Embed Size (px)
Citation preview

Applying for a CESR or CEGPR Specialist Applications Team Scotland 4 – 5 September 2014

Gui
danc
e on
you
r cu
rric
ulum
vita
e fo
r ap
plic
ants
for
entr
y on
to t
he S
peci
alis
t Re
gist
er o
r G
P Re
gist
er
This
sec
tion
giv
es g
uid
ance
on
wh
at t
o in
clu
de
in y
our
curr
icu
lum
vit
ae (
CV
)
Wha
t to
incl
ude
As
part
of
your
app
licat
ion,
you
mus
t in
clud
e a
CV t
hat
is le
ss t
han
thre
e m
onth
s ol
d. W
e st
rong
ly r
ecom
men
d th
at y
ou w
rite
you
r CV s
peci
fical
ly f
or t
his
appl
icat
ion.
The
info
rmat
ion
in y
our
CV m
ust
mat
ch t
he in
form
atio
n in
you
r ap
plic
atio
n.
The
tabl
e be
low
sho
ws
wha
t yo
u sh
ould
incl
ude
in y
our
CV a
nd t
he o
rder
the
sec
tions
sho
uld
be in
.
Sec
tion
D
etai
l
Pers
onal
det
ails
and
co
ntac
t in
form
atio
n
Your
nam
e on
you
r CV m
ust
mat
ch y
our
nam
e on
you
r pr
oof
of
iden
tity.
You
r co
ntac
t in
form
atio
n sh
ould
mat
ch t
he d
etai
ls w
e ho
ld w
hich
can
be
upda
ted
usin
g G
MC O
nlin
e.
Reg
istr
atio
ns
Giv
e yo
ur G
MC r
efer
ence
num
ber
and
deta
ils o
f an
y ot
her
med
ical
reg
ulat
ors
you
are
regi
ster
ed w
ith.
Mem
bers
hips
Li
st y
our
mem
bers
hips
of
prof
essi
onal
bod
ies.
Qua
lific
atio
ns
List
you
r qu
alifi
catio
ns.
Empl
oym
ent
hist
ory
1 -
pos
ts h
eld
Sta
rt w
ith t
he m
ost
rece
nt a
nd w
ork
back
war
ds.
Plea
se s
how
:
• po
st t
itle
(ple
ase
give
the
titl
e yo
u w
ere
empl
oyed
unde
r)
• da
tes
post
hel
d
• If
the
pos
t is
par
t tim
e, w
hat
perc
enta
ge o
f w
hole
tim
e
equi
vale
nt
• in
stitu
tion
nam
e an
d lo
catio
n
• th
e na
me
of y
our
supe
rvis
or (
espe
cial
ly r
equi
red
for
trai
ning
pos
ts)
Als
o gi
ve a
brief
job
des
crip
tion
that
cov
ers
the
dutie
s re
quired
fo
r th
at p
ost
and
indi
cate
the
leve
l of
supe
rvis
ion.
Empl
oym
ent
hist
ory
2 Sta
rt w
ith t
he m
ost
rece
nt a
nd w
ork
back
war
ds.
2

Sec
tion
D
etai
l
- ga
ps in
em
ploy
men
t Any
gap
s th
at s
pan
over
28
days
sho
uld
be a
ccou
nted
for
with
a
brie
f ex
plan
atio
n.
Aw
ards
Li
st a
ny a
war
ds y
ou h
ave
rece
ived
.
Res
earc
h ex
perien
ce
Giv
e a
brie
f ex
plan
atio
n of
any
res
earc
h yo
u ha
ve u
nder
take
n,
or h
ave
part
icip
ated
in.
Publ
icat
ions
Li
st y
our
publ
icat
ions
.
Pres
enta
tions
G
ive
deta
ils o
f an
y pr
esen
tatio
ns y
ou h
ave
give
n. Y
ou m
ay f
ind
it he
lpfu
l to
divi
de t
hem
up
into
inte
rnat
iona
l, na
tiona
l, re
gion
al
and
depa
rtm
enta
l to
show
the
ir im
port
ance
.
Con
tinui
ng
Prof
essi
onal
D
evel
opm
ent
(CPD
) Li
st y
our
CPD
act
ivity
in t
he la
st f
ive
year
s.
Con
fere
nces
att
ende
d G
ive
deta
ils o
f an
y co
nfer
ence
s yo
u ha
ve a
tten
ded.
You
may
fin
d it
help
ful t
o di
vide
the
m u
p in
to in
tern
atio
nal,
natio
nal,
regi
onal
an
d de
part
men
tal t
o sh
ow t
heir im
port
ance
.
Cou
rses
att
ende
d G
ive
deta
ils o
f an
y co
urse
s yo
u ha
ve a
tten
ded.
You
may
fin
d it
help
ful t
o di
vide
the
m u
p in
to in
tern
atio
nal,
natio
nal,
regi
onal
an
d de
part
men
tal t
o sh
ow t
heir im
port
ance
.
Aud
it Li
st a
nd g
ive
a br
ief
desc
ript
ion
of y
our
audi
t ac
tiviti
es.
Teac
hing
and
tra
inin
g ex
perien
ce
List
and
giv
e a
brie
f de
script
ion
of y
our
teac
hing
and
tra
inin
g ac
tiviti
es.
Man
agem
ent
expe
rien
ce
List
and
giv
e a
brie
f de
script
ion
of y
our
man
agem
ent
activ
ities
.
Proc
edur
es
List
the
pro
cedu
res
you
have
per
form
ed
Any
ext
ra a
ctiv
ities
If
the
re is
any
thin
g el
se r
elev
ant
to t
his
appl
icat
ion
you
can
list
it he
re.
Form
attin
g yo
ur C
V
• N
umbe
r ea
ch p
age
• Sho
w y
our
surn
ame
and
initi
als
at t
he t
op o
f ea
ch p
age
• U
se b
ulle
t po
ints
• In
clud
e a
shor
t de
scri
ptio
n fo
r ea
ch it
em.
3

Com
mon
mis
take
s Yo
ur C
V w
ill b
e re
turn
ed t
o yo
u if
it do
es n
ot m
eet
the
abov
e st
anda
rds.
The
mos
t co
mm
on
erro
rs a
re t
hat
the
CV:
• is
out
of
date
• w
as w
ritt
en t
o ap
ply
for
a jo
b an
d is
wor
ded
inap
prop
riat
ely
• do
es n
ot p
rovi
de s
uffic
ient
info
rmat
ion
• is
not
in a
sui
tabl
e st
ruct
ure
• ha
s in
form
atio
n th
at d
oes
not
mat
ch t
he e
mpl
oym
ent
lett
ers
that
you
sub
mit
(for
exa
mpl
e, p
ost
date
s, job
titl
es,
hosp
ital
nam
es,
or s
uper
visi
ng c
onsu
ltant
s do
not
mat
ch)
• do
es n
ot in
clud
e a
brie
f jo
b de
scri
ptio
n un
der
each
pos
t he
ld
• ha
s in
form
atio
n th
at d
oes
not
mat
ch t
he a
pplic
atio
n fo
rm.
4

Gui
danc
e on
sel
ectin
g re
fere
es
This
pag
e h
elp
s ap
plic
ants
to
cho
ose
refe
rees
wh
o w
ill g
ive
stru
ctu
red
rep
orts
in
su
pp
ort
of
thei
r ap
pli
cati
on f
or e
ntr
y o
nto
th
e S
pec
ialis
t or
GP
Reg
iste
r w
ith
a C
ES
R
or C
EGP
R.
You
mus
t gi
ve t
he n
ames
and
det
ails
of
six
refe
rees
who
we
can
cont
act
to a
sk f
or
stru
ctur
ed r
epor
ts.
App
licat
ions
whe
re w
e do
not
rec
eive
at
leas
t fiv
e st
ruct
ured
rep
orts
tha
t m
eet
the
requ
irem
ents
bel
ow a
re n
ot li
kely
to
be s
ucce
ssfu
l.
Plea
se m
ake
sure
whe
n no
min
atin
g yo
ur r
efer
ees
that
:
• yo
u ha
ve t
heir a
ppro
val b
efor
e su
bmitt
ing
your
app
licat
ion
• th
ey a
re w
illin
g to
com
plet
e a
stru
ctur
ed r
epor
t fo
r yo
u
• yo
u ha
ve m
ade
them
aw
are
of t
he in
form
atio
n th
ey w
ill b
e as
ked
for
• yo
u gi
ve t
hem
a c
opy
of y
our
CV
We
will
nee
d re
port
s fr
om a
t le
ast
five
of y
our
refe
rees
, on
e of
wh
om m
ust
be
you
r fi
rst
refe
ree
(see
'Wh
o to
ch
oose
' bel
ow
).
Bef
ore
you
choo
se y
our
refe
rees
, yo
u sh
ould
rea
d ou
r gu
idan
ce t
o re
fere
es t
o se
e w
hat
we
ask
them
to
do.
Who
to
choo
se
Your
fir
st r
efer
ee s
houl
d be
you
r cu
rren
t m
edic
al d
irec
tor,
div
isio
nal d
irec
tor/
clin
ical
di
rect
or,
or s
omeo
ne o
f eq
uiva
lent
sen
iori
ty –
for
exa
mpl
e, a
sup
erin
tend
ent
if yo
u ar
e ov
erse
as.
Your
oth
er r
efer
ees
• A
t le
ast
two
of y
our
refe
rees
sho
uld
be d
octo
rs in
the
spe
cial
ty y
ou a
re a
pply
ing
for,
or
a c
lose
ly-r
elat
ed s
peci
alty
.
• If
you
hav
e un
dert
aken
Sp
ecia
lty
or G
P t
rain
ing
, on
e of
the
str
uctu
red
repo
rts
shou
ld b
e fr
om y
our
mos
t re
cent
pro
gram
me
dire
ctor
, re
gion
al s
peci
alty
adv
iser
or
educ
atio
nal s
uper
viso
r.
•
All
of y
our
refe
rees
sho
uld
eith
er b
e on
the
Spe
cial
ist
or G
P Reg
iste
r or
be
of
equi
vale
nt s
tand
ing
• And
the
y sh
ould
be
able
to
com
men
t fr
om t
heir o
wn
dire
ct o
bser
vatio
ns o
n yo
ur
curr
ent
leve
l of
expe
rtis
e.
5

Plea
se b
ear
in m
ind
– re
fere
es w
ho h
ave
retir
ed f
rom
pra
ctic
e m
ore
than
thr
ee y
ears
ago
m
ay n
ot b
e ab
le t
o co
mm
ent
on y
our
curr
ent
skill
s.
If y
ou a
re u
nabl
e to
arr
ange
for
the
nec
essa
ry r
efer
ees,
you
are
str
ongl
y re
com
men
ded
to
dela
y yo
ur a
pplic
atio
n un
til y
ou a
re a
ble
to d
o so
.
Perio
d of
ref
eren
ce
Whe
re p
ossi
ble,
you
sho
uld
nom
inat
e re
fere
es w
ho c
an c
omm
ent
auth
orita
tivel
y fr
om t
heir
own
dire
ct o
bser
vatio
n on
the
last
fiv
e ye
ars
of y
our
prac
tice.
How
ever
, w
e ac
cept
tha
t th
ere
may
be
reas
ons
(suc
h as
a c
aree
r br
eak)
for
you
to
nam
e so
me
refe
rees
fro
m a
n ea
rlie
r pe
riod
.
How
we
will
con
tact
you
r re
fere
es
GM
C r
egis
tere
d r
efer
ees
You
shou
ld g
ive
us t
he G
MC n
umbe
r of
eac
h re
fere
e w
ho is
reg
iste
red
with
the
GM
C.
We
will
on
ly c
onta
ct t
hem
usi
ng t
he c
onta
ct d
etai
ls w
e ha
ve o
n re
cord
for
the
m.
Bef
ore
you
subm
it yo
ur a
pplic
atio
n, y
ou s
houl
d as
k yo
ur r
efer
ee t
o m
ake
sure
the
ir c
onta
ct
deta
ils a
re u
p to
dat
e. T
hey
can
chan
ge t
heir d
etai
ls t
hrou
gh t
heir G
MC O
nlin
e ac
coun
t, o
r by
ph
onin
g us
.
We
will
usu
ally
con
tact
ref
eree
s by
em
ail.
If y
our
refe
ree
does
not
hav
e an
em
ail a
ddre
ss
regi
ster
ed w
ith u
s, w
e w
ill c
onta
ct t
hem
by
post
inst
ead.
Non
-GM
C r
egis
tere
d r
efer
ees
If y
our
refe
ree
has
neve
r be
en r
egis
tere
d w
ith u
s, p
leas
e gi
ve t
heir e
mai
l add
ress
. W
hen
we
rece
ive
thei
r re
port
we
will
car
ry o
ut c
heck
s to
ver
ify it
.
6

Stru
ctur
ed R
epor
t For
m
A
pplic
atio
n fo
r ent
ry o
nto
the
Spec
ialis
t Reg
iste
r thr
ough
spe
cial
ty e
quiv
alen
ce
Why
you
hav
e be
en s
ent t
his
form
Yo
ur n
ame
and
cont
act d
etai
ls h
ave
been
giv
en b
y th
e do
ctor
nam
ed o
n pa
ge tw
o of
this
form
, to
act a
s a
refe
ree
to p
rovi
de a
stru
ctur
ed re
port
as p
art o
f the
ir ap
plic
atio
n to
the
GM
C fo
r ent
ry o
nto
the
Spec
ialis
t Reg
iste
r thr
ough
spe
cial
ty e
quiv
alen
ce.
The
appl
ican
t has
app
lied
in th
e sp
ecia
lty s
how
n on
the
form
. Thi
s ap
plic
atio
n ro
ute
requ
ires
appl
ican
ts to
dem
onst
rate
to u
s th
roug
h th
e do
cum
enta
ry e
vide
nce
that
they
pro
vide
, tha
t the
ir tra
inin
g, q
ualif
icat
ions
and
exp
erie
nce,
whe
reve
r obt
aine
d, a
re e
quiv
alen
t to
the
curri
culu
m
requ
irem
ents
for t
he a
war
d of
a C
ertif
icat
e of
Com
plet
ion
of T
rain
ing
(CC
T) in
the
spec
ialty
in
whi
ch th
ey a
re a
pply
ing.
If th
e ap
plic
ant i
s ap
plyi
ng in
a s
peci
alty
whi
ch is
not
app
rove
d fo
r the
aw
ard
of a
CC
T th
ey w
ill ne
ed to
dem
onst
rate
that
thei
r tra
inin
g or
qua
lific
atio
ns fr
om o
utsi
de th
e U
K to
geth
er w
ith th
eir e
xper
ienc
e w
here
ver o
btai
ned
in a
non
-CC
T sp
ecia
lty a
re e
quiv
alen
t to
the
know
ledg
e an
d sk
ill co
nsis
tent
with
pra
ctic
e as
a c
onsu
ltant
in a
ny o
f the
UK
heal
th s
ervi
ces.
If
you
are
not s
ure
if th
e sp
ecia
lty is
one
in w
hich
the
GM
C is
sue
a C
CT,
then
ple
ase
refe
r to
the
web
lin
k to
the
appr
oved
cur
ricul
a.
Ple
ase
com
plet
e al
l sec
tions
of t
he re
port
form
. If,
und
er a
ny o
f the
hea
ding
s, y
ou d
o no
t hav
e di
rect
kno
wle
dge
of th
e ap
plic
ant p
leas
e en
ter ‘
No
dire
ct k
now
ledg
e’ in
that
sec
tion,
unl
ess
you
are
a m
edic
al d
irect
or w
hen
you
wou
ld n
eed
to
cons
ult w
ith y
our c
olle
ague
s be
fore
com
plet
ing
the
form
and
use
the
know
ledg
e yo
u ha
ve o
f the
ap
plic
ant’s
invo
lvem
ent i
n de
partm
enta
l act
ivity
. Oth
er re
fere
es m
ay b
e ab
le to
com
men
t on
thes
e as
pect
s.
To a
ssis
t you
in c
ompl
etin
g th
is s
truct
ured
repo
rt yo
u sh
ould
refe
r to
the
follo
win
g:
1.
Th
e cu
rrent
nea
rest
CC
T cu
rricu
lum
to th
e sp
ecia
lty th
e ap
plic
ant i
s ap
plyi
ng in
. w
ww
.gm
c-uk
.org
/edu
catio
n/po
stgr
adua
te/a
ppro
ved_
curri
cula
_sys
tem
s.as
p
2.
The
spec
ialty
spe
cific
gui
danc
e on
evi
denc
e to
be
supp
lied
for t
he n
eare
st s
peci
alty
to th
e on
e th
e ap
plic
ant i
s ap
plyi
ng in
. w
ww
.gm
c-uk
.org
/doc
tors
/regi
stra
tion_
appl
icat
ions
/ssg
.asp
3.
G
uida
nce
for r
efer
ees
ww
w.g
mc-
uk.o
rg/d
octo
rs/re
gist
ratio
n_ap
plic
atio
ns/re
fere
e_gu
idan
ce.a
sp
Th
ank
you
for y
our c
oope
ratio
n.
7

Stru
ctur
ed R
epor
t for
spe
cial
ty e
quiv
alen
ce
1. T
he a
pplic
ant
Nam
e of
app
lican
t
Dr X
YZ
GM
C re
fere
nce
num
ber
1234
567
Spec
ialty
of a
pplic
ant
Gen
eral
psy
chia
try
Ref
eree
det
ails
D
r AB
C
8

2. Y
our c
rede
ntia
ls
If yo
u ar
e re
turn
ing
this
form
by
post
, the
offi
cial
hos
pita
l/uni
vers
ity/in
stitu
te s
tam
p m
ust b
e st
ampe
d ov
er th
is s
ectio
n an
d ev
ery
page
of t
his
repo
rt.
If yo
u do
not
hav
e an
offi
cial
sta
mp
plea
se s
ubm
it th
is re
port
unde
r cov
er o
f a le
tter
on h
eade
d pa
per f
rom
you
r hos
pita
l/uni
vers
ity/in
stitu
te.
You
do n
ot n
eed
to s
tam
p th
is fo
rm if
it is
bei
ng re
turn
ed b
y em
ail
Stam
p
Plea
se s
tate
•
Your
spe
cial
ty, q
ualif
icat
ions
, cur
rent
pos
ition
and
pla
ce o
f wor
k;
• Yo
ur p
ositi
on a
nd p
lace
of w
ork
whe
n th
e ap
plic
ant w
as w
orki
ng w
ith y
ou;
•
Your
rela
tions
hip
to th
e ap
plic
ant f
or e
xam
ple
supe
rvis
or to
trai
nee,
col
leag
ue to
col
leag
ue, M
edic
al
Dire
ctor
to s
peci
alis
t.
3. K
now
ledg
e, s
kills
and
per
form
ance
(Dom
ain
1)
3a) L
evel
and
mai
nten
ance
of p
rofe
ssio
nal p
erfo
rman
ce. P
leas
e lis
t bel
ow th
e ap
plic
ant’s
pos
t(s) t
o w
hich
this
re
port
appl
ies
givi
ng fo
r eac
h po
st li
sted
:
• Th
e tit
le o
f eac
h po
st
• N
ame
of th
e ho
spita
l/ins
titut
e
• St
art a
nd e
nd d
ates
•
A de
scrip
tion
of th
e ap
plic
ant’s
role
and
leve
l of r
espo
nsib
ility
(bot
h cl
inic
al a
nd m
anag
eria
l if a
pplic
able
).
3b
) If y
ou th
ink
the
appl
ican
t has
the
full
rang
e, d
epth
, bre
adth
of e
xper
ienc
e an
d sk
ills to
thos
e re
quire
d by
the
CC
T cu
rric
ulum
(if a
pply
ing
in a
CC
T sp
ecia
lty) o
r a s
ubst
antiv
e co
nsul
tant
in a
ny o
f the
UK
Hea
lth S
ervi
ces
(if
appl
ying
in a
non
CC
T sp
ecia
lty),
plea
se li
st fr
om y
our d
irect
obs
erva
tion
how
the
appl
ican
t dem
onst
rate
d th
ese
and
wha
t evi
denc
e w
as a
vaila
ble.
If
you
do n
ot th
ink
the
appl
ican
t has
the
full
rang
e, d
epth
, bre
adth
of e
xper
ienc
e an
d sk
ills re
quire
d, p
leas
e lis
t:
• Th
e sk
ills a
nd c
ompe
tenc
ies
not c
over
ed in
the
abov
e po
sts
• Th
e sp
ecia
lty a
reas
whe
re y
ou h
ave
not o
bser
ved
or h
ave
no d
irect
kno
wle
dge
of th
e ap
plic
ant;
or
• W
here
the
appl
ican
t did
not
dem
onst
rate
the
appr
opria
te d
epth
and
bre
adth
of s
kills
and
com
pete
ncie
s.
9

3c) P
leas
e ex
plai
n w
heth
er th
e ap
plic
ant h
as d
emon
stra
ted
appl
icat
ion
of k
now
ledg
e an
d ex
perie
nce
to p
ract
ise
(for e
xam
ple
reco
gnis
ing
and
wor
king
with
in th
e lim
its o
f the
ir co
mpe
tenc
e). I
n pa
rticu
lar,
how
they
:
• Ke
ep u
p to
dat
e w
ith C
ontin
uous
Pro
fess
iona
l Dev
elop
men
t (C
PD)
• Ap
ply
the
skills
and
atti
tude
s of
a c
ompe
tent
teac
her/t
rain
er
• M
ake
appr
opria
te re
ferr
als
to c
olle
ague
s an
d ke
ep c
lear
and
legi
ble
reco
rds?
If so
giv
e ex
ampl
es fr
om y
our d
irect
obs
erva
tion
of w
orki
ng w
ith th
e ap
plic
ant.
4.
Saf
ety
and
qual
ity (D
omai
n 2)
4a) H
as th
e ap
plic
ant p
ut in
to e
ffect
sys
tem
s to
pro
tect
pat
ient
s an
d im
prov
e ca
re (f
or e
xam
ple
by ta
king
par
t and
re
spon
ding
to th
e ou
tcom
e of
aud
it, a
ppra
isal
s, p
erfo
rman
ce re
view
s, ri
sk m
anag
emen
t and
clin
ical
gov
erna
nce
proc
edur
es, a
nd re
porti
ng a
dver
se d
rug
reac
tions
or c
once
rns
abou
t ris
ks to
pat
ient
s)?
If
so, p
leas
e ex
plai
n ho
w th
e ap
plic
ant h
as d
emon
stra
ted
this
and
giv
e ex
ampl
es fr
om y
our d
irect
obs
erva
tion
of
wor
king
with
the
appl
ican
t.
4b
) Doe
s th
e ap
plic
ant m
onito
r and
resp
ond
to ri
sks
to s
afet
y an
d sa
fegu
ard
and
prot
ect t
he h
ealth
and
wel
lbei
ng
of v
ulne
rabl
e pe
ople
(for
exa
mpl
e re
spon
ding
to ri
sks
pose
d by
pat
ient
s an
d fo
llow
ing
infe
ctio
n co
ntro
l pr
oced
ures
)?
If so
giv
e ex
ampl
es fr
om y
our d
irect
obs
erva
tion
of w
orki
ng w
ith th
e ap
plic
ant.
10

4c) H
as th
e ap
plic
ant p
rote
cted
pat
ient
s an
d co
lleag
ues
from
any
risk
pos
ed b
y th
eir h
ealth
?
If yo
u ar
e aw
are
of a
ny re
leva
nt c
ircum
stan
ces,
ple
ase
expl
ain
whe
ther
the
appl
ican
t has
dem
onst
rate
d th
is. I
f so
give
exa
mpl
es fr
om y
our d
irect
obs
erva
tion
of w
orki
ng w
ith th
e ap
plic
ant.
5.
Com
mun
icat
ions
, par
tner
ship
and
team
wor
king
(Dom
ain
3)
5a)
Doe
s th
e ap
plic
ant c
omm
unic
ate
effe
ctiv
ely
with
pat
ient
s (fo
r exa
mpl
e ke
epin
g th
em in
form
ed a
bout
pro
gres
s of
thei
r car
e) a
nd c
olle
ague
s in
clin
ical
and
man
agem
ent s
ituat
ions
with
in a
nd o
utsi
de th
e te
am (f
or e
xam
ple
pass
ing
on in
form
atio
n w
hen
patie
nts
trans
fer,
enco
urag
ing
colle
ague
s to
con
tribu
te to
dis
cuss
ions
)?
Pl
ease
exp
lain
whe
ther
the
appl
ican
t has
dem
onst
rate
d th
is. I
f so
give
exa
mpl
es fr
om y
our d
irect
obs
erva
tion
of
wor
king
with
the
appl
ican
t.
5b
) Doe
s th
e ap
plic
ant w
ork
cons
truct
ivel
y w
ith c
olle
ague
s by
sup
porti
ng th
em, d
eleg
atin
g ef
fect
ivel
y, a
ctin
g as
a
posi
tive
role
mod
el a
nd p
rovi
ding
effe
ctiv
e le
ader
ship
?
Plea
se e
xpla
in w
heth
er th
e ap
plic
ant h
as d
emon
stra
ted
this
. If s
o gi
ve e
xam
ples
from
you
r dire
ct o
bser
vatio
n of
w
orki
ng w
ith th
e ap
plic
ant.
11

5c) D
oes
the
appl
ican
t est
ablis
h an
d m
aint
ain
partn
ersh
ips
with
pat
ient
s, e
ncou
rage
them
to ta
ke a
n in
tere
st in
th
eir h
ealth
and
obt
ain
appr
opria
te c
onse
nt fo
r tre
atm
ent?
Pl
ease
exp
lain
whe
ther
the
appl
ican
t has
dem
onst
rate
d th
is. I
f so
give
exa
mpl
es fr
om y
our d
irect
obs
erva
tion
of
wor
king
with
the
appl
ican
t.
6.
Mai
ntai
ning
trus
t (D
omai
n 4)
6a
) Doe
s th
e ap
plic
ant s
how
resp
ect f
or p
atie
nts
(for e
xam
ple
is p
olite
, con
side
rate
and
hon
est w
ith p
atie
nts
and
impl
emen
ts s
yste
ms
to p
rote
ct p
atie
nt c
onfid
entia
lity)
?
Plea
se e
xpla
in w
heth
er th
e ap
plic
ant h
as d
emon
stra
ted
this
. If s
o gi
ve e
xam
ples
from
you
r dire
ct o
bser
vatio
n of
w
orki
ng w
ith th
e ap
plic
ant.
6b
) H
as th
e ap
plic
ant t
reat
ed p
atie
nts
and
colle
ague
s fa
irly
and
with
out d
iscr
imin
atio
n (fo
r exa
mpl
e be
ing
hone
st
and
obje
ctiv
e w
hen
appr
aisi
ng o
r ass
essi
ng c
olle
ague
s, w
ritin
g re
fere
nces
, giv
ing
cons
truct
ive
feed
back
, rai
sing
is
sues
of c
olle
ague
s’ p
erfo
rman
ce a
nd re
spon
ding
pro
mpt
ly to
com
plai
nts)
?
Plea
se e
xpla
in w
heth
er th
e ap
plic
ant h
as d
emon
stra
ted
this
. If s
o gi
ve e
xam
ples
from
you
r dire
ct o
bser
vatio
n of
w
orki
ng w
ith th
e ap
plic
ant.
12

6c) H
as th
e ap
plic
ant a
cted
with
hon
esty
and
inte
grity
(for
exa
mpl
e be
ing
hone
st a
nd a
ccur
ate
in a
ny fi
nanc
ial
deal
ings
, pra
ctic
e re
ports
, and
obt
aini
ng a
ppro
pria
te e
thic
al a
ppro
val f
or re
sear
ch p
roje
cts)
?
Plea
se e
xpla
in w
heth
er th
e ap
plic
ant h
as d
emon
stra
ted
this
. If s
o gi
ve e
xam
ples
from
you
r dire
ct o
bser
vatio
n of
w
orki
ng w
ith th
e ap
plic
ant.
7.
Any
furt
her c
omm
ents
7a)
If yo
u ar
e fa
milia
r with
the
UK
med
ical
regi
stra
tion
syst
em, w
ould
you
sup
port
this
app
lican
t for
app
rova
l for
en
try o
nto
the
Spe
cial
ist R
egis
ter?
If
you
wou
ld s
uppo
rt ap
prov
al fo
r ent
ry o
nto
the
Spe
cial
ist R
egis
ter,
wou
ld y
ou e
mpl
oy th
is d
octo
r as
a co
nsul
tant
in
any
of t
he U
K he
alth
ser
vice
s?
If yo
u w
ould
not
sup
port
this
app
lican
t for
app
rova
l of e
ntry
ont
o th
e S
peci
alis
t Reg
iste
r or w
ould
not
em
ploy
this
ap
plic
ant a
s a
cons
ulta
nt, p
leas
e st
ate
why
. If
you
are
awar
e of
any
dis
cipl
inar
y is
sues
ple
ase
give
det
ails
bel
ow.
Plea
se a
lso
add
any
furth
er c
omm
ents
you
wis
h to
mak
e ab
out t
his
indi
vidu
al’s
app
licat
ion
to th
e G
MC
.
13

8. Y
our d
ecla
ratio
n
I dec
lare
that
the
info
rmat
ion
I hav
e gi
ven
on th
is s
truct
ured
repo
rt is
true
and
acc
urat
e to
the
best
of m
y kn
owle
dge.
I un
ders
tand
that
it w
ill be
use
d by
the
GM
C, a
nd a
ny re
leva
nt th
ird p
arty
the
GM
C in
volv
es in
an
eval
uatio
n of
this
doc
tor’s
app
licat
ion,
as
part
of th
e ev
iden
ce fo
r mak
ing
a de
cisi
on o
n w
heth
er th
e ap
plic
ant i
s el
igib
le fo
r ent
ry o
nto
the
GM
C’s
Spe
cial
ist R
egis
ter.
I und
erst
and
that
this
stru
ctur
ed re
port
may
be
rele
ased
to th
e ap
plic
ant i
f the
y re
ques
t a c
opy
or it
form
s pa
rt of
th
e do
cum
enta
ry e
vide
nce
in re
latio
n to
an
appe
al b
y th
e ap
plic
ant a
gain
st a
dec
isio
n of
the
GM
C.
Plea
se re
turn
the
form
to u
s as
soo
n as
pos
sibl
e, b
ut n
o la
ter t
han
21 d
ays
from
«G
MC
_DAT
E_X»
, to:
equi
vale
nce@
gmc-
uk.o
rg
If yo
u re
turn
the
form
from
an
emai
l add
ress
that
you
hav
e no
t reg
iste
red
with
the
GM
C w
e m
ay m
ake
enqu
iries
to
con
firm
the
repo
rt ha
s co
me
from
the
refe
ree.
Al
tern
ativ
ely,
if y
ou d
o no
t hav
e ac
cess
to e
mai
l ple
ase
sign
and
dat
e an
d co
mpl
ete
sect
ion
2 of
the
form
and
re
turn
it to
us
at:
Gen
eral
Med
ical
Cou
ncil
Spec
ialis
t App
licat
ions
Tea
m
3 H
ardm
an S
treet
, M
anch
este
r M
3 3A
W
Plea
se n
ote
if yo
u ar
e re
turn
ing
the
stru
ctur
ed re
port
by
post
ple
ase
sign
and
dat
e in
the
spac
e pr
ovid
ed. I
f you
are
retu
rnin
g th
e st
ruct
ured
repo
rt b
y em
ail t
hen
plea
se d
ate
and
eith
er in
sert
an
elec
tron
ic s
igna
ture
or s
impl
y ty
pe y
our n
ame
into
the
sign
atur
e fie
ld b
elow
.
Nam
e:
Sign
atur
e:
(onl
y if
send
ing
a pa
per c
opy)
Dat
e:
14

Impo
rtan
t no
tice
abou
t ev
iden
ce in
sup
port
of
spec
ialty
equ
ival
ence
app
licat
ions
Your
app
licat
ion
will
be
supp
orte
d by
a la
rge
amou
nt o
f ev
iden
ce.
The
GM
C a
nd t
he R
oyal
Col
lege
or
Facu
lty m
ust
be c
erta
in t
hat
the
evid
ence
you
pro
vide
is a
tru
e an
d ac
cura
te
refle
ctio
n of
you
r tr
aini
ng a
nd e
xper
ienc
e.
We
do n
ot a
ccep
t or
igin
al d
ocum
ents
, on
ly c
opie
s. T
hrou
gh a
uthe
ntic
atio
n an
d va
lidat
ion
we
can
be s
atis
fied
that
the
se c
opie
s ar
e ge
nuin
e.
We
also
nee
d to
be
assu
red
of p
atie
nt c
onfid
entia
lity
and
ther
efor
e do
not
acc
ept
docu
men
ts
feat
urin
g de
tails
of
patie
nts
or c
olle
ague
s th
at h
ave
not
been
ano
nym
ised
.
Plea
se m
ake
sure
you
rea
d an
d co
mpl
y w
ith t
he g
uida
nce
belo
w w
hen
com
pilin
g yo
ur
evid
ence
.
Plea
se n
ote
that
all
evid
ence
sho
uld
be s
ubm
itted
sin
gle
side
d on
A4
pape
r. T
his
is s
o it
can
be s
cann
ed a
nd s
ent
elec
tron
ical
ly t
o th
e Roy
al C
olle
ge o
r Fa
culty
. Yo
ur a
pplic
atio
n m
ay b
e de
laye
d if
it is
not
on
A4
pape
r, o
r if
it is
dou
ble
side
d.
Auth
entic
atio
n
Evid
ence
of
regi
stra
tion
with
ano
ther
med
ical
reg
ulat
or o
r qu
alifi
catio
ns o
btai
ned
outs
ide
the
UK m
ust
be a
uthe
ntic
ated
by
the
awar
ding
bod
y, o
r by
a s
olic
itor.
This
mea
ns t
hat
the
awar
ding
bod
y, o
r so
licito
r, m
ust
stam
p, s
ign
and
date
a c
op
y of
the
qu
alifi
catio
n or
reg
istr
atio
n to
con
firm
tha
t it
is g
enui
ne,
whe
n th
ey v
iew
it a
long
side
the
or
igin
al.
Suc
h co
pies
are
som
etim
es k
now
n as
cer
tifie
d co
pies
.
We
will
not
sub
mit
evid
ence
to
the
Roy
al C
olle
ge f
or a
sses
smen
t un
less
it h
as b
een
corr
ectly
au
then
ticat
ed.
Any
evi
denc
e no
t co
rrec
tly a
uthe
ntic
ated
will
be
retu
rned
to
you.
Valid
atio
n
Each
pag
e of
eve
ry p
iece
of
evid
ence
tha
t sh
ows
your
tra
inin
g an
d ex
peri
ence
his
tory
mus
t be
val
idat
ed.
Plea
se e
nsur
e th
at a
ll do
cum
enta
ry e
vide
nce
you
subm
it is
spe
cific
to
you
and
cont
ains
you
r na
me.
Whe
re p
ossi
ble,
it s
houl
d co
ntai
n th
e na
me
of t
he h
ospi
tal i
t re
late
s to
an
d be
dat
ed t
o sa
y w
hen
the
trai
ning
/exp
erie
nce
took
pla
ce.
Who
can
val
idat
e ev
iden
ce fo
r you
?
15

Trai
ning
and
exp
erie
nce
evid
ence
mus
t be
val
idat
ed b
y so
meo
ne in
a m
edic
al s
uper
viso
ry
posi
tion
at t
he h
ospi
tal w
here
the
tra
inin
g or
exp
erie
nce
took
pla
ce.
They
mus
t be
abl
e to
co
nfirm
tha
t it
is a
tru
e an
d ac
cura
te r
ecor
d.
Val
idat
ion
of t
rain
ing
and
expe
rien
ce e
vide
nce
can
not
be d
one
by a
sol
icito
r. T
his
is b
ecau
se
they
do
not
have
the
med
ical
exp
ertis
e to
ver
ify t
he in
form
atio
n is
a t
rue
and
accu
rate
rec
ord
of y
our
clin
ical
act
iviti
es.
Wha
t doe
s va
lidat
ion
mea
n?
Each
pag
e m
ust
show
:
• Th
e ho
spita
l sta
mp
whe
re t
he t
rain
ing
or e
xper
ienc
e to
ok p
lace
.
• Th
e na
me
of t
he p
erso
n si
gnin
g th
e do
cum
ent
– pr
inte
d an
d in
ful
l
• Th
e po
sitio
n of
the
per
son
sign
ing
the
docu
men
t –
prin
ted
and
in f
ull
• Th
e or
igin
al s
igna
ture
of
the
pers
on v
alid
atin
g th
e do
cum
ent.
It is
impo
rtan
t th
at t
he c
opy
of t
he e
vide
nce
mus
t co
ntai
n th
e o
rig
inal
sig
natu
re o
f th
e pe
rson
val
idat
ing
the
evid
ence
. Pl
ease
do
not
send
a p
hoto
copy
of
the
valid
ator
’s s
igna
ture
. W
e m
ay w
ant
to c
onta
ct t
his
pers
on,
so y
ou m
ust
ensu
re t
heir n
ame
and
posi
tion
is c
lear
. An
exam
ple
may
look
like
thi
s:
Whe
re a
doc
umen
t ha
s m
ultip
le p
ages
, th
e fir
st p
age
and
any
cons
olid
atio
n sh
eets
mus
t sh
ow
the
stam
p, s
igna
ture
, na
me
and
job
title
as
desc
ribe
d ab
ove.
The
y m
ust
also
sho
w t
he
num
ber
of p
ages
the
doc
umen
t co
ntai
ns.
Any
pag
es t
here
afte
r m
ay s
impl
y sh
ow t
he s
tam
p an
d si
gnat
ure.
So
as a
n ex
ampl
e, if
a lo
g bo
ok h
as 9
8 pa
ges,
the
per
son
valid
atin
g th
e lo
g bo
ok w
ould
sta
mp,
con
firm
the
ir n
ame
and
posi
tion,
and
sig
n th
e fr
ont
page
. Th
ey w
ould
als
o
16

mak
e a
stat
emen
t su
ch a
s “I
con
firm
I h
ave
valid
ated
thi
s an
d th
e fo
llow
ing
97 p
ages
of
this
lo
g bo
ok”.
The
y sh
ould
the
n st
amp
and
sign
the
fol
low
ing
page
s. T
heir n
ame
and
posi
tion
wou
ld n
ot b
e ne
cess
ary.
Onl
ine
e-po
rtfo
lios
also
nee
d to
be
valid
ated
in li
ne w
ith t
his
guid
ance
.
Lette
rs
All
lett
ers
you
subm
it as
evi
denc
e m
ust
be p
rovi
ded
on le
tter
hea
ded
pape
r an
d be
sig
ned
by
the
send
er.
An
elec
tron
ic s
igna
ture
is n
ot a
ccep
tabl
e. A
n or
igin
al in
k si
gnat
ure
is r
equi
red.
If
you
send
the
ori
gina
l, it
does
not
hav
e to
be
valid
ated
. H
owev
er,
phot
ocop
ies
of o
rigi
nal
lett
ers
mus
t be
val
idat
ed in
line
with
the
gui
danc
e ab
ove.
We
will
not
acc
ept
pape
rwor
k th
at:
• is
not
val
idat
ed
• do
es n
ot m
ake
any
spec
ific
refe
renc
e to
you
.
We
will
not
sub
mit
evid
ence
to
the
Roy
al C
olle
ge f
or a
sses
smen
t un
less
it h
as b
een
corr
ectly
va
lidat
ed.
Any
evi
denc
e no
t co
rrec
tly v
alid
ated
will
be
retu
rned
to
you.
Patie
nt o
r col
leag
ue c
onfid
entia
lity
Whe
n su
bmitt
ing
your
evi
denc
e, y
ou s
houl
d al
so r
emem
ber
your
res
pons
ibili
ties
and
com
mitm
ents
und
er G
ood
med
ical
pra
ctic
e (G
MP)
. D
omai
n 4
of G
MP
and
your
CES
R
appl
icat
ion
is a
bout
mai
ntai
ning
tru
st.
With
reg
ards
to
com
mun
icat
ing
info
rmat
ion,
GM
P st
ates
:
“Whe
n co
mm
unic
atin
g pu
blic
ly,
incl
udin
g sp
eaki
ng t
o or
wri
ting
in t
he m
edia
, yo
u m
ust
mai
ntai
n pa
tient
con
fiden
tialit
y. Y
ou s
houl
d re
mem
ber
whe
n us
ing
soci
al m
edia
tha
t co
mm
unic
atio
ns in
tend
ed f
or f
rien
ds o
r fa
mily
may
bec
ome
mor
e w
idel
y av
aila
ble.
”
Wha
t th
is m
eans
for
you
r ap
plic
atio
n is
tha
t al
l ide
ntifi
able
pat
ient
info
rmat
ion
MU
ST
be
anon
ymis
ed b
efor
e yo
u se
nd it
to
us.
You
shou
ld a
lso
excl
ude
the
pers
onal
dat
a of
col
leag
ues
or t
rain
ees
whi
ch is
not
alrea
dy in
the
pub
lic d
omai
n, s
uch
as t
heir a
ppra
isal
s.
Iden
tifia
ble
pers
onal
dat
a m
akes
it p
ossi
ble
for
som
eone
to
iden
tify
the
subj
ect
of t
he
info
rmat
ion.
In
cert
ain
inst
ance
s, s
ome
info
rmat
ion
will
be
help
ful t
o th
e ev
alua
tors
. Fo
r ex
ampl
e th
e ge
nder
and
/or
year
and
mon
th s
omeo
ne w
as b
orn
may
hel
p id
entif
y th
at y
ou
have
und
erta
ken
a pr
oced
ure
on a
ran
ge o
f pe
ople
. Add
ress
es a
nd f
ull n
ames
sho
uld
alw
ays
be r
emov
ed.
Whe
n yo
u re
mov
e th
is d
ata
you
shou
ld b
e aw
are
that
cer
tain
ink
may
ble
ed t
hrou
gh a
m
arke
r pe
n w
hen
we
scan
you
r ev
iden
ce.
This
usu
ally
hap
pens
whe
n a
lase
r pr
inte
r ha
s be
en
used
. W
e w
ould
sug
gest
you
use
a c
rayo
n or
red
actio
n so
ftw
are
inst
ead
of a
mar
ker
pen
as
this
ens
ures
info
rmat
ion
rem
ains
ano
nym
ised
thr
ough
our
sca
n pr
oces
s.
17

If w
e re
ceiv
e ev
iden
ce w
hich
has
iden
tifia
ble
pers
onal
info
rmat
ion,
we
will
ret
urn
it to
you
an
d re
ques
t th
at y
ou r
emov
e th
e da
ta.
The
rele
vant
Roy
al C
olle
ge o
r Fa
culty
will
be
mad
e aw
are
that
you
r or
igin
al e
vide
nce
incl
uded
som
e pe
rson
al d
ata.
If
you
subm
it fu
rthe
r ev
iden
ce w
hich
has
not
bee
n an
onym
ised
cor
rect
ly a
t th
e po
int
we
are
read
y to
sen
d yo
ur
appl
icat
ion
to t
he R
oyal
Col
lege
or
Facu
lty f
or e
valu
atio
n, w
e w
ill e
xclu
de t
hese
doc
umen
ts
and
retu
rn t
hem
to
you.
We
will
not
ano
nym
ise
any
data
on
your
beh
alf.
It
is y
our
resp
onsi
bilit
y to
ens
ure
you
are
wor
king
in li
ne w
ith t
he G
ood
med
ical
pra
ctic
e fr
amew
ork.
You
the
refo
re s
houl
d be
abl
e to
de
mon
stra
te y
our
com
mitm
ent
to im
plem
entin
g sy
stem
s to
pro
tect
pat
ient
con
fiden
tialit
y.
Failu
re t
o co
mpl
y w
ith t
hese
req
uire
men
ts m
ay c
onst
itute
a b
reac
h of
the
Dat
a Pr
otec
tion
Act
19
98 a
nd t
he p
atie
nt c
onfid
ential
ity s
tand
ards
in G
ood
med
ical
pra
ctic
e.
You
may
be
refe
rred
to
our
Fitn
ess
to P
ract
ise
Direc
tora
te.
A la
rge
perc
enta
ge o
f th
e ap
plic
atio
ns w
e re
ceiv
e fo
r th
e fir
st t
ime
are
not
righ
t an
d w
e ha
ve
to r
etur
n th
em t
o th
e ap
plic
ant.
The
mos
t co
mm
on p
robl
em w
ith t
he e
vide
nce
subm
itted
is
that
the
doc
umen
ts a
re n
ot a
uthe
ntic
ated
, no
t va
lidat
ed o
r no
t an
onym
ised
. By
follo
win
g th
e gu
idan
ce a
bove
, w
e w
ill b
e ab
le t
o pr
oces
s yo
ur a
pplic
atio
n m
uch
quic
ker.
18

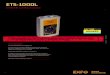
Example checklist
19

Name GMC Number Application ID
Evidence Item Submitted Evidence Status Notes Re-submitted Evidence
All posts since PMQ are listed
Posts held match CV and employment letters
Application FormPending Further
InformationSome of the dates in your application form do not match your employment letters.
Posts held are in reverse chronological order starting with the most recent posts, matching application form and employment letters
CV meets guidance on website: Brief job description, supervisor names present, details of CPD/Presentations/Audit
CVPending Further
Information
CV not accepted. Please see GMC guidance on how to format your CV
Please ensure that for each post you include the dates, written in full, and a description of each role. Please ensure the dates in your CV exactly match those in your online application form and employment letters.
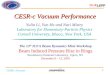
Curriculum version:
CESR (CCT specialty) - Applicant must have completed either a specialist postgraduate qualification or minimum of six months training in the CCT specialty they apply for. Training and/or qualifications can be from anywhere in the world
CESR (non-CCTspecialty) - Applicant must have completed either a specialist postgraduate qualification or minimum of six months specialist training in any non-CCT specialty. The training and/or qualification must be from outside the UK
CESR in CCT Specialty:
Check for minimum requirements:
Link to curriculum that application will be assessed against: Link to Specialty Specific Guidance:
State training post and/or qualification that fulfils minimum requirements or comment to applicant on what is needed to confirm eligibility:
Application Form
CV
20

Evidence Item Submitted Evidence Status Notes Re-submitted Evidence
Primary medical qualification (PMQ)
Not Required
Specialist medical qualification(s)
1. Doctorate cerificatePending Further
Information
1. MD - not accepted as not authenticated. The authenticated copy should be signed, stamped and dated by either a solicitor/public notary or member of staff at the awarding body.
Curriculum or syllabus (if undertaken outside the UK)
1. Curriculum Accepted 1. Curriculum - accepted
Specialist registration outside the UK
1. Validated copy of my Specialist registration
Accepted 1. Specialist registration - accepted.
Honours and prizesPending Further
Information
Do you have any honours or prizes which you could submit in support of your application?
Other relevant qualifications and certificates
1. FRCS 2. Masters degree
Accepted1-2. Qualifications - accepted
Qualifications
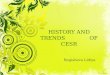
Domain 1 - Knowledge, skills and performance
21

Appraisals and assessments
1. Appraisals 2009 - 2013
2. Learning agreement
3. Work Based assessments (DOPS, DOPS,OSAT)
Pending Further Information
1. Appraisals - not accepted as not fully validated. We require the hospital stamp and full name, job title and signature of the medical supervisor validating the document on each page 2. Learning agreement - accepted3a. 20 x assessments - accepted. 3b. 10 x assessments - not accepted as not fully validated. Where documents are double sided each side must be validated.
Records of In Training Assessment (RITAs), Annual Review of Competency Progress (ARCPs) and other training assessments
Document supplied in appraisal and assessment section
AcceptedCross reference to comments/documents in Appraisals and assessments section.
360° and multi-source feedback
1. 360 degree colleague feedback
Accepted1. 360 feedback - accepted.
Awards and discretionary points letters
Pending Further Information
Do you have any awards and discretionary points letters which you are able to submit in support of your application?
Personal development plans (PDP)
Document supplied in appraisal and assessment section
AcceptedCross reference to evidence and comments in appraisal section.
Participation in assessment, appraisal and appointments process
1. Approved assessor 2. Reviewer for journal
Pending Further Information
1-2. Please can you confirm in which section this evidence has been submitted? Please see SSG for guidance on evidence that can be submitted in this section.
Assessments and Appraisals
22

Logbooks 1. Logbooks x 3 Accepted 1. Logbooks - accepted
Consolidation, cumulative data sheets, summary lists and annual caseload statistics
1. Consolidation sheets x 3 Accepted 1. Consolidation sheets - accepted
Medical reports
1. Letters to GP discussing patient management 2. Case based discussions supplied in the appraisal and assessment section
Pending Further Information
Cross reference to referral letters.
Are you satisfied that you have provided a suitable range of evidence to demonstrate your experience across the breadth and depth of the curriculum?
Case histories
1. Validated clinic letters 2. Case based discussions supplied in appraisal and assessment form
Pending Further Information
Cross reference to referral letters. Cross reference to referral letters.
Are you satisfied that you have provided a suitable range of evidence to demonstrate your experience across the breadth and depth of the curriculum.
Referral letters discussing patient handling
1. Referral lettersPending Further
Information
Although some effort has been made to redact patient data on 3 letters patient names have not been redacted from the body of the text and on all letters patient names and addresses are still visible through he marker pen used. Please ensure all documents are anonymised for patient data.
Logbooks
23

Patient lists1. Ultrasound list for patients 2. Cases seen
Pending Further Information
Cross reference to relevant sections.
Please see SSG for guidance on evidence that can be submitted in this section.
Departmental (or trust) workload and annual caseload statistics
Pending Further Information
Please see SSG for guidance on evidence that can be submitted in this section.
Rotas, timetables and job plans
1. Rotas and timetables2. List of clinical dates
Pending Further Information
1. Rotas and timetables - accepted2. List of clinic dates - not accepted as not validated and there is no reference you by name - please provide a validated copy which clearly states your involvement
Courses relevant to curriculum
1. Microsurgical skill course 2. VR in a day Macular course 3. International uveitis symposium 4. Ultrasound course OCT course
Accepted1. Microsurgical skill courses - accepted. 2-4. 3 x certificates - accepted.
Portfolios (electronic or revalidation)
1. Electronic portfolio on College website
Pending Further Information
Cross reference to relevant sections.
Please note that the evaluators will not have access to your online portfolio and will only be able to evaluate your evidence based on the hard copy evidence which is accepted by the GMC as part of your application.
24

Generic guidance on documents to be supplied in evidence for an application for a Certificate of Eligibility for Specialist Registration (CESR) or a Certificate of Eligibility for GP Registration (CEGPR)
Generic - for applications in all specialties This guidance is to help doctors who are applying for a CESR or a CEGPR. You will also need to read:
the specialty specific guidance for your specialty (or the nearest specialty if you are not applying in a CCT specialty)
the CCT curriculum for your specialty (or the nearest specialty if you are not applying in a CCT specialty).
Please also make sure you have read our online guidance for making your application, including checking which application type you are eligible for in our Certification route finder.
Can I get advice before I submit my application?
You can contact us and ask to speak to the Certification team for advice before you apply. You are strongly advised to contact the Royal College or Faculty for guidance before you submit an application or a reapplication.
Submitting your evidence
Do not submit original documents.
All your copies must be authenticated or validated, and anonymised. You can read an explanation of this in our important notice about evidence.
You will also need to submit translations of any documents that are not in English. Please ensure the translations you submit meet our translation requirements.
How much evidence to submit
This guidance on documents to supply is not exhaustive and you may have alternative evidence. We recognise that you may not have all the evidence listed here and you may wish to delay submitting an application until you are able to gather it.
Your evidence must cover the knowledge, skills and qualifications to demonstrate the required competencies in all of the generic and specialty specific areas of the CCT curriculum for your specialty (or the nearest specialty if you are not applying in a CCT specialty). If evidence is missing from one area of the curriculum for example, then the application may fail.
Please refer to the specialty specific guidance for your specialty (or the nearest specialty if you are not applying in a CCT specialty), as some evidence suggested here may not be relevant to the specialty in which you are applying. The specialty specific guidance will cover evidence key to your specialty.
25

will help us to deal with your application more quickly if you make sure that you send us only evidence that is directly relevant.
Our guidance on compiling your evidence will help you to decide what is relevant and what is not. We recommend that you read it carefully.
Evidence that is more than five years old will be given less weight than more recent evidence, so you may not need to include it. As a general guide, we would usually expect to see between 800 and 1000 pages of evidence.
Types of evidence are divided into four different domains. We recommend that you apportion the evidence you provide with your application as shown in the pie chart.
Domain 1: 75%
Domain 2: 20%
Domains 3 and 4: 5%
It is important to note that you will not be able to compensate for shortfalls in your evidence of training and experience in a particular area of the curriculum by providing extra evidence in other areas.
Unsuccessful applications or poor evidence
It is our experience that applications from doctors are often submitted with inadequate or poor evidence. We strongly recommend that you closely match your experiences against the current curriculum and provide evidence of equivalence across all areas. We also strongly recommended that all your referees should be fully conversant with the current curriculum and able to provide detailed support for your competence across all or most areas.
Evidence breakdown
75%
20% 5%
Domain 1Domain 2Domains 3 and 4
26

Domain 1 - Knowledge, skills and performance
Qualifications Primary medical qualification (PMQ) If you hold full registration with us, you do not need to submit your PMQ as we saw it when we assessed your
application for registration.
If you do not hold registration, please provide an authenticated copy of your PMQ.
Specialist medical qualification(s) Please provide an authenticated copy of any specialist medical qualifications you hold.
For College examinations the College may confirm details of any examinations you have undertaken.
There are no qualifications from outside Europe that enable automatic entry to the Specialist Register in any specialty. An evaluation is made based on an applicants whole career and therefore two applicants with the same qualifications but different training and/or experience may not receive the same decision.
Please list unsuccessful attempts at examinations (where you have not subsequently been successful) in the application form.
Curriculum or syllabus (if undertaken outside the UK) Please provide a validated copy of your curriculum or syllabus.
This should include the requirements of the qualification and must relate to the specialty in which you are applying. The curriculum or syllabus (including assessment methods) must be the one that was in place when you undertook your training.
If a formal curriculum or syllabus (including assessment methods) is not available please provide a letter from the awarding body outlining the content of the training programme or examination.
For qualifications, we will look to evaluate:
where the curriculum covers areas of the CCT curriculum
the complexity of the work undertaken
how examinations are evaluated or quality assured (external assessment).
Specialist registration outside the UK Please provide a validated copy of details of the registration requirements of that authority.
This will demonstrate what is expected of a registrant by that authority and how your application for registration was evaluated.
27

The
Roy
al C
olle
ge o
f Su
rgeo
ns o
f Edi
nbur
gh
The
Roy
al C
olle
ge o
f Su
rgeo
ns o
f Eng
land
T
he R
oyal
Col
lege
of
Phys
icia
ns a
nd S
urge
ons
of G
lasg
ow
Roy
al C
olle
ge o
f Sur
geon
s in
Irel
and
Inte
rcol
legi
ate
Spe
cial
ty E
xam
inat
ion
in G
ener
al S
urge
ry
Siv
akum
ar G
opal
swam
y
We
have
ple
asur
e in
adv
isin
g yo
u th
at t
he P
anel
of
Exa
min
ers
in
Gen
eral
Sur
gery
has
rep
orte
d to
the
Int
erco
lleg
iate
Spe
cial
ty B
oard
an
d th
e Jo
int
Com
mit
tee
on I
nter
coll
egia
te E
xam
inat
ions
tha
t yo
u ha
ve s
ucce
ssfu
lly
met
the
requ
ired
sta
ndar
ds to
Pas
s the
Int
erco
lleg
iate
S
peci
alty
Exa
min
atio
n he
ld o
n
11th S
epte
mbe
r 20
09
CH
AIR
MA
N
/U
H«
*.
V.«
AA
MA
4
INT
ER
CO
LL
EG
IAT
E S
PEC
IAL
TY
BO
AR
D I
N G
EN
ER
AL
SU
RG
ER
Y
4SK
AA
/1
CH
AIR
MA
N
JOIN
T C
OM
MIT
TE
E O
N I
NT
ER
CO
LL
EG
IAT
E E
XA
MIN
AT
ION
S
Inte
rcol
legi
ate
Spec
ialty
Boa
rds
Join
t Com
mit
tee
on I
nter
colle
giat
e E
xam
inat
ions
2 H
ill P
lace
Edi
nbur
gh E
H8
9DS
Tel
: 013
1 66
2 92
22 F
ax: 0
131
662
944
28

Ad
elp
hi
Tra
ns
lati
on
s L
td
Fu
li S
erv
ice
Tra
iwta
tio
n A
gw
ncy
Stu
dio
402
T
he W
ork
sta
tio
n 15
Pa
tern
ost
er
Row
S
he
ffie
ld,
S1
2BX
T
el:
+4
4(0
)11
4 27
2 37
72
Fa
x:+
44
(0)1
14
221
0401
CE
RT
IFIC
AT
E O
F T
RA
NS
LAT
ION
PN
3052
Thi
s do
cum
ent
is t
o ce
rtif
y th
at A
DE
LP
HI
TR
AN
SL
AT
ION
S L
TD
. pro
vide
d th
e fo
llow
ing
serv
ices
for
Dr.
Gop
alsw
amy
Siv
akum
ar:
The
tra
nsla
tion
from
Fre
nch
into
Eng
lish
of a
med
ical
cer
tific
ate
from
the
Uni
vers
ity
of S
tras
bour
g.
Thi
s ta
sk w
as p
erfo
rmed
by
a pr
ofes
sion
al t
rans
lato
r, D
eann
e B
entle
y. T
o th
e be
st o
f th
e tr
ansl
ator
's k
now
ledg
e an
d ab
ility
the
y ha
ve p
rovi
ded
accu
rate
tra
nsla
tions
oft
he
orig
inal
doc
umen
ts.
The
res
ultin
g tr
ansl
atio
ns i
nto
Eng
lish
are
as a
ccur
ate
in m
eani
ng a
s it
is p
ossi
ble
to
mak
e th
em g
iven
the
natu
re o
fthe
sou
rce
mat
eria
l.
Dat
e: 2
1st
Apr
il 20
1 lr
-
AD
EL
PH
I T
RA
NS
LA
TID
NS
CE
RT
IFIC
AT
E
OF
T
RA
NS
LA
TIO
N
DA
TE
Zl^
Afi
^lL
W
l
Kie
r B
ooth
PR
OJE
CT
MA
NA
GE
R
AD
EL
PHI
TR
AN
SLA
TIO
NS
LT
D.
^0
F7
X
£»
8 i
*
AD
ELP
HI
TRA
NS
LATI
ON
S
o
•7
7—
n
%
# •
Me
mb
er
®®
C)
Aw
oc
iali
on
ot
Tro
nsl
olk
m
Co
m p
on
ie J
Rcg
isw
rcd
' Hik
e1
iho
rnd
iftb
Mew
s.
i'ho
rnd
iRe i
'ark
\M
iiW,
Ch
ap
cko
wn
. S
iit'
tiki
d.
S35
IV
I In
corp
om
icd
in L
nd
iim
! a
iid W
ule
s *
Rog
isic
R-d
Nn.
06
98
97
VJ
* V
A I
No
K73
4495
87
29

FRENCH REPUBLIC
STRASBOURG UNIVERSITY 1
UNIVERSITY DIPLOMA In view of the education code •
In view ofthe decision ofthe board of directors atthe University of Louis Pasteur on the Sth July 2003
In view ofthe supporting documents produced by Mr. SIVAKUMAR GOPALSWAMY, bom on the 1 lth April 1974 in
COIMBATORE (INDIA) for the registration of his university diploma in laparoscopic surgery.
In view of the jury's statement attesting that the interested party has fulfilled the knowledge and aptitude requirements as set
out in the regulations
the UNIVERSITY DIPLOMA IN LAPAROSCOPIC SURGERY
is awarded to M R . S I V A K U M A R G O P A L S W A M Y
as from the 23rd May 2008, to enjoy the rights and obligations attaching thereto
Adelphi Translations Ltd Full Service
Tranuatlon Agency
The holder
/0EEAO20070334
Certificate of Translation Adetphi Translations Date 2 ^ A P o u ? 3 ^ signed j ^ M
STRASBOURG, 23 May 2008
President
[signature]
Alain BERETZ
Stamp: LOUIS PASTEUR UNIVERSITY
University Department of MEDICAL SCIENCE
•STRASBOURG*
30

Ad«lphi Translations Ltd
R E P U B L I Q U E F R A N C A I S E
UNIVERSITE STRASBOURG I
DIPLOME D'UNIVERSITE
Vu lc code de I'education
Vu la deliberation du conseil d'administration de PUniversite Louis Pasteur du 8 juillet 2003
Vu les pieces justificatives produites par M. SIVAKUMAR GOPALSWAMY, ne te 11 avril 1974 a COIMBATORE (IN'DH), en vue de son inscription an diplome d'univcrsitc de chirurgie laparoscopique
Vu les proces-verbaux du jury attestant que I'interesse a satisfait au controle des connaissances et des aptitudes prevu par les tcxlcs reglementaires
le DIPLOME D'UNIVERSITL UU CHIRURGIE LAP AROS COP IQUH
est decerne a M . S I V A K U M A R G O P A L S W A M Y
a compter du 23 mai 2008, pour en jouir avec les droits et les devoirs qui y sont attaches.
Le titulaire
/0EKAO20070334
Certificate of Translation Adelphi Translations Date t v ^ / t f f c l L T O r t signed M ^
Fait a STRASBOURG, le 23 mai 2008
Lc Presi Jent
Alain BERETZ * . \
31

R E P U B L I Q U E F R A N C A I S E
UNIVERSITE STRASBOURG 1
DIPLOME D'UNIVERSITE
CERTIFIED TRUE COPY PETER JAMES DEXTER
Notary Public 14 Rosewin Row Truro TR1 1HG
Cornwall UK Tel: 44 (0)1872 261614
/ •
t - i
Vu le code de I'education
Vu la deliberation du conseil d'administration de PUniversite Louis Pasteur du 8 juillet 2003
Vu les pieces justificatives produites par M. SIVAKUMAR GOPALSWAMY, ne lc 11 avril 1974 a COIMBATORE (INDE), en vue de son inscription au diplome d'universite de chirurgie laparoscopique
Vu les proces-verbaux du jury attestant que I'interesse a satisfait au controle des connaissances et des aptitudes prevu par les textes reglementaires
le DIPLOME D'UNIVERSITE DE CHIRURGIE LAPAROSCOPIQUE
est decerne a M . S I V A K U M A R G O P A L S W A M Y
a compter du 23 mai 2008, pour en jouir avec Ics droits et les devoirs qui y sont attaches.
Le titulaire
/0EEAO20070334
Fait a STRASBOURG, lc 23 mai 2008
Le President
Alain BERETZ
{-S ;tfc.ir-U;.:\.;ts,1 i £ ;
K ^ - g>y
32

Honours and prizes Please provide copies of certificates or letters showing what the prize or honour was for, including the selection and eligibility criteria and pool of eligible individuals.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
Other relevant qualifications and certificates Please provide copies of certificates.
For example: degrees or diplomas in relevant areas such as management, business, IT, communication, education or law.
Assessments and appraisals Appraisals and assessments Please provide validated copies of the evidence required in this area.
For non training posts you should provide evidence of ongoing evaluation of your performance.
This may take the format of formal appraisals by the department head or line manager (clinical director, medical director, professor).
In the UK, a revalidation or appraisal portfolio would be appropriate (if it is completed retrospectively less weight will be given to the information provided).
Alternative evidence may include letters (written at the time) commenting on your performance. In addition where no formal appraisal or assessment forms are available you must provide validated information on the method of career review or progression There are many different forms of assessment which form part of the various CCT curricula. Many of these tools are available for those not in training to use.
33

An
nu
al
Ap
pra
isa
l fo
r a
ll D
oct
ors
R
oyal
Com
wal
l Hps
pita
ls
hV
ffi
NH
ST
rust
NH
S M
edic
al A
pp
rais
al
Fir
st N
ame
Em
ploy
ee
Num
ber
Ap
pra
ise
r
Dat
e o
f A
pp
rais
al
Ann
ual
App
rais
al F
orm
fo
r C
on
sulta
nts
, A
ssoc
iate
Spe
cial
ists
, S
peci
alty
, S
taff
Gra
de &
Tru
st D
octo
rs
SIV
AK
UM
AR
1011
2057
(Loc
ated
at t
he
bo
tto
m o
f yo
ur p
aysl
ip)
Dr
Lisa
Had
don
23/1
/201
2 D
ate
of L
ast
Ap
pra
isa
l
Last
Nam
e
GM
C
Num
ber
Res
pons
ible
O
ffic
er
GO
PA
LSW
AM
Y
6104
961
Dr
Ray
Sin
clai
r
Dec
201
0 N
ext
Ap
pra
isa
l D
ate
(11
Mon
ths
Tim
e)
Dec
201
2
Intr
od
uct
ion
Th
e fi
eld
s a
bo
ve a
re m
an
da
tory
The
RC
HT
201
1/12
App
rais
al D
ocum
ent w
as a
gree
d in
May
201
1 an
d in
clud
es 6
sec
tions
for
com
plet
ion
prio
r to
the
appr
aisa
l dis
cuss
ion
and
supp
orte
d by
det
ail i
n yo
ur p
rofe
ssio
nal p
ortfo
lio.
Thi
s do
cum
ent
repl
aces
the
reva
lidat
ion
pilo
t too
lkit
and
the
'old
form
4' s
tyle
app
rais
al d
ocum
ents
, whi
ch h
ave
both
bee
n w
ithdr
awn.
R
OY
AL
CO
RN
WA
LL
HO
ti.
^^
^'
^^
Pro
fess
iona
l P
rofil
e an
d cu
rre
nt
Job
Pla
n ^
RO
YA
LC
OR
NW
AL
L H
OS
PIT
AL
Pro
bity
and
Hea
lth S
tate
men
t T
RU
R^
TR
^S
LJ
Eva
lua
tion
of p
revi
ou
s P
DP
Su
pp
ort
ing
Info
rmat
ion
(GM
C G
uida
nce)
:- T
o be
hel
d in
you
r po
rtfol
io fo
r re
view
at
appr
aisa
l dis
cuss
ion
and
deta
iled
in th
is d
ocum
ent.
1. C
ontin
uing
pro
fess
iona
l dev
elop
men
t 2.
Qua
lity
impr
ovem
ent
activ
ity
3. S
igni
fican
t ev
ents
4.
Fee
dbac
k fr
om c
olle
ague
s 5.
Fee
dbac
k fr
om p
atie
nts
(whe
re a
pplic
able
) 6.
Rev
iew
of c
ompl
aint
s an
d co
mpl
imen
ts
5 G
ood
Med
ical
Pra
ctic
e R
evie
w
>•.
• D
omai
n on
e -
Kno
wle
dge
Ski
lls a
nd P
erfo
rman
ce
• D
omai
n tw
o -
Saf
ety
and
Qua
lity
op\a
s^c
Dom
ain
thre
e -
Com
mun
icat
ion,
par
tner
ship
and
Tea
mw
ork^
p-c
t, a
nd
Dom
ain
four
- M
aint
aini
ng T
rust
" "-
SS
SS
E""
6
Cu
rre
nt
PD
P
Thes
e m
ust b
e co
mpl
eted
by
you
befo
re th
e ap
prai
sal d
iscu
ssio
n. T
he fi
rst 2
are
as a
re b
rief a
nd fa
dual
. S
uppo
rting
In
form
atio
n re
quire
s so
me
care
, but
the
stat
emen
ts s
houl
d pr
efer
ably
be
brie
f and
fact
ual.
It is
in th
e G
ood
Med
ical
Pra
dice
R
evie
w th
at y
ou a
re in
vite
d to
dem
onst
rate
how
the
supp
ortin
g in
form
atio
n yo
u ha
ve p
rovi
ded
dem
onst
rate
s th
at y
ou a
re u
p to
dat
e an
d fit
to p
radi
ce.
You
r app
rais
er w
ill s
ign
off
your
app
rais
al b
y co
mpl
etin
g th
e S
umm
ary
of D
iscu
ssio
n ba
sed
on G
ood
Med
ical
Pra
ctic
e an
d al
so th
e fo
ur s
tate
men
ts.
The
App
rais
er w
ill a
lso
agre
e th
e fin
al s
hape
of y
our
PD
P.
The
sum
mar
y of
the
appr
aisa
l and
sh
ould
be
com
plet
ed d
urin
g an
d im
med
iate
ly a
fter t
he d
iscu
ssio
n. T
his
is th
e re
spon
sibi
lity o
f you
r App
rais
er.
Thi
s d
ocu
me
nt
mus
t be
mar
ked
Priv
ate
and
Con
fiden
tial
and
addr
esse
d as
bel
ow:
FA
O:
Mat
t M
cKee
, Lea
rnin
g &
Dev
elop
men
t, K
now
ledg
e S
pa, R
oyal
Cor
nwal
l Ho
spita
l,
34

An
nu
al
Ap
pra
isa
l fo
r a
ll D
oc
tors
R
oyal
Cor
nvva
ll H
ospi
tals
hV
ifcl
N
HS
Tru
st
1: P
rofe
ssio
nal
Pro
file
and
Rec
ord
of
App
rais
al
(A
tii £ •o
•a
< E
o X
Te
l&
emai
l
Fla
t 6
, 2
Str
an
gw
ays
Te
rra
ce,
Tru
ro T
RI 2
NY
0773
8677
480
vgsh
iva
@ya
ho
o.c
om
(A
tn
OJ
•o
•a
< c (D
E
>«
o a E
UJ
Te
l&
emai
l
De
pa
rtm
en
t o
f S
urg
ery
, S
"1 flo
or,
To
we
r B
lock
, R
oya
l C
orn
wa
ll H
ospi
tal
Tru
ro.
TR
1 3
LJ.
01
87
2-2
53
29
9 S
iva
kum
ar.
go
pa
lsw
am
y@rc
ht.
corn
wa
ll. n
hs. u
k
Pro
fess
ion
al
Qu
ali
fica
tio
ns
M.B
.,B
.S.,
M S
(M
ast
er
of
Sur
gery
) G
ener
al S
urg
ery
DN
B (
(Dip
lom
ate
in
Na
tion
al
Bo
ard
) G
en
era
l S
urge
ry
MR
CS
(In
terc
olle
gia
te)
DM
AS
(D
iplo
ma
in m
inim
al
acc
ess
)
FR
CS
(G
en
era
l S
urg
ery
)
Co
lle
ge
/Un
ive
rsit
y
Th
e T
am
ilna
du
Dr
MG
R M
ed
ica
l U
niv
ers
ity,
Indi
a T
he
Ta
miln
ad
u D
r M
GR
Me
dic
al
Un
ive
rsity
, In
dia
Na
tion
al
Bo
ard
E
xam
ina
tion
s,
Min
istr
y o
f H
ea
lth &
F
am
ily W
elf
are
, G
ovt
.of
Indi
a, N
ew
D
elhi
. In
dia
Ro
yal
Co
lleg
e o
f S
urg
eo
ns,
E
din
bu
rgh
. U
K
Uni
vers
ity L
ouis
P
ast
eu
r, F
ran
ce
Ro
yal
Co
lleg
e o
f S
urg
eo
ns,
E
din
bu
rgh
. UK
Da
te C
om
ple
ted
Jan
19
97
Se
p 2
00
3
May
20
04
Dec
20
05
May
20
08
Sep
20
09
GM
C R
eg
istr
ati
on
D
eta
ils
Typ
e o
f R
eg
istr
atio
n H
eld
F
ull
Regis
tratio
n
Date
of
Fir
st
Fu
ll R
eg
istr
atio
n
May
2006
Cu
rre
nt
Po
st
Locu
m C
onsu
ltant
Surg
eon
Date
of
Ap
po
intm
en
t 01/0
5/2
011
RO
YA
L C
OR
NW
ALL
HO
SP
ITA
L T
RE
LIS
KE
TR
UR
O T
R1
3LJ
Qhf
iKh
Afc
ma
d,,
Bre
ast
o^
•s
35

An
nu
al A
pp
rais
al
for
all
Doc
tors
R
oyal
Cor
nwal
l Hos
pita
ls F
J/gf
rl In
itia
ls:
NH
STr
ust
Ke
y R
esp
on
sib
ilit
ies
Res
pons
ibili
ties
New
and
follo
w u
p cl
inic
s, w
ard
roun
ds, t
heat
res,
1 i
n 10
on
Cal
l, M
DT,
mor
tality
and
mor
bidi
ty a
nd x
-ray
mee
tings
, Te
achi
ng a
nd tr
aini
ng, a
udits
, adm
in w
orks
, man
agem
ent m
eetin
gs.
Oth
er
curr
en
t p
ost
s/ro
les
- (in
clud
ing
locu
m p
osts
and
Priv
ate
Pra
ctic
e)
Pos
t/Rol
e
Hon
orar
y T
each
ing
Fel
low
, P
enin
sula
Med
ical
Sch
ool,
UK
.
Sta
rt d
ate 01
/10/
2010
Su
mm
ary
o
f C
urr
en
t J
ob
Pla
n-
(You
r jo
b pl
an m
ust
be p
art o
f you
r su
ppor
ting
info
rmat
ion)
:
Are
a
Dire
ct C
linic
al C
are
(DC
C)
Cor
e S
uppo
rting
Pro
fess
iona
! act
ivity
(S
PA
)
Add
ition
al
Sup
porti
ng P
rofe
ssio
nal a
ctiv
ity (
SP
A)
Add
ition
al R
espo
nsib
ilitie
s
Ext
erna
l Dut
ies,
on
calls
p T
rave
lling
A
y
^ —
-*
*—
Jl
.VrC
U-ia
rl
PA 8-
10
2 1.5 1
Hou
rs flexi
ble
RO
YA
L C
OR
NW
ALL
Ho
o,
..^
o SK
i R
OY
AL
CO
RN
WA
LL H
OS
PIT
AL
TR
ELI
SK
E
TR
UR
O T
R1
3LJ
si
bn
^tr
nr
iCop
\ast
tc
Co
ns
uW
^S
urg
eo
n B
reas
l and
Gen
eral
36

RITAs, ARCPs and training assessments Formal records of assessment have been in place in the UK since 1996 (for posts of Registrar, Specialist Registrar, and Specialty Registrar). If you have undertaken training in the UK in these grades you should provide a validated copy of your formal records. In addition if you held any of these approved training posts (except locum posts), please provide evidence of your training number.
If you have undertaken training outside the UK you must provide evidence of formal periodic assessment during your training. This evidence must have been completed at the time the training was undertaken (if it is completed retrospectively less weight will be given to the information provided). If you do not supply formal assessment documents, you must provide the curriculum to demonstrate how you were assessed. A detailed letter of verification from an educational supervisor would satisfy this requirement.
If that training was recognised by relevant authorities outside the UK please provide evidence and recognition standards.
If areas for development were highlighted please provide evidence to demonstrate that you have subsequently addressed them There are many different forms of assessment which form part of the CCT curriculum. Many of these tools are available for those not in training to use.
360˚ and multi-source feedback You may wish to supply evidence of feedback from colleagues of all levels (peers, nursing, auxiliary staff, patients, management) completed at the time and may be in the format of letters, references for posts applied for etc.
Awards and discretionary points letters You must provide copies of certificates and letters.
Personal development plans (PDP) For details of what to include please see NHS clinical governance support information.
You must also provide evidence of review of your PDP at appraisal. PDPs normally form part of your annual appraisal system and you should submit them with appraisal documentation.
37

ES
S INTE
RC
OLL
EGIA
TE
_ „
•
• —
.
- _
-
,^
M.
»
SCUUSULLU
M
Cli
nic
al
Ev
alu
ati
on
Ex
erc
ise
(C
EX
) PR
OG
RAM
ME
lA^W
Ql^
flif
t^
ne
lg u
estio
nsIu
sing
Fay
[cK
fEl|
Tra
inee
n A
sses
sor
Nam
e:
^j
Q^
Qp
^J
ig^
jO
^ N
ame:
^
^ P
/f'Y
JJ
L'*
-
GM
C n
um
be
r:
fa/O
lj^
6/
Po
sitio
n:
OO
rJS
Vi-
T^^
r S
pe
cia
lty:
o
a
Car
dio
Gen
OD
D
Neu
ro
OM
FS
Oto
l D
DD
D
Pae
d P
last
T
&O
U
rol
GM
C n
umbe
r:
^^
?
Si 7
O
£
(or
othe
r pr
ofes
sion
al r
egis
tratio
n nu
mbe
r)
Ho
spita
l: 'jl
oy
Q^
Co
V-
tf
^Q
UL
Inst
itutio
na
l e-m
ail:
/i*
/.
lky
fr{@
jte
£f-
, t^
lru
^e
j/.
Tra
inm
g p
ost
(e.
g. C
T1/
ST
1): "
J^
jsJ
' ^
A*
^-
Tra
inin
g:
No
Q
Wri
tte
n•
Web
/CD
g-W
ork
sh
op
O
Clin
ica
l se
ttin
g (e
.g. O
utpa
tient
s):
7 ^
fif
aA*^
Sum
mar
y o
f th
e cl
inic
al p
rob
fem
:
Foc
us o
f en
coun
ter:
H
isto
ry
Exa
m
Dia
gnos
is
Man
agem
ent
Exp
lana
tion
0
Con
sent
Com
plex
ity o
f th
e c
ase:
1.
App
ropr
iate
for e
ariy
yea
rs tr
aini
ng
2. A
ppro
pria
te fo
r the
com
plet
ion
of e
arly
yea
rs tr
aini
ng o
r ear
ly s
peci
alty
trai
ning
3. A
ppro
pria
te fo
r the
cen
tral
per
iod
of s
peci
alty
trai
ning
4. A
ppro
pria
te for
Cer
tific
ate
of C
ompl
etio
n of
Tra
inin
g (C
CT
)
AS
SE
SS
ME
NT
RA
TIN
GS
You
r as
sess
men
t ra
tings
sho
uld
be ju
dged
aga
inst
the
stan
dard
laid
out
in th
e s
ylla
bus
for t
he tr
aine
e's
stag
e of
trai
ning
How
do
yo
u ra
te t
his
tra
inee
in
the
fr:
Out
stan
ding
S
atis
fact
ory
Dev
elop
men
t re
quire
d N
ot a
sses
sed
1. H
isto
ry ta
king
ski
lls
y 7
2. P
hysi
cal e
xam
inat
ion
skill
s
3. D
iagn
ostic
ski
lls a
nd u
nder
lyin
g kn
owle
dge
base
/
4. M
anag
emen
t an
d fo
llow
-up
plan
ning
7"
y
5. C
linic
al ju
dgem
ent
and
deci
sion
mak
ing
6. C
omm
unic
atio
n an
d lis
teni
ng sk
ills
y -t 7.
Org
anis
atio
n an
d tim
e m
anag
emen
t
FE
ED
BA
CK
: Ver
bal f
eedb
ack
is a
man
dato
ry c
ompo
nent
of t
his
asse
ssm
ent.
Ple
ase
use
this
spa
ce to
reco
rd a
reas
of s
treng
th
and
sugg
estio
ns o
f dev
elop
men
t whi
ch w
ere
high
light
ed d
urin
g di
scus
sion
with
the
trai
nee:
fiw
rcl
TTO
VW
I U
uW
^X
^e
^w
,
vw
\
GLO
BA
L S
UM
MA
RY
Afte
r su
mm
aris
ing
the
disc
ussi
on w
ith th
e tra
inee
in th
e b
ox a
bove
, ple
ase
com
plet
e th
e ov
eral
l lev
el a
t whi
ch th
e C
linic
al
Eva
luat
ion
Exe
rcis
e w
as p
erfo
rmed
on
this
occ
asio
n, if
ther
e w
as s
uffic
ient
evi
denc
e to
mak
e a
judg
emen
t:
Leve
l 0
Bel
ow th
at e
xpec
ted
for e
arly
yea
rs tr
aini
ng
Leve
l 1
App
ropr
iate
for
early
yea
rs tr
aini
ng
Leve
l 2
App
ropr
iate
for c
ompl
etio
n of
ear
ly y
ears
trai
ning
or e
arly
spe
cial
ty tr
aini
ng
Leve
l 3
App
ropr
iate
for
cen
tral p
erio
d of
spe
cial
ty tr
aini
ng
~7 /
Leve
l 4
App
ropr
iate
for
the
Cer
tific
ate
of C
ompl
etio
n of
Tra
inin
g (C
CT
)
Tim
e ta
ken
for f
eedb
ack
(min
s):
Tim
e ta
ken
for o
bser
vatio
n (m
ins)
: T
ime
take
n fo
r fee
dbac
k (m
ins)
: r\
**
•*.
Dat
e:
\^
^ (-
£t
fj>f
Tra
inee
's s
ign
atu
re:
^^
^j
^C
^J
Ass
ess
or'
s si
gn
atu
re:
^ T
V^
^v
.
Oct
ob
er
20
10
P
a?
8M
l] C
OR
NW
ALL
HO
SPIT
ALS
TR
US
T
Sh
eik
n A
lim
?ti
R
OYA
L C
OR
NW
ALL
HO
SPIT
AL
^ons
utta
nt'O
neO
pfas
ii,.'.
TR
SS
^U
. Br
east
and
Gen
enl
fe,
38

.„
^
Gen
eral
Sur
gery
PB
A:
Ap
pe
nd
ice
cto
m
AP
PR
OV
ED
SU
RG
ICA
L TE
MP
LATE
Jun
06
Tra
inee: = S
- 6o
?ftu
vJ&
**y
Ass
ess
or:
/*
f . p
J
tffL
vrM
JCtf
^ D
ate:
A
2-/<
> ^
^^
7
Sta
rt tim
e:
tZ-"
* E
nd
tim
e:
/3-r
o D
ura
tio
n:
3~o
Opera
tion
mo
re d
ifficu
lt th
an
usu
al?
Y
e s
(If
yes,
sta
te r
easo
n)
The
Tra
inee
sh
ou
ld e
xpla
in w
ha
t he/s
he
in
ten
ds
to d
o t
hro
ug
ho
ut
the
pro
ced
ure
T
he
Ass
ess
or
sho
uld
pro
vid
e v
erb
al p
rom
pts
, if
req
uir
ed
, and
inte
rve
ne
if
pa
tien
t sa
fety
is
at
risk
.
Ra
tin
g:
N =
No
t o
bse
rve
d o
r n
ot
ap
pro
pri
ate
D
= D
eve
lopm
ent
req
uir
ed
S
= S
atis
fact
ory
sta
nd
ard
fo
r C
CT
(no
pro
mp
tin
g o
r in
terv
en
tio
n r
eq
uir
ed
)
Com
pete
ncie
s an
d D
efin
ition
s
ci
02
03 04
C5
PLI
PL2
PL3
PL4
PLS
.
•IIH
P
R1
PR
2
PR
3
PR
4
PRS
PR
6
PR
7
PRS
KO
I E
1 E2
E3
E4
Dem
onst
rate
s so
und
know
ledg
e of
indi
catio
ns a
nd c
ontra
indi
catio
ns
incl
udin
g al
tem
ativ
es to
sur
qery
Dem
onst
rate
s aw
aren
ess
of s
eque
lae
of o
pera
tive
or n
on o
pera
tive
man
agem
ent
Dem
onst
rate
s so
und
know
ledg
e of
com
plic
atio
ns o
f sur
gery
Exp
lain
s th
e pe
riope
rativ
e pr
oces
s to
the
patie
nt a
nd/o
r re
lativ
es o
r car
ers
and
chec
ks
unde
rsta
ndin
q
Exp
lain
s lik
ely
outc
ome
and
time
to re
cove
ry a
nd c
heck
s un
ders
tand
ing
Dem
onst
rate
s re
cogn
ition
of a
nato
mic
al a
nd p
atho
logi
cal a
bnor
mal
ities
(an
d re
leva
nt c
om
orbi
ditie
s) a
nd s
elec
ts a
ppro
pria
te o
pera
tive
stra
tegi
es/te
chni
ques
to d
eal w
ith th
ese
e.g.
nu
tritio
nal s
tatu
s D
emon
stra
tes
abilit
y to
mak
e re
ason
ed c
hoic
e of
app
ropr
iate
equ
ipm
ent,
mat
eria
ls o
r de
vice
s (if
any
) ta
king
into
acc
ount
app
ropr
iate
inve
stig
atio
ns e
.q. x
-ray
s
Che
cks
mat
eria
ls, e
quip
men
t and
dev
ice
requ
irem
ents
with
ope
ratin
g ro
om s
taff
Ens
ures
the
oper
atio
n si
te is
mar
ked
whe
re a
pplic
able
Che
cks
patie
nt r
ecor
ds, p
erso
nally
rev
iew
s in
vest
igat
ions
Che
cks
in th
eatre
that
con
sent
has
bee
n ob
tain
ed
Giv
es e
ffect
ive
brie
fing
to th
eatre
team
Ens
ures
pro
per
and
safe
pos
ition
ing
ofth
e pa
tient
on
the
oper
atin
g ta
ble
Dem
onst
rate
s ca
refu
l ski
n pr
epar
atio
n
Dem
onst
rate
s ca
refu
l dra
ping
oft
he p
atie
nt's
ope
rativ
e fie
ld
Ens
ures
gen
eral
equ
ipm
ent a
nd m
ater
ials
are
dep
loye
d sa
fely
(e.
g. c
athe
ter,
diat
herm
y)
Ens
ures
app
ropr
iate
dru
gs a
dmin
iste
red
Arr
ange
s fo
r and
dep
loys
spe
cial
ist
supp
ortin
g eq
uipm
ent
(e.g
. im
age
inte
nsifi
ers)
ef
fect
ivel
y
Dem
onst
rate
s kn
owle
dge
of o
ptim
um s
kin
inci
sion
/ po
rtal /
acc
ess
Ach
ieve
s an
ade
quat
e ex
posu
re th
roug
h pu
rpos
eful
dis
sect
ion
in c
orre
ct ti
ssue
pla
nes
and
id
entif
ies
all s
truct
ures
cor
rect
ly
Com
plet
es a
sou
nd w
ound
rep
air w
here
app
ropr
iate
Pro
tect
s th
e w
ound
with
dre
ssin
gs, s
plin
ts a
nd d
rain
s w
here
app
ropr
iate
Rat
ing
N/D
/S
S
2 S s
^: S
%
$ S
J 9 ?•
5 5 5 S
5 J S S
r- s
Com
men
ts
/?
RO
YA
L C
OR
NW
AL
L H
0&
IT
AL
S T
RU
ST
,*
.
PBA
Ass
essm
ent P
rodu
ced
by
OC
ApR
G&
Wp
£&
RN
MM
e^
^J
^L
l/2
S
tie
Hc
fl
Ah
ma
d
TR
UR
O^
f 3LJ
C
onsu
ltant
Onc
opla
stic
TR
UR
O T
R1
3LJ
^^
an
d G
en
er
ai
Su
rg
eo
n
39

Com
pete
ncie
s an
d D
efin
ition
s
IT1(
G)
IT2(
G)
IT3(
G)
IT4(
G)
IT5(
G)
IT6(
G)
IT7(
G)
IT8(
G)
IT9(
G)
IT10
(G)
ITI 1
(G)
IT12
(T)
IT13
(T)
ITM
(T)
IT15
(T)
IT16
(T)
IT17
(T>
PM
I
PM
2
PM
3
PM
4
Follo
ws
an a
gree
d, lo
gica
l seq
uenc
e or
pro
toco
l for
the
proc
edur
e
Con
sist
ently
han
dles
tiss
ue w
ell w
ith m
inim
al d
amag
e
Con
trols
ble
edin
g pr
ompt
ly b
y an
app
ropr
iate
met
hod
Dem
onst
rate
s a
soun
d te
chni
que
of k
nots
and
sut
ures
/sta
ples
Use
s in
stru
men
ts a
ppro
pria
tely
and
saf
ety
Pro
ceed
s at
app
ropr
iate
pac
e w
ith e
cono
my
of m
ovem
ent
Ant
icip
ates
and
resp
onds
app
ropr
iate
ly to
var
iatio
n e.
g. a
nato
my
Dea
ls c
alm
ly a
nd e
ffect
ivel
y w
ith u
nexp
ecte
d ev
ents
/com
plic
atio
ns
Use
s as
sist
a nt
(s) t
o th
e be
st a
dvan
tage
at a
ll tim
es
Com
mun
icat
es c
lear
ly a
nd c
onsi
sten
tly w
ith th
e sc
rub
team
Com
mun
icat
es c
lead
y an
d co
nsis
tent
ly w
ith th
e an
aest
hetis
t
Per
foim
s ex
plor
atio
n of
the
right
ilia
c fo
ssa
in a
logi
cal f
ashi
on
Mob
ilises
and
del
iver
s ap
pend
ix in
to w
ound
saf
ely
Div
ides
and
liga
tes
the
mes
oapp
endi
x sa
fely
and
sec
urel
y
Div
ides
the
appe
ndix
saf
ety
and
secu
res
appe
ndix
stu
mp
Exa
min
atio
n of
the
term
inal
ileu
m a
nd p
elvi
c or
gans
whe
n th
e ap
pend
ix is
foun
d to
be
mac
rosc
opic
ally
nor
mal
Man
ages
intra
perit
onea
l con
tam
inat
ion
at e
nd o
f pro
cedu
re a
ppro
pria
tely
Ens
ures
the
patie
nt is
tran
sfer
red
safe
ly fr
om th
e op
erat
ing
tabl
e to
bed
Con
stru
cts
a cl
ear o
pera
tion
note
Rec
ords
dea
r an
d ap
prop
riate
pos
t ope
rativ
e in
stru
ctio
ns
Dea
ls w
ith s
peci
men
s. L
abel
s an
d or
ient
ates
spe
cim
ens
appr
opria
tely
Rat
ing
N/D
/S
$ s J J J / J1 -S
J 5 <7 9 5 s c J 5 ) V
£ r
Com
men
ts
Leve
l atw
hic
h co
mpl
eted
ele
men
ts o
fth
e P
BA
w
ere
perf
orm
ed o
n th
is o
ccas
ion
Tic
k as
ap
prop
riate
Leve
l 0
Insu
ffici
ent
evid
ence
obs
erve
d to
sup
port
a su
mm
ary
judg
emen
t
Leve
l 1
Una
ble
to p
erfo
rm th
e pr
oced
ure,
or
part
obse
rved
, und
er s
uper
visi
on
Leve
l 2
Abl
e to
per
form
the
proc
edur
e, o
r pa
rt ob
serv
ed, u
nder
sup
ervi
sion
Leve
l 3
Abl
e to
per
form
the
proc
edur
e w
ith m
inim
um s
uper
visi
on (
need
ed o
ccas
iona
l hel
p)
Leve
l 4
Com
pete
nt to
per
fonn
the
proc
edur
e un
supe
rvis
ed (c
ould
dea
l with
com
): E
taya
lCom
waB
HoB
^taf
g E
kfe
HHS
Tru
st
Co
mm
en
ts b
y A
sse
sso
r (i
ncl
ud
ing
stre
ng
ths
an
d a
rea
s fo
r d
eve
lop
me
ijjt)
:
Ve7
Mee
k <J
Wl €
^->
, £
Co
mm
en
ts b
y T
rain
ee
:
Tra
ine
e S
ign
atu
re:
C^
fi
J^
r u
J^
/C
^ f
vu
st-
SU
RG
ICA
L D
IVIS
ION
Ass
ess
or
Sig
na
ture
: _
A
.
PBA
Ass
essm
ent:
Pro
duce
d by
OC
Ag
pp
gff
clfc
Ata
tt&
CG
en
era
l S
urge
iy 2
/2
Co
nsu
ltan
t O
nco
pla
stic
B
rea
st a
nd
Ge
ne
ral
Su
rge
oi.
Gin
t)
43
7745
?
40

Participation in assessment, appraisal and appointments process
You could demonstrate this in a number of ways including:
invitations to appraisals or assessments
minutes or other records of attendance.
These could provide evidence of:
attendance at appraisal or assessment courses
participation in Deanery ARCP and RITA processes
participation in the appointments process for medical colleagues
involvement in interview panels and interview appointment related courses
involvement in workplace based assessments (as assessor)
All of the above must be anonymised (with respect to individual appraisee information).
41

Logbooks, records of daily clinical practice and portfolios The evidence you supply here must demonstrate that you have achieved all the requirements and competencies as set down in the CCT curriculum for your specialty.
Where you have, for a substantial period of time, worked in a specialised area, you should submit evidence that at one stage in your career you achieved the requirements and competencies of the curriculum for your specialty and that have maintained these skills. You will also need to provide evidence that your current specialised practice allows you to meet all of the requirements of Good Medical Practice.
Logbooks Photocopies of operating lists and theatre record books are not satisfactory evidence of procedures. If you did not complete a logbook at the time you undertook the procedures, you should create a logbook from the information you have and then have it validated. It should contain the following information:
only procedures that you were personally involved in
patient ID number but not the name
age and gender
date of the procedure
full name of the procedure
your role in the procedure (assisted, performed personally, performed under direct supervision of someone more senior, supervised a junior)
any critical incidents
name of the hospital or clinic where procedure was performed
outcomes data.
It is important that these cover the full range of the curriculum demonstrating the breadth and depth of the specialty. This may mean that you have to go back further than 5 years.
All evidence in this area must be validated and anonymised for individual patient data.
42

Mr Sivakumar Gopalswamy. GMCNO-6104961
MBBS, MS, DNB, MRCS, DLS, FRCS (Gen Surg).
LOG BOOK CONSOLIDATION SHEET
From 01/08/2007 to 31/07/2008.
ROYAL CORNWALL HOSPITALS TRUS t ROYAL CORNWALL HOSPiTAL
TRELISKE TRURO TR1 3LJ
f-—,>- - >
NJdML^ Sheikh Ahmad
Consultant Oncoplastic Breast and General Surgoon 43

A- Assisting, PTS- Performed Trainer Scrubbed, P- Performed Independently, T-
L-Laparoscopic, LA- Lap Assisted, LO- Lap converted to Open OPERATION
Appendicectomy Groin Hernia Repair
-Recurrent Umbilical/Paraumbilical hernia repair
Parastomal Hernia Repair Circumcision
Orchidopexy
Herniotomy Orchidectomy
ACE/PEG tube change Incisional Hernia Repair Small Bowel Resection and Anastamosis
Hemicolectomy-Right Hemicolectomy- Left
Transverse colectomv Subtotal Colectomy Total Colectomy with TME
Hartmann's Procedure
Reversal of Hartmanns Anterior Resection
APR Proctectomy 8J Pouch Formation
Abdominal Rectopexy
Delorme's Procedure
Colonoscopy &/ polypectomy Haemorroidectomy-open/stappled
HALO &/RAR
Perianal Fistula Repair Closure of Loop stoma
TOTAL 52
11
2 4
4
3 1
7
2 3
5 6
17 4
2 4
1
10 6
35
6 4 4
3
35 9
10 12 9
P
43
6 2
4
1 1
2
3 2 1
1
2
12 4
2 5
a i
PTS 3
3
1 3
1
4
1
2 7
2
2 1
7 1
10
2
1
2
20
3 4
5 5
i
Training Junior Trainee, E- Emergency
A 1
2
3
3 1 2 2
1
8 1
2 1
1
5
25 4
4
3
1
3 1
4 2 1
T
5
E
50 3
1
1
1
1
1
6
3 1 1
1
5
1
L
39
3
1
10
11
1
4
LA
1
1
1 2
LO
1
1
1
3
ROYAL CORNWALL HOSPITAL TRELISKE
TRURO TR1 3LJ
( -.^-
v Sheikh A h m a d S Gopalswamy
Consultant Oncoplastic Consolidation Aug 07 to July 08 Breast and General Surgeon 44

Consolidation, cumulative data sheets, summary lists and annual caseload statistics
You should provide a summary of the total numbers for the various procedures listed in the logbook. This should be completed annually and include your role in the procedure.
It is important that the logbooks cover the full range of the curriculum demonstrating the breadth and depth of the specialty. This may mean that you have to go back further than five years.
All evidence in this area must be validated and anonymised for individual patient data.
Medical reports You should provide examples across the breadth of your practice following the Academy of Medical Royal Colleges and NHS agreed format:
A Clinician’s Guide to Record Standards - Part 1
A Clinician’s Guide to Record Standards - Part 2
You can use these to demonstrate:
your involvement or role in cases
the types and complexity of cases you are involved in
your handling of patient paperwork
your respect and protection of confidential information
triangulation with logbook information.
All evidence in this area must be validated and anonymised for individual patient data.
45

Case histories Case histories that you provide should include:
patient ID number
dates
diagnosis
nature of your involvement in the management of the case
which curriculum competencies were involved.
You can use these to demonstrate:
your involvement or role in cases
the types and complexity of cases you are involved in
your handling of patient paperwork
your respect and protection of confidential information
triangulation with logbook information.
All evidence in this area must be validated and anonymised for individual patient data.
46

Referral letters discussing patient handling Please provide a variety of copies of letters to cover all aspects of your work and to demonstrate the breadth of your practice. This may include examples of letters:
requesting a second opinion
advising clinical colleagues or answering particular questions regarding patient management
from clinical colleagues regarding applicants involvement in patient management.
You can use these to demonstrate:
your involvement or role in cases
the types and complexity of cases you are involved in
your relationship with your colleagues in other disciplines
your handling of patient paperwork
your recognition of the limits of your professional competence
your respect and protection of confidential information.
All evidence in this area must be validated and anonymised for individual patient data.
Patient lists You may wish to include copies of patient lists. You can use these to demonstrate:
your involvement or role in cases
the types and complexity of cases you are involved in
your participation in teaching and training (where you are supervising a junior colleague)
the volume of cases you undertake
triangulation with rota, timetable and job plan information
triangulation with logbook information.
All evidence in this area must be validated and anonymised for individual patient data.
47

Department of Gastroenterology Surgery
Patient Letter
Royal C o r n w a l l Hospi ta ls I t f lS f c i NHSTrust
Truro, Cornwall TR1 SLJ
Consultant: Mr S Gopalswamy, Locum Consultant Surgeon
Secretary:
• T e l :
Ref: SG/AD/C445803
NHSNumber: C ^ A ^ 'SB Dateofbir th: DateTyped: 05.12.11
Dear Dr
Re:
Many thanks for seeing this gentleman who is 64 years old and he was diagnosed with a 17mm tubulovillous low grade adenoma in the rectum. It was completely excised. He gave us a very strong family history of bowel cancer. His mum and brother were diagnosed with bowel cancer and also his aunts and grandfather. If you could kindly assess whether he needs any further genetic tests. I am enclosing a copy of my clinic letter for your reference. If you have any concerns please do not hesitate to contact us.
Kind Regards
Yours sincerely
Sivakumar Gopalswamy Locum Consultant Surgeon to
Surgeon
Cc:
Qheikh Ahmad
Breast and General surg
48

Departmental (or trust) workload statistics and annual caseload statistics
You can use these to demonstrate:
the size of the hospital in which you work
the volume of work undertaken within your trust and the percentage that you undertake
the range of work that you undertake and that is undertaken within your trust
triangulation with logbook information
All evidence in this area must be validated.
Rotas, timetables and job plans Where you have undertaken a number of roles provide details for each post or role. You can use these documents to demonstrate:
details of clinical and non-clinical duties you undertake
your on-call commitment
your participation in meetings and teaching
triangulation with logbook information.
All evidence in this area must be validated.
Courses relevant to curriculum
Portfolios (electronic or revalidation) Do not submit your whole portfolio. You need to separate the evidence in it and submit that under the correct headings as set out in this guidance.
49

Ply
mou
th A
TL
S G
roup
C
ours
e D
irec
tor:
D
r A
nne
Hic
ks, C
onsu
ltant
- E
mer
genc
y M
edic
ine
Em
erge
ncy
Dep
artm
ent,
Lev
el 0
6, D
erri
ford
Hos
pita
l, Pl
ymou
th
Cou
rse
Adm
inis
trat
or:
Alis
on M
cDon
ald
Res
usci
tatio
n D
epar
tmen
t, L
evel
05,
Der
rifo
rd H
ospi
tal,
Plym
outh
PL
6 SD
H.
Tel
: 017
52 4
3196
4 E
.mai
l: al
ison
.mcd
onal
dl@
iiis
.net
es
11th J
uly
2012
Mr
S G
opal
swam
y F
lat 6
, N
o 2
Str
ange
way
s T
erra
ce
TR
I2N
Y
Dea
r S
iva
Re
: A
dva
nce
d T
raum
a U
fe S
up
po
rt C
ou
rse
, 13
?* -
IS
? Ju
ne
2012
D
err
ifo
rd H
osp
ita
l, P
lym
ou
th
Con
grat
ulat
ions
on
succ
essf
ully
com
plet
ing
the
abov
e co
urse
.
Yo
ur
ma
rks
in t
he
wri
tte
n pa
pers
we
re:
Pre
-Cou
rse
MC
Q P
aper
: 38
MC
Q1
: 33
Po
st-C
ou
rse
MC
Q P
aper
: 32
You
r ce
rtifi
cate
will
be
sent
to
you
with
in 3
-6
mon
ths
oft
he
cour
se.
Ple
ase
do n
ot h
esita
te t
o co
ntac
t m
e sh
ould
you
req
uire
any
furt
her
info
rmat
ion.
Bes
t wis
hes.
You
rs s
ince
rely
Alis
on M
cDon
ald
Adm
inis
trat
or /
Cou
rse
Co-
ordi
nato
r
SW
iw*
?. c
0o
\as
t»c
^tA
LS
TR
US
T
TH
0RO
-VR
A3U
J
50

Details of posts and duties (including both training and experience posts)Employment letters and contracts of employment The information in these letters and contracts must match your CV. They will confirm the following:
dates you were in post
post title, grade, training
type of employment: permanent, fixed term, or part time (including percentage of whole time equivalent)
All evidence in this area must be validated.
Job descriptions These must match the information in your CV. They will confirm the following:
your position within the structure of your department
your post title
your clinical and non clinical commitment
your involvement in teaching or training.
All evidence in this area must be validated.
51

Job plans Where you have undertaken a number of roles, provide details for each post or role. You can use these documents to demonstrate:
the main duties and responsibilities of the post
your out of hours responsibilities, including rota commitments
that you have covered for colleagues' periods of leave
any professional supervision and management of junior medical staff that you have undertaken
your responsibilities for carrying out teaching, examination and accreditation duties
your contribution to postgraduate and continuing medical education activity, locally and nationally
any responsibilities you had that relate to a special interest
requirements to participate in medical audit and in continuing medical education
your involvement in research
your managerial, including budgetary, responsibilities where appropriate
your participation in administration and management duties.
All evidence in this area must be validated.
52

Research, publications and presentations Research papers, grants, patent designs Please include any research relevant to your current practice.
If the research is published - please submit the first page of the published paper.
If the research is not published - please provide a summary or abstract of the research.
Colleges may undertake web searches to check the information you provide.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information
working with colleagues (where research is joint or multi disciplinary)
continuing professional development.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated.
53

Publications within specialty field Include a copy of the front page of each publication.
More weight is given where:
the applicant is first author
the publication has a high impact factor.
You must not change the listing of the authors (the order in which the authors are listed) in papers where there is more than one author.
Colleges may undertake web searches to check the information you provide.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information
working with colleagues (where publications are joint or multi disciplinary)
continuing professional development.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge:
Presentations, poster presentations You may wish to supply invitations to present at national or international meetings to demonstrate your recognition within your specialty. You may also supply feedback from presentations or meeting agendas or programmes that show your participation.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information
continuing professional development
teaching and training.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated by the hospital or relevant body who can attest to the event.
54

Ver
tical
Ext
ende
d P
edic
le T
hera
peut
ic M
am
mo
pla
sty
- A
n ad
vanc
ed
brea
st c
onse
rvat
ion
tech
niq
ue
V.A
. B
onel
io, S
. Gop
alsw
amy,
P.
J. D
rew
, S.
Ahm
ad
Dep
ortm
ent
of
Bre
ast S
urge
ry,
Roy
al C
ornw
all H
ospi
tals
NH
S T
rust
, T
ruro
TR
I S
U |R
oyal
Cot
Tiw
allH
fxpi
Uls
h!li±
j|
The
na
tiona
l re
-exc
isio
n ra
te
follo
win
g st
anda
rd
brea
st
cons
erva
tion
surg
ery
is a
roun
d 25
%.
We
offe
r V
ertic
al
Ext
ende
d P
edic
le
The
rape
utic
M
amm
opla
sty
(VEP
TM)
as a
n al
tern
ativ
e to
sui
tabl
e pa
tient
s in
or
der
to
try
and
redu
ce
this
re
-exc
isio
n ra
te
whi
lst
prov
idin
g a
satis
fact
ory
cosm
etic
res
ult.
The
aim
of
th
is
stud
y is
to
in
vest
igat
e w
heth
er
this
pr
oced
ure
prov
ides
an
onco
logi
cally
saf
e an
d co
smet
ical
ly
acce
ptab
le
alte
rnat
ive
to
trad
ition
al
brea
st
cons
erva
tion
tech
niqu
es.
Dat
a w
as c
olle
cted
pro
spec
tivel
y ov
er a
per
iod
of e
ight
een
mon
ths.
S
uita
ble
patie
nts
wer
e of
fere
d st
anda
rd
brea
st
cons
erva
tion
surg
ery
in t
he
form
of
W
ide
Loca
l E
xcis
ion
(WLE
) or V
EPTM
. P
atie
nt
dem
ogra
phic
s,
Tum
our
size
(m
m)
and
wei
ght
of
tissu
e re
mov
ed (
g),
hist
olog
y, c
lose
st m
argi
ns (
mm
) an
d th
e ne
ed fo
r fu
rthe
r su
rger
y w
as n
oted
.
Figu
re 2
: Skin
mar
king
of t
umou
r and
late
ral s
kin
mar
king
For
ty-f
our
patie
nts
elec
ted
to h
ave
VEPT
M o
ver
this
per
iod
of t
ime
. T
wen
ty-n
ine
of t
hese
pat
ient
s op
ted
to h
ave
a co
ntra
late
ral r
educ
tion
proc
edur
e fo
r sy
mm
etris
atio
n.
The
mea
n tu
mou
r si
ze (
mm
) w
as 2
5 (r
ange
10-
117)
. Th
e m
ean
tum
our
wei
ght
(g)
was
100
whi
lst
the
max
imum
am
ount
of
tissu
e re
mov
ed w
as 3
77.
Nat
iona
l re-
exci
sion
rat
es fo
llow
ing
stan
dard
BCS
vs
loca
l re
-exc
isio
n ra
tes
follo
win
g VE
PTM
••d
fa, r
„,tK
lort
° "*
•'»
IIH n
-au
liliH
i
25S
re-e
xcis
ion
rate
nat
iona
lly
9* r
e-ex
cisi
on ra
te lo
cally
In t
he U
nite
d K
ingd
om,
arou
nd 2
5% o
f pa
tient
s w
ill r
equi
re
re-e
xcis
ion
folto
win
g a
wid
e lo
cal
exci
sion
du
e to
in
com
plet
e re
sect
ion
mar
gins
.
Our
dat
a sh
owed
tha
t 9%
of
the
patie
nts
havi
ng V
EPTM
(n
=4)
requ
ired
furt
he
r su
rger
y in
con
tras
t to
th
e 25
% r
e-
exci
sion
rat
e in
WLE
.
All
thes
e pa
tient
s un
derw
ent
a co
mpl
etio
n m
aste
ctom
y.
All
patie
nts
wer
e sa
tisfie
d w
ith
the
cosm
etic
out
com
e an
d th
ere
wer
e no
sig
nific
ant
com
plic
atio
ns.
In a
dditi
on o
ur m
aste
ctom
y ra
te w
as r
educ
ed t
o 14
% a
s a
resu
lt of
th
e in
crea
sed
num
ber
of V
EPTM
per
form
ed.
Figu
re 3
: Pos
t-ope
ratiw
res
ult
Our
re
-exc
isio
n ra
te
of
9%
com
pare
s w
ell
with
th
e lit
erat
ure
avai
labl
e, r
epor
ting
a re
-exc
isio
n ra
te o
f 7-1
1%
follo
win
g VE
PTM
. In
add
ition
to
achi
evin
g m
ore
com
plet
e re
sect
ion
mar
gins
, VE
PTM
ha
s de
crea
sed
the
num
ber
of
com
plet
ion
mas
tect
omie
s pe
rform
ed w
ithin
our
dep
artm
ent.
Red
ucin
g th
e si
ze o
f th
e af
fect
ed
brea
st a
lso
faci
litat
es
post
-ope
rativ
e ra
diat
ion
ther
apy
as l
ower
rad
iatio
n do
ses
are
nece
ssar
y an
d th
ere
is a
gre
ater
un
iform
ity
in
the
deliv
ery
of r
adia
tion.
A
dvan
ced
brea
st c
onse
rvat
ion
surg
ery
usin
g VE
PTM
redu
ces
re-e
xcis
ion
rate
s w
ithou
t co
mpr
omis
ing
cosm
esis
. O
ther
issu
es s
uch
as th
e co
st o
f ha
ving
bila
tera
l sur
gery
and
pr
oduc
ing
an o
bjec
tive
post
-ope
rativ
e ae
sthe
tic e
valu
atio
n of
the
cos
met
ic r
esul
t sh
ould
be
cons
ider
ed.
Mul
ti-ce
ntre
ra
ndom
ised
con
trol
led
tria
ls a
re r
equi
red
to
conf
irm t
he e
ffica
cy
and
cost
-effe
ctiv
enes
s of
VEP
TM i
n re
duci
ng re
-exc
isio
n an
d m
aste
ctom
y ra
tes.
I.Kob
berm
an A
, e
tal.
, Im
pact
of
rou
tine
cavi
ty s
have
mar
gins
on
brea
st
canc
er r
e-ex
cisi
on r
ates
. A
nn S
urgJ
3nco
l. 20
11 M
ay;1
8(5)
:134
9-55
. E
pub
2010
Nov
3
2.C
hurg
1n S
, et
al.
, R
econ
stru
ctio
n op
tions
fo
llow
ing
brea
st c
onse
rvat
ion
ther
apy.
Cle
ve C
lin J
Med
. 20
08 M
ar;7
5 S
uppl
1:5
24-9
. R
evie
w.
3.lw
uctiu
kwu
OC
, et
al.
, The
ro
le o
f on
copl
astic
the
rape
utic
mam
mop
last
y 1n
bre
ast
canc
er s
urge
ry -
A r
evie
w.,
Sur
gica
l Onc
olog
y (2
011)
,doi
:10.
1016
/j.su
ronc
.201
1.01
.002
Con
uct:
Vic
tcnU
ton
ello
itc
urlit
ioiw
UD
Stn
iitl.c
on
1 S
heik
h A
hmad
\C
onsu
itant
Onc
opla
stic
B
reas
t an
d G
ener
al S
urge
on
55

CPD and CME CPD record certificates, certificates of attendance, workshops and at local, national and international meetings or conferences
You should provide a variety of these to cover all aspects of your work and to demonstrate the breadth of your practice. Where you have specialised the provision of CPD records covering the other aspects of the relevant curriculum is important to demonstrate the maintenance of your skills.
Please provide details of the events you have attended describing the content. Support this with documentary evidence of your attendance (CPD certificates etc).
CPD registration points from UK Medical Royal College (or equivalent body overseas)
Please provide evidence of registration within a formal system. Royal Colleges or Faculties may confirm attainment of their requirements.
Membership of professional bodies and organisations List the following for your current membership of professional bodies and organisations. Provide documentary evidence showing membership information:
organisation name
date of joining
status of membership (member, associate etc)
how membership is achieved (evaluation, examination, is membership restricted or open to all?)
Where membership has been attained through an evaluation or examination and you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated.
56

&
BAPRAS Brilish Association ol Plastic Roconstructive and Aesthetic Surgeons
University Hosp i t a l s l i l ZE^ Coventry and Warwickshire
NHS Trust
Certificate of Attendance
This is to certify that
Sivakumar Gopalswamy
attended the
Master Class on Breast Aesthetic and Reconstructive Surgery
on 8th July 2010
at the National Motorcycle Museum, Solihull, UK
5 CME credits accredited by BAPRAS
Organised by
Department of Plastic Surgery University Hospital
Coventry, UK
Mr On^f'Osmani Organiser
Mr Alan Park Chairman
57

Teaching and trainingTeaching timetables Where you have undertaken a number of roles provide details for each post or role, indicate the level of the teaching.
Where teaching is not formal (timetabled) indicate how you participate in teaching.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated.
Lectures Please include evidence showing the audience and topics covered, such as posters advertising event, educational timetable from trust education centre, letter from education centre indicating your involvement in specialty trainee formal education programme.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information
continuing professional development
teaching and training
communication skills.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated.
58

Feedback or evaluation forms from those taught Please provide copies of feedback from teaching events you have participated in.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information
continuing professional development
teaching and training
leadership
relationships with colleagues
communication skills.
All evidence in this area must be validated and anonymised for individual patient data.
Letters from colleagues You can use copies of letters from colleagues to demonstrate similar information to feedback forms (see above).
All evidence in this area must be validated and anonymised for individual patient data.
Attendance at teaching or appraisal courses Please provide documentary evidence that you attended the courses and information on the content of the course including whether they were generic or aimed at medical professionals.
59

) S
iva
kum
ar
Go
pa
lsw
am
y -
Te
ach
ing
eva
lua
tio
n.d
oc
Pa
ge
1
Tea
chin
g E
valu
atio
n F
orm
I
AM
A
H-^
V
k^g
S
TU
O^
O-
T
(Pos
t/Des
igna
tion)
I
AT
TE
ND
ED
A (
Ple
ase
circ
le):
^f
tS
r Q
ui
M ,
Q_
Tit
le
By
H t
G
oP
A L
$>
&F
\M W
Typ
e o
f P
rese
ntat
ion
Fee
dbac
k S
mal
l G
roup
Le
ctur
e (Z
L-/
/NM
C
Su
bje
ct
Mod
e o
f P
rese
ntat
ion
Str
uct
ure
of
pres
enta
tion
Bor
ing
Poo
r
Cla
rity
of
pres
enta
tion
1 O
paqu
e
Con
tent
of
pres
enta
tion
1 2
Ade
quat
e
Det
ail o
f pr
esen
tatio
n 1
2 To
o li
ttle
We
re e
xpla
natio
ns
adeq
uate
?
Did
th
e se
ssio
n in
vite
pa
rtic
ipat
ion?
H
ow w
ould
you
ra
te y
our
know
ledg
e of
th
e su
bje
ct b
efo
re t
he
pres
entio
n?
How
wou
ld y
ou r
ate
you
r kn
owle
dge
of
the
sub
ject
aft
er
the
pres
entio
n?
How
muc
h of
th
e su
bje
ct d
o th
ink
you
will
re
tain
ove
r th
e lo
ng
term
? I
wou
ld h
ave
been
b
ett
er
off
sp
endi
ng
time
in t
he
libra
ry
1 N
o
Thr
eate
ning
Ze
ro
©
No
chan
ge
1
Ver
y li
ttle
Of
cour
se!
I w
ould
rec
omm
end
this
1
2 se
ssio
n to
my
colle
ague
s -
. .
, '
^ C
erta
inly
not
4 (3
en
gagi
ng
©
5
Exc
elle
nt
Q
Cle
ar
ft ©
3 3
4 iS
S
^ E
5.
^ E
xces
sive
Ver
y cl
ear
4 F
<&
E
ngag
ing
Lots
©
Lots
mor
e
Lo
ts'
* C
D
Cer
tain
ly n
ot
o W
ith
ou
t he
sita
tion
^^
^^
^^
o ^^
iro^
tt:^
v
—^
os
^
60

Participation in assessment or appraisal and appointments processes
You may provide the following types of evidence to support this area:
copies of invitations to appraisals or assessments including attendance at appraisal/assessment courses
evidence of participation in the Deanery ARCP or RITA processes
evidence of participation in appointments for trainees (including invitations to participate and interview panel information, including attendance at interview and appointment related courses).
You can use these documents to demonstrate:
contribution to postgraduate and continuing medical education activity, locally and nationally
any responsibilities which relate to a special interest
participation in administration, management duties
participation in teaching and training
communication, partnership and teamwork
relationships with colleagues (including giving feedback)
leadership.
All evidence in this area must be validated.
61

Domain 2 – Safety and quality
Participation in audit, service improvementAudits undertaken by applicant You should provide evidence of the five stages of the audit process:
1. Definition of criteria and standards
2. Data collection
3. Assessment of performance against criteria and standards
4. Identification of changes (alterations to practice)
5. Re-evaluation
Evidence you could supply includes:
audit reports (collections of data alone are not considered as a full clinical audit)
publications
submissions to ethics committee (not satisfactory alone)
presentations of audit work (see above for details required for presentations)
letter from audit or clinical governance lead confirming participation in audit or governance activities
guidelines produced to reflect lessons learned within audit
notes from self-reflective diaries.
You can use these documents to demonstrate:
the types and complexity of cases you are involved in
triangulation with logbook information continuing professional development
communication, partnership and teamwork
relationships with colleagues, patients
leadership
62

ISSN 2042 779 ClinicalAudits.com
Abstract
Aims - The purpose of this audit was to analyse current patterns of GP referrals for thyroid ultrasound in our institution and thus to determine whether these referrals conform to the recent recommendations published by the British Thyroid Association.
Methods - For this audit, data was collected retrospectively for all patients who undenvent thyroid ultrasound examination in our radiology department from November 2010 to November 2011 (12 months period). Spectrum of clinical indications used by GPs to initiate thyroid ultrasound was analysed, and the appropriateness of such referrals was measured against the set of recommendations adopted from the UK Thyroid Association consensus of opinion. 100% compliance was proposed as the target.
Results - Total of 499 patients who unden/vent thyroid ultrasound scan in the set time period were identified. 105 (21%) patients were referred by GPs. Of these, 102 (97.2%) of GP referrals were considered as reasonably acceptable, whereas compliance fell short of the target by 2.8% owing to 4 patients referred by their GP inappropriately.
Conclusions - Although the observed compliance rate with audit criteria was reasonably high at 97.2 %, the target of 100% was not achieved. Thus, this audit highlighted the potential need to improve the quality of GP referrals for thyroid US, A number of changes and a reaudit in 12 months time to evaluate their effect were proposed accordingly.
Introduction
Currentiy, iocal arrangements at our institution permit open access referrai for thyroid Ultrasound (US) from general practitioners (GP). While we recognise that the traditional referral pathways may still be of value, this practice finds increasingly limited support in the literature and current UK consensus of opinion1"4. Furthermore, there is a growing belief that initiation of thyroid US by GPs may cause a delay in the diagnosis of cancer when US is requested inappropriately.
Because primary care thyroid US requests comprise a significant proportion of the workload in our radiology department, we felt that there was a need to assess the trends and appropriateness of GP referrals for thyroid US in our institution, which was the focus of this audit.
Aims
This audit aims to analyse current patterns of GP referrals for Thyroid US in our institution, and thus to determine whether such referrals conform to the recommendations of the UK consensus of opinion published by the British Thyroid Association in 2007. RADIOLOGY DEPARTMENT
NEWHAM UNIVERSITY HOSPITAL NHSTRUST GLEN ROAD, PLAISTOW 'ONDON E13 8SL
I confirm this is true and accurate record 2 Dr MD, FRCR Consultant Radiologist Barts Health NHS Trust, Newham University Hospital Glen Road, Plaistow London E13 SSL
@bartshealth.nhs.uk 63

ISSN 2042-4779 ClinicalAudits.com
Abst rac t J
Aims - To complete an audit cycle by re-audit of the diagnostic yield of locally performed ultrasound ( US ) guided thyroid fine-needle aspiration (FNA) one year after the initial audit, and thus to evaluate the trends since the first round, and ensure consistency ofthe procedure performance in our institution.
Methods - For this re-audit, we retrospectively analysed success rates of US-guided thyroid FNA biopsies performed in 146 patients in our department over 12-months period (November 2010 to November 2011). The findings were measured against standards based on the literature and results of the initial audit which had previously assessed institutional performance in 221 patients over 16-months period (September 2008 to January 2010).
Results - Total of 146 US guided FNA biopsies performed in the set time period were identified. FNA retrieved diagnostic material in 91.5% and 85.1% of solid and cystic thyroid nodules respectively, which is a reasonable level of performance when measured against predetermined targets (80% and 70% for solid and cystic thyroid nodules). In addition, improvement trends in the success rates were observed since the first round.
Conclusions - The re-audit demonstrated satisfactorily high tevel of performance well above predetermined targets. Although no changes need to be made based on the result of the audit, further audit is proposed to encourage the current trends.
Re-audit of Ultrasound guided Thyroid Fine Needle Aspiration success rates: maintaining trends.
Introduction
Ultrasound guided fine-needle aspiration (FNA) remains the mainstay in the initial workup of thyroid nodules and is routinely performed in our radiology department. Clearly, maintaining high success rate of thyroid FNA is important and will inspire confidence amongst both the referring clinicians and patients. By contrast, insufficient specimen is undesirable because it triggers a repeat FNA causing delay in the diagnosis and treatment in addition to amplified patient's anxiety and increased workload. Yet, adequate samples are not always attainable. It is widely acknowledged that FNA adequacy rates vary depending on several factors including the operator's skill, techniques used, and intrinsic nature of the thyroid nodule. Thus, we believe that al! efforts should be made to maintain and improve the success rates of thyroid FNA, which was the focus of this audit.
The initial audit analysed success rates of thyroid FNA performed in 221 patients over 16-months period (September 2008 to January 2010), revealing satisfactory levei of ^, performance, with an overall technical success rate of 83%, including 88% and 78 % J ^ diagnostic yield for solid and cystic nodules respectively. However, although the ^ o } standards were met, it was felt that there was a room for further improvement through J ^ * optimisation of techniques for sample retrieval combined with amplified collaborations >C J* with pathologists and clinical colleagues. ^ / ^ <£?
I confirm this is true and accurate record 2 /S o ^ $?$' Dr MD, FRCR Consultant Radiologist A K \hs tf^^S'S* Barts Health NHS Trust, Newham University Hospital y ^ ^ ^ ^ ^ Glen Road, Plaistow London E138SL W tFjf&^f
[email protected] - # Q / ^ 64

multi disciplinary working.
All evidence in this area must be validated.
Reflective diaries For details of what to include please see NHS clinical governance support information.
You can use this document to demonstrate
triangulation with logbooks
relationships with colleagues
your recognition of the limits of your professional competence
handling of critical incidents or complaints
how you have changed your practice in the light of experiences (part of audit).
As this evidence is self produced for its content to be given weight it must be supported or triangulated by other evidence.
Service Improvement and clinical governance meetings This area could be demonstrated in a number of ways including:
invitations to attend meetings
minutes of meetings demonstrating your attendance and participation in the meeting.
You can use these documents to demonstrate:
communication, partnership and teamwork
relationships with colleagues
leadership
multi disciplinary working
participation in audit or clinical governance.
All evidence in this area must be validated and anonymised for individual patient data.
65

Safety Health and safety Please provide evidence to support awareness and following Health and Safety requirements.
This can be demonstrated by:
declaration of health on your application form
attendance at appropriate course
involvement in infection control (membership of committees etc)
logbook information on infections
audit on infections and subsequent changes in activity.
66

Domain 3 – Communication, partnership and teamwork
Communication Colleagues Please provide evidence to support your communication with colleagues, both within your immediate team and the
wider team (including non clinical).
This can be demonstrated by:
letters from colleagues (examples of shared cases or “To whom it may concern letters” or testimonials)
letters of correspondence between you and your colleagues, demonstrating collaboration over management of patient care across multidisciplinary teams
management – including organising staff rotas
presentations
copies of appraisals or references written for colleagues (these must be anonymised with relation to colleague data).
You can use these documents to demonstrate:
communication, partnership and teamwork
relationships with colleagues
leadership
multi disciplinary working
participation in directorate and management meetings
honesty and objectivity.
All evidence in this area must be validated.
67

Patients This area could be demonstrated in a number of ways including:
thank you letters and cards from patients
letters from colleagues (examples of cases shared or “To whom it may concern letters” / testimonials)
complaints and responses to complaints.
This may include complaints received against your department or a colleague where you have been involved in the resolution. This is to demonstrate how you handle complaints. Having a complaint made against you will not adversely influence your application. You must anonymise colleague information from this evidence.
360° feedback.
You can use these documents to demonstrate:
communication
relationships with patients
honesty and integrity
protecting patient confidentiality.
All evidence in this area must be anonymised for individual patient data.
68

Partnership and teamwork Working in multidisciplinary teams This area could be demonstrated in a number of ways including:
invitations to attend meetings
minutes of meetings demonstrating your attendance and participation in the meeting
job plans which indicate this as a duty
appraisals which include this information.
You can use these documents to demonstrate:
communication, partnership and teamwork
relationships with colleagues
leadership
multi disciplinary working.
All evidence in this area must be validated and anonymised for individual patient data.
Management and leadership experience This area could be demonstrated in a number of ways including:
invitations to attend meetings
minutes of meetings demonstrating your attendance and participation in the meeting
job plans which indicate this as a duty
appraisals which include this information.
You can use these documents to demonstrate:
communication, partnership and teamwork
relationships with colleagues
leadership
management skills.
All evidence in this area must be validated and anonymised for individual patient data.
69

Chairing meetings and leading projects This area could be demonstrated in a number of ways including:
invitations to attend meetings
minutes of meetings demonstrating your attendance and participation in the meeting
job plans which indicate this as a duty
appraisals which include this information
project reports
letters from colleagues
publications or presentations.
You can use these documents to demonstrate:
communication, partnership and teamwork
relationships with colleagues
leadership
multi disciplinary working
participation in directorate and management meetings
continuing professional development.
Where you have not provided evidence of success in an examination that is a requirement of the CCT curriculum, evidence in this area may contribute to your demonstration of equivalent knowledge.
All evidence in this area must be validated and anonymised for individual patient data.
70

Domain 4 – Maintaining trust
Acting with honesty and integrity Honesty and integrity You can demonstrate this with:
the declarations on your application form
statements from your referees
appraisal forms
having no restrictions on your registration (UK based doctors)
Certificate of Good Standing (overseas based doctors).
Equality and human rights (including disability, human rights, race, religion and ethnicity awareness and equal opportunities)
You can demonstrate this with:
evidence of attendance at relevant courses (please provide details of course content)
feedback from patients and colleagues
statements from your referees
testimonials.
Data protection You can demonstrate this with:
attendance at relevant courses (please provide details of course content)
feedback from patients and colleagues
your application and evidence being appropriately anonymised.
71

Relationships with patients Testimonials and letters from colleagues You may include “To whom it may concern letters”.
All evidence in this area must be anonymised for individual patient data.
Thank you letters, cards from colleagues and patients Please ensure that these are anonymised (for individual patient data).
Complaints and responses to complaints This is to demonstrate how you handle complaints. Having a complaint made against you will not adversely influence your application.
You may include complaints received against the department within which you worked or one against a colleague where you have been involved in the resolution.
You may provide a reflective diary of how you would handle a hypothetical complaint.
All evidence in this area must be anonymised for individual patient data.
72