Embed Size (px)
Citation preview
International Journal of Public Health Research 2015; 3(5): 254-263
Published online August 30, 2015 (http://www.openscienceonline.com/journal/ijphr)
Application of Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’ Requirements for Mityana General Hospital, Uganda
Philip Govule1, *
, John Francis Mugisha1, Simon Peter Katongole
1, Everd Maniple
1, Miisa Nanyingi
1,
Robert Anguyo DDM Onzima2
1Faculty of Health Sciences, Uganda Martyrs University, Kampala, Uganda 2Department of International Public Health, Liverpool School of Tropical Medicine, Kampala, Uganda
Email address
[email protected] (P. Govule), [email protected] (J. F. Mugisha), [email protected] (S. P. Katongole),
[email protected] (E. Maniple), [email protected] (M. Nanyingi), [email protected] (R. A. D. Onzima)
To cite this article Govule Philip, Mugisha John Francis, Katongole Simon Peter, Maniple Everd, Nanyingi Miisa, Anguyo Robert DDM Onzima. Application of
Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’ Requirements for Mityana General Hospital, Uganda.
International Journal of Public Health Research. Vol. 3, No. 5, 2015, pp. 254-263.
Abstract
Introduction: With reducing number of health workers amidst increasing disease burden, ever increasing population and limited
resources, health systems are faced with challenges of providing adequate and quality health care globally. The application of
provider-population ratio or fixed staff establishments have overtime, not matched the changing human resource needs of health
care organizations. This study aimed to estimate human resource requirements of Mityana hospital basing on workload as an
alternative to the existing approaches. Methodology: We employed descriptive cross-sectional design and the Workload Indicator
of Staffing Needs (WISN) methodology. We utilized focus group discussion, observation and document review to obtain
information from key informants; generated annual service statistics from the hospital’s records. The quantitative data were
analyzed using the WISN software and spread sheet. Results: All the cadres studied had the same hours of work in a year (1,664),
except nursing assistants whose annual available working time was1,696 hours. All the cadres were experiencing additional
workload due to use of their time for activities other than their primary duties. Medical officers used more than 50% of their time
for such (non-primary) activities compared to the laboratory staff (15%). As a result, the calculated WISN staff requirements
were very high compared to the existing staff levels. Mityana hospital had 44% of the posts filled for the studied cadres. The
nurses and midwives had the highest calculated requirements (72 and 45 respectively) and the highest staff positions filled (57%
and 84% respectively) making them experience the lowest work pressure (49% each). The highest work pressure was
experienced by medical officers and medical clinical officers (82% each). Conclusion: The study reveals shortages in health
workforce in Mityana hospital. Non-primary activities contributed to work pressure in different units of the hospital, resulting
into long hours of shifts which could have compromised quality of health care. This method (WISN) estimates staffing
requirements based on actual service provision. Stakeholders facing human resource challenges and scarcity can employ it in
prioritizing health cadres for recruitment and deployment based on existing work pressure.
Keywords
Workload Indicators of Staffing Needs (WISN), Health Workers’ Requirements, Mityana Hospital, Uganda
1. Introduction
In order to improve health care delivery, health services’
managers are faced with increasing challenges in provision of
adequate and quality health care amidst inadequate numbers
of health workforce to meet the demand of the ever growing
population [1] [2]. “Availability of trained health workers is
one of the most critical limiting factors for the delivery of a
minimum health package” [3]: pg 17. In health care delivery,
human resource is a major input and its level and mix is a
major determinant of cost and quality. Expenditures on human
resource in most health systems around the world account for
over 70% of recurrent budgets [4]. There is global health

International Journal of Public Health Research 2015; 3(5): 254-263 255
workforce shortage of 7.2 million and it is projected to reach
12.9 million by 2035 [5].
The Number of trained health personnel has historically
been inadequate hence the need to use this scarce resource
effectively [6]. There is an increasing need for health
organizations to identify the most appropriate staffing levels
and skill mix to ensure efficient and effective use of the
limited resources [7]. With its efficient use, health personnel
can make a major contribution to the health of a nation. Often
this is not the case as the required cadres are frequently
missing in specific geographical areas or health facilities
where they are needed most; or in surplus where need is low
resulting into inefficiencies. These imbalances result into
spending too much time on activities requiring little time –
leaving little time for processes that require more time [8] [9].
In developed countries there has been a general shortage of
health care personnel, with shortage of nurses at 400,000; and
projected to reach one million by 2020. By the same time
(2020) about 200,000 physicians will be lacking [10]. In
developing countries, especially sub-Saharan Africa there has
been worse and chronic shortage experienced all through. It is
estimated that 1.5 million health workers are lacking [11]. In
Uganda, the gap of health workers required in government
health facilities is over 44% [12]. These shortages hinder
delivery and maintenance of quality healthcare across the
world [13]. Poor planning and management of human
resource for health among other factors, contribute to the
shortages. In order to solve some of these problems, many
countries devolved service delivery and public administration
to sub-national and district-levels, including health services
management, but there are no coordination mechanisms
between central and decentralized units of government to
address issues such as urban-rural imbalances in the
distribution of the workforce [14].
Similarly, efforts by Uganda government, such as
decentralization (including of health workforce), incentives to
attract and retain health workforce in lower health centres and
hard to reach areas [15] have yielded minimal results. The
Uganda health sector human resource policy review reveals
that 20% of the districts have critical shortage of health
workforce compared to population [16]. This has caused
disparity in delivery of health care across the county. Even still,
supply of the right number and quality of people in health care
institutions for attainment of health care objectives has
remained a challenge to managers. These bottlenecks task the
health managers with challenge of identifying methods for
allocating this scarce resource (in numbers and skills) in order
to optimize society-wide service delivery. The required
number of health workers and their skill mix in a health
facility will depend on the workload and the range of services
in the facility which in most cases is related to the minimum
health care package of the facility [18].
One crucial discovery is that most health care institutions
base their staffing on practitioner-to-population ratio,
historical patterns of staffing and professional judgment.
Others adopted more sophisticated methods of analyzing
(their) staffing needs, like case-load profiling, acuity measures,
queuing theory, production functions, treatment care standards
and other combination factors by use of regression analysis
[19]. All these methods failed to estimate staffing
requirements in accordance with the actual workload and have
not taken into context variations in local demand for health
services [2]. In attempt to address the human resource
constraints, the Workload Indicators of Staffing Needs (WISN)
was developed by Shipp in 1998 and made popular by the
World Health Organization (WHO) as a way to analyze and
compute the different health cadres required by health
facilities, based on workload [20]. WISN encompasses the
routine activities of a particular cadre, the duration per activity
and other activities carried out by a particular cadre which is
not reflected in the employment contract and the annual
available working time [21]. Application of WISN in planning
and projection of human resources for health helps to rectify
many of the observed deficiencies in access to human resource
for health when it is required, irrespective of where people in
need reside or to which socio-economic group they belong.
This is inline with the assertion that a “well planned human
resource for health is appropriate for the provision of adequate
and quality healthcare services to the healthcare needs of local
populations to increase health status and decrease healthcare
costs” [21]. This implies each health facility having its own
staffing requirements depending on (its) workload. Following
its development by WHO, the WISN has been used to
determine staffing requirements in Papua New Guinea, the
United Republic of Tanzania, Kenya, Sri Lanka and also in six
other countries: Bahrain, Egypt, Hong Kong, Oman, Sudan
and Turkey among others [18]. WISN has also been used in
Namibia to rationalize the staff requirements for nurses,
doctors, pharmacists and pharmacist assistants [22]. In East
Africa, the method was used in Tanzania to determine the
staffing needs for quality prenatal care for nurse officers,
nurse midwives and nursing assistants [23] – it was used to
calculate the staffing requirements for medical officers, nurses
and laboratory staff in Kenya [21]. In Uganda, this method
was initially used to determine the nursing staff requirements
in Lacor, a private not for profit (PNFP) hospital in Northern
Uganda in 2005 [6]. The method was later experimented by
the government of Uganda in two districts of Mbale and
Mukono [24]. Considering that the staffing requirements for
health facilities differ, we sought to apply WISN in
determining staff requirements in a selected hospital in
Central Uganda. One of the possible issues argued is that the
method is burdensome since determining staffing
requirements is required by each health facility independently.
This looks a bit awkward; but it is known to have specific
returns of effectiveness and efficiency following its use in the
long run [25].
The Uganda Health Sector Strategic Plan III (HSSIP
2010/11-2014/15) stipulates the minimum staffing standards
(basing mainly on practitioner-to-population ratio, historical
patterns of staffing and professional judgment) at 75% for all
health facilities to enable meeting the growing demand of
health care, with the ratios of senior, mid-level and lower
health cadres at 1:5:2 respectively [26] [27]. Unfortunately,
256 Govule Philip et al.: Application of Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’
Requirements for Mityana General Hospital, Uganda
the overall national staffing level for health workers has
remained low (at 56%). Further analysis of the staffing level
of Mityana hospital revealed low staffing at 63.2% of
approved posts for some cadres and excesses of 2% for others
[27]. These observations depict deficiencies in use of fixed
staffing norms as applied in distribution of health workers,
estimation of work pressure and determination of staffing
requirements. This study aimed to estimate staff requirement
based on workload, so as to generate evidence to inform
policy makers and implementers to address issues on
distribution of staff, workload pressure, review and re-align
task-allocations between staff cadres and improve the quality
of health care.
2. Objectives
To apply WISN in determining health workers requirements
in order to improve health services in Mityana General
Hospital, central Uganda.
The methodological steps to achieve the objective included
to establish available working time (AWT) for selected
categories of health workers and to establish the additional
and support workload experienced by different categories of
health workers.
The specific objectives included to establish
workload-based staffing requirements for different categories
of health workers; and to compare WISN-based staffing
requirement with the existing staffing levels for Mityana
General Hospital, central Uganda.
3. Methodology
We conducted a descriptive cross-sectional study in
Mityana General Hospital adapting the WISN methodology
initially developed by Shipp [18] where we estimated the
available working time by reviewing the health staff records.
We used both focus group discussion and key informant
interview define and quantify the workload load components:
health service, support and additional activities. We employed
focus group discussion (1 FGD for each cadre) to set activity
standards. We conducted key informant interviews using
predetermined checklists to obtain data regarding the activity
standards for the various cadres while focus group discussions
were used to obtain information regarding the challenges
faced by various cadres in accordance with the workload. For
the interviews, we employed different checklists for relevant
cadres with designs guided by national WISN standards
produced by the Uganda MoH in partnership with United
States Agency for International Development, IntraHealth and
Uganda Capacity Program. Service statistics’ data were
collected from the hospital management information system
reports and registers. The data collected from key informant
interviews were then transferred to the WISN software (WISN
English version 1.1.132.0).
3.1. Sampling Technique
This study targeted six cadres namely; medical officers,
medical clinical officers, nurses, midwives, laboratory staff
and nursing assistants. These cadres were considered because
they are the ones mostly affected by increased workload.
Secondly, they have relatively larger numbers of staff for
which internal deployment and transfers can easily be carried
out. We interviewed 10 midwives, 5 laboratory staff, 9 nursing
assistants, 6 medical clinical officers, 8 nurses and 4 medical
officers of at least one year experience each.
3.2. Variables
The variables of this study include; available working time,
activity standards, annual workload, category allowance
standards (CAS), individual allowance standards (IAS), staff
levels, workload pressure and staffing requirement.
3.2.1. Available Working Time (AWT)
AWT = A-(B+C+D+E)
Where:-
A = the number of potential working days in a year
B = the number of public holidays
C = the number of off-duty days due to annual leave
D = the number of off-duty days due to sickness
E = the number of off-duty days due to other leaves
3.2.2. Activity Standards
Activity standard (AS) which is also referred to as the
amount of time necessary for a well-trained skilled and
motivated worker to perform an activity to professional
standards in a given circumstance was used to assess length of
‘professional time’ taken to execute tasks and put into
perspective primary activities; and other individually and
group-conducted activities. We later used the set AS to
calculate the standard workload, category allowance factor
(CAF) and individual allowance factors (IAF).
(i). The standard workload: This was calculated using the
formula;
Standard workload = Available Working TimeActivity Standard
The activity standard was obtained through key informant
interview with health staff of each cadre.
(ii). Category allowance factor (CAF): This was calculated
by summing up the percentages of time it takes all
members of the staff category to perform activities for
which the annual statistics were not available known as
category allowance standard (CAS). The CAF was
used in subsequent variables to compute the number of
staff needed.
CAF = 11 − ∑CAS%
(iii). IAS was obtained by calculating how much time
additional activities of certain cadres require by;
a. Writing down the number of staff who performed each
activity and the time it took them.
b. Multiplying the number of staff by the time the activity
International Journal of Public Health Research 2015; 3(5): 254-263 257
required in one year
c. Calculating the total IAS in a year by adding the results
obtained in (b) above
The individual allowance standards was then used to derive
the individual allowance factor using the formula;
IAF = IASAWT
The result was also used to compute the staff requirement to
cover additional activities of certain cadres and determining
the additional workload of the staff in Mityana hospital.
3.2.3. Annual Workload
The annual workload for each staff category were obtained
from the hospital reports; and laboratory and ANC registers.
These figures were used to calculate the basic staff
requirements and the total staff requirements for each
category.
3.2.4. Workload-Based Staffing Requirements
The results obtained from the above variables were then
used to compute the workload-based staffing requirements
using the formula:
WISN staff requirement
= �Annual workload x CAFStandard workload " + IAF
3.2.5. Staffing Gaps
The staffing gaps were established by subtracting the WISN
staffing requirements from the existing staffing level.
3.2.6. Workload Pressure
The workload pressure was calculated using the formula:
Workload pressure = (100- (existing/computed staff x100)
3.3. Data Analysis
Data were analyzed using excel spreadsheets, the WISN
software and manually. Considering that activity standards
were obtained through interviewing staff who reported
different activity, we obtained an average activity standard
before transferring to WISN software . In order to do this,
templates were generated in excel where various averages and
uniform time standards were calculated for the service
standards, CAS and IAS. The information was then
transferred to the WISN software and results generated in
accordance with the objectives of the study. Focus group
discussions were analyzed manually by a team of researchers
and the results obtained were used to substantiate the study’s
findings.
3.4. Quality Control
We adhered to standard quality control protocols of WISN
methods. The data collected were immediately entered to
quickly identify missing data, which was then obtained before
the end of the study. More so, the researchers assigned to
interview the particular cadres, were themselves peers of such
professions which enabled proper guidance of the respondents
in giving accurate information. The data were analyzed by two
persons independently to ensure reliability.
3.5. Limitations of the Study
Like any other WISN study, this study was conducted using
data retrospectively generated from the preceding year.
Significant differences in workload in the consecutive years
may affect validity of results. However, they remain useful for
planning purposes since workload variations across years and
seasons is comparable.
4. Results
The present study applied WISN method in determining
staffing requirements for medical officers, clinical officers,
nursing assistants, laboratory staff, midwives and nurses in
Mityana general hospital.
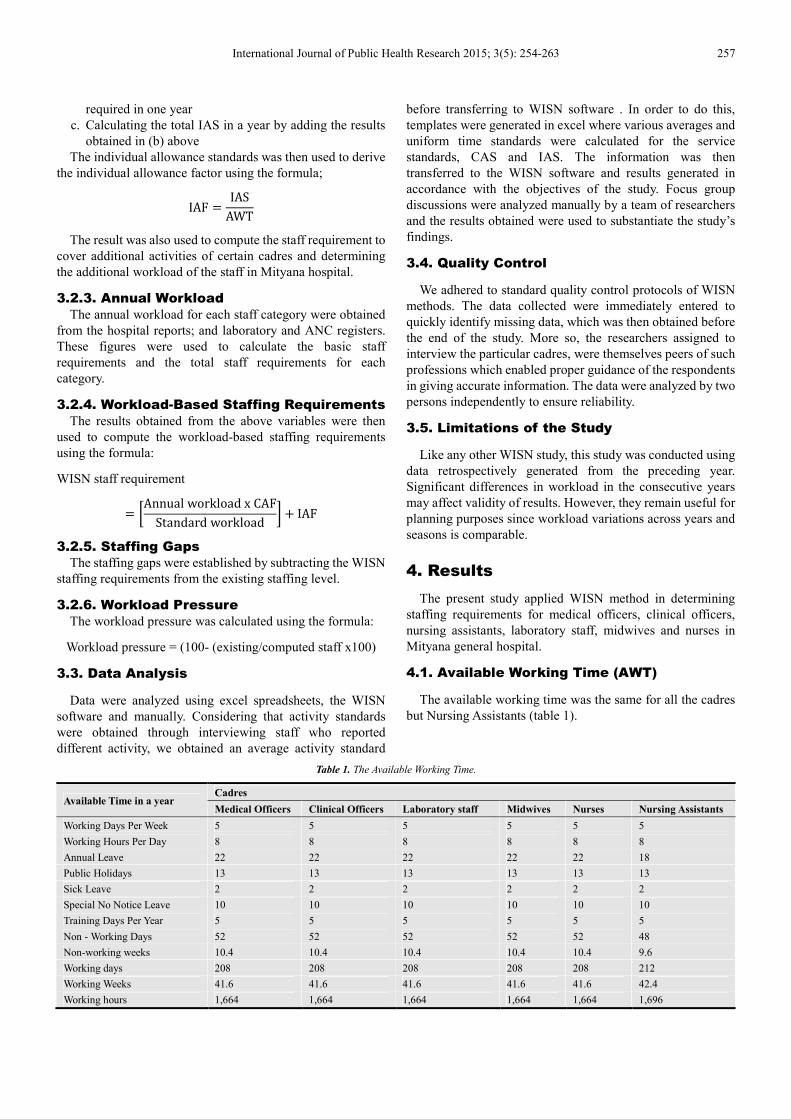
4.1. Available Working Time (AWT)
The available working time was the same for all the cadres
but Nursing Assistants (table 1).
Table 1. The Available Working Time.
Available Time in a year Cadres
Medical Officers Clinical Officers Laboratory staff Midwives Nurses Nursing Assistants
Working Days Per Week 5 5 5 5 5 5
Working Hours Per Day 8 8 8 8 8 8
Annual Leave 22 22 22 22 22 18
Public Holidays 13 13 13 13 13 13
Sick Leave 2 2 2 2 2 2
Special No Notice Leave 10 10 10 10 10 10
Training Days Per Year 5 5 5 5 5 5
Non - Working Days 52 52 52 52 52 48
Non-working weeks 10.4 10.4 10.4 10.4 10.4 9.6
Working days 208 208 208 208 208 212
Working Weeks 41.6 41.6 41.6 41.6 41.6 42.4
Working hours 1,664 1,664 1,664 1,664 1,664 1,696
258 Govule Philip et al.: Application of Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’
Requirements for Mityana General Hospital, Uganda
The fewer annual leave days the nursing assistants took
explains the variation in AWT. This is due to the fact that in
Uganda, they fall under the government staff category of U8
that is entitled to18 days of annual leave.
On further interviews with another hospital management
team member, we discovered that although the standing order
provides for 40 training days per year for every public servant,
not all members of the staff category had gone for training. It
was proper to use the training days as provided in the standing
orders and not the actual trainings days taken by a few
members of the staff category because we realized (during
focus group discussion) that the reason some cadres did not
attend training was a result of staff shortage and high
workload. Using the actual days would mean promoting this
gap as the norm, which will then increase the AWT and reduce
the number of staff actually required to produce quality
services. These facts came out so clear during the focus group
discussion where one of the participants expressed with
sadness:
We have terrible shortage of nurses which affects the
quality of nursing care, but luckily, nurses prolong the
hours of work in order to cover some shifts.
Laboratory staffs were often recalled from leave because
they are few.
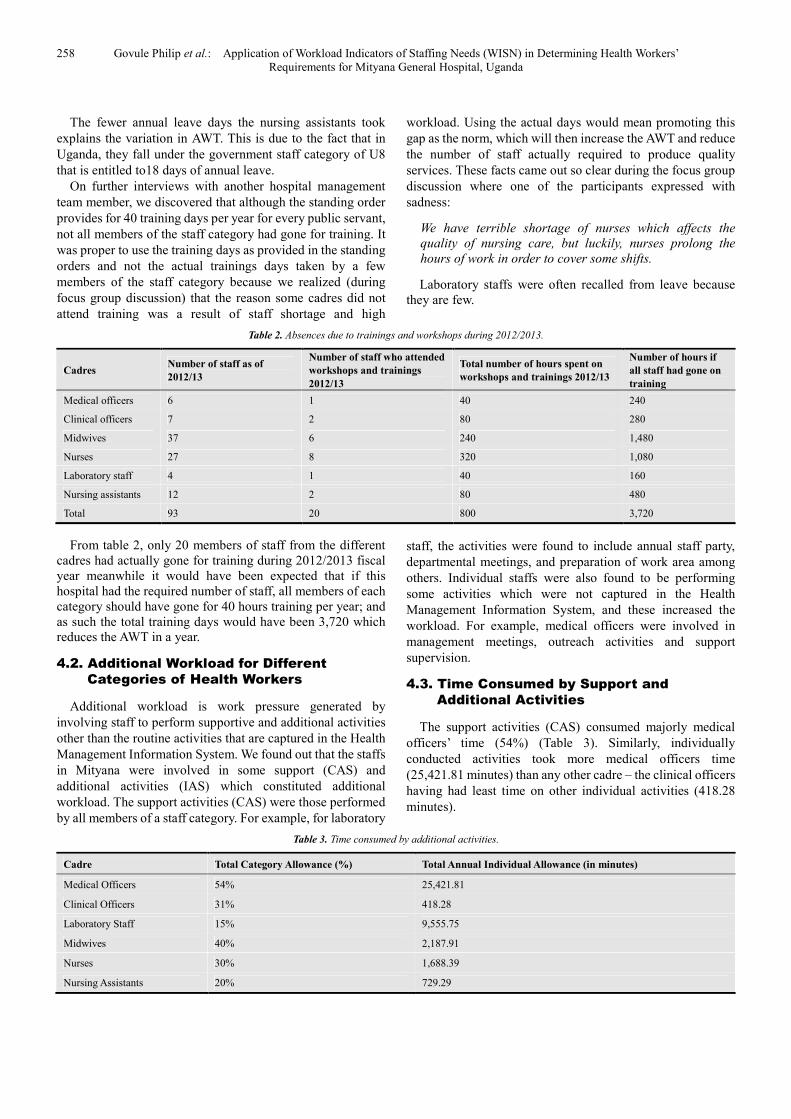
Table 2. Absences due to trainings and workshops during 2012/2013.
Cadres Number of staff as of
2012/13
Number of staff who attended
workshops and trainings
2012/13
Total number of hours spent on
workshops and trainings 2012/13
Number of hours if
all staff had gone on
training
Medical officers 6 1 40 240
Clinical officers 7 2 80 280
Midwives 37 6 240 1,480
Nurses 27 8 320 1,080
Laboratory staff 4 1 40 160
Nursing assistants 12 2 80 480
Total 93 20 800 3,720
From table 2, only 20 members of staff from the different
cadres had actually gone for training during 2012/2013 fiscal
year meanwhile it would have been expected that if this
hospital had the required number of staff, all members of each
category should have gone for 40 hours training per year; and
as such the total training days would have been 3,720 which
reduces the AWT in a year.
4.2. Additional Workload for Different
Categories of Health Workers
Additional workload is work pressure generated by
involving staff to perform supportive and additional activities
other than the routine activities that are captured in the Health
Management Information System. We found out that the staffs
in Mityana were involved in some support (CAS) and
additional activities (IAS) which constituted additional
workload. The support activities (CAS) were those performed
by all members of a staff category. For example, for laboratory
staff, the activities were found to include annual staff party,
departmental meetings, and preparation of work area among
others. Individual staffs were also found to be performing
some activities which were not captured in the Health
Management Information System, and these increased the
workload. For example, medical officers were involved in
management meetings, outreach activities and support
supervision.
4.3. Time Consumed by Support and
Additional Activities
The support activities (CAS) consumed majorly medical
officers’ time (54%) (Table 3). Similarly, individually
conducted activities took more medical officers time
(25,421.81 minutes) than any other cadre – the clinical officers
having had least time on other individual activities (418.28
minutes).
Table 3. Time consumed by additional activities.
Cadre Total Category Allowance (%) Total Annual Individual Allowance (in minutes)
Medical Officers 54% 25,421.81
Clinical Officers 31% 418.28
Laboratory Staff 15% 9,555.75
Midwives 40% 2,187.91
Nurses 30% 1,688.39
Nursing Assistants 20% 729.29
International Journal of Public Health Research 2015; 3(5): 254-263 259
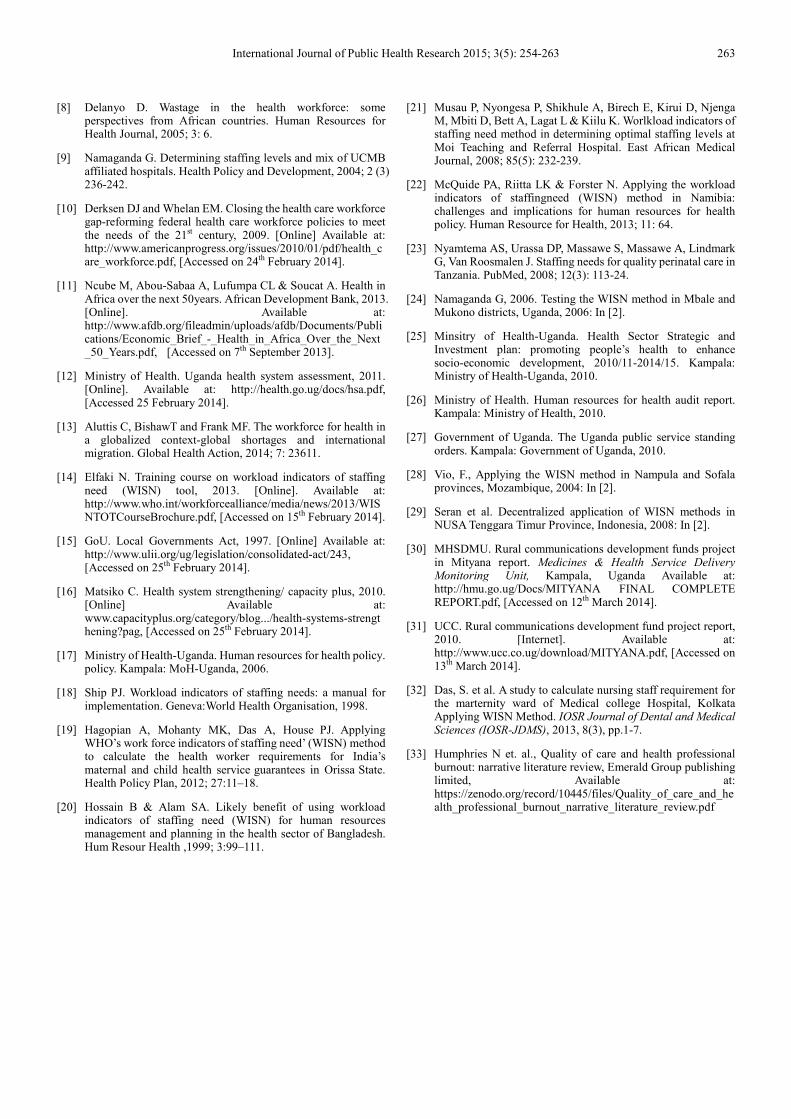
Table 4. Workload-based staffing requirements.
Cadre Basic staff requirement CAF BSR IAF Total staff required
Medical Officers 5.63 2.17 12.22 15.13 28
Clinical Officers 27.01 1.45 39.16 0.25 40
Laboratory Staff 10.7 1.18 12.62 5.69 18
Midwives 41.99 1.67 70.12 1.3 72
Nurses 30.6 1.43 43.75 1 45
Nursing Assistants 22.94 1.39 31.88 0.43 32
4.4. Workload Based Staffing Requirements
(BSR) for Different Categories of Health
Workers
The basic staff requirement (BSR) column in table 4 shows
the number of staff that would have been required in Mityana
general hospital if all members of that staff category dedicated
their entire time in their primary professional activities. For
example, only 6 medical officers would have been required if
all their time were dedicated to their primary activities.
However, because of the additional workload, more are
required.
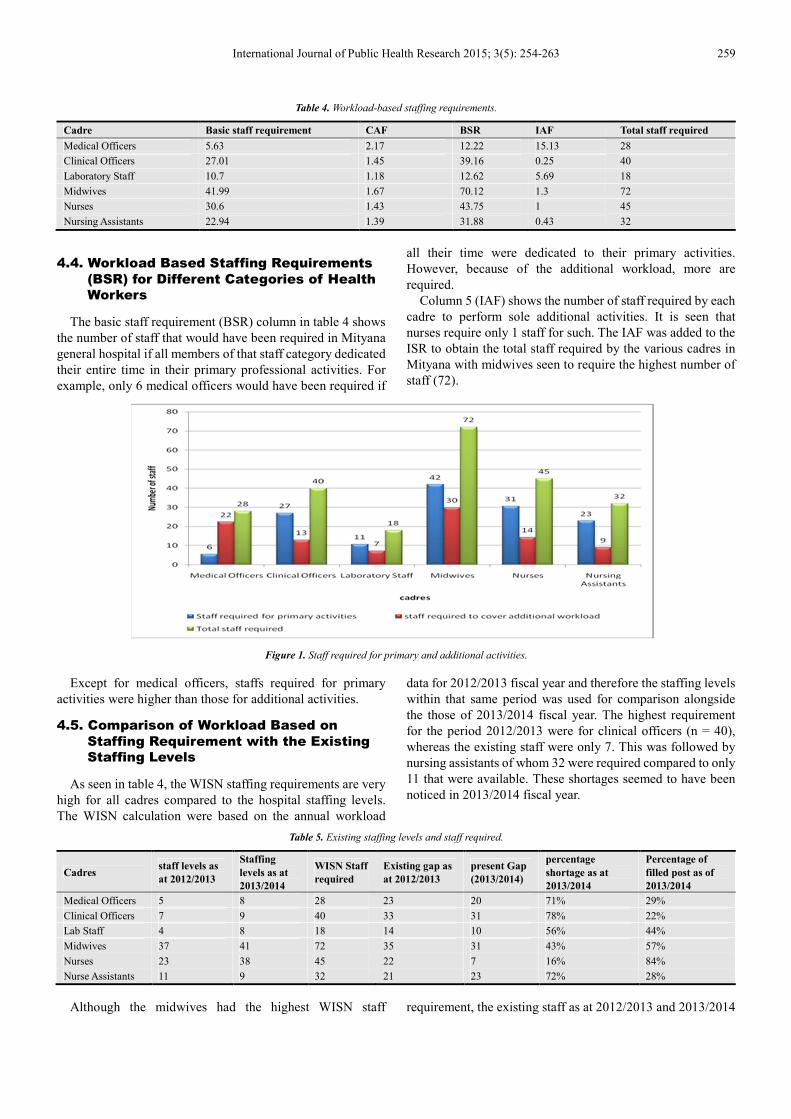
Column 5 (IAF) shows the number of staff required by each
cadre to perform sole additional activities. It is seen that
nurses require only 1 staff for such. The IAF was added to the
ISR to obtain the total staff required by the various cadres in
Mityana with midwives seen to require the highest number of
staff (72).
Figure 1. Staff required for primary and additional activities.
Except for medical officers, staffs required for primary
activities were higher than those for additional activities.
4.5. Comparison of Workload Based on
Staffing Requirement with the Existing
Staffing Levels
As seen in table 4, the WISN staffing requirements are very
high for all cadres compared to the hospital staffing levels.
The WISN calculation were based on the annual workload
data for 2012/2013 fiscal year and therefore the staffing levels
within that same period was used for comparison alongside
the those of 2013/2014 fiscal year. The highest requirement
for the period 2012/2013 were for clinical officers (n = 40),
whereas the existing staff were only 7. This was followed by
nursing assistants of whom 32 were required compared to only
11 that were available. These shortages seemed to have been
noticed in 2013/2014 fiscal year.
Table 5. Existing staffing levels and staff required.
Cadres staff levels as
at 2012/2013
Staffing
levels as at
2013/2014
WISN Staff
required
Existing gap as
at 2012/2013
present Gap
(2013/2014)
percentage
shortage as at
2013/2014
Percentage of
filled post as of
2013/2014
Medical Officers 5 8 28 23 20 71% 29%
Clinical Officers 7 9 40 33 31 78% 22%
Lab Staff 4 8 18 14 10 56% 44%
Midwives 37 41 72 35 31 43% 57%
Nurses 23 38 45 22 7 16% 84%
Nurse Assistants 11 9 32 21 23 72% 28%
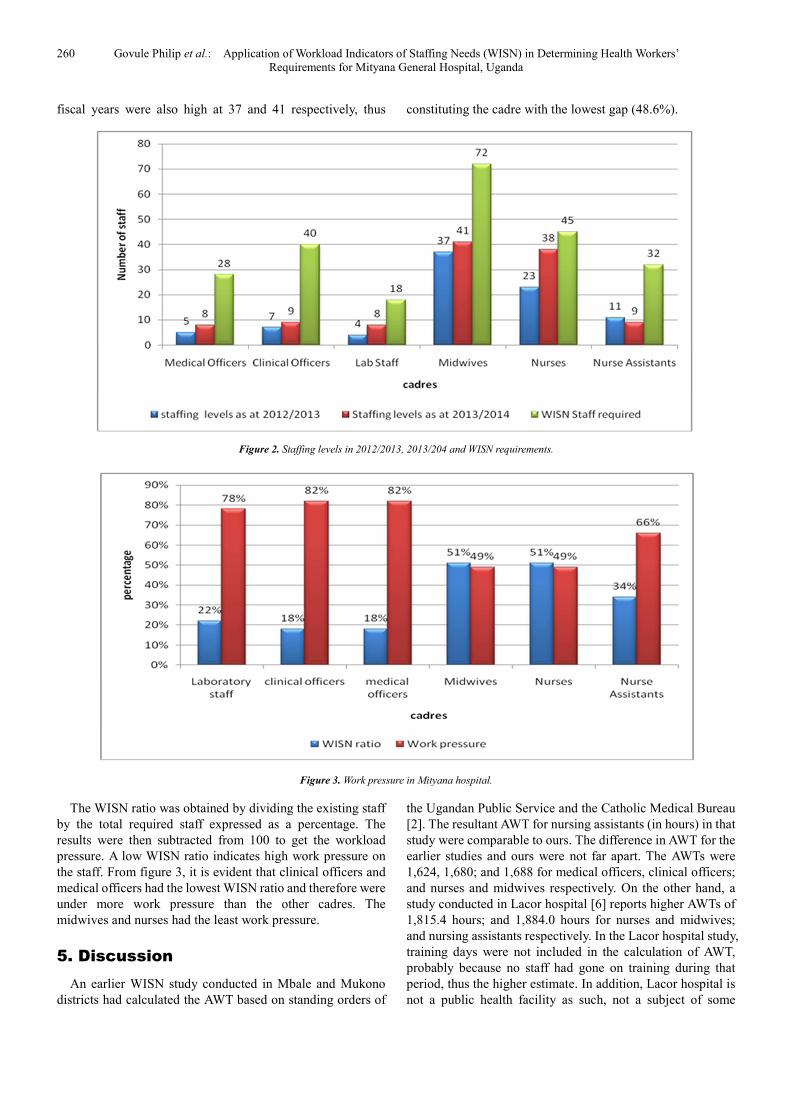
Although the midwives had the highest WISN staff requirement, the existing staff as at 2012/2013 and 2013/2014
260 Govule Philip et al.: Application of Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’
Requirements for Mityana General Hospital, Uganda
fiscal years were also high at 37 and 41 respectively, thus constituting the cadre with the lowest gap (48.6%).
Figure 2. Staffing levels in 2012/2013, 2013/204 and WISN requirements.
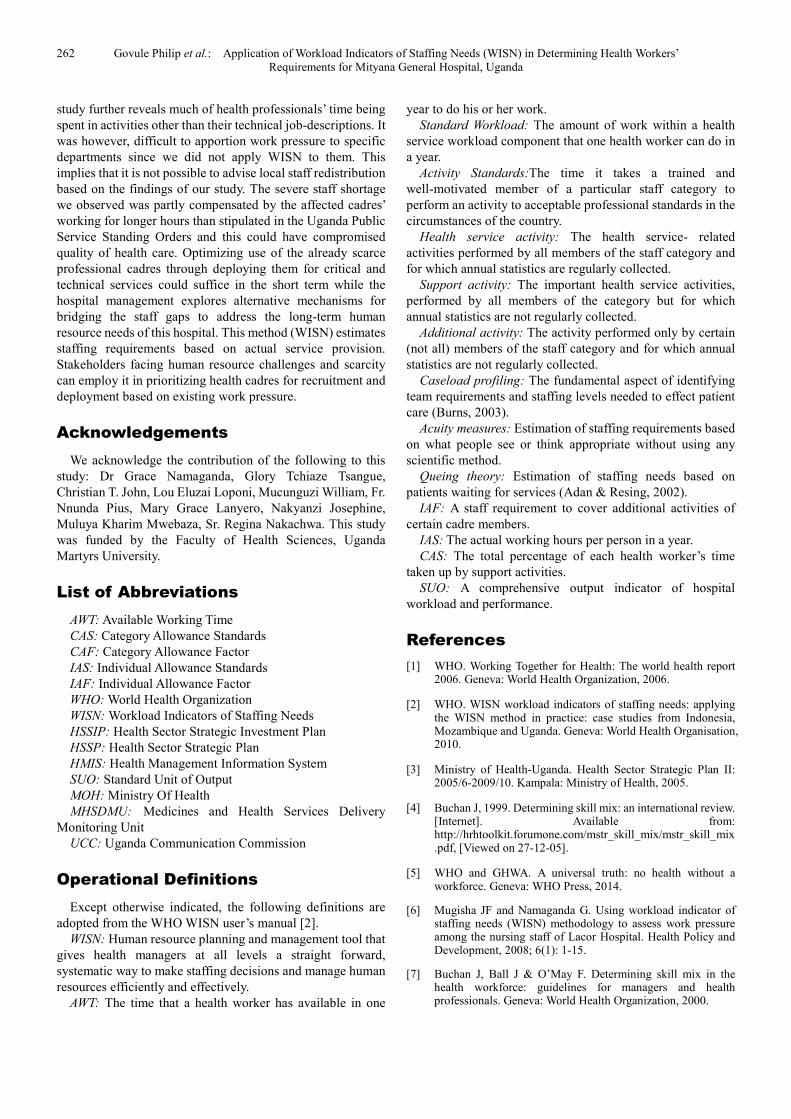
Figure 3. Work pressure in Mityana hospital.
The WISN ratio was obtained by dividing the existing staff
by the total required staff expressed as a percentage. The
results were then subtracted from 100 to get the workload
pressure. A low WISN ratio indicates high work pressure on
the staff. From figure 3, it is evident that clinical officers and
medical officers had the lowest WISN ratio and therefore were
under more work pressure than the other cadres. The
midwives and nurses had the least work pressure.
5. Discussion
An earlier WISN study conducted in Mbale and Mukono
districts had calculated the AWT based on standing orders of
the Ugandan Public Service and the Catholic Medical Bureau
[2]. The resultant AWT for nursing assistants (in hours) in that
study were comparable to ours. The difference in AWT for the
earlier studies and ours were not far apart. The AWTs were
1,624, 1,680; and 1,688 for medical officers, clinical officers;
and nurses and midwives respectively. On the other hand, a
study conducted in Lacor hospital [6] reports higher AWTs of
1,815.4 hours; and 1,884.0 hours for nurses and midwives;
and nursing assistants respectively. In the Lacor hospital study,
training days were not included in the calculation of AWT,
probably because no staff had gone on training during that
period, thus the higher estimate. In addition, Lacor hospital is
not a public health facility as such, not a subject of some

International Journal of Public Health Research 2015; 3(5): 254-263 261
policies and legislations related to work schedules for public
health workers. The Uganda Public Service Standing Order
[28] stipulates that ‘a public officer must undertake staff
development activities for a minimum of forty (40) hours in a
financial year to improve his or her competencies’. The use of
actual time taken to perform an activity rather than the
standard time, or not including that activity because it was not
done in that period may lower the total staff requirement
because it will mean calculating a required staff that is
necessary to continue performing in an environment which
denies them the right to go for training or take days off to rest.
The calculated staff requirements in Mityana hospital
considered all the official leaves, public holidays, trainings etc
as provided in the standing orders, because only then will they
be properly motivated and empowered (with knowledge and
skills) to provide quality service. Due to shortage, some staffs
were denied these rights inorder to improve staff availability.
If the staffs of the various categories were to use their time
mainly for the primary activities for which they were
professionally trained, the total staff requirement would not be
as high. In Mityana hospital, non-primary activities consumed
chunks of time of critical cadres like the medical officer.
Although additional activities such as operational research,
management meetings, staff meetings, and appraisals amongst
others are necessary for the smooth running of services, it is
obviously detrimental when large portion of a professional’s
time is spent on them: especially in contexts with scarce
professionals like Uganda. These findings were also supported
by the focus group discussions that were conducted for the
various cadres. One of such discussions with the midwives
revealed mismatch between number of mothers delivering
each day and availability of midwives, yet, despite the
shortage (of midwives), some midwives continued to be
assigned to perform other activities. In addition, this study
observes that even with the high workload at the maternity,
some midwives were assigned to be dispensing medicines due
to shortage in those departments. These facts are similar to
those of other WISN studies elsewhere in Uganda. A WISN
study in Lacor hospital (Uganda) [6] reports 17 midwives
involved in doing “non-midwifery work” like dispensing
medicines and performing nursing procedures in outpatient
department and general wards as a result of inadequate
nursing staff. This further worsened the shortage of midwives
in this hospital. Earlier WISN studies made similar revelations
elsewhere in Mozambique [28] and Indonesia [30]. Different
members of staff are required to perform primary, support and
additional services, with the number of staff required
increasing as additional workload increases. With the
exception of medical officers, the staff required for primary
activities in Mityana were higher than those required for
support and additional activities – an ideal situation. This is
required to be the general practice because the primary
activities are those for which the professional in each cadre
has been trained and recruited to perform. The major
involvement of the medical officers in other activities most of
the time has high quality implications. Additionally,
employing upto 22 medical officers just to perform additional
services is not only reflective of ineffective deployment but
adds to local brain waste in a context where this cadre is
scarcest. Other than thinking of additional medical officers,
the management of Mityana hospital should first consider
maximizing use of this ‘precious’ cadre in professional
engagements.
High gaps exist in required staff and the status quo. For
example in 2012/2013 there was a shortage of 33 clinical
officers. Though the staff level for this cadre was increased to
9 in 2013/2014, this increase reflected negligible addition
given the 31 more needed. The cadres like medical officers,
clinical officers and nurse assistants with more than 70% staff
shortages (each) is not surprising since (only) 63% of the
approved posts had been filled in Mityana hospital [31] –
implying that there was already a shortage of 37%. In addition,
this 37% shortage was based on the government of Uganda’s
estimation of staffing requirements using staff to population
ratio which unfortunately was calculated based on the 2010
population of 306,000 people [32] compared to the currently
over 800,000 people [31]. This implies that the 37% shortage
was not in consideration of the extra population and this
justifies the high staffing gaps we have highlighted. This calls
for relevant authorities to adjust staff to population health
worker needs to meet the taste of time as population changes.
In 2012/2013, the nursing assistants in Mityana were 11 – a
number that has regressed to 2 contrary to the other cadres
whose staffing levels are on the rise. This may be attributed to
the present policy to phase-out this cadre in Uganda that is
making nursing assistants to leave in pursuit of alternative
careers. In addition, those who reach retirement age are not
replaced. This seems to be quite detrimental to the hospital as
the study reveals that this staff category still shoulders high
workload and eradicating them may increase the pressure on
the existing staff who are already under much pressure.
Surprisingly, the nursing assistant, a cadre due for extinction
from Uganda’s health system still experiences higher
workload than the nurses. These findings are similar to that of
a study which reveals work pressure on nursing assistant as
twice higher than for nurses [6]. If left unattended to, the
resultant effects of this high work pressure may be similar to
that of a study which was conducted in Tanzania in 2008,
which reveals that shortage of health workers leads to high
work pressure which in turn leads to staff spending less time
on each activity than is set by activity standards [23]. This
indicates that the quality of services being delivered is even
below the locally accepted standards. The study [23] further
reveals that high workload pressure leads to poor health
workers’ attitude, lack of morale, absenteeism and passivity in
attending to patients. High workload pressure translates to
poor quality services and has negative impact on staff
motivation leading to high staff-turnover which in turn widens
the staff shortages [33].
6. Conclusions
This study revealed overall shortage of all cadres evaluated
– clinical officers and medical officers most affected. The
262 Govule Philip et al.: Application of Workload Indicators of Staffing Needs (WISN) in Determining Health Workers’
Requirements for Mityana General Hospital, Uganda
study further reveals much of health professionals’ time being
spent in activities other than their technical job-descriptions. It
was however, difficult to apportion work pressure to specific
departments since we did not apply WISN to them. This
implies that it is not possible to advise local staff redistribution
based on the findings of our study. The severe staff shortage
we observed was partly compensated by the affected cadres’
working for longer hours than stipulated in the Uganda Public
Service Standing Orders and this could have compromised
quality of health care. Optimizing use of the already scarce
professional cadres through deploying them for critical and
technical services could suffice in the short term while the
hospital management explores alternative mechanisms for
bridging the staff gaps to address the long-term human
resource needs of this hospital. This method (WISN) estimates
staffing requirements based on actual service provision.
Stakeholders facing human resource challenges and scarcity
can employ it in prioritizing health cadres for recruitment and
deployment based on existing work pressure.
Acknowledgements
We acknowledge the contribution of the following to this
study: Dr Grace Namaganda, Glory Tchiaze Tsangue,
Christian T. John, Lou Eluzai Loponi, Mucunguzi William, Fr.
Nnunda Pius, Mary Grace Lanyero, Nakyanzi Josephine,
Muluya Kharim Mwebaza, Sr. Regina Nakachwa. This study
was funded by the Faculty of Health Sciences, Uganda
Martyrs University.
List of Abbreviations
AWT: Available Working Time
CAS: Category Allowance Standards
CAF: Category Allowance Factor
IAS: Individual Allowance Standards
IAF: Individual Allowance Factor
WHO: World Health Organization
WISN: Workload Indicators of Staffing Needs
HSSIP: Health Sector Strategic Investment Plan
HSSP: Health Sector Strategic Plan
HMIS: Health Management Information System
SUO: Standard Unit of Output
MOH: Ministry Of Health
MHSDMU: Medicines and Health Services Delivery
Monitoring Unit
UCC: Uganda Communication Commission
Operational Definitions
Except otherwise indicated, the following definitions are
adopted from the WHO WISN user’s manual [2].
WISN: Human resource planning and management tool that
gives health managers at all levels a straight forward,
systematic way to make staffing decisions and manage human
resources efficiently and effectively.
AWT: The time that a health worker has available in one
year to do his or her work.
Standard Workload: The amount of work within a health
service workload component that one health worker can do in
a year.
Activity Standards:The time it takes a trained and
well-motivated member of a particular staff category to
perform an activity to acceptable professional standards in the
circumstances of the country.
Health service activity: The health service- related
activities performed by all members of the staff category and
for which annual statistics are regularly collected.
Support activity: The important health service activities,
performed by all members of the category but for which
annual statistics are not regularly collected.
Additional activity: The activity performed only by certain
(not all) members of the staff category and for which annual
statistics are not regularly collected.
Caseload profiling: The fundamental aspect of identifying
team requirements and staffing levels needed to effect patient
care (Burns, 2003).
Acuity measures: Estimation of staffing requirements based
on what people see or think appropriate without using any
scientific method.
Queing theory: Estimation of staffing needs based on
patients waiting for services (Adan & Resing, 2002).
IAF: A staff requirement to cover additional activities of
certain cadre members.
IAS: The actual working hours per person in a year.
CAS: The total percentage of each health worker’s time
taken up by support activities.
SUO: A comprehensive output indicator of hospital
workload and performance.
References
[1] WHO. Working Together for Health: The world health report 2006. Geneva: World Health Organization, 2006.
[2] WHO. WISN workload indicators of staffing needs: applying the WISN method in practice: case studies from Indonesia, Mozambique and Uganda. Geneva: World Health Organisation, 2010.
[3] Ministry of Health-Uganda. Health Sector Strategic Plan II: 2005/6-2009/10. Kampala: Ministry of Health, 2005.
[4] Buchan J, 1999. Determining skill mix: an international review. [Internet]. Available from: http://hrhtoolkit.forumone.com/mstr_skill_mix/mstr_skill_mix.pdf, [Viewed on 27-12-05].
[5] WHO and GHWA. A universal truth: no health without a workforce. Geneva: WHO Press, 2014.
[6] Mugisha JF and Namaganda G. Using workload indicator of staffing needs (WISN) methodology to assess work pressure among the nursing staff of Lacor Hospital. Health Policy and Development, 2008; 6(1): 1-15.
[7] Buchan J, Ball J & O’May F. Determining skill mix in the health workforce: guidelines for managers and health professionals. Geneva: World Health Organization, 2000.
International Journal of Public Health Research 2015; 3(5): 254-263 263
[8] Delanyo D. Wastage in the health workforce: some perspectives from African countries. Human Resources for Health Journal, 2005; 3: 6.
[9] Namaganda G. Determining staffing levels and mix of UCMB affiliated hospitals. Health Policy and Development, 2004; 2 (3) 236-242.
[10] Derksen DJ and Whelan EM. Closing the health care workforce gap-reforming federal health care workforce policies to meet the needs of the 21st century, 2009. [Online] Available at: http://www.americanprogress.org/issues/2010/01/pdf/health_care_workforce.pdf, [Accessed on 24th February 2014].
[11] Ncube M, Abou-Sabaa A, Lufumpa CL & Soucat A. Health in Africa over the next 50years. African Development Bank, 2013. [Online]. Available at: http://www.afdb.org/fileadmin/uploads/afdb/Documents/Publications/Economic_Brief_-_Health_in_Africa_Over_the_Next_50_Years.pdf, [Accessed on 7th September 2013].
[12] Ministry of Health. Uganda health system assessment, 2011. [Online]. Available at: http://health.go.ug/docs/hsa.pdf, [Accessed 25 February 2014].
[13] Aluttis C, BishawT and Frank MF. The workforce for health in a globalized context-global shortages and international migration. Global Health Action, 2014; 7: 23611.
[14] Elfaki N. Training course on workload indicators of staffing need (WISN) tool, 2013. [Online]. Available at: http://www.who.int/workforcealliance/media/news/2013/WISNTOTCourseBrochure.pdf, [Accessed on 15th February 2014].
[15] GoU. Local Governments Act, 1997. [Online] Available at: http://www.ulii.org/ug/legislation/consolidated-act/243, [Accessed on 25th February 2014].
[16] Matsiko C. Health system strengthening/ capacity plus, 2010. [Online] Available at: www.capacityplus.org/category/blog.../health-systems-strengthening?pag, [Accessed on 25th February 2014].
[17] Ministry of Health-Uganda. Human resources for health policy. policy. Kampala: MoH-Uganda, 2006.
[18] Ship PJ. Workload indicators of staffing needs: a manual for implementation. Geneva:World Health Organisation, 1998.
[19] Hagopian A, Mohanty MK, Das A, House PJ. Applying WHO’s work force indicators of staffing need’ (WISN) method to calculate the health worker requirements for India’s maternal and child health service guarantees in Orissa State. Health Policy Plan, 2012; 27:11–18.
[20] Hossain B & Alam SA. Likely benefit of using workload indicators of staffing need (WISN) for human resources management and planning in the health sector of Bangladesh. Hum Resour Health ,1999; 3:99–111.
[21] Musau P, Nyongesa P, Shikhule A, Birech E, Kirui D, Njenga M, Mbiti D, Bett A, Lagat L & Kiilu K. Worlkload indicators of staffing need method in determining optimal staffing levels at Moi Teaching and Referral Hospital. East African Medical Journal, 2008; 85(5): 232-239.
[22] McQuide PA, Riitta LK & Forster N. Applying the workload indicators of staffingneed (WISN) method in Namibia: challenges and implications for human resources for health policy. Human Resource for Health, 2013; 11: 64.
[23] Nyamtema AS, Urassa DP, Massawe S, Massawe A, Lindmark G, Van Roosmalen J. Staffing needs for quality perinatal care in Tanzania. PubMed, 2008; 12(3): 113-24.
[24] Namaganda G, 2006. Testing the WISN method in Mbale and Mukono districts, Uganda, 2006: In [2].
[25] Minsitry of Health-Uganda. Health Sector Strategic and Investment plan: promoting people’s health to enhance socio-economic development, 2010/11-2014/15. Kampala: Ministry of Health-Uganda, 2010.
[26] Ministry of Health. Human resources for health audit report. Kampala: Ministry of Health, 2010.
[27] Government of Uganda. The Uganda public service standing orders. Kampala: Government of Uganda, 2010.
[28] Vio, F., Applying the WISN method in Nampula and Sofala provinces, Mozambique, 2004: In [2].
[29] Seran et al. Decentralized application of WISN methods in NUSA Tenggara Timur Province, Indonesia, 2008: In [2].
[30] MHSDMU. Rural communications development funds project in Mityana report. Medicines & Health Service Delivery Monitoring Unit, Kampala, Uganda Available at: http://hmu.go.ug/Docs/MITYANA FINAL COMPLETE REPORT.pdf, [Accessed on 12th March 2014].
[31] UCC. Rural communications development fund project report, 2010. [Internet]. Available at: http://www.ucc.co.ug/download/MITYANA.pdf, [Accessed on 13th March 2014].
[32] Das, S. et al. A study to calculate nursing staff requirement for the marternity ward of Medical college Hospital, Kolkata Applying WISN Method. IOSR Journal of Dental and Medical Sciences (IOSR-JDMS), 2013, 8(3), pp.1-7.
[33] Humphries N et. al., Quality of care and health professional burnout: narrative literature review, Emerald Group publishing limited, Available at: https://zenodo.org/record/10445/files/Quality_of_care_and_health_professional_burnout_narrative_literature_review.pdf





























