Embed Size (px)
Citation preview
Most people would agree that eating is more than anecessity—it’s also a major social function. In light
of this, it’s remarkable that we often overlook oralhygiene, a critical area of personal health. Havingstrong, well-aligned teeth and proper bone structure ofthe face and jaw are essential ingredients for maintain-ing proper physical health. Not only do they provide theframework for chewing and consuming a varied diet,but they also impart confidence in the social aspects thatcome with enjoying a meal or beverage with others.
Most of us would also agree that a trip to the dentist,oral surgeon, or orthodontist isn’t our favorite way tospend time. Often, the procedures are expensive andpainful with less than optimal results. On top of that,treatments are often time intensive and, in the case oforthodontics, unattractive until the treatment ends. Oralhealth care professionals struggle with trial-and-errormethods that can cause patient anxiety and prolongalready time-consuming treatments. Fortunately, com-puter graphics and all the computer-aided drawing andmanufacturing (CAD/CAM), scanning, and imagingtechnology is changing dentistry. Simplicity, efficiency,and quality are factors any consumer and practitionercan appreciate.
Metal mouthEnter any middle or junior high school and you’ll find
kids with braces on their teeth. They sport the metal orclear plastic brackets with wires and colorful bands todecorate their mouths with a flourish. They don’t seemto mind that their pearly whites aren’t the most attrac-tive component of their smiles. It’s considered normalamong that age group. Besides, the payoff in just a cou-ple of years is a smile that they can be proud of.
On the other hand, it isn’t common to find adultswearing orthodontic appliances to correct misalignedteeth. The main reason is that adults don’t want to havethe “metal mouth” look of adolescence. They think itcompromises professionalism or looks out of place. Timeis also a factor. Patients must schedule regular office vis-its, which can involve time off from work or otherwisebe inconvenient.
Grown-up orthodonticsRecently, a company called Align Technology
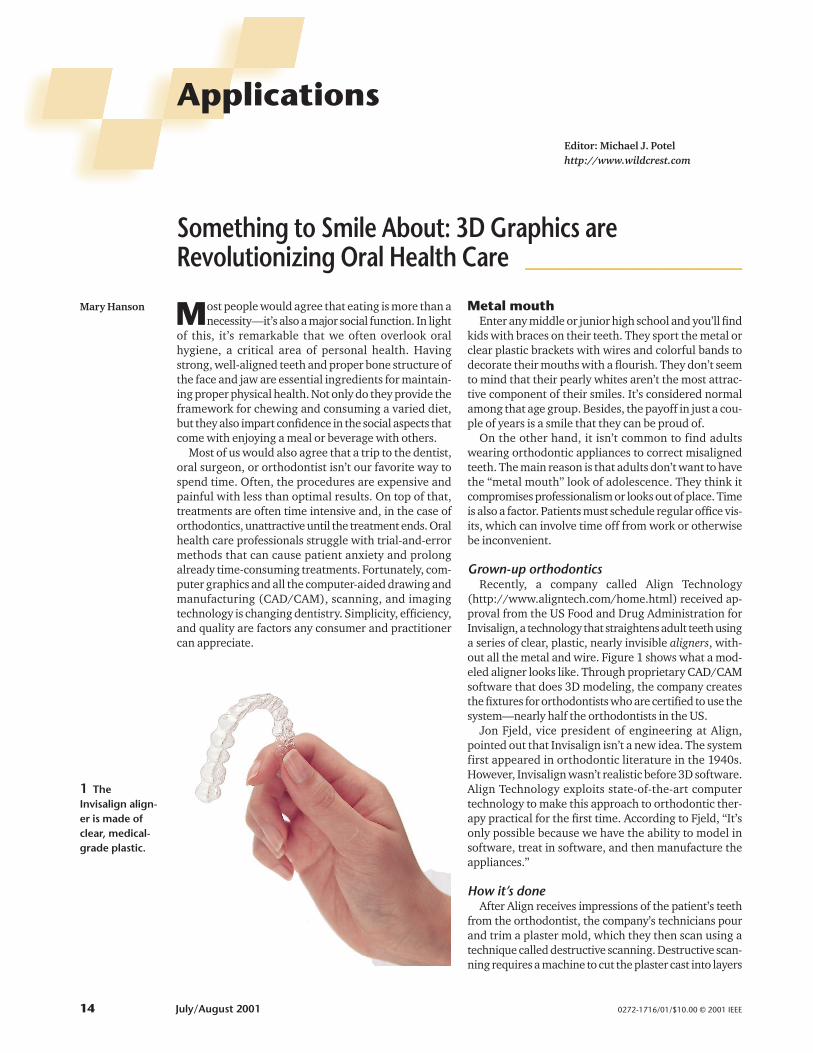
(http://www.aligntech.com/home.html) received ap-proval from the US Food and Drug Administration forInvisalign, a technology that straightens adult teeth usinga series of clear, plastic, nearly invisible aligners, with-out all the metal and wire. Figure 1 shows what a mod-eled aligner looks like. Through proprietary CAD/CAMsoftware that does 3D modeling, the company createsthe fixtures for orthodontists who are certified to use thesystem—nearly half the orthodontists in the US.
Jon Fjeld, vice president of engineering at Align,pointed out that Invisalign isn’t a new idea. The systemfirst appeared in orthodontic literature in the 1940s.However, Invisalign wasn’t realistic before 3D software.Align Technology exploits state-of-the-art computertechnology to make this approach to orthodontic ther-apy practical for the first time. According to Fjeld, “It’sonly possible because we have the ability to model insoftware, treat in software, and then manufacture theappliances.”
How it’s doneAfter Align receives impressions of the patient’s teeth
from the orthodontist, the company’s technicians pourand trim a plaster mold, which they then scan using atechnique called destructive scanning. Destructive scan-ning requires a machine to cut the plaster cast into layers
Mary Hanson
0272-1716/01/$10.00 © 2001 IEEE
Something to Smile About: 3D Graphics areRevolutionizing Oral Health Care ____________________
ApplicationsEditor: Michael J. Potelhttp://www.wildcrest.com
14 July/August 2001
1 TheInvisalign align-er is made ofclear, medical-grade plastic.
for scanning, ultimately destroying the cast. The tech-nique generates a series of digital photographs and resultsin a volumetric model of each arch based on a standardset of algorithms. The resolution of the polygonal files isabout 100,000 triangles. Align then uses its proprietarysoftware to generate a 3D movie that shows the series ofthe necessary movements of the patient’s teeth from thecurrent to the desired position. The procedure’s accura-cy is within 50 microns. To do all this, Align uses WindowsNT 4.0 workstations with Pentium III processors at 700MHz with 512 Mbytes of RAM, a 9-Gbyte hard drive, andan ASUS AGP-V7700 graphics card.
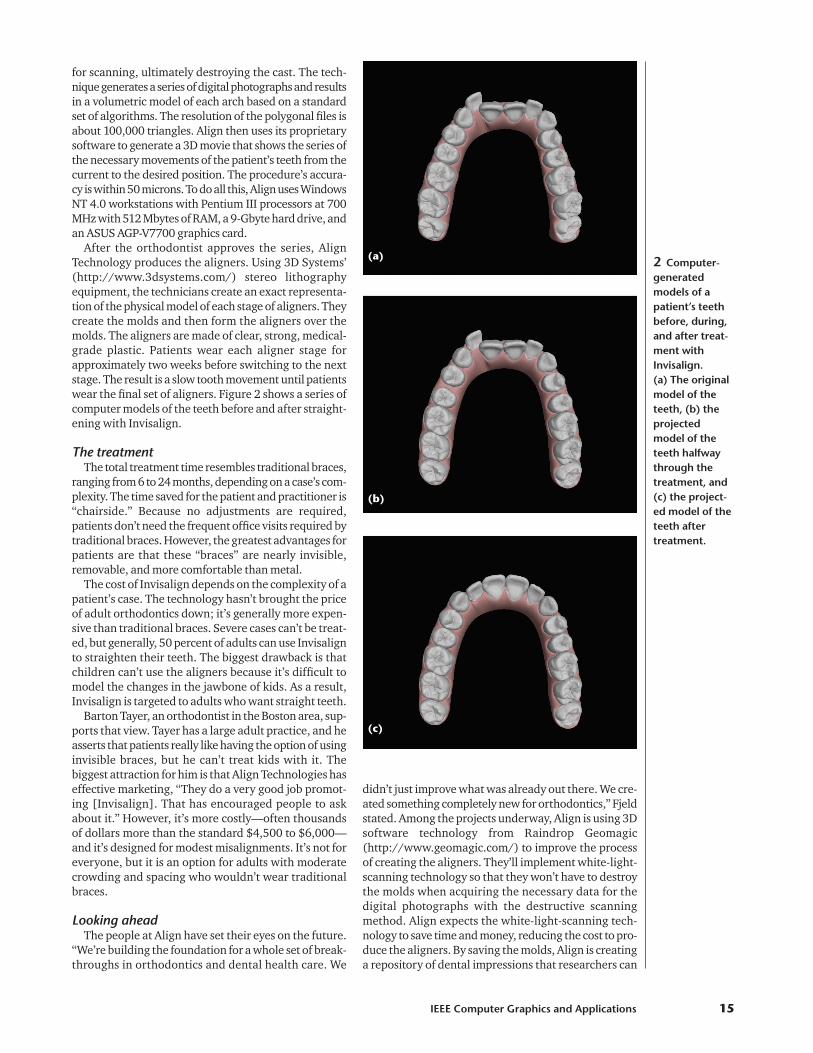
After the orthodontist approves the series, AlignTechnology produces the aligners. Using 3D Systems’(http://www.3dsystems.com/) stereo lithographyequipment, the technicians create an exact representa-tion of the physical model of each stage of aligners. Theycreate the molds and then form the aligners over themolds. The aligners are made of clear, strong, medical-grade plastic. Patients wear each aligner stage forapproximately two weeks before switching to the nextstage. The result is a slow tooth movement until patientswear the final set of aligners. Figure 2 shows a series ofcomputer models of the teeth before and after straight-ening with Invisalign.
The treatmentThe total treatment time resembles traditional braces,
ranging from 6 to 24 months, depending on a case’s com-plexity. The time saved for the patient and practitioner is“chairside.” Because no adjustments are required,patients don’t need the frequent office visits required bytraditional braces. However, the greatest advantages forpatients are that these “braces” are nearly invisible,removable, and more comfortable than metal.
The cost of Invisalign depends on the complexity of apatient’s case. The technology hasn’t brought the priceof adult orthodontics down; it’s generally more expen-sive than traditional braces. Severe cases can’t be treat-ed, but generally, 50 percent of adults can use Invisalignto straighten their teeth. The biggest drawback is thatchildren can’t use the aligners because it’s difficult tomodel the changes in the jawbone of kids. As a result,Invisalign is targeted to adults who want straight teeth.
Barton Tayer, an orthodontist in the Boston area, sup-ports that view. Tayer has a large adult practice, and heasserts that patients really like having the option of usinginvisible braces, but he can’t treat kids with it. Thebiggest attraction for him is that Align Technologies haseffective marketing, “They do a very good job promot-ing [Invisalign]. That has encouraged people to askabout it.” However, it’s more costly—often thousandsof dollars more than the standard $4,500 to $6,000—and it’s designed for modest misalignments. It’s not foreveryone, but it is an option for adults with moderatecrowding and spacing who wouldn’t wear traditionalbraces.
Looking aheadThe people at Align have set their eyes on the future.
“We’re building the foundation for a whole set of break-throughs in orthodontics and dental health care. We
didn’t just improve what was already out there. We cre-ated something completely new for orthodontics,” Fjeldstated. Among the projects underway, Align is using 3Dsoftware technology from Raindrop Geomagic(http://www.geomagic.com/) to improve the processof creating the aligners. They’ll implement white-light-scanning technology so that they won’t have to destroythe molds when acquiring the necessary data for thedigital photographs with the destructive scanningmethod. Align expects the white-light-scanning tech-nology to save time and money, reducing the cost to pro-duce the aligners. By saving the molds, Align is creatinga repository of dental impressions that researchers can
IEEE Computer Graphics and Applications 15
2 Computer-generatedmodels of apatient’s teethbefore, during,and after treat-ment withInvisalign. (a) The originalmodel of theteeth, (b) theprojectedmodel of theteeth halfwaythrough thetreatment, and(c) the project-ed model of theteeth aftertreatment.
(a)
(b)
(c)

use for future studies of orthodontics. Fjeld predicts thatthe white-light-scanning technology will be in place bysummer 2001.
People at Align are also working on a way to treat kidswith Invisalign. Treating adults creates the least num-ber of variables to work with because adults aren’t grow-ing anymore. Now that they have been successful withthat phase, they’re working with the changing struc-tures of a child’s mouth to create a system suitable fortreating kids with Invisalign.
Dental implantsDental implants have been around for decades, offer-
ing an alternative to dentures and bridges and providingreplacement teeth that look more natural. Implants maybe used to replace a single missing tooth or a completefunctional set for individuals who have lost many or allof their teeth. Despite the advances in prosthetic teeth,the procedure for implantation is still wrought with dif-ficulties. The process is complicated and can leave apatient feeling frustrated with less-than-ideal results.
The basics of implantsA traditional dental implant has three main parts:
� the implant, which prosthodontists surgically placeand anchor to the jawbone;
� the crown, which replaces the lost tooth; and� the abutment, which screws into the implant and
holds the crown in place.
The abutment corrects for offsets and angles that dete-riorated bone causes. Often, fitting the abutment can bethe most difficult aspect of dental implants. Besidesdeteriorated bone, standard parts contribute to ill-fit-ting abutments because they’re difficult to perfect foreach individual case. Additionally, a technician makesthe adjustments by hand—a somewhat imprecisemethod. As a result, an abundance of radiographs andanesthetic may be required while verifying the abutmentplacement. This may also necessitate several office vis-its for the patient, which translates into higher costs andinconvenience, not to mention discomfort.
The existing technology for dental implants wasn’tdesigned with the restorative dentist or prosthodontistin mind. According to Julian Osorio, a practicingprosthodontist and founder of Atlantis Components, acustom dental products company (http://www.atlantis-comp.com), “The emphasis was on the surgical phaseof the implant procedure, and the needs of the restora-tive dentist were an afterthought and were essentiallyignored. The results exhibited this fact in the unaccept-able aesthetics of the final crown.” As a result, Osoriodecided to create a more efficient way to implant teethusing computer graphics.
Easy precisionAtlantis’ technique uses software that Raindrop
Geomagic customized for Atlantis. Figure 3 showsimages that represent various modeling phases in a casein which the patient had no teeth. Dentists or prostho-dontists make a study cast of the area where the abut-ment will be placed. They then scan the cast into thecomputer using a 3D optical scanner, creating a 3D pointcloud (the digitized study cast consists of somewherebetween 50,000 and 200,000 points). Technicians atAtlantis use Raindrop Geomagic’s Studio software to cre-ate a polygonal surface from the point cloud. Atlantisuses proprietary software to virtually assemble the dig-ital teeth data with an unmodified (or template) versionof their product. This template is a 3D model of an ide-ally shaped dental abutment. Technicians virtually mod-ify this template so that it fits within the gap created bythe missing teeth. The system directly uses the digitaldata to fabricate the dental abutment used to restoremissing teeth.
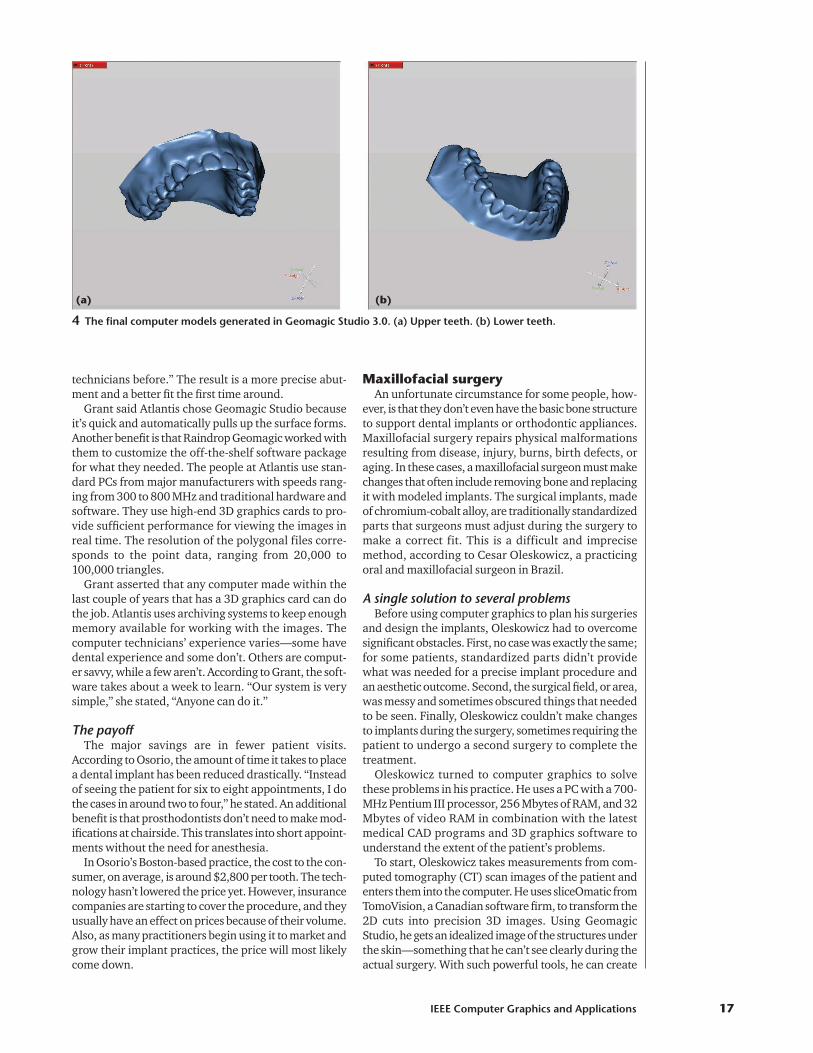
The computer generates the tool path—the instruc-tions the milling machine uses to create the final prod-uct from the 3D model—and sends it to the millingmachines that create the titanium abutment. Figure 4shows the final models of upper and lower teeth thatGeomagic Studio 3.0 generated. Bethany Grant, an engi-neer at Atlantis Components explained, “Now we’redoing everything virtually that was hand done by the
Applications
16 July/August 2001
3 A series of 3Dcomputerimages repre-senting variousphases of themodeling forone patient. (a) A surfacerepresentationof the dentalstudy casts in acase where thepatient had noteeth. (b) ModifiedAtlantis abut-ment modelsshowing whatwas designed tocomplete therestoration forthis patient. (c) A represen-tation of therestoration planpartially translu-cent overlaid onthe patient’sstudy casts. Thisgives a goodpicture of whatthe finalrestoration willlook like—complete withcrowns.
(a)
(b)
(c)
technicians before.” The result is a more precise abut-ment and a better fit the first time around.
Grant said Atlantis chose Geomagic Studio becauseit’s quick and automatically pulls up the surface forms.Another benefit is that Raindrop Geomagic worked withthem to customize the off-the-shelf software packagefor what they needed. The people at Atlantis use stan-dard PCs from major manufacturers with speeds rang-ing from 300 to 800 MHz and traditional hardware andsoftware. They use high-end 3D graphics cards to pro-vide sufficient performance for viewing the images inreal time. The resolution of the polygonal files corre-sponds to the point data, ranging from 20,000 to100,000 triangles.
Grant asserted that any computer made within thelast couple of years that has a 3D graphics card can dothe job. Atlantis uses archiving systems to keep enoughmemory available for working with the images. Thecomputer technicians’ experience varies—some havedental experience and some don’t. Others are comput-er savvy, while a few aren’t. According to Grant, the soft-ware takes about a week to learn. “Our system is verysimple,” she stated, “Anyone can do it.”
The payoffThe major savings are in fewer patient visits.
According to Osorio, the amount of time it takes to placea dental implant has been reduced drastically. “Insteadof seeing the patient for six to eight appointments, I dothe cases in around two to four,” he stated. An additionalbenefit is that prosthodontists don’t need to make mod-ifications at chairside. This translates into short appoint-ments without the need for anesthesia.
In Osorio’s Boston-based practice, the cost to the con-sumer, on average, is around $2,800 per tooth. The tech-nology hasn’t lowered the price yet. However, insurancecompanies are starting to cover the procedure, and theyusually have an effect on prices because of their volume.Also, as many practitioners begin using it to market andgrow their implant practices, the price will most likelycome down.
Maxillofacial surgeryAn unfortunate circumstance for some people, how-
ever, is that they don’t even have the basic bone structureto support dental implants or orthodontic appliances.Maxillofacial surgery repairs physical malformationsresulting from disease, injury, burns, birth defects, oraging. In these cases, a maxillofacial surgeon must makechanges that often include removing bone and replacingit with modeled implants. The surgical implants, madeof chromium-cobalt alloy, are traditionally standardizedparts that surgeons must adjust during the surgery tomake a correct fit. This is a difficult and imprecisemethod, according to Cesar Oleskowicz, a practicingoral and maxillofacial surgeon in Brazil.
A single solution to several problemsBefore using computer graphics to plan his surgeries
and design the implants, Oleskowicz had to overcomesignificant obstacles. First, no case was exactly the same;for some patients, standardized parts didn’t providewhat was needed for a precise implant procedure andan aesthetic outcome. Second, the surgical field, or area,was messy and sometimes obscured things that neededto be seen. Finally, Oleskowicz couldn’t make changesto implants during the surgery, sometimes requiring thepatient to undergo a second surgery to complete thetreatment.
Oleskowicz turned to computer graphics to solvethese problems in his practice. He uses a PC with a 700-MHz Pentium III processor, 256 Mbytes of RAM, and 32Mbytes of video RAM in combination with the latestmedical CAD programs and 3D graphics software tounderstand the extent of the patient’s problems.
To start, Oleskowicz takes measurements from com-puted tomography (CT) scan images of the patient andenters them into the computer. He uses sliceOmatic fromTomoVision, a Canadian software firm, to transform the2D cuts into precision 3D images. Using GeomagicStudio, he gets an idealized image of the structures underthe skin—something that he can’t see clearly during theactual surgery. With such powerful tools, he can create
IEEE Computer Graphics and Applications 17
4 The final computer models generated in Geomagic Studio 3.0. (a) Upper teeth. (b) Lower teeth.
(a) (b)
Applications
18 July/August 2001
It appears that the graphics that haverevolutionized oral health care require nothingmore than a relatively up-to-date computer and alittle training on some innovative software. Thevalue of automation in health care is clear andseveral companies are creating software forCAD/CAM purposes. The two described herestand out in the oral health care field asgroundbreakers, and they’re raising the bar thatdefines state of the art.
GeomagicThe common thread among the three examples
of oral health care techniques discussed in thisarticle is the CAD/CAM software they use (or will
use) from Raindrop Geomagic. The companydevelops technologies that automatically turnphysical parts and objects into digital models foruse in design, engineering, manufacturing, andmarketing. Ping Fu, an expert in 3D geometricmodeling and visualization, and HerbertEdelsbrunner, an internationally recognized expertin computational algorithms, geometry, andtopology, started the company in 1996. Theycurrently have 15 software engineers and thesoftware is primarily developed within thecompany. They use OpenGL as the renderingengine and optimize the software for the nVidiagraphics processors with real-time support ofcolor, texture, and bump maps.
Geomagic software was based on many years ofresearch rooted in combinatorics, geometry, and
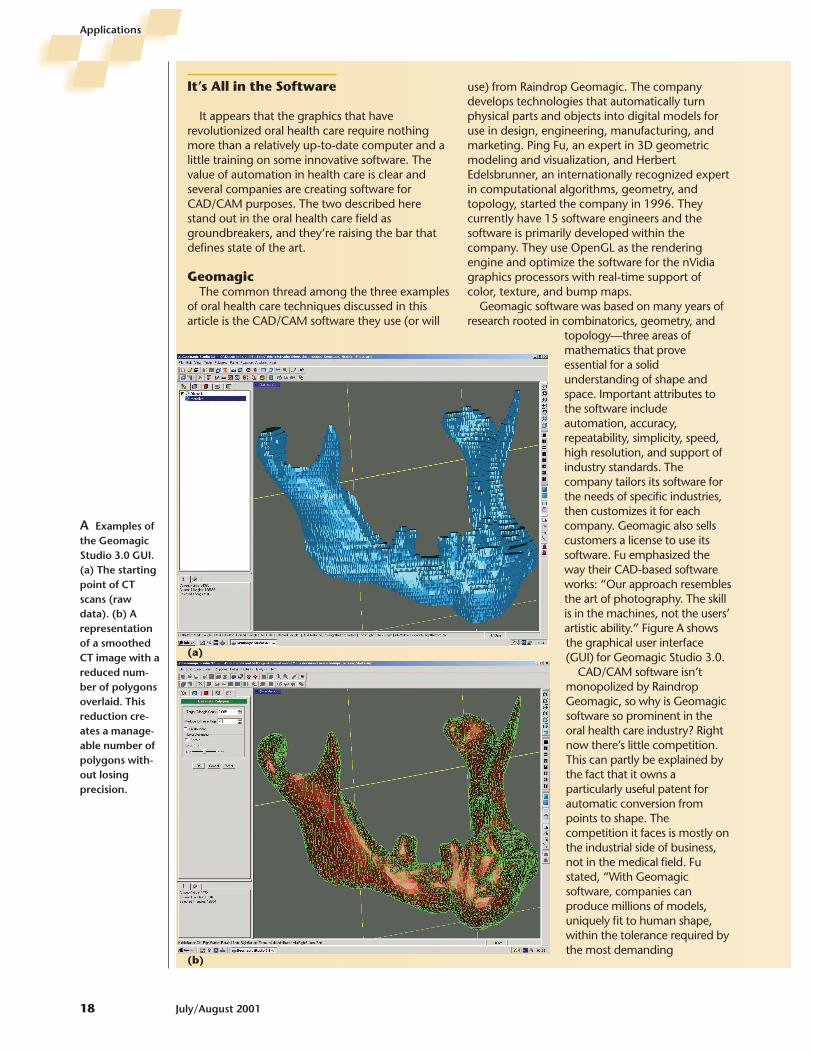
topology—three areas ofmathematics that proveessential for a solidunderstanding of shape andspace. Important attributes tothe software includeautomation, accuracy,repeatability, simplicity, speed,high resolution, and support ofindustry standards. Thecompany tailors its software forthe needs of specific industries,then customizes it for eachcompany. Geomagic also sellscustomers a license to use itssoftware. Fu emphasized theway their CAD-based softwareworks: “Our approach resemblesthe art of photography. The skillis in the machines, not the users’artistic ability.” Figure A showsthe graphical user interface(GUI) for Geomagic Studio 3.0.
CAD/CAM software isn’tmonopolized by RaindropGeomagic, so why is Geomagicsoftware so prominent in theoral health care industry? Rightnow there’s little competition.This can partly be explained bythe fact that it owns aparticularly useful patent forautomatic conversion frompoints to shape. Thecompetition it faces is mostly onthe industrial side of business,not in the medical field. Fustated, “With Geomagicsoftware, companies canproduce millions of models,uniquely fit to human shape,within the tolerance required bythe most demanding
A Examples ofthe GeomagicStudio 3.0 GUI.(a) The startingpoint of CTscans (rawdata). (b) Arepresentationof a smoothedCT image with areduced num-ber of polygonsoverlaid. Thisreduction cre-ates a manage-able number ofpolygons with-out losingprecision.
(a)
(b)
It’s All in the Software

IEEE Computer Graphics and Applications 19
manufacturing processes. [This is] a benchmark notachieved by any other software, at a price point andthroughput required to make customizedmanufacturing a profitable and practical process.”The cost of the software depends on the area ofuse, but a ballpark figure is $20,000 plus a one-timeengineering fee for customization. Users can run iton a PC with Windows or Unix.
Raindrop Geomagic plans to continuedeveloping software for use in multiple fields. Itaims to streamline the processes that companiesuse to create the article of interest. One way thatGeomagic does this is by creating templates. Byusing templates adapted for each case, users cansave a lot of time, and the technology may bemore cost effective.
TomoVisonTomoVision (http://www.tomovision.com/)
produces medical imagery programs that enhanceresearchers’, physicians’, and medical professionals’operational and clinical effectiveness. Aside fromsurgical planning and implant design, this softwareis used to calculate anatomical volume and surfaceby body composition physicians, generate accurate3D anatomical models by biomedical engineers,and enhance 2D and 3D visualizations byradiologists. Each of these health care fields usesspecific tools such as fast image display andprocessing, measurement, segmentation, editing,and filtering.
According to Yves Martel, founder ofTomoVision, the company is a one-man show. Thefirst version of the software was an in-house tool atthe Montreal Polytechnical School designed for aresearcher segmenting magnetic resonanceimages (MRIs) of a rat. The first commercial releasewas in 1994 in collaboration with the School ofHigh Technology (Ecole de TechnologieSuperieure, or ETS) in Montreal. At first it ran on aSGI workstation using SGI’s original GL graphicslibrary. Since January 2000, it has been ported toWindows using OpenGL. The program is writtenin C, and the interface is done with Yves’ Tools, aproprietary interface toolkit that lends moreflexibility and portability than conventionalinterface tools. Figure B shows the GUI.
The software runs on a Windows (95 to 2000)platform on any PC with a good OpenGL graphicscard and plenty of memory. A typical user wantsto be able to analyze hundreds of medical slices,and each of these can take up to 1 Mbyte.SliceOmatic comes in three modules: Basic, Tag,and 3D. The Basic module lets users read theimages, do some 2D measurement on them,reslice them, and select a region of interest in theimages. Martel admitted, “The first moduledoesn’t get you very far, but some researchersdon’t require more than Basic.” The Tag modulelets users segment the images, and the 3D module
uses the segmented images to create rough 3Dsurfaces.
Each module costs $2,000. Martel said thatwhile the software isn’t generally customized, hecan do that: “If somebody wants somethingspecific, I’ll probably do it for them.” Martel triedto make the interface as intuitive as possible, butit’s a powerful tool. It comes with a tutorial thatusers can download with the software from theTomoVision Web pages.
The competition for TomoVision includessoftware called Analyze, which was created at theMayo Clinic (http://www.analyzedirect.com/);Materialise, based in Europe(http://www.materialise.com), and 3D Doctor,designed by Able Software Corporation(http://www.ablesw.com/3d-doctor/). The Tagmodule, which permits segmentation, is whatdifferentiates sliceOmatic from the competitionand makes it a desirable software package forCesar Oleskovicz. “No other software on themarket does that,” Bartel noted. TomoVision isstriving for better segmentation in new editions.The company continues to collaborate withresearchers at the ETS to ensure that the softwareuses the latest segmentation techniques.
Teaming upDespite the power of TomoVision’s software,
some researchers and practitioners use more thanone software package to achieve their goals. Forexample, Oleskovicz’s oral and maxillofacial surgerypractice uses sliceOmatic and Geomagic Studio tocreate graphics because Geomagic Studio hascapabilities that sliceOmatic doesn’t. For instance,sliceOmatic-created images have a staircase lookinstead of the smooth and natural look thatGeomagic Studio images have because of a filteringprocess. Another advantage to teaming up the twotypes of software is that Geomagic Studio has thecapability to manipulate images. The graphics inFigure 5 (next page) from Oleskovicz’s cases camefrom animations he created using both sliceOmaticand Geomagic Studio.
B GUI ofsliceOmatic. Theimage is a 2Daxial cut of a CTscan prior toany manipula-tion. This iswhat radiolo-gists and sur-geons typicallysee.
images of the facial structures with which he will workduring the surgery, as Figure 5 shows.
Once Oleskowicz obtains the images, he can deter-mine how much bone he must remove and then replaceit with an implant. Oleskowicz chose Geomagic softwarebecause it was less expensive than any other softwarethat was available and he got support from RaindropGeomagic to get started: “They spent time with me tohelp me learn how to use the software.”
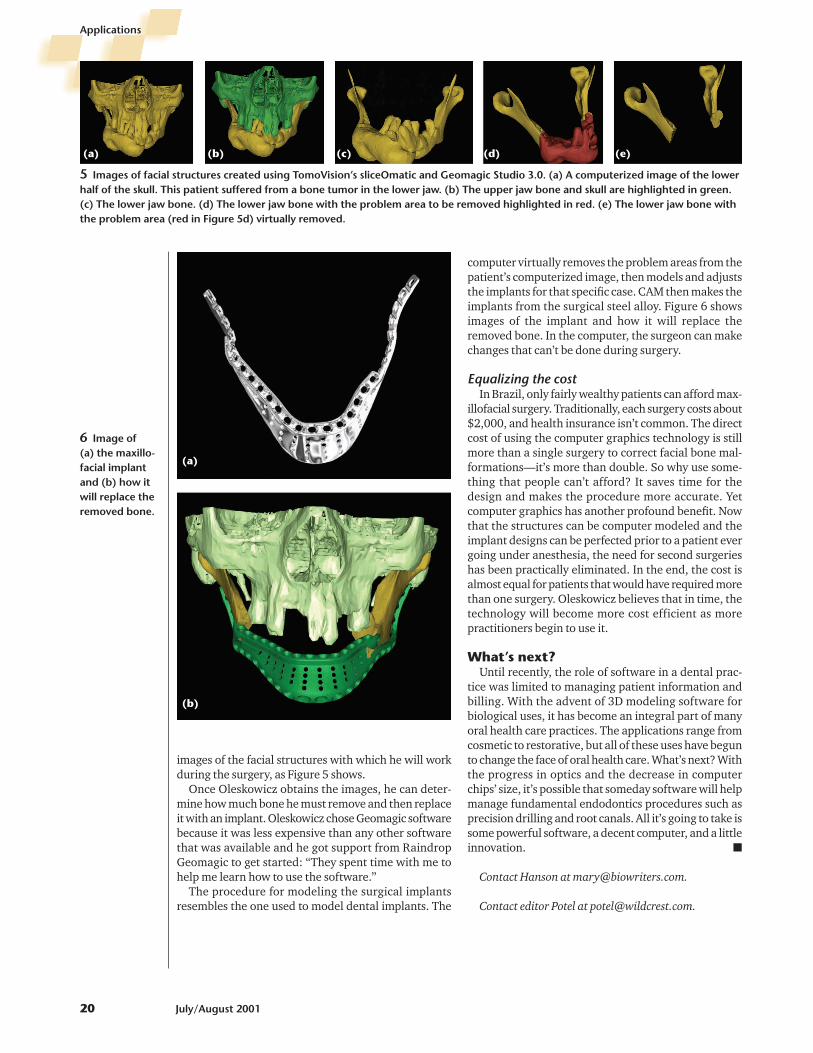
The procedure for modeling the surgical implantsresembles the one used to model dental implants. The
computer virtually removes the problem areas from thepatient’s computerized image, then models and adjuststhe implants for that specific case. CAM then makes theimplants from the surgical steel alloy. Figure 6 showsimages of the implant and how it will replace theremoved bone. In the computer, the surgeon can makechanges that can’t be done during surgery.
Equalizing the costIn Brazil, only fairly wealthy patients can afford max-
illofacial surgery. Traditionally, each surgery costs about$2,000, and health insurance isn’t common. The directcost of using the computer graphics technology is stillmore than a single surgery to correct facial bone mal-formations—it’s more than double. So why use some-thing that people can’t afford? It saves time for thedesign and makes the procedure more accurate. Yetcomputer graphics has another profound benefit. Nowthat the structures can be computer modeled and theimplant designs can be perfected prior to a patient evergoing under anesthesia, the need for second surgerieshas been practically eliminated. In the end, the cost isalmost equal for patients that would have required morethan one surgery. Oleskowicz believes that in time, thetechnology will become more cost efficient as morepractitioners begin to use it.
What’s next?Until recently, the role of software in a dental prac-
tice was limited to managing patient information andbilling. With the advent of 3D modeling software forbiological uses, it has become an integral part of manyoral health care practices. The applications range fromcosmetic to restorative, but all of these uses have begunto change the face of oral health care. What’s next? Withthe progress in optics and the decrease in computerchips’ size, it’s possible that someday software will helpmanage fundamental endodontics procedures such asprecision drilling and root canals. All it’s going to take issome powerful software, a decent computer, and a littleinnovation. �
Contact Hanson at [email protected].
Contact editor Potel at [email protected].
Applications
20 July/August 2001
5 Images of facial structures created using TomoVision’s sliceOmatic and Geomagic Studio 3.0. (a) A computerized image of the lowerhalf of the skull. This patient suffered from a bone tumor in the lower jaw. (b) The upper jaw bone and skull are highlighted in green.(c) The lower jaw bone. (d) The lower jaw bone with the problem area to be removed highlighted in red. (e) The lower jaw bone withthe problem area (red in Figure 5d) virtually removed.
(a) (b) (c) (d) (e)
6 Image of (a) the maxillo-facial implantand (b) how itwill replace theremoved bone.
(a)
(b)





























