeks after the systemic illness has subsided.7 Symptoms evolve over hours and are most prominent at
initial presentation, with relatively rapid resolution over the next few days. The mental status usually remains clear throughout the course of the illness. The presence of extreme irritability should raise suspicion about the diagnosis.
Examination reveals a pure cerebel-lar syndrome with marked involvement of gait and significant truncal ataxia.
The average child recovers in less than 2 weeks after disease onset. It is a self-limited condition that requires no spe-cific intervention or investigations. Ce-rebrospinal fluid (CSF) analysis can be performed with no risk of herniation, and it usually reveals a mild pleocyto-sis with negative viral and bacterial cul-tures. MRI tends to be normal or shows mild, non-specific changes.
Acute CerebellitisAcute cerebellitis may occur after a
systemic illness or be the direct result of infection in the cerebellum. Com-mon agents reported to cause acute cer-ebellitis are rotavirus, mycoplasma, and human herpesvirus 6. Clinical features include altered sensorium and mani-festations of raised intracranial pres-sure, in addition to features of a pure cerebellar syndrome. CSF analysis is likely to reveal pleocytosis, and in rare cases, antibodies against an infectious agent have been demonstrated.8 It must be mentioned that performing a spinal tap in the face of significant cerebellar edema can be life-threatening. Imag-ing can reveal abnormalities suggestive of edema in the cerebellum. Fatalities have been reported from acute cereb-ellitis.9,10 In essence, acute cerebellitis
differs from APCA by the presence, in some cases, of systemic symptoms such as fever and neck stiffness, symptoms and signs of raised intracranial pressure due to rapid compression of the fourth ventricle, and risk of death; there-fore, there is a pressing need for early therapy. There is considerable overlap between APCA and acute cerebellitis, so it may be difficult to distinguish be-tween the two conditions.
Toxic IngestionAccidental ingestion of drugs in chil-
dren in the preschool years may account for up to 30% of cases of acute ataxia. The Purkinje cells of the cerebellum are especially susceptible to toxic injury. Accidental ingestion of anticonvulsants, lead, eucalyptus oil, insecticides such as paraquat and phosphine, dextrometho-rphan, and shellfish poisoning may cause prominent cerebellar symptoms.11 Clini-cal features include depressed menta-tion or agitation, seizures, and cerebellar signs. The latter may be masked by the overall acuity of the situation. Parents should be asked to bring in all prescrip-tion medication for household members, and a urine/serum drug screen is essen-tial in the initial battery of tests.
Benign Paroxysmal VertigoBenign paroxysmal vertigo (BPV)
must be differentiated from benign par-oxysmal positional vertigo, which is the most common cause of vertigo in adults. BPV is characterized by brief spells of vertigo and ataxia. An otherwise healthy child suddenly looks frightened, pale, and wants to hold on to a parent for sup-port during episodes of BPV.12 The du-ration of symptoms is a few minutes at most, after which the child experiences no confusion or sleepiness.13 The typical age of onset is age 1 to 4 years, and reso-lution occurs around the age of 7 to 10 years. Examination is invariably normal between spells, as are imaging studies.14 A family history of migraine is found in
Accidental ingestion of drugs in children in the preschool years may account for up to 30% of cases of acute ataxia.

PEDIATRIC ANNALS 43:4 | APRIL 2014 Healio.com/Pediatrics | 157
FEATURE
many cases, and BPV itself is believed to be a migraine precursor.15
Acute Disseminated EncephalomyelitisADEM is an immune-mediated phe-
nomenon that presents after a viral ill-ness or immunization and is character-ized by encephalopathy (confusion, irritability, somnolence, personality changes) and acute onset of multifocal neurological deficits — most commonly ataxia.16 Seizures, cranial nerve palsies, hemiparesis, fever, and meningismus are frequently present.17 Imaging reveals bright lesions in the subcortical white matter, cerebellum, and basal ganglia. CSF is abnormal about half the time, with elevated white cells and protein. ADEM is usually a monophasic illness.
Inner Ear DiseaseOne of the rare complications of
acute otitis media is labyrinthitis, which is an extension of the middle ear bac-terial infection to the inner ear or laby-rinth, causing sensorineural hearing loss, tinnitus, nystagmus, and vertigo.18 The vertigo leads to ataxia. Fever, full-ness and pain in the ear, and mastoiditis may serve as clues to the diagnosis. The presence of nystagmus in a child with acute otitis media is often a reliable clue to the presence of impending labyrinthi-tis, so it should be treated expeditiously. The presence of contrast enhancement of the labyrinth on MRI is a sensitive indicator of disease process in this area. CT is less reliable.19
Children Age 5 to 16 years (School Age) Concussion
Cerebellar concussion is a clinical syn-drome wherein a head injury is followed by transient deficits in functioning of the cerebellum, with intact consciousness throughout. Patients typically present with a wide-based gait, truncal instability, and dysarthria. Most cases follow severe injuries;20 however, a few children have
been noted to have cerebellar concussion following relatively minor head trauma.21 The pathophysiology is believed to be damage to the connections between the cerebellum and the cortex, especially the superior cerebellar peduncle, following severe head injury. Transient vasospasm is the purported mechanism behind ataxia following mild injuries.22,23 No specific intervention is required and resolution is usually complete.
StrokeStrokes in the region of the cerebel-
lum (posterior circulation) are easily missed, as strokes are uncommon in childhood and posterior circulation strokes present with subtle symptoms that are often non-specific, with no clear-cut motor or sensory disturbances. Posterior circulation strokes present with dizziness about three-quarters of the time, nausea/vomiting or gait distur-bances about one-half of the time, and headache about a one-third of the time.24 Onset of symptoms is abrupt. Examina-tion may reveal ataxia with tendency to fall to the affected side, as well as verti-cal nystagmus, in addition to other clas-sic cerebellar signs. Presence of altered level of consciousness, hemiplegia, and cranial nerve weakness, when present, may quickly guide the clinician to an appropriate diagnosis. MRI is the diag-nostic test of choice because CT scan can miss a stroke in the cerebellum and brain stem. The majority of cerebellar strokes are caused by arteriopathy that may follow infection (such as varicella), vasculitis (such as Kawasaki disease), or dissection. Edema following a stroke is most prominent in the first 24 hours, and if it is in the region of the posterior circulation, then it is particularly omi-nous.25 Rapid swelling may compress the brain stem. The vast majority of such patients will die without surgical intervention.26 Therefore, all cerebellar strokes must be closely observed in an intensive care setting.
Multiple SclerosisMultiple sclerosis (MS) is an autoim-
mune demyelinating disease that affects different parts of the nervous system over time. About 50% of the children younger than the age of 5 years who have MS and 5% to 15% of adolescents who have MS present with acute ataxia, making it a relatively frequent disease manifestation.27,28 Children with MS have more frequent disease relapses than their adult counterparts, and they expe-rience significant cognitive decline and severe residual disability in their early adult years. Early imaging in the form of MRI with administration of contrast material and referral to a neurologist for initiation of therapy is essential.
Prescription Drug Use, Substance Abuse, and Poisoning
Adolescents who present with acute ataxia should be questioned regarding drugs of abuse as well as therapeutic agents they may be using for medical purposes. Benzodiazepines, phenytoin, and carbamazepine are the anticonvul-sants most likely to cause ataxia follow-ing acute intoxication. Free as well as total levels of drugs must be measured in these situations. Antineoplastics, such as fluorouracil (5-FU), cytarabine (ara-C), and methotrexate, may induce acute cerebellar damage. Drugs of abuse that may cause ataxia are toluene, cocaine, heroin, and phencyclidine. Toluene in-toxication can occur due to glue-sniffing or acute exposure in areas that are poorly ventilated.29 Cocaine use predisposes to cerebellar infarctions, as does envenom-ation due to a scorpion sting.11
Basilar Migraine Children with basilar migraine pres-
ent with an aura consisting of ataxia, diplopia, tinnitus, tingling in their ex-tremities, or alteration in the level of their consciousness that lasts from 5 minutes to 1 hour. A severe, pounding headache follows within 1 hour of these
158 | Healio.com/Pediatrics PEDIATRIC ANNALS 43:4 | APRIL 2014
FEATURE
symptoms and is typically accompanied by nausea/vomiting and photophobia/phonophobia. The headache may be unilateral or bilateral and is relieved by sleep. The average duration of the head-ache is 30 minutes to 3 days. Examina-tion is unremarkable, with no clear cer-ebellar signs other than ataxia. Initial episodes warrant an MRI.
Guillain-Barré SyndromeChildren may present with ataxia
due to disease processes in the periph-
eral nerves that do not allow appropri-ate sensory signals to reach the higher coordinating centers. A classic exam-ple of this is Guillain-Barré syndrome. A preceding viral infection or gastro-enteritis is noted in at least half of all cases. Children may experience severe pain in the lower extremities or back prior to the onset of weakness.30 Weak-ness and ataxia reach a nadir within 4 weeks. Rare instances may progress to involvement of the respiratory muscles and quadriparesis. Diagnostic testing
may include imaging of the spinal cord to rule out myelitis and spinal fluid analysis, although in most instances the diagnosis remains a clinical one that can be made with assurance at the bedside due to the triad of ataxia, areflexia, and motor weakness. Nerve conduction studies may be performed in atypical cases to confirm the diag-nosis. Coordination with a neurologist and intensivist is vital in children be-ing prepared for treatment of Guillain-Barré syndrome.
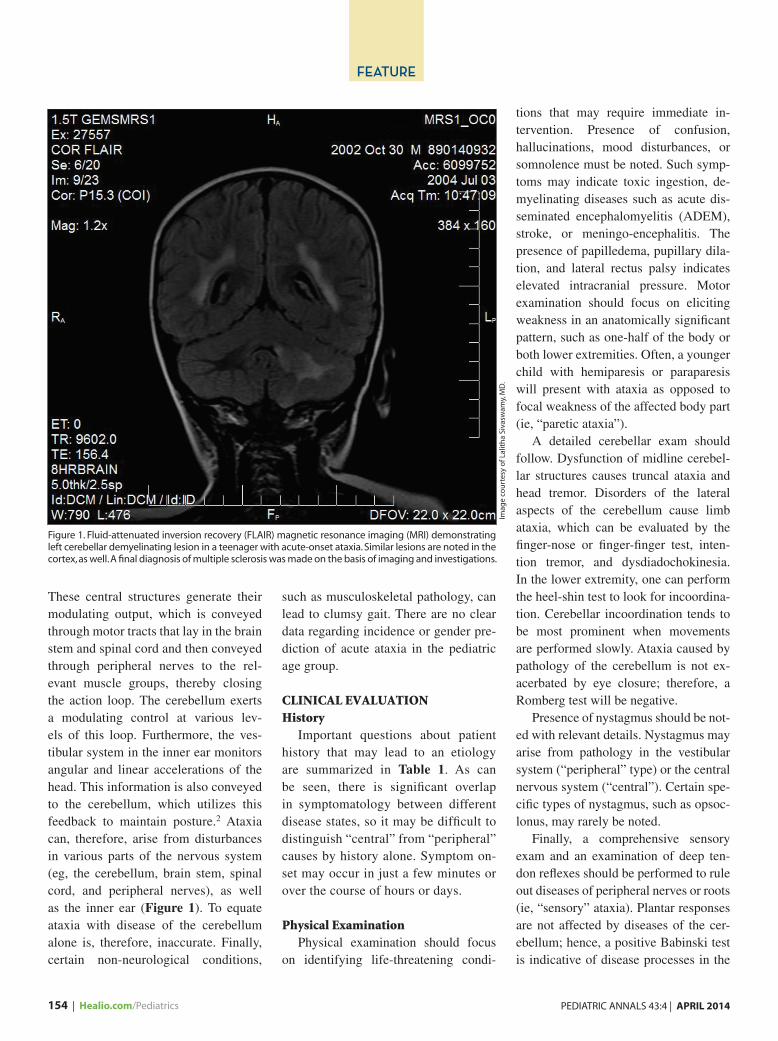
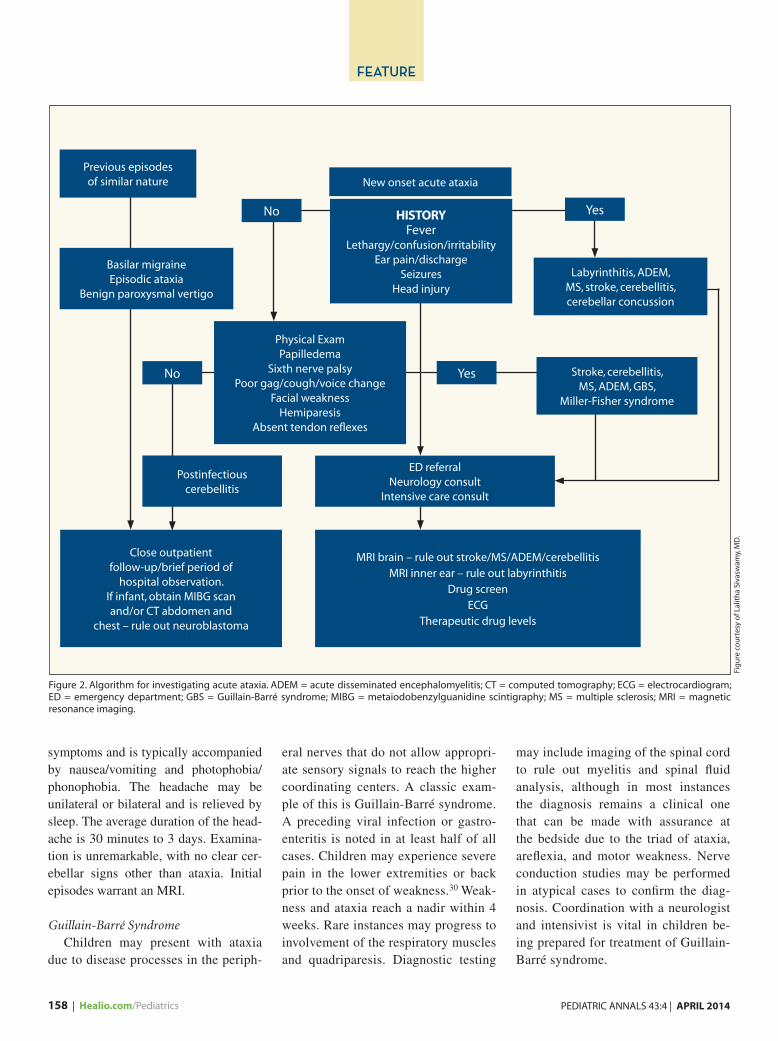
Figure 2. Algorithm for investigating acute ataxia. ADEM = acute disseminated encephalomyelitis; CT = computed tomography; ECG = electrocardiogram; ED = emergency department; GBS = Guillain-Barré syndrome; MIBG = metaiodobenzylguanidine scintigraphy; MS = multiple sclerosis; MRI = magnetic resonance imaging.
Previous episodes of similar nature
Basilar migraineEpisodic ataxia
Benign paroxysmal vertigo
Physical ExamPapilledema
Sixth nerve palsyPoor gag/cough/voice change
Facial weaknessHemiparesis
Absent tendon reflexes
Postinfectious cerebellitis
ED referral Neurology consult
Intensive care consult
Close outpatient follow-up/brief period of
hospital observation.If infant, obtain MIBG scan and/or CT abdomen and
chest – rule out neuroblastoma
MRI brain – rule out stroke/MS/ADEM/cerebellitis MRI inner ear – rule out labyrinthitis
Drug screen ECG
Therapeutic drug levels
Stroke, cerebellitis, MS, ADEM, GBS,
Miller-Fisher syndrome
Labyrinthitis, ADEM, MS, stroke, cerebellitis, cerebellar concussion
HISTORYFever
Lethargy/confusion/irritabilityEar pain/discharge
Seizures Head injury
New onset acute ataxia
No Yes
YesNo
Fig
ure
co
urt
esy
of L
alit
ha
Siva
swam
y, M
D.

PEDIATRIC ANNALS 43:4 | APRIL 2014 Healio.com/Pediatrics | 159
FEATURE
Episodic Ataxia Hereditary episodic ataxia (EA) re-
fers to a group of dominantly inherited conditions characterized by periods of cerebellar dysfunction that lead to acute ataxia. Seven different subtypes are recognized, of which EA2 is the most common. Attacks are precipitated by fatigue or strong emotion (such as an-ger or sadness) and may last for hours. In addition to ataxia, patients may ex-perience vertigo, nausea, vomiting, and (rarely) seizures.31 Patients may have migranous headaches and downbeat nystagmus between spells. The muta-tion responsible for EA2 is located on the CACNA1A gene.
CONCLUSIONAn algorithm for work-up of acute
ataxia is presented in Figure 2. Ataxia can cause significant anxiety for the child and family due to the dramatic na-ture of the symptoms. The fact that most children with acute onset ataxia will have rapid resolution of their symptoms must be emphasized to parents and care-givers. Collaboration with a child neu-rologist, radiologist, and intensive care physician may be of benefit in cases where serious intracranial pathology is a consideration.
REFERENCES 1. Ryan MM, Engle EC. Acute ataxia in child-
hood. J Child Neurol. 2003;18(5):309-316. 2. Brazis PW, Masdeau JC, Biller J. Localiza-
tion in Clinical Neurology. 4th ed. Philadel-phia, PA: Lippincott Williams & Wilkins; 2001:309-327.
3. Desai J, Mitchell WG. Acute cerebellar ataxia, acute cerebellitis, and opsclonus-
myoclonus syndrome. J Child Neurol. 2012;27(11):1482-1488.
4. Gorman MP. Update on diagnosis, treat-ment, and prognosis in opsoclonus-myclo-nus-ataxia syndrome. Curr Opin Pediatr. 2010;22(6):745-750.
5. Gieron-Korthals MA, Westberry KR, Emman-uel PJ. J Child Neurol. 1994;9(4):381-384.
6. Adams C, Diadori P, Schoenroth L, Frit-zler M. Autoantibodies in childhood post varicella cerebellar ataxia. Can J Neurol Sci. 2000;27(4):316-320.
7. Nussinovitch M, Prais D, Volovitz D, Sha-piro R, Amir J. Post-infectious acute cer-ebellar ataxia in children. Clin Pediatr. 2003;42(7):581-584.
8. Gayatri N, Tyagi A, Mahadevan U. Acute hy-drocephalus in a child with mycoplasma cer-ebellitis. Brain Dev. 2009;31(8):618-621.
9. Kamate M, Chetal V, Hattiholi V. Fulminant cerebellitis: a fatal clinically isolated syn-drome. Pediatr Neurol. 2009;41(3):220-222.
10. Hacohen Y, Niotakis G, Aujla A, et al. Acute life threatening cerebellitis presenting with no apparent cerebellar signs. Clin Neurol Neuro-surg. 2011;113(10):928-930.
11. Manto M. Toxic agents causing cerebellar ataxias. Handb Clin Neurol. 2012;103:201-213. doi: 10.1016/B978-0-444-51892-7.00012-7.
12. Basser LS. Benign paroxysmal vertigo of childhood (a variant of vestibular neuronitis). Brain. 1964;87:141-152.
13. Marcelli V, Piazza F, Pisani F, Marciano E. Neuro-otological features of benign parox-ysmal vertigo and benign paroxysmal posi-tioning vertigo in children: a follow up study. Brain Dev. 2006;28(2):80-84.
14. Cuvellier JC, Lepine A. Childhood periodic syndromes. Pediatr Neurol. 2010; 42(1):1-11.
15. Lanzi G, Balottin U, Fazzi E, Mira E, Pia-centino G. Benign paroxysmal vertigo in childhood: a longitudinal study. Headache. 1986;26(10):494-497.
16. Hynson JL, Kornberg AJ, Coleman LT, et al. Clinical and radiological features of acute disseminated encephalomyelitis in childhood. Neurology. 2001;56(10):1308-1312.
17. Tenembaum S, Chamoles N, Fejerman N. Acute dissmeniated encephalomyelitis: a long- term follow- up study of 84 pediatric patients. Neurology. 2002;59(8):1224-1231.
18. Kitsko DJ, Dohar JE. Inner ear and facial nerve complications of acute otitis media, including vertigo. Curr Allergy Asthma Rep. 2007;7(6):444-450.
19. Pelligrini S, Gonzalez Macchi ME, Sommer-fleck PA, Bernaldez PC. Intratemporal com-plications from acute otitis media in children: 17 cases in two years. Acta Otorrinolaryngol Esp. 2012;63(1):21-25.
20. Fumeya H, Hideshima H. Cerebellar concus-sion- three case reports. Neurol Med Chir. 1994;34(9):612-615.
21. Gohil JR, Munshi SS. Post concussion ataxia following minor head injury. Indian Pediatr. 2006;43(9):829.
22. Haggard P, Miall RC, Wade D, et al. Dam-age to cerebellocortical pathways after closed head injury: a behavioral and magnetic reso-nance imaging study. J Neurol Neurosurg Psychiatry. 1995;58(4):433-438.
23. Yeoh HK, Lind CR, Law AJ. Acute transient cerebellar dysfunction and stuttering follow-ing mild closed head injury. Childs Nerv Syst. 2006;22(3):310-313.
24. Edlow JA, Newman-Toker DE, Savitz SI. Diagnosis and initial management of cerebellar infarction. Lancet Neurol. 2008;7(10):951-964.
25. Mackay MT, Prabhu SP, Coleman L. Child-hood posterior circulation in arterial ischemic stroke. Stroke. 2010;41(10):2201-2209.
26. Heros SC. Surgical treatment of cerebellar in-farction. Stroke. 1992;23(7):937-938.
27. Bigi S, Banwell B. Pediatric multiple sclero-sis. J Child Neurol. 2012;27(11):1378-1383.
28. Banwell B, Ghezzi A, Bar-Or A, Mikael-off Y, Tardieu M. Multiple sclerosis in chil-dren: clinical diagnosis, therapeutic strate-gies, and future directions. Lancet Neurol. 2007;6(10):887-902.
29. King MD. Neurological sequelae of toluene abuse. Hum Toxicol. 1982;1(3):281-287.
30. Bradshaw B, Jones H Jr. Guillain-Barre syn-drome in childhood: clinical course, elec-trodiagnosis and prognosis. Muscle Nerve. 1992;15(4):500-506.
31. Winchester S, Mikati MA. Ataxia. In Dulac O, Lassonde M, Sarnat HB, eds. Handbook of Clinical Neurology. Amsterdam, Netherlands: Elsevier; 2013:1213-1217.