Embed Size (px)
Citation preview

Received 07/14/10Revised 07/16/10
Accepted 09/19/11
Applying Buddhist Practicesto Recovery: What I Learned FromSkiing With a Little Buddha Wisdom
]ane Warren
The author describes how 5 Buddhist practices—enlightenment, compassion,acceptance, mindfulness/meditation, and the spiritual community—can serveas a foundation for an integrated recovery model that incorporates numerousperspectives from the 12-step program of Alcoholics Anonymous. An applicationof the model illustrates how it is applied to real-life recovery.
Keywords: Buddhism, spirituality, recovery, meditation, mindfulness
The number one public health enemy in the United States is substance abuse.Sixty-one million Americans smoke, 15 million abuse prescription drugs,at least 20 million abuse alcohol, and consequences range from problem-atic to life threatening (Califano, 2007; Merta, 2001). Because of substanceabuse, approximately 85,000 deaths occur each year in the United Stateswith estimated costs of more than $185 billion (Saitz, 2005). The abuse ofprescription drugs is currently the fastest growing drug problem in theUnited States (Substance Abuse and Mental Health Services Administra-tion [SAMHSA], 2010). Alcohol use and abuse cross the life span from theyoung to the elderly (Barnes et al., 2010; Borsari, Murphy, & Barnett, 2007;Masten, Faden, Zucker, & Spear, 2009; Saitz, 2005; SAMHSA, 2009; Schaus etal., 2009). Abuse of substances, including the less stigmatized consumptionhabits such as money, food, and work, can be devastating to individualsand families (Anderson, 2008; Bliss & Pecukonis, 2009; Kalischuk, 2010;Schaffer, Jeglic, & Stanley, 2008; Singletary, 2009; Warren, Nunez, Klepper,Rosario, & King, 2010).
How does the person in recovery maintain an enlightened way of beingwhen surrounded by suffering, temptafions, and opportimifies to relapse? Inthis article, I present a brief overview of addictions and offer an integratedmodel to support recovery. Five Buddhist practices serve as the founda-tion for an integrated recovery model. Stories and perspectives from bothBuddhism and Alcoholics Anonymous (AA; 1976) are interwoven into themodel to illustrate some of the similarities in the two perspectives. A first-person narrative. Lessons From Skiing, is offered to demonstrate how theideas from the model can be applied in real life.
Jane Warren, Department of Professional Studies, University of Wyoming. Correspondence concerningthis article should be addressed to Jane Warren, Department of Professional Studies and Counseling,University of Wyoming, Department 3374,1000 East University Avenue, Education Building, Room338, Laramie, WY 82071 (e-mail: [email protected]).
© 2012 by the American Counseling Association. All rights reserved.
34 journal of Addictions & Offender Counseling • April 2012 • Volume 33

Addiction: A Moving Target
Throughout history and cultures, attitudes about substance use and abusehave changed (Bliss, 2009; Merta, 2001; Miller & Bogenschultz, 2007; My-ers, 2002; Stolberg, 2009). These changing beliefs often create myths andmisconceptions about the nature of addiction. In the 1930s, individualswho were addicted were considered to be morally defective and lackingin willpower (Bliss, 2009; Myers, 2002). Alcohol taxes were labeled as "sin"taxes. Persons with addictions experienced shame and isolation and werestigmatized. Although attitudes about substances change (Stolberg, 2009),addictions and persons with addictions continue to be viewed negativelyin the treatment world (Adams & Madson, 2007; Lay & McGuire, 2008;Myers, 2002). The person with an addiction is subject to stigma, meaningthat the focus is placed on the alleged defects of an individual's status,physical characteristics, or character Stigma evolved originally to definea lower moral status of a person or group of persons (Lay & McGuire,2008). Negative attitudes can manifest in a belief that the person with theaddiction is lazy and carmot fully recover
One stigma-shattering event was the establishment in the late 1930s ofAlcoholics Anonymous (AA) as a community of support for individualswho were struggling with alcoholism. AA was a fellowship of men andwomen who, through sharing their experiences, strengths, and hope, wouldbe able to solve their common problem and help others to recover (AA,1976). "We are not an organization in the conventional sense of the word.There are no fees or dues whatsoever The only requirement is an honestdesire to stop drinking" (AA, 1976, p. xiii). AA is considered an effectivetreatment by many and offers support for attaining and maintaining sobrietywith a wide range of addictions, such as narcotics, pills, cocaine, food, andsex (Okundaye, Smith, & Lawrence-Webb, 2001; Stevens & Smith, 2009). Inmany ways, AA opened the door to viewing recovery as a possibility andincluded others who shared commitment and compassion. Addiction wasnot viewed as a moral weakness or sin.
Currently, research continues to identify biological, environmental, andgenetic factors that contribute to the development and progression of ad-diction. Addiction is often defined as a chronic, relapsing brain diseasecharacterized by unending drug seeking and use, despite life-threateningconsequences. Drugs change the structure and functions of the brain, andthese long-lasting brain changes lead to the harmful behaviors seen inpeople who abuse drugs (National Institute on Drug Abuse, 2007). Ac-cording to the Diagnostic and Statistical Manual of Mental Disorders (4th ed.;American Psychiatric Association, 1994), substance dependence includesalcohol, drugs, food, gambling, and sex. To be considered addictive, thebehavior includes increased tolerance, withdrawal, and increased quantityand frequency of use (Merta, 2001). Despite the enormous personal andsocial costs of addictions, there is little consensus regarding the most ef-
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 35

fective treatments for enabling recovery (Bliss, 2009; Fruett, Nishimura, &Priest, 2007).
Although there are differing views of addictions, there is little debate aboutthe importance of recovery, the process of sobering up or sobriety from asubstance or experience that is life threatening and seemingly unstoppable.The traditional disease model focuses on powerful biological determinantsof addictions, supports medical-based interventions, and considers addic-tions that are rooted in biological factors beyond an individual's control(Marlatt, 2002). Although the biological factors are important, they mayrepresent only a part of a more integrated perspective (Bliss, 2009; Hes-selbrock, Hesselbrock, & Epstein, 1999).
Integrated Recovery
Integrative models of recovery can address many factors operating withinand outside of any person's life (Warren, Stech, Douglas, & Lambert, 2010). Astrengths-based, multidimensional approach is needed (Moxley & Washing-ton, 2001; Pruett et al., 2007). Okundaye et al. (2001) described recovery as aholistic, continuous process of becoming, involving others, using collabora-tion, creating growth without limits, and emphasizing five key strengths: (a)empowerment, (b) suspension of disbelief, (c) dialogue and collaboration, (d)membership, (e) synergy, and (f) regeneration. Bliss (2009) suggested that AAprovides a hoHstic perspective for recovery given how it supports
reduced egocentrism, higher levels of functioning, increased awareness, and im-proved relationships with self, others, and . . . although AA explains the etiologyof alcoholism as being a threefold illness (physical, mental, and spiritual), it [has ajstrong emphasis on spirituality in the recovery from alcoholism suggest[ing] the roleof spirituality cannot be discounted in examining the etiology of alcoholism, (p. 17)
Spirituality and Recovery
Integrated recovery usually includes spiritual dimensions. Spiritualityhas been described as the integration of the whole of human life includ-ing biological, mental, social, and spiritual aspects of each person's life(Myers, Sweeney, & Witmer, 2000). A number of scholars have suggestedthat spirituality is the core of Wellness (Cashwell, Bentley, & Bigbee, 2007;Myers & Sweeney, 2008). The Holistic Flow Model of Spiritual Wellnessintegrates "companionship, mind, life's work, emotions, body, beauty, andreligion" (Purdy & Dupey, 2005, p. 98) and considers spirituality as thecentral life energy (fiow) "from which individuals act, feel, think, and feel"(p. 98) and is "irmate, ever present" (p. 98), perpetuating transcendence,and embracing change. When an individual is in balance, "the spirit islike water, moving freely" (Purdy & Dupey, 2005, p. 98) and the personexperiences connectedness, compassion, faith, and meaning. According toCashwell et al. (2007),
36 Journal of Addictions & Offender Counseling • April 2012 • Volume 33
spirituality is a developmental process that is both active and passive wherein beliefs,disciplined practice, and experiences are grounded and integrated to result in increasedmindfulness (nonjudgmental awareness of present experiences), heartfulness (experi-ence of compassion and love), and soulfulness (connections) beyond ourselves, (p. 67)
The definition of spirituality created by Cashwell et al. (2007) succinctlyillustrates an integrated perspective and nicely parallels a Buddhist phi-losophy. A Buddhist perspective offers a nonjudgmental spiritual modelthat is useful for understanding addictions (Groves & Farmer, 1994). Maria tt(2002) presented a concise overview of how several Buddhist principles canbe useful in the treatment of addictive behaviors, including mindfulnessmeditation, the middle way, impermanence, compassion, and the eightfoldpath. Although Buddhism has been described as an organized religion,for many scholars it is considered "more of a philosophy than a religion"(Kumar, 2002, p. 41). For this article. Buddhism is considered an integratedway of perceiving and being.
Buddhism
Buddhism began with the awakening of Gautama Siddhartha (563-483B.C.), known as Buddha, who was born to a wealthy family and shelteredfrom suffering. When he went into the world, he "saw a sick person, anold woman, a dead man, and a mendicant" (Batchelor, 1999, p. 19). Theperson who begged (mendicant) relied only on charity, owned no property,served the poor, and did not seem to suffer. Buddha wondered why somesuffered and others did not. He embarked on a journey seeking wisdomfrom different spiritual practices and teachers hoping to find solutionsto suffering. After 7 years of wandering, while meditating under a Bodhi(Bodhi-enlightenment) tree, he realized that although negative conditionsare inevitable, the suffering can be managed, as was evident with themendicant (Warren, Klepper, Lambert, Nunez, & Williams, 2011, p. 135).
Buddha means an enlightened being (Warren et al., 2011, p. 136). An en-lightened being has realized that there is a way to manage suffering. Theway to respond to suffering is to follow the four noble truths: (a) sufferingis inevitable, (b) the cause of suffering is craving (attachment), (c) suffer-ing can be managed, and (d) the eightfold path and the middle way. Theeightfold path is having the right (wise) view, intention, speech, action,livelihood, effort, mindfulness, and concentration (Gyatso, 2005; Kumar,2002). The middle way balances demands, desires, attachments, and crav-ings with reasonable limitations (Marlatt, 2002; Warren et al., 2011).
By engaging the senses, concentrating focus, and letting go, an experienceof inner peace is attained (Simpkins & Simpkins, 2001). The mind can betrained to offer love, kindness, compassion, and tolerance. This trained andpeaceful mind is described as nirvana, whereas its absence, samsara, is themind of daily living and suffering (Groves & Farmer, 1994).
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 37
Integrated Recovery Model
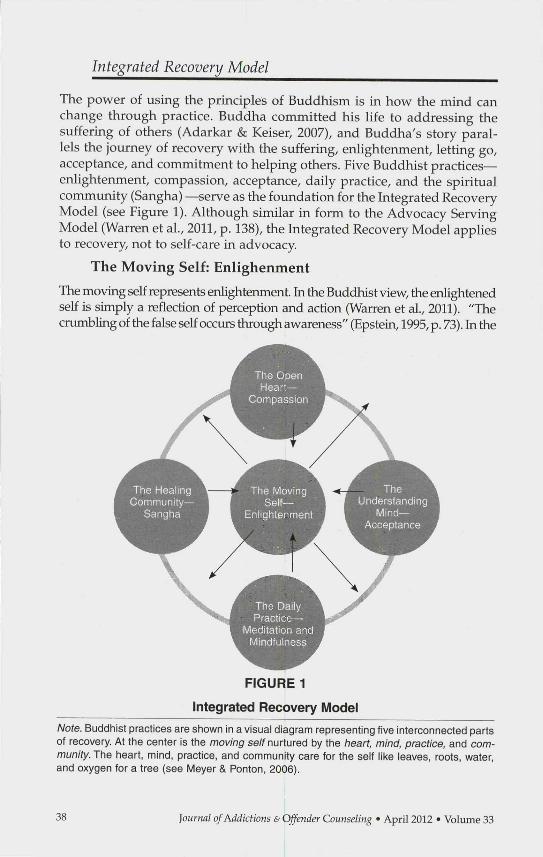
The power of using the principles of Buddhism is in how the mind canchange through practice. Buddha committed his life to addressing thesuffering of others (Adarkar & Keiser, 2007), and Buddha's story paral-lels the journey of recovery with the suffering, enlightenment, letting go,acceptance, and commitment to helping others. Five Buddhist practices—enlightenment, compassion, acceptance, daily practice, and the spiritualcommunity (Sangha) —serve as the foundation for the Integrated RecoveryModel (see Figure 1). Although similar in form to the Advocacy ServingModel (Warren et al, 2011, p. 138), the Integrated Recovery Model appliesto recovery, not to self-care in advocacy.
The Moving Self: Enlighenment
The moving self represents enlightenment. In the Buddhist view, the enlightenedself is simply a reflection of perception and action (Warren et al., 2011). "Thecrumbling of the false self occurs through awareness" (Epstein, 1995, p. 73). In the
FIGURE 1
Integrated Recovery iVIodel
Note. Buddhist practices are shown in a visual diagram representing five interconnected partsof recovery. At the center Is the moving se/f nurtured by the heart, mind, practice, and com-munity. The heart, mind, practice, and community care for the self like leaves, roots, water,and oxygen tor a tree (see Meyer & Ponton, 2006).
Journal of Addictions & Offender Counseling • April 2012 • Volume 33

AA tradition, self-examination is essential to recovery when a fearless and moralinventory is made and shared with others (AA, 1976; Stevens & Smith, 2009).The mind stays closed when attached to perfection (Epstein, 1995). Opennesshelps the recovering person see beyond her or his own grandiose worldviewand provides a fiamework for understanding the impact of the addiction onthe self and on others. "Simple but not easy; a price had to be paid. It meantdestruction of self-centeredness" (AA, 1976, p. 14). The unaware person is likethe retired business man who relaxes in Florida complaining of the sad state ofthe nation (AA, 1976).
Recovery is about being humble: "As we awaken we discover that we arenot Hmited by who we think we are" (Kornfield, 2000, p. 55). The personin recovery must not become inflated by her or his sense of importance. Astory that demonstrates the impact of self-grandiosity is the Emperor Wuand the Bodhidharma. Emperor Wu ascended to his throne by overtak-ing the previous monarch. After a battle and while sitting in his garden,he had a sense of being small and unimportant. However, with this mo-mentary experience he also felt free. Feeling crowded by the walls of hislife around him, he sought wisdom from a famous wise man from India,Monk Bodhidharma. This monk was a legend. When the monk arrived, hewas dressed modestly and wanted no recognition. The emperor noticedthat while in the presence of the monk, his own thoughts became simple,like remembering the taste of vegetable soup. The emperor was seekinga deeper meaning of his own hfe, so he asked the Bodhidharma, "I havefunded many monasteries. What merit have I earned?" "No merit," saidthe Bodhidharma. For a moment, the emperor pulled back into his ego selfbut thought perhaps the monk did not understand. He then asked, "Whatis the point of your holy teaching?" The monk responded, "Vast emptiness.Nothing holy." Then the emperor asked, "Who are you, standing in frontof me?" "I don't know," said the Bodhidharma (Tarrant, 2004). The monkseemed not to be overly attached to anything. The story represents thepotential traps in seeking recognition and praise, which contributes to thefear that our lives are insubstantial and to the habit of trying to measureourselves. The humbled self does not demand an identity and, thus, canopenly love others. Opening the heart to the world can mean witnessingharsh realities of human despair and destruction from addictions.
The Open Heart: Compassion
The open heart culminates in compassion. Compassion is unconditionalacceptance of others and self. Rogers (1957) epitomized compassion whenhe wrote, "I feel neither approval nor disapproval. . . simply acceptance"(p. 98). He set the stage for the essential elements of the healing relationshipwith unconditional positive regard, empathetic understanding, genuine-ness, and congruence. In recovery, compassion is evident in the healingpowers of caring relationships (Breggin, 2008; Rogers, 1957). Contact withthose who suffer allows intrinsic understanding of life's difficulties such
journal of Addictions & Offender Counseling • April 2012 • Volume 33 39

as poverty, discrimination, illness, and oppression (Moxley & Washington,2001; Roysircar, 2009; Warren et al., 2011). Compassion is "active caring"(Kumar, 2002, p. 42), and one single empathie encounter can have such asubstantial impact that it can lead a person to change (Miller, 2000). "In-dividuals in recovery can be valorized as heroes" (Moxley & Washington,2001, p. 256). How genuine caring affects others is not clearly known; itmay simply be a relationship condition that enables corrective emotionalexperiences and allows another to be an "active self-healer" (Greenberg,Watson, Elliott, & Bohart, 2001, p. 383).
Compassion in recovery is giving a voice to pain, moving beyond thewalls of treatment settings and going into jails, homeless shelters, homes,courts, and AA meetings (Warren et al., 2011). Stories of recovery can bepainful and difficult.
The alcoholic is like a tornado roaring his way through the lives of others. Heartsare broken. Sweet relationships are dead. Affections have been uprooted. Selfish andinconsiderate habits have kept the home in turmoü. We feel a man is unthinking whenhe says that sobriety is enough. He is like the farmer who came up out of his cyclonecellar to find his home ruined. To his wife he remarked, "Don't see anything the matterhere. Ma. Ain't it grand the wind stopped blowin?' (AA, 1976, p. 82)
The recovering person listens compassionately to the stories of othersand from those stories empowers change in self and others (Moxley &Washington, 2001). Compassion for others fosters acceptance.
The Understanding Mind: AcceptanceThe understanding mind is manifested in acceptance. Buddha suggestedthat attachment creates suffering. Expectations imprison. With acceptance,the metaphorical cage of expectations transforms, analogous to being letout to a large and open meadow where there are no walls, no structuralprotections, only light, space, and openness, which provide no answers(Tarrant, 2004). With the right view, action, effort, and focus, a peaceful wayof being results, as if each day were the first day of life. With this perspec-tive, the recovering person can move with tranquility. Although sufferingis inevitable, the enlightened view perceives suffering as simply part ofliving (Groves & Farmer, 1994). Enlightenment is realizing that peace andsuffering are "One" (Simpkins & Simpkins, 2001, p. 6), and every feelinghas an opposite. Avoidance of uncomfortable feelings can increase cravings(Cleveland & Harris, 2010) whereas acceptance is experiencing a feelingfully without avoidance (Philippot & Segal, 2009).
And acceptance is the answer to all of my problems today. When I am disturbed, itis because I find some person, place, thing, or situation . . . unacceptable to me, andI can End no serenity until I accept that person, place, thing or situation as beingexactly the way it is supposed to be at this moment. (AA, 1976, p. 449)
A story reflecting the experience of acceptance is regarding a powerfulprince who hated the wind (Warren et al., 2011). Because of his power hecould demand his desires. He wished the annoying wind to be gone. The
4Ö Journal of Addictions & Offender Counseling • April 2012 • Volume 33

wind disappeared. The prince felt satistied. Soon, however, no clouds came,no rain fell, and all was dying. The prince then begged for the wind to re-turn. The wind returned (Korntield, 1993). As in life, both pain and joy exist;both are needed. Acceptance that change needs to happen is foundationalto recovery. Recovery is change (Groves & Farmer, 1994).
It takes courage (Goud, 2005) to change old habits and recognize howpeople grasp, cling, judge, and fear. "The shame, fear, and guilt associatedwith alcoholism and other drug addictions could be overcome by acceptanceand admission of unmanageability of an addictive life-style" (Okundayeet al., 2001, p. 76). Habits are like the story of the frog and the scorpion.The scorpion, who always bites and kills frogs, asked the frog to take himacross the pond. The frog inquired, "But would you not kill me, that is inyour nature?" The scorpion responded he would not, given if he did, theywould both drown. The frog agreed and upon moving across the pond,the scorpion bit him and they both drowned. While going down, the frogasked the scorpion, "Why?" and the scorpion responded, "Because that iswhat I always do." Old habits, maps, fictions, and stories are like "bad art"(Tarrant, 2004, p. 169). Without change, death may result.
The person in recovery is wise to flow with life events. Suffering is not per-manent and is a transformational force. The Japanese word for a Zen monk isunsui, meaning clouds and water. Lives are similar to the rain, which nurturesthe world and ultimately tiansforms. "Eventually we flow, passing beyondintention, clinging to nothing, while nothing clings to us" (Tarrant, 1998, p.194). The Greek philosopher HeracHtus understood the experience of changewhen he said that we can never step in the same river twice nor meet the sameperson again; every moment is unique and not repeated (Korrifield, 2000).
In Buddhist thought, rigid attachment to limited goals and preferencesleaves one vulnerable to suffering (Robins, 2002). Assuming that a prob-lem should be easily solved or, conversely, that it cannot be solved, is ademand that can set up burnout or learned helplessness (Toporek, Lewis, &Crethar, 2009). "I must keep my magic magnifying mind on my acceptanceand off my expectation, for my serenity is directly proportional to my levelof acceptance" (AA, 1976, p. 452). Relapses, loss, stress, fear, and conflictare part of a sober life just as they are part of an addicted one (Moxley &Washington, 2001). Acceptance in recovery embraces every small step inthe direction of desired change even if it seems slow (Warren et al., 2011).The AA movement had 100 members in its 4th year (1939) of existence,and by 2007, the fellowship reported more than 1.2 million members in theUnited States (AA, 2007). The growth of AA took many years of incrediblepatience and effort; consequently, today "wherever you can find a liquorstore, you can find an AA group" (Stevens, & Smith, 2009, p. 290).
Daily Practice: Meditation and Mindfulness
Recovery is a daily practice. Lives are full of distractions, complications,and demands. Time is needed to breathe, quiet the mind, be in solitude.
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 41
and find beauty in Ufe. In Buddhism, meditation is one of the primary waysto bring about change (Groves & Farmer, 1994). Buddha purported that noone can attain Wellness and enlightenment without practicing meditation.With meditation there is "no purpose," (p. 71) only enhanced awarenessand mindfulness (Ray, 2004). The natural world meditates. In the fall, treesgo dormant. Bears hibemate. Humans can learn from nature.
Two common ways to meditate in the Buddhist tradition are samatha(concentration) and vipassana (insight). Samatha meditation focuses on oneidea to the exclusion of all else. This type of meditation can lead to mindful-ness—experiencing the world in an open way, cultivating awareness in daüyactivities such as walking, eating, and bathing. Vipassana meditation resultsin new views, like bringing a lamp into a dark room (Groves & Farmer, 1994).
Mindfulness meditation enables awareness and acceptance of thoughts,feelings, and physical sensations as they arise and allows recognition thatthey are impermanent. To acknowledge and accept rather than to modifyor suppress experiences enables nonjudgmental acceptance of moment-to-moment life events (Germer, 2005; Groves & Farmer, 1994; Kabat-Zinn, 1990,2003; Kumar, 2002; Marcus & Zgierska, 2009). Mindfulness skills can provideeffective coping strategies in the face of high-risk situations (Bowen et al.,2009; Carlson & Larkin, 2009; Witkiewitz, Marlatt, & Walker, 2005; Zgierska &Marcus, 2010). Kabat-Zinn (2003) considered mindfulness as a form of medi-cine for treating "dis-ease," which has been characterized as "three 'poisons':greed, hatred (aversion), and ignorance/delusion [unawareness]" (p. 145).
Mindfulness develops and deepens over time. Mindfulness is not aboutgetting anywhere or fixing anything; instead, it is an invitation to bewhere one already is and to know the inner and outer landscape of thedirect experience in each moment. Simpkins and Simpkins (2001) andBatchelor (1999) offer creative suggestions for mediation, yoga, andmind relaxation exercises, which are useful for any person in recovery.Mindfulness skills enhance Wellness (Baer, 2003; Marlatt, 2002; Robins,2002). Part of staying sober is the use of daily reminders through medi-tations, slogans, and readings: "One day at a time" and "Let go and letGod" focus the recovering person.
When we retire at night, we constructively review our day. Were we resentful, selfish,dishonest, or afraid? Do we owe an apology? Have we kept something to ourselveswhich should be discussed with another person at once? Were we kind and lovingtoward all? (AA, 1976, p. 86)
The Healing Community: Sangha
One of the most important strategies for maintaining recovery is connect-ing with others. Sangha means spiritual community and includes nature,art, and others (Warren et al., 2011). Cormectedness is being with others,breathing the same air and feeling the energy that together enables therecovering person to transcend the self and realize the interdependenceof all lives (Purdy & Dupey, 2005).
42 Journal of Addictions & Offender Counseling • April 2012 • Volume 33

Connecting to nature can be likened to a plant's need for water. Natureteaches acceptance, change, and perseverance, skills that are critical torecovery. There is guidance in nature, which can be witnessed easily. Rainforests teach of medicinal healings, deserts teach endurance, and wolvesteach resiliency. Nature teaches wisdom about life and nurtures the soul(Warren et al., 2011, p. 141; see also Elkins, 1995).
Art offers wisdom, perspective, and companionship (Adarkar & Keiser,2007; Tarrant, 2004). To apply art to recovery means being with art. Artteaches individuals to recognize perspective in paintings, musical perfor-mances, photographs, quilts, and dance (Warren et al., 2011). Books providedoors into colorful, light, and dark worlds that have not yet been person-ally experienced; however, these experiences may be faced eventually bymany individuals. Authors become sponsors when they share stories ofchange, hope, success. Poetry offers an alternative lens to see the world(Adarkar & Keiser, 2007) and allows the person in recovery to question, seethe invisible, and hear the silence of snow. Poet means "maker" and poetrynurtures the imagination (Tarrant, 1998, p. 231). For recovery, imaginationof what could be is critical (Warren et al., 2011).
Of course, the recovery journey includes peers and mentors who may besponsors, comembers in AA, or friends who will not let us lie (Moxley &Washington, 2001). Tarrant (2004) suggested that "to connect, to help, to beof use in this world, you have to walk with people. You have to let themact upon you also, and you won't remain unchanged" (p. 82). Throughcommunity, mentors emerge to guide individuals through blind spots andcoach them when they need to be encouraged (Warren et al., 2011).
Life will take on new meaning. To watch people recover, to see them help others, towatch loneliness vanish, to see a fellowship grow up about you, to have a host offriends—this is an experience you must not miss. (AA, 1976, p. 89)
Being awakened allows the heart to open as if it were the first day of life,just being born, not knowing anything, and experiencing it all (Kornfield,2000). To the wise heart, everything can make sense. Recovery is an inte-grating experience (Moxley & Washington, 2001) that includes the self, themind, the heart, the practice, and the community.
Practical Application of the Integrated Model:Lessons From Skiing
How to respond to a brain, risk factors, and a culture that nurtures over-consumption is a challenging task. As Buddha discovered, it is a dailyjourney of learning to being humble, living mindfully, nurturing accep-tance, feeling compassion, and connecting to comm^unity. I illustrate theIntegrated Recovery Model through a description of a personal 90-minute,cross-country skiing experience.
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 43

It was a cold winter day, quiet with a frozen silence and peace. As I moved on thetrail, I noticed all that I needed was right there. I was warm, moving, breathing, andwitnessing nature in its most innocent form. I was grateful that I carried little, notneeding big backpacks or complicated equipment. Traveling lightly eases any journey.Keep it simple. As I moved along lightly, I realized I was skiing like an athlete, movingfast, maybe considering racing, imagining becoming an Olympic star; then suddenly,I crashed into the snow-fUIed trailside. Pulling together my pride and lost ski poles,I realized I lost focus into grandiosity, thus fell. Stay humble and pay attention. Nowback on my feet moving along the trail, I heard the squirrels squealing with apparentfrustration that their home turf was being invaded. I pondered their predicament,feeling compassion for their situation. Thank you little squirrels for helping me to beaware of the impact I have on others. As I moved into the last 20 minutes of the trail,I felt hunger; my mind began to think of soup and crackers. Traveling lightly, I hadno treats. I embraced this hunger, imagining many who had no food. I felt Hfe. AsI pondered this little ski adventure, I realized that life lessons are everywhere. Theordinary is extraordinary, even if it is a squirrel. Keep it simple and only pack whatyou really need in life. Pay attention or you might stumble. Thinking you rule theearth can lead to a fall. Show compassion wherever you are. You are never alone. Thehealing community is everywhere. A 90-minute cross-country ski trail is a universe.
Although applying Buddhist practices to recovery may be helpful, thereare limitations. To impose personal values on anyone is an unethical practice(American Counseling Association, 2005). Buddhism could be negative forsomeone who may perceive it to be a religious ideology and in conflict withthe individual's own beliefs. Buddhist traditions date back more than 2,500years; thus, the ideas presented in this article are not representative of thewhole of Buddhism (Adarkar & Keiser, 2007; Kumar, 2002).
Integrating AA wisdom with the Buddhist philosophy could be problematicfor many individuals, especially if it is aligned alone with one philosophyor another. Each philosophy is a powerful and separate system, and someindividuals may not see the common ground of the different perspectives.U.S. society is plagued with many painful consequences of addiction inits varied forms. To accept that which we cannot change may be the man-tra for the serenity prayer; however for some, the words of the serenityprayer could be interpreted as minimizing the belief that these troublingconditions need to be changed. In fact, the acceptance of what cannot bechanged can work well with an integrated recovery model, which consid-ers holistic and potential changes in the mind, the heart, the community,and the self (Robins, 2002).
An important part of recovery is spirituality (Miller & Bogenschultz, 2007;Moxley & Washington, 2001). Problems with alcohol and drug use canhave a negative impact on a person's spiritual life (Wallace, 1996). Givenhow mindfulness and spirituality continue to be linked to sobriety andWellness (Bowen et al., 2009; Carlson & Larkin, 2009; Groves & Farmer,1994; Kabat-Zinn, 2003; Witkiewitz et al., 2005; Zgierska & Marcus, 2010),perhaps concepts from Buddhism could be considered beneficial to recovery.Multidimensional and longitudinal scientific studies of spirituality need todetermine which, if any, aspects of various spiritual models are related torecovery (Groves & Farmer, 1994; Miller & Bogenschultz, 2007).
44 journal of Addictions & Offender Counseling • April 2012 • Volume 33

The strengths of Buddhist practices, such as the use of compassion andmindfulness, can enhance joy in the smallest things in life, and these prac-tices "can lead to a greater sensitivity to the fullness of life. Rather thanrequiring constant stimulation or excitement, the mindful person findsrichness even in the mundane" (Cashwell et al., 2007, p. 72).
References
Adams, J. B., & Madson, M. B. (2007). Reflection and outlook for the future of addictions treat-ment and training: An interview with William R. Miller. Journal of Teaching in the Addictions,5, 95-109. doi:10.1300/J188v05n01_07
Adarkar, A., & Keiser, D. L. (2007). The Buddha in the classroom: Toward a critical spiritualpedagogy. Journal of Transformative Education, 5, 246-261.
Alcoholics Anonymous. (2007). AA fact file [Online]. Retrieved from http://aa.orgAlcoholics Anonymous (AA) World Services. (1976). Alcoholics Anonymous (3rd ed.). New
York, NY: Author.American Counseling Association. (2005). ACA code of ethics. Alexandria, VA: Author.American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders
(4th ed.). Washington, DC: Author.Anderson J. (2008, February 7). Craving the high that risky trading can bring. Retrieved at http: / /
www.nytimes.com/2008/02/07/business/worldbusiness/07trader.html_Baer, R. A. (2003). Mindfulness training as a clinic intervention: A conceptual and empirical
review. Clinical Psychology: Science and Practice, 10, 125-143. doi:10.1093/clipsy/bpg015Barnes, A. J., Moore, A. A., Xu, H., Ang, A., Tallen, L., Mirkin, M., & Ettner, S. L. (2010).
Prevalence and correlates of at-risk drinking among older adults: The project SHAREstudy. Journal of General Internal Medicine. Advance online publication. doi:10.1007/S11606-010-1341-X
Batchelor, M. (1999). Thorson's principles of Zen. London, England: Harper Collins.Bliss, D. L. (2009). Beyond the disease model: Reframing the etiology of alcohoHsm from a spiri-
tual perspective. Journal of Teaching in the Addictions, 8,10-26. doi:10.1080/15332700903396556Bliss, D. L., & Pecukonis, F. (2009). Screening and brief intervention practice model for social
workers in non-substance abuse practice settings. Journal of Social Work Practice in the Ad-dictions, 9, 21-40. doi:10.1080/15332560802646604
Borsari, B., Murphy, J. G., Barnett, N. P. (2007). Predictors of alcohol use during the first yearof college: Implications for prevention. Addictive Behaviors, 32, 2062-2086. doi:10.1016/j.addbeh.2007.01.017 PMID: 17321059
Bowen, S., Chawla, N., Collins, S. E., Witkiewitz, K., Hsu, S., Grow, J., . . . Marlatt, A. (2009).Mindfulness-based relapse prevention for substance use disorders: A pilot efficacy trial.Substance Abuse, 30, 295-305. doi:10.1080/08897070903250084
Breggin, P. R. (2008). Practical applications: 22 guidelines for counseling and psychotherapy.Ethical Human Psychology and Psychiatry, 10, 43-57. doi:10.1891/1559-4343.10.1.43
Califano, J. A. (2007). High society: How substance abuse ravages America and what to do about it.New York, NY: Perseus Books.
Carlson, B. E., & Larkin, H. (2009). Meditation as a coping intervention for treatment ofaddiction. Journal or Religion and Spirituality in Social Work: Social Thought, 18, 379-392.doi:l 0.1080 /15426430903263260
Cashwell, C. C, Bentley, D. P., & Bigbee, A. (2007). Spirituality and counselor Wellness. Journalof Humanistic Counseling, Education and Development, 46, 66-81.
Cleveland, H. H., & Harris, K. S. (2010). The role of coping in moderating within-day asso-ciations between negative triggers and substance use craving: A daily diary investigation.Addictive Behaviors, 35, 60-63. doi:10.1016/j.addbeh.2009.08.010
Elkins, D. (1995). Psychotherapy and spirituality: Toward a theory of the soul. Journal ofHumanistic Psychology, 35, 78-98. doi:10.1177/00221678950352006
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 45
Epstein, M. (1995). Thoughts without a thinker: Psychotherapy from a Buddhist perspective. Cam-bridge, MA: Perseus Books.
Germer, C. K. (2005). Mindfulness: What is it? What does it matter? In C. K. Germer, R. D.Siegel, & P. R. Fulton (Eds.), Mindfulness and psychotherapy (pp. 3-27). New York, NY: Guilford.
Goud, N. H. (2005). Courage: Its nature and development. Journal of Humanistic Counseling,Education and Development, 44, 102-.116.
Greenberg, L. S., Watson, J. C, Elliott, R., & Bohart, A. C. (2001). Empathy Psychotherapy, 38,380-384.Groves, P., & Farmer, R. (1994). Buddhism and addictions. Addiction Research, 1, 183-194.
doi:10.3109/16066359409109142Gyatso, G. K. (2005). How to solve our human problems: The four noble truths. New York, NY:
Tharpa Productions.Hesselbrock, M. N., Hesselbrock, V. M., & Epstein, E. E. (1999). Theories of etiology of alcohol
and other drug use disorders. In B. S. McCrady & E. E. Epstein (Eds.), Addictions: A compre-hensive guidebook (pp. 50-72). New York, NY: Oxford University Press.
Kabat-Zirm, J. (1990). Full catastrophe living: Using the wisdom of your body and mind to face stress,pain, and illness. New York, NY: Delta.
Kabat-Zirm, J. (2003). Mindfulness based interventions in context: Past, present and future.Clinical Psychology: Science and Practice, W, 144-156. doi:10.1093/clipsy/bpg016
Kalischuk, R. G. (2010). Co-creating life pathways: Problem gambling ancl its impact onfamilies. The Family Journal: Counseling and Therapy for Couples and Families, 18, 7-17 doi:10/1177/1066-480709357898
Kornfield, J. (1993). A path with heart. New York, NY: Bantam Books.Kornfield, J. (2000). Afler the ecstasy, the laundry. New York, NY: Bantam Books.Kumar, S. M. (2002). An introduction to Buddhism for the cognitive-behavioral therapist.
Cognitive and Behavioral Practice, 9, 40-43. doi:10.1016/S1077-7229(02)80038-4Lay, K., & McGuire, L. (2008). Teaching students to deconstruct life experience with ad-
dictions: A structured reflection exercise. Journal of Teaching and Addictions, 7, 145-163.doi:10.1080/15332700802269227
Marcus, M. T., & Zgierska, A. (2009). Mindfulness-based therapies for substance use disorders:Part 1. Substance Abuse, 30, 263265. doi:10.1080/08897070903250027
Marlatt, G. A. (2002). Buddhist philosophy and the treatment of addictive behavior. Cognitiveand Behavioral Practice, 9, 44-50. doi:10.1016/S1077-7229(02)80039-61
Masten, A. S., Faden, V. B., Zucker, R. A., & Spear, L. P (2009). A developmental perspectiveon underage alcohol use. Alcohol Research and Health, 31, 3-15.
Merta, R. J. (2001). Addictions coimseling. Journal of Counseling and Human Development, 33,1-15.Meyer, D., &: Ponton, R. (2006). The healthy tree: A metaphorical perspective of counselor
well-being. Journal of Mental Health Counseling, 18, 189-201.Miller, W. R. (2000). Rediscovering fire: Small interventions, large effects. Psychology of Addic-
tive Behaviors, 14, 6-18. doi:10.1037//0893-164X.14.I.6Miller, W. R, & Bogenschultz, M. P (2007). Spirituality and addiction. Southem Medical Journal, 100,433^36.Moxley, D. P., & Washington, O. G. (2001). Strengths-based recovery practice in chemical
dependency: A transpersonal perspective. Families in Society, 82, 251-262.Myers, J. E., & Sweeney, T. J. (2008). Wellness cotmseling: The evidence base for practice.
Journal of Counseling & Development, 81, 466-471.Myers, J. E., Sweeney, T. J., & Witmer, J. M. (2000). The wheel of Wellness counseling for well-
ness: A holistic model for treatment planning. Journal of Counseling & Development, 78,251-266.Myers, P. L. (2002). Beware of the man of one book. Journal of Teaching in the Addictions, 1,
69-90. doi:10.1300/J188v01n01_06National Institute on Drug Abuse. (2007). Drugs, brains, and behavior: The science of addiction.
Retrieved from http://www.drugabuse.gov/scienceofaddiction/sciofaddiction.pdfOkundaye, J. N., Smith, P., & Lawrence-Webb, C. (2001). Incorporating spirituality and the
strengths perspective into social work practice with addicted individuals. Journal of SocialWork Practice in the Addictions, 1, 65-82. doi:10.1300/J160v01n01_06
Philippot, P., & Segal, Z. (2009). Mindfulness based psychological interventions: Developingemotional awareness for better being. Journal of Consciousness Studies, 16, 285-306.
46 Journal of Addictions & Offender Counseling • April 2012 • Volume 33
Pruett, J. M., Nishimura, N. J., & Priest, R. (2007). The role of meditation in addiction recovery.Counseling and Values, 52, 71-84.
Purdy, M., & Dupey, P (2005). Holistic flow model of spiritual Wellness. Counselingand Values, 49,95-106.Ray, R. R. (2004). The pocket Tibetan Buddhism reader. Boston, MA: Shambhala.Robins, C. J. (2002). Zen principles and mindfulness practice in dialectical behavioral therapy.
Cognitive and Behavioral Practice, 9, 50-57. doi:10.1016/S1077-7229(02)80040-2Rogers, C. R. (1957). The necessary and sufficient conditions of therapeutic personality change.
Journal of Counseling Psychology, 21, 95-103.Roysircar, G. (2009). The big picture of advocacy: Counselor, heal society and thyself. Journal
of Counseling & Development, 87, 288-294.Saitz, R. (2005). Unhealthy alcohol use. New England Journal of Medicine, 352, 596-607.
doi:10.1056/NEJMcp042262Schaffer, M., Jeglic, E. L., (& Stanley, B. (2008). The relationship between suicidal behavior,
ideation, and binge drinking among college students. Archives of Suicide Research, 12,124-132.doi:10.1080/13811110701857111
Schaus, J. F., Sole, M. L., McCoy, T. P, Mullett, N., Bolden, J., Sivasithamparam, J., & O'Brien, M.C. (2009). Screerüng for high-risk drinking in a college student health center: Characterizingstudents based on quantity, frequency, and harms [Part of special issue on College drinking:New research from the National Institute on Alcohol Abuse and Alcoholism's Rapid Responseto College Drinking Problems Initiative]. Journal of Studies on Alcohol and Drugs, 16, 34 dd.
Simpkins, C. A., & Simpkins, A. (2001). Simple Tibetan Buddhism: A guide to tantric living.Boston, MA: Tuttle.
Singletary, M. (2009, May 7). National addiction to easy credit remains consumers' downfall. Re-trieved from http://www.washingtonpost.com/wp-dyn/content/article/2009/05/06/AR2009050603875.html
Stevens, P., & Smith, R. L. (2009). Substance abuse counseling: Theory and practice (4th ed.). Up-per Saddle River, NJ: Merrill Prentice-Hall.
Stolberg, V B. (2009). Historical images and reviews in the teaching of addictions studies.Journal of Teaching in the Addictions, 8, 65-83. doi:10.1080/15332700903396648
Substance Abuse and Mental Health Services Administration. (2009). Results from the 2008national survey on drug use and health: National findings (HHS Publication No. SMA 09-4434).Rockville, MD: U.S. Department of Health & Human Services.
Substance Abuse and Mental Health Services Administration, Office of Applied Studies.Qune 18, 2010). The DAWN report: Trends in emergency department visits involving nonmedicaluse of narcotic pain relievers. Rockville, MD: U.S. Department of Health & Human Services.
Tarrant, J. (1998). The light inside the dark: Zen, soul and the spiritual life. New York, NY: Harper Collins.Tarrant, J. (2004). Bring me the rhinoceros and other Zen Koans to bring you joy. New York,
NY: Harmony Books.Toporek, R. L., Lewis, J. A., & Crethar, H. C. (2009). Promoting systemic change through the
ACA advocacy competencies. Journal of Counseling & Development, 87, 260-268.Wallace, J. (1996). Theory of 12-step-oriented treatment. In F. Rotgers, D. S. Keller, & J. Mor-
genstern (Eds.), Treating substance abuse: Theory and technique. New York, NY: Guilford Press.Warren, J., Klepper, K., Lambert, S., Nunez, J., & Williams, S. (2011). Applying Buddhist
practices to advocacy: The advocacy serving model. Journal of Creativity in Mental Health, 6,132-148. doi:10.1080/15401383.2011.579876
Warren, J. A., Nunez, J., Klepper, K. K., Rosario, R., & King, G. R. (2010). Driving under theinfluence (DUD programs: One state's reality and all states' responsibility. Retrieved from http:/ /counselingoutntters.com/vistas/vistaslO/Article_82.pdf
Warren, J. A., Stech, M., Douglas, K. I., & Lambert, S. (2010). Enhancing case conceptualiza-tion through film: The addiction web. Journal of Creativity in Mental Health, 5, 1-15. doi:10.1080/15401383.2010.507663
Witkiewitz, K., Marlatt, G. A., & Walker, D. (2005). Mindfulness-based relapse prevention for alcohol andsubstance use disorders. Joumal of Cognitive Psychotherapy, 19,211-228. doi:10.1891 /jcop.2005.19.3.211
Zgierska, A., & Marcus M. T. (2010). Mindfulness-based therapies for substance use disorders:Part 2. Substance Abuse, 31, 77-78. doi:10.1080/08897071003641248
Journal of Addictions & Offender Counseling • April 2012 • Volume 33 47

Copyright of Journal of Addictions & Offender Counseling is the property of Wiley-Blackwell and its content
may not be copied or emailed to multiple sites or posted to a listserv without the copyright holder's express
written permission. However, users may print, download, or email articles for individual use.