Embed Size (px)
Citation preview

1
VALUE• Competitive
Premiums• Profit Allocations to
Subscribers• 15% RM Credit
PROTECTION• Your Reputation –
Our Business• Claims Expertise• Risk Management
PARTNERSHIP• Service #1• Broad Coverage• Joint Defense• Patient Safety
Mission
The MPIE Advantage
OUR BUSINESS IS PROTECTING YOURS!
An interview of Pamela L. Popp, MA, JD, DFASHRM, CPHRM, DSA, AIMExecutive Vice President/Chief Risk OfficerWestern Litigation, Inc.
Appreciating the Risk of Sepsis
This information is provided as a risk management resource and should not be construed as legal, compliance, technical or clinical advice. This information may refer to specific local regulatory or legal issues that may not be relevant to your organization. Consult your professional advisors or legal counsel for guidance on issues specific to your organization. This material may not be reproduced or distributed without the express, written permission of MPIE.
Physician Attestation Form
Physicians and advanced practice professionals must complete the Attestation Form and return it to MPIE in order to receive credit for the premium discount program. The form was included in the email that contained the webinar connection instructions.
Return the form to:
• Email: [email protected]
• Fax: 616.741.1999
Asking Questions
Pamela L. Popp, MA, JD, DFASHRM, CPHRM, DSA, AIMExecutive Vice President/Chief Risk Officer
Western Litigation, Inc.
Presenter

2
What is Sepsis?
A Bit of History
Source: Google.
The Merinoff Symposium 2010: Sepsis hosted a gathering of international experts, where they discussed the issues surrounding sepsis, including a global definition and a declaration that sepsis is a medical emergency.
Not a New Issue
“Sepsis is a life threatening condition that arises when the body’s response to an infection injures its own tissues and organs. Sepsis leads to shock, multiple organ failure and death especially if not recognized early and treated promptly. Sepsis remains the primary cause of death from infection despite advances in modern medicine, including vaccines, antibiotics and acute care. Millions of people die of sepsis every year worldwide.”
Source: Czura.
• Dangerous‒ Mortality rate of 40%, half
of all hospital deaths, estimates of 200,000–400,000 deaths/year in US
• Prevalent‒ 1 million discharges per
year include sepsis dx
• Preventable‒ 50% of cases could have
been dx earlier
Why Sepsis?
• Expensive
‒ Most costly inpatient condition
‒ $24 billion in healthcare costs yearly
‒ LOS extends by 11 days, additional $33,000/pt
‒ 6.2% of all healthcare costs
‒ 92,000 readmissions/yr
Sources: Liu et al.; Torio and Moore; Hines et al.
The National Quality Forum (NQF), which vetted the measure for CMS, noted that sepsis continues to be a big problem at many hospitals. "The national bill for sepsis [associated with] pneumonia grew twice as fast as the overall growth in hospital charges -- about a 180% increase from 1997 to 2005, accounting for over $54 billion per year," the NQF wrote. "When combined with pneumonia, sepsis is the 3rd largest consumer of Medicare, 4th largest consumer of Medicaid, and 5th largest consumer of private insurance financial resources and total hospital days."
High Resources
• Symptoms are subtle—may delay time to ED
• Symptoms mimic other (less severe) conditions
• Condition escalates quickly
• No one specialty or department “owns” sepsis
• Community hospitals may not have infectious specialties/resources
Challenges

3
• Lack of general knowledge of symptoms
• Prolonged treatment, healing
• Post sepsis syndrome
• Extensive medical bills
• Loss of limbs/life
• Confusion as to “cause”
The Patient’s Perspective
• According to polling conducted by Harris Interactive commissioned by Sepsis Alliance, fewer than half of adult Americans have ever heard of sepsis.
General Public Awareness
Source of data: Harris Interactive.
• Limited guidelines for reference
• Focus on infection, miss the signs
• Patient compromises quickly
• Quick decisions needed on limited information
• “Someone missed it” pressure
The Provider’s Perspective
• Preventable patient harm
• Expensive claims/lawsuits
The Organization’s Perspective
Why Sepsis?
5% death occurs before treatment
sought
15% develops while inpatient
80% from community, arrives via ER

4
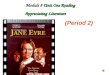
Clinical Ramifications of Sepsis
Common Sources of Sepsis
© world-sepsis-day.org
Sepsis: Sources of Sepsisby Lindgruen-GmbH / CC BY-NC-SA 3.0
Infection to SIRS to Shock
Sepsis Mortality Rate
Source of data: Kumar et al.
© world-sepsis-day.org
Sepsis Is an Emergency by Lindgruen-GmbH / CC BY-NC-SA 3.0
What used to be called SEPSIS . . .
Is now called INFECTION• The previous definition focused on
inflammation—signs of which can arise even with uncomplicated infection.
• BUT inflammatory criteria did poorly in identifying which patients would have bad outcomes.
Old versus New Definitions
Photo courtesy of Comstock
Sources: Singer et al.; Singer.

5
What used to be called SEVERE SEPSIS . . .
Is now called SEPSIS• “Life-threatening organ
dysfunction caused by a dysregulated host response to infection”
• Sepsis redefined focuses on organ dysfunction rather than inflammation.
Old versus New Definitions
Source: Singer et al.
What used to be called SEPTIC SHOCK . . .
Is still essentially called SEPTIC SHOCK• “A subset of sepsis in
which underlying circulatory and cellular/metabolic abnormalities are profound enough to substantially increase mortality”
Old versus New Definitions
Source: Singer et al.
• Over 62% of survivors are readmitted to the hospital within 30 days of discharge
• Susceptible to sepsis reoccurrence
• Long-term problems include:
‒ Amputations, anxiety, memory loss, chronic pain
• Increased mortality post admission
Postsepsis Syndrome
Source: Sutton and Friedman.
Reimbursement Ramifications of Sepsis
Cost Impact
Source: Pfuntner et al.
Sepsis is the most costly inpatient hospital condition
Sepsis annual hospital costs (2011) $20.3 Billion
Sepsis average cost per hospital stayDouble the average cost per stay across all other conditions $18,400
Sepsis average annual cost growthAnnual growth 3x the growth rate of overall hospital costs
11.5%
Highest Condition Driving Readmissions
Source: Hines et al.
Medicare (65+)
Medicaid (18-64y)
Private(18-64y)
Total
All cause readmissions (1000s) 1,800 700 600 3,100
Sepsis readmissions (1000s) 92.9 17.6 14.8 125.3
Sepsis readmission rate 21.3% 23.8% 15.4%
Percentage of total payer readmissions (rank)
5.1% (2nd) 2.6% (8th) 2.4% (5th) 4.0%
Cost of sepsis readmissions ($M)
1,410 319 272 2,001
Percentage of costs of total payer readmission costs
5.9% 4.2% 3.4% 5.0%

6
• Average Mortality is 12%, Average LOS is 7 days
• Mortality in DRG 870 is 200% higher, LOS and Average Cost for DRG 870 is 300% higher than others
• Only 5% of Cases get coded with DRG 870
Reimbursement: Coding Failure
31
• Average Direct Cost is $10,000
• Average Reimbursement Amount is $9,000
• Average direct costs for 870 is $55,990
Reimbursement: Coding Failure
32
• Sepsis is the largest contributor to readmissions
• Average mortality rises from 10% to 15% in readmission cases
Readmissions: Impact of Sepsis
Sepsis to Sepsis readmissions account for 50% of total readmissions
Data Analysis
• 2017 review of case cases where ‘sepsis’ was in the narrative descriptor
‒ Conservative number, could expand to include those where ‘post op infection’, ‘pneumonia’ or other descriptor utilized
• 32,000 cases out of 100,000 database
• Incurred for these cases totaled $2 billion
WLI Database 2017 WLI Sepsis Database

7
WLI Sepsis Database WLI Sepsis Cost Analysis
Total Incurred $
Costs by Key Injury Category
Amputation ALAE $26,915.24Amputation Indemnity $77,776.79Amputation Total Incurred $104,692.02
Brain damage ALAE $77,936.68Brain damage Indemnity $259,925.00Brain damage Total Incurred $337,861.68
Death ALAE $45,968.30Death Indemnity $99,193.43Death Total Incurred $145,161.73
Primary Patient Safety Issues Identified
• Key patients at risk:
‒ Post operative
‒ Obstetrical
‒ Elderly
‒ Newborns
‒ Chemotherapy
‒ Dialysis
WLI Data Analysis
Ironshore, 2017

8
Litigation Examples
December 16, 2015, $2.6 Million Verdict in Medical Malpractice Case
• On April 14, 2013, the 33 year-old woman presented to a local hospital with chief complaints of shortness of breath, back pain, nausea, vomiting, chills, dizziness and painful urination. Hours later, it was noted by nursing staff that the patient’s urine was dark in color.
• The family’s attorneys argued that the presence of an infection was clear and that the medical staff needed to administer antibiotics and make prompt arrangements for her to be transferred to a facility with the capabilities to care for her condition, such as an intensive care unit. Instead, treatment was delayed more than ten hours before antibiotics were administered.
• The patient died just two days later from sepsis. Experts for the family testified that this woman’s symptoms on presentation to the hospital “screamed of kidney infection, UTI and sepsis,” but the diagnosis was missed for a critically long period of time.
REAL CASE SCENARIO
October 2014, $1.6 Million Verdict in Medical Malpractice Case
• A 63-year-old male admitted with shortness of breath was diagnosed with pneumonia. The hospitalist’s impression was that the patient had acute bronchitis with mild respiratory distress. The hospitalist ordered antibiotics and breathing treatments. Later that day, the patient, in severe respiratory distress with neck swelling, was unable to swallow. He was transferred to the ICU. Otolaryngology and pulmonary consults were ordered (not STAT).
• Fifteen minutes after admission to the ICU, the patient had respiratory arrest. Intubation was difficult due to his swollen neck. He was initially resuscitated but died a short time later. An autopsy revealed a mediastinal abscess and sepsis. The infected soft tissues surrounding the pharynx completely obstructed the upper airway, which led to respiratory arrest and death.
• Expert reviewers noted that signs of sepsis were present at admission and not recognized.
REAL CASE SCENARIO
Pending Medical Malpractice Case
• After an uneventful delivery, the new mother becomes febrile with a rash. She returns to the hospital via the ED, where the ED staff entered her symptoms into the chart and received a “sepsis alert.”
• The alert was disregarded, per the nurse, “because we always see those” and it was simply thought to be a false positive result. Her OB was contacted by the ED physician, but since the delivery was ‘normal’, the OB did not come in to see the patient.
• The patient was discharged home after she was rehydrated and her temperature decreased.
• The patient died less than 24 hours later of septic shock.
Early expert reviewers noted that signs of sepsis were present upon arrival and not recognized.
REAL CASE SCENARIO
REAL CASE SCENARIO
The patient, a 26 yr old radiology tech, left sick from work, and stopped by an urgent care where she was diagnosed with the flu (she had recently received a flu shot).
The next day she called her mother and said, "Mom, I've never been this sick". Her parents met her in the emergency room, and providers told them that she had a high heart rate, low blood pressure and a low temperature. About 12 hours later, the hospital called her parents and told them she had taken a turn for the worse.
"They told us sepsis had set in, and it was too late," her mother said. "By that time, all her organs had begun to fail. There was nothing they could do."
Discovery Challenges

9
Standard of Care
In malpractice, “the average degree of skill, care, and diligence exercised by members of the same profession, practicing in light of the present state of medical and surgical science.”
Interesting Article on the Standard of CareJournal of Clinical Oncology, VOLUME 27 NUMBER 32 NOVEMBER 10 2009 --What Does the Medical Profession
Mean By “Standard of Care?” http://jco.ascopubs.org/content/27/32/e192.full.pdf+html
If the Standard of Care looks at the practice of physicians in the same specialty on the same clinical topic;
And the SS Guidelines are published to encourage world wide awareness and usage;
Then do the SS Guidelines become the new Standard of Care?
Impact on Standard of Care
“The recommendations in this document are intended to provide guidance for the clinician caring for a patient with severe sepsis or septic shock. Recommendations from these guidelines cannot replace the clinician’s decision-making capability when he or she is presented with a patient’s unique set of clinical variables.”
Surviving Sepsis Campaign (SCCM)
• Providers are expected to treat these patients as follows: Measure lactate level
Obtain blood cultures prior to antibiotics
Administer broad-spectrum antibiotics
Administer 30 mL/kg crystalloid for hypotension or lactate ≥4 mmol/L
Apply vasopressors (for hypotension that does not respond to initial fluid resuscitation to maintain a mean arterial pressure ≥65)
In the event of persistent arterial hypotension despite volume resuscitation (septic shock) or initial lactate ≥4 mmol/L (36 mg/dL), measure central venous pressure and central venous oxygen saturation
Remeasure lactate if initial lactate is elevated
• The measure calls for both severe sepsis and septic shock patients to receive the first three procedures within their first 3 hours of care, and for septic shock patients to receive the last four procedures within 6 hours.
CMS Core Measures
HREN 2016
1. Did you have screening processes in place for sepsis when plaintiff was a patient there?
2. If yes, what are those processes? And was the plaintiff screened for sepsis? If no, why? If yes, how?
3. Was plaintiff suffering from sepsis on admission? If yes, what level? If no, did the plaintiff become septic in the ED or during admission/transfer?
Sepsis Discovery Issues

10
4. What was the cause/source of the sepsis?
5. Did you discover it? If yes, when? And should you have discovered it sooner? If no, why not? And was it a deviation not to have discovered it?
6. What type of sepsis was it: severe sepsis or septic shock? What are your protocols to address each?
Sepsis Discovery Issues (cont’d)
7. Did you suspect plaintiff had sepsis before its diagnosis? If yes, did you do the following:
a. administer oxygenb. test blood for infectionc. give antibioticsd. give IV fluidse. measure serum lacate (lactic acid in blood)
and hemoglobin (protein in red blood cells)f. measure hourly urine output
Sepsis Discovery Issues (cont’d)
8. Could plaintiff’s damages have been avoided or lessened if sepsis were diagnosed/treated sooner?
9. Did plaintiff have a preexisting condition making him/her susceptible to sepsis? If yes, what was it?
10.What experts are best qualified to address the liability, causation and damages claims?
Sepsis Discovery Issues (cont’d)
Successful Mitigation Examples
Study: Hoag Hospital
60

11
61
Hoag Hospital
Risk Reduction Steps
Action Plan: Gather
• Statewide statistics on sepsis rates (available online at www.cms.gov)
• Hospital specific sepsis rate (typically found in the coding office and/or medical records)
• Definition of sepsis utilized by the facility for reporting (reference ICD9 or 10 codes if needed)
• Average patient care cost and length of stay to compare to industry numbers ($18,400 and 14 days)
• Multiply the number of sepsis cases reported each month by the hospital times the average care cost and share with senior management members
Gather
# of sepsis cases/yr x (average cost per case) – (reimbursement) =
loss impact of sepsis to your facility
For example:
2,000/yr x ($15,000-$12,000) = $6m
Action Plan: Loss Impact
Action Plan: Implement
•Distribute sepsis bundle clinical guidelines with the medical staff, employed providers and all supporting clinical staff (consider pocket cards from Sepsis Alliance)
•Post sepsis symptom information in all ED, ICU patient rooms with information on how to contact a sepsis response team (often a rapid response team)
•Share an educational video, such as Faces of Sepsis or Sepsis as an Emergency from Sepsis Alliance with staff and providers to illustrate the toll sepsis, and Post Sepsis Syndrome, has on patients and their families
•Identify sepsis simulation training opportunities, from a rehearsed scenario to actual mannequin training
•Educate case workers on sepsis support resources, including Post Sepsis Syndrome resources, such as home care, psychological support and memory care
Implement
• Use visual clues throughout the facility
‒ Cafeteria, waiting rooms, ED waiting area
• Encourage staff to say “I suspect sepsis”
‒ Suspicion = Rule Out First!
• Hold interdisciplinary debriefs on cases
‒ What could have improved outcome?
• Support the post sepsis patient
Action Plan: Keep It Visible

12
Resources
Facts about sepsis, Centers for Disease Control 2017
Facts about sepsis, Centers for Disease Control 2017
Coopersmith, Craig, MD, FACS, FCCM (Professor of Surgery, Associate Director of Emory Critical Care Center, Emory University School of Medicine). Podcast interview with: Society for Critical Care Medicine. 2016 Feb 22. http://www.sccm.org/Podcasts/SCCMPod311.mp3
Czura CJ. Merinoff Symposium 2010: Sepsis—speaking with one voice. Mol Med 2011 Jan-Feb;17(1-2):2-3.
Davydow DS, Hough CL, Langa KM, et al. Depressive symptoms in spouses of older patients with severe sepsis. Crit Care Med 2012 Aug;40(8):2335-41.
Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med 2013 Feb;41(2):580-637.
ECRI Institute. Sepsis at a glance. 2016 [cited 2016 Jul 14]. https://www.ecri.org/components/HRC/Documents/Sepsis%20at%20a%20Glance.pdf
ECRI Institute. Sepsis: combating the hidden colossus. 2015 Dec 1 [cited 2016 Jul 14]. https://www.ecri.org/components/HRC/Pages/RMRep1215_Focus.aspx
ECRI Institute PSO. Improving recognition and management of sepsis and septic shock. PSO Navigator 2016 Aug;8(3):1-14.
Elixhauser A, Friedman B, Stranges E. Septicemia in U.S. hospitals, 2009. Healthcare Cost and Utilization Project Statistical Brief #122. 2011 Oct [cited 2015 Aug 20]. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb122.pdf
Google. Sepsis. [cited 2016 Jul 22]. https://www.google.com/#q=what+is+sepsis
Harris Interactive. Sepsis awareness 2013 [presentation]. 2013 Jun [cited 2016 Jul 5]. http://www.sepsisalliance.org/downloads/sepsisawareness2013.pdf
References

13
Hines AL, Barrett ML, Jiang HJ, et al. Costs for hospital stays in the United States, 2011. Healthcare Cost and Utilization Project Statistical Brief #172. 2014 Apr [cited 2016 Jul 22]. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb172-Conditions-Readmissions-Payer.pdf
Iwashyna TJ, Cooke CR, Wunsch H, et al. Population burden of long-term survivorship after severe sepsis in older Americans. J Am Geriatr Soc 2012 Jun;60(6):1070–7.
Jones C, Skirrow P, Griffiths RD, et al. Post-traumatic stress disorder-related symptoms in relatives of patients following intensive care. Intensive Care Med 2004 Mar;30(3):456-60.
Liu V, Escobar GJ, Greene JD, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA 2014 Jul 2;312(1):90-2.
Lupkin S. Newlywed Dies of Sepsis After Getting Flu. 2015 Jan 15 [cited 2016 Aug 4]. http://abcnews.go.com/Health/newlywed-dies-sepsis-flu/story?id=28253815
Pfuntner A, Wier LM, Steiner C. Costs for hospital stays in the United States, 2011. Healthcare Cost and Utilization Project Statistical Brief #168. 2013 Dec [cited 2016 Jul 22]. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb168-Hospital-Costs-United-States-2011.pdf
Popp PL. Hiding in plain sight: Why are we worried about Ebola and not sepsis? J Healthc Risk Manage 35(4):22-7. http://onlinelibrary.wiley.com/doi/10.1002/jhrm.21220/abstract
Rosendahl J, Brunkhorst FM, Jaenichen D, et al. Physical and mental health in patients and spouses after intensive care of severe sepsis: a dyadic perspective on long-term sequelae testing the Actor-Partner Interdependence Model. Crit Care Med 2013 Jan;41(1):69-75.
Semmler A, Widmann CN, Okulla T, et al. Persistent cognitive impairment, hippocampal atrophy and EEG changes in sepsis survivors. J Neurol Neurosurg Psychiatry 2013 Jan;84(1):62-9.
References
Singer, Mervyn, MD, FRCP (Professor of Intensive Care Medicine, University College London). Podcast interview with: EMcrit.org [blog]. 2016 Mar 7. http://emcrit.org/podcasts/sepsis-3/
Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016 Feb 23;315(8):801-10.
Sutton JP, Friedman B. Trends in septicemia hospitalizations and readmissions in selected HCUP states, 2005 and 2010. Healthcare Cost and Utilization Project Statistical Brief #161. 2013 Sep [cited 2016 Jul 22]. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb161.pdf
Torio CM, Moore BJ. National inpatient hospital costs: the most expensive conditions by payer, 2011. Healthcare Cost and Utilization Project Statistical Brief #204. 2016 May [cited 2016 Jun 24]. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb204-Most-Expensive-Hospital-Conditions.jsp
References
Q & A
Asking Questions
Physician Attestation Form
Physicians and advanced practice professionals must complete the Attestation Form and return it to MPIE in order to receive credit for the premium discount program. The form was included in the email that contained the webinar connection instructions.
Return the form to:
• Email: [email protected]
• Fax: 616.741.1999
Questions?
Contact MPIE at:[email protected]